
Abstract
Purpose
Lateral epicondylitis is generally considered an extra-articular condition. The role of minor instability in the aetiology of lateral elbow pain has rarely been considered. The aim of this study was to evaluate the correlation of lateral ligamentous laxity with aspects of intra-articular lateral elbow pathology and investigate the role of minor instability in lateral elbow pain.
Methods
Thirty-five consecutive patients aged between 20 and 60 years with recalcitrant lateral epicondylitis who had failed conservative therapy and had no previous trauma or overt instability, were included. The presence of three signs of lateral ligamentous patholaxity and five intra-articular findings were documented during arthroscopy. The relative incidence of each of these was calculated, and the correlation between patholaxity and intra-articular pathology was evaluated.
Results
At least one sign of lateral ligamentous laxity was observed in 48.6% of the studied cohort, and 85.7% demonstrated at least one intra-articular abnormal finding. Radial head ballottement was the most common sign of patholaxity (42.9%). Synovitis was the most common intra-articular aspect of pathology (77.1%), followed by lateral capitellar chondropathy (40.0%). A significant correlation was found between the presence of lateral ligamentous patholaxity signs and capitellar chondropathy (p = 0.0409), as well as anteromedial synovitis (p = 0.0408).
Conclusions
Almost one half of patients suffering from recalcitrant lateral epicondylitis display signs of lateral ligamentous patholaxity, and over 85% demonstrate at least one intra-articular abnormality. The most frequent intra-articular findings are synovitis and lateral capitellar chondropathy, which correlate significantly with the presence of lateral ligamentous patholaxity. The fact that several patients demonstrated multiple intra-articular findings in relation to laxity provides support to a sequence of pathologic changes that may result from a symptomatic minor instability of the lateral elbow (SMILE) condition.
Level of evidence
III.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Lateral epicondylitis is generally considered to be an extra-articular condition involving degeneration and tendinosis of the common extensor origin [24, 56]. The extensor carpi radialis brevis (ECRB) is the most commonly affected tendon, and debridement or release is considered to be the standard surgical therapy when non-operative measures have failed [8, 14, 22, 25, 29, 39–41, 43, 45, 55, 59, 60, 64]. This has been described through open, percutaneous and arthroscopic approaches [9, 45, 55]. Due to the lack of conclusive evidence in favour of any technique, patients are generally treated according to the surgeon’s preferred approach [28, 41, 47, 62]. Despite the plethora of non-surgical treatment modalities and surgical techniques available, a significant proportion of patients remain symptomatic with lateral elbow pain [7, 63].
Although the main aetiology of lateral epicondylitis is traditionally thought to be related to the extra-articular tendon, this may not be the primary issue, but may be part of a multi-factorial process involving extra-articular, intra-articular and systemic factors. The role of patholaxity or microinstability in the aetiology of lateral elbow pain has rarely been considered [36]. Lateral epicondylitis may result from overuse with repetitive loading, leading to tissue patholaxity and subsequent chondropathy. Similar clinical entities have been described elsewhere in the upper limb, both for the shoulder [30, 31, 34, 44, 50] and for the wrist [12, 35, 46, 57]. Repetitive stress loading of the medial side of the elbow leading to valgus instability, and pain has also been described [1, 27].
Elbow arthroscopy offers the opportunity to visualize the intra-articular compartments, identifying elements of pathology that may be missed by imaging or open techniques [5–7]. Although not comprehensive, there are now reports describing the presence of intra-articular findings that may have an aetiological role in ECRB tendinopathy. Baker et al. [8] described a 64% rate of capsular tears associated with arthroscopically treated lateral epicondylitis and a 69% rate of other intra-articular findings. Other reported findings associated with lateral elbow pain and snapping plica syndrome include: synovitis, radial head and capitellar erosion or chondromalacia and capsular tears [3, 33, 49]. However, the aetiology of these intra-articular findings in ECRB tendinopathy has not yet been described.
The aim of this study was to describe the signs of lateral ligamentous patholaxity and abnormal intra-articular findings associated with lateral epicondylitis, and to define the relative incidence and correlation between them. It was hypothesized that at least one intra-articular pathological finding would be present in the majority (75% or more) of patients undergoing surgery for recalcitrant lateral epicondylitis. Confirmation of this hypothesis would open new diagnostic perspectives and offer a solid base upon which to develop a pathology-directed approach to patients with persistent lateral elbow pain.
Materials and methods
Consecutive patients referred to the lead author for recalcitrant lateral epicondylitis were considered for enrolment between 2009 and 2016. Patients between 20 and 65 years of age were included if their symptoms had not responded to at least 6 months of conservative treatment (including ice, non-steroidal anti-inflammatory drugs, stretching, steroid injections and physical therapy). Patients were excluded if there was a previous history of trauma or signs of major instability (positive posterolateral drawer, posterolateral pivot shift and varus/valgus stress tests). Patients were also excluded if there were any radiographic or magnetic resonance imaging (MRI) features of trauma or arthritis.
All patients underwent elbow arthroscopy for their recalcitrant symptomatic lateral epicondylitis. A single examiner with extensive experience in elbow surgery performed all pre- and intra-operative evaluation.
Arthroscopy was performed with the patient in a modified lateral decubitus position using an axillary block and general anaesthesia. A pneumatic tourniquet was positioned high in the axilla and inflated to 250 mmHg after limb exsanguination. The operative arm was positioned with the shoulder in 100° forward flexion/90° internal rotation and held using an arm holder. The elbow was positioned in 90° of flexion, with the hand and forearm hanging free with only gravity force. Before establishing the arthroscopic portals, 30 cc of sterile saline solution was injected to distend the elbow joint using an 18-gauge needle inserted in the proximal posterior portal.
Standard posterior, posterolateral and midlateral portals were first established in order to explore the posterior compartment, the posteromedial gutter and the posterior aspect of the radiocapitellar joint. The anterior compartment of the elbow was then entered after the posterior compartment evaluation. A proximal anteromedial portal was created 2 cm proximal to the medial humeral epicondyle and 1 cm anterior to the intramuscular septum. Insertion of a 30° arthroscope into this portal allowed intra-articular diagnostic evaluation.
The presence of three intra-articular signs of lateral ligamentous patholaxity was prospectively documented as follows:
-
1.
Annular Drive Through (ADT) This finding is used to evaluate the anteroposterior excursion of the radial head inside the annular ligament. The test is performed with the arthroscope in the posterolateral portal, while the surgeon pushes the posterior radial head anteriorly with his thumb. If this allows enough space for a 4.2-mm shaver to slide between the radial head and the annular ligament with no or minimal resistance, the “annular drive through” is considered positive (video 1).
-
2.
Loose Collar Sign (LCS) Laxity of the annular ligament permits the radial neck to be exposed beyond the cartilaginous portion of the head at 90° of elbow flexion when looking from the anteromedial portal (Fig. 1).
Fig. 1 
Radial neck exposure (Loose Collar Sign, LCS) under the cartilaginous portion (arrow) may be associated with annular ligament redundancy and laxity (asterisks). Right elbow, anteromedial view; arrowhead capitellum, Rh radial head
-
3.
Laxity of the radial component of the lateral collateral ligament (R-LCL) R-LCL pull-up sign (RPS). This describes the ability to pull the R-LCL/annular ligament up towards the capitellum greater than 1 cm with an arthroscopic grasper introduced via the anterolateral portal (video 2).

The presence of five intra-articular specific pathologic findings was also prospectively documented as follows:
-
1.
Plica in the posterior compartment (Fig. 2).
Fig. 2 
A posterior plica has been described more than 20 years ago in lateral elbow pain syndromes. Nowadays, arthroscopy can provide an excellent representation of the plica (asterisks) and its relation to the capitellum and the radial head. Left elbow, posterolateral view; Ca capitellum, Rh radial head
-
2.
Synovitis anterior to the radial head, or anteromedially at the insertion of the annular ligament on the sigmoid notch (Figs. 3, 4).
Fig. 3 
Abundant synovitis at the level of the annular ligament insertion is a frequent finding in lateral elbow pain syndrome (asterisks). Right elbow, anteromedial view; Ca capitellum, Rh radial head
Fig. 4 
Synovitis may extend also to the anteromedial part of the joint and extend from the annular ligament insertion to the sigmoid notch (asterisks). Right elbow, anteromedial view; Ca capitellum, Rh radial head, Co coronoid process
-
3.
A focal “Chondropathy of the Lateral Aspect of the Capitellum” (CLAC lesion—Figs. 5, 6).
Fig. 5 
Chondropathy of the lateral aspect of the capitellum may be associated with lateral elbow pain (asterisk). Right elbow, anteromedial view; Ca capitellum, Rh radial head
Fig. 6 
A capsular distractive aspect in the articular side of the lateral capsule, at the level of the radiocapitellar joint (arrow). A minimal chondropathy of the capitellum is associated (asterisk)- CLAC lesion. Right elbow, anteromedial view; Ca capitellum, Rh radial head
-
4.
A capsular tear at the level of the radiocapitellar joint (Figs. 6, 7).
Fig. 7 
A partial capsular tear in the distal aspect of the lateral capsule, minimally beneath the level of the radiocapitellar joint (arrow). Right elbow, anteromedial view; Ca capitellum, Rh radial head
-
5.
Chondral damage of the anterosuperior aspect of the radial head, where it engages the sigmoid notch when the forearm is pronated (Fig. 8).
Fig. 8 
Radial head chondropathy may assume a specific distribution on the anterosuperior aspect and enter the sigmoid notch in pronation (arrow). Right elbow, anteromedial view; Ca capitellum, Rh radial head







Debridement of the synovitis was performed in most patients. Plication of the lateral capsule with an anchor placed high in the anterolateral aspect of the capitellum in order to reduce radial head ballottement was performed only in the presence intra-articular signs combined with positive ADT, LCS or RPS [4].
Institutional approval of the study protocol was obtained by the University of Milan (ID4610).
Statistical analysis
The relative incidence of the all reported findings was calculated. The relationship between at least one sign of patholaxity and the presence of an intra-articular finding was analysed. Data were expressed as mean ± standard deviation (SD). Fisher’s exact test was used to test differences in strength of association between categorical variables. A sample size of 35 was chosen to produce a two-sided 95% confidence interval with a width equal to 0.321 when the sample proportion was 0.7. Statistical analysis was performed using GraphPad Prism version 6.0 software (GraphPad Software Inc.). For all analysis, the significance level was set at p value less than 0.05.
Results
Thirty-five consecutive patients (15 males, 20 females) with a mean age of 47.1 years (SD: 8.6) were included in this study. The right limb was affected in 21 patients (60%). The elbow of the dominant arm was affected in 25 patients (71.4%).
Seventeen patients showed signs of lateral ligamentous patholaxity (48.6%), the most frequent of which was radial head ballottement associated with ADT (15 patients, 42.9%). Thirty patients presented with at least one intra-articular abnormal finding (85.7%), 19 had at least 2 (54.3%), and four had at least 3 (11.4%) findings (Table 1). Synovitis was the most common finding, present in 77.1% of the patients. The second most common finding was capitellar chondropathy (CLAC lesion), which was reported in 14 patients (40.0%).
A significant correlation was found between the presence of at least one sign of lateral ligamentous patholaxity (ADT, LCS or RPS) and the intra-articular presence of anteromedial synovitis (p = 0.0408) and capitellar chondropathy (p = 0.0409).
No significant correlations were found between signs of patholaxity and any other intra-articular finding.
Discussion
The most important finding of this study was that recalcitrant lateral elbow pain, diagnosed as lateral epicondylitis, is associated with high incidence of intra-articular findings which may be related to a condition of patholaxity termed “minor lateral elbow instability.”
The significant relationship between intra-articular findings (capitellar chondropathy and synovitis) and lateral ligamentous patholaxity supports the existence of a sequence of pathologic intra-articular changes that may result from a minor instability of the lateral elbow condition. Minor instability resulting from repetitive low-energy stress or shear is generally characterized by chondral damage, tendonitis, capsular pathology and ligamentous patholaxity [12, 13, 30, 31, 35, 44, 46, 57]. This is seen in other joints such as in the case of shoulder microinstability, which can be associated with pathologic sequelae, including partial rotator cuff and capsulolabral tears [10, 11, 15, 58]. Medial epicondylitis in unstable baseball pitchers’ elbows has been associated with intra-articular changes in the lateral joint compartment [54].
Intra-articular findings have been described in association with lateral epicondylitis surgery. In the posterior compartment, the presence of a plica with a meniscal appearance, which can extend anteriorly, has been reported by numerous authors [3, 33, 49, 51, 53, 61]. The anatomy and histology of this plica has been described in detail and a classification system has also been proposed. [2, 19, 21]. No synovial plicae were identified in our series, supporting that plica syndrome and abnormal intra-articular findings of the lateral aspect of the elbow may represent different conditions and that a plica may be another, less frequent cause of lateral elbow pain.
In the anterior compartment, Baker et al. first described the presence of capsular tears occurring at the level of the radiocapitellar joint (Figs. 6, 7) with three distinct patterns of pathologic changes in the lateral capsule and at the undersurface of the ECRB tendon [6, 8]. The type III lesion, as well as one located more anteroinferiorly than originally described in Baker’s paper (Fig. 7), was seen in this current study. Further anterior compartment findings identified in this study include a specific focus of synovitis located anterior to the radial head, or anteromedially at the insertion of the annular ligament on the sigmoid notch (Figs. 3, 4) [3, 16, 21, 33, 61], as well as chondropathy of the anterosuperior aspect of the radial head (with the head in a neutral position), that rotates into the sigmoid notch during pronation (Fig. 8) [2, 3, 16, 19, 33, 61].
Several simple daily activities, such as pouring a drink into a glass (Fig. 9), are performed with the shoulder in moderate abduction, pronation of the hand, and 50°–70° of elbow flexion. In this position, the hand and the forearm represent a weight for the elbow that creates a varus/pronation moment with progressive stretching of the R-LCL/annular ligament. Similarly, in many office-based jobs, people spend the majority of their time in a position based on elbow suspension, varus stress and pronation of the forearm. The role of the R-LCL was first described by Ciaudo et al. [17], with recent studies further stressing the importance of this ligament in elbow stability [52]. The R-LCL anatomically continues into the anterior portion of the annular ligament that may also become stretched. With time, this could lead to the following pathologic cascade:

A repetitive varus–pronation stress could cause R-LCL elongation and be the initiator of intra-articular changes in the lateral aspect of the elbow joint. Many simple daily activities, such as pouring a drink from a can into a glass, may produce this stress
-
1.
Elongation of R-LCL and annular ligament with relative hypermobility of the radial head (Fig. 10).
Fig. 10 
Elongation of annular ligament leaves the radial head more mobile and less congruent in the proximal radioulnar joint. Radial head ballottement and neck exposure are consequences of this incongruence. Although minimal, the persistent minor instability may lead to radial head chondropathy and synovitis
-
2.
Minor incongruence of the proximal radioulnar joint resulting in radial head impingement with the notch in pronation, and eventual radial head chondropathy. Intra-articular synovitis could be a result of joint inflammation (Fig. 11).
Fig. 11 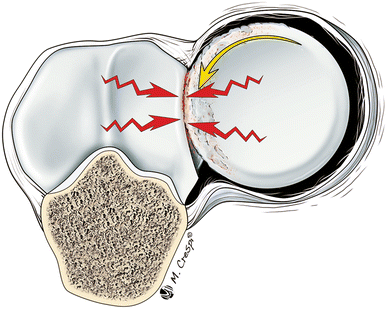
When the proximal radioulnar joint is pronated, the chondropathic part of the radial head enters the sigmoid notch and may produce anterior elbow pain. With progression of instability, friction between radial head and proximal ulna increases, worsening the chondropathy
-
3.
Shear or abrasion of the stretched R-LCL/anterolateral capsule over the lateral portion of the capitellum in moderate elbow varus and pronation, with the potential development of the CLAC lesion and possible capsular tears (Fig. 12).
Fig. 12 
The R-LCL is the first extra-articular structure on the distal aspect of the lateral elbow joint and continues into the anterior portion of the annular ligament. When the annular ligament loosens, the R-LCL becomes unstable as well. An unstable R-LCL may have an abrasive effect on the joint capsule and the capitellum, causing capsular tears and lateral capitellar chondropathy



Based on this pathologic cascade, it is postulated that the ECRB tendon acts as a dynamic stabilizer, resisting varus forces in support of a deficient or lax R-LCL (static stabilizer), given its unique extracapsular position parallel to the R-LCL [20]. With repetitive loads and overuse, ECRB tendinopathy (Fig. 13) would thus be the consequence of a sequence of events in a condition we have termed Symptomatic Minor Instability of the Lateral Elbow (SMILE). A flow chart of the proposed aetiology for this lateral elbow pain syndrome is schematically represented in Fig. 14.

ECRB acts as dynamic stabilizer against varus-pronation stress; when static stabilizers fail due to minor instability, ECRB is overloaded and becomes inflamed and painful

Flow chart for lateral elbow pain syndrome aetiology
This rationale could open new therapeutic perspectives for patients diagnosed with lateral epicondylitis including two possible arthroscopic treatments: firstly, debridement of synovitis to reduce the inflammatory pain; secondly, plication of the lateral capsule with an anchor placed high in the anterolateral aspect of the capitellum to reduce radial head ballottement when patholaxity signs are detected.
Image-based diagnosis and classification of the intra-articular findings evaluated in this study in association with lateral elbow pain is challenging. Ultrasound examination is still considered the imaging gold standard even if ultrasound is limited in the evaluation of joint cartilage and capsule [18, 26, 37, 38, 48]. MRI is limited by the need for different arm positions and reconstructions to fully investigate anomalies. MRI arthrography and tridimensional reconstruction may help increase the utility of MRI [23, 32, 42]. A detailed knowledge of the pathology and a precise clinical examination, along with a specific question from the requesting surgeon, may help focus the relevant investigation and can improve imaging-based diagnostics. a.
Limitations of this study include that it is a relatively small case series from a single surgeon/single examiner. Nevertheless, patients were recruited prospectively by an experienced surgeon in the field of elbow surgery. Given the lack of any suitable validated criteria, inclusion was determined through clinical assessment by the primary author, along with the development of two new discrete tests targeted to evaluate the anterior and posterior compartments of the joint instead of ECRB insertion. With regard to the intra-operative findings, laxity is a difficult feature to assess and quantify with respect to what may be considered as “physiological laxity” as opposed to “pathologic laxity”. This study used specific descriptors and defined as precisely and objectively as possible the findings regarded as pathologic by the lead author. Experience with analogous conditions in other joints does suggest that there is a spectrum of changes that must be appreciated and understood. For example, multidirectional shoulder instability is associated with patholaxity, though not all lax shoulders will develop symptoms of multidirectional instability [10, 11, 13, 15, 30, 31, 44, 58]. This study was primarily focused on the description of signs of ligamentous patholaxity in correlation with intra-articular findings at elbow arthroscopy. However, the aetiology of recalcitrant lateral epicondylitis may be multi-factorial: intra-articular, local extra-articular/tendon-related and systemic factors all contribute to the origin of lateral elbow pain. A focus of ongoing study will be to present the outcomes of the described interventions undertaken.
Conclusions
Over 85% of patients suffering from recalcitrant lateral epicondylitis demonstrate at least one pathologic intra-articular finding and almost 50% present at least one sign of lateral ligamentous patholaxity. The most frequent intra-articular findings are synovitis and “CLAC” lesions, both of which are significantly associated with the presence of lateral ligamentous patholaxity. The cumulative presence of several intra-articular findings provides support to a sequence of pathologic changes that culminates in “SMILE”.
References
Ahmad CS, ElAttrache NS (2004) Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med 23(4):665–676
Akagi M, Nakamura T (1998) Snapping elbow caused by the synovial fold in the radiohumeral joint. J Shoulder Elb Surg 7(4):427–429
Antuna SA, O’Driscoll SW (2001) Snapping plicae associated with radiocapitellar chondromalacia. Arthroscopy 17(5):491–495
Arrigoni P, Cucchi D, D’Ambrosi R, Menon A, Aliprandi A, Randelli P (2017) Arthroscopic R-LCL plication for symptomatic minor instability of the lateral elbow (SMILE). Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-017-4531-9
Arrigoni P, Fossati C, Zottarelli L, Brady PC, Cabitza P, Randelli P (2014) 70° frontal visualization of lateral compartment of the elbow allows extensor carpi radialis brevis tendon release with preservation of the radial lateral collateral ligament. Arthroscopy 30(2):29–35
Baker C, Cummings P (1998) Arthroscopic managementof miscellaneous elbow disorders. Oper Tech Sports Med 6:16–21
Baker CL, Jones GL (1999) Arthroscopy of the elbow. Am J Sports Med 27(2):251–264
Baker CL, Murphy KP, Gottlob CA, Curd DT (2000) Arthroscopic classification and treatment of lateral epicondylitis: two-year clinical results. J Shoulder Elb Surg 9(6):475–482
Baumgard SH, Schwartz DR (1982) Percutaneous release of the epicondylar muscles for humeral epicondylitis. Am J Sports Med 10(4):233–236
Boileau P, Zumstein M, Balg F, Penington S, Bicknell RT (2011) The unstable painful shoulder (UPS) as a cause of pain from unrecognized anteroinferior instability in the young athlete. J Shoulder Elb Surg 20(1):98–106
Burkhart SS, Morgan CD, Kibler WB (2003) The disabled throwing shoulder: spectrum of pathology part I: Pathoanatomy and biomechanics. Arthroscopy 19(4):404–420
Caggiano N, Matullo KS (2014) Carpal instability of the wrist. Orthop Clin North Am 45(1):129–140
Caprise PA, Sekiya JK (2006) Open and arthroscopic treatment of multidirectional instability of the shoulder. Arthroscopy 22(10):1126–1131
Carayannopoulos A, Borg-Stein J, Sokolof J, Meleger A, Rosenberg D (2011) Prolotherapy versus corticosteroid injections for the treatment of lateral epicondylosis: a randomized controlled trial. PM & R 3(8):706–715
Castagna A, Nordenson U, Garofalo R, Karlsson J (2007) Minor shoulder instability. Arthroscopy 23(2):211–215
Cerezal L, Rodriguez-Sammartino M, Canga A, Capiel C, Arnaiz J, Cruz A, Rolón A (2013) Elbow synovial fold syndrome. Am J Roentgenol 201:88–96
Ciaudo O, Guérin-Surville H (1980) Importance of damage to the medial fascia of the external lateral ligament (radial collateral ligament) in the mechanisms of luxations of the elbow. Study on the cadaver (author’s transl). J Chir (Paris) 117(4):237–239
Clarke AW, Ahmad M, Curtis M, Connell DA (2010) Lateral elbow tendinopathy: correlation of ultrasound findings with pain and functional disability. Am J Sports Med 38(6):1209–1214
Clarke RP (1988) Symptomatic, lateral synovial fringe (plica) of the elbow joint. Arthroscopy 4(2):112–116
Cohen MS, Romeo AA, Hennigan SP, Gordon M (2008) Lateral epicondylitis: anatomic relationships of the extensor tendon origins and implications for arthroscopic treatment. J Shoulder Elb Surg 17(6):954–960
Commandre FA, Taillan B, Benezis C, Follacci FM, Hammou JC (1988) Plica synovialis (synovial fold) of the elbow. Report on one case. J Sports Med Phys Fit 28(2):209–210
Creaney L, Wallace A, Curtis M, Connell D (2011) Growth factor-based therapies provide additional benefit beyond physical therapy in resistant elbow tendinopathy: a prospective, single-blind, randomised trial of autologous blood injections versus platelet-rich plasma injections. Br J Sports Med 45(12):966–971
Dewan AK, Chhabra AB, Khanna AJ, Anderson MW, Brunton LM (2013) MRI of the elbow: techniques and spectrum of disease: AAOS exhibit selection. J Bone Jt Surg Am 95(14):e99
Dines JS, Bedi A, Williams PN, Dodson CC, Ellenbecker TS, Altchek DW, Windler G, Dines DM (2015) Tennis Injuries: epidemiology, pathophysiology, and treatment. J Am Acad Orthop Surg 23(3):181–189
Dogramaci Y, Kalaci A, Savaş N, Duman IG, Yanat AN (2009) Treatment of lateral epicondilitis using three different local injection modalities: a randomized prospective clinical trial. Arch Orthop Trauma Surg 129(10):1409–1414
Dones VC, Grimmer K, Thoirs K, Suarez CG, Luker J (2014) The diagnostic validity of musculoskeletal ultrasound in lateral epicondylalgia: a systematic review. BMC Med Imaging 14:10
Dugas JR (2010) Valgus extension overload: diagnosis and treatment. Clin Sports Med 29(4):645–654
Dunkow PD, Jatti M, Muddu BN (2004) A comparison of open and percutaneous techniques in the surgical treatment of tennis elbow. J Bone Jt Surg Br 86(5):701–704
Emanet SK, Altan LI, Yurtkuran M (2010) Investigation of the effect of GaAs laser therapy on lateral epicondylitis. Photomed Laser Surg 28(3):397–403
Foster CR (1983) Multidirectional instability of the shoulder in the athlete. Clin Sports Med 2(2):355–368
Gerber C, Nyffeler RW (2002) Classification of glenohumeral joint instability. Clin Orthop Relat Res 400:65–76
Kijowski R, Tuite M, Sanford M (2005) Magnetic resonance imaging of the elbow. Part II: abnormalities of the ligaments, tendons, and nerves. Skelet Radiol 34(1):1–18
Kim DH, Gambardella RA, Elattrache NS, Yocum LA, Jobe FW (2006) Arthroscopic treatment of posterolateral elbow impingement from lateral synovial plicae in throwing athletes and golfers. Am J Sports Med 34(3):438–444
Kim S-H, Ha K-I, Yoo J-C, Noh K-C (2004) Kim’s lesion: an incomplete and concealed avulsion of the posteroinferior labrum in posterior or multidirectional posteroinferior instability of the shoulder. Arthroscopy 20(7):712–720
Kitay A, Wolfe SW (2012) Scapholunate instability: current concepts in diagnosis and management. J Hand Surg Am 37(10):2175–2196
Kniesel B, Huth J, Bauer G, Mauch F (2014) Systematic diagnosis and therapy of lateral elbow pain with emphasis on elbow instability. Arch Orthop Trauma Surg 134(12):1641–1647
Latham SK, Smith TO (2014) The diagnostic test accuracy of ultrasound for the detection of lateral epicondylitis: a systematic review and meta-analysis. Orthop Traumatol Surg Res 100(3):281–286
Levin D, Nazarian LN, Miller TT, O’Kane PL, Feld RI, Parker L, McShane JM (2005) Lateral epicondylitis of the elbow: US findings. Radiology 237(1):230–234
Lin Y-C, Tu Y-K, Chen S-S, Lin I-L, Chen S-C, Guo H-R (2010) Comparison between botulinum toxin and corticosteroid injection in the treatment of acute and subacute tennis elbow: a prospective, randomized, double-blind, active drug-controlled pilot study. Am J Phys Med Rehabil 89(8):653–659
Lindenhovius A, Henket M, Gilligan BP, Lozano-Calderon S, Jupiter JB, Ring D (2008) Injection of dexamethasone versus placebo for lateral elbow pain: a prospective, double-blind, randomized clinical trial. J Hand Surg Am 33(6):909–919
Lo MY, Safran MR (2007) Surgical treatment of lateral epicondylitis: a systematic review. Clin Orthop Relat Res 463:98–106
Magee T (2015) Accuracy of 3-T MR arthrography versus conventional 3-T MRI of elbow tendons and ligaments compared with surgery. AJR Am J Roentgenol 204:W70–W75
McAdams TR, Masters GW, Srivastava S (2005) The effect of arthroscopic sectioning of the lateral ligament complex of the elbow on posterolateral rotatory stability. J Shoulder Elb Surg 14(3):298–301
Neer CS, Foster CR (1980) Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder. A preliminary report. J Bone Jt Surg Am 62(6):897–908
Nirschl RP, Pettrone FA (1979) Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Jt Surg Am 61(6A):832–839
Pappou IP, Basel J, Deal DN (2013) Scapholunate ligament injuries: a review of current concepts. Hand (N Y) 8(2):146–156
Peart RE, Strickler SS, Schweitzer KM (2004) Lateral epicondylitis: a comparative study of open and arthroscopic lateral release. Am J Orthop 33(11):565–567
Poltawski L, Ali S, Jayaram V, Watson T (2012) Reliability of sonographic assessment of tendinopathy in tennis elbow. Skelet Radiol 41(1):83–89
Rajeev A, Pooley J (2015) Arthroscopic resection of humeroradial synovial plica for persistent lateral elbow pain. J Orthop Surg (Hong Kong) 23(1):11–14
Randelli P, Cucchi D, Butt U (2016) History of shoulder instability surgery. Knee Surg Sport Traumatol Arthrosc 24(2):305–329
Safran M, Ahmad CS, Elattrache NS (2005) Ulnar collateral ligament of the elbow. Arthroscopy 21(11):1381–1395
Savoie FH, VanSice W, O’Brien MJ (2010) Arthroscopic tennis elbow release. J Shoulder Elb Surg 19(2 Suppl):31–36
Sims SEG, Miller K, Elfar JC, Hammert WC (2014) Non-surgical treatment of lateral epicondylitis: a systematic review of randomized controlled trials. Hand (N Y) 9(4):419–446
Slutsky DJ, Trevare J (2014) Scapholunate and lunotriquetral injuries: arthroscopic and open management. Sports Med Arthrosc 22(1):12–21
Spatschil A, Landsiedl F, Anderl W, Imhoff A, Seiler H, Vassilev I, Klein W, Boszotta H, Hoffmann F, Rupp S (2006) Posttraumatic anterior-inferior instability of the shoulder: arthroscopic findings and clinical correlations. Arch Orthop Trauma Surg 126(4):217–222
Staples MP, Forbes A, Ptasznik R, Gordon J, Buchbinder R (2008) A randomized controlled trial of extracorporeal shock wave therapy for lateral epicondylitis (tennis elbow). J Rheumatol 35(10):2038–2046
Stefanou A, Marshall N, Holdan W, Siddiqui A (2012) A randomized study comparing corticosteroid injection to corticosteroid iontophoresis for lateral epicondylitis. J Hand Surg Am 37(1):104–109
Steinert AF, Goebel S, Rucker A, Barthel T (2010) Snapping elbow caused by hypertrophic synovial plica in the radiohumeral joint: a report of three cases and review of literature. Arch Orthop Trauma Surg 130(3):347–351
Szabo SJ, Savoie FH, Field LD, Ramsey JR, Hosemann CD (2006) Tendinosis of the extensor carpi radialis brevis: an evaluation of three methods of operative treatment. J Shoulder Elb Surg 15(6):721–727
Taylor SA, Hannafin JA (2012) Evaluation and management of elbow tendinopathy. Sports Health 4(5):384–393
Thanasas C, Papadimitriou G, Charalambidis C, Paraskevopoulos I, Papanikolaou A (2011) Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow epicondylitis: a randomized controlled clinical trial. Am J Sports Med 39(10):2130–2134
Timmerman LA, Andrews JR (1994) Undersurface tear of the ulnar collateral ligament in baseball players. A newly recognized lesion. Am J Sports Med 22(1):33–36
Wada T, Moriya T, Iba K, Ozasa Y, Sonoda T, Aoki M, Yamashita T (2009) Functional outcomes after arthroscopic treatment of lateral epicondylitis. J Orthop Sci 14(2):167–174
Wegmann K, Burkhart KJ, Bingoel AS, Ries C, Neiss WF, Müller LP (2014) Anatomic relations between the lateral collateral ligament and the radial head: implications for arthroscopic resection of the synovial fold of the elbow. Knee Surg Sports Traumatol Arthrosc 23(11):3421–3425
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest relevant to this study.
Funding
This study was not funded.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Video 1: Right elbow, Posterolateral viewing portal showing radial head ballottement and annular drive through (ADT) of a 4.2-mm shaver between the radial head and the annular ligament (MP4 3634 kb)
Video 2: Right elbow, Anteromedial 30° arthroscopic view over the lateral compartment showing a partial detachment with insertional elongation from the capitellum of the R-LCL. Laxity of the R-LCL that can easily be reduced to the humerus or translated more than 1 cm with a grasper or introduced via the anterolateral portal (R-LCL pull-up sign, RPS) (MP4 3894 kb)
Rights and permissions
About this article

Cite this article
Arrigoni, P., Cucchi, D., D’Ambrosi, R. et al. Intra-articular findings in symptomatic minor instability of the lateral elbow (SMILE). Knee Surg Sports Traumatol Arthrosc 25, 2255–2263 (2017). https://doi.org/10.1007/s00167-017-4530-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-017-4530-x