
Abstract
Objectives
The aim of this study was to assess social inequalities in overall mortality in a representative sample of the Italian population, and to evaluate the contribution of behavioural and metabolic risk (BMF) factors to these inequalities.
Methods
85,308 participants aged 25–74 years from the Italian Longitudinal Study were included in the study population and followed up for mortality (1999–2012). Level of education was used as a proxy for socioeconomic status. The contribution of BMF was estimated assessing the attenuation of the risk by education produced by the inclusion of BMF in regression model.
Results
Men with the lowest education had 62% and women had 57% greater risk of dying than those with the highest education. Among men, adjustment for BMF produced an attenuation of the mortality risk between extreme classes of education by 22%, while among women the risk attenuation was 7%.
Conclusions
Large educational differences in mortality were observed for both men and women. BMF reduced by approximately 20% differences in mortality relative risk between extreme classes of education in men. In contrast, a very low contribution was observed in women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over the last decades, a strong reduction in mortality occurred in industrialized countries, but substantial social inequalities in health persist in these populations, with lower mortality rates among individuals advantaged in terms of education, occupation and income (Kunst et al. 1998; Mackenbach et al. 1997). A large comparative study showed that inequalities are relatively small in Southern Europe, especially among women, compared to other European countries, in particular in Eastern European ones (Mackenbach et al. 2008). However, social inequalities still play a role in Italy, as showed by a recent study reporting that people with primary education have a 70% higher risk of death (79% men and 63% women) than those with tertiary education (Marinacci et al. 2013).
Understanding the main pathways whereby social determinants operate is a primary task in order to implement effective policies and strategies aimed at tackling health inequalities. Regarding this issue, there is evidence that behavioural risk factors are strongly shaped by social factors, including income, education, and employment (Braveman et al. 2011). For example, in Italy, the prevalence of obesity, physical inactivity and smoking increases with decreasing educational level, with the exception of smoking among women, for which the epidemiological transition is still ongoing and a higher prevalence is found among older women belonging to upper social strata (Salmaso et al. 2011).
On the other hand, the burden of disease and mortality explained by behavioural risk factors is very large: in Italy, it has been estimated that tobacco smoking, unhealthy diet, alcohol consumption and lack of physical activity are responsible for 30% of overall mortality (Piccinelli et al. 2015). Up to 80% of mortality from heart diseases, stroke and type 2 diabetes and over one-third of cancers could be prevented by eliminating those shared risk factors (WHO 2008).
Several studies have investigated the role of behavioural factors as mediators of socio-economic differences in mortality. However, results have a high variability across studies and the estimated contribution ranges from 12 to 72% (Harald et al. 2006; Laaksonen et al. 2008; Lantz et al. 1998; Schrijvers et al. 1999; Skalická et al. 2009; Strand and Tverdal 2004; Stringhini et al. 2010, 2011; van Oort et al. 2005; Woodward et al. 2003; Nandi et al. 2014; Nordahl et al. 2014). In general, behavioural factors have been found to contribute little to the socioeconomic gradient in mortality in Southern European countries (Eikemo et al. 2014), although, to our knowledge, no study has ever been conducted in Italy on this subject, except for smoking (Federico et al. 2013).
Aims
This study aims to assess social inequalities in overall mortality (excluding accidental causes), and cause-specific mortality (deaths from cancer, cardiovascular disease), as well as the contribution of behavioural risk factors (smoking, physical inactivity) and metabolic risk factors (obesity) to this gradient in a large cohort representative of the Italian population.
Methods
Data collection
The study population included all subjects aged 25–74 years who participated in the 1999–2000 edition of the Italian National Health Interview Survey (NHIS), followed up for mortality from 1999 to 2012. The NHIS is carried out mostly every 5 years by the Italian National Institute of Statistics (hereafter ISTAT). The survey provides detailed information on health conditions, including perceived health, long-term chronic diseases, disability, lifestyles (e.g., overweight and obesity, physical activity, smoking) and use of health services, as well as information on individual and household socioeconomic status. The NHIS edition here considered was conducted during the second semester of 1999 and the first semester of 2000 (from September 1999 to August 2000), with a response rate of 87%, on a representative sample of the Italian population. Data collection was conducted through face-to-face interview by trained interviewers, feature which allowed collecting data without missing values for all the variables investigated. Vital status, as well as causes of death for the deceased subjects, was obtained through individual level record-linkage with the Italian National Archive of Mortality 1999–2012. The follow-up was restricted to 85,308 subjects with complete information on fiscal code, as this was the linkage key of the cohort with the National Archive of Mortality. Subjects followed up did not differ significantly from those followed up regarding age (p = 0.10), sex (p = 0.65), and geographical area of residence (p = 0.14), whereas in the cohort enrolled in the study there was a lower proportion of low educated subjects (p < 0.001). The overall number of deaths observed corresponds to about 90% of the expected deaths calculated on the basis of the Italian mortality rates for the whole period. The Italian Longitudinal Study, authorized within the National Statistical Program, aims to prospectively follow up the samples of the National HIS, starting from the 1999–2000 NHIS edition, for mortality and morbidity.
Measurements
Information on socio-demographics, health status and exposure to risk factors (smoking, physical inactivity and obesity) at baseline was drawn from the NHIS. In particular, educational level was used as an indicator of socioeconomic status, classified into four categories: primary school or less (up to 5 years schooling), low secondary school (8 years), high school diploma (13 years), and university degree (≥ 17 years) (Cardano and Marinacci 2006). Regarding exposure to individual behaviours, information on smoking habit was classified into quartiles of lifetime smoking history, based on pack-years smoked (20 cigarettes per pack), keeping separate never smokers as the referent category. Information on physical activity practiced in the last 12 months with continuity was categorized into four levels: intense activity (sports: competitive or not), regular activity (jogging, gym, biking, gardening, etc.), light activity (walking, climbing stairs, etc.), and no physical activity. Regarding obesity, Body Mass Index (BMI) was calculated from height and weight self-reported in the survey, according to a standard procedure. The WHO classification was used to categorize BMI: normal weight (18.5 ≤ BMI < 25), underweight (BMI < 18.5), overweight (25 ≤ BMI < 30), and obese (BMI ≥ 30).
Health status at baseline was assessed through self-reported information both on general health, collected by means of the SF-12 questionnaire and used to compute a Physical Component Summary (PCS) index (Apolone et al. 2001), and on a list of 22 health conditions diagnosed by a physician, through which a Chronic Morbidity Index (CMI) was developed, based on their severity.
The outcomes investigated were mortality from all natural causes (excluding accidental causes of death; ICD-9: 000–799), neoplasms (ICD-9: 140–239; ICD-10: C00–D48) and cardiovascular diseases (ICD-9: 390–459; ICD-10: I00–I99). Respiratory diseases, and diseases of the digestive system (ICD-9: 520–579; ICD-10: K00–K93) were not considered in the analysis because too few subjects in the cohort died from these causes (13 and 14, respectively) in the reference category of education (university degree).
Statistical analysis
Poisson regression models with the Huber–White robust estimator of variance were used to evaluate the relative risk of death by educational level, stratifying by gender (Zou 2004). Different models were set up to assess the contribution of health and behavioural and metabolic risk factors (BMF) to social inequalities in mortality. Since morbidity could be a potential confounder or mediator of the association between BMF and mortality, the risk attenuation obtained adjusting for BMF was assessed through two different analyses, one with and the other without adjustment for health status at baseline. Regarding the former, Model 1 was set up with only age (5-year classes) and level of education, while in Model 2 risk factors (smoking, sedentary lifestyle, and BMI) were added. The same pattern of analyses was conducted including also health status, comparing Model 3 (age, level of education and health status) and Model 4 (age, level of education, behavioural risk factors and health status). Health status was assessed at baseline using the PCS indicator divided into quartiles and the CMI into five groups (subjects with diseases divided into quartiles, with those free of chronic diseases as the referent category). The contribution of factors (smoking, sedentary lifestyle and overweight) to educational inequalities in mortality was estimated in terms of Explained Fraction (EF), assessing the risk attenuation by education in Model 2 and Model 4, compared to Model 1 and Model 3, respectively. Regarding smoking, lifetime smoking history was assessed in the analyses as a mediator of educational differences in mortality.
The Explained Fraction was calculated by means of the following formula:
where unadjusted RR is the relative risk for the educational level considered, estimated in Model 1 and Model 3 and controlled only for age, compared to the highest education, while adjusted RR is the risk estimated in Model 2 and Model 4 and controlled also for BMF (Laaksonen et al. 2008). Since this methodology cannot be applied in the presence of an interaction between exposure and mediator, a test for interaction was performed between education and BMF on the risk of mortality.
A sensitivity analysis was also conducted, restricted to subjects who declared to be free of chronic diseases at baseline, to assess the contribution of BMF to social differences in mortality, independently from any assumption on role of health status (confounder or mediator) on the association between BMF and mortality.
All analyses were performed using the STATA V.13 software.
Results
The study population was composed of 85,291 participants, corresponding to 1,053,090 person-years. During a mean follow-up of 12.1 years (SD: 2.4), 7885 participants died from natural causes: 3384 from cancer, 2508 from cardiovascular diseases, 392 from digestive diseases and 363 from respiratory diseases.
Table 1 (men and women) show the distribution of educational level in the study population according to the age, geographical area, smoking habit, level of physical activity, BMI, and health status (PCS and CMI). In exploratory analyses, the geographic area of residence was included in the models as a potential confounder, but since it did not show any significant association with mortality, it was excluded from further analyses.
The proportion of women with primary school or less was higher than among men (37.2 vs 29.0%), whereas for graduates there were no differences between genders (8% men and 7.5% women). People living in the North of Italy had a higher level of education, compared to the rest of the country.
Among men, the prevalence of never smokers was highest among subjects with university degree (50.6%) and lowest in the least educated group (32.5%), whereas among women it was highest in the primary education group (79.0%) and lowest in the low secondary education category (60.0%). Among men, the proportion of subjects in the highest smoking category was similar and lowest in the two highest educational levels (13.1% for university degree and 12.9% for high school diploma), and highest in the lowest educational group (35.9%). Among women, the proportion of subjects in the highest smoking category increased steadily from university degree to primary school or less (from 2.3 to 3.2%). In both genders, people with primary school or less displayed the highest prevalence of physical inactivity, whereas intense and regular physical activity increased with increasing educational level. The prevalence of overweight people increased as educational level decreased in both men (from 34.7 to 48.8%) and women (from 15.7 to 41.0%). For obesity, there was a similar pattern in both men (from 4.8 to 16.3%) and women (from 3.3 to 20.9%).
Looking at the associations between natural mortality and exposure to risk factors (Table 2), in both Models 2 and 4 (analyses unadjusted and adjusted for health status, respectively), smoking was associated with a higher risk in both men and women, which increased according to the number of cigarettes smoked during lifetime. Regarding physical activity, sedentary men, as well as men performing light activity, displayed a significantly higher risk of natural mortality compared to those who practise intense physical activity. In women, only those who were sedentary showed a risk of mortality significantly increased, although lower than that observed among men. For BMI, we observed an opposite tendency between genders, with a protective association for overweight and obesity among men, and a higher risk associated with obesity in women, compared to normal-weight subjects.
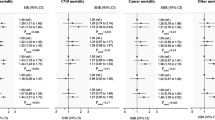
In all models (Table 3), the risk of death from natural causes was higher among subjects with primary school or less, compared to those with a university degree both among men (Model 1: RR = 1.62, 95% CI 1.34–1.96; Model 2: RR = 1.49, 95% CI 1.22–1.80; Model 3: RR = 1.42, 95% CI 1.17–1.72; Model 4: RR = 1.35, 95% CI 1.11–1.64) and women (Model 1: RR = 1.57, 95% CI 1.16–2.12; Model 2: RR = 1.53, 95% CI 1.14–2.07; Model 3: RR = 1.40, 95% CI 1.04–1.90; Model 4: RR = 1.42, 95% CI 1.05–1.92), with an inverse trend by educational level in all models (p < 0.05).
In all models, also men and women with low secondary school, or high school diploma displayed higher risks of mortality, compared to subjects with university degree.
For both genders, no interaction was found between education and smoking, BMI, or physical activity (all p > 0.05).
Examining the proportion of inequalities in mortality explained by risk factors, differences were found between men and women, as well as with or without considering health status at begin of the survey. Comparing results from Model 1 and Model 2 in men (Table 3), the fraction of inequalities in mortality between extreme educational categories explained by risk factors was 21.6% for primary school or less, 22.9% for lower secondary school and 6.6% for high school diploma (reference: university degree). Among women, the contribution of risk factors was 6.6% for primary school or less, 12.7% for low secondary school and 14.6% for high school diploma, compared to university degree (Table 3). In the analyses that take into account health status (Model 3 and Model 4), the explained fractions of BMF were slightly lower both in men and in women. In men, the contribution of the risk factors was 17.6% for primary school or less, 20.2% for low secondary school, and 3.9% for high school diploma (reference: university degree). Among women, it was 0% for primary school or less, 3.7% for low secondary school and 13.7% for high school diploma, compared with university degree (Table 3).
The explained fraction of inequalities in mortality from cancer between primary or less and university education was 15.8 and 12.2%, not adjusting and adjusting for health status, respectively, in men, while it was zero in women (Table 4).
Regarding cardiovascular mortality, in men the fraction of mortality explained by risk factors was 24.7% in the analysis not adjusted for health status and 21.8% in the adjusted one, whereas in women the corresponding figures were 20.2 and 14.0%, respectively (Table 5).
The results of the sensitivity analysis showed that among subjects without chronic diseases the fractions of inequalities in overall mortality explained by BMF were more consistent with those computed through the analyses adjusted for health at baseline, rather than with the unadjusted ones. In fact, among men the explained fraction of BMF between primary school or less and university degree was even lower than that obtained from the analysis adjusted for health (15.6%), whereas among women it was 0%, consistently with the results of this analysis (data not shown).
Discussion
The aim of this study was to measure the contribution of the main behavioural factors, including smoking habit, physical inactivity and metabolic factors, considering overweight, in explaining social inequalities in mortality. Among men, these three factors explained between 17.6 and 21.6% of the differences in overall mortality between extreme classes of education, while in women they explained between 0 and 6.6% of mortality inequalities. This lower value appears explained mainly by the higher proportion of smoking among women with high education, especially older women, due to a delay in the epidemic curve of tobacco consumption in Italy, whereas among men smoking exposure was more diffuse in low educated subjects. The risk attenuations produced by BMF after adjusting for health status at baseline were more similar to those obtained from the sensitivity analysis, where subjects reporting chronic disorders were excluded, compared to the analysis not adjusted for health, suggesting that health status was a confounder of the association rather than a mediator. In theory, health status can be a potential confounder or mediator, or both of the association between BMF and mortality. Regarding physical activity, health can be considered as a confounder of the association with mortality because chronic morbidity is expected to increase the likelihood of being sedentary, but also a mediator, as physical activity is known to lower the risk of chronic morbidity. Regarding smoking, the adjustment for health may represent an overadjustment, since health can be considered a mediator of the association between smoking and mortality, being on the causal pathway between exposure and mortality, even if health can also be a confounder of this association, as people with chronic morbidity would tend to reduce or quit smoking. Concerning obesity, health can be either a mediator of the association with mortality, for diseases like diabetes and hypertension, whose risk is increased by high BMI, or a confounder, as for disorders causing obesity directly (e.g., some endocrine pathologies), or for drugs that increase the risk of obesity (e.g., corticosteroids). Under the assumption that health status would be entirely a mediator of the association between BMF and mortality, the estimate unadjusted for health status would be more close to the true value, whereas the adjusted risk estimate would be more appropriate if health would act only as a confounder. Given that all the BMF considered may act as confounders or mediators of the BMF–mortality relationship, as discussed above, it seems likely that the true relative explanatory power of BMF is in between the two risk estimates.
For social differences in cancer mortality, BMF had an explained fraction slightly lower than that computed for overall mortality in men, and zero in women, whereas in both genders it was higher for cardiovascular mortality, which appears to reflect the stronger association of this with BMF.
In general, the fraction of mortality explained by BMF was lower in our study, compared to that computed in other studies. For example, a Finnish study estimated lifestyles to explain 45% of the difference in mortality among men and 38% among women between the lowest and the highest level of education, but the study considered a greater number of other factors, including vegetable consumption, fat consumption, and alcohol use (Laaksonen et al. 2008). A British study showed that smoking and BMI explained 33% among men and 25% among women of the social differences in mortality (McFadden et al. 2008). A Dutch study estimated an explained fraction of 53% for smoking, alcohol, physical activity and body mass index in a cohort including men and women together (Schrijvers et al. 1999). The higher contribution of these risk factors in these studies may be due to the fact that in our study overweight and obesity were protective factors for natural mortality among men, while among women those in the lowest educational category had the lowest prevalence of smoking.
For what concerns the relationship between individual behavioural factors and overall mortality, the results confirm associations reported by others studies for tobacco smoke (Strand and Tverdal 2004; van Oort et al. 2005; Woodward et al. 2003) and physical activity for both genders (Schrijvers et al. 1999; Woodward et al. 2003), demonstrating a good predictive validity of the self-reported information on these factors. The protective association observed in men with high BMI is debated in the literature, although recent studies have reported a similar effect (De Schutter et al. 2014; Veronese et al. 2015).
Although the relative explanatory power of BMF on the association between education and mortality was quite small, some authors have pointed out that nonetheless the absolute explanatory power may be much higher (Lynch et al. 2006; Khang et al. 2009). In fact, in contrast with the relative explanatory power, which is the attenuation in relative risk obtained from equalizing the prevalence of a risk factor across population strata, the absolute explanatory power describes the reduction of the difference in the incidence of an outcome between population strata when an exposure is eliminated from the population and, therefore, is a more useful indicator from a public health point of view. Absolute explanatory power depends mainly on the combination of absolute prevalence of BMF and the risk associated, which determine its population attributable proportion, rather than on differences in the prevalence of BMF across education categories, as for the relative explanatory power. The discrepancy between relative and absolute explanatory power will be stronger when differences in the prevalence of the risk factor between population strata are small, but the overall prevalence is high, because the elimination of the cases due to the exposure will impact differently on the relative risk and on the risk difference.
In spite of the low relative explanatory power of the risk factors considered, their absolute explanatory power is expected quite high in our study, because of their high prevalence and the high strength of association with mortality.
Strengths and limitations
The major strength of the study is the use of the Italian Longitudinal Study which allowed us to generalize our results to the Italian population. Another strong point is the possibility to adjust risk estimates for health status at baseline. The sensitivity analysis carried out on the cohort excluding subjects with chronic diseases confirmed the accuracy of the adjustment for health status performed in the main analysis.
A limitation of this study is the use of educational level as a single proxy for socioeconomic position, which may have not characterized appropriately the social strata in the cohort, possibly leading to an underestimation of the true social gradient compared to occupational social class (d’Errico et al. 2017), although educational level is an indicator used frequently in social epidemiology.
The inclusion in the cohort of older subjects may have caused an underestimation of the true differences in mortality between educational levels, as older subjects are a population of survivors and because subjects with low education tend to have higher mortality than those with high education. Also the lower proportion of subjects followed up among the low educated compared to the high educated likely produced an underestimate of the true social gradient in mortality. On the other hand, subjects with a higher prevalence of risk factors, more diffuse in lower educational strata, would also have an increased mortality risk and a reduced likelihood of surviving so long to be enrolled in the study. However, given the partial relative explanatory power of the BMF on educational differences in mortality, the selection effect linked to BMF exposure is expected to be smaller than that of overall mortality. Therefore, such a selection bias is expected to have lead to an overestimation of the relative explanatory power in this study.
Another limiting factor is the use of self-reported information on BMF, which can lead to a misclassification of the exposure to BMF (Patrick et al. 1994; Vartiainen et al. 2002) and, as a consequence, to an imperfect adjustment for these factors and to a flawed estimation of the explained fraction (Stringhini et al. 2011). In addition, except for smoking habit, for which the history of exposure relates to the entire life of subjects (use of pack-years), a misclassification of BMI and physical activity could have occurred, due to the absence of exposure information before baseline and during the follow-up period.
Among other limitations, the lack of information on social characteristics potentially correlated with behavioural and metabolic factors and mortality, such as negative life events, lack of social support, family conflicts, and financial difficulties, which are possible confounders of the association between BMF and mortality, could have lead to an overestimation of the strength of this association and of the proportion of mortality mediated by BMF. Furthermore, we could not consider in the analysis other behavioural factors, such as dietary habit and alcohol consumption, which could have led to an underestimation of the real explained fraction by these risk factors.
Conclusions
This study showed the presence of important differences in mortality from natural causes by educational level in both men and women. Adjustment for smoking habits, physical inactivity and BMI reduced the relative risk of mortality between extreme classes of education by < 20% in men, while it has had no effect in women. The results of the sensitivity analysis on healthy subjects suggest that the risk attenuation produced by adjustment for behavioural or metabolic factors should be evaluated comparing models adjusted also for health status. Substantial differences in mortality remained between extreme educational classes after controlling for health status and behavioural or metabolic factors, possibly related to other behavioural factors, such as dietary habit and alcohol consumption, which was not possible to consider in this study, for their key role in the development of several chronic diseases, or to environmental hazards. However, it seems difficult to exclude that the persistence of a gradient in mortality would be actually attributable to a direct effect of low education, or, more generally, of the disadvantaged material and psychosocial conditions associated with low education.
References
Apolone G, Mosconi P, Ware L (2001) Questionario sullo stato di salute SF-12. Guerini E Associati (in Italian)
Braveman P, Egerter S, Barclay C, Princeton NJ (2011) What shapes health-related behaviors? The role of social factors. Exploring the social determinants of health. Robert Wood Johnson Foundation: issue brief no. 1. http://www.nmpha.org/Resources/Documents/RWJF%20Issue%20Brief%2020The%20Role%20of%20Social%20Factors.pdf
Cardano M, Marinacci C (2006) Measuring social position. Epidemiol Prev 3:124–142 (in Italian)
d’Errico A, Ricceri F, Stringhini S, Carmeli C, Kivimaki M, Bartley M, McCrory C, Bochud M, Vollenweider P, Tumino R, Goldberg M, Zins M, Barros H, Giles G, Severi G, Costa G, Vineis P, LIFEPATH Consortium (2017) Socioeconomic indicators in epidemiologic research: a practical example from the LIFEPATH study. PLoS ONE 12(5):e0178071
De Schutter A, Lavie CJ, Kachur S, Patel DA, Milani RV (2014) Body composition and mortality in a large cohort with preserved ejection fraction: untangling the obesity paradox. Mayo Clin Proc 89(8):1072–1079
Eikemo TA, Hoffmann R, Kulik MC, Kulhánová I, Toch-Marquardt M, Menvielle G, Looman C, Jasilionis D, Martikainen P, Lundberg O, Mackenbach JP (2014) How can inequalities in mortality be reduced? A quantitative analysis of 6 risk factors in 21 European populations. EURO-GBD-SE Consortium. PLoS ONE 9(11):e110952
Federico B, Mackenbach JP, Eikemo TA, Sebastiani G, Marinacci C, Costa G, Kunst AE (2013) Educational inequalities in mortality in northern, mid and southern Italy and the contribution of smoking. J Epidemiol Community Health 67:603–609
Harald K, Pajunen P, Jousilahti P, Koskinen S, Vartiainen E, Salomaa V (2006) Modifiable risk factors have an impact on socio-economic differences in coronary heart disease events. Scand Cardiovasc J 40:87–95
Inequalities in health—National Report 2007–2009. Survey PASSI. Istituto Superiore di Sanità. http://www.epicentro.iss.it/passi/pdf2012/PASSI%20Disuguaglianze%20sociali%20e%20salute.pdf (in Italian)
Khang YH, Lynch JW, Yang S, Harper S, Yun SC, Jung-Choi K, Kim HR (2009) The contribution of material, psychosocial, and behavioral factors in explaining educational and occupational mortality inequalities in a nationally representative sample of South Koreans: relative and absolute perspectives. Soc Sci Med 68(5):858–866
Kunst AE, Groenhof F, Mackenbach JP (1998) Mortality by occupational class among men 30–64 years in 11 European countries. EU Working Group on Socioeconomic Inequalities in Health. Soc Sci Med 46:1459–1476
Laaksonen M, Talala K, Martelin T, Rahkonen O, Roos E, Helakorpi S, Laatikainen T, Prättälä R (2008) Health behaviours as explanations for educational level differences in cardiovascular and all-cause mortality: a follow-up of 60,000 men and women over 23 years. Eur J Pub Health 18(1):38–43
Lantz PM, House JS, Lepkowski JM, Williams DR, Mero RP, Chen J (1998) Socioeconomic factors, health behaviors, and mortality: results from a nationally representative prospective study of US adults. JAMA 279:1703–1708
Lynch J, Davey Smith G, Harper S, Bainbridge K (2006) Explaining the social gradient in coronary heart disease: comparing relative and absolute risk approaches. J Epidemiol Community Health 60(5):436–441
Mackenbach JP, Kunst AE, Cavelaars AE, Groenhof F, Geurts JJ (1997) Socioeconomic inequalities in morbidity and mortality in Western Europe. The EU Working Group on Socioeconomic Inequalities in Health. Lancet 349:1655–1659
Mackenbach JP, Stirbu I, Roskam AJ, Schaap MM, Menvielle G, Leinsalu M, Kunst AE (2008) Socioeconomic inequalities in health in 22 European countries. N Engl J Med 358:2468–2481
Marinacci C, Grippo F, Pappagallo M, Sebastiani G, Demaria M, Vittori P, Caranci N, Costa G (2013) Social inequalities in total and cause-specific mortality of a sample of the Italian population, from 1999 to 2007. Eur J Public Health 23(4):582–587
McFadden E, Luben R, Wareham N, Bingham S, Khaw KT (2008) Occupational social class, educational level, smoking and body mass index, and cause-specific mortality in men and women: a prospective study in the European Prospective Investigation of Cancer and Nutrition in Norfolk (EPIC-Norfolk) cohort. Eur J Epidemiol 23(8):511–522
Nandi A, Glymour MM, Subramanian SV (2014) Association among socioeconomic status, health behaviors, and all-cause mortality in the United States. Epidemiology 25(2):170–177
Nordahl H, Lange T, Osler M, Diderichsen F, Andersen I, Prescott E, Tjønneland A, Frederiksen BL, Rod NH (2014) Education and cause-specific mortality: the mediating role of differential exposures and vulnerability of behavioral risk factors. Epidemiology 25:389–396
Patrick DL, Cheadle A, Thompson DC, Diehr P, Koepsell T, Kinne S (1994) The validity of self-reported smoking: a review and meta-analysis. Am J Public Health 84:1086–1093
Piccinelli C, Pagano E, Segnan N (2015) Reducing non-communicable diseases and health care costs: building a prevention alliance. Epidemiol Prev 39(2):202–207 (in Italian)
Salmaso S, Baldissera S, D’Argenio P, Ferrante G, Maggini M, Minardi V, Possenti V, Quarchioni E, Alegiani S (2011) Inequalities in health – National Report 2007–2009. Survey PASSI. Istituto Superiore di Sanità. http://www.epicentro.iss.it/passi/pdf2012/PASSI%20Disuguaglianze%20sociali%20e%20salute.pdf (in italian)
Schrijvers CT, Stronks K, van de Mheen HD, Mackenbach JP (1999) Explaining educational differences in mortality: the role of behavioral and material factors. Am J Public Health 89(4):535–540
Skalická V, van Lenthe F, Bambra C, Krokstad S, Mackenbach J (2009) Material, psychosocial, behavioural and biomedical factors in the explanation of relative socio-economic inequalities in mortality: evidence from the HUNT study. Int J Epidemiol 38(5):1272–1284
Strand BH, Tverdal A (2004) Can cardiovascular risk factors and lifestyle explain the educational inequalities in mortality from ischaemic heart disease and from other heart diseases? 26 year follow up of 50 000 Norwegian men and women. J Epidemiol Community Health 58:705–709
Stringhini S, Sabia S, Shipley M, Brunner E, Nabi H, Kivimaki M, Singh-Manoux A (2010) Association of socioeconomic position with health behaviors and mortality. JAMA 303(12):1159–1166
Stringhini S, Dugravot A, Shipley M, Goldberg M, Zins M, Kivimäki M, Marmot M, Sabia S, Singh-Manoux A (2011) Health behaviours, socioeconomic status, and mortality: further analyses of the British Whitehall II and the French GAZEL prospective cohorts. PLoS Med 8(2):e1000419
van Oort FV, van Lenthe FJ, Mackenbach JP (2005) Material, psychosocial, and behavioural factors in the explanation of educational inequalities in mortality in The Netherlands. J Epidemiol Community Health 59:214–220
Vartiainen E, Seppala T, Lillsunde P, Puska P (2002) Validation of self reported smoking by serum cotinine measurement in a community-based study. J Epidemiol Community Health 56:167–170
Veronese N, Cereda E, Solmi M, Fowler SA, Manzato E, Maggi S, Manu P, Abe E, Hayashi K, Allard JP, Arendt BM, Beck A, Chan M, Audrey YJ, Lin WY, Hsu HS, Lin CC, Diekmann R, Kimyagarov S, Miller M, Cameron ID, Pitkälä KH, Lee J, Woo J, Nakamura K, Smiley D, Umpierrez G, Rondanelli M, Sund-Levander M, Valentini L, Schindler K, Törmä J, Volpato S, Zuliani G, Wong M, Lok K, Kane JM, Sergi G, Correll CU (2015) Inverse relationship between body mass index and mortality in older nursing home residents: a meta-analysis of 19,538 elderly subjects. Obes Rev 16(11):1001–1015
WHO (2008) 2008–2013 action plan for global strategy for the prevention and control of non-communicable diseases. World Health Organization, Geneva. http://www.who.int/nmh/publications/ncd_action_plan_en.pdf
Woodward M, Oliphant J, Lowe G, Tunstall-Pedoe H (2003) Contribution of contemporaneous risk factors to social inequality in coronary heart disease and all causes mortality. Prev Med 36:561–568
Zou G (2004) A modified Poisson regression approach to prospective studies with binary data. Am J Epidemiol 159:702–706
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animals rights
This article does not contain any study with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Piccinelli, C., Carnà, P., Stringhini, S. et al. The contribution of behavioural and metabolic risk factors to socioeconomic inequalities in mortality: the Italian Longitudinal Study. Int J Public Health 63, 325–335 (2018). https://doi.org/10.1007/s00038-018-1076-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-018-1076-8