
Abstract
Background
Injuries to lower extremities are common in team sports such as soccer, basketball, volleyball, football and field hockey. Considering personal grief, disabling consequences and high costs caused by injuries to lower extremities, the importance for the prevention of these injuries is evident. From this point of view it is important to know which screening tools can identify athletes who are at risk of injury to their lower extremities.
Objective
The aim of this article is to determine the predictive values of anthropometric and/or physical screening tests for injuries to the leg, anterior cruciate ligament (ACL), knee, hamstring, groin and ankle in team sports.
Methods
A systematic review was conducted in MEDLINE (1966 to September 2011), EMBASE (1989 to September 2011) and CINAHL (1982 to September 2011). Based on inclusion criteria defined a priori, titles, abstracts and full texts were analysed to find relevant studies.
Results
The analysis showed that different screening tools can be predictive for injuries to the knee, ACL, hamstring, groin and ankle. For injuries in general there is some support in the literature to suggest that general joint laxity is a predictive measure for leg injuries. The anterior right/left reach distance >4cm and the composite reach distance <4.0% of limb length in girls measured with the star excursion balance test (SEBT) may predict leg injuries. Furthermore, an increasing age, a lower hamstring/quadriceps (H:Q) ratio and a decreased range of motion (ROM) of hip abduction may predict the occurrence of leg injuries. Hyperextension of the knee, side-to-side differences in anterior-posterior knee laxity and differences in knee abduction moment between both legs are suggested to be predictive tests for sustaining an ACL injury and height was a predictive screening tool for knee ligament injuries. There is some evidence that when age increases, the probability of sustaining a hamstring injury increases. Debate exists in the analysed literature regarding measurement of the flexibility of the hamstring as a predictive screening tool, as well as using the H:Q ratio. Hip-adduction-to-abduction strength is a predictive test for hip adductor muscle strain. Studies do not agree on whether ROM of the hamstring is a predictive screening tool for groin injury. Body mass index and the age of an athlete could contribute to an ankle sprain. There is support in the literature to suggest that greater strength of the plantar flexors may be a predictive measure for sustaining an ankle injury. Furthermore, there is some agreement that the measurement of postural sway is a predictive test for an ankle injury.
Conclusions
The screening tools mentioned above can be recommended to medical staff and coaches for screening their athletes. Future research should focus on prospective studies in larger groups and should follow athletes over several seasons.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1. Introduction
Injuries to the lower extremities are common in team sports such as soccer, basketball, volleyball, football and field hockey.[1–3] For example, an anterior cruciate ligament (ACL) injury is a common injury to the knee in soccer. In female and male soccer players the injury rate per 1000 athlete exposures of ACL injuries is 0.28 and 0.09, respectively.[4] An incidence of 1.6 per 1000 player hours is reported in female handball players,[5] and in soccer players, 14–32% of all acute injuries are knee injuries.[6–11] Hamstring strains occur frequently in Australian football and soccer especially.[8–11] In basketball, soccer and volleyball a large amount of injuries involve ankle sprains.[12]
The personal and professional impairment of athletes caused by injuries can result in high costs for athletes and for society.[13] For instance, a severe knee injury might limit future sport participation. The development of knee osteoarthrosis is a long-term consequence of an ACL injury, which can cause permanent disability for the athlete.[14] An ankle sprain on the other hand can result in decreased ankle range of motion (ROM), persistent pain, swelling and chronic ankle instability,[15] whereas a hamstring strain can result in chronic symptoms and reduced performance as well.[16] Another negative consequence of an ACL injury, hamstring injury and an ankle sprain is the chance of re-injury.[16–25] In the US the costs of ACL injuries are estimated at $US1 billion per year[26] and the cost of treating ankle sprains is estimated at $US2 billion dollars per year.[27] Considering personal grief, disabling consequences and high costs caused by injuries, the importance of prevention is evident.
Development of screening tools may be a crucial component in preventing lower extremity injuries. Screening tools can be used preseason to identify athletes that are at high risk of developing an injury.[28,29] With this information, training programmes can be adjusted to the individual athlete. There is a need for the development of simple, low-cost screening tools, which can be used on a large scale in the clinic or the field.[29] There are numerous studies that have conducted prospective trials to find risk factors for predicting injury in athletes.[16,19,30–43] However, as it is important to know which of these screening tools are indeed reliable, valid and predictive for injury, the purpose of this systematic review was to identify tools for the prevention of lower extremity injuries and describe their reliability, validity, sensitivity and specificity.
2. Methods
2.1 Literature Search
To find articles concerning anthropometric and/or physical screening tools that can predict the proneness of injury in team sports, a systematic literature search was conducted in MEDLINE (1966 to September 2011), EMBASE (1989 to September 2011) and CINAHL (1982 to September 2011). A combination of the following search terms was used: group (i).‘hip injuries’, ‘knee injuries’, ‘ankle injuries’, ‘lower extremity injuries’, ‘athletic injuries’; group (ii).‘soccer injuries’, ‘basketball injuries’, ‘volleyball injuries’, ‘hockey injuries’, ‘team sports’, ‘ball sports’; group (iii).‘anthropometry’, ‘fatigue’, ‘musculoskeletal system’, ‘motor control’, ‘biomechanics’, ‘observational’, ‘joint instability’, ‘kinetics’, ‘core stability’; group (iv).‘predictive value of tests’, ‘sensitivity and specificity’, ‘reproducibility of results’, ‘reliability’, ‘validity’; and group (v).‘screening tool’, ‘screening test’, ‘risk factors’, ‘preseason screening’, ‘proneness’, ‘mass screening’, ‘risk assessment’, ‘screening’ and ‘prospective studies’. Within the groups, the search terms were connected with OR and between the groups with AND. In addition, a hand search was done on the reference lists in included articles. The results of the three searches were taken together and duplicates were filtered out. Furthermore, reference lists were screened to find additional articles.
2.2 Literature Selection
The titles and abstracts of the articles that were identified were reviewed by the first author (J.M.D.) for potential relevance. The full text of possibly relevant articles was analysed by two reviewers for final inclusion (J.M.D. and A.B.), based on the following inclusion criteria: (i) full text; (ii) published in English, German or Dutch; (iii) acute musculoskeletal injuries to lower extremities; (iv) athletes participating in ball team sports; (v) average age of athletes (≥13 years); (vi) physical screening tests and/or anthropometry; (vii) reliability, validity, sensitivity or specificity described in numbers; and (viii) predictive value described in numbers.
If disagreements on inclusion were present a third reviewer (K.A.P.M.L.) decided whether the article had to be included or not.
2.3 Data Extraction
Data were extracted by the first author from each included article. The subject characteristics, screening tool, reliability, validity, sensitivity or specificity, outcome measure, injury definition and measure of association with injury (e.g. odds ratio [OR] or relative risk [RR]) were summarized.
2.4 Methodological Quality
To examine the methodological quality, a modified version of the Cochrane Group on Screening and Diagnostic Test Methodology (Cochrane methods) was used.[44] Two authors assessed the quality of the included studies (J.M.D. and A.B.). The first four questions were replaced for a score of level of evidence defined by the Oxford Center for Evidence-Based Medicine.[45] The range of this score was from 1 to 5; 1 was the lowest score and 5 the highest. The design, selection criteria, setting, demographic information, description of the screening tool, reproducibility of the screening tool and percentage missing were used to score methodological quality. Furthermore, items about statistical analysis were added as well as outcome and confounders. The maximal score that could be reached was 16.
3. Results
3.1 Search Findings
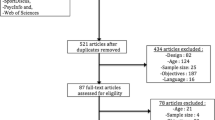
Appendix 1 in the Supplement Digital Content (http://links.adisonline.com/SMZ/A12) shows a summary of the search strategy and figure 1 shows the flow diagram of the search strategy. The assessment of the methodological quality of the included studies is shown in table I. The mean score was 15.5 (range 13–16). Table II shows the study characteristics of these studies.

Flow chart of search strategy.

Methodological quality of studies

Study characteristics of the studies included
3.2 Predictive Tools for Lower Extremity Injury
Some studies analysed screening tools for lower extremity injury in general (see table II for definitions of all injuries). The traumatic or acute injuries that were registered in the studies were contusion of the foot, calf, knee or thigh, partial rupture of the plantar aponeurosis, ankle sprain, total rupture of the Achilles tendon, ACL injury, medial collateral ligament injury, lateral collateral ligament injury, hamstring and groin strain,[69] fracture, dislocation, ligament sprain, muscle strain, contusion, tendinitis/bursitis and other type of injuries to the foot, ankle, leg, knee, thigh front, hamstring, groin and back.[68] In one study, the type of injuries were measured but not shown; however, ankle sprain and knee sprain were mentioned as examples of registered injuries.[35] Different screening tests were described to predict injuries to the lower extremities. In soccer players, two studies showed significant predictive values for increased generalized joint laxity (OR 5.3, p < 0.00;[68] OR 3.10, p = 0.02).[69] General joint laxity was determined as an overall score of joint laxity of the fingers, thumb, elbow, knees and trunk measured using the Beighton method.[68] The star excursion balance test (SEBT) was suggested to predict lower extremity injury in high-school basketball players (OR 2.50; p < 0.05) and specifically in girls (OR 6.5; p < 0.05).[35] In football, an increasing age placed players at a greater risk of injury to the lower extremities (OR 1.1 per year; 95% CI 1.0, 1.1; p = 0.05).[20]
3.3 Predictive Tools for Anterior Cruciate Ligament (ACL) Injury
Multiple significant screening tests were described for measuring the risk for sustaining an ACL injury. It has been shown that risk of an ACL injury could be predicted by hyperextension of the knee (OR 4.78; 95% CI 1.24, 18.44; p = 0.02) and side-to-side differences in anterior-posterior tibiofemoral translation (OR 4.03; 95% CI 1.68, 9.69; p = 0.00) in female soccer and basketball players.[39]
Knee and hip joint flexion-extension and adduction-abduction on a drop vertical jump task in female basketball and soccer players were analysed in another study.[37] The most important finding was that knee abduction moment was 2.5-fold greater in ACL-injured athletes (p < 0.00) and knee abduction moment predisposed the occurrence of an ACL injury with 73% specificity and 78% sensitivity.[37]
Although the Landing Error Scoring System (LESS) was described as a reliable and valid method,[76] predictive values for ACL injury could not be found in soccer, football, rugby, field hockey, basketball, gymnastics, lacrosse and volleyball players.[70]
3.4 Predictive Tools for Knee Injury
A definition of knee injury is shown in table II. Two studies described screening tools for knee injuries in general.[30,74] In one study, a clinical examination was performed by male football players.[30] However, none of the measured factors could predict acute knee injuries.[30] Height was a predictive screening tool for knee ligament injuries in Australian football players.[74]
3.5 Predictive Tools for Hamstring Strain
The included studies used different screening tools and showed mixed results. Three studies measured flexibility of the hamstrings in adult Australian football players but used different tests.[16,36,66] The sit and reach, active knee extension, passive straight leg raise, slump, active hip internal rotation ROM, active hip external rotation, dorsiflexion lunge test, lumbar spine extension ROM and the modified Thomas test were assessed.[36] Furthermore, the toe-touch test, end-range flexion hip, lumbar flexion, ratio lumbar spine and flexion-to-hip flexion were used to measure flexibility,[66] while a clinical examination, which included measuring the hamstring length and the hip ROM, were assessed as well, in combination with a Nordic hamstring strength test.[16] In addition, the thigh muscle strength and isokinetic strength testing of the hamstring and quadriceps muscles of both legs in Australian Rules football players were analysed.[20,65] Age was a significant screening tool for hamstring strains in football players (OR 1.4 [1 year]; 95% CI 1.2, 0.4; p < 0.00).[20] also, a decreased flexibility of the hamstring and an age older than 23 years were predictive for hamstring injuries in adult football players (RR 0.3; 95% CI 0.1, 0.8; p = 0.02 and RR 3.8; 95% CI 1.1, 14.0; p = 0.04, respectively).[36] However, flexibility of the hamstring was shown to be not significant as a screening tool in soccer players.[16] Another study also suggested that flexibility cannot predict risk on hamstring strain in Australian Rules football players.[66] The hamstring/quadriceps ratio (H : Q) was a significant predictor of a hamstring strain in Australian football players (area = 0.87, p = 0.01, 95% CI 0.71, 1.03; area = 0.88, p = 0.01, 95% CI 0.73, 1.03, respectively).[71]
3.6 Predictive Tools for Groin Injury
The definition of groin injury is described in table II. Screening tools to predict groin injuries were analysed in soccer,[41] football[20] and hockey players.[72,75] Hip adduction-to-abduction strength ratio was a significant predictor of a future adductor strain (RR 17 [based on a hip adduction of <80% of abduction strength]; p = 0.00).[72] Furthermore, a decreased ROM of hip abduction for groin strains was a predictive screening tool for a groin injury (OR 0.9 [1°]; 95% CI 0.8, 1.0; p = 0.05).[20]
From the literature, it was not clear as to whether hip flexibility was a significant screening tool for groin injuries.[20,72,75]
3.7 Predictive Tools for Ankle Sprain
The definition of ankle sprain for each of the included studies is described in table II. A high variation in postural sway (anteroposterior and mediolateral direction) was shown to be predictive for ankle injuries in male high-school basketball players (OR 1.22, p = 0.01; OR 1.22, p < 0.00).[38] Furthermore, a greater postural sway measured with unilateral ankle tests showed significant predictive values in high-school basketball players (OR 10.2; p = 0.00).[31] The unilateral ankle test was a modified Romberg test on a force platform and the compilation sway score on this test was an indication of overall ability to balance.[31] In high-school, university and intercollegiate athletics postural sway measured by a positive single leg balance (SLB) test was predictive of an ankle sprain after controlling for gender, sport, school, previous history of ankle sprain and taping (OR 2.54; 95% CI 1.02, 6.03; p < 0.05).[73] In Australian football players, an above average mean balance score of both limbs was a significant predictor for ankle ligament injury (OR 2.44; 95% CI 1.91, 7.48; p < 0.05).[74] No significant predictive values for postural sway were measured in volleyball players.[32]
The included studies also showed different results for ROM as a screening test. In soccer players (supination OR 1.21, p = 0.15; pronation OR 0.98, p = 0.95; dorsiflexion OR 0.94, p = 0.79)[19] and in basketball players (knee extended p = 0.71; knee flexed p = 0.30) the ROM of the ankle was not a predictive screening task.[31] However, in volleyball players, the ROM in dorsiflexion was shown as a significant screening tool (OR 0.63; 95% CI 1.04, 1.43; p < 0.05).[32] Body mass index (BMI) and age contributed to an ankle injury in basketball, volleyball and soccer athletes (p < 0.10).[67]
4. Discussion
The main purpose of this systematic review was to illustrate the predictive values for injury of lower extremity tests and to select screening tests that can be used in the clinic or field to identify athletes at risk of injury to the lower extremities. In addition, the reliability, validity, sensitivity and specificity of these tests was described. The main findings of our review show that, per body part, several screening tools are available to identify athletes at risk for injury.
4.1 Methodological Quality
The mean score on the modified Cochrane methods scoring list was 15.5 (range 13–16). All studies showed high scores. Approximately half of the studies did not describe the most important confounders and how they were taken into account. In addition, some studies showed a lack of demographic information, a lack of detailed description of screening tool to allow replication of the test, statistical analysis, reliability of the screening tool and definition of outcome. No specific checklist for this current topic of interest was available to the knowledge of the authors; therefore, a combination of items from the Cochrane and Oxford Center for Evidence-based Medicine checklists was made.[44] These checklists are well reported and accepted for use in methodological quality assessments.
4.2 Predictive Tools for Lower Extremity Injury
One study showed the SEBT was reliable and predictive of lower extremity injury in high-school basketball players.[35] Data were collected during one basketball season, therefore it might be difficult to generalize these results; however, the results of this study are promising.
In female senior soccer players, general joint laxity, a high performance in the functional test square hop and an age over 25 years were predictive for leg injuries.[68] Moreover, the square hop test showed an acceptable reliability. Although reliability of general joint laxity was not reported in this study, another study showed good reliability of this screening tool;[27] however, the ORs were significant but considering the skewness of the distributions of elite and non-elite players, no conclusions could be made.[68] Furthermore, hyperextension of the knee joint, a low postural sway, side-to-side differences in hamstring flexibility and ankle dorsiflexion can cause a greater risk of traumatic leg injuries in female soccer players.[69] Taking the reliability of the measurements into account, postural sway was the only screening test that was not reliable. In summary, there was agreement that general joint laxity was a predictive measure for injuries to the lower extremities.
It is not clear from these studies what type of specific injury the measures are exactly related to. This makes it difficult to conclude which screening tools are related to which injury. It is therefore difficult to make recommendations on screening tests that should be used by trainers in the field.
An increasing age was an indicator for being more susceptible to injury to the lower extremities in football players.[20] A limitation of this study was that minor injuries could have been underestimated due to injury registration problems. However, the most important limitation was that only 50% of the athletes completed all of the tests; consequently, the results of this study should be interpreted with care.
Studies on the reliability of screening tools that described no prospective relation to injury were not included in this review because of the inclusion and exclusion criteria used. Before a screening tool can be used in a prospective cohort design, reliability of the tool should be analysed. Therefore, we do want draw attention to this aspect, as these studies provide valuable information for future research. One study measured the inter- and intrarater reliability of nine screening tests, included in a test battery, in male elite soccer players.[3] The included tests were the deep squat test, one-legged squat test, inline lunge test, active hip flexion test, straight leg raise test, push-up test and diagonal lift test. The intrarater reliability of this test battery was good on both occasions (intraclass correlation coefficient [ICC] 0.80 and ICC 0.81). There were no significant differences between the test occasions (p = 0.31) and between the raters at the two test occasions, indicating good inter-rater reliability.[3] In Australian football clubs the inter-rater and test-retest reliability of lower extremity musculoskeletal screening tests were examined.[28] The sit and reach, active knee extension, passive straight leg raise, slump, active hip internal ROM, active hip external ROM, lumbar spine extension ROM and the modified Thomas test were evaluated. The inter-rater reliability of all tests was very good to excellent (ICC 0.88–0.97). Furthermore, the tests demonstrated a good test-retest reliability (ICC 0.63–0.99).[28] Another study analysed the inter- and intraobserver reliability of the modified Thomas test, hip internal and external rotation, combined elevation, ankle dorsiflexion lunge, bridging hold, prone four-point hold and calf heel raises.[29] The tests in general showed a poor interobserver reliability, four of ten tests had an ICC above 0.80 (ICC 0.27–0.99), and a higher intrarater reliability, nine tests scored an ICC above 0.80 (ICC 0.56–0.99).[29] Because the reliability of this test battery is not satisfactory, care must be taken in using it in prospective design studies to find screening tools for injuries to the lower extremities.
Based on this review, there is some support in the literature to suggest that general joint laxity is a predictive measure for leg injuries. The anterior right/left reach distance >4 cm and the composite reach distance <4.0% of limb length in girls measured with the SEBT may predict leg injuries. Furthermore, an increasing age, a lower H : Q ratio, and a decreased ROM of hip abduction may predict the occurrence of leg injuries. All these screening tools can be recommended to medical staff and coaches.
4.3 Predictive Tools for ACL Injury
Different tests were suggested as predictive measures for an ACL injury. Knee hyperextension and side-to-side differences in anterior-posterior tibiofemoral translation were shown as significant and reliable screening tools for ACL injury.[39] These results are difficult to generalize, because confounding variables were not taken into account.
Measuring neuromuscular control and joint load was a good and reliable tool to predict ACL injury risk in soccer, basketball and volleyball.[37] That is, an increased valgus motion and valgus moments at the knee joint during the impact phase of jump landing tasks were able to predict ACL injury in female athletes. Hewett et al.[37] admit that there are confounding variables and although they describe the neuromuscular parameters as the most important determinant for an ACL injury, generalizability is still a problem in this study.
Generalized joint laxity was a significant predictor for an ACL injury (RR 2.8) in another large prospective study that was excluded due to our criteria.[77] This is in agreement with Myer et al.[39] Furthermore, a small femoral notch width and, in women, a higher than normal BMI (RR 2.0) and KT-2000 arthrometer values that were 1 standard deviation or more above the mean were shown as significant screening tools in military recruits.[77] The presence of more than one of these screening tools greatly increased the RR of ACL injury. These results indicate that, potentially, these screening tests can be used in team sport athletes as well.
The reliability and validity of screening tests for ACL injury is analysed by a few studies that were excluded in this review, since they did not describe a predictive value. In basketball players, a two-dimensional (2D) video analysis showed a good correlation to excessive knee valgus on a sidestep (r2 = 0.58) and a side jump task (r2 = 0.64).[46] Another study also found correlates to laboratory-based measures, which could predict a high knee valgus with 73% sensitivity and 70% specificity in female basketball and soccer players.[34] Although knee valgus moment is predictive for an ACL injury,[37] Myer et al.[34] and McLean et al.[46] showed no direct relation between a 2-D video analysis and an ACL injury. Acceptable rater and inter-rater reliability (kappa [κ] value 0.75–0.85) and specificity (60–72%) of observational risk screening was shown; however, sensitivity values were insufficient (67–87%).[48] Sensitivity had a priority over specificity in this study; consequently, the desired level of sensitivity was 80% or higher, and that of specificity 50% or higher.[48] This explains why sensitivity values were indicated as insufficient. The inter-rater reliability and the criterion validity of the LESS were measured as well.[76] The LESS is a jump-landing assessment tool and a screening tool to identify athletes at potential risk for ACL injury. The inter-rater item reliability between expert rater versus novice rater showed moderate to excellent κ values (0.46–0.88).[76] The overall LESS score showed a good reliability (ICC 0.84; p < 0.001). Furthermore, the validity of the LESS was moderate to excellent.[76] However, it should be mentioned that only a significant phi correlation between LESS scores and 3-D scores was found for the item knee valgus ROM.[76] Although other measured items showed no significant phi correlation between LESS scores and 3D scores, they showed moderate to excellent agreement (84–100%).[76] In middle- and high-school soccer and basketball players the reliability of 3-D motion analysis was studied.[78] Kinematic and kinetic variables were measured during landing in young athletes. Most of these variables showed an excellent to good reliability (ICC 0.75–0.96).[78] These results suggest that this screening tool might help in identifying potential mechanisms related to injury risk factors.[78] In summary, the LESS score and landing 3-D motion analysis are reliable tools.
What is of note, is that two of three studies regarding ACL injury risk factors included in this systematic review examined female athletes only. Although female athletes are at a greater risk of sustaining an ACL injury, the risk for male athletes should not be neglected. The number of male athletes that sustain an ACL injury is still certainly high.[79]
Based on this review, hyperextension of the knee, side-to-side differences in anterior-posterior knee laxity and differences in knee abduction moment between both legs, are suggested to be predictive tests for sustaining an ACL injury and can be recommended to medical staff and coaches.
4.4 Predictive Tools for Knee Injury
A large cohort study on screening tests for acute knee injuries showed that a simple screening test such as a clinical examination, was not able to predict acute knee injuries in male football players, also, reliability of the clinical examination was analysed before using it in a prospective design (κ = 1.00).[30] Possibly, more advanced screening tests should be able to predict acute knee injuries. Acute knee injuries included dislocations, meniscus tears, cartilage lesions and sprains.[30] In addition, in Australian football players, height was suggested to be predictive,[74] more specifically, taller players were at risk of injury; however, injury rate could have been underestimated. Moreover, the power of the study was not enough to identify a small-to-medium effect.[74]
Based on this review, measuring height can be recommended as a screening tool for knee ligament injury.
4.5 Predictive Tools for Hamstring Strain
An age older than 23 years and the flexibility of the hamstring were shown to be reliable predictors for hamstring injury in Australian football players.[36] The RR was measured instead of OR. Considering the small number of observed hamstring injuries (n = 20), the power of the study was not high, therefore no causality between screening tests and injuries could be determined.[36] Additionally, age was a significant predictor of a hamstring injury in football players.[20] Considering the limitations of this study, the results should be interpreted with care. The study of Engebretsen et al.[16] was comparable in design with other studies on screening tools for acute knee injuries, groin injuries and acute ankle injuries.[19,30,41] The screening tasks used in this study (Nordic hamstring strength test and clinical examination) were not able to identify the athletes at risk of hamstring injury in male football players. The clinical examination included testing the hamstring flexibility using the passive knee extension test and, in this case, measurements of hamstring flexibility were not able to predict a hamstring injury in contrary to the results of Gabbe et al.[36] Furthermore, flexibility of the hamstring measured by the toe-touch test was not able to predict the occurrence of a hamstring injury.[66] It may be that the toe-touch test is not the most valid method to measure risk of a hamstring injury, because it measures flexibility in end range. A second limitation of the study was that only a small number of hamstring strains occurred, resulting in low power.[66]
In one study, there was no significant relation between H : Q strength ratio and hamstring injury shown.[65] This study only compared injured and non-injured athletes and looked at significant differences;[65] therefore, no conclusions can be made about the risk of sustaining groin injuries; further research is needed in this area. In contrary to the study of Bennell et al.,[65] a low H : Q ratio significantly predicted hamstring injury in Australian football players.[71] Although not reported in this study, reliability can be assumed and was supported in previous studies.[80] In the study of Cameron et al.,[71] areas under the receiving operating characteristic (ROC) curves were calculated. When the area value was higher than 0.8, a test had good predictive power. The H : Q ratio showed a value above 0.8 of the area under the ROC curve (0.88). These researchers recommended the use of the thigh muscle strength test to predict risk of hamstring injury in the field.[71]
In conclusion, based on this review, there is some evidence to suggest that an increase of age is an indicator for sustaining a hamstring injury and this should be recommended to medical staff and coaches. However, debate exists in the analysed literature that the flexibility of the hamstring, as well as the H : Q ratio, should be used as predictive screening tools also.
4.6 Predictive Tools for Groin Injuries
Isometric testing of the adductor muscles was not able to predict acute groin strains in soccer players.[41] In addition, the intertest reliability of this test was poor. However, it should be noted that only 22 acute time-loss injuries were reported, therefore the results should be interpreted with caution.[41] This study differed from the study of Engebretsen et al.,[16] as all groin injuries were included. This could potentially explain the differences in results between the studies.
A second study found that peak isometric torque and total abduction (sum of unilateral measurements) flexibility could not predict groin injuries in ice-hockey players.[75] Considering the fact that a selection bias may have occurred that caused an underestimation of the relation between peak isometric torque and total abduction flexibility and groin injuries, no conclusions can be made.[75]
Hip adduction-to-abduction strength was a reliable test and could predict hip adductor muscle strain in ice-hockey players.[72] However, in this study, only eight athletes with hip adductor muscle strains were registered; consequently, the results should be taken with care.
In football, decreased ROM in hip abduction showed sufficient reliability and was a significant screening test for groin strains.[20] Considering the limitations of this study, these results should also be interpreted with care.
In summary, based on this review, hip-adduction-to-abduction strength is a predictive test for hip adductor muscle strain. Studies do not agree on whether ROM of the hamstring is a predictive screening tool for groin injury.
4.7 Predictive Tools for Ankle Sprain
In male basketball, soccer and volleyball athletes it was suggested that a Q-angle test was not able to predict an ankle sprain injury.[67] No controlling for confounding variables was performed in this study, therefore results should be used carefully.[67]
Measuring balance prior to season could predict the chance of ankle sprain injury in high-school male and female basketball players.[31] The reliability of balance measurement tools was measured in this study and the test-retest reliability showed varying ICC’s (0.42–0.88).[31] The compilation score was the most reliable (0.88) and, consequently, this score was used to measure postural sway in this study.[31] However, this score described an overall balance ability, so further research is necessary to develop a reliable and valid method to measure postural sway in individual limbs. A high variation of postural sway in anteroposterior and mediolateral directions showed an acceptable reliability and could partly predict the increased risk of ankle injury in basketball players; nevertheless, it is important to note that the ORs were relatively low (OR 1.22, p < 0.00; OR 1.22, respectively).[38] This study did take confounding variables into account. The one-legged standing test used in this study could be used by basketball trainers to predict which athletes are at risk of an ankle injury.[38] Furthermore, postural sway measured by the SLB test could predict ankle sprain in high-school university and intercollegiate athletics. The confounding variables gender, sport, school, previous history of ankle sprain and taping were taken into account.[73] Moreover, the SLB test was shown to be a reliable test and the inter-rater reliability was good (κ = 0.90; p < 0.00).[73] In contrary to the findings in other included studies, the postural sway of professional volleyball players, measured by postural dynamic balance testing, was not identified as a significant screening tool.[32]
Five of the included studies measured postural sway; however, as explained, different methods are used. This could explain the inconsistent findings. Four studies showed postural sway as a predictive test for ankle injury[31,38,73,74] and one study did not.[32]
Ankle plantar flexion strength and a decreased dorsiflexion ROM predicted an ankle sprain injury in volleyball players.[32] Acceptable reliability of the Biodex Stability System (BSS) was shown in earlier studies.[81] Limitations of this study were a small sample size (n = 38) and eccentric strength of the plantar and dorsal flexors were not measured. Measuring the eccentric strength of the plantar and dorsal flexors could help in predicting the risk on ankle sprains;[32] hence, in future research, the predictive value of eccentric strength should possibly be evaluated.
In Australian football players, an above average mean balance score of both limbs was a reliable and significant predictor for ankle ligament injury.[74]
Although studies that described reliability but showed no predictive value of a screening tool were not included, it is important to mention that the test-retest reliability of ankle injury risk factors was analysed.[27] Generalized joint laxity, ankle ligamentous stability and ankle strength were suggested as reliable measures in healthy college-age athletes and were measured before and after the season (r > 0.75; p < 0.05). However, ROM measurements were not reliable.[27]
Based on this review, the BMI and age of an athlete could contribute to an ankle sprain. There is support in the literature to suggest that the higher strength of the plantar flexors may be a predictive measure for sustaining an ankle injury. Furthermore, there is some agreement that the measurement of postural sway is a predictive measure for an ankle injury.
5. Limitations
This systematic review provides a good overview of the predictive values of simple screening tools that are presently described in the literature; however, there are some limitations that need to be addressed.
First, there was a variety of tasks, playing levels of sport, age and type of team sports included in this review. Also, studies with both male and female athletes were included. This makes it difficult to compare the results and to make recommendations; consequently, further research should focus on measuring predictive values of promising screening tools. In addition, other populations, for example in other sports and age groups, should be evaluated. Screening in younger age groups, especially, has the potential for being effective in reducing injuries in team sports. Furthermore, most of the studies with the purpose of finding significant screening tools for an ACL injury are performed in female athletes. However, it is important that predictive values of screening tools for ACL injury in male athletes be examined also.
Second, studies that require more extensive methods of screening, such as 3-D motion analysis, were included also, as they can support more simple tasks. For example, Myer et al.[43] developed an algorithm to use in the field to predict ACL injuries, as a result, no laboratory tests will be necessary. A suggestion for future research is to analyse the prospective relationship of this algorithm with ACL injury.
There is a need for more prospective studies in the future. Ideally, they should involve large sample groups and should follow athletes over several seasons. In this way, better recommendations can be made to trainers and coaches. In future research it is also important to focus on the development of simple, reliable and valid screening tools.
6. Conclusion and Practical Implications
Based on this review, several screening tools for injuries to the ACL, knee, hamstring, groin and ankle can be recommended for use in the field. For injuries in general, there is some support in the literature to suggest that general joint laxity is a predictive measure for leg injuries. The anterior right/left reach distance >4 cm and the composite reach distance <4.0% of limb length in girls measured with the SEBT may predict leg injuries. Furthermore, an increasing age, a lower H : Q ratio, and a decreased ROM of hip abduction may predict the occurrence of leg injuries. Hyperextension of the knee, side-to-side differences in anterior-posterior knee laxity and differences in knee abduction moment between both legs are suggested to be predictive tests for sustaining an ACL injury and height was a predictive screening tool for knee ligament injuries. There is some evidence that when age increases the probability of sustaining a hamstring injury increases. Debate exists in the analysed literature as to whether measurement of the flexibility of the hamstring and the H : Q ratio are suitable for predictive screening tools. Hip-adduction-to-abduction strength is a predictive test for hip adductor muscle strain. Studies do not agree on whether ROM of the hamstring is a predictive screening tool for groin injury. BMI and the age of an athlete could contribute to an ankle sprain. There is support in the literature to suggest that the higher strength of the plantar flexors may be a predictive measure for sustaining an ankle injury. Furthermore, there is some agreement that the measurement of postural sway is a predictive test for an ankle injury. These screening tools can be implemented in injury prevention programmes. Medical staff and coaches can perform preseason screening by using one or more screening tools to predict which athletes have a greater risk of sustaining an injury to the lower extremities. The next step is to provide an individual training programme for the athletes at risk.
Screening tools can be divided into different groups the first being anthropometric tests. Age, BMI and height are often described as predictive screening tools. An advantage of these types of measurement is that they are easy to use by medical staff, coaches and trainers; on the other hand, age and height are not modifiable. However, it might alert coaches to the need of a prevention programme for their athletes who are of an increased age and taller than average. BMI on the other hand is a modifiable factor, therefore, collaboration with a dietitian should be part of a regular training programme especially in professional athletes. The second group of screening tests measure the flexibility or ROM; for example, the ROM of hip abduction is predictive for injury to the leg in general. Flexibility of joints can easily be measured with the use of a goniometer or an inclinometer.[28] Consequently, medical staff and coaches can integrate these kind of screening tools in their preseason screening. Furthermore, the third group of screening tests measure strength. H : Q ratios and strength of the plantar flexors are examples of predictive tests. To optimally measure strength, more extensive measurement tools are necessary, such as the Cybex dynamometer or the Biodex dynamometer.[68,69] These tools seem most appropriate for use in a clinical setting; a good alternative could be a handheld dynamometer. Balance measurements are the next group of screening tools. This group can be divided into tools that are easy to perform in the field, such as the SLB and the balance test, and tools that require more extensive equipment, i.e. force plates, such as the one-legged standing performance and unilateral ankle tests. Finally, there is a group of screening tests that are predictive for ACL injury, which include side-to-side differences in anterior-posterior knee laxity and knee abduction moment between both legs and require the use of a CompuKT knee arthrometer or specialized software.[37,39] Consequently, these screening tools might not be easily applicable in the field. Currently, researchers are trying to develop applicable screening tools such as the knee abduction moment algorithm and the LESS real time.[33,34,82]
References
Agel J, Evans TA, Dick R, et al. Descriptive epidemiology of collegiate men’s soccer injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2002–2003. J Athl Train 2007 Apr–Jun; 42 (2): 270–7
Dick R, Hootman JM, Agel J, et al. Descriptive epidemiology of collegiate women’s field hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2002–2003. J Athl Train 2007 Apr–Jun; 42 (2): 211–20
Frohm A, Heijne A, Kowalski J, et al. A nine-test screening battery for athletes: a reliability study. Scand J Med Sci Sports 2012; 22 (3): 306–15
Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train 2007 Apr–Jun; 42 (2): 311–9
Myklebust G, Maehlum S, Holm I, et al. A prospective cohort study of anterior cruciate ligament injuries in elite Norwegian team handball. Scand J Med Sci Sports 1998; 8: 149–53
Ekstrand J, Gillquist J. Soccer injuries and their mechanisms: a prospective study. Med Sci Sports Exerc 1983; 15 (3): 267–70
Arnason A, Gudmundsson A, Dahl HA, et al. Soccer injuries in Iceland. Scand J Med Sci Sports 1996; 6 (1): 40–5
Hawkins RD, Fuller CW. A prospective epidemiological study of injuries in four English professional football clubs. Br J Sports Med 1999; 33 (3): 196–203
Junge A, Dvorak J. Soccer injuries: a review on incidence and prevention. Sports Med 2004; 34 (13): 929–38
Walden M, Hagglund M, Ekstrand J. Injuries in Swedish elite football: a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand J Med Sci Sports 2005; 15 (2): 118–25
Walden M, Hagglund M, Ekstrand J. UEFA champions league study: a prospective study of injuries in professional football during the 2001–2002 season. Br J Sports Med 2005; 39 (8): 542–6
Fong DT, Hong Y, Chan LK. A systematic review on ankle injury and ankle sprain in sports. Sports Med 2007; 37 (1): 73–94
Alentorn-Geli E, Myer GD, Silvers HJ, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc 2009 Jul; 17 (7): 705–29
Øiestad BE, Engebretsen L, Storheim K, et al. Knee osteoarthritis after anterior cruciate ligament injury. Am J Sports Med 2009; 37: 1434–43
Mattacola CG, Dwyer MK. Rehabilitation of the ankle after acute sprain or chronic instability. J Athl Train 2002 Dec; 37 (4): 413–29
Engebretsen AH, Myklebust G, Holme I, et al. Intrinsic risk factors for hamstring injuries among male soccer players: a prospective study. Am J Sports Med 2010 Jun; 38 (6): 1147–53
Orchard J, Best TM. The management of muscle strain injuries: an early return versus the risk of recurrence. Clin J Sport Med 2002 Jan; 12 (1): 3–5
Donaldson CT, Dreese JC. Hamstring and quadriceps injuries. Curr Opin Orthrop 2006 Apr; 17: 145–8
Engebretsen AH, Myklebust G, Holme I, et al. Intrinsic risk factors for acute ankle injuries among male soccer players: a prospective study. Scand J Med Sci Sports 2010 Jun; 20 (3): 403–10
Arnason A, Sigurdsson SB, Gudmundsson A, et al. Risk factors for injuries in football. Am J Sports Med 2004 Jan–Feb; 32 (1 Suppl.): 5S–16S
Salmon L, Russell V, Musgrove T, et al. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy 2005; 21 (8): 948–57
Paterno MV, Schmitt LC, Ford KR, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med 2010; 38 (10): 1968–78
Shelbourne KD, Gray T, Haro M. Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med 2009; 37 (2): 246–51
Pinczewski LA, Lyman J, Salmon LJ, et al. A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: a controlled, prospective trial. Am J Sports Med 2007; 35 (4): 564–74
Mckay GD, Goldie P, Payne W, et al. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med 2001; 35 (2): 103–8
Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg 2000 May–Jun; 8 (3): 141–50
Baumhauer JF, Alosa DM, Renström TS, et al. Test-retest reliability of ankle injury risk factors. Am J Sports Med 1995 Sep–Oct; 23 (5): 571–4
Gabbe BJ, Bennell KL, Wajswelner H, et al. Reliability of common lower extremity musculoskeletal screening tests. Phys Ther Sport 2004 May; 5 (2): 90–7
Dennis RJ, Finch CF, Elliott BC, et al. The reliability of musculoskeletal screening tests used in cricket. Phys Ther Sport 2008 Feb; 9 (1): 25–33
Engebretsen AH, Myklebust G, Holme I, et al. Intrinsic risk factors for acute knee injuries among male football players: a prospective cohort study. Scand J Med Sci Sports 2010 Oct; 21: 645–52
McGuine TA, Greene JJ, Best T, et al. Balance as a predictor of ankle injuries in high school basketball players. Clin J Sport Med 2000 Oct; 10 (4): 239–44
Hadzic V, Sattler T, Topole E, et al. Risk factors for ankle sprain in volleyball players: a preliminary analysis. Isokinet Exerc Sci 2009; 17 (3): 155–60
Myer GD, Ford KR, Khoury J, et al. Development and validation of a clinic-based prediction tool to identify female athletes at high risk for anterior cruciate ligament injury. Am J Sports Med 2010 Oct; 38 (10): 2025–33
Myer GD, Ford KR, Khoury J, et al. Clinical correlates to laboratory measures for use in non-contact anterior cruciate ligament injury prediction algorithm. Clin Biomech (Bristol, Avon). 2010 Aug; 25 (7): 693–9
Plisky PJ, Rauh MJ, Kaminski TW, et al. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther 2006 Dec; 36 (12): 911–9
Gabbe BJ, Finch CF, Bennell KL, et al. Risk factors for hamstring injuries in community level Australian football. Br J Sports Med 2005 Feb; 39 (2): 106–10
Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med 2005 Apr; 33 (4): 492–501
Wang H, Chen C, Shiang T, et al. Risk-factor analysis of high school basketball-player ankle injuries: a prospective controlled cohort study evaluating postural sway, ankle strength, and flexibility. Arch Phys Med Rehabil 2006 Jun; 87 (6): 821–5
Myer GD, Ford KR, Paterno MV, et al. The effects of generalized joint laxity on risk of anterior cruciate ligament Injury in young female athletes. Am J Sports Med 2008 Jun; 36 (6): 1073–80
Zebis MK, Andersen LL, Bencke J, et al. Identification of athletes at future risk of anterior cruciate ligament ruptures by neuromuscular screening. Am J Sports Med 2009 Oct; 37 (10): 1967–73
Engebretsen AH, Myklebust G, Holme I, et al. Intrinsic risk factors for groin injuries among male soccer players: a prospective study. Am J Sports Med 2010 Oct; 38 (10): 2051–7
Myer GD, Ford KR, Khoury J, et al. Three-dimensional motion analysis validation of a clinic-based nomogram designed to identify high ACL injury risk in female athletes. Phys Sportsmed 2011 Feb; 39 (1): 19–28
Myer GD, Ford KR, Hewett TE. New method to identify athletes at high risk of ACL injury using clinic-based measurements and freeware computer analysis. Br J Sports Med 2011 Apr; 45 (4): 238–44
Devillé WL, Buntinx F, Bouter LM, et al. Conducting systematic reviews of diagnostic studies: didactic guidelines. BMC Med Res Methodol 2002 Jul; 3: 2–9
CEBM. Oxford Centre for Evidence-Based Medicine: levels of evidence (March 2009) [online]. Available from URL: http://www.cebm.net/index.aspx?o=1025 [Accessed 2012 Jul 5]
McLean SG, Walker K, Ford KR, et al. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br J Sports Med 2005 Jun; 39: 355–62
Baumhauer JF, Alosa DM, Renström AF, et al. A prospective study of ankle injury risk factors. Am J Sports Med 1995 Sep–Oct; 23 (5): 564–70
Ekegren CL, Miller WC, Celebrini RG, et al. Reliability and validity of observational risk screening in evaluating dynamic knee valgus. J Orthop Sports Phys Ther 2009 Sep; 39 (9): 665–74
Tropp H, Odenrick P, Gillquist J. Stabilometry recordings in functional and mechanical instability of the ankle joint. Int J Sports Med 1985 Jun; 6 (3): 180–2
Mangine RE, Noyes FR, Mullen MP, et al. A physiological profile of the elite soccer athlete. J Orthop Sports Phys Ther 1990; 12 (4): 147–52
Shambaugh JP, Klein A, Herbert JH. Structural measures as predictors of injury basketball players. Med Sci Sports Exerc 1991; 23 (5): 522–7
Watson AW. Ankle sprains in players of the field-games Gaelic football and hurling. J Sports Med Phys Fitness 1999 Mar; 39 (1): 66–70
Smith AM, Stuart MJ, Wiese-Bjornstal DM, et al. Predictors of injury in ice hockey players: a multivariate, multi-disciplinary approach. Am J Sports Med 1997 Jul–Aug; 25 (4): 500–7
Myer GD, Ford KR, Barber Foss KD, et al. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med 2009 Jan; 19 (1): 3–8
O’Conner D. Groin injuries in professional rugby league players: a prospective study. J Sports Sci 2004 Jul; 22 (7): 629–36
Reinking MF. Exercise-related leg pain in female collegiate athletes: the influence of intrinsic and extrinsic factors. Am J Sports Med 2006 Sep; 34 (9): 1500–7
Witvrouw E, Lysens R, Bellemans J, et al. Intrinsic risk factors for the development of anterior knee pain in an athletic population: a two-year prospective study. Am J Sports Med 2000 Jul–Aug; 28 (4): 480–9
Witvrouw E, Bellemans J, Lysens R, et al. Intrinsic risk factors for the development of patellar tendinitis in an thletic population a two-year prospective study. Am J Sports Med 2001 Mar–Apr; 29 (2): 190–5
Zazulak BT, Hewett TE, Reeves NP, et al. The effects of core proprioception on knee injury: a prospective biomechanical-epidemiological study. Am J Sports Med 2007 Mar; 35 (3): 368–73
Zazulak BT, Hewett TE, Reeves NP, et al. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med 2007 Jul; 35 (7): 1123–30
Knapik JJ, Bauman CL, Jones BH, et al. Preseason strength and flexibility imbalances associated with athletic injuries in female collegiate athletes. Am J Sports Med 1991 Jan–Feb; 19 (1): 76–81
Orchard J, Wood T, Seward H, et al. Comparison of injuries in elite senior and junior Australian football. J Sci Med Sport 1998 Jun; 1 (2): 83–8
Vaillant J, Bonnefoy-Crudaz F, Ribes A, et al. Assessing the value of two functional tests as predictive factors of ankle sprain in rugby players. Ann Phys Rehabil Med 2011; 54 Suppl. 1:e128
Roberts WO. Injuries in young ice hockey players [commentary]. Clin J Sport Med 2007 May; 17 (3): 225–6
Benell K, Wajswener H, Lew P, et al. Isokinetic strength testing does not predict hamstring injury in Australian Rules footballers. Br J Sports Med 1998 Dec; 32 (4): 309–14
Benell K, Tully E, Harvey N. Does the toe-touch test predict hamstring injury in Australian Rules footballers. Aust J Physiother 1999; 45 (2): 103–9
Pefanis N, Papaharalampous X, Tsiganos G, et al. The effect of Q angle on ankle sprain occurence. Foot Ankle Spec 2009 Feb; 2 (1): 22–6
Östenberg A, Roos H. Injury risk factors in female European football: a prospective study of 123 players during one season. Scand J Med Sci Sports 2000 Oct; 10 (5): 279–85
Söderman K, Alfredson H, Pietilä T, et al. Risk factors for leg injuries in female soccer players: a prospective investigation during one out-door season. Knee Surg Sports Traumatol Arthrosc 2001 Sep; 9 (5): 313–21
Smith HC, Johnson RJ, Shultz SJ, et al. A prospective evaluation of the Landing Error Scoring System (LESS) as a screening tool for anterior cruciate ligament injury risk. Am J Sports Med 2012; 40 (3): 521–6
Cameron M, Adams R, Maher C. Motor control and strength as predictors of hamstring injury in elite players of Australian football. Phys Ther Sport 2003 Nov; 4 (4): 159–66
Tyler TF, Nicholas SJ, Campbell RJ, et al. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med 2001 Mar–Apr; 29 (2): 124–8
Trojian TH, McKeag DB. Single leg balance test to identify risk of ankle sprains. Br J Sports Med 2006 Jul; 40 (7): 610–3; discussion 613
Hrysomallis C, McLaughlin P, Goodman C. Preseason and midseason balance ability of professional Australian footballers. J Strength Cond Res 2008 Jan; 22 (1): 210–1
Emery CA, Meeuwisse WH. Risk factors for groin injuries in hockey. Med Sci Sports Exerc 2001 Sep; 33 (9): 1423–33
Onate J, Cortes N, Welch C, et al. Expert versus novice interrater reliability and criterion validity of the landing error scoring system. J Sport Rehabil 2010 Feb; 19 (1): 41–56
Uhorchak JM, Scoville CR, Williams GN, et al. Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 West Point cadets. Am J Sports Med 2003 Nov–Dec; 31 (6): 831–42
Ford KR, Myer GD, Hewett TE. Reliability of landing 3D motion analysis: implications for longitudinal analyses. Med Sci Sports Exerc 2007 Nov; 39 (11): 2021–8
Arendt EA, Agel J, Dick R. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train 1999 Apr; 34 (2): 86–92
Molczyk L, Thigpen LK, Eickhoff J, et al. Reliability of testing the knee extensors and flexors in healthy adult women using a Cybex II isokinetic dynamometer. J Orthop Sports Phys Ther 1991; 14 (1): 37–41
Schmitz R, Arnold B. Intertester and intratester reliability of the Biodex Stability System. J Sport Rehabil. 1998; 7: 95–101
Padua DA, Boling MC, Distefano LJ, et al. Reliability of the landing error scoring system-real time, a clinical assessment tool of jump-landing biomechanics. J Sport Rehabil 2011 May; 20 (2): 145–56
Myklebust G, Engebretsen L, Hoff Braekken I, et al. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med 2003 Mar; 13: 71–8
Ross SE, Guskiewicz KM. Examination of static and dynamic postural stability in individuals with functionally stable and unstable ankles. Clin J Sport Med 2004 Nov; 14 (6): 332–8
Chomiak J, Junge A, Peterson L, et al. Severe injuries in football players: influencing factors. Am J Sports Med 2000; 28 (5 Suppl.): S58–68
Acknowledgements
No funding was received to assist in the preparation of this article. The authors have no conflicts of interest to declare that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dallinga, J.M., Benjaminse, A. & Lemmink, K.A.P.M. Which Screening Tools Can Predict Injury to the Lower Extremities in Team Sports?. Sports Med 42, 791–815 (2012). https://doi.org/10.1007/BF03262295
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03262295