
Abstract
Background
Ionizing radiation is an integral part of percutaneous coronary angiographies. Chronic exposure to low-dose radiation confers a risk for skin damage, eye lens opacities or cataracts, and malignant diseases to staff in the catheter laboratory. The RADPAD is a sterile surgical drape that reduces the effect of scatter radiation on the operator. We sought to assess the efficacy of RADPAD shields in reducing radiation dose experienced by operators during routine diagnostic coronary angiography.
Patients and methods
Sixty consecutive patients due to undergo elective coronary angiography were randomized in a 1:1 pattern to have their procedures performed with and without the RADPAD drape in situ. Dosimetry was performed on the left arm of the primary operator.
Results
There was no significant difference in the two main determents of radiation exposure in both groups: the screening times (102 ± 86 s for the RADPAD group vs. 105 ± 36 s for the control group, p = 0.9) and body mass index (BMI; 27.7 ± 4.2 kg/m2 for the RADPAD group vs. 27.9 ± 5.5 kg/m2 for the control group, p = 0.8). Moreover, there was no difference in the dose–area ratio (1337 ± 582 cGy/cm2 for the RADPAD group vs. 1541 ± 804 cGy/cm2 for the control group, p = 0.3) between the two patient groups. The primary operator radiation dose was significantly lower in the RADPAD group at 8.0 µSv (Q1: 3.2, Q3: 20.1) compared with 19.6 µSv (Q1: 7.1, Q3: 37.7) for the control group (p = 0.02).
Conclusion
The RADPAD significantly reduces radiation exposure to primary operators during routine diagnostic coronary angiography in patients with a BMI > 25 kg/m2. It reduces total radiation exposure to primary operators by 59%, and the radiation exposure rate by 47%.
Zusammenfassung
Hintergrund
Trotz der Verwendung von Strahlenschutzkleidung besteht durch die Streustrahlung eine Strahlenbelastung für den interventionell tätigen Kardiologen. RADPAD ist ein steriles Strahlenschutztuch, die die Belastung der Streustrahlung für den Untersucher reduziert. Die Autoren untersuchten, ob sich bereits bei diagnostischen Koronarangiographien die Belastung durch Streustrahlung für den Untersucher durch die Verwendung des RADPAD reduzieren lässt.
Methoden
Hierzu wurden 60 Patienten, bei denen eine diagnostische Koronarangiographie mit standardisiertem Untersuchungsablauf durchgeführt wurde, 1:1 randomisiert in eine Gruppe mit und eine ohne RADPAD.
Ergebnisse
Beide Gruppen zeigten hinsichtlich der Durchleuchtungszeit (105 ± 36 s in der Kontrollgruppe bzw. 102 ± 86 s in der Strahlenschutztuchgruppe, p = 0,9) und des Body-Mass-Index (27,9 ± 5,5 kg/m2 in der Kontrollgruppe bzw. 27,7 ± 4,2 kg/m2 in der Strahlenschutztuchgruppe, p = 0,98), welche die maßgeblichen Faktoren für die kumulative Streustrahlungsdosis sind, keine signifikanten Unterschiede. Auch hinsichtlich des Dosis-Flächen-Produkts (DFP) ergab sich zwischen beiden Gruppen kein Unterschied: Das DFP betrug in der Kontrollgruppe 1541 ± 804 cGy/cm2, in der Strahlenschutztuchgruppe 1337 ± 582 cGy/cm2 (p = 0,3). Die einwirkende Strahlenäquivalenzdosis erwies sich jedoch in Strahlenschutztuchgruppe mit 8,0 µSv (Q1: 3,2; Q3: 20,1) als signifikant geringer im Vergleich zu 19,6 µSv (Q1: 7,1; Q3: 37,7) in der Kontrollgruppe (p = 0,02).
Schlussfolgerung
Durch die Verwendung des Strahlenschutztuchs wurde im Vergleich zur Kontrollgruppe die Strahlenbelastung für den Untersucher bereits bei diagnostischen Koronarangiographien bei Patienten mit einem BMI > 25 kg/m2 signifikant reduziert. Insgesamt konnte die Strahlenbelastung des Untersuchers (−59 %) und die Strahlenbelastungsrate (−47 %) reduziert werden.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Although there have been many improvements over the past decades in optimizing coronary angiography, ionizing radiation remains an important issue. Chronic exposure to low-dose radiation as experienced by interventional cardiologists confers an increased risk for skin damage, eye lens opacities or cataracts, and various malignant diseases [1–4].
In any coronary angiography, the amount of radiation exposure to the operator is determined among other factors by the body mass index (BMI) of the patient, by the duration of the fluoroscopic procedure, and by the respective experience of the operator.
The RADPAD (Worldwide Innovations & Technologies, Inc., Kansas City, Kan.) is a sterile surgical drape containing bismuth and antimony. When positioned correctly on the patient between the image intensifier and the operator, the RADPAD has been shown to reduce the effect of scatter radiation on the operator. Utilization of the RADPAD has already been shown to reduce radiation exposure in routine percutaneous coronary intervention (PCI) procedures, complex PCI procedures [5], peripheral endovascular procedures [6], cardiac resynchronization therapy device implantation [7, 8], and fluoroscopically guided electrophysiological procedures [9].
We sought to assess the efficacy of RADPAD shields in reducing the radiation dose experienced by operators during routine diagnostic coronary angiography via transfemoral access.
Patients and methods
In total, 60 consecutive patients due to undergo elective coronary angiography were identified and randomized in a 1:1 pattern to have their procedures performed with and without the RADPAD drape. Patients with a history of coronary bypass surgery (CABG) were excluded.
During the angiography, standard shielding equipment was used, including a lead coat, thyroid shield, and protective lenses, in addition to a lead shield suspended from the ceiling between the image intensifier and the operator. All operators had undergone radiation awareness courses and were trained in the optimal placement of the RADPAD drape.
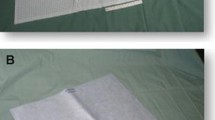
All coronary angiographies were performed from the right femoral artery. The RADPAD was positioned superior to the sheath insertion point, immediately below the lead shield suspended from the ceiling between the image intensifier and the operator (Fig. 1). All coronary angiographies were performed using the same angulations, the same number of frames, and the same settings in the same biplane cardiology intervention suite (Artis zee, Siemens, Germany).

Positioning of RADPAD. This figure shows the correct positioning of the RADPAD. The shield is placed on the patient’s leg around the area of sheath insertion (red lines)
The dosimeter was placed on the upper, outer aspect of the left arm of the operator, at the level of the mid humerus of the operator. Dosimetric measurements were obtained using an Unfors EDD meter (Unfors Instruments AB, Billdal, Sweden). The dosimeter was commenced at the start of the procedure, and the dose was recorded immediately after the end of the procedure. Screening times (ST) and dose–area ratios (DAR) for each individual procedure were collected prospectively. The study was approved by the local ethics committee of the Charité – Universitätsmedizin Berlin, and every patient gave informed consent to this study.
For continuous data with normal distribution, an independent-samples t test was used. Otherwise, the nonparametric Mann–Whitney U test was used. Continuous data with normal distribution are reported as mean ± SD, or otherwise as median and quartiles. A p value of <0.05 was accepted as statistically significant.
Results
During the study period, 60 patients were successfully randomized to undergo diagnostic angiography with RADPAD or no shield (no RADPAD). The mean age of the study group was 62.5 ± 12.8 years and 37% were female. The baseline characteristics of the study population according to the randomization groupings were similar (Table 1).
There was no significant difference in the two main determents of radiation exposure in both groups: the screening times (102 ± 86 s for the RADPAD group vs. 105 ± 36 s for the control group, p = 0.89) and BMI (27.7 ± 4.24 kg/m2 for the RADPAD group vs. 27.9 ± 5.53 kg/m2 for the control group, p = 0.85).
Furthermore, there was no difference in the DAR (1336.9 ± 581.6 cGy/cm2 for the RADPAD group vs. 1541.0 ± 803.7 cGy/cm2 for the control group, p = 0.26) between the two patient groups (Table 2).
The primary operator radiation dose was significantly lower in the RADPAD group at 8.0 µSv (Q1: 3.2, Q3: 20.1) compared with 19.6 µSv (Q1: 7.1, Q3: 37.7) for the control group (p = 0.02).
The dose rate, however, was not significantly lower in the RADPAD group at 5.8 μSv/min (Q1: 2.0, Q3: 15.8) compared with 11.0 μSv/min (Q1: 4.3, Q3: 19.3) for the control group, (p = 0.08; Table 2).
Next we analyzed operator radiation dose according to the BMI. We therefore divided the patients into two different BMI groups. The analysis revealed a significant dose reduction in the BMI group of >25 kg/m2 (RADPAD group 12.9 µSv [Q1: 4.5, Q3: 21.0] vs. 32.7 [Q1: 17.1, Q3: 39.0] for the control group, p = 0.006), whereas in the BMI group of <25 kg/m2 (RADPAD group 2.2 µSv [Q1: 2.1, Q3: 9.0] vs. 6.4 µSv [Q1: 3.7, Q3: 16.9] for the control group, p = 0.15) there was no statistically significant reduction (Table 3).
We then analyzed the effects of the RADPAD in reducing radiation exposure to the operator. Total radiation exposure to primary operators was reduced using the RADPAD by 59% overall. In the BMI group of >25 kg/m2 there was a 61% reduction in radiation exposure, whereas in the BMI group of <25 kg/m2 there was a 66% reduction (Table 3; Fig. 2).

Dose reduction. Primary operator dose reduction in all patients with a BMI of <25 kg/m2 and in patients with a BMI of >25 kg/m2. Data are expressed as mean ± SD. Red labels percent dose reduction
Discussion
The number of cardiologic interventional procedures has dramatically increased in the past decade [10] exposing the interventional cardiologist to more cumulative radiation exposure. Minimizing radiation exposure to patients and staff members is, therefore, important to interventional cardiologists. Even with standard protection equipment – including a lead coat, thyroid shield, and protective lenses, in addition to a lead shield suspended from the ceiling between the image intensifier and the operator – and techniques to minimize scatter radiation, including performing fluoroscopic imaging at the lowest available pulse rate, minimizing the number and duration of cine runs, minimizing the cine frame rate, and minimizing image amplification and collimation to areas of interest during PCI [4], radiation dose for the interventional cardiologists and the catheterization laboratory members remains a task of paramount importance.
Usage of the RADPAD has already been shown to reduce radiation exposure in complex PCI procedures with prolonged screening times [5]. The present randomized trial shows, however, for the first time that a sterile lead-free drape significantly reduces the radiation exposure to the interventional cardiologist already during routine diagnostic coronary angiography performed via the right femoral artery access with short screening times. Moreover, the study confirms that the use of the RADPAD is feasible and does not prolong the procedure as demonstrated by the short time employed for fluoroscopy.
This study had certain limitations. Radiation levels were measured only on the operator’s chest. It is conceivable that differences in radiation doses between the two groups may have been different from those observed if radiation levels had been measured at various sites including the left eye, the thyroid regions, and the left wrist.
Conclusion
This study showed that by using the RADPAD protection, total radiation exposure to primary operators could be reduced by half (59%) the amount without prolonging the procedure, despite the short screening time of a diagnostic coronary angiography. We therefore recommend, despite the additional costs involved (currently € 45, not reimbursed by the German health-care system), the integration of the RADPAD in diagnostic coronary angiography in patients with a BMI of >25 kg/m2. This probably also applies to non-coronary artery interventions, such as endomyocardial biopsy in patients with cardiomyopathies of heart failure with preserved ejection fraction either via a transradial or a transfemoral approach [11–13], and to electrophysiological ablation procedures [14].
References
Venneri L, Rossi F, Botto N, Andreassi MG, Salcone N, Emad A et al (2009) Cancer risk from professional exposure in staff working in cardiac catheterization laboratory: insights from the National Research Council’s Biological Effects of Ionizing Radiation VII Report. Am Heart J 157(1):118–124. doi:10.1016/j.ahj.2008.08.009
Koenig TR, Wolff D, Mettler FA, Wagner LK (2001) Skin injuries from fluoroscopically guided procedures: part 1, characteristics of radiation injury. Am J Roentgenol 177(1):3–11. doi:10.2214/ajr.177.1.1770003
Vano E, Gonzalez L, Fernandez JM, Haskal ZJ (2008) Eye lens exposure to radiation in interventional suites: caution is warranted. Radiology 248(3):945–953. doi:10.1148/radiol.2482071800
Amis ES Jr., Butler PF, Applegate KE, Birnbaum SB, Brateman LF, Hevezi JM et al (2007) American College of Radiology white paper on radiation dose in medicine. J Am Coll Radiol 4(5):272–284. doi:10.1016/j.jacr.2007.03.002
Murphy JC, Darragh K, Walsh SJ, Hanratty CG (2011) Efficacy of the RADPAD protective drape during real world complex percutaneous coronary intervention procedures. Am J Cardiol 108(10):1408–1410. doi:10.1016/j.amjcard.2011.06.061
Power S, Mirza M, Thakorlal A, Ganai B, Gavagan LD, Given MF et al (2015) Efficacy of a radiation absorbing shield in reducing dose to the interventionalist during peripheral endovascular procedures: a single centre pilot study. Cardiovasc Intervent Radiol 38(3):573–578. doi:10.1007/s00270-014-0997-8
Brambilla M, Occhetta E, Ronconi M, Plebani L, Carriero A, Marino P (2010) Reducing operator radiation exposure during cardiac resynchronization therapy. Europace 12(12):1769–1773. doi:10.1093/europace/euq356
Jones MA, Cocker M, Khiani R, Foley P, Qureshi N, Wong KC et al (2014) The benefits of using a bismuth-containing, radiation-absorbing drape in cardiac resynchronization implant procedures. Pacing Clin Electrophysiol 37(7):828–833. doi:10.1111/pace.12349
Germano JJ, Day G, Gregorious D, Natarajan V, Cohen T (2005) A novel radiation protection drape reduces radiation exposure during fluoroscopy guided electrophysiology procedures. J Invasive Cardiol 17(9):469–472
Bhargavan M (2008) Trends in the utilization of medical procedures that use ionizing radiation. Health Phys 95(5):612–627. doi:10.1097/01.HP.0000327659.42618.c1
Kherad B, Kohncke C, Spillmann F, Post H, Noutsias M, Pieske B et al (2016) Postprocedural radial artery occlusion rate using a sheathless guiding catheter for left ventricular endomyocardial biopsy performed by transradial approach. Bmc Cardiovasc Disord 16(1):253. doi:10.1186/s12872-016-0432-y
Noutsias M, Seeberg B, Schultheiss HP, Kuhl U (1999) Expression of cell adhesion molecules in dilated cardiomyopathy: evidence for endothelial activation in inflammatory cardiomyopathy. Circulation 99(16):2124–2131
Tschope C, Bock CT, Kasner M, Noutsias M, Westermann D, Schwimmbeck PL et al (2005) High prevalence of cardiac parvovirus B19 infection in patients with isolated left ventricular diastolic dysfunction. Circulation 111:879–886
Ma XX, Boldt LH, Zhang YL, Zhu MR, Hu B, Parwani A et al (2016) Clinical Relevance of Left Atrial Strain to Predict Recurrence of Atrial Fibrillation after Catheter Ablation: A Meta-Analysis. Echocardiography 33(5):724–733. doi:10.1111/echo.13184
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
B. Kherad, T. Jerichow, F. Blaschke, M. Noutsias, B. Pieske, C. Tschöpe, and F. Krackhardt declare that they have no competing interests.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki of 1975 (in its most recently amended version). Informed consent was obtained from all patients included in the study.
Rights and permissions
About this article

Cite this article
Kherad, B., Jerichow, T., Blaschke, F. et al. Efficacy of RADPAD protective drape during coronary angiography. Herz 43, 310–314 (2018). https://doi.org/10.1007/s00059-017-4560-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-017-4560-7