
Abstract
Introduction
Prostate cancer is the most common non-cutaneous malignancy diagnosed in men. Moving from histological observations since a long time, it has been recognized that innate and adaptive immunity actively participates in the pathogenesis, surveillance, and progression of prostate cancer.
Materials and methods
A PubMed and Web of Science databases search was performed for studies providing evidence on the roles of the innate and adaptive immunity during the development and progression of prostate cancer.
Conclusions
There are growing evidences that chronic inflammation is involved in the regulation of cellular events in prostate carcinogenesis, including disruption of the immune response and regulation of the tumor microenvironment. This review discusses the role played by the innate and adaptive immune system in the local progression of prostate cancer, and the prognostic information that we can currently understand and exploit.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most common non-cutaneous malignancy diagnosed in men [1] and represents the first most frequently diagnosed cancer and the second most common causes of cancer death worldwide in men [2].
Although many prognostic factors have been proposed, no reliable index for predicting the outcome of prostate cancer patients has yet been identified. Currently, the quantification of serum levels of prostate-specific antigen (PSA), a glycoprotein with serine protease activity secreted by the epithelial cells of the prostate gland, remains the most important tumoral marker. However it has important drawbacks. PSA is often elevated in non-neoplastic conditions, including benign prostatic hyperplasia, prostatitis, or prostate infarction [3, 4]. This has considerable clinical consequences, since this assessment forms the basis for primary clinical decisions [4]. It has been reported that PSA screening reduced the rate of death from prostate cancer by 20 % but was also associated with a high risk of overdiagnosis [5]. Transrectal ultrasound-guided prostate biopsy remains the gold standard for detecting prostate cancer [6]. Prostate biopsy has evolved from a paradigm of a small number of random biopsies to one of systematic, numerical, and anatomical strategy [7, 8]. However, the efficiency of this procedure is still debated and is limited in practice by patient tolerance and morbidity. Currently, clinical and pathological classifications are determined according to the World Health Organization (WHO) criteria, the Gleason grade, and the Tumor-Node-Metastasis (TNM) staging system [9, 10]. The Gleason biopsy grade is used in conjunction with other clinical and molecular variables, including serum PSA levels and clinical stage, to help make treatment decisions for prostate cancer and they are all incorporated into various “nomograms” to determine pre-operatively the risk of progression after specific therapy [11, 12]. Although several tools with potential clinical value have been proposed [13–15], there is still no reliable index for predicting the outcome of prostate cancer patients. While prostate cancer is one of the most common causes of cancer-related deaths among males worldwide, the majority of patients diagnosed with the disease have a relatively indolent form of prostate cancer that is unlikely to invade beyond the local tissue environment [16]. However, a subset of prostate tumors exhibit aggressive properties, including rapid proliferation and metastatic spread to distant organ sites, including the lymph nodes, lung, bone, and brain. It is indubitable that in the management of prostate cancer the major challenge remains to distinguish patients who need definite treatment from patients who have latent disease.
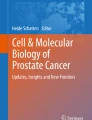
Decades of histological observations have led to the recognition of inflammatory and immune mediators as active participants in the pathogenesis, surveillance, and progression of prostate cancer [17–21] (Fig. 1). The advents of immunohistochemical techniques and experimental models have improved our understanding of the dynamics regulating the immune system in prostate cancer [22–24]. Gurel et al. [25] addressed this issue in a case–control study. Prostate samples were histologically examined for inflammation using the United States National Institutes of Health consensus grading system. They found that 86 % of the men who developed prostate cancer had signs of inflammation in ≥1 biopsy core, and 78 % of men without cancer had signs of inflammation in benign areas. Men with inflammation on ≥1 biopsy core were 1.78 times more likely to develop prostate cancer than those who had no histological evidence of inflammation [Odds Ratio (OR) 1.78, 95 % CI 1.04–3.06]. This association was more pronounced for high-grade disease (OR 2.24, 95 % CI 1.06–4.71) than for low-grade disease (OR 1.57, 95 % CI 0.83–3.00) [25].

Moving from histological observations, it has been recognized that inflammation and immunity actively participate in the pathogenesis, surveillance and progression of prostate cancer. CD3+ T-lymphocytes (a), CD20+ B-lymphocytes (b), and macrophages (c) represent the main immune cell components infiltrating prostate cancer (objective magnification 20×)
It is well known that complex interactions regulate immune cells in the tumor microenvironment [26–29]. Immune system cells infiltrating prostate cancer include cells associated with innate immune response i.e., macrophages [30, 31], neutrophils [32], mast cells (MCs) [33–35], and natural killer (NK) cells [36], as well as cells associated with an adaptive immune response i.e., T- and B-lymphocytes [37–41]. The histologic signature of chronic inflammation is now a common finding in benign as well as malignant prostate tissue [42]. An increase in luminal cell proliferation associated with inflammation likely enhances the susceptibility of epithelium to transform [28] (Fig. 2). The inflammatory infiltrate are mainly represented by CD3+ T-lymphocytes (70–80 %, mostly CD4+), CD20+ B-lymphocytes (10–15 %), and macrophages (15 %) (Fig. 1) [43]. Although it is thought that an immune response localized to the tumor inhibit cancer growth, it is now clear that some types of tumor-associated immune cells may also exert an opposite action, at least at some point of prostate cancer natural history [44]. A number of studies have suggested that inflammation may be important in the pathogenesis of prostate cancer by altering the tumor environment [19, 45, 46]. This review discusses the role played by innate and adaptive immune system in the local progression of prostate cancer, and the prognostic information that we can currently understand and exploit.

The histologic signature of chronic inflammation is now a common finding in benign as well malignant prostate tissue. Evidence supports the concept that tumor stromal cells are not merely a scaffold, but rather they influence growth, survival, and invasiveness of cancer cells, dynamically contributing to the tumor microenvironment. An increase in luminal cell proliferation associated with inflammation likely enhances the susceptibility of epithelium to transformation
The innate immunity
It is well known that “innate immunity” represents the body’s first defense to an abnormal situation, such as cancer, and does not involve specific recognition of immunogenic peptides, or antigens. Innate immune cells orchestrate an inflammatory environment that may function to either stimulate or inhibit cancer growth.
Various innate immune cells have been implicated in prostate cancer development and progression. Among these, macrophages are a primary source of secreted proinflammatory cytokines, and are generally distinguished in two different phenotypes: M1, with tumor inhibitor properties [production of inflammatory cytokines, reactive oxygen species (ROS), and activated immune response] and M2, with tumor-stimulatory properties (promote tissue repair and angiogenesis) [47–50]. Recently, Lanciotti et al. [50] observed that a high density of macrophages in prostate cancer was associated with poorer prognosis. Moreover they found higher prevalence of M2 macrophage phenotype, which resulted and more represented in prostate cancer Gleason score 7 to 8–10 and pT3a stage.
It is now recognized that proliferative inflammatory atrophy (PIA) lesions are associated with chronic inflammation of the prostate, and histological transitions have been noted between areas of PIA and high-grade prostate intraepithelial neoplasia (HGPIN), and between PIA and prostate cancer [30, 51]. A primary feature of the PIA lesions is the presence of mononuclear cells and/or polymorphonuclear cells in both epithelial and stromal compartments [30].
Fang et al. [31] reported that persistent co-culturing of immortalized prostate epithelial cells with macrophages, without adding any carcinogens, induces prostate tumorigenesis. This induction involves the alteration of signaling of macrophage androgen receptor (AR)-inflammatory chemokine CCL4-STAT3 activation, epithelial-to-mesenchymal transition (EMT), and down-regulation of p53/PTEN tumor suppressors [31]. Comito et al. [52] demonstrated that prostate cancer-associated fibroblasts (CAFs) are active factors of monocyte recruitment toward tumor cells, mainly acting through stromal-derived growth factor-1 (SDF-1, a small cytokine that belongs to the chemokine family) delivery and promote their transdifferentiation toward the M2 macrophage phenotype. The relationship between M2 macrophages and CAFs is reciprocal. M2-polarized macrophages are able to affect the transdifferentiation of fibroblasts to myofibroblasts, leading to their enhanced reactivity [52]. On the other side, prostate cancer cells themselves participate in this cross talk through the secretion of monocyte chemotactic protein-1 (MCP-1), facilitating monocyte recruitment, macrophage differentiation, and M2 polarization [52]. This cell complex cooperates in increasing tumor cell motility, ultimately fostering cancer cells to escape from primary tumor and metastatic spread, as well as in the activation of endothelial cells, and their bone marrow-derived precursors to drive the neoangiogenesis [52]. It has also been ascertained that the macrophage colony-stimulating factor 1 (CSF-1)/macrophage colony-stimulating factor receptor (CSF1R) signaling in tumor-infiltrating myeloid cells, including CD11b (ITGAM)+(F4/80 (EMR1)+ tumor-associated macrophages and CD11b+Gr-1 (LY6G)+ myeloid-derived suppressor cells can limit the efficacy of radiotherapy [53]. Fujii et al. [54] assessed the number of infiltrating macrophages and a series of adaptive immune cell populations, including CD3+ T-lymphocytes, CD20+ B-lymphocytes, in benign and malignant prostate tumors. They found that macrophages infiltrated benign glands to a higher extent than those of prostate cancer. The authors concluded that inflammation of the prostate may be pivotal on prostate carcinomas, particularly that involving M2-polarized macrophage infiltration [54]. Macrophage inhibitory cytokine-1 (MIC-1), also known as prostate-derived factor (PDF), a molecule of the transforming growth factor-beta (TGF-β) superfamily, has been associated with the progression of various types of cancers, including prostate cancer and found down-regulated in benign prostate hyperplasia [55]. Dubey et al. [56] analyzed MIC-1 expression in mouse prostate tissues to determine whether there was any correlation with age and inflammation. Their study first shows that the MIC-1 gene may be directly regulated by inflammation-associated cytokines in prostate cancer cells. The activation of the MIC-1 gene may be an early response due to inflammation, infection, or injury in the prostate for cell growth advantage leading to an environment favoring prostate cancer development. It is known that deregulation of expression and function of cytokines belonging to the TGF-β family is often associated with various pathologies [57]. One of these molecules is growth differentiation factor-15 (GDF-15). This stress-induced cytokine has been proposed to possess immunomodulatory functions and its high expression is often associated with prostate cancer progression [58]. Vaňhara et al. [58] recently discussed several studies that focused on the regulation of GDF-15 expression and its role in tissue homeostasis, repair, and the immune response with an emphasis on the role in prostate cancer development.
Other than macrophages, MCs have been suggested to support the outgrowth of certain cancers because of their proangiogenic properties. Pittoni and Colombo [33] have, recently discussed the role of MCs in mouse and human prostate cancer, showing that MCs can behave alternatively as “dangerous promoters, innocent bystanders, or essential guardians of tumors”, according to the stage and origin of transformed cells. In particular, MCs are essential for the outgrowth of early-stage tumors due to their matrix metalloproteinase 9 (MMP-9) production, become dispensable in advanced-stage, post-EMT, and are protective against neuroendocrine prostate tumor variants [33]. NK cells are innate lymphocytes that respond rapidly and non-specifically to viral infection and other pathogens. They are also known to form a unique link between innate and adaptive immunity [59]. NK cells not only exert cytotoxic activity against tumor cells or infected cells but also act to regulate the function of other immune cells through secretion of various cytokines and chemokines or cell contact-dependent mechanisms. Yuan et al. [60] have shown that at the early stage of tumor invasion, NK and MCs are the main types of tumor-infiltrating immune cells involved in focal degenerative products in the tumor capsules. The primary impact of these immune cells is that they are associated with focal disruptions of the tumor capsule, which selectively favor tumor stem cell proliferation and invasion.
Neutrophils are a key mediator of the innate immune system and are pivotal in the inflammatory response to infection or tissue damage [61]. Interestingly, an elevated neutrophil count may be a good indicator of a benign prostate biopsy. Men with a low neutrophil count and an increase of serum PSA level should strongly be considered for biopsy [62]. Conversely, Bekes et al. [63] have demonstrated that the primary tumors formed by highly disseminating variants of human prostate carcinoma recruit elevated levels of infiltrating MMP-9 secreting neutrophils and concomitantly exhibit enhanced levels of angiogenesis and intravasation. Specific inhibition of neutrophil influx by interleukin 8 (IL-8) resulted in the coordinated diminishment of tumor angiogenesis and intravasation. Thus, treatment of prostate cancers associated with neutrophil infiltration may benefit from specific targeting of neutrophil MMP-9 at early stages to prevent ensuing tumor angiogenesis and tumor metastasis. Furthermore, in metastatic castration-resistant prostate cancer patients treated with ketoconazole, the neutrophil-to-lymphocyte ratio, and PSA doubling time before treatment and prior response to androgen deprivation therapy may be associated with the progression-free survival time and used to form a risk stratification predictive nomogram [64].
The adaptive immunity
Adaptive immune cells are commonly associated with malignant neoplasms [65]. Analysis of two major prostate tumor-infiltrating lymphocyte subsets showed that capsular and perineural invasion as well as biochemical progression was related to strong infiltration of T- and B-lymphocytes. McArdle et al. [66] have shown that the presence of an increase in CD4+ T-lymphocyte infiltrate was associated with poor cancer-specific survival in patients with prostate cancer. Furthermore, when the analysis was confined to those patients with localized or locally advanced disease, only CD4+ T-lymphocyte count predicted survival [66].
Ammirante et al. [24] found that prostate cancer progression is associated with inflammatory infiltration and activation of the inflammation-responsive IkappaB kinase (IKK)-alpha, which stimulates metastasis by an NF-kappaB-independent, cell autonomous mechanism. They have shown that androgen ablation causes infiltration of regressing androgen-dependent tumors by leukocytes, including B-lymphocytes, in which IKK-beta activation results in the production of cytokines that activate IKK-alpha and STAT3 in prostate cancer cells, to enhance hormone-free survival. Recently, Liu et al. [41] investigated the distribution of CD1a+ dendritic cells, CD8+ and CD4+ T-lymphocytes in prostate cancer and correlated these with clinical indexes and pathological features. The number of CD1a+ cells correlated significantly with the number of intratumoral and stromal CD8+ and stromal CD4+ lymphocytes [41]. Survival analysis showed a tendency toward impaired progression-free survival in patients who underwent radical prostatectomy, with few CD1a+ cells. The expression of B7-H3 (i.e., one of the most recently identified members of the B7/CD28 superfamily of co-stimulatory molecules serving as an accessory modulator of T cell response) correlated inversely with the number of CD1a+ cells and intratumoral CD4+ lymphocytes. Additionally, a trend to a similar inverse relationship between B7-H3 expression and the number of CD8+ lymphocytes was found. B7-H3 is known to be aberrantly expressed in prostate cancer, and is able to have a role in regulating PC-3 cell progression in vitro [67].
Si et al. [68] assessed the response of regulatory T-lymphocytes following cryosurgery in prostate cancer patients by measuring their frequency and immune function. It has been shown that CD4+CD25+FoxP3+ regulatory T-lymphocytes play an important role in immune homeostasis because of their ability to suppress the activation of T-cells, and an increase in the number or functionality of regulatory T-lymphocytes could thus favor tumor development. Increased levels of CD4+CD25+FoxP3+ regulatory T-lymphocytes have been detected in patients with primary prostate cancer [69, 70]. Although pathologic examination of prostate glands removed from patients with prostate cancer commonly reveals infiltrating CD4+ and CD8+ T-lymphocytes, little is known about the phenotype of these cells, despite evidence suggesting a potential role for chronic inflammation in the etiology of prostate cancer. Sfanos et al. [71] suggested that Th17 and/or regulatory T-lymphocytes CD4+ T-lymphocytes might be involved in the development or progression of prostate cancer. Regulatory T-lymphocytes have been shown to express a variety of chemokine receptors, including CCR4, CCR7, CCR8, CXCR4, and CXCR5, depending on their activation status and tissue location [72]. Miller et al. [69] demonstrated that some prostate cancer cell lines, malignant ascites fluid, and prostate tumor biopsies in culture contain or secrete CCL22 (the CCR4 ligand) and chemoattract regulatory T-lymphocytes in an in vitro migration assay.
Although conflicting results have been highlighted when investigating the relationship between infiltration of lymphocytes and survival in prostate cancer, Davidsson et al. [73] performed a case–control study nested in a cohort of men treated with transurethral resection of the prostate and diagnosed incidentally with prostate cancer. Although infiltration of both CD4+ and CD8+ T-lymphocytes was frequently observed, the majority of the regulatory T-lymphocytes were CD4+. CD4+ or CD8+ T-lymphocytes were not associated with lethal prostate cancer. However, they found a nearly two-fold increased risk of lethal prostate cancer when comparing the highest with the lowest quartile of CD4+ regulatory T-lymphocytes. They concluded that men with greater numbers of CD4+ regulatory T-lymphocytes in their prostate tumor environment have an increased risk of dying of prostate cancer, and that the identification of CD4+ regulatory T-lymphocytes in tumor tissue may predict clinically relevant disease at the time of diagnosis independent of other clinical factors. In prostate cancer, increased expression of IL-17 at the mRNA level was shown in tissue from both prostate cancer and benign prostatic hyperplasia before it was known that Th17 T-lymphocytes represent a distinct CD4 effector T-cell lineage [38].
Although, the role of B-lymphocytes in cancer has been overshadowed by the interest in developing T-cell-mediated cellular responses, it is now apparent that B-lymphocytes can play a complementary role in the host response against tumor. Flammiger et al. [39] explored the impact of the density of T- and B-lymphocytes in prostate cancer tissue on PSA recurrence after radical prostatectomy in 3261 prostate cancer tissue samples. Patients with very low and very high numbers of CD3+ T-lymphocytes had a significantly shorter PSA recurrence-free survival compared to patients with intermediate numbers of T-lymphocytes. In contrast, the number of CD20+ B-lymphocytes was not associated with other clinical and histopathological parameters, suggesting that the density of T- but not B-lymphocytes plays a functional role in the biology of prostate cancer and may have an impact on clinical outcome in this neoplasia. As the status of pelvic lymph nodes primarily served as a prognostic marker for prostate cancer and are used to guide further treatments after surgery, Gannon et al. [74] investigated the immunological effects of prostate cancer by comparing metastatic and non-metastatic pelvic lymph nodes from 25 patients with carcinomatous involvement of lymph nodes and 26 control patients with no metastatic involvement by immunohistochemistry and histological analyses. They found a decreased abundance of CD20+ B-lymphocytes and CD38+ activated lymphocytes in metastatic lymph nodes comparatively to control lymph nodes, suggesting the development of an immunosuppressive microenvironment.
Chemokines and prostate cancer
Prostate cancer cells have been found to express survival, differentiation, chemotactic, and growth factors for their growth in ectopic organs, such as bone marrow [75]. One aspect that has not been exploited comprehensively until now is the contribution of autocrine and paracrine factors that affect prostate cancer growth, survival in a hostile environment, avoidance of immune surveillance, and adoption of alternate survival mechanisms upon chemotherapy stress. Tumor cell themselves are major producer of chemokines, and the significance of chemokine release at the tumor site has been the object of intense investigation in the recent past [76]. Moreover, recent data highlight an unexpected association between local chronic inflammation and tumorigenesis, suggesting that also host-derived chemokines could be of significant relevance [77].
Among the factors suspected to control prostate cancer, incidence and progression in terms of tumor cell survival, growth, angiogenesis and metastasis, chemokines, and their receptors, now intensively studied, have become a field of increasing interest and exploration [78]. It is important to notice that chemokine receptors are expressed and chemokines are produced by a variety of cells in prostate tumors, comprising not only cancer cells but also stromal cells (i.e., cancer-associated fibroblasts), endothelial cells, or infiltrating cells (i.e., macrophages, lymphocytes, NK cells, mast cells).
Tumors are not exclusively composed of neoplastic cells, but also include a significant number of host-derived cells, which in various ways affect tumor biology. Induction of a robust angiogenesis is of mayor relevance for tumor biology, not only for nutrients but also to provide new dissemination routes to malignant cells, and a similar role has been recently recognized to intratumor lymphatic vessels. Moreover, most tumors also present a significant number of infiltrating leukocytes [79]. In the resulting complex interplay between malignant and host-derived cells, a major role is played by chemokines, a family of chemotactic cytokines deputed to sense a chemical gradient and to mobilize cells in the gradient direction by activating specific receptors expressed on the cellular membrane [80]. Initially described as molecules regulating leukocyte recruitment at sites of inflammation, chemokines, and inflammatory CC chemokines in particular, have been shown more recently to also support the recruitment of tumor-infiltrating leukocytes, such as TAMs [81, 82]. Besides immune cells, chemokine receptors have been demonstrated also on tumor cells [83], and convincing evidence has been recently provided that chemokines and their cell surface receptors are involved in the metastasization of several human tumors [84, 85].
Finally, it is well established that chemokines also exert other biological functions not related to their chemotactic properties of potential relevance for tumor biology, including cell proliferation and survival from apoptotic stimuli, and regulation of angiogenesis [76, 86]. Thus, by supporting biological processes such as immune evasion, tumor growth, and tumor dissemination, chemokines may favor tumor biology in several ways, either by shaping the functional profile of infiltrating leukocytes or by activating stromal and neoplastic cells.
The most evidence of chemokine receptors endogenously expressed by cancer cells is provided for CXCR1, CXCR2, CXCR4, and CXCR7 but also other receptors such as CCR1, CCR2, CCR3, CCR5, CCR7, CCR9, CXCR3, CXCR6, CXCR5, CX3CR1 are involved in the multistep process of prostate cancer progression and metastasis [78, 87–92]. Mainly, the work on chemokines in prostate cancer has focused on not only the chemokines CXCL8, CXCL12, and CCL2 but also other chemokines such as CCL2, CCL4, CCL5, CCL9, CCL11, CCL18, CXCL1, CXCL2, CXCL5, CXCL6, CXCL12, and CXCL13 that appear to be produced by stromal cells, endothelial cells and human bone marrow endothelial cells, differentiated osteoblasts, and infiltrating leukocytes [78, 93–99]. Chemokine receptors can activate downstream effectors by complex mechanisms of chemokine-dependent activation of cryptic growth factors including survival kinases, or transactivate other receptors such as EGFR or ErbB family members [100, 101]. Changes of chemokine receptor cohorts may be necessary to activate tumor-promoting signals. During the transitions from normal to benign prostatic hyperplasia, from benign prostatic hyperplasia to prostate cancer, and subsequently through each steps of tumor progression and metastasization, a number of chemokines and chemokine receptors display variations in their expression. As an example, the more aggressive types of prostate cancer cell lines express higher levels of CCR2 compared with less aggressive cells and both CCR2 mRNA and protein levels increase in metastatic prostate cancers compared with localized ones [101]. So far, the signals and the mechanism of regulating the chemokine system in prostate cancer remain poorly studied and recently, most studies have analyzed the effects of nuclear receptors such as androgen [102, 103] and vitamin D3 receptors [104].
Current diagnosis for prostate cancer includes digital rectal examination, serum PSA levels, and biopsy [105]. PSA is a glycoprotein enzyme secreted by epithelial cells of the prostate gland [106]. It has been used as a biomarker for prostate cancer screening, and the results of PSA test often decide whether patients should undergo a prostate biopsy for prostate cancer detection. However, PSA is not reliable in diagnosing prostate cancer, since serum levels of PSA in patients with other prostatic diseases, such as benign hyperplasia, may also increase, producing high rates of false positive results and leading to overdetection of prostate cancer. Thus, several efforts have been focused on the identification of novel, more suitable, precise diagnostic biomarkers for prostate cancer [107]. Since chemokines are associated with more aggressive disease and poor prognosis in diverse malignancies, and significant modifications of chemokines repertoire occurred during tumorigenesis of prostate cancer, chemokine system may represent a promising diagnostic biomarker that may guide strategies to improve prostate cancer therapy. Recently, pilot studies have been driven to investigate the diagnostic relevance of chemokines in prostate cancer and CCL2, CCL18, CCL11, and CXCL8 have been found to be new potential serum biomarkers [108–112]. For example, the elevated serum levels of both CCL11 and CCL18 in prostate cancer patients than those in benign hyperplasia patients may provide a useful diagnostic tool to help distinguish between the two pathological conditions among men demonstrating low, but detectable, serum PSA values [109, 110]. Furthermore, increased serum levels of CXCL8 and CCL2 are associated with higher-grade tumors and correlate with poorer prostate cancer outcomes [108, 111].
Since chemokines and their receptors act as mediators of migration of immune cells to the site of inflammation and deregulated inflammatory response is associated with increased risk of cancer, the chemokines system could also contribute to the variable incidence of prostate cancer in the world and could be considered as an important risk factor for this malignancy [113]. Indeed, the incidence and mortality rates of prostate cancer are significantly higher in African-American men when compared with European-American men. A comparative microarray analysis of chemokine expression profiles of patients with primary prostate tumors showed that CCL5, CCR7, and CXCR4 were expressed at higher levels in African-American patients compared with European-American patients [114]. Interestingly, polymorphism of some chemokine genes is altered in prostate cancer, which could potentially correlate with the different expression levels of chemokines. For example, in a Turkish men population, a single nucleotide polymorphism of CXCL12 G801A has been reported and patients with the AA genotype presented a higher risk for developing an advanced disease status as compared to patients with GG homozygotes. In addition, the distribution of AA genotype was found significantly increased in the patients with bone metastases in comparison with those without bone metastases [115]. Furthermore, a case–control study revealed that CCL2 I/D gene variant contribute to the susceptibility and clinic-pathological characteristic of prostate cancer in North Indian men [116].
Due to the bench findings that chemokine system is directly involved in prostate cancer, chemokine targeting has been tested as a therapeutic option. Interestingly, targeting CCL2 has been demonstrated as effective therapeutic approach in preclinical prostate cancer models [117] and currently, neutralizing monoclonal antibody against CCL2 (CNTO888) has entered into phase I trials for safety and phase II clinical trials in prostate cancer to test efficacy [118, 119]. In the recent years, many efforts have been also addressed to the design, synthesis, and characterization of potential lead compounds for future CCR5 antagonist development that have been demonstrated to inhibit the proliferation of metastatic prostate cancer cell lines at a micromolar level [120, 121]. Furthermore, in the therapeutic setting of prostate cancer, the close relationship between chemotherapeutic drugs and chemokine receptors is noteworthy. In fact, it has been clearly demonstrated that chemokine receptors signaling counteracts chemotherapeutic drugs’ effect, suggesting that targeting of this signaling axis or its downstream effector pathway could sensitize prostate cancer to chemotherapy [122, 123]. Moreover, drugs acting as chemokine receptor antagonist show therapeutic enhancement due to improved chemo-preventive activities [124].
In conclusion, control of chemokines and inhibition of their receptor activation may add critical tools to reduce tumor growth, especially in chemo-hormonal refractory prostate cancer that is both currently incurable and the most aggressive form of the disease, accounting for most of the more than 28,000 annual deaths. In the near future, therapeutic approaches targeting chemokine system will be combined with the classical therapeutic approaches such as chemotherapy or other immune modulators and should provide new successfully therapeutic strategies for prostate and other cancers.
Conclusions
Prostate cancer is a dynamic and highly heterogeneous disease encompassing a wide variety of pathological entities and a range of different clinical behaviors [125–127]. A number of separate lines of research have pointed to a potential role for inflammation in prostatic carcinogenesis and tumor progression [38]. These lines involve epidemiological, genetic, histopathological, molecular pathological, and animal studies. Several lines of evidence support the concept that tumor stromal cells are not merely a scaffold, but rather they influence growth, survival, and invasiveness of cancer cells, dynamically contributing to the tumor microenvironment, together with immune cells [28, 128–131]. The immune cells recruited at prostate inflammatory lesions and myofibroblasts may contribute to the release of numerous proinflammatory cytokines and chemokines that in turn can promote the oxidative stress, genomic instability, and proliferation of epithelial cells [132]. It is now ascertained that the immune system has a dual role in cancer development and progression [133, 134]. It can eradicate malignant cells, but also, it can actively promote growth of malignant cells, their invasive capacities, and their ability to metastasize. Immune cells with predominantly anti-tumor functionality include cells of the innate immune system, such as NK cells, and cells of adaptive immunity, such as conventional dendritic cells and CD8+ T-lymphocytes. Immune cells with predominantly pro-tumor functionality include a broad spectrum of cells of the innate and adaptive immune system, including type 2 neutrophils and macrophages, plasmacytoid dendritic cells, myeloid-derived suppressor cells, and regulatory T-lymphocytes. The potential mechanistic relationships between the molecular events associated with the persistent inflammatory response and prostate carcinogenesis have important implications for optimizing the current therapies against different prostatic disorders and prostate cancer. Despite the relatively high prevalence of prostate cancer, only family history, ethnicity, and age are universally recognized as risk factors, all of which are not modifiable [135]. In this context, the role of chronic inflammation remains debated [135]. Although epidemiological, histopathological, and molecular evidence suggests a robust relationship between prostatic inflammation and the pathogenesis and progression of benign prostatic enlargement, the role of inflammation in prostate carcinogenesis remains controversial. The combination of Gleason score, perineural invasion, and the density of immune and inflammatory cells should be, however, included in routine pathology reports, to be used by clinicians while making therapeutic decisions in prostate cancer.
References
Shukla ME, Yu C, Reddy CA, Stephans KL, Klein EA, Abdel-Wahab M, et al. Evaluation of the current prostate cancer staging system based on cancer-specific mortality in the surveillance, epidemiology, and end results database. Clinical Genitourin Cancer. 2015;13(1):17–21 (PubMed PMID: 25571871).
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29 (PubMed PMID: 24399786).
Loeb S, Catalona WJ. Prostate-specific antigen in clinical practice. Cancer Lett. 2007;249(1):30–9 (PubMed PMID: 17258389).
Loeb S, Gashti SN, Catalona WJ. Exclusion of inflammation in the differential diagnosis of an elevated prostate-specific antigen (PSA). Urol Oncol. 2009;27(1):64–6 (PubMed PMID: 19111800).
Schroder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. 2009;360(13):1320–8 (PubMed PMID: 19297566).
Presti JC Jr. Prostate biopsy strategies. Nat Clin Prac Urol. 2007;4(9):505–11 (PubMed PMID: 17823604).
Taverna G, Maffezzini M, Benetti A, Seveso M, Giusti G, Graziotti P. A single injection of lidocaine as local anesthesia for ultrasound guided needle biopsy of the prostate. J Urol. 2002;167(1):222–3 (PubMed PMID: 11743310).
Scattoni V, Maccagnano C, Capitanio U, Gallina A, Briganti A, Montorsi F. Random biopsy: when, how many and where to take the cores?. World J Urol. 2014;32(4):859–69 (PubMed PMID: 24908067).
Egevad L. Recent trends in Gleason grading of prostate cancer: I. Pattern interpretation. Anal Quant Cytol Histol/Int Acad Cytol Am Soc Cytol. 2008;30(4):190–8. (PubMed PMID: 18773736).
Rubin MA. Targeted therapy of cancer: new roles for pathologists–prostate cancer. Modern Pathol: Off J US Can Acad Pathol, Inc. 2008;21(Suppl 2):S44–55 (PubMed PMID: 18437173).
McDunn JE, Li Z, Adam KP, Neri BP, Wolfert RL, Milburn MV, et al. Metabolomic signatures of aggressive prostate cancer. Prostate. 2013;73(14):1547–60 (PubMed PMID: 23824564).
Schmid M, Hansen J, Rink M, Fisch M, Chun F. The development of nomograms for stratification of men at risk of prostate cancer prior to prostate biopsy. Biomark Med. 2013;7(6):843–50 (PubMed PMID: 24266817).
Dimakakos A, Armakolas A, Koutsilieris M. Novel tools for prostate cancer prognosis, diagnosis, and follow-up. BioMed Res Int. 2014;2014:890697 (PubMed PMID: 24877145. Pubmed Central PMCID: 4024423).
Valdes-Mora F, Clark SJ. Prostate cancer epigenetic biomarkers: next-generation technologies. Oncogene. 2014;0 (PubMed PMID: 24837368).
Qu M, Ren SC, Sun YH. Current early diagnostic biomarkers of prostate cancer. Asian J Androl. 2014;16(4):549–54 (PubMed PMID: 24830695).
Klotz L. Prostate cancer overdiagnosis and overtreatment. Curr Opin Endocrinol Diabetes Obes. 2013;20(3):204–9 (PubMed PMID: 23609043).
Veeranki S. Role of inflammasomes and their regulators in prostate cancer initiation, progression and metastasis. Cell Mol Biol Lett. 2013;18(3):355–67 (PubMed PMID: 23793845).
Orsted DD, Bojesen SE. The link between benign prostatic hyperplasia and prostate cancer. Nat Rev Urol. 2013;10(1):49–54 (PubMed PMID: 23165396).
Nakai Y, Nonomura N. Inflammation and prostate carcinogenesis. Int J Urol: Off J Jpn Urol Assoc. 2013;20(2):150–60 (PubMed PMID: 22852773).
Taverna G, Seveso M, Giusti G, Hurle R, Graziotti P, Stifter S, et al. Senescent remodeling of the innate and adaptive immune system in the elderly men with prostate cancer. Curr Gerontol Geriatr Res. 2014;2014:478126 (PubMed PMID: 24772169. Pubmed Central PMCID: 3977481).
De Marzo AM, Platz EA, Sutcliffe S, Xu J, Gronberg H, Drake CG, et al. Inflammation in prostate carcinogenesis. Nat Rev Cancer. 2007;7(4):256–69 (PubMed PMID: 17384581. Pubmed Central PMCID: 3552388).
Ittmann M, Huang J, Radaelli E, Martin P, Signoretti S, Sullivan R, et al. Animal models of human prostate cancer: the consensus report of the New York meeting of the Mouse Models of Human Cancers Consortium Prostate Pathology Committee. Cancer Res. 2013;73(9):2718–36 (PubMed PMID: 23610450. Pubmed Central PMCID: 3644021).
Montironi R, Lopez-Beltran A, Mazzucchelli R, Scarpelli M, Galosi AB, Cheng L. Contemporary update on pathology-related issues on routine workup of prostate biopsy: sectioning, tumor extent measurement, specimen orientation, and immunohistochemistry. Anal Quant Cytol Histol/Int Acad Cytol Am Soc Cytol. 2014;36(2):61–70 (PubMed PMID: 24902358).
Ammirante M, Luo JL, Grivennikov S, Nedospasov S, Karin M. B-cell-derived lymphotoxin promotes castration-resistant prostate cancer. Nature. 2010;464(7286):302–5 (PubMed PMID: 20220849. Pubmed Central PMCID: 2866639).
Gurel B, Lucia MS, Thompson IM, Jr., Goodman PJ, Tangen CM, Kristal AR, et al. Chronic inflammation in benign prostate tissue is associated with high-grade prostate cancer in the placebo arm of the prostate cancer prevention trial. Cancer Epidemiol Biomarkers Prev: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2014;23(5):847–56. (PubMed PMID: 24748218. Pubmed Central PMCID: 4012292).
Klinke DJ 2nd. An evolutionary perspective on anti-tumor immunity. Front Oncol. 2012;2:202 (PubMed PMID: 23336100. Pubmed Central PMCID: 3541690).
Chiarugi P, Paoli P, Cirri P. Tumor microenvironment and metabolism in prostate cancer. Semin Oncol. 2014;41(2):267–80 (PubMed PMID: 24787298).
Goldstein AS, Witte ON. Does the microenvironment influence the cell types of origin for prostate cancer? Genes Dev. 2013;27(14):1539–44 (PubMed PMID: 23873937).
Sfanos KS, Hempel HA, De Marzo AM. The role of inflammation in prostate cancer. Adv Exp Med Biol. 2014;816:153–81 (PubMed PMID: 24818723).
Vykhovanets EV, Maclennan GT, Vykhovanets OV, Gupta S. IL-17 expression by macrophages is associated with proliferative inflammatory atrophy lesions in prostate cancer patients. Int J Clin Exp Pathol. 2011;4(6):552–65. (PubMed PMID: 21904631. Pubmed Central PMCID: 3160607. Epub 2011/09/10. eng).
Fang LY, Izumi K, Lai KP, Liang L, Li L, Miyamoto H, et al. Infiltrating macrophages promote prostate tumorigenesis via modulating androgen receptor-mediated CCL4-STAT3 signaling. Cancer Res. 2013;73(18):5633–46 (PubMed PMID: 23878190. PubMed Central PMCID: 3833080).
Okada K, Kojima M, Naya Y, Kamoi K, Yokoyama K, Takamatsu T, et al. Correlation of histological inflammation in needle biopsy specimens with serum prostate-specific antigen levels in men with negative biopsy for prostate cancer. Urology. 2000;55(6):892–8 (PubMed PMID: 10840104. Epub 2000/06/07. eng).
Pittoni P, Colombo MP. The dark side of mast cell-targeted therapy in prostate cancer. Cancer Res. 2012;72(4):831–5 (PubMed PMID: 22307838. Epub 2012/02/07. eng).
Taverna G, Giusti G, Seveso M, Hurle R, Colombo P, Stifter S, et al. Mast cells as a potential prognostic marker in prostate cancer. Dis Markers. 2013;35(6):711–20 (PubMed PMID: 24324287. Pubmed Central PMCID: 3844173).
Globa T, Saptefrti L, Ceausu RA, Gaje P, Cimpean AM, Raica M. Mast cell phenotype in benign and malignant tumors of the prostate. Pol J Pathol: Off J Pol Soc Pathol. 2014;65(2):147–53 (PubMed PMID: 25119176).
Frankel TL, Burns W, Riley J, Morgan RA, Davis JL, Hanada K, et al. Identification and characterization of a tumor infiltrating CD56(+)/CD16(−) NK cell subset with specificity for pancreatic and prostate cancer cell lines. Cancer Immunol Immunother. 2010;59(12):1757–69 PubMed PMID: 20734041. Epub 2010/08/25. eng.
Kryvenko ON, Jankowski M, Chitale DA, Tang D, Rundle A, Trudeau S, et al. Inflammation and preneoplastic lesions in benign prostate as risk factors for prostate cancer. Mod Pathol: Off J US Can Acad Pathol, Inc. 2012;25(7):1023–32 (PubMed PMID: 22460812. Epub 2012/03/31. eng).
Sfanos KS, De Marzo AM. Prostate cancer and inflammation: the evidence. Histopathology. 2012;60(1):199–215 (PubMed PMID: 22212087. Epub 2012/01/04. eng).
Flammiger A, Bayer F, Cirugeda-Kuhnert A, Huland H, Tennstedt P, Simon R, et al. Intratumoral T but not B lymphocytes are related to clinical outcome in prostate cancer. Apmis. 2012;120(11):901–8 (PubMed PMID: 23009114. Epub 2012/09/27. eng).
McDowell KL, Begley LA, Mor-Vaknin N, Markovitz DM, Macoska JA. Leukocytic promotion of prostate cellular proliferation. Prostate. 2010;70(4):377–89 (Pubmed Central PMCID: 3167472. Epub 2009/10/30. eng).
Liu Y, Saeter T, Vlatkovic L, Servoll E, Waaler G, Axcrona U, et al. Dendritic and lymphocytic cell infiltration in prostate carcinoma. Histol Histopathol. 2013;28(12):1621–8 (PubMed PMID: 23729368).
Hussein MR, Al-Assiri M, Musalam AO. Phenotypic characterization of the infiltrating immune cells in normal prostate, benign nodular prostatic hyperplasia and prostatic adenocarcinoma. Exp Mol Pathol. 2009;86(2):108–13 (PubMed PMID: 19111537).
De Nunzio C, Kramer G, Marberger M, Montironi R, Nelson W, Schroder F, et al. The controversial relationship between benign prostatic hyperplasia and prostate cancer: the role of inflammation. Eur Urol. 2011;60(1):106–17 (PubMed PMID: 21497433).
Lakshmi Narendra B, Eshvendar Reddy K, Shantikumar S, Ramakrishna S. Immune system: a double-edged sword in cancer. Inflamm Res: Off J Eur Hist Res Soc [et al]. 2013;62(9):823–34 (PubMed PMID: 23868500).
Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–44 (PubMed PMID: 18650914).
Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–7 (PubMed PMID: 12490959. Pubmed Central PMCID: 2803035).
Biswas SK, Mantovani A. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat Immunol. 2010;11(10):889–96 (PubMed PMID: 20856220).
Mantovani A, Sica A. Macrophages, innate immunity and cancer: balance, tolerance, and diversity. Curr Opin Immunol. 2010;22(2):231–7 (PubMed PMID: 20144856).
Sica A, Larghi P, Mancino A, Rubino L, Porta C, Totaro MG, et al. Macrophage polarization in tumour progression. Semin Cancer Biol. 2008;18(5):349–55 (PubMed PMID: 18467122).
Lanciotti M, Masieri L, Raspollini MR, Minervini A, Mari A, Comito G, et al. The role of M1 and M2 macrophages in prostate cancer in relation to extracapsular tumor extension and biochemical recurrence after radical prostatectomy. BioMed Res Int. 2014;2014:486798 (PubMed PMID: 24738060. Pubmed Central PMCID: 3967497).
De Marzo AM, Marchi VL, Epstein JI, Nelson WG. Proliferative inflammatory atrophy of the prostate: implications for prostatic carcinogenesis. Am J Pathol. 1999;155(6):1985–92 (PubMed PMID: 10595928. Pubmed Central PMCID: 1866955).
Comito G, Giannoni E, Segura CP, Barcellos-de-Souza P, Raspollini MR, Baroni G, et al. Cancer-associated fibroblasts and M2-polarized macrophages synergize during prostate carcinoma progression. Oncogene. 2014;33(19):2423–31 (PubMed PMID: 23728338).
Xu J, Escamilla J, Mok S, David J, Priceman S, West B, et al. CSF1R signaling blockade stanches tumor-infiltrating myeloid cells and improves the efficacy of radiotherapy in prostate cancer. Cancer Res. 2013;73(9):2782–94 (PubMed PMID: 23418320).
Fujii T, Shimada K, Asai O, Tanaka N, Fujimoto K, Hirao K, et al. Immunohistochemical analysis of inflammatory cells in benign and precancerous lesions and carcinoma of the prostate. Pathobiol: J Immunopathol Mol Cell Biol. 2013;80(3):119–26 (PubMed PMID: 23328608).
Kakehi Y, Segawa T, Wu XX, Kulkarni P, Dhir R, Getzenberg RH. Down-regulation of macrophage inhibitory cytokine-1/prostate derived factor in benign prostatic hyperplasia. Prostate. 2004;59(4):351–6 (PubMed PMID: 15065082).
Dubey S, Vanveldhuizen P, Holzbeierlein J, Tawfik O, Thrasher JB, Karan D. Inflammation-associated regulation of the macrophage inhibitory cytokine (MIC-1) gene in prostate cancer. Oncol Lett. 2012;3(5):1166–70 (PubMed PMID: 22783412. Pubmed Central PMCID: 3389684).
Pickup M, Novitskiy S, Moses HL. The roles of TGFbeta in the tumour microenvironment. Nat Rev Cancer. 2013;13(11):788–99 (PubMed PMID: 24132110).
Vanhara P, Hampl A, Kozubik A, Soucek K. Growth/differentiation factor-15: prostate cancer suppressor or promoter? Prostate Cancer Prostatic Dis. 2012;15(4):320–8 (PubMed PMID: 22370725).
Wang T, Welte T. Role of natural killer and Gamma-delta T cells in West Nile virus infection. Viruses. 2013;5(9):2298–310 (PubMed PMID: 24061543. Pubmed Central PMCID: 3798903).
Yuan H, Hsiao YH, Zhang Y, Wang J, Yin C, Shen R, et al. Destructive impact of T-lymphocytes, NK and Mast cells on basal cell layers: implications for tumor invasion. BMC Cancer. 2013;13:258 (PubMed PMID: 23705594. Pubmed Central PMCID: 3722065).
Jaillon S, Galdiero MR, Del Prete D, Cassatella MA, Garlanda C, Mantovani A. Neutrophils in innate and adaptive immunity. Semin Immunopathol. 2013;35(4):377–94 (PubMed PMID: 23553214).
Fujita K, Imamura R, Tanigawa G, Nakagawa M, Hayashi T, Kishimoto N, et al. Low serum neutrophil count predicts a positive prostate biopsy. Prostate Cancer Prostatic Dis. 2012;15(4):386–90 (PubMed PMID: 22777394).
Bekes EM, Schweighofer B, Kupriyanova TA, Zajac E, Ardi VC, Quigley JP, et al. Tumor-recruited neutrophils and neutrophil TIMP-free MMP-9 regulate coordinately the levels of tumor angiogenesis and efficiency of malignant cell intravasation. Am J Pathol. 2011;179(3):1455–70 (PubMed PMID: 21741942. Pubmed Central PMCID: 3157227).
Keizman D, Gottfried M, Ish-Shalom M, Maimon N, Peer A, Neumann A, et al. Pretreatment neutrophil-to-lymphocyte ratio in metastatic castration-resistant prostate cancer patients treated with ketoconazole: association with outcome and predictive nomogram. Oncologist. 2012;17(12):1508–14 (PubMed PMID: 22971522. Pubmed Central PMCID: 3528383).
Raval RR, Sharabi AB, Walker AJ, Drake CG, Sharma P. Tumor immunology and cancer immunotherapy: summary of the 2013 SITC primer. J Immunother Cancer. 2014;2:14 (PubMed PMID: 24883190. Pubmed Central PMCID: 4039332).
McArdle PA, Canna K, McMillan DC, McNicol AM, Campbell R, Underwood MA. The relationship between T-lymphocyte subset infiltration and survival in patients with prostate cancer. Br J Cancer. 2004;91(3):541–3 (PubMed PMID: 15266325. Pubmed Central PMCID: 2409839).
Yuan H, Wei X, Zhang G, Li C, Zhang X, Hou J. B7-H3 over expression in prostate cancer promotes tumor cell progression. J Urol. 2011;186(3):1093–9 (PubMed PMID: 21784485).
Si TG, Wang JP, Guo Z. Analysis of circulating regulatory T cells (CD4+ CD25+ CD127−) after cryosurgery in prostate cancer. Asian J Androl. 2013;15(4):461–5 (PubMed PMID: 23728588. Pubmed Central PMCID: 3739231).
Miller AM, Lundberg K, Ozenci V, Banham AH, Hellstrom M, Egevad L, et al. CD4+ CD25high T cells are enriched in the tumor and peripheral blood of prostate cancer patients. J Immunol. 2006;177(10):7398–405 (PubMed PMID: 17082659).
Yokokawa J, Cereda V, Remondo C, Gulley JL, Arlen PM, Schlom J, et al. Enhanced functionality of CD4+CD25(high)FoxP3+ regulatory T cells in the peripheral blood of patients with prostate cancer. Clin Cancer Res: Off J Am Assoc Cancer Res. 2008;14(4):1032–40 (PubMed PMID: 18281535).
Sfanos KS, Bruno TC, Maris CH, Xu L, Thoburn CJ, DeMarzo AM, et al. Phenotypic analysis of prostate-infiltrating lymphocytes reveals TH17 and Treg skewing. Clinical Cancer Research: Off J Am Assoc Cancer Res. 2008;14(11):3254–61 (PubMed PMID: 18519750. Pubmed Central PMCID: 3082357).
Zou L, Barnett B, Safah H, Larussa VF, Evdemon-Hogan M, Mottram P, et al. Bone marrow is a reservoir for CD4+CD25+ regulatory T cells that traffic through CXCL12/CXCR4 signals. Cancer Res. 2004;64(22):8451–5 (PubMed PMID: 15548717).
Davidsson S, Ohlson AL, Andersson SO, Fall K, Meisner A, Fiorentino M, et al. CD4 helper T cells, CD8 cytotoxic T cells, and FOXP3(+) regulatory T cells with respect to lethal prostate cancer. Modern Pathol: Off J US Can Acad Pathol, Inc. 2013;26(3):448–55 (PubMed PMID: 23041830).
Gannon PO, Alam Fahmy M, Begin LR, Djoukhadjian A, Filali-Mouhim A, Lapointe R, et al. Presence of prostate cancer metastasis correlates with lower lymph node reactivity. Prostate. 2006;66(16):1710–20 (PubMed PMID: 16955408).
Vindrieux D, Escobar P, Lazennec G. Emerging roles of chemokines in prostate cancer. Endocr Relat Cancer. 2009;16(3):663–73 (PubMed PMID: 19556286).
Balkwill FR. The chemokine system and cancer. J Pathol. 2012;226(2):148–57 (PubMed PMID: 21989643).
Vendramini-Costa DB, Carvalho JE. Molecular link mechanisms between inflammation and cancer. Curr Pharm Des. 2012;18(26):3831–52 (PubMed PMID: 22632748).
Salazar N, Castellan M, Shirodkar SS, Lokeshwar BL. Chemokines and chemokine receptors as promoters of prostate cancer growth and progression. Critical Rev Eukaryot Gene Expr. 2013;23(1):77–91 (PubMed PMID: 23557339. Pubmed Central PMCID: 3736734).
Gajewski TF, Schreiber H, Fu YX. Innate and adaptive immune cells in the tumor microenvironment. Nat Immunol. 2013;14(10):1014–22 (PubMed PMID: 24048123. Pubmed Central PMCID: 4118725).
Bonecchi R, Galliera E, Borroni EM, Corsi MM, Locati M, Mantovani A. Chemokines and chemokine receptors: an overview. Front Biosci. 2009;14:540–51 (PubMed PMID: 19273084).
Mantovani A, Savino B, Locati M, Zammataro L, Allavena P, Bonecchi R. The chemokine system in cancer biology and therapy. Cytokine Growth Factor Rev. 2010;21(1):27–39 (PubMed PMID: 20004131).
Chow MT, Luster AD. Chemokines in cancer. Cancer Immunol Res. 2014;2(12):1125–31 (PubMed PMID: 25480554. Pubmed Central PMCID: 4258879).
Allavena P, Germano G, Marchesi F, Mantovani A. Chemokines in cancer related inflammation. Exp Cell Res. 2011;317(5):664–73 (PubMed PMID: 21134366).
Koizumi K, Hojo S, Akashi T, Yasumoto K, Saiki I. Chemokine receptors in cancer metastasis and cancer cell-derived chemokines in host immune response. Cancer Sci. 2007;98(11):1652–8 (PubMed PMID: 17894551).
Ben-Baruch A. Organ selectivity in metastasis: regulation by chemokines and their receptors. Clin Exp Metastasis. 2008;25(4):345–56 (PubMed PMID: 17891505).
Zlotnik A, Burkhardt AM, Homey B. Homeostatic chemokine receptors and organ-specific metastasis. Nat Rev Immunol. 2011;11(9):597–606 (PubMed PMID: 21866172).
Wu Q, Dhir R, Wells A. Altered CXCR3 isoform expression regulates prostate cancer cell migration and invasion. Mol Cancer. 2012;11:3 (PubMed PMID: 22236567. Pubmed Central PMCID: 3320557).
Gillies K, Wertman J, Charette N, Dupre DJ. Anterograde trafficking of CXCR4 and CCR2 receptors in a prostate cancer cell line. Cell Physiol Biochem: Int J Exper Cell Physiol Biochem Pharmacol. 2013;32(1):74–85 (PubMed PMID: 23839224).
Kato T, Fujita Y, Nakane K, Mizutani K, Terazawa R, Ehara H, et al. CCR1/CCL5 interaction promotes invasion of taxane-resistant PC3 prostate cancer cells by increasing secretion of MMPs 2/9 and by activating ERK and Rac signaling. Cytokine. 2013;64(1):251–7 (PubMed PMID: 23876400).
Zhu F, Liu P, Li J, Zhang Y. Eotaxin-1 promotes prostate cancer cell invasion via activation of the CCR3-ERK pathway and upregulation of MMP-3 expression. Oncol Rep. 2014;31(5):2049–54 (PubMed PMID: 24604010).
Lam C, Pavel MA, Kashyap P, Salehi-Najafabadi Z, Valentino V, Yu Y. Detection of CXCR2 cytokine receptor surface expression using immunofluorescence. Methods Mol Biol. 2014;1172:193–200 (PubMed PMID: 24908306).
Peng C, Zhou K, An S, Yang J. The effect of CCL19/CCR7 on the proliferation and migration of cell in prostate cancer. Tumour Biol: J Int Soc Oncodevelop Biol Med. 2015;36(1):329–35 (PubMed PMID: 25256673).
Maxwell PJ, Neisen J, Messenger J, Waugh DJ. Tumor-derived CXCL8 signaling augments stroma-derived CCL2-promoted proliferation and CXCL12-mediated invasion of PTEN-deficient prostate cancer cells. Oncotarget. 2014;5(13):4895–908 (PubMed PMID: 24970800. Pubmed Central PMCID: 4148108).
Culig Z. CXCL8, an underestimated “bad guy” in prostate cancer. Eur Urol. 2013;64(2):189–90 (discussion 90-2. PubMed PMID: 23000087).
Benelli R, Stigliani S, Minghelli S, Carlone S, Ferrari N. Impact of CXCL1 overexpression on growth and invasion of prostate cancer cell. Prostate. 2013;73(9):941–51 (PubMed PMID: 23334998).
Lin TH, Liu HH, Tsai TH, Chen CC, Hsieh TF, Lee SS, et al. CCL2 increases alphavbeta3 integrin expression and subsequently promotes prostate cancer migration. Biochim Biophys Acta. 2013;1830(10):4917–27 (PubMed PMID: 23845726).
Fang LY, Izumi K, Lai KP, Liang L, Li L, Miyamoto H, et al. Infiltrating macrophages promote prostate tumorigenesis via modulating androgen receptor-mediated CCL4-STAT3 signaling. Cancer research. 2013;73(18):5633–46 (PubMed PMID: 23878190. Pubmed Central PMCID: 3833080).
Ammirante M, Shalapour S, Kang Y, Jamieson CA, Karin M. Tissue injury and hypoxia promote malignant progression of prostate cancer by inducing CXCL13 expression in tumor myofibroblasts. Proc Natl Acad Sci USA. 2014;111(41):14776–81 (PubMed PMID: 25267627. Pubmed Central PMCID: 4205637).
Chen G, Liang YX, Zhu JG, Fu X, Chen YF, Mo RJ, et al. CC chemokine ligand 18 correlates with malignant progression of prostate cancer. BioMed Res Int. 2014;2014:230183 (PubMed PMID: 25197632. Pubmed Central PMCID: 4150478).
Singh RK, Lokeshwar BL. The IL-8-regulated chemokine receptor CXCR7 stimulates EGFR signaling to promote prostate cancer growth. Cancer Res. 2011;71(9):3268–77 (PubMed PMID: 21398406. Pubmed Central PMCID: 3085571).
Ellem SJ, Taylor RA, Furic L, Larsson O, Frydenberg M, Pook D, et al. A pro-tumourigenic loop at the human prostate tumour interface orchestrated by oestrogen, CXCL12 and mast cell recruitment. J Pathol. 2014;234(1):86–98 (PubMed PMID: 25042571).
Lin WJ, Izumi K. Androgen receptor, ccl2, and epithelial-mesenchymal transition: A dangerous affair in the tumor microenvironment. Oncoimmunology. 2014;3:e27871 (PubMed PMID: 25339999. Pubmed Central PMCID: 4203538).
Izumi K, Fang LY, Mizokami A, Namiki M, Li L, Lin WJ, et al. Targeting the androgen receptor with siRNA promotes prostate cancer metastasis through enhanced macrophage recruitment via CCL2/CCR2-induced STAT3 activation. EMBO Mol Med. 2013;5(9):1383–401 (PubMed PMID: 23982944. Pubmed Central PMCID: 3799493).
Bao BY, Yao J, Lee YF. 1alpha, 25-dihydroxyvitamin D3 suppresses interleukin-8-mediated prostate cancer cell angiogenesis. Carcinogenesis. 2006;27(9):1883–93 (PubMed PMID: 16624828).
Velonas VM, Woo HH, dos Remedios CG, Assinder SJ. Current status of biomarkers for prostate cancer. Int J Mol Sci. 2013;14(6):11034–60 (PubMed PMID: 23708103. Pubmed Central PMCID: 3709717).
Balk SP, Ko YJ, Bubley GJ. Biology of prostate-specific antigen. J Clin Oncol. 2003;21(2):383–91 (PubMed PMID: 12525533).
Makarov DV, Loeb S, Getzenberg RH, Partin AW. Biomarkers for prostate cancer. Annu Rev Med. 2009;60:139–51 (PubMed PMID: 18947298).
Tsaur I, Noack A, Makarevic J, Oppermann E, Waaga-Gasser AM, Gasser M, et al. CCL2 chemokine as a potential biomarker for prostate cancer: a pilot study. Cancer Res Treat: Off J Korean Cancer Assoc. 2014. doi:10.4143/crt.2014.015 (PubMed PMID: 25483747).
Xu Y, Zhang L, Sun SK, Zhang X. CC chemokine ligand 18 and IGF-binding protein 6 as potential serum biomarkers for prostate cancer. Tohoku J Exper Med. 2014;233(1):25–31 (PubMed PMID: 24747338).
Sharma J, Gray KP, Harshman LC, Evan C, Nakabayashi M, Fichorova R, et al. Elevated IL-8, TNF-alpha, and MCP-1 in men with metastatic prostate cancer starting androgen-deprivation therapy (ADT) are associated with shorter time to castration-resistance and overall survival. Prostate. 2014;74(8):820–8 (PubMed PMID: 24668612).
Agarwal M, He C, Siddiqui J, Wei JT, Macoska JA. CCL11 (eotaxin-1): a new diagnostic serum marker for prostate cancer. Prostate. 2013;73(6):573–81 (PubMed PMID: 23059958. Pubmed Central PMCID: 3594486).
Miyake M, Lawton A, Goodison S, Urquidi V, Rosser CJ. Chemokine (C-X-C motif) ligand 1 (CXCL1) protein expression is increased in high-grade prostate cancer. Pathol Res Pract. 2014;210(2):74–8 (PubMed PMID: 24252309).
Bostwick DG, Burke HB, Djakiew D, Euling S, Ho SM, Landolph J, et al. Human prostate cancer risk factors. Cancer. 2004;101(10 Suppl):2371–490 (PubMed PMID: 15495199).
Wallace TA, Prueitt RL, Yi M, Howe TM, Gillespie JW, Yfantis HG, et al. Tumor immunobiological differences in prostate cancer between African-American and European-American men. Cancer Res. 2008;68(3):927–36 (PubMed PMID: 18245496).
Isman FK, Kucukgergin C, Dasdemir S, Cakmakoglu B, Sanli O, Seckin S. Association between SDF1-3′A or CXCR4 gene polymorphisms with predisposition to and clinicopathological characteristics of prostate cancer with or without metastases. Mol Biol Rep. 2012;39(12):11073–9 (PubMed PMID: 23053994).
Mandal RK, Agrawal T, Mittal RD. Genetic variants of chemokine CCL2 and chemokine receptor CCR2 genes and risk of prostate cancer. Tumour Biol: J Int Soc Oncodevelopment Biol Med. 2015;36(1):375–81 (PubMed PMID: 25266801).
Kirk PS, Koreckij T, Nguyen HM, Brown LG, Snyder LA, Vessella RL, et al. Inhibition of CCL2 signaling in combination with docetaxel treatment has profound inhibitory effects on prostate cancer growth in bone. Int J Mol Sci. 2013;14(5):10483–96 (PubMed PMID: 23698775. Pubmed Central PMCID: 3676850).
Zhang J, Patel L, Pienta KJ. Targeting chemokine (C-C motif) ligand 2 (CCL2) as an example of translation of cancer molecular biology to the clinic. Prog Mol Biol Transl Sci. 2010;95:31–53 (PubMed PMID: 21075328. Pubmed Central PMCID: 3197817).
Zhang J, Lu Y, Pienta KJ. Multiple roles of chemokine (C-C motif) ligand 2 in promoting prostate cancer growth. J Natl Cancer Inst. 2010;102(8):522–8 (PubMed PMID: 20233997. Pubmed Central PMCID: 2857800).
Arnatt CK, Adams JL, Zhang Z, Haney KM, Li G, Zhang Y. Design, syntheses, and characterization of piperazine based chemokine receptor CCR5 antagonists as anti prostate cancer agents. Bioorg Med Chem Lett. 2014;24(10):2319–23 (PubMed PMID: 24731275).
Arnatt CK, Zaidi SA, Zhang Z, Li G, Richardson AC, Ware JL, et al. Design, syntheses, and characterization of pharmacophore based chemokine receptor CCR5 antagonists as anti prostate cancer agents. Eur J Med Chem. 2013;69:647–58 (PubMed PMID: 24095757).
Bhardwaj A, Srivastava SK, Singh S, Arora S, Tyagi N, Andrews J, et al. CXCL12/CXCR4 signaling counteracts docetaxel-induced microtubule stabilization via p21-activated kinase 4-dependent activation of LIM domain kinase 1. Oncotarget. 2014;5(22):11490–500 (PubMed PMID: 25359780. Pubmed Central PMCID: 4294337).
Domanska UM, Timmer-Bosscha H, Nagengast WB, Oude Munnink TH, Kruizinga RC, Ananias HJ, et al. CXCR4 inhibition with AMD3100 sensitizes prostate cancer to docetaxel chemotherapy. Neoplasia. 2012;14(8):709–18 (PubMed PMID: 22952424. Pubmed Central PMCID: 3431178).
Rhee YH, Chung PS, Kim SH, Ahn JC. CXCR4 and PTEN are involved in the anti-metastatic regulation of anethole in DU145 prostate cancer cells. Biochem Biophys Res Commun. 2014;447(4):557–62 (PubMed PMID: 24525130).
Mackinnon AC, Yan BC, Joseph LJ, Al-Ahmadie HA. Molecular biology underlying the clinical heterogeneity of prostate cancer: an update. Arch Pathol Lab Med. 2009;133(7):1033–40 (PubMed PMID: 19642730. Epub 2009/08/01. eng).
Gerlinger M, Catto JW, Orntoft TF, Real FX, Zwarthoff EC, Swanton C. Intratumour heterogeneity in urologic cancers: from molecular evidence to clinical implications. Eur Urol. 2015;67(4):729–37 (PubMed PMID: 24836153).
Demichelis F, Stanford JL. Genetic predisposition to prostate cancer: Update and future perspectives. Urol Oncol. 2015;33(2):75–84 (PubMed PMID: 24996773).
Franco OE, Hayward SW. Targeting the tumor stroma as a novel therapeutic approach for prostate cancer. Adv Pharmacol. 2012;65:267–313 (PubMed PMID: 22959029. Epub 2012/09/11. eng).
Iacopino F, Angelucci C, Sica G. Interactions between normal human fibroblasts and human prostate cancer cells in a co-culture system. Anticancer Res. 2012;32(5):1579–88 (PubMed PMID: 22593435. Epub 2012/05/18. eng).
Parrinello S, Coppe JP, Krtolica A, Campisi J. Stromal-epithelial interactions in aging and cancer: senescent fibroblasts alter epithelial cell differentiation. J Cell Sci. 2005;118(Pt 3):485–96 (PubMed PMID: 15657080. Epub 2005/01/20. eng).
Gharaee-Kermani M, Kasina S, Moore BB, Thomas D, Mehra R, Macoska JA. CXC-type chemokines promote myofibroblast phenoconversion and prostatic fibrosis. PloS one. 2012;7(11):e49278 (PubMed PMID: 23173053. Pubmed Central PMCID: 3500280).
Mimeault M, Batra SK. Development of animal models underlining mechanistic connections between prostate inflammation and cancer. World J Clin Oncol. 2013;4(1):4–13 (PubMed PMID: 23539141. Pubmed Central PMCID: 3609015).
Gutkin DW, Shurin MR. Clinical evaluation of systemic and local immune responses in cancer: time for integration. Cancer Immunol Immunother. 2014;63(1):45–57 (PubMed PMID: 24100804. Pubmed Central PMCID: 4018188).
Fridman WH, Pages F, Sautes-Fridman C, Galon J. The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer. 2012;12(4):298–306 (PubMed PMID: 22419253).
Vignozzi L, Maggi M. Prostate cancer: intriguing data on inflammation and prostate cancer. Nat Rev Urol. 2014;11(7):369–70 (PubMed PMID: 24980193).
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible Editor: John Di Battista.
Rights and permissions
About this article

Cite this article
Taverna, G., Pedretti, E., Di Caro, G. et al. Inflammation and prostate cancer: friends or foe?. Inflamm. Res. 64, 275–286 (2015). https://doi.org/10.1007/s00011-015-0812-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-015-0812-2