
Abstract
Purpose
The purpose of this study was to compare the clinical results of isolated arthroscopic Bankart repair and those of arthroscopic Bankart repair with posterior capsulodesis for anterior shoulder instability with engaging Hill–Sachs lesions.
Methods
Thirty-five shoulders that underwent isolated arthroscopic Bankart repair (Bankart group) and 37 shoulders that underwent arthroscopic Bankart repair with posterior capsulodesis (remplissage group) for anterior shoulder instability with engaging Hill–Sachs lesions were evaluated retrospectively. The mean age at the time of the surgery was 26.1 ± 7.0 years in the Bankart group and 24.8 ± 9.0 years in the remplissage group.
Results
At the final follow-up, the Rowe and UCLA scores significantly improved in both the Bankart and remplissage groups (P < 0.001, in both groups). The post-operative mean deficit in external rotation at the side was 3° ± 10° in the Bankart group and 8° ± 23° in the remplissage group (P = n.s. and P = 0.044, respectively). There was no decrease in muscle strength in either group. The recurrence rate was 25.7 % in the Bankart group and 5.4 % in the remplissage group (P = 0.022).
Conclusions
Arthroscopic Bankart repair with posterior capsulodesis demonstrated good clinical outcomes with a low recurrence rate in the treatment for anterior shoulder instability with an engaging Hill–Sachs lesion. Although a limitation in external rotation was observed, there was no significant limitation of any other motion and no decrease in muscle strength after the remplissage procedure. Posterior capsulodesis alone for remplissage should be considered as a surgical technique that can replace the conventional method.
Level of evidence
Case–control study, Level III.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several studies have investigated the effects of the Hill–Sachs lesion on recurrent glenohumeral instability and identified it as a contributor in the failure of anterior soft tissue stabilization [4, 6, 9, 21]. With recurrent episodes of glenohumeral instability, the lesion becomes larger and deeper, thereby increasing the risk of further instability [4]. Various surgical options for the management of recurrent anterior shoulder instability with an engaging Hill–Sachs lesion have been introduced.
Filling of the bony defect in the humeral head with a portion of the posterior capsule and infraspinatus tendon was first described by Connolly in 1972 [12]. Filling the humeral defect converts it to an extra-articular lesion and prevents the humeral head from engaging with the glenoid rim; posterior capsulotenodesis acts as a stabilizer, thereby preventing anterior translation of the humeral head. Purchase et al. [28] modified Connolly’s procedure and were the first to use the term “remplissage” (“to fill” in French). They described the procedure as arthroscopic posterior capsulodesis and infraspinatus tenodesis to fill the Hill–Sachs lesion in addition to the arthroscopic Bankart procedure.
Although several authors have reported the clinical outcomes of the arthroscopic remplissage procedure [2, 4, 5, 14–16, 20, 24, 26, 28, 29, 40], they performed both infraspinatus tenodesis and posterior capsulodesis to fill the humeral head defect. This “non-anatomic procedure” may induce changes in shoulder biomechanics including range of motion (ROM) and muscle strength, resulting from abnormal undue tension on the posterior structure. Accordingly, it is thought to produce more unexpected post-operative adverse effects than isolated Bankart repair. To minimize these adverse effects, one may consider enforcing only posterior capsulodesis without infraspinatus tenodesis to reduce abnormal undue tension on the posterior structure. To our knowledge, there is no information on the clinical outcomes of arthroscopic posterior capsulodesis alone for remplissage.
The purpose of this study was to compare the clinical results of isolated arthroscopic Bankart repair with those of arthroscopic Bankart repair with posterior capsulodesis for anterior shoulder instability with engaging Hill–Sachs lesions. It was hypothesized that the remplissage procedure would have a lower recurrence rate than isolated Bankart repair. It was also hypothesized that some limitation in shoulder motion and decrease in strength of external rotators would be inevitable in the remplissage group compared to the isolated Bankart repair group.
Materials and methods
Seventy-two patients with an Instability Severity Index Score (ISIS) [3] of ≥3 and an isolated large (Calandra [8] grade 3) or engaging Hill–Sachs lesion confirmed on dynamic arthroscopic examination and without significant glenoid bone loss (glenoid deficit <25 %) on three-dimensional computed tomography (3D CT) were enroled in this study. Thirty-five patients underwent isolated arthroscopic Bankart repair (Bankart group), and 37 patients underwent arthroscopic Bankart repair with posterior capsulodesis alone for the remplissage procedure (remplissage group). Patients with only soft tissue lesions, hyperlaxity (2+ or greater laxity on the sulcus sign) or voluntary instability, glenoid defects >25 % of the inferior glenoid diameter, rotator cuff tears, severe pre-existing glenohumeral osteoarthritis, or epilepsy were excluded from the study. Patients who underwent the Latarjet procedure were also excluded. All patients underwent routine preoperative radiography and 3D CT scans to check for evidence of a substantial bony lesion of the glenoid and humerus. The glenoid bone deficit was calculated based on the AP distance using the bare area method [37] on the en face view of 3D CT [11, 18]; the depth of the Hill–Sachs lesion was measured directly on an axial CT image, in the area where the size of the lesion was the largest, with a digital measurement tool, and was defined as the longest length between the bottom of the lesion and the corresponding arc.
The mean patient age at the time of the surgery was 26.1 ± 7.0 years (range 14–46 years) in the Bankart group and 24.8 ± 9.0 years (range 14–52 years) in the remplissage group. The mean follow-up period was 22.9 ± 13.5 months (range 12–48 months) and 24.7 ± 9.5 months (range 19–31 months), respectively. Patient demographic details for both groups are summarized in Table 1. There were no significant differences in the demographic data between the two groups.
Surgical techniques
All surgeries were performed by the senior author, with the patient in a 70° beach chair position. With the arthroscope in the posterior portal, the arm was brought into abduction and external rotation (ER), and the humeral head was pushed anteriorly to confirm an engaging humeral defect over the anterior glenoid rim.
After completion of the anterior capsulolabral repair, the remplissage procedure was performed. Four limbs from the two single-loaded anchors were relayed by passage through the infraspinatus and the posterior joint capsule and pulled through the small skin incision. The knot pusher was pushed along the two limbs of each anchor to enable dissection of the muscular portion of the infraspinatus around the limb to the posterior capsule. Care was taken not to strip off the posterior capsule from the limb. Once all the muscular portions of the infraspinatus were stripped from the four limbs of both anchors, the limbs from each anchor were tied.
Post-operative rehabilitation
Patients of both groups underwent rehabilitation according to the same general protocol for each group. In the Bankart group, the shoulders were immobilized for 3 weeks post-operatively. In the meantime, only pendulum exercises were allowed. Three weeks after the surgery, passive elevation and ER were performed to achieve full ROM at 6 weeks post-operatively. Muscle strengthening exercises followed. Patients were allowed to participate in sport activities only after they had gained full range of shoulder motion without pain and near-normal muscle strength. In the remplissage group, use of a shoulder sling for inhibition of abduction and ER was recommended for 6 weeks. After 6 weeks, patients were allowed to remove the sling for active movements. Contact sports or “at-risk” work-related activities were not allowed for 6 months.
Preoperative and post-operative evaluations
A retrospective analysis of the prospectively collected patient data was performed. A thorough patient history regarding the cause of initial dislocation, type of dislocation, interval between the first and second dislocations, and frequency of dislocation was obtained before the surgery. The load-and-shift test and sulcus sign test were performed in both shoulders to check anterior, posterior, and inferior translations and general laxities.
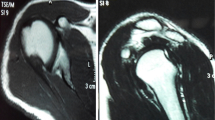
Preoperative and post-operative pain and instability were assessed with the visual analogue scale (VAS), with 0 indicating a painless stable shoulder and 10 indicating a severely painful unstable shoulder. Active and passive shoulder ROM in forward flexion (FF), ER at the side (ERs), external and internal rotations at 90° of abduction (ERa and IRa), and internal rotation to the posterior (IRp) were assessed, with the patient in the seated position. Quantitative muscle strength measurements were assessed with the use of a portable, hand-held Nottingham Mecmesin Myometer (Mecmesin Co, Nottingham, UK). The Rowe score [32] and the Shoulder Rating Scale of the University of California at Los Angeles (UCLA) score [13] were used for clinical assessment. In the remplissage group, all patients underwent preoperative magnetic resonance imaging (MRI), and magnetic resonance arthrography (MRA) was performed at least 6 months post-operatively to evaluate the integrity of the humeral defect filling as a structural outcome. The grade of the “filling” from the posterior joint capsule to the humeral head defect was assessed on the axial plane in the region where the size of the lesion was the largest on the MRA images. All values were measured directly using digital imaging software. The post-operative filling was classified into five categories based on the axial views of T2-weighted images [31]: grade 4, complete filling with no fluid equivalent signal; grade 3, partial filling with a minor defect (<50 % of the whole length of the lesion); grade 2, partial filling with a major defect (≥50 % of the whole length of the lesion); grade 1, minimal filling with a significant free fluid level; and grade 0, filling failure with dehiscence.
Final approval of exemption from review by the IRB was obtained for this study because of its retrospective nature (KHNMC IRB 2012-136).
Statistical analysis
The paired t test was performed to evaluate the differences in preoperative and post-operative values. For a comparison of results between the two groups, the Student’s t test was used, and the χ 2 test was used for comparing proportions between groups. The level of significance was set at 0.05 with associated 95 % confidence intervals. The SPSS software package (version 18.0; SPSS, Inc., an IBM Company, Chicago, Illinois) was used for all statistical analyses. For a power analysis, we additionally adopted a stringent approach of a conditional power analysis of two proportions using the Power and Sample Size Calculation Program (version 3.1.2, 2014).
Results
A detailed comparison of the preoperative variables in both groups is presented in Table 2. There was no significant difference between the two groups.
At the final follow-up, there were statistically significant discrepancies in IRp compared with the contralateral shoulder in the Bankart group (P = 0.009) and in ERs and IRp in the remplissage group (P < 0.001 and P = 0.002, respectively) (Table 3). Preoperative ROM and post-operative ROM in both groups are summarized in Table 4. At the final follow-up, there was a statistically significant restriction in ERs in the remplissage group (P = 0.044). However, there was no significant difference in post-operative ROM between the Bankart and remplissage groups.
The VAS score for pain during motion and instability and the Rowe and UCLA scores showed statistically significant improvement after the surgery in both groups (Table 5). When the two groups were compared, the remplissage group had better post-operative results for some of the variables. There was a significant difference in the VAS score for instability and in the Rowe score between the two groups (P = 0.004 and 0.011, respectively). At the final follow-up, there was a significant increase in the muscle strength of forward flexors in the Bankart group (P = 0.047) and of external rotators, internal rotators, and abductors in the remplissage group (P = 0.006, 0.009, and <0.001, respectively).
In the remplissage group, 20 of 37 patients underwent MRA at least 6 months post-operatively. The post-operative MRA examination of the fillings revealed grade 4 in 13 patients (65 %), grade 3 in three patients (15 %), grade 2 in two patients (10 %), grade 1 in one patient (5 %), and grade 0 in one patient (5 %).
The overall recurrence rate (positive apprehension sign, subluxation, or dislocation) in the Bankart group (25.7 %, nine of 35 patients) was significantly higher than that in the remplissage group (5.4 %, two of 37 patients) (P = 0.022), and the frank redislocation rates were 14.3 % (five patients) and 0 %, respectively (P = 0.023).
Among nine patients who had recurrent instability in the Bankart group, five patients who experienced a frank dislocation required additional surgery. Two patients underwent open Bankart repair as a revision surgery (at 12 and 25 months post-operatively, respectively); two patients underwent the Latarjet procedure (at 11 and 33 months post-operatively, respectively); and 1 patient underwent revision arthroscopic Bankart repair with the remplissage procedure (at 12 months post-operatively). Four patients who had positive apprehension sign or subluxation post-operatively did not require additional stabilization surgery. They recovered with conservative treatment, which included muscle strengthening exercises.
Among the two patients who had recurrent instability in the remplissage group, one had persistent pain and subjective apprehension sign without frank dislocation at 18 months post-operatively. As the MRA demonstrated a 100 % filling of the humeral defect, conservative treatment was adopted. The other patient also had subjective apprehension sign without frank dislocation at 6 months post-operatively when playing basketball at a competitive level, but underwent conservative treatment with no other event of recurrence.
At the final follow-up, in the Bankart group, 19 (57.6 %) of the 33 active patients showed complete return to preinjury activity levels (grade 1); 12 (36.4 %) showed near return to preinjury activity levels (≥90 % recovery) (grade 2); and 2 (6.0 %) showed return to preinjury activity levels with moderate limitations (≥70 % recovery) (grade 3). In the remplissage group, the post-operative filling was classified as grade 1 in 22 (68.8 %) of the 32 active patients, grade 2 in seven (21.9 %), and grade 3 in three (9.3 %). There was no significant difference in the return to sport activities between the two groups (n.s.).
Discussion
The most important finding of the present study was that arthroscopic Bankart repair with posterior capsulodesis was associated with a significantly lower recurrence rate than isolated Bankart repair. In addition, even though a limitation in ERs was observed, there was no significant limitation of any other motion and no decrease in muscle strength after the remplissage procedure.
Despite the advances of the arthroscopic Bankart repair technique, in some cases, it has been associated with a disappointing result. In 2000, Burkhart and De Beer [7] refocused attention on the role of the engaging Hill–Sachs lesion in recurrent anterior shoulder instability. They reported an unacceptable high failure rate of 67 % after arthroscopic Bankart repair in patients with glenohumeral bone deficiency and recurrence in all of the three cases with engaging Hill–Sachs lesions. Patel et al. [27] attributed most failures of prior surgeries for correction of instability to an unidentified Hill–Sachs lesion. Similarly, Lynch et al. [23] attributed up to 93 % of recurrent instability cases to large engaging Hill–Sachs lesions.
Although there are several studies on the treatment for glenoid bone loss [23, 25, 33–38], bone defects of the humeral head have not been thoroughly evaluated. There is little consensus regarding surgical indications or standard treatments to reconstruct defects of the humeral head [22]. Surgical procedures to correct bony defects of the humeral head include the remplissage procedure [5, 28, 29], osteoarticular humeral head allograft [10, 36], resurfacing arthroplasty [23], rotational osteotomy of humerus [39], transhumeral head plasty [30], and percutaneous humeroplasty [19].
Currently, the arthroscopic technique, which helps avoid complications frequently associated with open, non-physiologic procedures such as the Latarjet procedure, is of great interest in the field of shoulder surgery [17]. The remplissage procedure, initially described as an open technique, was re-described by Purchase et al. [28] as an arthroscopic technique in 2008. This is partially related to patient selection in this study, because the authors have performed the remplissage procedure since 2008.
In the present study, the first hypothesis was that the remplissage procedure provides more stability to the shoulder joint in the presence of an engaging Hill–Sachs lesion. Up until the final follow-up, the remplissage group had an overall recurrence rate of 5.4 % and a frank redislocation rate of 0 %, whereas the Bankart group had a significantly higher recurrence rate of 25.7 % and redislocation rate of 14.3 %. The Rowe score also showed a significantly higher improvement in the remplissage group than in the Bankart group. These results confirm that filling humeral head defects using a remplissage procedure can prevent engaging of the Hill–Sachs lesion with the glenoid rim and support Bankart repair. The overall recurrence rate in this study was lower than the 8 % recurrence rate following the combined procedure reported by Purchase et al. [28], but slightly higher than the 2 % recurrence rate reported by Boileau et al. [4] and 0 % recurrence rate reported by Franceschi et al. [14].
The second hypothesis was that some limitation in shoulder motion and decrease in strength of external rotators were inevitable after the remplissage procedure. As remplissage is a non-anatomic procedure, there have been concerns regarding a theoretical adverse effect on post-operative shoulder motion, particularly the loss of ER [1, 4, 14, 24, 40]. In the current study, tightness of the posterior capsule, which was secondary to undue tension during the remplissage procedure, resulted in a limitation of 8° in ER. Although ER was significantly limited in the remplissage group, there was no significant difference in post-operative ER between the Bankart and remplissage groups. Our results are in agreement with those reported by Boileau et al. [4], who also found an 8° restriction in ER and a 9° restriction in ERa. Nourissat et al. [24] presented a series of 15 arthroscopic Bankart repairs with remplissage, with a limitation of 4° in ERs and 3° in ERa. Franceschi et al. [14] also reported a 2° loss in ERs in 25 cases of arthroscopic Bankart repair with remplissage. In the current study, muscle strength was not decreased, and the strength of external rotators, internal rotators, and abductors was, in fact, significantly increased after remplissage. The infraspinatus muscle was split less than 1 cm in length, parallel with the muscle fibres, for posterior capsulodesis, and the tendon portion was not captured with the suture material. The key for yielding better muscle strength is to minimize injury to the infraspinatus muscle.
In this study, arthroscopic Bankart repair with the remplissage procedure differed from the original technique described by Purchase et al. [28] in that the Bankart lesion was repaired first, and the trans-cuff lateral portal was used as the main viewing portal. Since a Bankart repair is considered to have priority over a remplissage procedure, remplissage has been performed after completion of Bankart repair. Several authors have described different sequential steps. Most authors complete remplissage first and then repair Bankart lesions [4, 26, 28]. Koo et al. [20] described the so-called double pulley technique, in which, after both sides were prepared, they repaired the Bankart lesion first and then tied the remplissage sutures. Other authors performed the remplissage through the anterosuperior portal as the main viewing portal. However, the trans-cuff lateral portal in the present study enabled the surgeons to secure a better view of the Hill–Sachs lesion. Further, a small additional incision was made to dissect the infraspinatus muscle so that posterior capsulodesis could be performed into the Hill–Sachs lesion. Infraspinatus tenodesis is considered to possibly lead to strangulation of the tendon and entanglement of the multiple sutures in the subacromial space. Posterior capsulodesis, therefore, may reduce the possibility of infraspinatus tendon strangulation.
This study has several limitations. First, this study was a retrospective analysis and therefore has limitations similar to those seen in other retrospective studies. However, we conducted a retrospective analysis of prospectively collected patient data. Second, the mean follow-up period was relatively short. Post-operative complications after remplissage might occur during long-term follow-up. However, the arthroscopic remplissage procedure was introduced only recently, and the pros and cons of the procedure are still not clearly known. Lastly, posterior capsulodesis alone for remplissage was not compared directly with the conventional remplissage technique. However, this study is important for improving the technique of the remplissage procedure for anterior shoulder instability with an engaging Hill–Sachs lesion.
Conclusions
Arthroscopic Bankart repair with posterior capsulodesis demonstrated good clinical outcomes with a low recurrence rate in the treatment for anterior shoulder instability with an engaging Hill–Sachs lesion. Although a limitation in ER was observed, there was no significant limitation of any other motion and no decrease in muscle strength after the remplissage procedure. Posterior capsulodesis alone for remplissage should be considered as a surgical technique that can replace the conventional method.
References
Argintar E, Heckmann N, Wang L, Tibone JE, Lee TQ (2014) The biomechanical effect of shoulder remplissage combined with Bankart repair for the treatment of engaging Hill-Sachs lesions. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3092-4
Armitage MS, Faber KJ, Drosdowech DS, Litchfield RB, Athwal GS (2010) Humeral head bone defects: remplissage, allograft, and arthroplasty. Orthop Clin North Am 41(3):417–425
Balg F, Boileau P (2007) The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br 89(11):1470–1477
Boileau P, O’Shea K, Vargas P, Pinedo M, Old J, Zumstein M (2012) Anatomical and functional results after arthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am 94(7):618–626
Brilakis E, Mataragas E, Deligeorgis A, Maniatis V, Antonogiannakis E (2014) Midterm outcomes of arthroscopic remplissage for the management of recurrent anterior shoulder instability. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-2848-1
Burkhart SS, Danaceau SM (2000) Articular arc length mismatch as a cause of failed bankart repair. Arthroscopy 16(7):740–744
Burkhart SS, De Beer JF (2000) Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 16(7):677–694
Calandra JJ, Baker CL, Uribe J (1989) The incidence of Hill-Sachs lesions in initial anterior shoulder dislocations. Arthroscopy 5(4):254–257
Cetik O, Uslu M, Ozsar BK (2007) The relationship between Hill-Sachs lesion and recurrent anterior shoulder dislocation. Acta Orthop Belg 73(2):175–178
Chapovsky F, Kelly JD (2005) Osteochondral allograft transplantation for treatment of glenohumeral instability. Arthroscopy 21(8):1007
Chuang TY, Adams CR, Burkhart SS (2008) Use of preoperative three-dimensional computed tomography to quantify glenoid bone loss in shoulder instability. Arthroscopy 24(4):376–382
Connolly JF (1972) Humeral head defects associated with shoulder dislocations: their diagnostic and surgical significance. Instr Course Lect 21:42–54
Ellman H, Hanker G, Bayer M (1986) Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am 68(8):1136–1144
Franceschi F, Papalia R, Rizzello G, Franceschetti E, Del Buono A, Panasci M, Maffulli N, Denaro V (2012) Remplissage repair—new frontiers in the prevention of recurrent shoulder instability: a 2-year follow-up comparative study. Am J Sports Med 40(11):2462–2469
Giles JW, Elkinson I, Ferreira LM, Faber KJ, Boons H, Litchfield R, Johnson JA, Athwal GS (2012) Moderate to large engaging Hill-Sachs defects: an in vitro biomechanical comparison of the remplissage procedure, allograft humeral head reconstruction, and partial resurfacing arthroplasty. J Shoulder Elbow Surg 21(9):1142–1151
Haviv B, Mayo L, Biggs D (2011) Outcomes of arthroscopic “remplissage”: capsulotenodesis of the engaging large Hill-Sachs lesion. J Orthop Surg Res 6:29
Hovelius LK, Sandstrom BC, Rosmark DL, Saebo M, Sundgren KH, Malmqvist BG (2001) Long-term results with the Bankart and Bristow-Latarjet procedures: recurrent shoulder instability and arthropathy. J Shoulder Elbow Surg 10(5):445–452
Huysmans PE, Haen PS, Kidd M, Dhert WJ, Willems JW (2006) The shape of the inferior part of the glenoid: a cadaveric study. J Shoulder Elbow Surg 15(6):759–763
Kazel MD, Sekiya JK, Greene JA, Bruker CT (2005) Percutaneous correction (humeroplasty) of humeral head defects (Hill-Sachs) associated with anterior shoulder instability: a cadaveric study. Arthroscopy 21(12):1473–1478
Koo SS, Burkhart SS, Ochoa E (2009) Arthroscopic double-pulley remplissage technique for engaging Hill-Sachs lesions in anterior shoulder instability repairs. Arthroscopy 25(11):1343–1348
Kralinger FS, Golser K, Wischatta R, Wambacher M, Sperner G (2002) Predicting recurrence after primary anterior shoulder dislocation. Am J Sports Med 30(1):116–120
Longo UG, Loppini M, Rizzello G, Ciuffreda M, Berton A, Maffulli N, Denaro V (2014) Remplissage, humeral osteochondral grafts, weber osteotomy, and shoulder arthroplasty for the management of humeral bone defects in shoulder instability: systematic review and quantitative synthesis of the literature. Arthroscopy 30(12):1650–1666
Lynch JR, Clinton JM, Dewing CB, Warme WJ, Matsen FA 3rd (2009) Treatment of osseous defects associated with anterior shoulder instability. J Shoulder Elbow Surg 18(2):317–328
Nourissat G, Kilinc AS, Werther JR, Doursounian L (2011) A prospective, comparative, radiological, and clinical study of the influence of the “remplissage” procedure on shoulder range of motion after stabilization by arthroscopic Bankart repair. Am J Sports Med 39(10):2147–2152
Ochoa E Jr, Burkhart SS (2009) Glenohumeral bone defects in the treatment of anterior shoulder instability. Instr Course Lect 58:323–336
Park MJ, Tjoumakaris FP, Garcia G, Patel A, Kelly JDT (2011) Arthroscopic remplissage with Bankart repair for the treatment of glenohumeral instability with Hill-Sachs defects. Arthroscopy 27(9):1187–1194
Patel RV, Apostle K, Leith JM, Regan WD (2008) Revision arthroscopic capsulolabral reconstruction for recurrent instability of the shoulder. J Bone Joint Surg Br 90(11):1462–1467
Purchase RJ, Wolf EM, Hobgood ER, Pollock ME, Smalley CC (2008) Hill-sachs “remplissage”: an arthroscopic solution for the engaging hill-sachs lesion. Arthroscopy 24(6):723–726
Rashid MS, Crichton J, Butt U, Akimau PI, Charalambous CP (2014) Arthroscopic “Remplissage” for shoulder instability: a systematic review. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-2881-0
Re P, Gallo RA, Richmond JC (2006) Transhumeral head plasty for large Hill-Sachs lesions. Arthroscopy 22(7):798 e791–798 e794
Rhee YG, Cho NS, Yoo JH, Lee WG (2015) Filling index score of remplissage (FISOR): a useful measurement tool to evaluate structural outcome after remplissage. J Shoulder Elbow Surg 24:613–620
Rowe CR, Patel D, Southmayd WW (1978) The Bankart procedure: a long-term end-result study. J Bone Joint Surg Am 60(1):1–16
Saito H, Itoi E, Sugaya H, Minagawa H, Yamamoto N, Tuoheti Y (2005) Location of the glenoid defect in shoulders with recurrent anterior dislocation. Am J Sports Med 33(6):889–893
Scheibel M, Kraus N, Diederichs G, Haas NP (2008) Arthroscopic reconstruction of chronic anteroinferior glenoid defect using an autologous tricortical iliac crest bone grafting technique. Arch Orthop Trauma Surg 128(11):1295–1300
Schmid SL, Farshad M, Catanzaro S, Gerber C (2012) The Latarjet procedure for the treatment of recurrence of anterior instability of the shoulder after operative repair: a retrospective case series of forty-nine consecutive patients. J Bone Joint Surg Am 94(11):e75
Sekiya JK, Wickwire AC, Stehle JH, Debski RE (2009) Hill-Sachs defects and repair using osteoarticular allograft transplantation: biomechanical analysis using a joint compression model. Am J Sports Med 37(12):2459–2466
Sugaya H, Kon Y, Tsuchiya A (2005) Arthroscopic repair of glenoid fractures using suture anchors. Arthroscopy 21(5):635
Warner JJ, Gill TJ, O’Hollerhan JD, Pathare N, Millett PJ (2006) Anatomical glenoid reconstruction for recurrent anterior glenohumeral instability with glenoid deficiency using an autogenous tricortical iliac crest bone graft. Am J Sports Med 34(2):205–212
Weber BG, Simpson LA, Hardegger F (1984) Rotational humeral osteotomy for recurrent anterior dislocation of the shoulder associated with a large Hill-Sachs lesion. J Bone Joint Surg Am 66(9):1443–1450
Zhu YM, Lu Y, Zhang J, Shen JW, Jiang CY (2011) Arthroscopic Bankart repair combined with remplissage technique for the treatment of anterior shoulder instability with engaging Hill-Sachs lesion: a report of 49 cases with a minimum 2-year follow-up. Am J Sports Med 39(8):1640–1647
Acknowledgments
This research was supported by sports scientification of Convergent R&D Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (NRF-2014M3C1B1033319).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cho, N.S., Yoo, J.H., Juh, H.S. et al. Anterior shoulder instability with engaging Hill–Sachs defects: a comparison of arthroscopic Bankart repair with and without posterior capsulodesis. Knee Surg Sports Traumatol Arthrosc 24, 3801–3808 (2016). https://doi.org/10.1007/s00167-015-3686-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3686-5