
Abstract
It has been almost a decade since the hypothesis of active tau protein propagation in Alzheimer’s disease and associated tauopathies was formally raised. We view tau propagation as a cascade of events, starting with early tau misfolding, followed by transfer to another, anatomically connected, cell, contaminating in corruption of endogenous tau in the recipient cell through a seeding mechanism of templated misfolding. These mechanisms are very similar to those of other proteinopathies and to ideas about how prion pathologies spread through the brain. Nonetheless, the specific mechanisms underlying each of these steps remains uncertain and is a fertile ground for new experimental approaches potentially requiring new experimental models. We review, here, the state of the art of the research on tau prion-like propagation and we highlight some key challenges to understanding the detailed mechanisms of cell to cell propagation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Tau Prion-Like Propagation, State of the Art
In Alzheimer’s disease, tau deposition generally starts in the entorhinal cortex and then, following neuronal connections, progresses through the hippocampus, the limbic and association cortices (Fig. 23.1a) [7, 12, 13, 26, 33]. This stereotypical “staging scheme” was recently confirmed by tau PET scan studies [60, 71, 131, 132] and strongly correlates with cognitive decline [51]. Interestingly, although affecting different circuits, similar progression patterns through connected neuronal circuits have been identified in other tauopathies including Progressive Supranuclear Palsy (PSP) (Fig. 23.1b) [149, 155], Argyrophilic grain disease (Fig. 23.1c) [126], or more recently Pick’s disease [67].

Staging in tauopathies. Progressive appearance of tau pathology lesions in the brain of AD (a), PSP (b) and Argyrophilic grain disease (c). Light purple, purple and red respectively represents a small, moderate orFig. 23.1 (continued) severe amount tau pathology in the affected brain region. (a) In Alzheimer’s disease, tau deposition generally starts in the entorhinal cortex and then, following neuronal connections, progresses through the hippocampus, the limbic and association cortices (sketch inspired by Braak and Del Tredici [13]). (b) In PSP, tau deposition progresses from the system pallidus – subthalamic nucleus – substantia nigra to the pedonculopontine nucleus and premotor cortex. The whole basal ganglia and dentate nucleus are then affected followed by affection of cerebellum, putamen, caudate nucleus and all neocortical regions at the exception of temporal areas (sketch inspired by Williams et al. [155] and Braak and Del Tredici [13]). (c) In Argyrophilic grain disease, tau deposition starts in the ambiens gyrus and CA1 region of the hippocampus before affecting amygdala, transentorhinal cortex, subiculum and temporal lobe. In stage III, frontal lobe is affected (sketch inspired by Saito et al. [126])
The similarities between these pathologies as well as the clear neuron-to-neuron progression led to the hypothesis that cerebral proteinopathies share similar cellular and molecular pathways of pathological protein propagation. Other types of well-characterized cerebral proteinopathies that spreads through neuronal networks are prion-diseases. Therefore, it was postulated that all these pathologies could be gathered and that all these proteins could be considered as prion-like protein or prionoids (for review: Aguzzi and Rajendran [3], Clavaguera et al. [22], Frost and Diamond [45], Goedert et al. [53], Hall and Patuto [56], Jucker and Walker [72], Walker et al. [151], and Dujardin [29]).
The designation “prion-like” is subject to an intense semantic debate among researchers because, although it is evident that these proteins share similar pathological principles, major differences can also be pointed out [102]. Prion diseases are rare neurodegenerative pathologies characterized by the accumulation of misfolded prion proteins. In 1982, Prusiner and collaborators ventured the hypothesis that the protein prion itself would be an infectious agent, and the unique responsible of the pathology spreading in the body and between individuals [119]. This hypothesis was rapidly confirmed, even if the term “infectious” is still controversial [87], showing that abnormal prion proteins are able to convert normal prion proteins into the pathological form. The latter form soluble oligomers and consequently amyloid fibers. The mechanism of formation of the fibers by recruitment of monomers by an initial oligomer (or nucleus) is called seeding (Fig. 23.2) [72]. Interestingly, different strains of prion exist with dissimilar, and transmissible, fibril conformations [145]. Moreover, the pathological prions can be transferred from cell-to-cell, spreading the pathology in several brain areas.

Tau seeding. Tau monomers are naturally soluble, unfolded and flexible (orange). In pathophysiology context, some transient-to-stable folding can appear (black). In tauopathies, misfolding leads to the recruitment of several monomers into an unstable multimeric forms or oligomers. Through the addition of monomers in a seeding mechanism, misfolded tau proteins transmit their folding properties to a large number of naïve monomers and recruit them into a higher order stable fibril. The black structures represent the core of the fibril as shown by Fitzpatrick and collaborators [39]. Not to scale
This was the first description of a protein with such pathological properties but recently, the hypothesis that other proteins like the amyloid peptide (Aβ), alpha synuclein and Tau could share these properties has been raised. For the amyloid peptide and synuclein, the lesions are transmissible by a seeding mechanism [27, 63, 70, 73, 89, 90, 93, 100, 101, 139, 150]. Similarly to prions, different strains with different functional and physicochemical properties seem to co-exist [11, 109, 111, 161]. Lesions also appear to actively propagate across neural circuits for these two pathological proteins [43, 58, 90, 150].
These studies led the way to the hypothesis that tau could actively propagate trans-synaptically. Tau propagation (or spreading) is a broad term including several cellular pathways including active neuron-to-neuron transfer and the contamination of secondary cells potentially through a seeding mechanism (Fig. 23.3).

Tau prion-like propagation model. (a) In physiology normal tau proteins (orange) are predominantly located into the axonal part of neurons. (b) Tau propagation starts with an early misfolded event thatFig. 23.3 (continued) spreads through a neuron and a large number of tau proteins accumulate into the somatodendritic as well as the synaptic terminals of the neurons. (c) Misfolded tau proteins are transferred from neuron-to-neuron through the synapses and (d) in the recipient neuron, recruit endogenous tau, transmit their misfolding properties in a seeding mechanism and spread the pathology. Not to scale
Transmissibility of Tau Pathology, Tau Seeding?
Several studies have investigated the transmissibility and seeding of Tau pathology (Fig. 23.2) confirming this concept in vitro [44], in cellulo [46] or in vivo [20]. After these three studies, many have confirmed and reproduced this data. Briefly, Clavaguera and coworkers showed that injecting Tau aggregates extracted from mice overexpressing mutated Tau to mice overexpressing wild-type Tau was sufficient to induce Tau pathology [20]. It is interesting to note that when a Tau-immunodepleted extract is injected, no pathology can be detected showing that Tau is the responsible factor. The same group has also shown similar results injecting human brain lysates of several tauopathies and reproducing the morphology of the lesions seen in the human disease [19]. It is also worth noting- even if not reproduced so far in the literature- that they reported the formation of tau pathology in the brain of transgenic mice injected intraperitoneally with Tau aggregates [21]. Many following studies have shown injections of cerebral lysates or synthetic fibers in tau transgenic animals, potentiating the transmissibility [4, 24, 52, 65, 66, 68, 77, 79, 110, 128, 135, 138]. Several of these studies show the presence of murine Tau in the aggregates, suggesting that aggregates are able to recruit endogenous Tau proteins converting them to a pathological form [20, 25, 65, 104]. This is also supported by the observation that tau pathology is transmissible to wild type (WT) animals that don’t usually get any sign of tau pathology [20, 104], and by early observations that endogenous mouse tau was incorporated into the NFT that develop in transgenic P301L human tau overexpressing mice [130]. An interesting recent study show strong tau seeding in vivo when tau aggregates are injected into transgenic animals developing β-amyloid plaques [59]. Tau seeding in this study seems to be highly dependent on the formation of tau aggregation in neuritic processes around plaques. We showed that in human AD patients, tau seeding at the synapses seems to precede tau pathology [28] and that tau seeding was markedly increased when amyloid pathology is present in both mouse models and human brain [9]. These studies could show that amyloid pathology potentiates tau propagation likely at the synaptic terminals and actively triggers its progression outside of the hippocampal formation in the cortical regions where both pathologies ultimately “meet” in Alzheimer’s disease.
In parallel with data on animal models, in cellulo, several authors showed that after the incubation of aggregates, these were internalized and were able to promote aggregation of overexpressed Tau in cell lines [46, 55, 62, 107, 129, 141, 147, 156] but also in primary neurons or human iPS cells overexpressing human tau [106, 124, 142]. These studies showed, using truncated Tau species, that the microtubule-binding domain is necessary to promote aggregation. There is, however, a debate on what is the needed species of tau that is needed to promote tau aggregation or seeding. In a 2015 study, Mirbaha and coworkers observed that Tau trimer is the minimal unit with which a seeding mechanism could be observed [97]. The same authors in 2018 have identified a monomeric tau specie could be converted to a seeding competent form [96]. Although the minimal unit for seed-competency is still subject to debate, most of the studies agree to the idea that soluble oligomeric tau are the most seeding prone species [68, 79, 82, 83, 142].
Neuron-to-Neuron Transfer of Tau
Is Tau Transferred from One Cell to the Other?
Most of the models cited above analyzed the propagation of Tau pathology looking for cell-to-cell transfer of Tau pathology. In cell models, both the (presumably misfolded or posttranslationally modified) WT proteins [32] and aggregated truncated Tau proteins seem to transfer to secondary cells [15, 46, 78, 160]. Models of microfluidic axonal isolations strongly suggest that Tau is trans-synaptically transferred and that synapses are required for neuron-to-neuron transfer [15, 32, 142, 152]. In other cell models, transfer of tau-containing conditioned medium seems to be sufficient to transfer tau to secondary cells suggesting that cell-to-cell contact or the close synaptic environment might not be a prerequisite for tau uptake by cells [15, 78, 160]. We hypothesize that the synaptic uptake therefore is at least in part due to the relative proximity of the pre and post synaptic elements as well as the potentially high local concentrations of any tau released into the extremely small perisynaptic space.
Cell-to-cell transfer of tau was also suggested in in vivo models in which Tau pathology evolves from the injection site to closely connected areas [4, 20, 65, 138]. However, it is difficult from these particular models to firmly conclude and determine the part of active propagation of aggregates versus diffusion area of the injection. In order to answer this question, in two independent studies, a transgenic model using the neuropsin promoter allowing for the overexpression of mutated Tau specifically in the entorhinal cortex has been developed and used to convincingly show the propagation of tau pathology from the entorhinal cortex to recipient neurons in the hippocampus [25, 88].
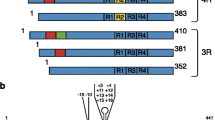
In addition, viral vector-mediated focal overexpression of tau proteins either in the hippocampus of rats or the entorhinal cortex of mice clearly and undoubtfully show that tau proteins can be cell-to-cell transported across long distances in accord with connectional neuroanatomical connections [30, 32, 153, 154]. The advantage of viral vector-mediated systems is that we can easily test different constructs and species of tau. Indeed, we could compare tau propagation of both mutant and wild-type tau as well as 3R versus 4R tau. We found that if the pathological conversion was faster for mutant tau, the long-distance propagation of tau pathological species was more efficient when 4R wild-type tau was used as compared to 3R and mutants [14, 30, 32]. Interestingly, we showed in two different models that the presence of endogenous tau was not required for tau cell-to-cell transfer. However, mouse tau was needed to observe pathological changes in secondary neurons [154] again arguing for the importance of endogenous tau in the pathological recruitment of tau. Worth noting, Tau cell-to-cell transfer was also observed in vivo in one model of lamprey [80, 85]. All together these studies demonstrate that tau can be transferred neuron-to-neuron (and, more generally, in some instances cell-to-cell) which leads to experiments aimed at understanding the cellular pathways implicated in this process (Fig. 23.4).

Mechanisms of cell-to-cell transfer. Different pathways of neuron-to-neuron transfer have been proposed and observed. Tau is secreted into the extracellular space via translocation through the plasma membrane (Purple), extracellular vesicles (Ectosomes – pink or exosomes – red originating from the fusion of multivesicular bodies (MVB) with the plasma membrane). Regular exocytosis (brown) has also been a proposed mechanism but is largely questionable. Tau can also be transferred between cells via nanotubes (light blue). Uptake of tau largely happens through endocytosis (clathrin-mediated or clathrin-independent) and regulated by heparan sulfate proteoglycans (HSPGs) (orange). Tau aggregates are able to escape the endosome to reach the cytoplasm. (Sketch inspired by Dujardin [29] and Mudher et al. [102])
Routes of Cell-to-Cell Transfer
Different routes of cell-to-cell transfer of tau have been proposed. In principle, cell to cell transfer of an intracellular protein like Tau could occur either through release into the extracellular space, or via direct cell-to-cell contact. Regarding the extracellular space, it necessitates two distinct mechanisms: Tau secretion and tau uptake (Fig. 23.4).
-
(a)
Tau secretion
Tau protein is a cytosolic protein thus its secretion via the conventional exocytosis implicating the Golgi apparatus is hardly conceivable. Therefore, several studies examined different routes of secretion and notably via extracellular vesicles. Two types of extracellular vesicles have particularly been shown to be involved in tau secretion: microvesicles (also called microparticles or ectosomes) and exosomes. The generation of microvesicles is still poorly understood but they are large vesicles (between 100 nm to 1 μm diameter) directly shed from plasma membrane. The release of exosomes is better characterized: during endocytosis, invagination of the plasma membrane leads to the formation of the primary endosome. Other invaginations occur in the membrane of this endosome leading to the formation of a multivesicular body. During this step, the intraluminal vesicles trap cytoplasmic material. When the multivesicular body fuses with the plasma membrane, the intraluminal vesicles are released and called exosomes. Exosomes are largely characterized (for review: Kowal et al. [81] and Rajendran et al. [120]) and were shown to carry prion [38], Aβ peptide [121] and synuclein [5, 84]. Moreover, it was shown that exosomes convey some lipids which potentiate fibrillogenesis and accelerates the formation of amyloid structures [162]. In the case of tauopathies, the implication of extracellular vesicles remains somewhat dependent on techniques and model systems used. Indeed, we and other authors describe the presence of Tau in both microvesicles [31] and exosomes purified from cells overexpressing Tau and from patient-derived cerebrospinal fluid [8, 31, 127, 134, 152], whereas other studies failed to reproduce these results in different models [37, 75, 116, 129, 143]. These discrepancies probably rely on the models used but also on the intracellular concentration of tau as it seems that tau is re-directed to exosomes when there is an accumulation in the cytoplasm. Contrariwise, tau seems to be present physiologically in larger microvesicles [31] (Fig. 23.4).
Regardless of whether tau is present in extracellular vesicles, several studies showed that extracellular tau is mostly found free in the medium, not -associated with vesicles [31, 76]. Several studies have proposed different secretory pathways by which tau reaches the extracellular space free. Katsinelos and coworkers found that phosphorylated tau can potentially be translocated across the plasma membrane via a type I unconventional protein secretion mechanism (Fig. 23.4) [76]. Interestingly, chaperone-mediated translocation through membranes seems to lead to secretion as well in another type of unconventional secretion mechanism [41]. Another study by Tang and colleagues showed that in case of overexpression, Tau seems to relocalize, thanks to the mTor kinase, in autophagic vesicles and in the endoplasmic reticulum, which could suggest also the existence of a mechanism of exocytosis [143]. Interestingly, in cellulo, Rab GTPase regulates tau secretion in the extracellular space arguing for an active tau secretion mechanism rather than a potential passive diffusion through the plasma membrane [98, 125]. Additionally, the presence of tau in the extracellular media is stimulated by neuronal activity [116, 158, 159]. Interestingly, Tau proteins seem to be mainly dephosphorylated and truncated in their carboxy-terminal part when secreted [74, 80, 99, 105, 113, 116, 136]. However, truncation of Tau is not retrieved in every model [18]. The mechanisms of secretion described above were mainly identified in vitro and it is likely that part of them represent a physiological secretion rather than pathological processes [18, 116]. In human CSF, where tau is used as a biomarker of Alzheimer disease, both freely soluble and exosome containing pools have been described [10, 108, 127, 152].
-
(b)
Tau uptake
Several studies have shown that tau placed in the extracellular medium is internalized into the soma of secondary cells arguing for the existence of one or several mechanism(s) of uptake [15, 46, 78, 106, 142, 157, 160]. Uptake of tau has also been observed in vivo [17, 142]. Tau monomers and oligomers are also efficiently internalized by human iPSC-derived neurons [146] and by astrocytes in culture [91, 112]. Interestingly, Piacentini and coworkers see a toxic effect of this uptake of oligomeric tau inside the astrocytes on the synaptic activity of neurons. Martini-Stoica and colleagues see that an increased uptake in astrocyte can markedly reduce tau propagation [91, 112]. Several studies showed that uptake of tau happens through endocytosis either clathrin-independent, likely through macropinocytosis, or clathrin-mediated [16, 35, 61, 94]. The uptake of free tau aggregates seems to be mediated by heparan sulfate [61, 122, 140] even if it is likely that other receptors are also implicated in these mechanisms (Figs. 23.4 and 23.5).

Model of uptake and subsequent pathology spreading in the recipient neuron. Tau is released by cells probably from synaptic terminals mostly freely, but also via extracellular vesicles and taken up by secondary cells through a clathrin-independent mechanism of endocytosis or micropinocytosis (orange). Once in the endosome, the endosomal membrane is ruptured, and tau gets into the cytoplasm (red). Once in the cytoplasm misfolded tau induces seeding and spread of the pathology (red). However, autophagic mechanisms are activated to clear tau out causing tau to be internalized inside autophagosomes (purple). Once there, the autophagosome fusion with the lysosome leads to degradation of its content (yellow) or secretion via multivesicular bodies (MVB) (light blue)
This uptake mechanism through the endocytic pathway might actively participate in the pathological propagation mechanism (Fig. 23.5). Indeed, three independent studies demonstrated that tau aggregates can induce a rupture of the endomembrane [16, 35, 40] and reach the cytoplasm. Calafate and coworkers report that BIN1, a genetic risk factor for late-onset Alzheimer’s disease, negatively regulates this endocytic pathway and that a loss of function of BIN1 subsequently results in more uptake and more underlying tau seeding of aggregates [16]. When the endosomal membrane is ruptured autophagy pathways are activated through the galectin-8 and NDP52 receptors [35]. Stress-mediated or pharmacological inhibition of autophagy also potentiate tau aggregation arguing for a key role of autophagy in tau pathology propagation [35, 133]. Michel and co-workers even suggest that tau aggregation from monomers can happen directly inside the endocytosis vesicles and thereby favor tau pathology spreading [94] (Fig. 23.5). Worth noting, exosomes containing tau proteins are also endocytosed and hijacking the endosomal pathway are transferred to several connected neurons [114] (Fig. 23.5).
-
(c)
Nanotubes
Although a secretory pathway is likely to take part in the propagation of Tau pathology, another route has been identified: nanotubes [1, 144] (Fig. 23.4). Nanotubes are filamentous-actin-containing membranous structures with a diameter of 50 to 800 nm forming bridges that connect remote cells. They have been shown to carry prion proteins as well as viruses [54, 137]. Tardivel and co-authors showed that tau could spread through these tunneling nanotubes and that interestingly extracellular tau can induce the formation of these structures.
Existence of “Strains” of Tau Aggregates
The question that actual strains of tau aggregates exist, parallel to the clinical strains observed in prion diseases, has been highly investigated and the answers are not yet definitive. What “strain” means for prion diseases is, based on the same protein template, there exist different but stable conformations of misfolding that are transmissible to native non-misfolded proteins. In prion disease, these different conformers convey different biological properties, including their clinical course and aggressiveness of disease.
In support of this idea, there is substantial evidence for tau that different conformers exist and have various behaviors in pathology. Indeed, different species were described with distinct behaviors in term of tau propagation phenotypes. Differences in different tau preparations ability to undergo cell to cell transfer and seeded misfolding, differences in structure of tau aggregates in different diseases, and differences in the patterns of tau in varied neuropathological diseases like AD compared to Pick’s disease or PSP all point to the existence of something analogous to strains for tau. Firstly, comparing mutant and WT tau gives some insight. In fact, mutated tau proteins seem to bear different fiber morphologies and biochemical characteristics that influence the ability of seeding [6, 34, 47]. It is interesting to observe that the specific fibers’ conformation of mutant tau can be transmitted and conserved by WT tau [34, 47]. In vivo, the propagation and conformations of mutant vs WT tau is also different [30, 32]. Secondly, the different isoforms of tau – particularly the presence or absence of the exon 10 in the respectively called 4R or 3R isoforms – impacts tau behavior. It is of note that fibers made of various Tau isoforms bear variable properties [2, 36, 49, 86, 107], and 3R and 4R tau proteins differ in behavior in in vivo propagation [30]. These properties could explain the different morphologies of lesions observed in human pathologies and transmissible to animal or cell models [19, 128] and the differences in spatiotemporal evolution of Tau pathology between so-called 3R (Pick’s disease) and 4R (PSP, Corticobasal degeneration) tauopathies.
Comparing tau fibers from different sporadic tauopathies and their capacity to seed led to the identification of potential strains [19, 77, 128]. The Diamond laboratory used a stable cell reporter assay [48, 62] to model seeding using brain lysate from several human cases with various tauopathies. They show that the shapes of resulting intracellular aggregates differ from case to case and that this could be transmitted to mice. Different regional pattern of progression in the brain are also observed consistent with the existence in sporadic tauopathies of different tau strains [77, 128].
Structural analysis of tau are difficult to carry out due to the biophysical properties of tau. Nevertheless, recent studies of Cryogenic Electron Microscopy have clearly identified the structure of aggregated tau, either in Alzheimer’s disease [39] or in Pick’s disease [36]. As the content in isoforms differs, the structures of the fibrils are different as well explaining the shapes of fibers as previously observed with electron microscopy. Mirbaha and colleagues also recently suggested that even a single monomer can bear a stable and transmissible conformation that seed aggregation [96]. This result also argues for the presence of specific strains but contradicts previous results showing that monomeric tau in solution has only transient folding [103], raising the question of what stabilizes the monomeric tau into a stable conformation under some circumstances but not others. Whether monomeric tau can have stable structures with a seeding potential in AD and other tauopathies is therefore really intriguing but must be currently viewed as uncertain.
In conclusion, tau species share with prion strains different behavior in tau pathology propagation (fibrils structures; lesions structures; cell types affected; brain regional patterns etc.). Structural evidence shows at least three stable conformations (straight filaments, paired helical filaments, and wide filaments in Pick bodies) but much more structural work in underway [36]. It remains unknown if these stable conformational changes can be reliably transmitted in a human disease setting. Techniques used in the research and diagnosis for prion such as protein misfolding cyclic amplification are also not available for use for tau proteins mostly because tau needs the addition of a polyanion such as heparin to aggregate in vitro [92]. This is one of the challenges for future studies of tau propagation.
Tau Prion-Like Propagation, Challenges and Future Directions
Extensive studies have been conducted in the past decade to understand tau propagation and the underlying cellular and molecular pathways, researchers are still facing several challenges.
Using More Sporadic Tauopathies Models
Tau pathological changes such as hyperphosphorylation or aggregation are fairly frequent in the human brain of even non-demented people. However, for diverse and mostly unknown reasons, in cell and animal models, tau pathology is fairly hard to model. Therefore, most of the time, researchers have to use artifices such as mutating the tau gene (MAPT gene) and/or artificially cleaving tau protein in order to obtain markers of tau pathology. Mutations of the MAPT gene are rare events that only occur in rare genetic familial frontotemporal dementia cases and don’t occur in all the other sporadic tauopathies such as AD, PSP, Pick’s Disease etc. [42, 50]. Tau propagation studies are no exception to this limitation. Some examples: the main cell reporter assay for the study of tau seeding is a truncated and mutated version of tau protein [62]; the main animal model used for the study of tau cell-to-cell transfer is a mutant version of tau [25, 88]; the main animal model used to study tau transmission and seeding is the PS19 mouse model that bears a P301S mutation [65]. Using these tau versions is indeed convenient but one could ask their relevance for sporadic tauopathies especially knowing the previously described structural differences between mutant and WT tau [6, 34, 47]. Some studies tried to use more “sporadic” models of tau propagation. For example, Clavaguera and collaborators were able to induce transmission/seeding of tau pathology into a mouse model overexpressing a WT form of human tau protein [20] or even into WT mice [20, 104]. We used WT rats and overexpressed WT 3R or 4R tau into their hippocampus using lentiviral vectors resulting in the long-distance transfer of tau proteins and also propagation of pathological epitopes [30, 32]. These results are promising but they have limitations as well because (1) of the very long kinetic needed to analyze them (analysis 8–24 months after pathology transduction), (2) you hardly get the full tau pathology phenotypes with only weak aggregation in neurofibrillary tangles, neurodegeneration, or synaptic and behavioral deficits). These limitations of the models probably rely on fundamental kinetic differences in the rodents brain (month of pathological development at max) compared to the human brains (years of pathological evolution). Metabolism, brain clearance and neuroinflammation also seem to occur faster in rodents than in humans. In addition to that, fundamental molecular differences cannot be ignored as mice only express the 4R isoforms of tau when humans express both 3R and 4R. The use of more humanized models such as tau Knock-In rodents, human iPS cells and/or organoids might give us more insights in the future. In conclusion, it would be interesting to invent efficient tools to study tau pathological propagation in a “sporadic” environment to tackle the specific mechanisms of tau release uptake and instructive misfolding.
Tau Propagation, Physiological Versus Pathological Mechanisms
As stated just above, one drawback of some models of tau propagation is that the pathological phenotypes such as tau phosphorylation, misfolding and/or aggregation can be limited. This leads us to hypothesize that at least part of the described mechanisms of tau propagation are happening physiologically. Indeed, for example, regarding the trans-synaptic transfer of tau, in a recent in vivo study we showed that this transfer could happen in the absence of epitopes of tau hyperphosphorylation and misfolding [30]. This result suggests that the trans-synaptic transfer of tau can be a physiological mechanism. This idea is also supported by the fact that tau propagation still occurs in absence of any pathological conversion in a mouse lacking endogenous tau [154]. However, several questions remain: is this physiological mechanism conserved in a diseased brain? Are the routes of cell-to-cell transfer the same in physiology versus pathology? Is the kinetic of this transfer impacted? Some elements of response are present in the literature. Firstly, the routes seem to differ: tau secretion via exosomes, for instance, seem to happen only when tau accumulate intracellularly and not physiologically [31]. Secondly, the kinetic of nanotubes formation is impacted by the extracellular presence of tau aggregates [144]. Finally, numerous studies all show that secreted tau proteins are mostly non-phosphorylated, monomeric, soluble and truncated [18, 31, 41, 75, 76, 99, 113, 115, 116, 127, 129, 134, 143, 159]. This goes in line with a physiological secretion of tau and could explain the presence of tau in the cerebrospinal fluid of every individuals independently of neuronal death [57]. However, on the other side, tau uptake seems to be more efficient for aggregated species than monomeric tau [97, 142]. Understanding this discrepancy between secretion and uptake may be a key point for understanding the exact mechanisms of tau propagation. Whether this is due to different kinetic of uptake, route of uptake or intracellular stability after uptake is difficult to understand at that time.
Precisely Identify the Kinetics of Tau Life Cycle Events
Understanding tau propagation also comes by deciphering the kinetic of events in the brain. This notion is largely unknown and very dependent on the models used but the current literature can inform us about the slow versus fast points of this process. Firstly, it seems that the neuron-to-neuron transfer of tau is a slow point both in vitro and in vivo where we can observe it only after respectively days or weeks/months [15, 25, 32, 88]. It is interesting and counterintuitive to notice that both secretion and uptake are fast points as they can be observed in hours mostly in vitro [15, 31, 46, 78, 106, 116, 142, 157,158,159,160]. The discrepancy between transfer and secretion/uptake probably rely on (1) the sensitivity of the histology techniques used to see tau transfer and (2) the mostly non-physiologic amount of tau used to observe fast secretion and fast uptake. Lastly, tau seeding seems to be a process regulated by a sigmoidal growth with a long lag phase, an exponential growth phase and a plateau phase [62]. In vitro, when the right conditions are reunited (high intracellular content of tau, presence of tau truncation/mutation favoring misfolding etc.), the whole seeding process can happen in less than 24 h [28] when in vivo the lag phase takes probably weeks and also relies on the amount and quality of tau in the recipient brain. Indeed, inducing seeding and aggregates formation in a tau transgenic animal with a mutation (as soon as 2 weeks post induction in animals such as PS19 mice (see Ahmed et al. [4] and Iba et al. [65, 66]) is faster than for a tau transgenic animal without a mutation (months post-injection in animals such as alz17 or hTau mice (see Castillo-Carranza et al. [17] and Clavaguera et al. [20] or in WT animals [20])). The fast/exponential appearance of neurofibrillary tangle after the lag phase in vivo is supported by observations using 2-photon microscopy [25]. Thus both transfer and seeding have their fast and slow points. It is also evident that factors such as the presence of amyloid beta [9, 59, 69, 117, 148] or brain activity [116, 158, 159] can also accelerate these slow points.
Identify Good Therapeutic Strategies
Identifying tau propagation as a key mechanism of tauopathies and particularly AD has raised some hope to find a disease-modifying treatment tackling the progression of the disease. An obvious target is the extracellular species of tau. This led to intense research by academic and industry teams around the development of immunotherapies. Most of the studies find a high potential for reducing tau propagation in diverse models. Examples include the work of Holtzman’s team showing a reduction of tau uptake and seeding in vitro in addition to reduction of tau pathology in a transgenic mouse model of genetic Frontotemporal Lobar Dementia [160]. Antibodies against oligomeric tau (TOMA antibodies) showed reduction of seeding after injection of oligomers in the brain of hTau mouse model [17]. We more recently showed diverse efficacies of different antibodies raised against total tau and also phosphorylated tau or truncated tau onto uptake and seeding of high molecular weight tau [105, 106]. Recent studies confirm these data in other models and trying to assess the potential of different epitopes [23, 24]. Beside the use of immunotherapy, tau propagation research could lead to additional efforts to develop therapies by targeting the pathway by which tau propagates. This includes the mediators of tau propagation like targeting the mechanisms of secretion (chaperones, exosome formations), the mechanisms of tau uptake (the endosomal pathway), stimulating the autophagy pathways to favor clearance, stimulation of deacetylase [95] etc. To our knowledge, this research is still preliminary but the understanding of mechanisms of tau propagation might lead to more potential therapies in the future.
Understand the Regional Patterns, the Cell Vulnerabilities
It is striking to notice the differences between the pattern of progression of the different tauopathies in the human brain. While they are all patterns of tau aggregation, they are quite heterogenous. Why are some pathologies very focal (Pick’s disease or Argyrophilic Grain Disease) and some more global (PSP and AD)? Why tau progression leads to asymmetry in some diseases and global symmetry in others? Interestingly, the human data show for example that in AD the neurons receiving the neurofibrillary tangles are strongly interconnected but dentate gyrus granule cells, which receive the bulk of the perforant pathway projection from the early affected entorhinal cortex, are relatively resistant [64]. On the other hand, Pick bodies, another type of lesion made of tau aggregates are predominantly present in these particular granule cells in the dentate gyrus that are resistant to the alternatively folded form of tau found in neurofibrillary tangles [118]. These differences are thought to be due to different cell populations vulnerabilities to tau pathology [123]. This also suggests unique relationships between specific misfolded tau species and host cell characteristics. It would be really important to understand why different brain areas and neuronal subtypes are selectively vulnerable for different forms of inclusions? Beyond the observation that propagation is therefore dependent on both the anatomy and the properties of the recipient cell, these concepts are largely unexplored so far.
Conclusions
Tau propagation, this sequence of events leading to the progression of the disease in the brain of tauopathies (Fig. 23.2), has now been experimentally described. We can distinguish several pathways leading to tau propagation: (1) the transfer from cell-to-cell of both pathological and non-pathological species of tau (Fig. 23.4) and (2) the transmission of tau pathology in a second neuron via a seeding mechanism (Fig. 23.1). The most plausible route of tau transfer is through the extracellular space and particularly via its secretion (mostly freely in the medium but also through extracellular vesicles) and uptake into recipient neurons (Fig. 23.4). This uptake likely occurs via an endocytic mechanism. Once in the endosome, tau aggregates cause the endosomal membrane to rupture and reach the cytoplasm. It has been demonstrated that when they reach the cytoplasm, tau aggregates induce recruit endogenous naïve tau proteins in a seeding mechanism (Fig. 23.5). The similarities between these mechanisms and the prion protein spreading mechanism has opened a discussion between researchers over the idea that we can reunite tau, prion and other proteins under the banner of prion-like proteins. This semantic debate is still open but we clearly, here, brought arguments for the existence of strong convergence points but as well pointed out differences. Many other questions remain to be answered. Why would different brain areas and neuronal subtypes be selectively vulnerable for different forms of inclusions? What causes the initial misfolding events that are then propagated across neural systems? Why distinct and specific neural systems would respond differently to tau “strains”? What causes toxicity of neural networks? What is the impact of known molecular differences (isoforms and posttranslational modifications) onto these mechanisms? And, perhaps most importantly, can these insights help in the design and application of tau as a therapeutic target to slow progressive neurodegeneration in AD and other tauopathies?
References
Abounit S, Wu JW, Duff K, Victoria GS, Zurzolo C. Tunneling nanotubes: a possible highway in the spreading of tau and other prion-like proteins in neurodegenerative diseases. Prion. 2016;10(5):344–51. https://doi.org/10.1080/19336896.2016.1223003.
Adams SJ, DeTure MA, McBride M, Dickson DW, Petrucelli L. Three repeat isoforms of tau inhibit assembly of four repeat tau filaments. PLoS One. 2010;5(5):e10810. https://doi.org/10.1371/journal.pone.0010810.
Aguzzi A, Rajendran L. The transcellular spread of cytosolic amyloids, prions, and prionoids. Neuron. 2009;64(6):783–90. https://doi.org/10.1016/j.neuron.2009.12.016.
Ahmed Z, Cooper J, Murray TK, Garn K, McNaughton E, Clarke H, Parhizkar S, Ward MA, Cavallini A, Jackson S, Bose S, Clavaguera F, Tolnay M, Lavenir I, Goedert M, Hutton ML, O’Neill MJ. A novel in vivo model of tau propagation with rapid and progressive neurofibrillary tangle pathology: the pattern of spread is determined by connectivity, not proximity. Acta Neuropathol. 2014;127(5):667–83. https://doi.org/10.1007/s00401-014-1254-6.
Alvarez-Erviti L, Seow Y, Yin H, Betts C, Lakhal S, Wood MJ. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat Biotechnol. 2011;29(4):341–5. https://doi.org/10.1038/nbt.1807.
Aoyagi H, Hasegawa M, Tamaoka A. Fibrillogenic nuclei composed of P301L mutant tau induce elongation of P301L tau but not wild-type tau. J Biol Chem. 2007;282(28):20309–18. https://doi.org/10.1074/jbc.M611876200.
Arnold SE, Hyman BT, Flory J, Damasio AR, Van Hoesen GW. The topographical and neuroanatomical distribution of neurofibrillary tangles and neuritic plaques in the cerebral cortex of patients with Alzheimer’s disease. Cereb Cortex. 1991;1(1):103–16.
Asai H, Ikezu S, Tsunoda S, Medalla M, Luebke J, Haydar T, Wolozin B, Butovsky O, Kugler S, Ikezu T. Depletion of microglia and inhibition of exosome synthesis halt tau propagation. Nat Neurosci. 2015;18(11):1584–93. https://doi.org/10.1038/nn.4132.
Bennett RE, DeVos SL, Dujardin S, Corjuc B, Gor R, Gonzalez J, Roe AD, Frosch MP, Pitstick R, Carlson GA, Hyman BT. Enhanced Tau aggregation in the presence of amyloid beta. Am J Pathol. 2017;187(7):1601–12. https://doi.org/10.1016/j.ajpath.2017.03.011.
Blennow K. A review of fluid biomarkers for Alzheimer’s disease: moving from CSF to blood. Neurol Ther. 2017;6(Suppl 1):15–24. https://doi.org/10.1007/s40120-017-0073-9.
Bousset L, Pieri L, Ruiz-Arlandis G, Gath J, Jensen PH, Habenstein B, Madiona K, Olieric V, Bockmann A, Meier BH, Melki R. Structural and functional characterization of two alpha-synuclein strains. Nat Commun. 2013;4:2575. https://doi.org/10.1038/ncomms3575.
Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 1991;82(4):239–59.
Braak H, Del Tredici K. The pathological process underlying Alzheimer’s disease in individuals under thirty. Acta Neuropathol. 2011;121(2):171–81. https://doi.org/10.1007/s00401-010-0789-4.
Caillierez R, Begard S, Lecolle K, Deramecourt V, Zommer N, Dujardin S, Loyens A, Dufour N, Auregan G, Winderickx J, Hantraye P, Deglon N, Buee L, Colin M. Lentiviral delivery of the human wild-type tau protein mediates a slow and progressive neurodegenerative tau pathology in the rat brain. Mol Ther. 2013;21(7):1358–68. https://doi.org/10.1038/mt.2013.66.
Calafate S, Buist A, Miskiewicz K, Vijayan V, Daneels G, de Strooper B, de Wit J, Verstreken P, Moechars D. Synaptic contacts enhance cell-to-cell Tau pathology propagation. Cell Rep. 2015;11(8):1176–83. https://doi.org/10.1016/j.celrep.2015.04.043.
Calafate S, Flavin W, Verstreken P, Moechars D. Loss of Bin1 promotes the propagation of Tau pathology. Cell Rep. 2016;17(4):931–40. https://doi.org/10.1016/j.celrep.2016.09.063.
Castillo-Carranza DL, Gerson JE, Sengupta U, Guerrero-Munoz MJ, Lasagna-Reeves CA, Kayed R. Specific targeting of tau oligomers in Htau mice prevents cognitive impairment and tau toxicity following injection with brain-derived tau oligomeric seeds. J Alzheimers Dis. 2014;40(Suppl 1):S97–S111. https://doi.org/10.3233/JAD-132477.
Chai X, Dage JL, Citron M. Constitutive secretion of tau protein by an unconventional mechanism. Neurobiol Dis. 2012;48(3):356–66. https://doi.org/10.1016/j.nbd.2012.05.021.
Clavaguera F, Akatsu H, Fraser G, Crowther RA, Frank S, Hench J, Probst A, Winkler DT, Reichwald J, Staufenbiel M, Ghetti B, Goedert M, Tolnay M. Brain homogenates from human tauopathies induce tau inclusions in mouse brain. Proc Natl Acad Sci U S A. 2013;110(23):9535–40. https://doi.org/10.1073/pnas.1301175110.
Clavaguera F, Bolmont T, Crowther RA, Abramowski D, Frank S, Probst A, Fraser G, Stalder AK, Beibel M, Staufenbiel M, Jucker M, Goedert M, Tolnay M. Transmission and spreading of tauopathy in transgenic mouse brain. Nat Cell Biol. 2009;11(7):909–13. https://doi.org/10.1038/ncb1901.
Clavaguera F, Hench J, Lavenir I, Schweighauser G, Frank S, Goedert M, Tolnay M. Peripheral administration of tau aggregates triggers intracerebral tauopathy in transgenic mice. Acta Neuropathol. 2014;127(2):299–301. https://doi.org/10.1007/s00401-013-1231-5.
Clavaguera F, Lavenir I, Falcon B, Frank S, Goedert M, Tolnay M. “Prion-like” templated misfolding in tauopathies. Brain Pathol. 2013;23(3):342–9. https://doi.org/10.1111/bpa.12044.
Courade JP, Angers R, Mairet-Coello G, Pacico N, Tyson K, Lightwood D, Munro R, McMillan D, Griffin R, Baker T, Starkie D, Nan R, Westwood M, Mushikiwabo ML, Jung S, Odede G, Sweeney B, Popplewell A, Burgess G, Downey P, Citron M. Epitope determines efficacy of therapeutic anti-Tau antibodies in a functional assay with human Alzheimer Tau. Acta Neuropathol. 2018;136(5):729–45. https://doi.org/10.1007/s00401-018-1911-2.
Dai CL, Hu W, Tung YC, Liu F, Gong CX, Iqbal K. Tau passive immunization blocks seeding and spread of Alzheimer hyperphosphorylated Tau-induced pathology in 3 x Tg-AD mice. Alzheimers Res Ther. 2018;10(1):13. https://doi.org/10.1186/s13195-018-0341-7.
de Calignon A, Polydoro M, Suarez-Calvet M, William C, Adamowicz DH, Kopeikina KJ, Pitstick R, Sahara N, Ashe KH, Carlson GA, Spires-Jones TL, Hyman BT. Propagation of tau pathology in a model of early Alzheimer’s disease. Neuron. 2012;73(4):685–97. https://doi.org/10.1016/j.neuron.2011.11.033.
Delacourte A, David JP, Sergeant N, Buee L, Wattez A, Vermersch P, Ghozali F, Fallet-Bianco C, Pasquier F, Lebert F, Petit H, Di Menza C. The biochemical pathway of neurofibrillary degeneration in aging and Alzheimer’s disease. Neurology. 1999;52(6):1158–65.
Desplats P, Lee HJ, Bae EJ, Patrick C, Rockenstein E, Crews L, Spencer B, Masliah E, Lee SJ. Inclusion formation and neuronal cell death through neuron-to-neuron transmission of alpha-synuclein. Proc Natl Acad Sci U S A. 2009;106(31):13010–5. https://doi.org/10.1073/pnas.0903691106.
DeVos SL, Corjuc BT, Commins C, Dujardin S, Bannon RN, Corjuc D, Moore BD, Bennett RE, Jorfi M, Gonzales JA, Dooley PM, Roe AD, Pitstick R, Irimia D, Frosch MP, Carlson GA, Hyman BT. Tau reduction in the presence of amyloid-beta prevents tau pathology and neuronal death in vivo. Brain. 2018;141(7):2194–212. https://doi.org/10.1093/brain/awy117.
Dujardin S. De la cellule au primate, propagation physiopathologique de la protéine Tau (From cells to primates, pathophysiological propagation of tau protein). Catalogue SCD Lille. 2015;2:1–334.
Dujardin S, Begard S, Caillierez R, Lachaud C, Carrier S, Lieger S, Gonzalez JA, Deramecourt V, Deglon N, Maurage CA, Frosch MP, Hyman BT, Colin M, Buee L. Different tau species lead to heterogeneous tau pathology propagation and misfolding. Acta Neuropathol Commun. 2018;6(1):132. https://doi.org/10.1186/s40478-018-0637-7.
Dujardin S, Begard S, Caillierez R, Lachaud C, Delattre L, Carrier S, Loyens A, Galas MC, Bousset L, Melki R, Auregan G, Hantraye P, Brouillet E, Buee L, Colin M. Ectosomes: a new mechanism for non-exosomal secretion of tau protein. PLoS One. 2014;9(6):e100760. https://doi.org/10.1371/journal.pone.0100760.
Dujardin S, Lecolle K, Caillierez R, Begard S, Zommer N, Lachaud C, Carrier S, Dufour N, Auregan G, Winderickx J, Hantraye P, Deglon N, Colin M, Buee L. Neuron-to-neuron wild-type Tau protein transfer through a trans-synaptic mechanism: relevance to sporadic tauopathies. Acta Neuropathol Commun. 2014;2:14. https://doi.org/10.1186/2051-5960-2-14.
Duyckaerts C, Hauw JJ. Diagnosis and staging of Alzheimer disease. Neurobiol Aging. 1997;18(4 Suppl):S33–42.
Falcon B, Cavallini A, Angers R, Glover S, Murray TK, Barnham L, Jackson S, O’Neill MJ, Isaacs AM, Hutton ML, Szekeres PG, Goedert M, Bose S. Conformation determines the seeding potencies of native and recombinant Tau aggregates. J Biol Chem. 2015;290(2):1049–65. https://doi.org/10.1074/jbc.M114.589309.
Falcon B, Noad J, McMahon H, Randow F, Goedert M. Galectin-8-mediated selective autophagy protects against seeded tau aggregation. J Biol Chem. 2018;293(7):2438–51. https://doi.org/10.1074/jbc.M117.809293.
Falcon B, Zhang W, Murzin AG, Murshudov G, Garringer HJ, Vidal R, Crowther RA, Ghetti B, Scheres SHW, Goedert M. Structures of filaments from Pick’s disease reveal a novel tau protein fold. Nature. 2018;561(7721):137–40. https://doi.org/10.1038/s41586-018-0454-y.
Faure J, Lachenal G, Court M, Hirrlinger J, Chatellard-Causse C, Blot B, Grange J, Schoehn G, Goldberg Y, Boyer V, Kirchhoff F, Raposo G, Garin J, Sadoul R. Exosomes are released by cultured cortical neurones. Mol Cell Neurosci. 2006;31(4):642–8. https://doi.org/10.1016/j.mcn.2005.12.003.
Fevrier B, Vilette D, Archer F, Loew D, Faigle W, Vidal M, Laude H, Raposo G. Cells release prions in association with exosomes. Proc Natl Acad Sci U S A. 2004;101(26):9683–8. https://doi.org/10.1073/pnas.0308413101.
Fitzpatrick AWP, Falcon B, He S, Murzin AG, Murshudov G, Garringer HJ, Crowther RA, Ghetti B, Goedert M, Scheres SHW. Cryo-EM structures of tau filaments from Alzheimer’s disease. Nature. 2017;547(7662):185–90. https://doi.org/10.1038/nature23002.
Flavin WP, Bousset L, Green ZC, Chu Y, Skarpathiotis S, Chaney MJ, Kordower JH, Melki R, Campbell EM. Endocytic vesicle rupture is a conserved mechanism of cellular invasion by amyloid proteins. Acta Neuropathol. 2017;134(4):629–53. https://doi.org/10.1007/s00401-017-1722-x.
Fontaine SN, Zheng D, Sabbagh JJ, Martin MD, Chaput D, Darling A, Trotter JH, Stothert AR, Nordhues BA, Lussier A, Baker J, Shelton L, Kahn M, Blair LJ, Stevens SM Jr, Dickey CA. DnaJ/Hsc70 chaperone complexes control the extracellular release of neurodegenerative-associated proteins. EMBO J. 2016;35(14):1537–49. https://doi.org/10.15252/embj.201593489.
Forrest SL, Kril JJ, Halliday GM. Reply: will FTLD-tau work for all when FTDP-17 retires? Brain. 2018; https://doi.org/10.1093/brain/awy179.
Freundt EC, Maynard N, Clancy EK, Roy S, Bousset L, Sourigues Y, Covert M, Melki R, Kirkegaard K, Brahic M. Neuron-to-neuron transmission of alpha-synuclein fibrils through axonal transport. Ann Neurol. 2012;72(4):517–24. https://doi.org/10.1002/ana.23747.
Friedhoff P, von Bergen M, Mandelkow EM, Davies P, Mandelkow E. A nucleated assembly mechanism of Alzheimer paired helical filaments. Proc Natl Acad Sci U S A. 1998;95(26):15712–7.
Frost B, Diamond MI. Prion-like mechanisms in neurodegenerative diseases. Nat Rev Neurosci. 2010;11(3):155–9. https://doi.org/10.1038/nrn2786.
Frost B, Jacks RL, Diamond MI. Propagation of tau misfolding from the outside to the inside of a cell. J Biol Chem. 2009;284(19):12845–52. https://doi.org/10.1074/jbc.M808759200.
Frost B, Ollesch J, Wille H, Diamond MI. Conformational diversity of wild-type Tau fibrils specified by templated conformation change. J Biol Chem. 2009;284(6):3546–51. https://doi.org/10.1074/jbc.M805627200.
Furman JL, Holmes BB, Diamond MI. Sensitive detection of proteopathic seeding activity with FRET flow cytometry. J Vis Exp. 2015;106:e53205. https://doi.org/10.3791/53205.
Furukawa Y, Kaneko K, Nukina N. Tau protein assembles into isoform- and disulfide-dependent polymorphic fibrils with distinct structural properties. J Biol Chem. 2011;286(31):27236–46. https://doi.org/10.1074/jbc.M111.248963.
Ghetti B, Oblak AL, Boeve BF, Johnson KA, Dickerson BC, Goedert M. Invited review: frontotemporal dementia caused by microtubule-associated protein tau gene (MAPT) mutations: a chameleon for neuropathology and neuroimaging. Neuropathol Appl Neurobiol. 2015;41(1):24–46. https://doi.org/10.1111/nan.12213.
Giannakopoulos P, Herrmann FR, Bussiere T, Bouras C, Kovari E, Perl DP, Morrison JH, Gold G, Hof PR. Tangle and neuron numbers, but not amyloid load, predict cognitive status in Alzheimer’s disease. Neurology. 2003;60(9):1495–500.
Gibbons GS, Banks RA, Kim B, Xu H, Changolkar L, Leight SN, Riddle DM, Li C, Gathagan RJ, Brown HJ, Zhang B, Trojanowski JQ, Lee VM. GFP-mutant human Tau transgenic mice develop tauopathy following CNS injections of Alzheimer’s brain-derived pathological Tau or synthetic mutant human Tau fibrils. J Neurosci. 2017;37(47):11485–94. https://doi.org/10.1523/JNEUROSCI.2393-17.2017.
Goedert M, Clavaguera F, Tolnay M. The propagation of prion-like protein inclusions in neurodegenerative diseases. Trends Neurosci. 2010;33(7):317–25. https://doi.org/10.1016/j.tins.2010.04.003.
Gousset K, Schiff E, Langevin C, Marijanovic Z, Caputo A, Browman DT, Chenouard N, de Chaumont F, Martino A, Enninga J, Olivo-Marin JC, Mannel D, Zurzolo C. Prions hijack tunnelling nanotubes for intercellular spread. Nat Cell Biol. 2009;11(3):328–36. https://doi.org/10.1038/ncb1841.
Guo JL, Lee VM. Seeding of normal Tau by pathological Tau conformers drives pathogenesis of Alzheimer-like tangles. J Biol Chem. 2011;286(17):15317–31. https://doi.org/10.1074/jbc.M110.209296.
Hall GF, Patuto BA. Is tau ready for admission to the prion club? Prion. 2012;6(3):223–33. https://doi.org/10.4161/pri.19912.
Hall GF, Saman S. Death or secretion? The demise of a plausible assumption about CSF-tau in Alzheimer disease? Commun Integr Biol. 2012;5(6):623–6. https://doi.org/10.4161/cib.21437.
Hamaguchi T, Eisele YS, Varvel NH, Lamb BT, Walker LC, Jucker M. The presence of Abeta seeds, and not age per se, is critical to the initiation of Abeta deposition in the brain. Acta Neuropathol. 2012;123(1):31–7. https://doi.org/10.1007/s00401-011-0912-1.
He Z, Guo JL, McBride JD, Narasimhan S, Kim H, Changolkar L, Zhang B, Gathagan RJ, Yue C, Dengler C, Stieber A, Nitla M, Coulter DA, Abel T, Brunden KR, Trojanowski JQ, Lee VM. Amyloid-beta plaques enhance Alzheimer’s brain tau-seeded pathologies by facilitating neuritic plaque tau aggregation. Nat Med. 2018;24(1):29–38. https://doi.org/10.1038/nm.4443.
Hoenig MC, Bischof GN, Seemiller J, Hammes J, Kukolja J, Onur OA, Jessen F, Fliessbach K, Neumaier B, Fink GR, van Eimeren T, Drzezga A. Networks of tau distribution in Alzheimer’s disease. Brain. 2018;141(2):568–81. https://doi.org/10.1093/brain/awx353.
Holmes BB, DeVos SL, Kfoury N, Li M, Jacks R, Yanamandra K, Ouidja MO, Brodsky FM, Marasa J, Bagchi DP, Kotzbauer PT, Miller TM, Papy-Garcia D, Diamond MI. Heparan sulfate proteoglycans mediate internalization and propagation of specific proteopathic seeds. Proc Natl Acad Sci U S A. 2013;110(33):E3138–47. https://doi.org/10.1073/pnas.1301440110.
Holmes BB, Furman JL, Mahan TE, Yamasaki TR, Mirbaha H, Eades WC, Belaygorod L, Cairns NJ, Holtzman DM, Diamond MI. Proteopathic tau seeding predicts tauopathy in vivo. Proc Natl Acad Sci U S A. 2014;111(41):E4376–85. https://doi.org/10.1073/pnas.1411649111.
Hu X, Crick SL, Bu G, Frieden C, Pappu RV, Lee JM. Amyloid seeds formed by cellular uptake, concentration, and aggregation of the amyloid-beta peptide. Proc Natl Acad Sci U S A. 2009;106(48):20324–9. https://doi.org/10.1073/pnas.0911281106.
Hyman BT, Van Hoesen GW, Damasio AR, Barnes CL. Alzheimer’s disease: cell-specific pathology isolates the hippocampal formation. Science. 1984;225(4667):1168–70.
Iba M, Guo JL, McBride JD, Zhang B, Trojanowski JQ, Lee VM. Synthetic tau fibrils mediate transmission of neurofibrillary tangles in a transgenic mouse model of Alzheimer’s-like tauopathy. J Neurosci. 2013;33(3):1024–37. https://doi.org/10.1523/JNEUROSCI.2642-12.2013.
Iba M, McBride JD, Guo JL, Zhang B, Trojanowski JQ, Lee VM. Tau pathology spread in PS19 tau transgenic mice following locus coeruleus (LC) injections of synthetic tau fibrils is determined by the LC’s afferent and efferent connections. Acta Neuropathol. 2015;130(3):349–62. https://doi.org/10.1007/s00401-015-1458-4.
Irwin DJ, Brettschneider J, McMillan CT, Cooper F, Olm C, Arnold SE, Van Deerlin VM, Seeley WW, Miller BL, Lee EB, Lee VM, Grossman M, Trojanowski JQ. Deep clinical and neuropathological phenotyping of Pick disease. Ann Neurol. 2016;79(2):272–87. https://doi.org/10.1002/ana.24559.
Jackson SJ, Kerridge C, Cooper J, Cavallini A, Falcon B, Cella CV, Landi A, Szekeres PG, Murray TK, Ahmed Z, Goedert M, Hutton M, O’Neill MJ, Bose S. Short fibrils constitute the major species of seed-competent Tau in the brains of mice transgenic for human P301S Tau. J Neurosci. 2016;36(3):762–72. https://doi.org/10.1523/JNEUROSCI.3542-15.2016.
Jacobs HIL, Hedden T, Schultz AP, Sepulcre J, Perea RD, Amariglio RE, Papp KV, Rentz DM, Sperling RA, Johnson KA. Structural tract alterations predict downstream tau accumulation in amyloid-positive older individuals. Nat Neurosci. 2018;21(3):424–31. https://doi.org/10.1038/s41593-018-0070-z.
Jarrett JT, Lansbury PT Jr. Seeding “one-dimensional crystallization” of amyloid: a pathogenic mechanism in Alzheimer’s disease and scrapie? Cell. 1993;73(6):1055–8.
Johnson KA, Schultz A, Betensky RA, Becker JA, Sepulcre J, Rentz D, Mormino E, Chhatwal J, Amariglio R, Papp K, Marshall G, Albers M, Mauro S, Pepin L, Alverio J, Judge K, Philiossaint M, Shoup T, Yokell D, Dickerson B, Gomez-Isla T, Hyman B, Vasdev N, Sperling R. Tau positron emission tomographic imaging in aging and early Alzheimer disease. Ann Neurol. 2016;79(1):110–9. https://doi.org/10.1002/ana.24546.
Jucker M, Walker LC. Self-propagation of pathogenic protein aggregates in neurodegenerative diseases. Nature. 2013;501(7465):45–51. https://doi.org/10.1038/nature12481.
Kane MD, Lipinski WJ, Callahan MJ, Bian F, Durham RA, Schwarz RD, Roher AE, Walker LC. Evidence for seeding of beta -amyloid by intracerebral infusion of Alzheimer brain extracts in beta -amyloid precursor protein-transgenic mice. J Neurosci. 2000;20(10):3606–11.
Kanmert D, Cantlon A, Muratore CR, Jin M, O’Malley TT, Lee G, Young-Pearse TL, Selkoe DJ, Walsh DM. C-terminally truncated forms of Tau, but not full-length Tau or its C-terminal fragments, are released from neurons independently of cell death. J Neurosci. 2015;35(30):10851–65. https://doi.org/10.1523/JNEUROSCI.0387-15.2015.
Karch CM, Jeng AT, Goate AM. Extracellular Tau levels are influenced by variability in Tau that is associated with tauopathies. J Biol Chem. 2012;287(51):42751–62. https://doi.org/10.1074/jbc.M112.380642.
Katsinelos T, Zeitler M, Dimou E, Karakatsani A, Muller HM, Nachman E, Steringer JP, Ruiz de Almodovar C, Nickel W, Jahn TR. Unconventional secretion mediates the trans-cellular spreading of Tau. Cell Rep. 2018;23(7):2039–55. https://doi.org/10.1016/j.celrep.2018.04.056.
Kaufman SK, Sanders DW, Thomas TL, Ruchinskas AJ, Vaquer-Alicea J, Sharma AM, Miller TM, Diamond MI. Tau prion strains dictate patterns of cell pathology, progression rate, and regional vulnerability in vivo. Neuron. 2016;92(4):796–812. https://doi.org/10.1016/j.neuron.2016.09.055.
Kfoury N, Holmes BB, Jiang H, Holtzman DM, Diamond MI. Trans-cellular propagation of Tau aggregation by fibrillar species. J Biol Chem. 2012;287(23):19440–51. https://doi.org/10.1074/jbc.M112.346072.
Kim D, Lim S, Haque MM, Ryoo N, Hong HS, Rhim H, Lee DE, Chang YT, Lee JS, Cheong E, Kim DJ, Kim YK. Identification of disulfide cross-linked tau dimer responsible for tau propagation. Sci Rep. 2015;5:15231. https://doi.org/10.1038/srep15231.
Kim W, Lee S, Jung C, Ahmed A, Lee G, Hall GF. Interneuronal transfer of human tau between lamprey central neurons in situ. J Alzheimers Dis. 2010;19(2):647–64. https://doi.org/10.3233/JAD-2010-1273.
Kowal J, Tkach M, Thery C. Biogenesis and secretion of exosomes. Curr Opin Cell Biol. 2014;29:116–25. https://doi.org/10.1016/j.ceb.2014.05.004.
Lasagna-Reeves CA, Castillo-Carranza DL, Sengupta U, Guerrero-Munoz MJ, Kiritoshi T, Neugebauer V, Jackson GR, Kayed R. Alzheimer brain-derived tau oligomers propagate pathology from endogenous tau. Sci Rep. 2012;2:700. https://doi.org/10.1038/srep00700.
Lasagna-Reeves CA, Castillo-Carranza DL, Sengupta U, Sarmiento J, Troncoso J, Jackson GR, Kayed R. Identification of oligomers at early stages of tau aggregation in Alzheimer’s disease. FASEB J. 2012;26(5):1946–59. https://doi.org/10.1096/fj.11-199851.
Lee HJ, Patel S, Lee SJ. Intravesicular localization and exocytosis of alpha-synuclein and its aggregates. J Neurosci. 2005;25(25):6016–24. https://doi.org/10.1523/JNEUROSCI.0692-05.2005.
Lee S, Kim W, Li Z, Hall GF. Accumulation of vesicle-associated human tau in distal dendrites drives degeneration and tau secretion in an in situ cellular tauopathy model. Int J Alzheimers Dis. 2012;2012:172837. https://doi.org/10.1155/2012/172837.
Levarska L, Zilka N, Jadhav S, Neradil P, Novak M. Of rodents and men: the mysterious interneuronal pilgrimage of misfolded protein tau in Alzheimer’s disease. J Alzheimers Dis. 2013;37(3):569–77. https://doi.org/10.3233/JAD-131106.
Liberski PP. Prion, prionoids and infectious amyloid. Parkinsonism Relat Disord. 2014;20(Suppl 1):S80–4. https://doi.org/10.1016/S1353-8020(13)70021-X.
Liu L, Drouet V, Wu JW, Witter MP, Small SA, Clelland C, Duff K. Trans-synaptic spread of tau pathology in vivo. PLoS One. 2012;7(2):e31302. https://doi.org/10.1371/journal.pone.0031302.
Luk KC, Kehm V, Carroll J, Zhang B, O’Brien P, Trojanowski JQ, Lee VM. Pathological alpha-synuclein transmission initiates Parkinson-like neurodegeneration in nontransgenic mice. Science. 2012;338(6109):949–53. https://doi.org/10.1126/science.1227157.
Luk KC, Kehm VM, Zhang B, O’Brien P, Trojanowski JQ, Lee VM. Intracerebral inoculation of pathological alpha-synuclein initiates a rapidly progressive neurodegenerative alpha-synucleinopathy in mice. J Exp Med. 2012;209(5):975–86. https://doi.org/10.1084/jem.20112457.
Martini-Stoica H, Cole AL, Swartzlander DB, Chen F, Wan YW, Bajaj L, Bader DA, Lee VMY, Trojanowski JQ, Liu Z, Sardiello M, Zheng H. TFEB enhances astroglial uptake of extracellular tau species and reduces tau spreading. J Exp Med. 2018;215(9):2355–77. https://doi.org/10.1084/jem.20172158.
Meyer V, Dinkel PD, Rickman Hager E, Margittai M. Amplification of Tau fibrils from minute quantities of seeds. Biochemistry. 2014;53(36):5804–9. https://doi.org/10.1021/bi501050g.
Meyer-Luehmann M, Coomaraswamy J, Bolmont T, Kaeser S, Schaefer C, Kilger E, Neuenschwander A, Abramowski D, Frey P, Jaton AL, Vigouret JM, Paganetti P, Walsh DM, Mathews PM, Ghiso J, Staufenbiel M, Walker LC, Jucker M. Exogenous induction of cerebral beta-amyloidogenesis is governed by agent and host. Science. 2006;313(5794):1781–4. https://doi.org/10.1126/science.1131864.
Michel CH, Kumar S, Pinotsi D, Tunnacliffe A, St George-Hyslop P, Mandelkow E, Mandelkow EM, Kaminski CF, Kaminski Schierle GS. Extracellular monomeric tau protein is sufficient to initiate the spread of tau protein pathology. J Biol Chem. 2014;289(2):956–67. https://doi.org/10.1074/jbc.M113.515445.
Min SW, Sohn PD, Li Y, Devidze N, Johnson JR, Krogan NJ, Masliah E, Mok SA, Gestwicki JE, Gan L. SIRT1 Deacetylates Tau and reduces pathogenic Tau spread in a mouse model of tauopathy. J Neurosci. 2018;38(15):3680–8. https://doi.org/10.1523/JNEUROSCI.2369-17.2018.
Mirbaha H, Chen D, Morazova OA, Ruff KM, Sharma AM, Liu X, Goodarzi M, Pappu RV, Colby DW, Mirzaei H, Joachimiak LA, Diamond MI. Inert and seed-competent tau monomers suggest structural origins of aggregation. elife. 2018;7 https://doi.org/10.7554/eLife.36584.
Mirbaha H, Holmes BB, Sanders DW, Bieschke J, Diamond MI. Tau trimers are the minimal propagation unit spontaneously internalized to seed intracellular aggregation. J Biol Chem. 2015;290(24):14893–903. https://doi.org/10.1074/jbc.M115.652693.
Mohamed NV, Desjardins A, Leclerc N. Tau secretion is correlated to an increase of Golgi dynamics. PLoS One. 2017;12(5):e0178288. https://doi.org/10.1371/journal.pone.0178288.
Mohamed NV, Plouffe V, Remillard-Labrosse G, Planel E, Leclerc N. Starvation and inhibition of lysosomal function increased tau secretion by primary cortical neurons. Sci Rep. 2014;4:5715. https://doi.org/10.1038/srep05715.
Morales R, Duran-Aniotz C, Castilla J, Estrada LD, Soto C. De novo induction of amyloid-beta deposition in vivo. Mol Psychiatry. 2012;17(12):1347–53. https://doi.org/10.1038/mp.2011.120.
Mougenot AL, Nicot S, Bencsik A, Morignat E, Verchere J, Lakhdar L, Legastelois S, Baron T. Prion-like acceleration of a synucleinopathy in a transgenic mouse model. Neurobiol Aging. 2012;33(9):2225–8. https://doi.org/10.1016/j.neurobiolaging.2011.06.022.
Mudher A, Colin M, Dujardin S, Medina M, Dewachter I, Alavi Naini SM, Mandelkow EM, Mandelkow E, Buee L, Goedert M, Brion JP. What is the evidence that tau pathology spreads through prion-like propagation? Acta Neuropathol Commun. 2017;5(1):99. https://doi.org/10.1186/s40478-017-0488-7.
Mukrasch MD, Bibow S, Korukottu J, Jeganathan S, Biernat J, Griesinger C, Mandelkow E, Zweckstetter M. Structural polymorphism of 441-residue tau at single residue resolution. PLoS Biol. 2009;7(2):e34. https://doi.org/10.1371/journal.pbio.1000034.
Narasimhan S, Guo JL, Changolkar L, Stieber A, McBride JD, Silva LV, He Z, Zhang B, Gathagan RJ, Trojanowski JQ, Lee VMY. Pathological Tau strains from human brains recapitulate the diversity of tauopathies in nontransgenic mouse brain. J Neurosci. 2017;37(47):11406–23. https://doi.org/10.1523/JNEUROSCI.1230-17.2017.
Nicholls SB, DeVos SL, Commins C, Nobuhara C, Bennett RE, Corjuc DL, Maury E, Eftekharzadeh B, Akingbade O, Fan Z, Roe AD, Takeda S, Wegmann S, Hyman BT. Characterization of TauC3 antibody and demonstration of its potential to block tau propagation. PLoS One. 2017;12(5):e0177914. https://doi.org/10.1371/journal.pone.0177914.
Nobuhara CK, DeVos SL, Commins C, Wegmann S, Moore BD, Roe AD, Costantino I, Frosch MP, Pitstick R, Carlson GA, Hock C, Nitsch RM, Montrasio F, Grimm J, Cheung AE, Dunah AW, Wittmann M, Bussiere T, Weinreb PH, Hyman BT, Takeda S. Tau antibody targeting pathological species blocks neuronal uptake and interneuron propagation of Tau in vitro. Am J Pathol. 2017;187(6):1399–412. https://doi.org/10.1016/j.ajpath.2017.01.022.
Nonaka T, Watanabe ST, Iwatsubo T, Hasegawa M. Seeded aggregation and toxicity of {alpha}-synuclein and tau: cellular models of neurodegenerative diseases. J Biol Chem. 2010;285(45):34885–98. https://doi.org/10.1074/jbc.M110.148460.
Olsson B, Lautner R, Andreasson U, Ohrfelt A, Portelius E, Bjerke M, Holtta M, Rosen C, Olsson C, Strobel G, Wu E, Dakin K, Petzold M, Blennow K, Zetterberg H. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: a systematic review and meta-analysis. Lancet Neurol. 2016;15(7):673–84. https://doi.org/10.1016/S1474-4422(16)00070-3.
Peelaerts W, Bousset L, Van der Perren A, Moskalyuk A, Pulizzi R, Giugliano M, Van den Haute C, Melki R, Baekelandt V. Alpha-synuclein strains cause distinct synucleinopathies after local and systemic administration. Nature. 2015;522(7556):340–4. https://doi.org/10.1038/nature14547.
Peeraer E, Bottelbergs A, Van Kolen K, Stancu IC, Vasconcelos B, Mahieu M, Duytschaever H, Ver Donck L, Torremans A, Sluydts E, Van Acker N, Kemp JA, Mercken M, Brunden KR, Trojanowski JQ, Dewachter I, Lee VM, Moechars D. Intracerebral injection of preformed synthetic tau fibrils initiates widespread tauopathy and neuronal loss in the brains of tau transgenic mice. Neurobiol Dis. 2015;73:83–95. https://doi.org/10.1016/j.nbd.2014.08.032.
Petkova AT, Leapman RD, Guo Z, Yau WM, Mattson MP, Tycko R. Self-propagating, molecular-level polymorphism in Alzheimer’s beta-amyloid fibrils. Science. 2005;307(5707):262–5. https://doi.org/10.1126/science.1105850.
Piacentini R, Li Puma DD, Mainardi M, Lazzarino G, Tavazzi B, Arancio O, Grassi C. Reduced gliotransmitter release from astrocytes mediates tau-induced synaptic dysfunction in cultured hippocampal neurons. Glia. 2017;65(8):1302–16. https://doi.org/10.1002/glia.23163.
Plouffe V, Mohamed NV, Rivest-McGraw J, Bertrand J, Lauzon M, Leclerc N. Hyperphosphorylation and cleavage at D421 enhance tau secretion. PLoS One. 2012;7(5):e36873. https://doi.org/10.1371/journal.pone.0036873.
Polanco JC, Li C, Bodea LG, Martinez-Marmol R, Meunier FA, Gotz J. Amyloid-beta and tau complexity – towards improved biomarkers and targeted therapies. Nat Rev Neurol. 2018;14(1):22–39. https://doi.org/10.1038/nrneurol.2017.162.
Polydoro M, Dzhala VI, Pooler AM, Nicholls SB, McKinney AP, Sanchez L, Pitstick R, Carlson GA, Staley KJ, Spires-Jones TL, Hyman BT. Soluble pathological tau in the entorhinal cortex leads to presynaptic deficits in an early Alzheimer’s disease model. Acta Neuropathol. 2014;127(2):257–70. https://doi.org/10.1007/s00401-013-1215-5.
Pooler AM, Phillips EC, Lau DH, Noble W, Hanger DP. Physiological release of endogenous tau is stimulated by neuronal activity. EMBO Rep. 2013;14(4):389–94. https://doi.org/10.1038/embor.2013.15.
Pooler AM, Polydoro M, Maury EA, Nicholls SB, Reddy SM, Wegmann S, William C, Saqran L, Cagsal-Getkin O, Pitstick R, Beier DR, Carlson GA, Spires-Jones TL, Hyman BT. Amyloid accelerates tau propagation and toxicity in a model of early Alzheimer’s disease. Acta Neuropathol Commun. 2015;3:14. https://doi.org/10.1186/s40478-015-0199-x.
Probst A, Tolnay M, Langui D, Goedert M, Spillantini MG. Pick’s disease: hyperphosphorylated tau protein segregates to the somatoaxonal compartment. Acta Neuropathol. 1996;92(6):588–96.
Prusiner SB. Novel proteinaceous infectious particles cause scrapie. Science. 1982;216(4542):136–44.
Rajendran L, Bali J, Barr MM, Court FA, Kramer-Albers EM, Picou F, Raposo G, van der Vos KE, van Niel G, Wang J, Breakefield XO. Emerging roles of extracellular vesicles in the nervous system. J Neurosci. 2014;34(46):15482–9. https://doi.org/10.1523/JNEUROSCI.3258-14.2014.
Rajendran L, Honsho M, Zahn TR, Keller P, Geiger KD, Verkade P, Simons K. Alzheimer’s disease beta-amyloid peptides are released in association with exosomes. Proc Natl Acad Sci U S A. 2006;103(30):11172–7. https://doi.org/10.1073/pnas.0603838103.
Rauch JN, Chen JJ, Sorum AW, Miller GM, Sharf T, See SK, Hsieh-Wilson LC, Kampmann M, Kosik KS. Tau internalization is regulated by 6-O sulfation on heparan sulfate proteoglycans (HSPGs). Sci Rep. 2018;8(1):6382. https://doi.org/10.1038/s41598-018-24904-z.
Rebeck GW, Hyman BT. Neuroanatomical connections and specific regional vulnerability in Alzheimer’s disease. Neurobiol Aging. 1993;14(1):45–7; discussion 55-46
Reilly P, Winston CN, Baron KR, Trejo M, Rockenstein EM, Akers JC, Kfoury N, Diamond M, Masliah E, Rissman RA, Yuan SH. Novel human neuronal tau model exhibiting neurofibrillary tangles and transcellular propagation. Neurobiol Dis. 2017;106:222–34. https://doi.org/10.1016/j.nbd.2017.06.005.
Rodriguez L, Mohamed NV, Desjardins A, Lippe R, Fon EA, Leclerc N. Rab7A regulates tau secretion. J Neurochem. 2017;141(4):592–605. https://doi.org/10.1111/jnc.13994.
Saito Y, Ruberu NN, Sawabe M, Arai T, Tanaka N, Kakuta Y, Yamanouchi H, Murayama S. Staging of argyrophilic grains: an age-associated tauopathy. J Neuropathol Exp Neurol. 2004;63(9):911–8.
Saman S, Kim W, Raya M, Visnick Y, Miro S, Saman S, Jackson B, McKee AC, Alvarez VE, Lee NC, Hall GF. Exosome-associated tau is secreted in tauopathy models and is selectively phosphorylated in cerebrospinal fluid in early Alzheimer disease. J Biol Chem. 2012;287(6):3842–9. https://doi.org/10.1074/jbc.M111.277061.
Sanders DW, Kaufman SK, DeVos SL, Sharma AM, Mirbaha H, Li A, Barker SJ, Foley AC, Thorpe JR, Serpell LC, Miller TM, Grinberg LT, Seeley WW, Diamond MI. Distinct tau prion strains propagate in cells and mice and define different tauopathies. Neuron. 2014;82(6):1271–88. https://doi.org/10.1016/j.neuron.2014.04.047.
Santa-Maria I, Varghese M, Ksiezak-Reding H, Dzhun A, Wang J, Pasinetti GM. Paired helical filaments from Alzheimer disease brain induce intracellular accumulation of Tau protein in aggresomes. J Biol Chem. 2012;287(24):20522–33. https://doi.org/10.1074/jbc.M111.323279.
Santacruz K, Lewis J, Spires T, Paulson J, Kotilinek L, Ingelsson M, Guimaraes A, DeTure M, Ramsden M, McGowan E, Forster C, Yue M, Orne J, Janus C, Mariash A, Kuskowski M, Hyman B, Hutton M, Ashe KH. Tau suppression in a neurodegenerative mouse model improves memory function. Science. 2005;309(5733):476–81. https://doi.org/10.1126/science.1113694.
Schwarz AJ, Yu P, Miller BB, Shcherbinin S, Dickson J, Navitsky M, Joshi AD, Devous MD Sr, Mintun MS. Regional profiles of the candidate tau PET ligand 18F-AV-1451 recapitulate key features of Braak histopathological stages. Brain. 2016;139(Pt 5):1539–50. https://doi.org/10.1093/brain/aww023.
Sepulcre J, Grothe MJ, d’Oleire Uquillas F, Ortiz-Teran L, Diez I, Yang HS, Jacobs HIL, Hanseeuw BJ, Li Q, El-Fakhri G, Sperling RA, Johnson KA. Neurogenetic contributions to amyloid beta and tau spreading in the human cortex. Nat Med. 2018; https://doi.org/10.1038/s41591-018-0206-4.
Silva JM, Rodrigues S, Sampaio-Marques B, Gomes P, Neves-Carvalho A, Dioli C, Soares-Cunha C, Mazuik BF, Takashima A, Ludovico P, Wolozin B, Sousa N, Sotiropoulos I. Dysregulation of autophagy and stress granule-related proteins in stress-driven Tau pathology. Cell Death Differ. 2018; https://doi.org/10.1038/s41418-018-0217-1.
Simon D, Garcia-Garcia E, Royo F, Falcon-Perez JM, Avila J. Proteostasis of tau. Tau overexpression results in its secretion via membrane vesicles. FEBS Lett. 2012;586(1):47–54. https://doi.org/10.1016/j.febslet.2011.11.022.
Smolek T, Jadhav S, Brezovakova V, Cubinkova V, Valachova B, Novak P, Zilka N. First-in-rat study of human Alzheimer’s disease Tau propagation. Mol Neurobiol. 2018; https://doi.org/10.1007/s12035-018-1102-0.
Sokolow S, Henkins KM, Bilousova T, Gonzalez B, Vinters HV, Miller CA, Cornwell L, Poon WW, Gylys KH. Pre-synaptic C-terminal truncated tau is released from cortical synapses in Alzheimer’s disease. J Neurochem. 2015;133(3):368–79. https://doi.org/10.1111/jnc.12991.
Sowinski S, Jolly C, Berninghausen O, Purbhoo MA, Chauveau A, Kohler K, Oddos S, Eissmann P, Brodsky FM, Hopkins C, Onfelt B, Sattentau Q, Davis DM. Membrane nanotubes physically connect T cells over long distances presenting a novel route for HIV-1 transmission. Nat Cell Biol. 2008;10(2):211–9. https://doi.org/10.1038/ncb1682.
Stancu IC, Vasconcelos B, Ris L, Wang P, Villers A, Peeraer E, Buist A, Terwel D, Baatsen P, Oyelami T, Pierrot N, Casteels C, Bormans G, Kienlen-Campard P, Octave JN, Moechars D, Dewachter I. Templated misfolding of Tau by prion-like seeding along neuronal connections impairs neuronal network function and associated behavioral outcomes in Tau transgenic mice. Acta Neuropathol. 2015;129(6):875–94. https://doi.org/10.1007/s00401-015-1413-4.
Stohr J, Watts JC, Mensinger ZL, Oehler A, Grillo SK, DeArmond SJ, Prusiner SB, Giles K. Purified and synthetic Alzheimer’s amyloid beta (Abeta) prions. Proc Natl Acad Sci U S A. 2012;109(27):11025–30. https://doi.org/10.1073/pnas.1206555109.
Stopschinski BE, Holmes BB, Miller GM, Manon VA, Vaquer-Alicea J, Prueitt WL, Hsieh-Wilson LC, Diamond MI. Specific glycosaminoglycan chain length and sulfation patterns are required for cell uptake of tau versus alpha-synuclein and beta-amyloid aggregates. J Biol Chem. 2018;293(27):10826–40. https://doi.org/10.1074/jbc.RA117.000378.
Takahashi M, Miyata H, Kametani F, Nonaka T, Akiyama H, Hisanaga S, Hasegawa M. Extracellular association of APP and tau fibrils induces intracellular aggregate formation of tau. Acta Neuropathol. 2015;129(6):895–907. https://doi.org/10.1007/s00401-015-1415-2.
Takeda S, Wegmann S, Cho H, DeVos SL, Commins C, Roe AD, Nicholls SB, Carlson GA, Pitstick R, Nobuhara CK, Costantino I, Frosch MP, Muller DJ, Irimia D, Hyman BT. Neuronal uptake and propagation of a rare phosphorylated high-molecular-weight tau derived from Alzheimer’s disease brain. Nat Commun. 2015;6:8490. https://doi.org/10.1038/ncomms9490.
Tang Z, Ioja E, Bereczki E, Hultenby K, Li C, Guan Z, Winblad B, Pei JJ. mTor mediates tau localization and secretion: implication for Alzheimer’s disease. Biochim Biophys Acta. 2015;1853(7):1646–57. https://doi.org/10.1016/j.bbamcr.2015.03.003.
Tardivel M, Begard S, Bousset L, Dujardin S, Coens A, Melki R, Buee L, Colin M. Tunneling nanotube (TNT)-mediated neuron-to neuron transfer of pathological Tau protein assemblies. Acta Neuropathol Commun. 2016;4(1):117. https://doi.org/10.1186/s40478-016-0386-4.
Telling GC, Parchi P, DeArmond SJ, Cortelli P, Montagna P, Gabizon R, Mastrianni J, Lugaresi E, Gambetti P, Prusiner SB. Evidence for the conformation of the pathologic isoform of the prion protein enciphering and propagating prion diversity. Science. 1996;274(5295):2079–82.
Usenovic M, Niroomand S, Drolet RE, Yao L, Gaspar RC, Hatcher NG, Schachter J, Renger JJ, Parmentier-Batteur S. Internalized Tau oligomers cause neurodegeneration by inducing accumulation of pathogenic Tau in human neurons derived from induced pluripotent stem cells. J Neurosci. 2015;35(42):14234–50. https://doi.org/10.1523/JNEUROSCI.1523-15.2015.
Varghese M, Santa-Maria I, Ho L, Ward L, Yemul S, Dubner L, Ksiezak-Reding H, Pasinetti GM. Extracellular Tau paired helical filaments differentially affect Tau pathogenic mechanisms in mitotic and post-mitotic cells: implications for mechanisms of Tau propagation in the brain. J Alzheimers Dis. 2016;54(2):477–96. https://doi.org/10.3233/JAD-160166.
Vasconcelos B, Stancu IC, Buist A, Bird M, Wang P, Vanoosthuyse A, Van Kolen K, Verheyen A, Kienlen-Campard P, Octave JN, Baatsen P, Moechars D, Dewachter I. Heterotypic seeding of Tau fibrillization by pre-aggregated Abeta provides potent seeds for prion-like seeding and propagation of Tau-pathology in vivo. Acta Neuropathol. 2016;131(4):549–69. https://doi.org/10.1007/s00401-015-1525-x.
Verny M, Jellinger KA, Hauw JJ, Bancher C, Litvan I, Agid Y. Progressive supranuclear palsy: a clinicopathological study of 21 cases. Acta Neuropathol. 1996;91(4):427–31.
Volpicelli-Daley LA, Luk KC, Patel TP, Tanik SA, Riddle DM, Stieber A, Meaney DF, Trojanowski JQ, Lee VM. Exogenous alpha-synuclein fibrils induce Lewy body pathology leading to synaptic dysfunction and neuron death. Neuron. 2011;72(1):57–71. https://doi.org/10.1016/j.neuron.2011.08.033.
Walker LC, Levine H 3rd, Mattson MP, Jucker M. Inducible proteopathies. Trends Neurosci. 2006;29(8):438–43. https://doi.org/10.1016/j.tins.2006.06.010.
Wang Y, Balaji V, Kaniyappan S, Kruger L, Irsen S, Tepper K, Chandupatla R, Maetzler W, Schneider A, Mandelkow E, Mandelkow EM. The release and trans-synaptic transmission of Tau via exosomes. Mol Neurodegener. 2017;12(1):5. https://doi.org/10.1186/s13024-016-0143-y.
Wegmann S, Bennett RE, Amaral AS, Hyman BT. Studying tau protein propagation and pathology in the mouse brain using adeno-associated viruses. Methods Cell Biol. 2017;141:307–22. https://doi.org/10.1016/bs.mcb.2017.06.014.
Wegmann S, Maury EA, Kirk MJ, Saqran L, Roe A, DeVos SL, Nicholls S, Fan Z, Takeda S, Cagsal-Getkin O, William CM, Spires-Jones TL, Pitstick R, Carlson GA, Pooler AM, Hyman BT. Removing endogenous tau does not prevent tau propagation yet reduces its neurotoxicity. EMBO J. 2015;34(24):3028–41. https://doi.org/10.15252/embj.201592748.
Williams DR, Holton JL, Strand C, Pittman A, de Silva R, Lees AJ, Revesz T. Pathological tau burden and distribution distinguishes progressive supranuclear palsy-parkinsonism from Richardson’s syndrome. Brain. 2007;130(Pt 6):1566–76. https://doi.org/10.1093/brain/awm104.
Woerman AL, Aoyagi A, Patel S, Kazmi SA, Lobach I, Grinberg LT, McKee AC, Seeley WW, Olson SH, Prusiner SB. Tau prions from Alzheimer’s disease and chronic traumatic encephalopathy patients propagate in cultured cells. Proc Natl Acad Sci U S A. 2016;113(50):E8187–96. https://doi.org/10.1073/pnas.1616344113.
Wu JW, Herman M, Liu L, Simoes S, Acker CM, Figueroa H, Steinberg JI, Margittai M, Kayed R, Zurzolo C, Di Paolo G, Duff KE. Small misfolded Tau species are internalized via bulk endocytosis and anterogradely and retrogradely transported in neurons. J Biol Chem. 2013;288(3):1856–70. https://doi.org/10.1074/jbc.M112.394528.
Wu JW, Hussaini SA, Bastille IM, Rodriguez GA, Mrejeru A, Rilett K, Sanders DW, Cook C, Fu H, Boonen RA, Herman M, Nahmani E, Emrani S, Figueroa YH, Diamond MI, Clelland CL, Wray S, Duff KE. Neuronal activity enhances tau propagation and tau pathology in vivo. Nat Neurosci. 2016;19(8):1085–92. https://doi.org/10.1038/nn.4328.
Yamada K, Holth JK, Liao F, Stewart FR, Mahan TE, Jiang H, Cirrito JR, Patel TK, Hochgrafe K, Mandelkow EM, Holtzman DM. Neuronal activity regulates extracellular tau in vivo. J Exp Med. 2014;211(3):387–93. https://doi.org/10.1084/jem.20131685.
Yanamandra K, Kfoury N, Jiang H, Mahan TE, Ma S, Maloney SE, Wozniak DF, Diamond MI, Holtzman DM. Anti-tau antibodies that block tau aggregate seeding in vitro markedly decrease pathology and improve cognition in vivo. Neuron. 2013;80(2):402–14. https://doi.org/10.1016/j.neuron.2013.07.046.
Yonetani M, Nonaka T, Masuda M, Inukai Y, Oikawa T, Hisanaga S, Hasegawa M. Conversion of wild-type alpha-synuclein into mutant-type fibrils and its propagation in the presence of A30P mutant. J Biol Chem. 2009;284(12):7940–50. https://doi.org/10.1074/jbc.M807482200.
Yuyama K, Yamamoto N, Yanagisawa K. Accelerated release of exosome-associated GM1 ganglioside (GM1) by endocytic pathway abnormality: another putative pathway for GM1-induced amyloid fibril formation. J Neurochem. 2008;105(1):217–24. https://doi.org/10.1111/j.1471-4159.2007.05128.x.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Dujardin, S., Hyman, B.T. (2019). Tau Prion-Like Propagation: State of the Art and Current Challenges. In: Takashima, A., Wolozin, B., Buee, L. (eds) Tau Biology. Advances in Experimental Medicine and Biology, vol 1184. Springer, Singapore. https://doi.org/10.1007/978-981-32-9358-8_23
Download citation
DOI: https://doi.org/10.1007/978-981-32-9358-8_23
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-32-9357-1
Online ISBN: 978-981-32-9358-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)