
Abstract
Schizophrenia is a chronic manic-depressive illness. It is a mental illness characterized by a combination of symptoms such as perceptual misinterpretation, cognitive impairment, and emotional dysfunction. Schizophrenia is a serious mental illness that affects various parts of the brain. “A majority of individuals with schizophrenia have poor insight regarding the fact that they have a psychotic illness, “ says the DSM (Diagnostic and Statistical Manual of Mental Disorders). There are a myriad of symptoms associated with schizophrenia illness, arising from different basis. Hence, it adds slight complexity to its further diagnosis. Symptoms must last 6 months and include at least 1 month of active symptoms for an accurate diagnosis. For a precise diagnosis, several clinical symptoms, including physical, psychiatric, and psychological indicators, must be evaluated. Clinical examination includes a variety of tests to diagnose, including blood tests and medical imaging. Combinatorial methods can be used to make accurate diagnoses. Considering the neurochemical changes in mental disorders, identification of biomarkers in psychiatry is becoming increasingly important in order to facilitate diagnosis. The International Classification of Diseases, eleventh revision, has also adopted standardized criteria (ICD-11) for specific Schizophrenia diagnosis. Various diagnostic tests, such as MRIs, CT scans, and blood tests, are usually performed to assess the patient’s health. With the aid of diagnostic tool, several causative factors in schizophrenia pathophysiology have been identified. It is providing a more promising future for easy and safe diagnosis of schizophrenic patient. To achieve even greater improvements in patient care, psychiatrists and researchers synchronized work contributes to improving and developing modified medicine tools.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Schizophrenia is a chronic manic-depressive illness. It is a mental illness characterized by a combination of symptoms such as perceptual misinterpretation, cognitive impairment, and emotional dysfunction. Schizophrenia is a serious mental illness that affects various parts of the brain. “A majority of individuals with schizophrenia have poor insight regarding the fact that they have a psychotic illness, “ says the DSM (Diagnostic and Statistical Manual of Mental Disorders). There are a myriad of symptoms associated with schizophrenia illness, arising from different basis. Hence, it adds slight complexity to its further diagnosis. Symptoms must last 6 months and include at least 1 month of active symptoms for an accurate diagnosis. For a precise diagnosis, several clinical symptoms, including physical, psychiatric, and psychological indicators, must be evaluated. Clinical examination includes a variety of tests to diagnose, including blood tests and medical imaging. Combinatorial methods can be used to make accurate diagnoses. Considering the neurochemical changes in mental disorders, identification of biomarkers in psychiatry is becoming increasingly important in order to facilitate diagnosis. The International Classification of Diseases, eleventh revision, has also adopted standardized criteria (ICD-11) for specific Schizophrenia diagnosis. Various diagnostic tests, such as MRIs, CT scans, and blood tests, are usually performed to assess the patient’s health. With the aid of diagnostic tool, several causative factors in schizophrenia pathophysiology have been identified. It is providing a more promising future for easy and safe diagnosis of schizophrenic patient. To achieve even greater improvements in patient care, psychiatrists and researchers synchronized work contributes to improving and developing modified medicine tools.
4.1 Introduction
Initially, the term schizophrenia was introduced in the year 1911 but it took 70 years to consider schizophrenia under the category of disease as per the Diagnostic and Statistical Manual of Mental Disorders—third edition (DSM-III) (Tomasik et al. 2012). The term Schizophrenia is derived from the Greek origin, “schizo” (splitting) and “phren” (mind). Swiss psychiatrist Dr. Eugen Bleuler coined the term “Schizophrenia” and in 1911 emphasized the word schizophrenia that, dementia praecox nothing but schizophrenia as it causes differentiation in psychic functions (Ashok et al. 2012).
Mental disorders are usually associated with high risk rate of its occurrence, death, morbidity, and mental instability as per World Health Organization. Schizophrenia is a difficult brain disorder that makes it challenging to distinguish between what is real and what is not, to think clearly, manage emotions, relate to others, and function normally.
L. Bender, Boston psychiatrist and neuropathologist, described schizophrenia as “congenital encephalopathy” (Weinberger and Levitt 2011). It affects human perception by affecting person behavior, thinking, and vision toward the world. Loss of coordination in neurological function leads to a chronic mental health disorder called as Schizophrenia. It is a psychological illness in which people seem like they have lost touch with the fact and are in schizotypal state. The exact cause of schizophrenia is not known, but a blend of causes of schizophrenia is associated with Genes, Environment, or Change in Brain Structures (Sawa and Snyder 2002). It is characterized by symptoms such as delusions, hallucinations, disorganized speech or behavior, and impaired cognitive ability (Chatterjee 2018; Chatterjee and Mittal 2019).
Difficulty can be associated with concentration and memory. Treatment is usually life-long and often involves a combination of medications, psychotherapy, and coordinated specialty care services. Symptoms may persist long when untreated but when treated in a coordinated manner, it can help individuals to carry out normal schedule as a normal and healthy volunteer. As suggested by L. Bende psychiatric disorders are also influenced by environmental factors such as institutional care and non-friendly behavior (Walter et al. 2010). These types of environmental factors affect psychological development and lead to psychological disorder.
Diagnosis is totally dependent on symptoms for the complete estimation of the disorder under its clinical manifestation.
4.2 Clinical Manifestations
Schizophrenia symptoms are categorized mainly into three types,
4.2.1 Positive
Positive symptoms are identified and distinguished from healthy individuals. The symptoms include hallucinations, delusions, and abnormal motor behavior with varying degrees of severity.
4.2.2 Negative
Negative symptoms are associated with high morbidity rate and usually not easily identify. The negative symptoms included avolition, alogia, anhedonia, and diminished emotional expression.
4.2.3 Cognitive
Cognitive refers to conscious intellectual activity (such as reasoning or remembering). And cognitive symptoms involve hampering conscious intellectual activity. These ultimately lead to impairment in the individual’s communication skills by affecting speech and responsiveness. Usually impairment is observed in attentiveness, focus of mind, and memory.
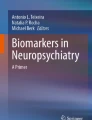
Schizophrenia appears in numerous forms. Common types of symptoms include person who hears voices and has extreme fear, or feelings that are unusual and unnatural. Dopamine excessive secretion via secretory neurons is associated with schizophrenia. Drugs that are treating schizophrenia like chlorpromazine, haloperidol, and thiothixene either decrease secretion of dopamine at dopaminergic nerve endings or decrease the effect of dopamine on neurons (Guyton and Hall 2006). Various neurotransmitters such as γ-aminobutyric acid (GABA), glutamate, dopamine, serotonin, and oxytocin contribute the most in causing schizophrenia, among this major role is played by dopamine (Bansal and Chatterjee 2021). These are chemical messengers in the body, used by nervous system to communicate between neurons or from neurons to muscles. Neurotransmitters play an important role in neurodevelopmental disorders. As depicted in (Fig. 4.1) the progression of schizophrenia can be divided into four stages via neurotransmitter interference (Insel and Cuthbert 2010; Bansal and Chatterjee 2021). The figure specifies and represents about clinical symptoms with its diagnosis.

The four stages describing progression of schizophrenia
The authors conducted a literature review and discussed the roles of dopamine and glutamate in schizophrenia, including loss of senses, motion, memory, and depression. A low level dopamine amount is usually linked to brain disorders, including schizophrenia (Birtwistle and Baldwin 1998; Bansal and Chatterjee 2021). Though, the patient also experiences physical changes such as weight gain or loss, diabetes, and suicidal thoughts. The feature of this stage is behavior reappearance, which can be diagnosed through a clinical interview.
4.3 Rationale
Due to the heterogeneity of this mental disorder and the lack of specific effective biomarkers, diagnosing SZ is a difficult problem. Several clinical symptoms, including physical, psychiatric, and psychological indicators, must be assessed for appropriate diagnosis. To diagnose, clinical examination includes a variety of tests, including blood tests and medical imaging. The combinatorial methods can be implemented for efficient diagnosis.
4.4 Diagnosis
For appropriate treatment prior diagnosis of this mental disorder is essential. Schizophrenia is a heterogenic mental illness that requires accurate diagnosis (Shepherd et al. 2012). There are accurate methods available for care and recover of people with schizophrenia. Efficient feature selection techniques result in high classification accuracy as well as improved identification of affected brain regions (Chatterjee et al. 2019). Hence it is really essential to diagnose the symptoms of schizophrenia as soon as possible for effective care and treatment. The manual DSM-5 elaborates that schizophrenia diagnosis will be based on its symptoms. Clinicians or researchers corelate patients’ symptoms with the standard reference book or manual called Diagnostic and Statistical Manual of Mental Disorders (DSM-5) Fifth Edition, published under American Psychiatric Association (APA), where APA is national medical specialty society ensuring access to excellence for psychiatric diagnosis and treatment (APA, DSM-5, 2022). As per the guidelines provided by DSM-5, schizophrenia is diagnosed on the basis of two or more symptoms resembling, hallucinations, delusions, or disorganized speech for minimum 1 month. The other essential symptoms associated are gross disorganization and reduced emotional expression.
Further DSM-5 criteria for diagnosis of schizophrenia comprise:
-
Initially, work performance personal care is getting diminished before the onset of symptoms.
-
Indications of disturbance lasted for minimum 6 months.
-
Depressive or bipolar disorder with psychotic symptoms, as well as schizoaffective disorder, has been weeded out.
The disturbance is not the result of any substance or another medical/health condition.
The International Classification of Diseases, eleventh revision, has also adopted standardized criteria (ICD-11) for specific diagnosis of schizophrenia (First et al. 2015). The International Classification of Diseases and Related Health Problems (ICD) works for maintaining international health reporting and information standard under the ambience of World Health Organization (WHO). ICD-10 diagnostic guidelines, each disorder’s diagnostic information is generally divided into three sections. The first section describes the main clinical features as well as “any important but less specific associated features.” The second section contains “Diagnostic Guidelines, “ which “indicate the number and balance of symptoms usually required before a confident diagnosis can be made.“ The third section, “Differential Diagnosis, “ lists other ICD-10 disorders that must be distinguished from the disorder under consideration.
The inconsistency of the diagnostic details included in the ICD-10 Clinical Descriptions and Diagnostic Guidelines (CDDG), particularly with regard to differential diagnosis, is a significant shortcoming in terms of its usefulness to clinicians.
As a result, ICD-11 Working Groups were tasked with compiling data using standardized template, for providing diagnostic information about the disorders under their purview (known as a “Content Form”). The ICD-11 CDDG is being developed with a uniform structure utilizing the information provided in the Content Forms as basis of the information. This format is effective in producing more reliable clinical judgments in ICD-11 in comparison with ICD-10 and hence is currently being tested in a series of Internet-based field studies using standardized case material, and it will also be tested in clinical settings. For example, the proposed ICD-11 diagnosis of schizophrenia requires the occurrence of at least two of seven symptoms for at least 1 month. Although statements about the duration of symptoms are frequently included (for example, the diagnostic guidelines for schizophrenia state that “symptoms should have been clearly present for the majority of the time during a period of one month or more”).
Guidelines also elaborate about individuals diagnosed with schizophrenia and bipolar disorder have a high prevalence rate of PTSD. Post-traumatic stress disorder (PTSD) is associated with condition that advances as a result of witnessing a highly threatening or horrific event or series of events. Anger, shame, sadness, humiliation, or guilt, including survivor guilt, is the common symptom of PTSD (First et al. 2015). Schizophrenia results in psychosis and is associated with considerable disability and may affect all areas of life including personal, family, social, educational, and occupational functioning. The first-episode psychosis usually appears between age 16 and 30 and is considered as part of diagnosis, where psychosis is the state of mind indulging person to lose contact with reality and affecting his ability to differentiate between fact and fallacy. Such circumstances are classified under psychotic episodes. National Institute of Mental Health (NIMH) reports on U.S data for about 100,000 new cases per year for psychosis. Schizophrenia causes psychosis and it may hinder person’s personal, social and professional life as well.
The diagnosis of schizophrenia can be efficiently achieved with the help of studying various parameters comprising of medical history, functional and structural neuroimaging techniques, clinical and physical examination. As per the mental or physical symptoms of the patient, physicians decide medical history and physical examination. Usually various diagnostic tests like MRI or CT scans or blood tests are performed to analyze health condition of the patient. If the physical symptoms are not in accordance, then physician may recommend a psychiatrist or psychologist, healthcare professionals, those are professionally fully trained for further counseling, guidance, diagnosis, and treat mental illnesses where clinical examination comprises blood tests as well as medical imaging (Tomasik et al. 2012).
Schizophrenia basically associated with brain and hence classified as brain disorder, but recently due to its impact on peripheral systems it is also categorized under systemic disorder. The changes are usually associated with cerebrospinal fluid, liver, and skin cells of patients. Blood is such a fluid component of the body that circulates throughout. Hence, blood samples can be easily retrieved without much clinical interventions and considering patients comfort. It is usually carrying molecule those are balancing activity of both central and peripheral purposes. Hence blood may still be a useful component for diagnostic, or certain monitoring purposes as it reflects any change associated with human physiology. Blood of the patient is usually tested for molecular changes in metabolic, immune, and hormonal pathways occurring in schizophrenia patients. These altered molecules lead to high accuracy in diagnosis. Blood samples of schizophrenia patients show considerable changes that are used for diagnosis.
There are certain biomarkers expressed in blood, specific for particular genotype of patient and are responsible for diagnosis and therapeutics (Tomasik et al. 2012). To specify the indication of biological material the term “biomarker” was first introduced in 1973. Biomarkers are biological molecules, genes, or such a molecule that is associated with any sort of clinical condition to be identified. These molecules are usually found in blood, other body fluids, or tissues of the patient. The Biomarker Definition Working Group, which was funded by the National Institutes of Health (NIH), defined a biomarker as “a characteristic that is objectively measured and evaluated as an indication of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention” in 2000.
The concept of biomarkers was further elaborated by Fitzgerald and colleagues in the year 2016 as a molecule having functional variability that acts as a marker or indicator of disease or response to therapy (Fitz Gerald 2016). Recently, science and technology has supreme opportunity to scrutinize inflammation as a potential biomarker in schizophrenia. For a broad range and complete analysis, a set of vivid types of biomarkers may be needed for precise diagnosis along with the application of advance technology such as combination of genomic, proteomic, and immunoassay technologies. Usually, most common biomarker associated with this disorder is inflammatory response. Inflammation can serve as a potential biomarker in schizophrenia as it is a set cascade of reactions to various stimuli, involving activation of immune system, influx of blood, vascularization, and recruitment of mediators such as cytokines, complement activation (Miller and Goldsmith 2019). Inflammation is an indicator of autoimmune disorders and severe infections, enhancing the risk of schizophrenia (Benros et al. 2014). Evidence proves about schizophrenia patients show inflammatory marker as anomalies in blood samples, cerebrospinal fluid (CSF), and central nervous system (CNS), including leukocytes, cytokines, and acute phase reactants (Kirkpatrick and Miller 2013; Mazza et al. 2019). A large number of inflammatory markers, including interferon gamma (IFN-g), IL-1b, IL-1 receptor antagonist (IL-1RA), IL-6, IL-8, IL-10, IL-12, were found to be elevated in a recent meta-analysis of first-episode psychosis (FEP) and chronic individuals with psychosis (Goldsmith et al. 2016).
It has been practically proven that non-steroidal anti-inflammatory drugs (NSAIDs) or other agents with anti-inflammatory effects may help improve mental illness in certain schizophrenia patients (Nitta et al. 2013; Sommer et al. 2014). Hence presence of inflammatory markers in the blood may act as an indication of response to such agents. Considering this finding, it suggests that inflammation may be involved in the pathogenesis of schizophrenia, at least in some patients, and is thus a candidate biomarker for a variety of disorder-related phenomena. The exposure to various sources of infection including prenatal maternal, viral, bacterial infection (Brown et al. 2010) as well as exposure to the parasite Toxoplasma gondii acts as a risk factor (Torrey et al. 2007). These risk factors converge toward schizophrenia via common inflammatory response. The risk factors are considered as progenitors of schizophrenia. Detecting inflammatory biomarkers for individuals at clinical high risk (CHR) for psychosis is critical, because they may serve as important diagnostic, prognostic, and theranostic predictors. Individuals with CHR are a diverse group (Fusar-Poli et al. 2017). As per the estimation made within 2 years, approximately 20% of CHR individuals convert to a first-episode psychosis (FEP). Finally, understanding the role of inflammatory biomarkers in treatment response, as well as their relationship with specific psychotic symptoms, may provide important data to support a putative causal role for the immune system in psychosis.
A recent meta-analysis provided the first systematic evidence for changes in inflammatory markers in CHR patients versus healthy controls (HC) (Park and Miller 2019). In seven studies that looked at 10 cytokines and the acute phase reactant, CRP or “C-reactive protein,” IL-6 was found to be significantly elevated and IL-1b was found to be significantly decreased in CHR patients compared to healthy controls (Delaney et al. 2019; Focking et al. 2016).
Meta-analysis estimated risk associated with schizophrenia enhances due to elevated level of inflammatory markers like in maternal blood circulation CRP, IL-8, and IL-10 during pregnancy (Zhang et al. 2018). It is especially common in medicine and epidemiology, where it is frequently used to combine results from observational studies, guide policy decisions, and help determine the efficacy of medical interventions. Meta-analysis focuses on, reviewing and quantitative analysis and synthesis of raw data, Gene V Glass is a statistician and social scientist from the USA. He introduced the term “meta-analysis” and initiated using it in his presidential address to the American Educational Research Association in April 1976 in San Francisco.
For instance, a meta-analysis of 40 published data was performed to determine the magnitude and direction of the relationship, or effect size, between insight and symptom domains in schizophrenia, as well as moderator variables associated with the variations in effect sizes across studies. According to the discoveries of this meta-analysis, in schizophrenia, the relationships between insight and symptom domains are significant but modest. To summarize, the findings revealed a negative relationship between insight and global, positive, and negative symptomatology, implying that as global, positive, and negative symptoms increased, so did the degree of insight. In schizophrenia, there was an affirmative correlation between insight and depressive symptoms, implying that as the level of insight increased, so did the level of depressive symptoms. The findings of this meta-analysis have far-reaching implications for future research. The relationship between insight and symptoms has been studied extensively, and meta-analytic results indicate that, while statistically significant, these relationships are only moderate at best (Mintz et al. 2003). Certain comorbid infections are linked to schizophrenia and have a higher prevalence. Schizophrenia is also linked to an increased risk of death from infectious diseases such as pneumonia and influenza (Saha et al. 2007). A variety of different infectious agents have been linked to an increased risk of schizophrenia (Brown and Derkits 2010).
Lower urinary tract infections (UTIs) were found to be more common in schizophrenia patients, particularly during episodes of illness exacerbation, and this may be a recurring phenomenon. Recurrent urinary tract infections have also been reported in acute psychosis or during an acute relapse of schizophrenia (Laney et al. 2015; Miller et al. 2013). In a meta-analysis, it was discovered a 1.7-fold increase in the jeopardy of positive T. gondii IgM antibodies—a marker of acute/recent exposure or reinfection—in patients with acute psychosis (especially exacerbations of chronic schizophrenia) compared to controls. Most previous research has concentrated on T. gondii IgG Immunoglobulins, which are a marker of lifetime toxoplasmosis exposure, whereas IgM antibodies are a marker of acute/recent infection. Toxoplasma gondii (T. gondii) exposure is a strong risk factor for schizophrenia.
In this study by Monroe et al. (2015), meta-analysis was carried out to find relationship between T. gondii IgM antibodies and acute psychosis in schizophrenia to see if infections were involved with relapse in schizophrenia, also increased seroprevalence of T. gondii, antibodies were found in patients with acute psychosis who were compared to controls. An augmented seroprevalence of T. gondii IgM in patients with acute psychosis adds to and expands on previous findings, implying that infections may play a role in the etiopathophysiology of relapse in some patients with schizophrenia (Monroe et al. 2015). In each study, data were extracted for sample size and the number of subjects seropositive for T. gondii IgM antibodies for acute psychosis and controls. Hence the data is relevant for the serodiagnosis that comprises diagnosis based on the study of blood sera in relevance with the meta-analysis, thus making diagnosis and coprevalence of other symptomatic infection with schizophrenia. Several other studies have discovered an increased prevalence of active viral and chlamydial infections in hospitalized patients suffering from acute psychosis (Ahokas et al. 1987). From the analysis of Fellerhoff et al. the data showed 9.4-fold increased risk of chlamydial infection in 72 schizophrenia patients compared to 225 controls (Fellerhoff et al. 2007). The current study’s findings suggest a link between T. gondii, C. trachomatis infection, and schizophrenia. More research is needed in the future to determine the relationship between the two types of infection and schizophrenia (Park et al. 2012).
Past and ongoing neuroimaging studies have found morphological brain alterations in schizophrenia, and magnetic resonance spectroscopy (MRS) studies have revealed about changes in living brain chemistry and molecular alterations in schizophrenia. For the purpose of diagnosis standardized tools and techniques are described as follows.
4.5 Magnetic Resonance Spectroscopy (MRS) for Schizophrenia
Ackerman et al. initiated in vivo MRS, being a non-invasive technique that provides useful information about brain chemistry (Ackerman et al. 1980). The most commonly used cores for in vivo studies comprises 31P and ‘H. 31PMRS is particularly well suited for studying neurodevelopmental aspects of schizophrenia pathophysiology by measuring phosphorus-containing metabolites, where the stable isotope of phosphorus is phosphorus-31 for the study. 31P MRS can be used in the brain as part of a clinical protocol to provide accurate measurements of crucial metabolites (Novak et al. 2014). There is mounting evidence that schizophrenia is associated with abnormalities in the composition and metabolism of cell membrane phospholipids (PLs) in the brain. In schizophrenia, 31P MRS was used to measure the metabolic precursors and degradation products of PL metabolism (Komoroski et al. 2008). Metabolite ratios were quantified precisely enough to detect significant differences between brain regions. Using high-resolution (Fusar-Poli et al. 2017) P NMR spectroscopy, the absolute concentrations of the individual PL metabolites phosphocholine (pc), glycerophosphocholine (gpc), phosphoethanolamine (pe), and glycerophosphoethanolamine tissue from frontal, temporal, and occipital cortex of brain for schizophrenia were determined. Pettegrew et al. discovered reduced PMEs (phosphomonoester) and elevated (phosphodiester) PDEs in the dorsal prefrontal cortex of drug-naive schizophrenics in their groundbreaking study (Pettegrew et al. 1991). Since then, most studies have found lower PMEs and higher PDEs in first-episode schizophrenia. PMEs are reduced in chronic, schizophrenia, but the results for PDEs are differing.
Tissue samples are extracted using a modified Bligh–Dyer method (Bligh and Dyer 1959). In this method brain tissue is given chemical treatment followed by incubation period and thawing. Following subsequent steps, then aqueous layer is used for NMR analysis (Komoroski et al. 2008). For the study, PL metabolites in the three brain regions for the three complete subject groups were considered. The results for the relevant metabolite ratios pe/gpe and pc/gpc, summed PMEs (pe + pc = “PME”), and summed phosphodiesters (gpe + gpc = “PDE”) are also provided. These sum-up values approximate the quantities measured in the in vivo 31P MR spectra of the brain. The metabolite concentrations found here are comparable to those found in vivo using (Fusar-Poli et al. 2017) P MRS (Jensen et al. 2002). Although higher gpc is detected in the occipital cortex, the control region, as well as the frontal and temporal cortex, it eventually confirms in vivo results of increased PDEs in schizophrenia. The study considering MRI data has been thoroughly investigated by Chatterjee et al. (2020) about changes in the volume of gray matter as the characteristics of schizophrenia patients in comparison to healthy controls. The findings show a significant decrease in gray matter volume in schizophrenia patients’ brains, most notably in the inferior frontal gyrus, superior temporal gyrus, middle occipital gyrus, and insula. This study added a boon to the way for further research into the underlying neurobiology of the schizophrenic brain contributing to clinical interventions (Chatterjee et al. 2020). fMRI scans use the same fundamental atomic physics principles as MRI scans; however, MRI scans image anatomical structure and fMRI scans image metabolic function. As a result, the images produced by MRI scans are three-dimensional representations of anatomic structure. Another tool used for neuroimaging is functional magnetic resonance imaging (fMRI). The most widely used technique for studying the functional activation patterns of the brain is functional magnetic resonance imaging (fMRI). The fMRI data is four-dimensional, consisting of three-dimensional brain images collected over time (Chatterjee 2018).
4.6 Molecular Pathology of Schizophrenia
Pathology is the study of the causes and consequences of disease or injury. Generally, the term pathology implies the study of diseases. It encompasses a wide range of biological research fields and medical disciplines.
There are three major concepts in context to development of schizophrenia. According to the neurochemical abnormality, the psychiatric manifestations of the disease are caused by an imbalance of dopamine, serotonin, glutamate, and GABA. Evidence indicated that the number of dopamine receptors are increased in a brain proportion. As demonstrated (possibly two-thirds) of patients with schizophrenia utilizing receptor assay techniques (Owen et al. 1978; Lee et al. 1978).
Burt et al. conducted a study in rat to assess dopamine receptor supersensitivity, using the haloperidol-binding technique (Burt et al. 1977). In later studies, haloperidol was replaced with Spiroperidol 20 (due to its advantages) as a dopamine receptor assay and linked changes in receptor sensitivity in human post-mortem brain to changes in dopamine concentrations and dopamine turnover measured as concentrations of the metabolites homovanillic acid (H.V.A.) and dihydroxyphenylacetic acid (DOPAC). Dopamine turnover was not increased in schizophrenic patients, but there was a significant increase in postsynaptic receptor sensitivity as measured by the spiroperidol-binding technique. Dopamine neuron hyperactivity may be the primary disturbance in some schizophrenic illnesses.
Because of their opposing effects on the adenylate cyclase system, two distinct subtypes of dopamine (DA) receptors have been identified. Kebabian and Calne proposed that DA receptors linked to adenylate cyclase stimulation be classified as D1 receptors, while DA receptors that do not increase enzymatic activity be classified as D2 receptors (Kebabian and Calne 1979). When assays are performed in the presence of guanine nucleotides, the apparent affinity of agonists for D2 receptors labeled with [3H] spiroperidol ([3H]SPD) is reduced. This finding implies that D2 receptors regulate adenylate cyclase via a guanine nucleotide-binding protein. Direct evidence of D2 receptor inhibition of adenylate cyclase has been obtained in studies with pituitary and striatal tissue from rats. D1 and D2 receptor interplay may be important in schizophrenia and the development of novel antipsychotic drugs (APDs) to treat all symptoms of schizophrenia.
4.7 Neuroimaging in Schizophrenia: Advancement in Technique
Schizophrenia, once thought to be a psychological disorder with no organic brain substrate, has been the subject of intense neuroimaging research. Where Neuroimaging process of creating images of the structure or activity of the brain or other parts of the nervous system using techniques such as magnetic resonance imaging or computerized tomography. Magnetic resonance imaging, magnetic resonance spectroscopy, diffusion tensor imaging, functional magnetic resonance imaging, and radionuclide imaging are examples of neuroimaging techniques currently in use (Yildirim and Tureli 2015). Neuroimaging techniques have emerged as critical tools for investigating brain dysfunctions that underpin psychiatric disorders.
Functional neuroimaging techniques revealed that schizophrenia patients have diffuse functional disorders in various areas and networks of the brain is known as the default mode network. Neuroimaging techniques have contributed promptly to the scientific community’s understanding of the pathophysiology of schizophrenia.
Physicians recently geared up diagnosis with the help of medical imaging field, computer aided diagnosis systems (CADS) is the computer-based system using advanced image processing and artificial intelligence (AI) techniques that helps in rapid decisions with automation and accurate diagnosis.
Methods applied for accurate diagnosis are categorized under Functional and structural neuroimaging techniques (McGuire et al. 2008; Aine et al. 2017). The magnetic resonance imaging (MRI) is a widespread technique revealing structural/functional brain abnormalities associated with schizophrenia. Both structural/functional brain abnormalities can be explored with the help of its three-dimensional resolution. Magnetic resonance imaging (MRI) is a medically associated non-invasive neuroimaging technique that is associated with detailed imaging of the organs and tissues of the body. The magnetic field and computer-generated radio waves create three-dimensional anatomical images. MRI structural neuroimaging focuses on visualizing abnormalities in context to white matter (WM), gray matter (GM), and CSF tissues of the brain. (Diwadkar et al. 2011; Varshney et al. 2016).
To establish an accurate diagnosis of SZ, several artificial intelligence (AI) tools are combined with modern image/signal processing methodologies.
4.8 Computed Tomography (CT Scan)Analysis
It is a type of tomography in which a computer directs the movement of the X-ray source and detectors, analyses the data, and generates the image. During CT scan (Fig. 4.2) the X-ray beam moves around the body circularly, during a brain CT scan, allowing for many different views of the brain.

Principle of computed tomography
Ventricular enlargement and cortical atrophy are found in some schizophrenic patients. Ventriculomegaly has been found associated with advanced age, impairment of cognitive abilities, poor treatment response, and the prevalence of unpleasant symptoms (Smith et al. 1997). Since the presence of cortical atrophy and/or ventricular enlargement is typically considered to be pathologic signs (Bigler 1987). The first computerized tomography (CT) study of schizophrenic patients was published in 1976 by Johnstone, Crow, Frith, Stevens, and Kreel. Astonishingly, they discovered a higher incidence of ventricular enlargement and cerebral atrophy in their schizophrenic subjects (Bigler 1987).
Study conducted by Malla et al., regarding brain CT scan on 114 patients, had been diagnosed with first-episode schizophrenia. The Computed Tomographic Rating Scale for Schizophrenia was used to obtain ratings on sulcal and ventricular enlargement, as well as the sylvian fissure. CT ratings were also compared to those of a group of chronic schizophrenia patients. Results obtained showed patients with a first episode of schizophrenic psychosis had morphological changes similar to those seen in chronic schizophrenia. Such changes are most likely influenced by age rather than sex, clinical symptoms, or duration of untreated psychosis (Malla et al. 2002).
4.8.1 Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is a medical imaging technique that is non-invasive. It creates detailed images of patient’s organs and tissues by using a magnetic field and computer-generated radio waves. The working principle of MRI is based on, hydrogen atoms experience a small torque when exposed to a magnetic field. It rotates at a specific resonant frequency. This external stimulus causes the hydrogen atom to transition from equilibrium to an excited state. When the stimulus is removed, the excited state spontaneously decays back to equilibrium with time, and the nucleus emits an energy that can be detected with the MRI unit’s receiver coils and converted into gray-scale pixelated images via complex mathematical transformations (Texada and Singh 2010).
The contrast resolution of magnetic resonance imaging (MRI) is four times that of CT.
The process in MRI is different; it is based on a complex interplay of diverse tissue reactions to applied magnetic fields, whereas CT is based on differential X-ray beam attenuation.
A study reported for schizophrenia, during first episode there is a 4% decrease in gray matter volume, whereas white matter is unaffected. From the initial strike, this structural shift was obvious (Lieberman et al. 2001; Kasai et al. 2003). Auditory hallucinations have been linked to volume loss in the superior temporal gyrus, while negative symptoms have been linked to volume loss in the prefrontal lobe (Szeszko et al. 2000). In cases of first-time psychosis, MRI is recommended, especially if there are unusual symptoms, rapid or atypical development of psychosis, dementia, and the presence of focal neurologic deficits or symptoms. The most consistent finding from computed tomography (CT) and magnetic resonance imaging (MRI) studies to date has been slightly enlarged lateral ventricles, which may be indicative of volumetric reduction of gray matter in the frontal and temporal regions, though the amygdala and hippocampal regions have also been implicated (Chua and McKenna 1995; Malla et al. 2002).
If the physicians do not find a physical cause for the suspected symptoms of SZ, they may refer the patient to a psychiatrist, psychologist, or other related experts. The main psychological assessment focuses on clinical interviews based on diagnostic and statistical manual (DSM-IV) of mental disorders conducted by clinical psychiatrists to diagnose patients with SZ (Maj 1998).
4.9 Psychometric Analysis
Psychological testing might also be used by physician to dig deeper into the symptoms of schizophrenia. These tests may involve the following:
Cognitive testing, personality evaluations, the Rorschach (inkblot) test are the example of open-ended or projective testing. For a psychological examination, information can also be acquired by the therapist in questionnaire format from family or friends including parameters such as:
Behavioral changes in the patient, previous social functioning level, family health history including clinical history of family in context to mental illness. Medical and psychological issues in the past, medications. Psychiatrists and other medical professionals were preferred in the past. Clinician can also discriminate in patient if symptoms are caused by schizophrenia or are the effect of any medications. Substances like marijuana can cause psychotic symptoms. Certain toxicology test can be used to evaluate chemical substances contributing to psychotic symptoms. Symptoms can occur when inebriated as well as during withdrawal.
For the diagnostic interview of people at ultrahigh risk (UHR) of psychosis, several psychometric tests are available. The development of psychometric tools to identify subjects at ultrahigh clinical risk (UHR) of psychosis in the future has enabled preventative screening using diagnosis with interventions. Jackson and McGorry were the first to initiate reliability studies in 1991, using a semi-structured interview to psychometrically assess first-episode subjects in order to determine the presence of prodromal signs and symptoms (Jackson et al. 1994). As per the findings, Yung and colleagues established the first clinical service for UHR individuals in 1995 and developed the first UHR psychometric instrument (Yung et al. 1996). The Royal Park Multidiagnostic Instrument for Psychosis (RPMIP) is a validity-oriented assessment procedure for acute psychotic episodes that uses serial interviews and multiple information sources to build a clinical database.
4.9.1 Cognitive Analysis
There is evidence supporting use of cognitive behavior study to control schizophrenia. Extensive evidences are in accordance that core feature of schizophrenia is cognitive impairment; assessing cognitive function is a vital step in patient’s analysis with schizophrenia. Schizophrenia reflects into cognitive deficits as well as positive, negative, and disorganized group of symptoms.
According to the finding, (Schaefer et al. 2013) schizophrenia is associated with impairment cognitive performance domains is evident from hundreds of studies and thousands of individuals. A instrument called, The Brief Assessment of Cognition in Schizophrenia (BACS) helps in quick assessing the aspects of cognition to be most impaired and showed correlation with outcome in schizophrenia patients. The time required for the testing with the BACS is approximately 30 min with minimal extra time for scoring and training demands (Kaneda and Keefe 2015). Dr. Kaneda attempted to create an abbreviated version of the BACS (Abbreviated BACS, A-BACS) to make it more convenient for clinical work, based on the initial Japanese BACS. Hence is in charge of creating the Japanese version of the BACS. Dr. Keefe conducts BACS testing battery and the MATRICS battery (BACS Symbol Coding).
The BACS was found to be sensitive to cognitive impairment in schizophrenia patients as a standard battery of tests that took over 2 h to administer. In both patients (r = 0.76) and healthy controls (r = 0.90), the BACS composite scores were strongly in accordance with the standard battery composite scores. These psychometric properties make the BACS a promising tool for analyzing cognition in patients with schizophrenia regularly (Keefea et al. 2004).
Reviews highlight large deficits in cognitive behavior, the areas of verbal episodic memory (Heinrichs and Zakzanis 1998; Reichenberg and Harvey 2007), executive functioning (Reichenberg and Harvey 2007), or processing speed (Dickinson et al. 2007), the most consistent finding across studies has been an overall, generalized impairment across neuropsychological measures that persists in every clinical state and across patients’ lifetimes. Another study conducted by Hidese et al. suggested about Japanese version of the BACS (BACS-J) measures, the working memory and motor speed scores are associated with several structural alterations in the brains of patients with schizophrenia (Hidese et al. 2017).
4.9.2 Clinical Observations and Analysis
In healthcare, clinical observations refer to the act of measuring, questioning, evaluating, or otherwise observing a patient or a specimen from a patient; making a clinical judgment. Collecting data based on result, answer, judgment, or knowledge gained from monitoring a patient or a specimen procured from a patient is collectively referred to as clinical observations. An assessment was conducted using neuropsychological screening instrument and two everyday behavior observation scales in describing cognitive and functional capacity in patients with multiepisode schizophrenia (Bagge et al. 2017). The nature and number of symptoms, as well as functional capacity disturbances, vary throughout the course of schizophrenia in the patient (Tandon et al. 2009).
Patients selected in the study were within the age range of 18–65 years, International Classification of Diseases 10 F20.0–F20.9 (schizophrenia) or F25.0–F25.9 (schizoaffective disorder) diagnoses in the last 5 years. Exclusion criteria included acute serious psychotic episodes or physical illness, alcohol or drug abuse in the year preceding the study, a diagnosed cerebral disorder at the time of admission to the unit, and a limited ability to communicate (Bagge et al. 2017).
The Barrow Neurological Institute psychologist scored the Screen for Higher Cerebral Functions (BNIS); nursing staff scored the Frontal Systems Behavior Scale (FrSBe) Family Version and the Functional Independence Measure (FIM) V.4.0. The findings from this study suggest that the BNIS, FrSBe, and FIM may be useful assessment tools in clinical work with middle-aged patients who have multiple episode schizophrenia spectrum disorders and require comprehensive care. The findings indicate that the investigated group has significant cognitive impairment, executive dysfunction, and functional disability. Executive dysfunction has been linked to frontal lobe dysfunction. The Barrow Neurological Institute Screen for Higher Cerebral Functions (BNIS) situated in Phoenix, Arizona, USA is a world leader in the treatment, research, and education of brain and spinal diseases, conditions, and injuries. It is led by Barrow President and CEO Michael T. Lawton, MD, one of the world’s leading neurosurgeons. Clinical Trial Numbers for Barrow used to test stroke survivors who are young and middle - aged for cognitive dysfunction. The BNIS and the Mini-Mental State Examination (MMSE) is considered for the patients (Redfors et al. 2014).
4.10 Psychological
Suicidal behavior is more common in people with schizophrenia, although there is little understanding of the psychological factors that add to this vulnerability. The biopsychosocial “Cry of Pain” paradigm offers a comprehensive framework for understanding suicidal behavior. However, the model’s efficacy in connection to suicide in schizophrenia has yet to be investigated (Bolton et al. 2007). The Overlap model, for example, considers the influence of psychosocial milieu (primarily social support), biological vulnerability, psychiatric disorder, personality factors, and family history; the Three Elements model, which includes risk factors, predisposing factors, potentiating factors, and suicidal threshold; and the Cubic model, which takes into account the “press” of external events, the “pain” of unmet psychological needs, and the “perturbation” of the state of mind, Suicide as a Career within the context of a person’s life; and the Suicide Trajectory model, which focuses on the combination of biological, psychological, cognitive, and environmental elements that trigger the “last straw” of suicide thoughts and deeds (Sangadah and Kartawidjaja 2020).
Suicidal ideation and preparation, it has been believed, are key steps that lead to a self-harm attempt that may result in death, with previous unsuccessful suicide attempts increasing the probability of further successful suicide attempts (Kontaxakis et al. 2004).
A large body of research has found a variety of socio-demographic and clinical characteristics that are associated with an elevated risk of suicide in the general population and also apply to schizophrenia. Being a man, being younger, being socially isolated, misusing substances, being unhappy and/or feeling hopeless, having attempted suicide before, and having a family history of suicide are all risk factors (Caldwell and Gottesman 1992).
Not only does a theoretical approach help us comprehend suicidal behavior in schizophrenia, but it also helps us grasp the putative underlying causes of suicide in general. There are three broad theoretical views to consider. To begin with, there may be central elements of suicidal behavior that are shared by a variety of mental illnesses, implying a single transdiagnostic, albeit multi-factorial, causative process that acts across a variety of disorders. Second, there may be characteristics that are unique to individual diagnoses, reflecting non-uniform mechanisms underpinning suicidal behavior, such as acting on voices that demand suicide. Third, and in contrast to the previous scenario, suicidal behavior could be linked to a cluster of symptoms linked to a single disease. Depression is a likely contender because it is typically comorbid with schizophrenia, with some estimates claiming that 50% of those with psychotic symptoms also had one or more major depressive episodes (An Der Heiden et al. 2005).
It is also crucial to keep in mind that any of the three speculative scenarios listed above could apply. A fourth option is that there are factors that are part of a general transdiagnostic mechanism in that they apply to a variety of psychiatric diseases but are modulated by aspects of a specific disorder. To give a specific example, stress may be a generally predictor of suicide risk, but it is exacerbated by specific characteristics of psychosis.
4.10.1 Stressors Presence
The first section of the “Cry of Pain” model argues that people with schizophrenia are more probable than the common population to commit suicide as a result of an increased number of stressful events due to the illness’s burden and enhanced sensitivity to stress.
4.10.2 Presence of External Stress
Significant losses appear to precede suicide in people with schizophrenia, but not as much as in the general population (Heilä et al. 1999).
4.10.3 Presence of Internal Stress
Because of increased emotions of entrapment, helplessness, and melancholy, stressors linked with internal issues related to psychosis may plausibly lead to suicide behavior in schizophrenia (Beck-Sander et al. 1997).
4.10.4 Stressors Appraisal
The importance of external and internal stressors is assessed as suggestive of defeat or rejection, in accordance with the second component of the Cry of Pain model.
4.10.5 External Stress Appraisal
Birchwood and colleagues’ research backs up this theory, claiming that particular sorts of sickness assessments, such as loss (for example, status and goals), threat, shame, or imprisonment, might lead to depression (Birchwood et al. 1993).
4.10.6 Internal Stress Appraisal
Hallucinations and delusions were found to be positively linked with self-reports of entrapment, according to the Cry of Pain model. The voices were perceived as critical of the individual and as signaling poor social value, which had negative impacts on auditory hallucinations. Surprisingly, depression was a byproduct of these unfavorable evaluations rather than being the fundamental cause (Birchwood et al. 1993).
4.10.7 Impairment of Cognitive Processes and Cognitive Biases
According to the Cry of Pain model, reasoning and problem-solving biases may be particularly essential components of suicide behavior because they restrict the invention and implementation of constructive alternatives. Autobiographical memory biases are thought to play a vital role in suicidal thoughts and behaviors because they prevent certain types of experiences (especially positive experiences) from being encoded and preventing individuals from updating schema, potentially blocking access to effective problem-solving incidents (Bentall et al. 2001).
4.10.8 Reasons and Problem-Solving of Biases
Suicidal people, including those who have delusions, have been shown to have suboptimal reasoning processes, which include accumulating less data before making decisions (i.e., “jumping to conclusions”), excessive responses (i.e., “ dualistic thinking”), and metacognitive or belief inflexibility. Suicidal people have been demonstrated to be bad at addressing problems, especially interpersonal ones. In a battery of tests designed to examine the development and appraisal of solutions during social problem-solving, people diagnosed with schizophrenia were compared to those diagnosed with bipolar illness and a nonpsychiatric control group. When compared to nonpsychiatric controls, those with bipolar illness and schizophrenia did worse on all measures of social problem-solving (Garety et al. 2005).
4.10.9 Related to Memory and Memory Retrieval Deficiencies
Working memory was found to be the foundation for these cognitive elements, and executive processes in working memory integrated the representation of social information essential for adequate and acceptable social interactions. Working memory directs expectations regarding cognitive and social information while also facilitating automatic processing, freeing up cognitive resources for other tasks. As a result, deficits in executive working memory processes are likely to increase the demands of effortful processing and decrease social problem-solving capacity (Barch 2006).
4.11 Questionnaire
4.11.1 Positive and Negative Symptoms Questionnaire
When considering patient outcomes, it is critical to assess both positive and negative symptoms. The state of a patient’s premorbid functioning might signal both negative and positive symptoms. Andreasen proposed a link between negative feelings and premorbid functioning in 1982. Addington and Addington investigated this concept further (1993). Males exhibited much worse premorbid functioning than females, according to the study. Furthermore, in contrast to individuals with negative symptoms, those with positive symptoms experienced a significant reduction in symptomatology with time, according to a longitudinal research. Furthermore, there was a substantial difference in the amount of time spent in therapy between individuals who had unpleasant symptoms and those who did not. Brain imaging techniques, both functional and structural, have become an important aspect in evaluating positive and negative symptoms. There is a lot of contradictory information out there about how effective these tactics are. It implies that, brain imaging, focused on the temporal and frontal lobes, can reveal anatomical brain defects particular to schizophrenia patients. Deficits in semantic, episodic, and short-term memory, impulsivity, and other cognitive domains have been linked to the loss of brain matter in these locations. Large ventricles are a typical feature in schizophrenia patients and can help explain cognitive problems. Andreasen explained in 1985 that functional and structural imaging modalities may not reflect common features characterized by positive symptoms. The ventricles of the participants were found to be somewhat smaller. However, there appeared to be common brain abnormalities stated in the previous article when examining negative symptoms, implying that negative symptoms are linked to left hemisphere abnormalities. While imaging techniques have some advantages, they are not always practicable in outpatient or inpatient clinical settings. While the visual impact can reassure patients and aid in the detection of other neurological irregularities, it may not be a cost-effective measure due to insurance fees, time constraints, and a lack of skilled workers when it comes to patient load. Some practices may request MRI and CT scans to rule out any brain damage or to look for organic disorders that could be the cause of underlying psychosis, but this is not always necessary. Functional imaging was only determined to be “relevant pathology” in 11% of MRIs, showing that it is not the end-all source for those seeking a diagnosis. Patients may then be referred to certified professionals who will assess their current mental abilities (Sangadah and Kartawidjaja 2020).
4.12 Conclusion and Scope of Future Work
Detailed data on the severity and distribution of psychosis symptoms across schizophrenia spectrum subdiagnoses, as well as brain scanning and pharmacological data, may help to improve comprehension of the nature of cognitive impairment and problems with daily functioning in patients with multiple episode schizophrenia and complex care needs. Future medical research is expected to pave the way for a more promising future in schizophrenia treatment and, theoretically, cure. For more improvements in patient care, the synchronizing role of psychiatrists and researchers must be performed for the improvement and development of modified medicine tools. It will undoubtedly contribute to a brighter future for schizophrenia patients.
References
Ackerman JJH, Grove HT, Wong GG, Gadian DG, Radda GR (1980) Mapping of metabolite in whole animal by 31P NMR using surface coil. Nature 283:167–170. https://pubmed.ncbi.nlm.nih.gov/7350541/. https://doi.org/10.1038/283167a0
Ahokas AR, Rimón M, Koskiniemi A, Vaheri I, Julkunen S, Sarna. (1987) Viral antibodies and interferon in acute psychiatric disorders. J Clin Psychiatry 48:194–196
Aine C, Bockholt HJ, Bustillo JR, Canive JM, Caprihan A, Gasparovic C, Hanlon FM, Houck JM, Jung RE, Lauriello J, Liu J, Mayer AR, Perrone-Bizzozero NI, Posse S, Stephen JM, Turner JA, Clark VP, Calhoun VD (2017) Multimodal neuroimaging in schizophrenia: description and dissemination. Neuroinformatics 15(4):343–364. https://doi.org/10.1007/s12021-017-9338-9
An Der Heiden W, Könnecke R, Maurer K, Ropeter D, Häfner H (2005) Depression in the long-term course of schizophrenia. Eur Arch Psychiatry Clin Neurosci 255(3):174–184. https://doi.org/10.1007/s00406-005-0585-7
Ashok AH, Baugh J, Yeragani VK (2012) Paul eugen bleuler and the origin of the term schizophrenia (SCHIZOPRENIEGRUPPE). Indian J Psychiatry 54:95–96. https://doi.org/10.4103/0019-5545.94660
Bagge EN, Esbjörnsson E, Sunnerhagen KS (2017) Cognitive screening and behavioral observation of functional ability in patients with multiple episode schizophrenia: an exploratory study. BMJ 7(6):1–10. https://doi.org/10.1136/bmjopen-2016-014783
Bansal V, Chatterjee I (2021) Role of neurotransmitters in schizophrenia: a comprehensive study. Kuwait J Sci 48(2). https://doi.org/10.48129/kjs.v48i2.9264
Barch DM (2006) What can research on schizophrenia tell us about the cognitive neuroscience of working memory? Neuroscience 139(1):73–84. https://doi.org/10.1016/j.neuroscience.2005.09.013
Beck-Sander A, Birchwood M, Chadwick P (1997) Acting on command hallucinations: a cognitive approach. Br J Clin Psychol 36(1):139–148. https://doi.org/10.1111/j.2044-8260.1997.tb01237.x
Benros ME, Pedersen MG, Rasmussen H, Eaton WW, Nordentoft M, Mortensen PB (2014) A nationwide study on the risk of autoimmune diseases in individuals with a personal or a family history of schizophrenia and related psychosis. Am J Psychiatry 171:218–226. https://doi.org/10.1176/appi.ajp.2013.13010086
Bentall RP, Corcoran R, Howard R, Blackwood N, Kinderman P (2001) Persecutory delusions: a review and theoretical integration. Clin Psychol Rev 21(8):1143–1192. https://doi.org/10.1016/S0272-7358(01)00106-4
Bigler ED (1987) The clinical significance of cerebral atrophy in dementia. Arch Clin Neuropsychol 2:177–190
Birchwood M, Mason R, MacMillan F, Healy J (1993) Depression, demoralization and control over psychotic illness: a comparison of depressed and non-depressed patients with a chronic psychosis. Psychol Med 23(2):387–395. https://doi.org/10.1017/S0033291700028488
Birtwistle J, Baldwin D (1998) Role of dopamine in schizophrenia and Parkinson’s disease. Br J Nurs 7(14):832–841. https://doi.org/10.12968/bjon.1998.7.14.5636
Bligh EG, Dyer WJ (1959) A rapid method of total lipid extraction and purification. Can J Biochem 1959(37):911–917. https://doi.org/10.1139/o59-09
Bolton C, Gooding P, Kapur N, Barrowclough C, Tarrier N (2007) Developing psychological perspectives of suicidal behaviour and risk in people with a diagnosis of schizophrenia: we know they kill themselves but do we understand why? Clin Psychol Rev 27(4):511–536. https://doi.org/10.1016/j.cpr.2006.12.001
Brown AS, Derkits EJ (2010) Prenatal infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry 167(2010):261–280. https://doi.org/10.1176/appi.ajp.2009.09030361
Brown S, Kim M, Mitchell C, Inskip H (2010) Twenty-five year mortality of a community cohort with schizophrenia. Br J Psychiatry 196:116–121. https://doi.org/10.1192/bjp.bp.109.067512
Burt DR, Creese I, Snyder SH (1977) Antischizophrenic drugs: chronic treatment elevates dopamine receptor binding in brain. Science 196(4287):326–328. https://doi.org/10.1126/science.847477
Caldwell CB, Gottesman II (1992) Schizophrenia—a high-risk factor for suicide: clues to risk reduction. Suicide Life Threat Behav 22(4):479–493. https://doi.org/10.1111/j.1943-278X.1992.tb01040.x
Chatterjee I (2018) Mean deviation based identification of activated voxels from time-series fMRI data of schizophrenia patients. F1000Res 7:1615. https://doi.org/10.12688/f1000research.16405.2
Chatterjee I, Mittal K (2019) A concise study of schizophrenia and resting-state fMRI data analysis. Qeios 414:2. https://doi.org/10.32388/599711.2
Chatterjee I, Kumar V, Sharma S, Dhingra D, Rana B, Agarwal M, Kumar N (2019) Identification of brain regions associated with working memory deficit in schizophrenia. F1000Res 8:124. https://doi.org/10.12688/f1000research.17731.1
Chatterjee I, Kumar V, Rana B, Agarwal M, Kumar N (2020) Identification of changes in grey matter volume using an evolutionary approach: an MRI study of schizophrenia. Multimedia Syst 26:383–396. https://doi.org/10.1007/s00530-020-00649-6
Chua SE, McKenna PJ (1995) Schizophrenia—A brain disease? A critical review of structural and functional cerebral abnormality in the disorder. Br J Psychiatry 166:563–582. https://doi.org/10.1192/bjp.166.5.563
Delaney SB, Fallon A, Alaedini R, Yolken A, Indart T, Feng Y, Wang D, Javitt (2019) Inflammatory biomarkers in psychosis and clinical high risk populations. Schizophr Res 206:440–443. https://doi.org/10.1016/j.schres.2018.10.017
Dickinson D, Ramsey ME, Gold JM (2007) Overlooking the obvious: a meta-analytic comparison of digit symbol coding tasks and other cognitive measures in schizophrenia. Arch Gen Psychiatry 64(5):532–542. https://doi.org/10.1001/archpsyc.64.5.532
Diwadkar VA, Pruitt P, Goradia D, Murphy E, Bakshi N, Keshavan MS, Rajan U, Reid A, Zajac-Benitez C (2011) Fronto-parietal hypoactivation during working memory independent of structural abnormalities: conjoint fMRI and sMRI analyses in adolescent offspring of schizophrenia patients. Neuroimage 58(1):234–241. https://doi.org/10.1016/j.neuroimage.2011.06.033
Fellerhoff B, Laumbacher B, Mueller N, Gu S, Wank R (2007) Associations between Chlamydophila infections schizophrenia and risk of HLA-A10. Mol Psychiatry 12:264–272. https://doi.org/10.1038/sj.mp.4001925
First MB, Reed GM, Hyman SE, Saxena S (2015) The development of the ICD-11 clinical descriptions and diagnostic guidelines for mental and behavioural disorders. World Psychiatry 14:82–90
Fitz Gerald GA (2016) Measure for measure: biomarker standards and transparency. Sci Transl Med 8(343):343fs10. https://doi.org/10.1126/scitranslmed.aaf8590
Focking M, Dicker P, Lopez LM, Cannon M, Schafer MR, McGorry PD, Smesny S, Cotter DR, Amminger GP (2016) Differential expression of the inflammation marker IL12p40 in the at-risk mental state for psychosis: a predictor of transition to psychotic disorder? BMC Psychiatry 16(1):326
Fusar-Poli P, Rutigliano G, Stahl D, Davies C, Bonoldi I, Reilly T, McGuire P (2017) Development and validation of a clinically based risk calculator for the transdiagnostic prediction of psychosis. JAMA Psychiat 74:493–500. https://doi.org/10.1001/jamapsychiatry.2017.0284
Garety PA, Freeman D, Jolley S, Bebbington PE, Kuipers E, Dunn G, Fowler DG, Dudley R (2005) Reasoning, emotions, and delusional conviction in psychosis. J Abnorm Psychol 114(3):373–384. https://doi.org/10.1037/0021-843X.114.3.373
Goldsmith DR, Rapaport MH, Miller BJ (2016) A meta-analysis of blood cytokine network alterations in psychiatric patients: comparisons between schizophrenia, bipolar disorder and depression. Mol Psychiatry 21:1696–1709. https://doi.org/10.1038/mp.2016.3
Guyton AC, Hall JE (2006) Textbook of medical physiology, 11th edn. Elsevier Saunders, Philadelphia
Heilä H, Heikkinen ME, Isometsä ET, Henriksson MM, Marttunen MJ, Lönnqvist JK (1999) Life events and completed suicide in schizophrenia. A comparison of suicide victims with and without schizophrenia. Schizophr Bull 25(3):519–531. https://doi.org/10.1093/oxfordjournals.schbul.a033398
Heinrichs RW, Zakzanis KK (1998) Neurocognitive deficit in schizophrenia: a quantitative review of the evidence. Neuropsychology 12(3):426–445. https://doi.org/10.1037/0894-4105.12.3.426
Hidese S, Ota M, Matsuo J, Ishida I, Hiraishi M, Teraishi T, Hattori K, Kunugi H (2017) Association between the scores of the Japanese version of the brief assessment of cognition in schizophrenia and whole-brain structure in patients with chronic schizophrenia: a voxel-based morphometry and diffusion tensor imaging study. Psychiatry Clin Neurosci 71:826–835. https://doi.org/10.1111/pcn.12560
Insel T, Cuthbert B (2010) Research Domain Criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry 167(7):748–751. https://doi.org/10.1176/appi.ajp.2010.09091379
Jackson HJ, McGorry PD, McKenzie D (1994) The reliability of DSM-III prodromal symptoms in first-episode psychotic patients. Acta Psychiatr Scand 90(5):375–378. https://doi.org/10.3109/00048679609062654
Jensen JE, Drost DJ, Menon RS, Williamson PC (2002) In vivo brain 31 P-MRS: measuring the phospholipid resonances at 4 tesla from small voxels. NMR Biomed 15:338–347. https://doi.org/10.1002/nbm.776
Kaneda Y, Keefe RSE (2015) An abbreviated version of the brief assessment of cognition in schizophrenia (BACS). Eur J Psychiatry 29(2):131–134. https://doi.org/10.4321/S0213-61632015000200004
Kasai K, Shenton ME, Salisbury DF et al (2003) Progressive decrease of left superior temporal gyrus gray matter volume in patients with first episode schizophrenia. Am J Psychiatry 160:156–164. https://doi.org/10.1176/appi.ajp.160.1.156
Kebabian JW, Calne DB (1979) Multiple receptors for dopamine. Nature 277:93–96. https://doi.org/10.1038/277093a0
Keefea R, Goldbergb TE, Harveyc PD, Goldd JM, Poea MP, Coughenour L (2004) The brief assessment of cognition in schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res 68:283–297. https://doi.org/10.1016/j.schres.2003.09.011
Kirkpatrick B, Miller BJ (2013) Inflammation and schizophrenia. Schizophr Bull 39:1174–1179. https://doi.org/10.1093/schbul/sbt141
Komoroski RA, Pearce JM, Mrak RE (2008) 31 P NMR spectroscopy of phospholipid metabolites in postmortem schizophrenic brain. Magn Reson Med 59:469–474. https://doi.org/10.1002/mrm.21516
Kontaxakis V, Havaki-kontaxaki B, Margariti M, Stamouli S, Kollias C, Christodoulou G (2004) Suicidal ideation in inpatients with acute schizophrenia. Can J Psychiatry 49(7):5–8. https://doi.org/10.1177/070674370404900709
Laney D, Philip N, Miller BJ (2015) Recurrent urinary tract infections in acute psychosis. Schizophr Res 164(2015):275–276. https://doi.org/10.1016/j.schres.2015.02.018
Lee T, Seeman P, Tourtellotte WW, Farley IJ, Hornykeiwicz. (1978) Binding of 3H-apomorphine in schizophrenic brains. Nature 274:897–900. https://doi.org/10.1038/274897a0
Lieberman J, Chakos M, Wu H et al (2001) Longitudinal study of brain morphology in first episodes of schizophrenia. Biol Psychiatry 49:487–499. https://doi.org/10.1016/s0006-3223(01)01067-8
Maj M (1998) Critique of the DSM–IV operational diagnostic criteria for schizophrenia. Br J Psychiatry 172(6):458–460. https://doi.org/10.1192/bjp.172.6.458
Malla AK, Mittal C, Lee M, Scholten DJ, Assis L, Norman MG (2002) Computed tomography of the brain morphology of patients with first-episode schizophrenic psychosis. J Psychiatry Neurosci 7(5):350–358
Mazza MG, Lucchi S, Rossetti A, Clerici M (2019) Neutrophil-lymphocyte ratio, monocyte-lymphocyte ratio and platelet-lymphocyte ratio in non-affective psychosis: a meta-analysis and systematic review. World J Biol Psychiatry 21:326. https://doi.org/10.1080/15622975.2019.1583371
McGuireP OD, Howes J, Stone P, Fusar-Poli. (2008) Functional neuroimaging in schizophrenia: diagnosis and drug discovery. Trends Pharmacol Sci 29(2):91–98. https://doi.org/10.1016/j.tips.2007.11.005
Miller BJ, Goldsmith DR (2019) Inflammatory biomarkers in schizophrenia, implications for heterogeneity and neurobiology. Biomark Neuropsychiatry 1(2019):1–11. https://doi.org/10.1016/j.bionps.2019.100006
Miller BJ, Graham KL, Bodenheimer CM, Culpepper NH, Waller JL, Buckley PF (2013) A prevalence study of urinary tract infections in acute relapse of schizophrenia. J Clin Psychiatry 73:271–277. https://doi.org/10.4088/JCP.12m08050
Mintz AR, Dobson KS, Romney DM (2003) Meta-analysis, the relationships between insight and symptom. Schizophr Res 61:75–88. https://doi.org/10.1016/s0920-9964(02)00316-x
Monroe JM, Buckley PF, Miller BJ (2015) Meta-analysis of anti-toxoplasma gondii IgM antibodies in acute psychosis. Schizophr Bull 41(4):989–998. https://doi.org/10.1093/schbul/sbu159
Nitta MT, Kishimoto N, Müller M, Weiser M, Davidson JM, Kane (2013) Adjunctive use of nonsteroidal anti-inflammatory drugs for schizophrenia: a meta-analytic investigation of randomized controlled trials. Schizophr Bull 39:1230–1241. https://doi.org/10.1093/schbul/sbt070
Novak J, Wilson M, Mac Pherson L, Arvanitis TN, Davies NP, Peet AC (2014) Clinical protocols for 31 P MRS of the brain and their use in evaluating optic pathway gliomas in children. Eur J Radiol 83(2014):e106–e112. https://doi.org/10.1016/j.ejrad.2013.11.009
Owen F, Cross AJ, Crow TJ, Longden A, Poulter M, Riley GJ (1978) Increased dopamine-receptor sensitivity in schizophrenia. Lancet 2:223–225. https://doi.org/10.1016/S0140-6736(78)91740-3
Park S, Miller BJ (2019) Meta-analysis of cytokine and C-reactive protein levels in high-risk psychosis. Schizophr Res 226:5–12. https://doi.org/10.1016/j.schres.2019.03.012
Park MH, Kwon YJ, Jeong HY, Lee HY, Hwangbo Y, Yoon HJ (2012) Association between intracellular infectious agents and schizophrenia. Clin Psychopharmacol Neurosci 10(2):117–123. https://doi.org/10.9758/cpn.2012.10.2.117
Pettegrew JW, Keshavan MS, Panchalingam K, Strychor S, Kaplan DB, Tretta MG, Allen M (1991) Alterations in brain high-energy phosphate and membrane phospholipid metabolism in first-episode, drug-naïve schizophrenics. A pilot study of the dorsal prefrontal cortex by in vivo phosphorus-31 nuclear magnetic resonance spectroscopy. Arch Gen Psychiatry 48:563–568. https://doi.org/10.1001/archpsyc.1991.01810300075011
Redfors PC, Hofgren I, Eriksson L, Holmegaard H, Samuelsson, Jood K (2014) The Barrow neurological institute screen for higher cerebral functions in cognitive screening after stroke. J Stroke Cerebrovasc Dis 23(2):349–355. https://doi.org/10.1016/j.jstrokecerebrovasdis.2013.04.026
Reichenberg A, Harvey PD (2007) Neuropsychological impairments in schizophrenia: integration of performance-based and brain imaging findings. Psychol Bull 133(5):833–858. https://doi.org/10.1037/0033-2909.133.5.833
Saha S, Chant D, McGrath J (2007) A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry 64:1123–1131. https://doi.org/10.1001/archpsyc.64.10.1123
Sangadah K, Kartawidjaja J (2020) No 主観的健康感を中心とした在宅高齢者における健康関連指標に関する共分散構造分析. Orphanet J Rare Dis 21(1):1–9
Sawa A, Snyder SH (2002) Schizophrenia: diverse approaches to a complex disease. Science 296:692. https://doi.org/10.1126/science.1070532
Schaefer J, Giangrande E, Daniel R, Dickinson WD (2013) The global cognitive impairment in schizophrenia: consistent over decades and around the world. Schizophr Res 150:42. https://doi.org/10.1016/j.schres.2013.07.009
Shepherd AM, Laurens KR, Matheson SL, Carr VJ, Green MJ (2012) Systematic meta-review and quality assessment of the structural brain alterations in schizophrenia. Neurosci Biobehav Rev 36(4):1342–1356. https://doi.org/10.1016/j.neubiorev.2011.12.015
Smith GN, Flynn SW, Kopala LC et al (1997) A comprehensive method of assessing routine CT scans in schizophrenia. Acta Psychiatr Scand 96:395–401. https://doi.org/10.1111/j.1600-0447.1997.tb09935.x
Sommer IE, Westrhenen R, Begemann MJ, de Witte LD, Leucht S, Kahn RS (2014) Efficacy of anti-inflammatory agents to improve symptoms in patients with schizophrenia: an update. Schizophr Bull 40(2014):181–191. https://doi.org/10.1093/schbul/sbt139
Szeszko PR, Bilder RM, Lencz T et al (2000) Reduced anterior cingulate gyrus volume correlates with executive dysfunction in men with first episode schizophrenia. Schizophr Res 43:97–108. https://doi.org/10.1016/s0920-9964(99)00155-3
Tandon R, Nasrallah HA, Keshavan MS (2009) Schizophrenia, “just the facts” 4. Clinical features and conceptualization. Schizophr Res 110:1–23. https://doi.org/10.1016/j.schres.2009.03.005
Texada JC, Singh SP (2010) Magnetic resonance imaging. In: Canon CL (ed) Radiology specialty board review, 1st edn. McGraw Hill, New York, pp 149–159
Tomasik JE, Schwarz PC, Guest S, Bahn. (2012) Blood test for schizophrenia. Eur Arch Psychiatry Clin Neurosci 262(2):79–83. https://doi.org/10.1007/s00406-012-0354-3
Torrey EF, Bartko JJ, Lun ZR, Yolken RH (2007) Antibodies to toxoplasma gondii in patients with schizophrenia: a meta-analysis. Schizophr Bull 33(2007):729–736. https://doi.org/10.1093/schbul/sbl050
Varshney AC, Prakash N, Mittal P, Singh (2016) A multimodel approach for schizophrenia diagnosis using fMRI and sMRI dataset. In: The International symposium on intelligent systems technologies and applications. Springer, Berlin, pp 869–877. https://doi.org/10.1007/978-3-319-47952-1_69
Walter G, Robertson M, Rey JM, Soh N, Malhi GS (2010) Electroconvulsive therapy in young people and the pioneering spirit of lauretta bender. Acta Neuropsychiatr 22(5):253–254. https://doi.org/10.1111/j.16015215.2010.00487.x
Weinberger DR, Levitt P (2011) Neurodevelopmental origins of schizophrenia. In: Schizophrenia. Wiley‐Blackwell, Oxford, pp 393–412. https://doi.org/10.1002/wps.20474
Yildirim A, Tureli D (2015) Schizophrenia: a review of neuroimaging techniques and findings. East J Med 20:1–6
Yung AR, McGorry PD, McFarlane CA, Jackson HJ, Patton GC, Rakkar A (1996) Monitoring and care of young people at incipient risk of psychosis. Schizophr Bull 22(2):283–303. https://doi.org/10.1093/schbul/22.2.283
Zhang JW, Luo P, Huang L, Peng Q, Huang. (2018) Maternal C-reactive protein and cytokine levels during pregnancy and the risk of selected neuropsychiatric disorders in offspring: a systematic review and meta-analysis. J Psychiatr Res 105:86–94. https://doi.org/10.1016/j.jpsychires.2018.09.002
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Choudhari, M.R., Chatterjee, I. (2023). A Diagnostic Perspective of Schizophrenia: From Past to Present. In: Chatterjee, I. (eds) Cognizance of Schizophrenia:: A Profound Insight into the Psyche. Springer, Singapore. https://doi.org/10.1007/978-981-19-7022-1_4
Download citation
DOI: https://doi.org/10.1007/978-981-19-7022-1_4
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-7021-4
Online ISBN: 978-981-19-7022-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)