
Abstract
Discovery of innovative anxiolytics is severely hampering. Existing anxiolytics are developed decades ago and are still the therapeutics of choice. Moreover, lack of new drug targets forecasts a severe jeopardy in the future treatment of the huge population of CNS-diseased patients. We simply lack the knowledge on what is wrong in brains of anxious people (normal and diseased). Translational research, based on interacting clinical and preclinical research, is extremely urgent. In this endeavor, genetic and genomic approaches are part of the spectrum of contributing factors. We focus on three druggable targets: serotonin transporter, 5-HT1A, and GABAA receptors. It is still uncertain whether and how these targets are involved in normal and diseased anxiety processes. For serotonergic anxiolytics, the slow onset of action points to indirect effects leading to plasticity changes in brain systems leading to reduced anxiety. For GABAA benzodiazepine drugs, acute anxiolytic effects are found indicating primary mechanisms directly influencing anxiety processes. Close translational collaboration between fundamental academic and discovery research will lead to badly needed breakthroughs in the search for new anxiolytics.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Anxiety disorders
- Anxiolytics
- Serotonin
- GABAA-benzodiazepine receptor complex
- Animal models
- Translational research
Introduction
Anxiety disorders are among the most prevalent psychiatric disorders. In DSM5, anxiety disorders include separation anxiety disorder, selective mutism, specific phobia, social anxiety disorder, panic disorder, agoraphobia, and generalized anxiety disorder. The impact of anxiety disorders is high; studies in Europe [1] or the USA [2] estimate anxiety disorders at approximately 14% and 22%, respectively, of the population. Moreover, anxiety disorders are often comorbid with other psychiatric disorders, including mood and substance abuse disorders. Anxiety disorders are quite heterogeneous, and the individual disorders (e.g., panic disorder versus phobia or generalized anxiety disorder) are quite distant from each other. No laboratory blood test or brain scan or any other biomarker is yet available to distinguish between either disorder. The complex classification of the various anxiety disorders complicates or even hinders the finding and development of new psychoactive drugs, notably because one-to-one translation to preclinical animal models of such anxiety disorders is extremely difficult to realize, if not impossible. Although a classification in intermediate phenotypes [3] that are based on neurobiological mechanisms probably underlying pathological anxiety processes has been suggested, this has not led to novel, innovative treatments for anxiety yet. Another hypothesis is based on the assumption that dysfunctional neurotransmitter systems underlie disturbances in the regulation of anxiety processes in the CNS. However, dysfunctional neurotransmitter systems are difficult to prove, and a direct relationship between certain neurotransmitter systems (e.g., the serotonergic or GABA-ergic system) is difficult to establish. Actually, drugs influencing these systems and exerting anxiolytic properties were found serendipitously (benzodiazepines; BDZ) or developed initially for other purposes (selective serotonin reuptake inhibitors; SSRIs) many decades ago. Since 2007, no new anxiolytic agents have been approved by the US Food and Drug Administration [4], and SSRIs (and to a lesser extent serotonin-norepinephrine reuptake inhibitors; SNRIs) remain the mainstay for the treatment of anxiety disorders (often augmented or preceded by certain BDZs for a limited time period). Not all patients respond well to serotonergic therapy, either due to bothersome side effects or treatment resistance.
The last decades’ intense efforts have been made both in preclinical and clinical studies, to find and test other mechanisms targeting anxiety-involved mechanisms in the CNS in order to detect new and/or improved treatments for the various anxiety disorders.
In the following parts, the existing anxiolytics and putative new promising anxiety targets will be described. First, using a translational approach, serotonergic targets, in particular the serotonergic transporter and 5-HT1A- and 5-HT2 receptors, will be outlined, followed by the involvement of the GABAA system in anxiety and anxiety disorders. Some new potential targets will be shortly introduced (CRF1 receptor, neurokinin1 (NK1) receptors, glucocorticoid receptors, and glutamatergic receptors [5, 6].
The Serotonin Transporter (5-HTT)
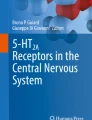
There are at least 14 different serotonin receptor types (5-HT1 (A,B,D,E,F), 5-HT2 (A,B, C), 5-HT3, 5-HT4, 5-HT5 (A,B), 5-HT6, and 5-HT7). Except for the 5-HT3 receptor, all 5-HT receptors are G-protein coupled. Signaling via these G-protein-coupled serotonin receptors is extremely diverse, and we are still largely in the dark how these various 5-HT receptors operate in and contribute to the extremely complex interaction in the various ongoing functions in the CNS. This diversity in combination with a complex distribution of the various receptors in the brain seems to bring the serotonergic system in an important position to modulate various functions in the brain. Disruption of various aspects of serotonergic neurotransmission contributes to changes in vulnerability or even psychopathology, including depression, anxiety disorders, schizophrenia, and others [7]. All 5-HT receptors are postsynaptically located on non-serotonergic neurons (heteroreceptors), but 5-HT1A and 5-HT1B/1D receptors are also present as autoreceptors on the soma (5-HT1A) or synaptic area (5-HT1B/1D) of serotonergic cells (Fig. 8.1). The serotonin transporter (5-HTT) is localized both in the synaptic area and on the cell bodies of 5-HT neurons (Fig. 8.2). If serotonergic neurons fire, 5-HT is released into the synaptic cleft where it exerts its action on nearby pre- and postsynaptic serotonergic receptors. The 5-HTT is a key regulator of 5-HT signaling. The reuptake of serotonin by serotonergic neurons via the 5-HTT is the main mechanism for clearing extracellular 5-HT after its release; this leads to the termination of 5-HT signaling and recycles 5-HT in the neuron for subsequent release via uptake by the vesicular monoamine transporter (VMAT2). Another major route to end serotonergic activity is via uptake of synaptic 5-HT by surrounding glial cells where it is degraded to its main metabolite 5-hydroxyindole acetic acid (5-HIAA) by monoamine oxidase-A (MAO-A).

Cartoon showing a serotonergic neuron and two postsynaptic non-serotonergic neuron (top and right). The various 5-HT receptors and the 5-HTT are schematically localized on these three neurons. 5-HT1A receptors are present as somatodendritic autoreceptors and postsynaptic heteroreceptors. 5-HT1B/1D receptors are present as presynaptic receptors in the synaptic cleft and as postsynaptic heteroreceptors. The 5-HTT is present in the presynaptic part and at the soma of the serotonergic neuron. All other receptor(types) are postsynaptically located

Schematic representation of serotonin (5-HT) in the terminal and synapse. G-protein-coupled receptors are located presynaptically (5-HT autoreceptors 5-HT1A/1B) or postsynaptically (5-HT 1/2/3/4/5/6/7 receptors). 1: 5-HT is released from the presynaptic neuron and binds to a heterotrimeric G-protein postsynaptic receptor. Heterotrimeric G-protein complexes contain an α, β, and γ subunit, which in an inactive state are bound to GDP. 2: 5-HT acts on postsynaptic receptors and induces a change in the conformation of the postsynaptic receptor. GDP is phosphorylated to GTP and binds to the α subunit, which subsequently becomes active. The β and γ subunits are freed. 3: Extracellular 5-HT is taken up by the 5-HTT into the presynaptic neuron. 4: Back in the presynaptic neuron 5-HT is broken down by MAO to 5-HIAA (occurs also extracellularly) or is being stored in vesicles for future release. MAO, monoamine oxidase; 5-HIAA, 5-hydroxyindole acetic acid; SERT, serotonin transporter. Figure adapted from Vinkers et al. [113]
SSRIs are presently considered as the first-line pharmaceutical treatment for anxiety disorders, whereas SNRIs are considered second- or third-line treatments [8]. In a meta-analysis the differential efficacy of SSRIs and SNRIs and placebo in the treatment of anxiety disorders (together with depression, obsessive-compulsive disorder (OCD) and post-traumatic stress disorder) were estimated in children and adolescents [8]. SSRIs and SNRIs were about equally effective in treating anxiety disorders and more beneficial than placebo. Well-known, but still remarkable, is the placebo effect. This is a general observation in psychiatric treatments, both in pediatric and adult applications [9]. Notwithstanding this influential factor, it is generally accepted that psychotropic drugs that inhibit the 5-HTT in the CNS, exert anxiolytic activity in various patient groups with diverse anxiety and fear disturbances.
For an extensive time, the 5-HT transporter has been implicated in processes involved in anxiety mechanisms. Blocking the 5-HTT leads to an acute rise in the synaptic concentration of serotonin. However, anxiolytic efficacy (similarly to depression) only emerges after longer treatment (weeks to months), indicating that long-term plasticity changes in presumed anxiety mechanisms have to take place. It is still largely unknown what those mechanisms are and how they come about. But the pathogenesis of anxiety disorders (and particularly GAD) is clearly influenced by many factors; moreover, many complex interactions between biological factors, experimental influences, and psychological mechanisms are involved [10]. In linkage studies and non-hypothesis-driven genome-wide association studies (GWAS) in large populations with various anxiety disorder problems, an association with the 5-HTT was never found [10], although some evidence emerged that a highly interconnected molecular network around GAD is part of the anxiety spectrum of disorders [11]. Candidate gene studies on putative individual nodes of this putative anxiety network have generated considerable evidence in favor of the serotonergic system and its impact on anxiety-related endophenotypes [10, 12].
Polymorphisms in the 5-HTT-gene and its associated transcriptional control area influence the activity of the serotonergic system [13]. Although focusing on anxiety, the 5-HTT gene and its variations (SLC6A4), producing a 5-HTT protein, are associated with several human behavioral and neurological traits but also with various medical disorders (e.g., myocardial infarction, pulmonary hypertension, irritable bowel syndrome, and sudden infant death syndrome) [14]. This indicates the important role of serotonergic neurotransmission in various aspects of our healthy and diseased biology. The emerging developmental role of serotonin [15] in psychiatric disorders, including anxiety-related ones, suggests that developmental disturbances in changing serotonin levels during critical periods in development (windows) may have long-lasting effects on brain function, particularly on later anxiety-related behaviors in adulthood [16, 17].
Most research involving the role of the 5-HTTs in psychiatry including anxiety disorders has been performed in adult populations. Lower 5-HTT expression and function in genotypes with the S-allele of the 5-HTTLPR (5-HTT length polymorphism) are associated with anxiety and depression [18, 19]. Subsequently, the 5-HTTPRL and associated variations in coding and noncoding regions of the 5-HTT-gene have been associated with many aspects of psychiatric disorders [14, 20]. The human 5-HTT is located at chromosome 17 (17q11.2) and consists of 14 exons spanning around 40kB; the emerging 5-HTT protein of 630 amino acids comprises 12 membrane domains (see Fig. 8.3). The expression of the human 5-HTT gene is modulated by a length variation (L and S variants) in the 5-HTTLPR and two SNPs in the same region (rs25531 and rs25332), all located upstream of the start of transcription. The single-nucleotide polymorphism rs25531 subdivides the L-allele into LA and LG alleles; the LA allele is associated with increased expression of activity compared to LG or S-alleles. A variable number of tandem repeat (VNTR) polymorphisms, called STin2, are present in intron 2, together with various SNPs influencing the activity of the 5-HTT protein. This polymorphism is tri-allelic, with 9-, 10-, or 12-repeat alleles. The latter allele is associated with enhanced 5-HTT expression [21]. It seems possible that individuals with low 5-HTT expressing genotypes, when exposed to SSRIs, have higher 5-HTT occupancy and saturation, theoretically associated with increasing central and peripheral serotonin availability. This might manifest itself as more side effects [21]. The 5-HTT is an extremely important modulator of the serotonergic neuronal system; duration and magnitude of serotonergic neurotransmission is largely steered by 5-HTT activity, thereby fine-tuning 5-HT signaling. Dysfunctions in these signaling pathways have been related to several psychiatric disorders and traits, including anxiety. Although initially, the S- and L-variants of the 5-HTTPRL were associated with differential vulnerability to neuropsychiatric disorders (or as a predictor of response to SSRIs), recent findings show a far more complicated pattern, where various polymorphisms inside the promoter region influence the activity of the 5-HT reuptake properties of the 5-HTT [22].

Different alterations in the human, rhesus, and rodent 5-HTT gene resulting in changed transcription levels of 5-HTT. (a) Humans and rhesus macaques have short or long alleles for the 5-HTTLPR resulting in either lower or higher transcription levels, respectively. Since rodents do not carry an orthologue of this polymorphism, knockout of the 5-HTT can be achieved by (b) replacing exon 2 with a neo cassette (mice) or by (c) inducing a premature stop codon in exon 3 (rats) resulting in the absence of functional 5-HTT protein. (Figure adapted from Houwing et al. [56])
The story of modulation of serotonergic transmission via 5-HT mechanisms reveals the complexity of factors involved in the genetic-function coupling of any psychiatric disorder. The identification of specific gene variants and their involvement in anxiety is quite troublesome. It is increasingly clear that these variations may influence “intermediate biological phenotypes” in concert with other (background) genes, epigenetic factors, and environmental and developmental factors. Such complex interactions likely seem to contribute to the risk or resilience to develop certain psychiatric conditions. Using intermediate phenotypes may enable the search for associations between specific candidate genes (e.g., for 5-HTT) that mediate between a modulating allele and a complex disease phenotype [23].
Various studies on the 5-HTTPRL-promoter area are testing gene X environment and gene X gene interactions [24,25,26,27]. In general, S-alleles of 5-HTTPRL are associated with enhanced risk for a variety of psychiatric disorders, including anxiety. Caspi et al. [28] hypothesized the S-allele as a “risk” or “vulnerability” allele; the role of the L-allele is less clear although it has been suggested as risk factor for development of psychopathological traits [29]. Because L- and S-alleles are common to each human, and psychopathology does not happen in every individual, it is assumed that our genome includes “protective” alleles (e.g., CRF1-receptor variants) rendering individuals resilient to pathology [30,31,32].
Genes certainly contribute to the risk to develop anxiety disorders and underlie anxious traits. No candidate genes have emerged playing a primary role in the expression for a vulnerability to anxiety or anxiety disorders [33, 34]. Meta-analysis of genotypes implicated in mental disorders with varying levels of heritability has indicated that for anxiety disorders, only three genes have been identified that contribute to anxious phenotypes (in contrast to, e.g., 50 genes for schizophrenia [33]). The former study did not implicate the 5-HTT and associated promoter area (5-HTTPRL) as a candidate gene involved in anxiety disorders. These complex findings indicate the difficulties in discovering new targets for anxiolytic drugs. This reflects that such complex neurobehavioral traits or disorders like the anxiety disorders are not caused by single genes, but probably by disturbances in extensive networks comprising of numerous parts and pathways that are created by many biological mechanisms.
Preclinical Evidence for the 5-HTT in Anxiety
Human linkage and association studies have not identified genes that contribute influentially in the modulation of anxiety or anxiety disorders; therefore, animal pathology and models might be of considerable importance in studying the involvement of genes in anxiety disorders as well. Human anxiety pathology is also present to a certain degree in animal pathology [35], and studies in animal anxiety models have considerably enhanced our knowledge of the neurobiological mechanisms involved in anxiety. Animal models can be very helpful in delineating putative genes involved in either anxiety or anxiety-associated traits [12, 36]. In order to progress in our search for fundamental mechanisms involved in anxiety processes and those in anxiety disorders, we need a translational approach; data from anxiety research, including genetic and environmental factors, should lead to fundamental research in animal models but also the reverse. The availability of cell-specific and inducible knockout and knock-ins, optogenetic technology [37], and, more recently, the Crispr/Cas 9 technology [38] enables selective operations in cellular mechanisms and circuit functions that are coupled to the gene’s function [37]. These techniques are now starting to be applied in animal models of fear and anxiety.
Numerous preclinical anxiety and fear tests have been developed and used over time [39,40,41]. Animal tests and models of anxiety are based on face validity (is it measuring something analogous to human anxiety symptoms?), predictive validity (is it sensitive to clinically efficacious anxiolytics?), and construct validity (are the same pathophysiological mechanisms involved as in human anxiety disorders?). Till up now, none of the currently available anxiety tests or models does meet all of these criteria unequivocally. Griebel and Holmes [6] give an extensive review on preclinical models and tests used in anxiety and fear research. Many animal tests and models of anxiety are based on natural behavior patterns in rodents (often rats and mice [42]). Such, often ethologically derived models include “approach-avoidance” tasks [40]. Animals are typically exposed to aversive situations like an open field, elevated plus maze or light/dark box. The level of anxiety is measured by the amount of avoidance of the aversive environment (open area, light). Besides the “unconditioned” procedures, several “conditioned” paradigms are also used to model anxiety disorders, including conflict procedures like the Vogel-lick test, defensive burying, four-plate test, and fear-potentiated startle. Various other paradigms are used to measure anxiety levels including physiological parameters [43], social interaction, predator stress, and stress-induced vocalizations [44]. Over the last decades, several models were introduced to investigate the role of the 5-HTT and adaptive 5-HT signaling in the in vivo action of SSRIs. In a transgenic knock-in mouse model, a single amino acid substitution (M172) in one of the 14-membrane domains led to diminished activity of SSRIs in emotional behavior, although the recognition of 5-HT and its clearance were not affected [45]. 5-HTT-overexpressing mice showed reduced anxiety levels [46, 47] and enhanced 5-HT2A/2C receptor functioning [48]. This 5-HTT-overexpressing model in combination with the effects associated with 5-HTT knockout (5-HTT−/−) mice might shed light on the compensatory effects observed on the life-span but also on those after chronic SSRI administration. 5-HTT−/− mice [49] and rats [50] have been created, and in both genotypes, extracellular 5-HT in the brain is enhanced [14, 51]. These enhanced extracellular 5-HT levels are associated with neurodevelopmental changes in 5-HT synthesis and metabolism [14]. The 5-HTT−/− rodent model has been regarded as a rather extreme example of the human 5-HTTLPR polymorphism, and as such, animals have difficulties to cope with stress and display anxiogenic behavior [52,53,54,55]. Heterozygous 5-HTT knockout rodents (5-HTT+/−) might be seen as a better model for the human 5-HTTPRL model, because the reduced 5-HTT expression is more or less comparable to the expression in human S-allele carriers. 5-HTT+/− animals have reduced 5-HTT expression and function, with 40–50% less 5-HTT protein levels [49, 51]. However, few neurochemical changes are present in 5-HTT+/− rodents compared to wild types (5-HTT+/+) [56]. Several serotonergic parameters, like basal extracellular levels and intracellular 5-HT levels, are not affected [51, 57], although often when challenged, 5-HTT+/− animals differ from 5-HTT+/+ animals [56]. 5-HTT+/− mice did not differ in anxiety levels from 5-HTT+/+ mice in an open field or in novelty-suppressed feeding [58]. There is evidence that the 5-HTT genotype may determine the stress response to the environment, particularly during early life stress (ELS) [56]. It has as yet to be established what mechanisms possibly underlie the 5-HTT gene variation X ELS interaction and specifically how that may lead to enhanced anxiety. Whether the 5-HTT+/− rodent is a good animal model to study the effects of anxiolytic drugs in situations where the animal is challenged toward showing anxiogenic behavior has to be awaited.
In wildtype mice and rats, often measured in different strains, SSRIs display anxiolytic activity [6]. In humans, SSRIs are also the first-line pharmaceutical agents to treat generalized anxiety disorder (GAD), post-traumatic stress disorder (PTSD), panic disorder (PD), and social anxiety disorder (SAD). Although none of the presently available animal anxiety tests and models specifically models for the specific human anxiety disorders, many tests/models have properties that predict for specific aspects present in the various anxiety disorders. Although in the early years (1960s till 1990s) of pharmacological treatment of anxiety disorders, BDZs were often first-line treatment, SSRIs have taken this position later on, mainly due to several safety issues (dependence liability, memory disturbances, tolerance, sedation). In an extensive summary of all published results in animal experiments on various pharmacological targets [6], SSRIs exerted in approx. 40% anxiolytic activity, were ineffective in 40% of the studies, and had 20% anxiogenic activity (in over 400 publications). Similar to human anxiety disorder treatment, the effects in animal tests and models are inconsistent. However, most, if not all, animal experimentation is performed using acute studies, whereas anxiolytic activity of SSRIs in humans occurs after at least 4–6 weeks of chronic treatment. Many patients do not respond to SSRIs, and disturbing side effects such as sexual dysfunction, sometimes associated with an initial transient period of enhanced anxiety, have contributed to a reduced acceptability of SSRIs in daily clinical practice.
In our own research, we mainly concurred with this preclinical anxiolytic profile of SSRIs. In a behavioral paradigm for screening putative anti-panic drugs, SSRIs like fluvoxamine and clomipramine (a TCA with predominant 5-HTT blockade) inhibited conditioned ultrasonic distress vocalizations (USV) in adult male rats [59]. SSRIs were also anxiolytic in guinea pig isolation calls [60], whereas in an approach-avoidance ambivalent situation in rats, SSRIs were inactive [61]. In a mouse model of anticipatory anxiety, stress-induced hyperthermia, antidepressants including SSRIs are inactive [62]. SSRIs are also inactive in the fear-potentiated startle [63]. In an ultrasonic vocalization model in isolated rat pups, SSRIs appeared anxiolytic [64].
The 5-HT1A Receptor and Anxiety
The anxiolytic activity of SSRIs that in some way is caused by the enhanced 5-HT release due to blockade of the 5-HTT must be effectuated by the effects of the released 5-HT on one or more 5-HT receptors; an important candidate is the 5-HT1A receptor (5-HT1AR). Already in 1979 it was found that buspirone, a partial 5-HT1AR agonist (and dopamine D2R antagonist) exerts mild anxiolysis in human anxiety patients, notably in GAD [65]. This could be confirmed in rodent models of anxiety [7, 66]. Clinically, development of new 5-HT1AR agonists for anxiety disorders (e.g., ipsapirone, gepirone, tandospirone, flesinoxan) failed. However, 5-HT1A receptors remain a clinically attractive target implied in anxiety and depression [7, 57, 66,67,68,69]. 5-HT1ARs are inhibitory G-protein-coupled receptors and present as autoreceptors on serotonergic neurons and as heteroreceptors (Fig. 8.1) on non-serotonergic neurons (e.g., GABA-ergic). The somatodendritic 5-HT1A autoreceptors regulate the serotonergic tone via feedback inhibition in concert with the 5-HTT [7]. Postsynaptic 5-HT1A heteroreceptors are abundantly distributed and expressed in the brain although restricted to specific and in high density in limbic areas like hippocampus and various parts of the frontal cortex. Autoreceptors are present in the dorsal and median raphé nuclei. There is evidence from genetic and imaging studies in humans that 5-HT1AR density or regulation is associated with anxiety [70]. A C(−1019)G polymorphism (rs6295) in the promoter region of the 5-HT1AR gene (Htr1a) was associated with mood-related variables like amygdala reactivity [71]. Increased 5-HT1A autoreceptor expression was associated with enrichment of the G-allele; postsynaptically the C-allele was enhanced [72]. In panic disorder with agoraphobia patients [73], variations in the rs6295 polymorphism had functional consequences in defensive behavior, amygdala activity, and neural plasticity, suggesting that differentiation in 5-HT1AR activities plays a role in anxiety and fear.
Griebel and Holmes [6] summarized the effects of 5-HT1AR agonists in animal models of anxiety and fear. Of the 855 studies reported, approx. 65% of 5-HT1AR agonists exerted anxiolytic activity, 30% was inactive and 5% anxiogenic. Moreover, knocking-out (KO) the 5-HT1AR in three mouse strains [74,75,76] led to enhanced anxiety in most standard anxiety tests. This unanimous finding in different labs that inactivation of all 5-HT1AR genes led to more anxious mice is rather striking. Later research found, however, that the anxious phenotype was dependent on the paradigm applied [77, 78] and one strain (but not the other two) of 5-HT1AR KO mice had reduced sensitivity to anxiolytic effects of diazepam, associated with changes in particular α-subunits of the GABAA- benzodiazepines (BDZ) R complex [79]. Apparently, such a dysfunction of the GABAA-BDZ complex is not a prerequisite for the “anxiogenic” phenotype of 5-HT1AR KO mice. The enhanced anxiety in the 5-HT1AR KO mouse could not be antagonized by SSRIs [80]. Moreover, overexpression of 5-HT1ARs reduced anxiety [81]. These data strongly support a role for 5-HT1ARs in anxiety and fear processes. Further research on differential roles of pre- and postsynaptic 5-HT1ARs in anxiety, using rescue experiments on forebrain (postsynaptic) 5-HT1ARs, indicated a critical role for the latter in development of the anxiogenic phenotype [82]. Pharmacological blockade of 5-HT1ARs during early development, but not in adulthood, enhanced anxiety in normal mice [83, 84]. The complex regulation of anxiety processes during development and adulthood again indicates the complexity of the neural substrates, including genetic regulation, environmental influences, and its interactions. Simple relationships between a certain receptor (in this case 5-HT1AR) and the complexity involved in the regulation of anxiety and fear but also its pathology are highly unlikely. However, rodent models (genetic and behavioral) are extremely useful in trying to untangle the different underlying parts and functions.
In our own (preclinical) research, both partial and full 5-HT1AR agonists displayed anxiolytic activity. The azapirones (buspirone, ipsapirone, tandospirone, and zalospirone) are partial 5-HT1AR agonists. Flesinoxan is a potent and selective full 5-HT1AR agonist [66]. 5-HT1AR agonists have limited anxiolytic activity in animal anxiety models based on release of suppressed behavior (both conditioned and unconditioned procedures like Geller-Seifter conflict, Vogel-lick test, four-plate, open field, elevated plus maze, light-dark box and social interaction test). In general 5-HT1AR agonists are very active in animal models of stress-evoked behaviors both in conditioned and unconditioned situations like fear-potentiated startle, shock-induced USV, conditioned USV, defensive burying, stress-induced hyperthermia, rat pup, and guinea pig pup isolation calls [66]. Biased 5-HT1AR agonists [85, 86] display either selectivity for 5-HT1A autoreceptors (F13714) or 5-HT1A heteroreceptors (F15599). However, both compounds had anxiolytic activity in several anxiety tests [87], not solving a potential role distribution between pre- and postsynaptic 5-HT1ARs in anxiety, although evidence is gathering that postsynaptic 5-HT1ARs, e.g., in the prelimbic cortex [88], may play a conclusive role.
Buspirone is worldwide marketed as anxiolytic, whereas tandospirone is only available in Japan and China. Flesinoxan was tested in phase III clinical trials as a potential anxiolytic (and antidepressant), but did not show superior activity compared to placebo and was subsequently abandoned. Although buspirone (and to a lesser extent tandospirone) are clinically effective anxiolytics, 5-HT1AR agonists have not emerged as a breakthrough and successor of BDZ in the treatment of anxiety disorders.
Other 5-HT Receptors and Anxiety
Agonists and antagonists for practically all 5-HT receptors have been synthetized over the last 30 years and subsequently also tested in (mostly simple) anxiety tests. Griebel and Holmes [6] summarize results on frequently tested compounds, including 5-HT2R antagonists, 5-HT3R antagonists, and others. In 314 experiments 5-HT2R antagonists were around 43% anxiolytic and 5-HT3R antagonists (232 experiments) in 65%. Źmudzka et al. [87] essentially confirmed these data on 5-HT receptors and anxiety. Although in the 1990s the 5-HT3R antagonists were considered the anxiolytics of the future based on animal results, they did not confirm their anxiolytic profile in human anxiety disorders [89]. Thus far, no promising new serotonin receptor ligands have been introduced to the market as new anxiolytics.
GABAA Receptors (GABAAR) and Anxiety
GABAA (γ-aminobutyric acid, type A) receptors are the molecular targets of BDZ, chemical structures that were serendipitously found in the 1950s and were developed as the main anxiolytics of the ensuing decades. Besides anxiolysis, the classical BDZs also exerted sedation, epileptic seizure suppression, muscle relaxation, and hypnotic effects [90]. It took over 20 years before the molecular target of the BDZ, the GABAA receptor (GABAAR) was discovered [91]. The GABAAR is the target of clinically important anxiolytics, including BDZ, and is an ionotropic inhibitory receptor [90]. Although BDZs are excellent anxiolytics both in man and animals and are very safe in overdosing, it was realized that long-term use carries risks of tolerance, physical and psychological dependence, and withdrawal signs after discontinuation. Moreover, adverse side effects of sedation and cognitive slowing were found [92]. As a consequence, the SSRIs (and to a lesser extent the SNRIs) are now the first-line pharmacological treatment option for many anxiety disorders, whereas the BDZs are prescribed as second- or third-line treatment if antidepressants are ineffective and cognitive behavioral therapy has failed [4]. Notwithstanding the reluctance to prescribe BDZs, its use is still high in many countries; more than 5% of adults in the USA are prescribed BDZ each year [93].
Ionotropic GABAARs are ubiquitous in the brain and are crucial in the temporal precise activity of neuronal circuitry and synchronized oscillatory activity of neuronal populations [94]. The diversity of this inhibitory neurotransmission regulating these networks is on one side regulated by the large variety in interneurons but also by the extremely diverse group of GABA receptors on the receiving side. GABAR consist of five subunits that surround a central pore in a pentameric composition (Fig. 8.4). When the endogenous ligand (GABA) binds to the GABAR, chloride ions flow into the neuron, leading to hyperpolarization of the cell membrane and inhibition of cell firing. GABAAR are synaptically and extrasynaptically localized and molecularly very heterogeneous via variable subunit composition (Fig. 8.4). This heterogeneity determines the physiological/pharmacological properties [90, 95]. The various subunits (α1-6; β1-3; γ1-3; δ, ε, θ, and ρ1-3) make up, although not randomly, the GABAAR. Most GABAARs are composed of two α, two β, and one γ subunit. GABA binds to the GABA site, which is formed by α and β subunits, and the BDZ binding site by one of the α subunits (α1, 2, 3, or 5) and a γ2 subunit. Circa 60% of GABAARs are of the α1β2γ2 subtype, 15–20% of α2β3γ2, 10–15% of α3βnγ2; the rest has variable subunit composition [96].

Schematic picture of the GABAA receptor. A shows a global picture of the 2 α, the 2 β, and the γ subunits and the direction of the chloride influx. Fig. 1B shows a top view with the subunits arranged around a central pore, the chloride channel. The GABA and BDZ binding sites are indicated. (Figure adapted from Vinkers and Olivier [104])
GABAAR subtype selective compounds and mouse models with subunit point mutations have generated promising insight in the contribution of the different subunits in the different clinical effects of BDZ [90]. BDZ do not open the chloride channel in absence of the endogenous ligand GABA. Different pharmacological agents act at different GABAAR sites, including GABA itself and various GABAAR agonists (e.g., muscimol) or antagonists (e.g., bicuculline). Classical BDZ (e.g., chlordiazepoxide and diazepam) binds to the GABAA-BDZ modulatory site. Other drug classes, including alcohol, barbiturates, and neurosteroids, also bind to the GABAAR. The allosteric binding site for BDZ is always formed by two α-subunits (α1, 2, 3, or 5), two β-subunits, and the γ2 subunit. Only if the GABA receptor is activated, stimulation of the BDZ site modulates the channel opening (frequency and/or time). Ligands at the BDZ binding site are allosteric modulators and modify the efficacy and/or the affinity of GABA in a positive way (positive allosteric modification-PAM), negative way (NAM), or not (neutral), by stabilizing different three-dimensional conformations of the GABAAR complex. The potency of a certain ligand is determined by its specificity for a certain receptor subtype and affinity/efficacy modulation [97]. BDZ have anxiolytic, sedative, hypnotic, muscle-relaxant, and anticonvulsant properties. If anxiolysis is the primary indication, sedative-hypnotic properties are unwanted. Classic BDZ are nonselectively activating α1,2,3, and 5 subunits and bring automatically these unwanted effects. Extensive research, mainly in genetically engineered mice where certain GABAARα subunits (GABRA) were made insensitive to diazepam binding, leaving the GABA site intact, illustrated that different subunits represent different functions. The broad therapeutic (and side) effects of BDZ are due to activation of α-subunits [90, 98]. Extensive preclinical work implicated α2 and α3 subunits in the modulation of anxiety, but intensive efforts (partial agonists, inverse agonists) have not yielded new and highly specific anxiolytics. Moreover, the main negative effects of all GABAAR agonistic ligands (PAMs), i.e., tolerance and addiction, are still present in these new ligands [99], and none of these drugs has advanced to the market. A big outstanding question is whether activation of all α-subunits leads to tolerance/addiction or activation of only one specific subunit [100]. Also the once promising development of the so-called Z-drugs (zolpidem, zaleplon, and zopiclone) did not yield anxiolytics without tolerance/dependence problems. Interestingly, pregabalin, a structural analogue of GABA, is anxiolytic, although via a non-BDZ-like mechanism. Pregabalin is approved in 2007 for anxiety disorders in the EU, but not in the USA [101]. There is some evidence that activation of α1-subunits is essential in the addictive potential of BDZ ligands [102, 103], but processes underlying tolerance development are complex and endpoint-dependent [104]. All these failures have probably been a major reason why pharmaceutical companies have left the development of innovative drugs for anxiety disorders that target the GABAAR-BDZ complex.
Other Mechanisms and Anxiety
Although only preclinically investigated, many pharmacological mechanisms seem to be involved in the modulation of anxiety and fear, and intense efforts have tried to find new mechanisms outside the GABAAR-BDZ complex and the serotonergic system; no new clinically effective drugs have emerged thus far. The situation since 2012 (described by Griebel and Holmes [6]) has not changed. Still most preclinical drug discovery is focused on neuropeptides and glutamate targets. Preclinically, CRF1R antagonists, CCK2R antagonists, and neurokinin1,2R antagonists have anxiolytic-like activity, but no clinically successful drugs have emerged [6]. Several findings strongly implicated the glutamatergic system in anxiety and anxiety disorders [105]. Glutamate neurotransmission is complex due to the large number of signaling receptors and the wide and diverse distribution in the CNS. Metabotropic glutamate receptors (mGluRs) play a role in the modulation of anxiety in preclinical studies. Various ligands for mGluR subtype receptors have been tested clinically but failed to reach the market. Ketamine was recently found to have anxiolytic activity in social anxiety disorder [106] and refractory anxiety disorder patients [107] but also in animal anxiety models [108]. Ketamine, an NMDA (N-methyl-D-aspartate) R antagonist, exerts a rapid onset of antidepressant action in depressed patients and is particularly effective in anxious depression [109]. Most clinical studies utilize intravenous ketamine administration, which is a severe limitation for therapeutic use. Moreover, ketamine has serious side effects and abuse potential, which limits its widespread use as rapid onset therapeutic [110]. Further research into the efficacy of one of the enantiomers of ketamine (R,S) or one of its metabolites (e.g., 2R,6R)-hydroxynorketamine [111, 112]) may lead to a new, fast-acting anxiolytic (and antidepressant) treatment.
Conclusions
Discovery and development of innovative anxiolytics is severely hampering. Existing anxiolytics are developed decades ago and are still the therapeutics of choice. Moreover, the lack of new effective drug targets is not only disappointing but does indicate how the future treatment of the enormous population of CNS-disorder patients is in jeopardy. The reasons for this lack of progress are manyfold and are, besides, e.g., regulatory, financial, and marketing reasons, also due to our limited knowledge of the mechanisms and pathophysiology of the various anxiety disorders. We simply lack the knowledge on what is wrong in the brains of anxious people (normal and disordered). It is also not clear yet whether DSM5-based anxiety disorder classification is justifying the underlying disturbed processes in the brain. Whether the new classification of psychiatric diseases, the Research Domain Criteria (RDoC) project, as part of the 2008 NIMH strategic plan’s call for new ways of classifying mental illnesses—based on dimensions of observable behavior and neurobiological measures—will be helpful in the research process has to be awaited. Translational research, with exchanging theories and data coming from clinical and preclinical research, is extremely urgent, because intrusive investigations of the human brain are impossible. In this endeavor, genetic and genomic approaches are part of the spectrum of contributing factors. The initial idea of identifying individual genes causing the disease very soon appeared an illusion. It becomes increasingly clear that anxiety disorders, probably similar to the fundamental mechanisms involved in anxiety and fear processes in the brain, are caused by the (inter)actions of hundreds of genes including environmental factors (epigenesis) and gene X gene interactions. In the present contribution, main focus has been on three druggable targets, 5-HTT, 5-HT1A receptor, and GABAA receptor, whereas other approaches have been summarized. Although the therapeutics, acting via these targets were found before the mechanisms involved were unraveled, it is still uncertain whether or how these targets are involved in normal and diseased anxiety processes. In case of the serotonergic anxiolytics, the slow onset of action points to indirect effects leading to plasticity changes in certain systems in the brain that finally lead to reduced anxiety. In case of the GABAA receptors, a direct anxiolytic effect is found which indicates primary mechanisms directly influencing anxiety processes. Close translational collaboration between fundamental academic and discovery research might lead to badly needed breakthroughs in the development of drugs, not only for anxiety disorders but also other brain diseases.
References
Wittchen HU, Jacobi F. Size and burden of mental disorders in Europe – a critical review and appraisal of 27 studies. Eur Neuropsychopharmacol. 2005 Aug;15(4):357–76.
Kessler RC, Ruscio AM, Shear K, Wittchen HU. Epidemiology of anxiety disorders. Curr Top Behav Neurosci. 2010;2:21–35.
Ressler KJ, Mayberg HS. Targeting abnormal neural circuits in mood and anxiety disorders: from the laboratory to the clinic. Nat Neurosci. 2007 Sep;10(9):1116–24.
Stein MB, Craske MG. Treating anxiety In 2017: optimizing care to improve outcomes. JAMA. 2017 Jul 18;318(3):235–6.
Cryan JF, Sweeney FF. The age of anxiety: role of animal models of anxiolytic action in drug discovery. Br J Pharmacol. 2011 Oct;164(4):1129–61.
Griebel G, Holmes A. 50 years of hurdles and hope in anxiolytic drug discovery. Nat Rev Drug Discov. 2013 Sep;12(9):667–87.
Olivier B. Serotonin: a never-ending story. Eur J Pharmacol. 2015 Apr 15;753:2–18.
Locher C, Koechlin H, Sr Z, Werner C, Pine DS, Kirsch I, Et A. Efficacy and safety of selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and placebo for common psychiatric disorders among children and adolescents: a systematic review and meta-analysis. JAMA Psychiatry. 2017 Oct 1;74(10):1011–20.
Janiaud P, Cornu C, Lajoinie A, Djemli A, Cucherat M, Kassai BI. The perceived placebo effect comparable between adults and children? A meta-regression analysis. Pediatr Res. 2017 Jan;81(1–1):11–7.
Gottschalk MG, Domschke K. Genetics of generalized anxiety disorder and related traits. Dialogues Clin Neurosci. 2017 Jun;19(2):159–68.
Okbay A, Baselmans BM, De Neve JE, Turley P, Nivard MG, Fontana MA, et al. Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat Genet. 2016 Jun;48(6):624–33.
Kas MJ, Krishnan V, Gould TD, Collier DA, Olivier B, Lesch KP, et al. Advances in multidisciplinary and cross-species approaches to examine the neurobiology of psychiatric disorders. Eur Neuropsychopharmacol. 2011 Jul;21(7):532–44.
Lesch KP. Molecular foundation of anxiety disorders. J Neural Transm. 2001;108(6):717–46.
Murphy DL, Lesch KP. Targeting the murine serotonin transporter: insights into human neurobiology. Nat Rev Neurosci. 2008 Feb;9(2):85–96.
Teissier A, Soiza-Reilly M, Gaspar P. Refining the role of 5-Ht In postnatal development of brain circuits. Front Cell Neurosci. 2017;11:139.
Marin O. Developmental timing and critical windows for the treatment of psychiatric disorders. Nat Med. 2016 Nov;22(11):1229–38.
Suri D, Teixeira CM, Cagliostro MK, Mahadevia D, Ansorge MS. Monoamine-sensitive developmental periods impacting adult emotional and cognitive behaviors. Neuropsychopharmacology. 2015 Jan;40(1):88–112.
Caspi A, Sugden K, Moffitt TE, Taylor A, Craig IW, Harrington H, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science. 2003 Jul 18;301(5631):386–9.
Lesch KP, Bengel D, Heils A, Sabol SZ, Greenberg BD, Petri S, et al. Association of anxiety-related traits with a polymorphism in the serotonin transporter gene regulatory region. Science. 1996 Nov 29;274(5292):1527–31.
Haddley K, Bubb VJ, Breen G, Parades-Esquivel UM, Quinn JP. Behavioural genetics of the serotonin transporter. Curr Top Behav Neurosci. 2012 Jan 20;12:503–35.
Zhu J, Klein-Fedyshin M, Stevenson JM. Serotonin transporter gene polymorphisms and selective serotonin reuptake inhibitor tolerability: review of Pharmacogenetic evidence. Pharmacotherapy. 2017 Sep;37(9):1089–104.
Iurescia S, Seripa D, Rinaldi M. Role of the 5-HTTPRL and Snp promoter polymorphisms on serotonin transporter gene expression: a closer look at genetic architecture and in vitro functional studies of common and uncommon allelic variants. Mol Neurobiol. 2016 Oct;53(8):5510–26.
Murrough JW, Charney DS. The serotonin transporter and emotionality: risk, resilience, and new therapeutic opportunities. Biol Psychiatry. 2011 Mar 15;69(6):510–2.
Drabant EM, Ramel W, Edge MD, Hyde LW, Kuo JR, Goldin PR, et al. Neural mechanisms underlying 5-HTTPRL-related sensitivity to acute stress. Am J Psychiatry. 2012 Apr;169(4):397–405.
Montag C, Fiebach CJ, Kirsch P, Reuter M. Interaction of 5-HTTPRL and a variation on the oxytocin receptor gene influences negative emotionality. Biol Psychiatry. 2011 Mar 15;69(6):601–3.
Pluess M, Velders FP, Belsky J, Van Ijzendoorn MH, Bakermans-Kranenburg MJ, Jaddoe VW, et al. Serotonin transporter polymorphism moderates effects of prenatal maternal anxiety on infant negative emotionality. Biol Psychiatry. 2011 Mar 15;69(6):520–5.
Stollstorff M, Bean SE, Anderson LM, Devaney JM, Vaidya CJ. Rationality and emotionality: serotonin transporter genotype influences reasoning Bias. Soc Cogn Affect Neurosci. 2012 Mar 5;8(4):404–9.
Caspi A, Hariri AR, Holmes A, Uher R, Moffitt TE. Genetic sensitivity to the environment: the case of the serotonin transporter gene and its implications for studying complex diseases and traits. Am J Psychiatry. 2010 May;167(5):509–27.
Glenn AL. The other Allele: exploring the long allele of the serotonin transporter gene as a potential risk factor for psychopathy: a review of the parallels in findings. Neurosci Biobehav Rev. 2011 Jan;35(3):612–20.
Belsky J, Jonassaint C, Pluess M, Stanton M, Brummett B, Williams R. Vulnerability genes or plasticity genes? Mol Psychiatry. 2009 Aug;14(8):746–54.
Homberg JR, Lesch KP. Looking on the bright side of serotonin transporter gene variation. Biol Psychiatry. 2011 Mar 15;69(6):513–9.
Stein MB, Campbell-Sills L, Gelernter J. Genetic variation In 5-HTTPRL is associated with emotional resilience. Am J Med Genet B Neuropsychiatr Genet. 2009 Oct 5;150b(7):900–6.
Gatt JM, Burton KL, Williams LM, Schofield PR. Specific and common genes implicated across major mental disorders: a review of meta-analysis studies. J Psychiatr Res. 2015 Jan;60:1–13.
Smoller JW, Block SR, Young MM. Genetics of anxiety disorders: The complex road from Dsm To Dna. Depress Anxiety. 2009;26(11):965–75.
Fernando AB, Robbins TW. Animal models of neuropsychiatric disorders. Annu Rev Clin Psychol. 2011 Apr;7:39–61.
Flint J, Shifman S. Animal models of psychiatric disease. Curr Opin Genet Dev. 2008 Jun;18(3):235–40.
Tye KM, Deisseroth K. Optogenetic investigation of neural circuits underlying brain disease in animal models. Nat Rev Neurosci. 2012 Apr;13(4):251–66.
Walters BJ, Azam AB, Gillon CJ, Josselyn SA, Zovkic IB. Advanced in vivo use of Crispr/Cas9 and anti-sense Dna inhibition for gene manipulation in the brain. Front Genet. 2015;6:362.
Belzung C, Lemoine M. Criteria of validity for animal models of psychiatric disorders: focus on anxiety disorders and depression. Biol Mood Anxiety Disord. 2011 Nov 7;1(1):9.
Cryan JF, Holmes A. The ascent of mouse: advances in modelling human depression and anxiety. Nat Rev Drug Discov. 2005 Sep;4(9):775–90.
Haller J, Aliczki M, Gyimesine PK. Classical and novel approaches to the preclinical testing of anxiolytics: a critical evaluation. Neurosci Biobehav Rev. 2013 Dec;37(10 Pt 1):2318–30.
Rodgers R. Animal models of ‘anxiety’: where next? Behav Pharmacol. 1997 Nov;8(6–7):477–96.
Bouwknecht JA, Olivier B, Paylor RE. The stress-induced hyperthermia paradigm as a physiological animal model for anxiety: a review of pharmacological and genetic studies in the mouse. Neurosci Biobehav Rev. 2007;31(1):41–59.
Olivier B, Zethof T, Pattij T, Van Boogaert M, Van Oorschot R, Leahy C, et al. Stress-induced hyperthermia and anxiety: pharmacological validation. Eur J Pharmacol. 2003 Feb 28;463(1–3):117–32.
Thompson BJ, Jessen T, Henry LK, Field JR, Gamble KL, Gresch PJ, et al. Transgenic elimination of high-affinity antidepressant and cocaine sensitivity in the presynaptic serotonin transporter. Proc Natl Acad Sci USA. 2011 Mar 1;108(9):3785–90.
Jennings KA, Loder MK, Sheward WJ, Pei Q, Deacon RM, Benson MA, et al. Increased expression of the 5-HT transporter confers a low-anxiety phenotype linked to decreased 5-HT transmission. J Neurosci. 2006 Aug 30;26(35):8955–64.
Line SJ, Barkus C, Rawlings N, Jennings K, Mchugh S, Sharp T, et al. Reduced sensitivity to both positive and negative reinforcement in mice over-expressing the 5-hydroxytryptamine transporter. Eur J Neurosci. 2014 Dec;40(12):3735–45.
Dawson N, Ferrington L, Lesch KP, Kelly PA. Cerebral metabolic responses to 5-HT2A/C receptor activation in mice with genetically modified serotonin transporter (Sert) expression. Eur Neuropsychopharmacol. 2011 Jan;21(1):117–28.
Bengel D, Murphy DL, Andrews AM, Wichems CH, Feltner D, Heils A, et al. Altered brain serotonin homeostasis and locomotor insensitivity to 3, 4-Methylenedioxymethamphetamine (“Ecstasy”) in serotonin transporter-deficient mice. Mol Pharmacol. 1998 Apr;53(4):649–55.
Smits BM, Mudde JB, Van De Belt J, Verheul M, Olivier J, Homberg J, et al. Generation of gene knockouts and mutant models in the laboratory rat by Enu-driven target-selected mutagenesis. Pharmacogenet Genomics. 2006 Mar;16(3):159–69.
Homberg JR, Olivier JD, Smits BM, Mul JD, Mudde J, Verheul M, et al. Characterization of the serotonin transporter knockout rat: a selective change in the functioning of the serotonergic system. Neuroscience. 2007 Apr 27;146(4):1662–76.
Adamec R, Burton P, Blundell J, Murphy DL, Holmes A. Vulnerability to mild predator stress in serotonin transporter knockout mice. Behav Brain Res. 2006 Jun 3;170(1):126–40.
Kalueff AV, Olivier JD, Nonkes LJ, Homberg JR. Conserved role for the serotonin transporter gene in rat and mouse neurobehavioral endophenotypes. Neurosci Biobehav Rev. 2010;34(3):373–86.
Olivier JD, Van Der Hart MG, Van Swelm RP, Dederen PJ, Homberg JR, Cremers T, et al. A study in male and female 5-HT transporter knockout rats: an animal model for anxiety and depression disorders. Neuroscience. 2008 Mar 27;152(3):573–84.
Wellman CL, Izquierdo A, Garrett JE, Martin KP, Carroll J, Millstein R, et al. Impaired stress-coping and fear extinction and abnormal corticolimbic morphology in serotonin transporter knock-out mice. J Neurosci. 2007 Jan 17;27(3):684–91.
Houwing DJ, Buwalda B, Van Der Zee EA, De Boer SF, Olivier JDA. The serotonin transporter and early life stress: translational perspectives. Front Cell Neurosci. 2017;11:117.
Holmes A, Li Q, Murphy DL, Gold E, Crawley JN. Abnormal anxiety-related behavior in serotonin transporter null mutant mice: the influence of genetic background. Genes Brain Behav. 2003 Dec;2(6):365–80.
Muller JM, Morelli E, Ansorge M, Gingrich JA. Serotonin transporter deficient mice are vulnerable to escape deficits following inescapable shocks. Genes Brain Behav. 2011 Mar;10(2):166–75.
Molewijk HE, Van Der Poel AM, Mos J, Van Der Heyden JA, Olivier B. Conditioned ultrasonic distress vocalizations in adult male rats as a behavioural paradigm for screening anti-panic drugs. Psychopharmacology (Berl). 1995 Jan;117(1):32–40.
Molewijk HE, Hartog K, Van Der Poel AM, Mos J, Olivier B. Reduction of guinea pig pup isolation calls by anxiolytic and antidepressant drugs. Psychopharmacology (Berl). 1996 Nov;128(1):31–8.
Molewijk HE, Van Der Poel AM, Olivier B. The ambivalent behaviour “stretched approach posture” in the rat as a paradigm to characterize anxiolytic drugs. Psychopharmacology (Berl). 1995 Sep;121(1):81–90.
Zethof TJ, Van Der Heyden JA, Tolboom JT, Olivier B. Stress-induced hyperthermia as a putative anxiety model. Eur J Pharmacol. 1995 Dec 27;294(1):125–35.
Joordens RJ, Hijzen TH, Peeters BW, Olivier B. Fear-potentiated startle response is remarkably similar in two laboratories. Psychopharmacology (Berl). 1996 Jul;126(2):104–9.
Olivier B, Molewijk HE, Van Der Heyden JA, Van Oorschot R, Ronken E, Mos J, et al. Ultrasonic vocalizations in rat pups: effects of serotonergic ligands. Neurosci Biobehav Rev. 1998;23(2):215–27.
Goldberg HL, Finnerty RJ. The comparative efficacy of buspirone and diazepam in the treatment of anxiety. Am J Psychiatry. 1979 Sep;136(9):1184–7.
Olivier B, Soudijn W, van Wijngaarden I. The 5-HT1A receptor and its ligands: structure and function. Prog Drug Res. 1999;52:103–65.
Akimova E, Lanzenberger R, Kasper S. The serotonin-1a receptor in anxiety disorders. Biol Psychiatry. 2009 Oct 1;66(7):627–35.
Lanfumey L, Mongeau R, Cohen-Salmon C, Hamon M. Corticosteroid-serotonin interactions in the neurobiological mechanisms of stress-related disorders. Neurosci Biobehav Rev. 2008 Aug;32(6):1174–84.
Savitz J, Lucki I, Drevets WC. 5-HT(1a) receptor function in major depressive disorder. Prog Neurobiol. 2009 May;88(1):17–31.
Lesch KP, Gutknecht L. Focus on the 5-HT1A receptor: emerging role of a gene regulatory variant in psychopathology and pharmacogenetics. Int J Neuropsychopharmacol. 2004 Dec;7(4):381–5.
Fakra E, Hyde LW, Gorka A, Fisher PM, Munoz KE, Kimak M, et al. Effects of Htr1a C(-1019)G on amygdala reactivity and trait anxiety. Arch Gen Psychiatry. 2009 Jan;66(1):33–40.
Le François B, Czesak M, Steubl D, Albert PR. Transcriptional regulation at a Htr1a polymorphism associated with mental illness. Neuropharmacology. 2008 Nov;55(6):977–85.
Straube B, Reif A, Richter J, Lueken U, Weber H, Arolt V, et al. The functional -1019c/G Htr1a polymorphism and mechanisms of fear. Transl Psychiatry. 2014 Dec 16;4:E490.
Heisler LK, Chu HM, Brennan TJ, Danao JA, Bajwa P, Parsons LH, et al. Elevated anxiety and antidepressant-like responses in serotonin 5-HT1A receptor mutant mice. Proc Natl Acad Sci USA. 1998 Dec 8;95(25):15049–54.
Parks CL, Robinson PS, Sibille E, Shenk T, Toth M. Increased anxiety of mice lacking the Serotonin1a receptor. Proc Natl Acad Sci USA. 1998 Sep 1;95(18):10734–9.
Ramboz S, Oosting R, Amara DA, Kung HF, Blier P, Mendelsohn M, et al. Serotonin receptor 1a knockout: an animal model of anxiety-related disorder. Proc Natl Acad Sci USA. 1998 Nov;95(24):14476–81.
Pattij T, Hijzen TH, Groenink L, Oosting RS, Van Der Gugten J, Maes RA, et al. Stress-induced hyperthermia in the 5-HT1A receptor knockout mouse is normal. Biol Psychiatry. 2001 Apr 1;49(7):569–74.
Van Bogaert MJ, Oosting R, Toth M, Groenink L, Van Oorschot R, Olivier B. Effects of genetic background and null mutation of 5-HT1A receptors on basal and stress-induced body temperature: modulation by serotonergic and Gabaa-Ergic drugs. Eur J Pharmacol. 2006;550(1–3):84–90.
Sibille E, Pavlides C, Benke D, Toth M. Genetic inactivation of the serotonin(1a) receptor in mice results in downregulation of major GABA(A) receptor alpha subunits, reduction of GABA(A) receptor binding, and benzodiazepine-resistant anxiety. J Neurosci. 2000 Apr 15;20(8):2758–65.
Santarelli L, Saxe M, Gross C, Surget A, Battaglia F, Dulawa S, et al. Requirement of hippocampal neurogenesis for the behavioral effects of antidepressants. Science. 2003 Aug 8;301(5634):805–9.
Kusserow H, Davies B, Hortnagl H, Voigt I, Stroh T, Bert B, et al. Reduced anxiety-related behaviour in transgenic mice overexpressing serotonin 1a receptors. Brain Res Mol Brain Res. 2004 Oct 22;129(1–2):104–16.
Gross C, Zhuang X, Stark K, Ramboz S, Oosting R, Kirby L, et al. Serotonin1a receptor acts during development to establish normal anxiety-like behaviour in the adult. Nature. 2002 Mar 28;416(6879):396–400.
Lo Iacono L, Gross C. Alpha-Ca2+/Calmodulin-dependent protein kinase Ii contributes to the developmental programming of anxiety in serotonin receptor 1a knock-out mice. J Neurosci. 2008 Jun 11;28(24):6250–7.
Vinkers CH, Oosting RS, Van Bogaert MJ, Olivier B, Groenink L. Early-life blockade of 5-HT1A receptors alters adult anxiety behaviour and benzodiazepine sensitivity. Biol Psychiatry. 2010;67(4):309–16.
Assié MB, Bardin L, Auclair AL, Carilla-Durand E, Depoortere R, Koek W, et al. F15599, a highly selective post-synaptic 5-HT(1a) receptor agonist: in-vivo profile in behavioural models of antidepressant and serotonergic activity. Int J Neuropsychopharmacol. 2010 Nov;13(10):1285–98.
Newman-Tancredi A. Biased agonism at serotonin 5-HT1A receptors: preferential postsynaptic activity for improved therapy of Cns disorders. Neuropsychiatry. 2011;1(2):149–64.
Żmudzka E, Salaciak K, Sapa J, Pytka K. Serotonin receptors in depression and anxiety: insights from animal studies. Life Sci. 2018 Oct 1;210:106–24.
Yamashita PS, Rosa DS, Lowry CA, Zangrossi H Jr. Serotonin actions within the prelimbic cortex induce anxiolysis mediated by serotonin 1a receptors. J Psychopharmacol. 2018 Dec 19:269881118817384.
Olivier B, van Wijngaarden I, Soudijn W. 5-HT(3) receptor antagonists and anxiety; a preclinical and clinical review. Eur Neuropsychopharmacol. 2000 Mar;10(2):77–95.
Rudolph U, Knoflach F. Beyond classical benzodiazepines: novel therapeutic potential of GABA(A) receptor subtypes. Nat Rev Drug Discov. 2011;10(9):685–97.
Möhler H, Okada T. Benzodiazepine receptor: demonstration in the central nervous system. Science. 1977 Nov 25;198(4319):849–51.
Lader M. benzodiazepines revisited--will we ever learn? Addiction. 2011 Dec;106(12):2086–109.
Olfson M, King M, Schoenbaum M. Benzodiazepine use in the United States. JAMA Psychiatry. 2015 Feb;72(2):136–42.
Engin E, Benham RS, Rudolph U. An emerging circuit pharmacology of GABAA receptors. Trends Pharmacol Sci. 2018 Aug;39(8):710–32.
Sigel E, Ernst M. The benzodiazepine binding sites of GABAA receptors. Trends Pharmacol Sci. 2018 Jul;39(7):659–71.
Möhler H, Fritschy JM, Rudolph U. A new benzodiazepine pharmacology. J Pharmacol Exp Ther. 2002 Jan;300(1):2–8.
Farb DH, Ratner MH. Targeting the modulation of neural circuitry for the treatment of anxiety disorders. Pharmacol Rev. 2014 Oct;66(4):1002–32.
Möhler H. GABAA receptors in central nervous system disease: anxiety, epilepsy, and insomnia. J Recept Signal Transduct Res. 2006;26(5–6):731–40.
Cheng T, Wallace DM, Ponteri B, Tuli M. Valium without dependence? Individual GAABAA receptor subtype contribution toward benzodiazepine addiction, tolerance, and therapeutic effects. Neuropsychiatr Dis Treat. 2018;14:1351–61.
Vinkers CH, Van Oorschot R, Nielsen EO, Cook JM, Hansen HH, Groenink L, et al. GABA(A) receptor alpha subunits differentially contribute to diazepam tolerance after chronic treatment. Plos One. 2012;7(8):E43054.
Millan MJ, Goodwin GM, Meyer-Lindenberg A, Ove OS. Learning from the past and looking to the future: emerging perspectives for improving the treatment of psychiatric disorders. Eur Neuropsychopharmacol. 2015 May;25(5):599–656.
Tan KR, Brown M, Labouebe G, Yvon C, Creton C, Fritschy JM, et al. Neural bases for addictive properties of benzodiazepines. Nature. 2010 Feb 11;463(7282):769–74.
Tan KR, Rudolph U, Luscher C. Hooked on benzodiazepines: GAABA receptor subtypes and addiction. Trends Neurosci. 2011 Apr;34(4):188–97.
Vinkers CH, Olivier B. Mechanisms underlying tolerance after long-term benzodiazepine use: a future for subtype-selective GABA(A) receptor modulators? Adv Pharmacol Sci. 2012;2012:416864.
Krystal JH, Mathew SJ, D’souza DC, Garakani A, Gunduz-Bruce H, Charney DS. Potential psychiatric applications of metabotropic glutamate receptor agonists and antagonists. Cns Drugs. 2010 Aug;24(8):669–93.
Taylor JH, Landeros-Weisenberger A, Coughlin C, Mulqueen J, Johnson JA, Gabriel D, et al. Ketamine for social anxiety disorder: a randomized, placebo-controlled crossover trial. Neuropsychopharmacology. 2018 Jan;43(2):325–33.
Glue P, Medlicott NJ, Harland S, Neehoff S, Anderson-Fahey B, Le NM, et al. Ketamine’s dose-related effects on anxiety symptoms in patients with treatment refractory anxiety disorders. J Psychopharmacol. 2017 Oct;31(10):1302–5.
Fraga DB, Olescowicz G, Moretti M, Siteneski A, Tavares MK, Azevedo D, et al. Anxiolytic effects of ascorbic acid and ketamine in mice. J Psychiatr Res. 2018 May;100:16–23.
Ionescu DF, Niciu MJ, Richards EM, Zarate CA Jr. Pharmacologic treatment of dimensional anxious depression: a review. Prim Care Companion Cns Disord. 2014;16(3)
Sanacora G, Frye MA, Mcdonald W, Mathew SJ, Turner MS, Schatzberg AF, et al. A consensus statement on the use of ketamine in the treatment of mood disorders. JAMA Psychiatry. 2017 Apr 1;74(4):399–405.
Highland JN, Morris PJ, Zanos P, Lovett J, Ghosh S, Wang AQ, et al. Mouse, rat, and dog bioavailability and mouse oral antidepressant efficacy of (2r,6r)-hydroxynorketamine. J Psychopharmacol. In Press. 2018;
Zhang K, Hashimoto K. An update on ketamine and its two enantiomers as rapid-acting antidepressants. Expert Rev Neurother. 2018 Dec;4:1–10.
Vinkers CH, Olivier B, Bouwknecht JA, Groenink L, Olivier JDA. Stress-induced hyperthermia, the serotonin system and anxiety. Open Pharmacol J. 2010;4:15–29.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Olivier, J.D.A., Olivier, B. (2020). Translational Studies in the Complex Role of Neurotransmitter Systems in Anxiety and Anxiety Disorders. In: Kim, YK. (eds) Anxiety Disorders. Advances in Experimental Medicine and Biology, vol 1191. Springer, Singapore. https://doi.org/10.1007/978-981-32-9705-0_8
Download citation
DOI: https://doi.org/10.1007/978-981-32-9705-0_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-32-9704-3
Online ISBN: 978-981-32-9705-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)