
Abstract
Introduction: Vasospasm remains a major cause of poor outcome after subarachnoid hemorrhage (SAH) following rupture of intracranial aneurysms. The pathogenesis still remains misty due to its complexity even though a lot of progress has been made in understanding various causative mechanisms through intense clinical and experimental research.
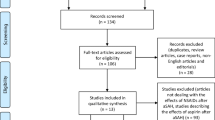
Method: Study carried out by a review of English literature on topics related to pathogenesis and management of post SAH induced vasospasm.
Result: Evidence-based information available points toward multifactorial biochemical phenomena instigated by Ferrous Hemoglobin which revolve around:
-
(a)
Concept of early brain injury and evidence of cortical spreading depression
-
(b)
Effect of ischemia in pre-vasospasm period and blood–brain barrier disruption.
-
(c)
Role of Nitric oxide (NO), Endothelin-1 levels, and oxidative stress on smooth muscle cells.
-
(d)
Changes induced by free radical production, lipid peroxidation, and alteration of ionic channels.
-
(e)
Differential upregulation of genes.
Conclusion: To date the understanding of pathophysiology of delayed vasospasm has made significant stride for which the role of research using animal models cannot be overemphasized. The treatment of this complex condition still remains vague.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
2.1 Introduction
Vasospasm remains a major cause of poor outcome after subarachnoid hemorrhage (SAH) following rupture of intracranial aneurysms. The pathogenesis still remains misty due to its complexity even though a lot of progress has been made in understanding various underlying mechanisms through intense clinical and experimental research. Though statistically 3.4% of population harbor incidental aneurysm [1] yet, depending on the risk factors, their rate of rupture varies from 0% to 100% with an annual rupture rate of 0–6.5% [2]. The risk factors vary from size of aneurysm, age of patient, history of smoking, and hypertension to pathophysiology of aneurysm formation. In familial aneurysms, however, the risk of rupture is threefolds the normal [3]. Despite lot of progress in understanding of the molecular changes culminating into delayed vasospasm, the exact interplay of various pathophysiological substrates remains an enigma. Interestingly, aneurysmal SAH was recognized since the time of Hippocrates and the outcome remains quite grim even to date [4].
2.2 Delayed Cerebral Vasospasm
Though management of aneurysmal SAH remains a major neurocritical care issue delayed cerebral vasospasm, which occurs usually between 3 and 14 days of SAH, remains the most elusive challenge [5]. Based on the belief that vasospasm is the main culprit for deterioration in SAH patients several trials antagonizing the suspected precursors of vasospasm were conducted, however, they failed to achieve a good functional outcome [6, 7]. Hence the role of vasospasm as the sole prognostic factor in clinical outcome after SAH remains questionable. On the contrary, it now seems evident that the pathological events starting at the very onset of SAH, which culminates into various biochemical changes, need to be understood better. Vasospasm and DCI may be the extreme manifestation of the same pathophysiological process rather than isolated phenomena. This has led to the concept of “Early Brain Injury.”
Most of the management regimes for treatment of vasospasm has been directed toward the end result of pathophysiological phenomenon rather than treating the causative mechanism. Based on it, till now, the main treatment modalities include partial Triple H therapy (Hypervolemia, Hemodilution, and Hypertension), calcium channel antagonists, chemical or mechanical vasodilation. As a result, it still remains to be proven whether any of these treatment modalities have an evidence-based prognostic benefit in a patient with refractory vasospasm [8]. The diversity of opinion is reflected on the deliberations in 15 international conferences dedicated to vasospasm and SAH till the year 2019.
The process of vasospasm is far from the mere feature of spasm of blood vessels [9] and its ischemic consequences [10]. Clinical observation and experimental evidence point to the evolution of vasospasm as a complex multifactorial phenomenon that may remain subclinical or may progress to clinically manifested vasospasm with its devastating consequences [11,12,13,14,15]. There are various other pathophysiological mechanisms implicated in the clinical manifestations after SAH apart from vasospasm namely microcirculatory dysfunction, ionic disbalance, cortical spreading depolarization, micro-thrombosis, and inflammation at neuronal cell level [16].
2.3 The Pathophysiological Changes After SAH
2.3.1 Understanding Early Brain Injury
The event of SAH initiates a process of transient global ischemia which has a consequential bearing on the further pathophysiological events that follow. These may be in the form of brief microcirculatory arrest, blood–brain barrier disruption, microvascular constriction, brain edema [17]. The impact of these phenomena weighs heavily on the further events which progress in complex chain manifesting in the form of cerebral inflammation, dysregulation of blood flow, cortical spreading depolarization, microthrombi formation, and apoptosis [18]. These changes may be self-limiting with minimal or no clinical consequence or may progress into severe form leading to clinical deterioration with poor prognosis or fatal outcome.
2.4 What Leads to Vaso Constriction?
To date, a wide-ranging biochemical and molecular mechanisms have been implicated in vasospasm. These processes include mopping up of nitric oxide (NO), high levels of endothelin 1 (ET-1) activity [19], alteration of ionic channels [20], lipid peroxidation, and free radical production [21]. These contribute to smooth muscle changes through oxidative stress [15] and apoptosis of endothelial cells [22]. There is now clear identification of upregulation of genes, which can point to individual susceptibility [23, 24]. Needless to say, the root cause of all these phenomena is triggered off by the release of ferrous components from the disintegrated hemoglobin released by the ruptured aneurysm in the subarachnoid space.
The role of oxidative stress [25]seems to have taken a center stage through its mechanism of direct activation of calcium channels and also through production of vasoactive molecules. The action of reactive oxygen species leads to vasoconstriction by its action on arachidonic acid which in turn leads to release of vasoactive lipids. Though the role of bilirubin oxidative products, formed as a result of hemoglobin break down, has been also considered but its role is not convincing [26] (Fig. 2.1).

Factors contributing to vasospasm
2.4.1 Endothelin 1 (The Physiological Vasoconstrictor)
There are several substrates that contribute to the progression of vasospasm. ET-1 is a potent vasoconstrictor released in vascular wall whose levels are detected to be high in CSF following SAH. The exact levels, which can induce vasoconstriction, are still not determined because experimental studies need much higher levels than what is normally witnessed clinically after SAH. This raises the question of whether ET-1 needs potentiation by other factors [27, 28]. There is also evidence of enhanced ET-1 receptor expression and function in experimental animals suggesting its activation after SAH [29]. The role of Ca+ in the smooth muscle contraction is evident in acute phase of SAH as influx of Ca+ in the cells leads to phosphorylation of myosin light chain by stimulation of myosin light chain kinase [30]. The sustained contraction of the smooth muscles is regulated by the postulated mechanism of RhoA kinase activity which is stimulated by ET-1. Rho kinase is formed by ET-1 activation of Rho A. This initiates a cascade of chemical changes whereby Rho kinase inhibits myosin phosphatase subunit (MYPT1) of myosin light chain phosphatase (MLCP) augmenting phosphorylation of myosin light chain (MLC) [31]. Thus, once triggered the prolonged contraction of vascular smooth muscle is sustained by the enhanced phosphorylated MLC independent of intracellular Ca+ levels [32]. Further studies endorsed these postulates whereby the expression of Rho-associated protein kinase (ROCK), MYPT1 subunits, Protein kinase C (PKC), and upregulation of ET-1 receptor are demonstrated after SAH [33].
2.4.2 Nitric Oxide (The Physiological Vasodilator)
Endothelial nitric oxide is a potent physiological vasodilator that maintains a balancing act with ET-1 to maintain a steady patency of vessel lumen. It is produced by activation of endothelial nitric oxide synthase (eNOS). It produces cyclical guanine monophosphate (cGMP) through its stimulation effect of guanyl cyclase. The end result, which is vascular smooth muscle relaxation, is achieved by dephosphorylation of MLC through activation of cGMP-dependent protein kinases [34]. Following SAH the nascent NO liberated by the endothelium is mopped by hemoglobin to which it has a very strong affinity leading to reduction of local NO concentration tilting the balance for other substrates to induce vasospasm in an unchallenged situation. Furthermore, various molecular cascades of events lead to endothelial cell apoptosis reducing the NO secreting cell population [35]. There is also activation of protein kinase C after SAH which has an inhibitory regulation on NOS resulting in lower levels of NO [36]. Hence, it is derived that in normal situation a steady balance between NO and Endothelin-1 plays a vital role in maintaining the lumen of cerebral blood vessels.
2.4.3 Inflammatory Changes Leading to Apoptosis
Investigations of cerebral arteries of patients who died after SAH and vasospasm revealed apoptotic changes of vascular endothelial cells [36]. The endothelial loss further reduces NO production exposing the bare vascular smooth muscles to spasmogenic substances like ET-1 to act directly. This apoptotic change is in response to a molecular cascade of events which is demonstrated in experimental studies and takes place through inflammatory mediators, e.g., tumor necrosis factor alfa and interleukin-1beta [37] and activated caspase-3 [35, 38].
In addition, release of inflammatory substances as a reaction to blood in the subarachnoid space potentiates spasmogenic effect and brain ischemia. Potent among them are thromboxane A2, serotonin released from platelets [39, 40], and ET-1 released from leucocytes [41]. Elevated ICAM-1 (intracellular adhesion molecule 1), TNF alfa, CD18 suggests interplay of various inflammatory mediators in response to SAH [42,43,44]. Studies suggest that there is c-Jun N-terminal kinase (JNK) pathway activation after SAH which is one of the signalling cassettes of mitogen-activated protein kinase (MAPK) pathways [45]. JNK is known to play an important role in cytokine production, inflammatory changes, and also apoptosis.
2.4.4 The Ischemic Insult
The very critical event after SAH is a sudden rise in the ICP which is dependent on the amount and duration of blood released in the subarachnoid space. Decreased perfusion of the brain contributes to global ischemia which has a serious consequence if it does not reverse early. An immediate impact on the cerebral blood flow is reflected in reduction of brain parenchymal oxygen pressure [46]. Though many patients may not survive the immediate impact of raised ICP, severe ischemic secondary insult in the surviving patients leads to blood–brain barrier (BBB) disruption [47] contributing to further brain damage, progressive cerebral edema [48] and delayed apoptosis of cerebral and vascular cells [22]. Any ischemia in the brain lasting for more than a few minutes will trigger a cascading chain reaction at the molecular level due to release of various biochemical substrates, which propagates BBB disruption. One of the inducible factors is HIF-1 which, when excessively activated, overexpresses its target gene VEGF (vascular endothelial growth factor) which increases BBB permeability. It also overexpresses BNIP3 and Nip3-like proteins, which are known mediators of apoptosis [49, 50]. Experimental studies using HIF-alpha inhibitors show attenuated expression of HIF-alpha with a reduction in vasospasm [51]. In addition to apoptosis triggered by activated HIF-1alpha and BNIP3 [50], elevated levels of pro-apoptotic p53 proteins in vasospastic cerebral arteries seem to play a role in the phenomenon of induction of vasospasm [52,53,54].
2.4.5 Free Oxygen Radicals
Autoxidation of hemoglobin leads to liberation of reactive oxygen species (ROS), which play a role in arterial narrowing. The use of antioxidants demonstrated reversal of its effect on experimental vasospasm [55, 56]. The effect of ROX on bilirubin leads to oxidation products of bilirubin which has an inhibiting effect on endothelial nitric oxide synthase (NOS) leading to dampening of physiological vasodilation because of reduced production of NO [57]. The role of ROS in vasoconstriction is also postulated because of its stimulation effect on production of vasoconstrictor metabolites of arachidonic acid which have shown to decrease cerebral blood flow by blocking calcium-activated potassium channels in experimental animals [58]. The superoxide radicals (SOR) produced after SAH from NADPH oxidase have an indirect vasoconstrictive effect as these SOR combine with NO to produce peroxynitrite which in turn inhibits eNOS [59]. This mechanism is corroborated by reversal of vasospasm using NADPH inhibitors experimentally [60].
2.4.6 Is Vasospasm All About Cerebral Vasculature?
Until recent past, cerebral vasospasm was related to constriction changes in cerebral vasculature as a result of reactive changes secondary to effect of blood and its products released in the subarachnoid space after SAH. However, the mechanism seems to be related to the phenomenon of spreading depression set off by glial cell dysfunction (Cortical Spreading Depolarization) which is heavily dependent upon the changes secondary to pathophysiology of SAH [61,62,63,64]. Following the event of SAH there is a marked change in the milieu of ions in the neuroglial cells resulting in a significant increase of extracellular potassium with simultaneous decrease of extracellular sodium, chloride, and calcium ions due to their influx in the cell along with water. This results in a state of EEG silence [65,66,67].
Normally increase in functional activity of brain is directly proportional to increase blood flow and oxygen uptake, which enhances metabolism and glucose uptake [68, 69]. This coupling of flow and metabolism is regulated by interaction between astrocytes, neurons, and endothelial cells, which is mediated by electrical and chemical changes in milieu contributed by agents like nitric oxide (NO), carbon dioxide, endothelin 1, alteration of ionic channels, adenosine, lipid peroxidation, and free radical production. The role of astrocytes in maintaining the local extracellular potassium concentration is important as they are described as perfect potassium electrodes [70], acting as a spatial buffer in local change of potassium [71].
Extracellular acidosis and hypercapnia have a linear correlation with cerebral vasodilation with maximum dilation achievable up to pH 7. This acidosis-induced dilation due to high extraluminal H+ concentration is mediated through activated KATP & KCa’, Even though there is contribution of NO in moderate increase in extraluminal proton concentration however its role becomes ineffective at a lower pH of 7 [72,73,74,75]. The aggravation of cerebral ischemia is augmented by periodic waves of Cortical Spreading Depolarization (CSD), which develop as a complex biochemical change secondary to oxyhemoglobin, ET-1, and K+ ions [76]. The major trigger for CSD is changed in ionic milieu which happens due to inactivation of Na+/K+-ATPase activity at synaptic membrane level after SAH [77]. CSD thus contributes to spasm in distal small vessels and cellular necrosis (Fig. 2.2).

Cortical Spreading depolarization
2.5 Diagnosis of Vasospasm
The diagnosis of vasospasm is best performed with a modality that can demonstrate the cerebral blood vessels and their caliber. Hence, CT angiogram (CTA), MR angiogram (MRA), or Digital Subtraction Angiography (DSA) are the options to study the vascular territory involved in vasospasm. However, all these modalities are appropriate to diagnose spasm in large and medium-size intracranial vessels but their utility in diagnosis of small vessels vasospasm is very limited. Though the diagnostic ability of these modalities is good for moderate-to-severe vasospasm but the logistic feasibility of repeating these studies precludes them for use in daily monitoring of status of vasospasm. DSA provides a more detailed picture of the status of vessels and the cross circulation but the intraluminal maneuvering of catheters and use of contrast medium can aggravate vasospasm in a spastic vessel [78]. CT perfusion studies are a useful substitute and can be helpful in diagnosing the imminent ischemia as well as the status of perfusion but the exact degree and distribution of spasm in the vasculature would not be apparent through this investigation.
Transcranial Doppler Ultrasound (TCD) is now being extensively used as a handy modality to assess the degree and extent of vasospasm. It has the logistic advantage of being noninvasive, easy to repeat, available at the bedside, and user friendly. The assessment through TCD is not only operator dependent but it has bearing on the anatomy of cerebral vasculature, exact site of vasospasm, the thickness of temporal bony window, viscosity of blood, ICP status, fluctuation of CO2, and systemic blood pressure levels. Though it does not fulfil all the needed criteria for a detailed diagnosis, it gives a fair reading of velocity of blood flow in all the major vessels, thus alerts the observer on the magnitude of impending or existing vasospasm. TCD diagnosis of vasospasm in the MCA has a sensitivity of 39–94% and specificity of 85–100% [79]. There are different windows of access to mainly three intracranial vessels namely, the most commonly used middle cerebral artery (MCA) and anterior cerebral artery (ACA) both through the thin temporal squama, the basilar artery (BI) through the foramen magnum, and the transorbital window for the anterior cerebral vessels. TCD monitoring should ideally be done on a daily basis and the mean velocity of MCA would normally be between 80 and 100 cm/s. The respective values for mild, moderate, and severe vasospasm of MCA are 100–120, 120–200, and >200 cm/s, respectively [80].
The Lindegaard ratio of flow velocity between MCA and extracranial Internal Carotid Artery (ICA), which has got an almost 90% accuracy of detecting angiographic vasospasm, is a useful method for diagnosis of vasospasm whereby vasospasm is established if the ratio of MCA/ICA is more than 3 and a value of 6 or more indicates very severe vasospasm [81, 82]. A similar ratio of flow between BA and extracranial vertebral artery (EVA) has been advocated to establish vasospasm of BA [83].
2.6 Management Options for Vasospasm
2.6.1 Trials on Targeted Substrates
2.6.1.1 Lipid Peroxidation Inhibitors
Since lipid peroxidation induced by free radicals has a potent role in inducing vasospasm hence its inhibition by a nonglucocorticoid 21-aminosteroid (Tirilazad mesylate) was tried by virtue of its radical scavenging action and membrane stabilizing properties. Tirilazad mesylate underwent a global multi-centric randomized, double-blind trial with an aim to look for improvement in vasospasm and outcome at 3 months follow up. Though there was a significant reduction of vasospasm using 6 mg/kg/day, the benefits failed to reach a statistical significance even though it showed better efficacy in males in contrast to female patients [84].
2.6.2 Role of Endothelin-1 Antagonist
Endothelin-1 an endogenous potent vasoconstrictor which maintains a balancing act with nascent NO, is a potent vasodilator, released by the endothelium of cerebral arteries. CSF studies after SAH demonstrate an increase in ET-1 levels. There are two types of Endothelin-1 receptors, Endothelin A (ETA) receptor and Endothelin B (ETB) receptor [85]. ETA is directly responsible for smooth muscle contraction and hence a random placebo-controlled trial (CONSCIOUS 1) with Endothelin 1A antagonist (Clazosentan) was carried out to look for relief from ischemia and infarction of the brain [6]. Though the trial demonstrated significant benefit in terms of angiographic vasospasm, it did not show any impact on DCI [7]. Subsequently, CONSCIOUS-2 and CONSCIOUS-3, Phase III trials were conducted, respectively, for clipped and coiled patients with no significant advantage on either mortality, morbidity, or long-term functional outcome [86].
2.6.3 Is There Any Role of Statins?
Due to the unique combination of anti-inflammatory properties, dampening effect on reactive oxygen production, upregulating effect on NO synthase, and reduction of excitotoxicity the statins were also tried to look for amelioration of vasospasm and DCI. Limited studies endorse some beneficial effects of statins but there was asymptomatic alteration in liver function noted as a side effect [87]. However, the STASH trial (Simvastatin in Aneurysmal Subarachnoid Hemorrhage Trial) could not establish the use of statins in acute phase of treatment of SAH [88].
2.6.4 Augmenting NO Activity
2.6.5 Sildenafil Citrate
Sildenafil citrate is a phosphodiesterase inhibitor which along with NO is known to relax the smooth muscles by preventing hydrolysis of cyclic guanosine monophosphate (cGMP) and inducing smooth muscle relaxation. Its role is already established in vertebrobasilar insufficiency, angina, and erectile dysfunction. Experimental studies suggested a beneficial effect of intrathecal sildenafil apart from its smooth muscle relaxation to produce changes in cognitive function [89]. To avoid the logistic implication of intrathecal sildenafil therapy, treatment through enteral route was tried on a series of patients in a pilot study which claims to show benefit in limited number of patients with refractory vasospasm. However, there were considerable side effects of the drug and no controlled study has been undertaken to prove its efficacy [90].
2.6.5.1 Nascent NO Donors
The mopping up of nascent NO released from the vascular endothelium by oxyhemoglobin is an important biochemical phenomenon that has a major implication in the pathophysiology of vasospasm. Hence, any therapy to augment the availability of NO would be a logical and efficacious way to prevent or reverse vasospasm [91]. The main hurdle is the ultra-short life of NO which remains active for a very brief period. Accordingly, intrathecal instillation of sodium nitroprusside as a potent NO donor was carried out in a study with very good angiographic evidence of reversal of vasospasm (Fig. 2.3). Though the study showed reversal of early vasospasm with its prevention in imminent cases, however, its role in refractory vasospasm was not established [92]. Other nitric oxide donors like NaNO2 were reported to be useful in animal models [93], but its efficacy in humans is yet to be established.

(a, b) Treatment of vasospasm using NO donor. (a) Pre-treatment and (b) Post-treatment. Reversal of vasospasm in a clipped patient with TCD value of 300 cm/s using intrathecal NO donor (sodium Nitroprusside) instillation. Note may be made on the effect of therapy on perforators
2.6.5.2 Magnesium Sulfate
Magnesium is long known to be an important cation, which has a role in various metabolic processes. Its role resembling a physiological calcium antagonist [94] was intensely studied with considerable improvement in DCI and vasospasm in animal studies [95, 96]. Magnesium Sulfate (MgSO4) was therefore put through Phase I and Phase II trials with potentially encouraging results. A subsequent Phase II trial IMASH (Intravenous Magnesium Sulfate for Aneurysmal Subarachnoid Hemorrhage) was undertaken which, however, failed to show any significant good outcome at 6 months [97]. A further MASH-II (Magnesium in Aneurysmal Subarachnoid Hemorrhage II Study) using Mg therapy for 20 days after SAH failed to demonstrate any beneficial effect [98]. The lower CSF penetration and the side effects of Mg therapy were considered as important reasons for the suboptimal response.
2.7 Treatment Regime for SAH/Vasospasm
2.7.1 Optimizing Physiological Disruption
2.7.1.1 Catecholamine Surge and Increased Sympathetic Activity
SAH is associated with increased catecholamine surge, which has a bearing on the prognosis [99, 100]. This in turn enhances sympathetic activity manifested in the form of cardiovascular changes recorded in ECG and also neurogenic pulmonary edema in severe cases [101]. Hence, close monitoring of cardiac and pulmonary function is of utmost importance specifically in patients manifesting with extracranial sympathetic manifestations and appropriate remedial measures are to be instituted, e.g., positive pressure ventilation for neurogenic pulmonary edema.
2.7.1.2 Controlling Body Temperature
Fever is a recognized entity in SAH which is common in patients with poor grade SAH or intraventricular hematomas [102]. For every degree Celsius change in body temperature, the glucose utilization demand in different areas of brain increases by 5 to 10%. Poor outcome has been documented with patients of SAH associated with fever [103]. Contrarily hypothermia has a protective effect on brain by reducing the rate of metabolism and free radical production, maintaining integrity of blood–brain barrier and aerobic metabolism and also lowering excitatory neurotransmitters release [104, 105]. The role of targeted temperature control therapy, therefore, is claimed in several studies to have a significantly beneficial role in restoring the alteration in brain metabolism secondary to SAH [106,107,108].
2.7.1.3 Electrolyte Management
Fluctuation in serum sodium levels is well known in SAH with observation of initial rise followed by significant fall in the second week [109]. The reason for hyponatremia is related to various factors which include cerebral salt wasting syndrome, SIADH, glucocorticoid deficiency. Despite hyponatremia being a known cause of reduced cerebral function and infarction of the brain, its contribution to poor outcomes is not clear [110].
Hypernatremia is commonly a manifestation of hypothalamic insult and may be associated with diabetes insipidus. It has been shown to have a poor outcome as per studies available [111, 112]. Based on the above observations serum sodium level within the normal physiological range is ideal even though the exact relationship of sodium imbalance with outcome is not fully established.
2.7.1.4 Maintaining Cerebral Perfusion
To counter the effects of decreased perfusion and poor blood flow secondary to vasospasm and DCI the triple H therapy (Hypervolemia, Hypertension, and Hemodilution) was in vogue with the aim to improve circulatory blood volume, cerebral perfusion pressure, and reduce the viscosity of blood. Low molecular weight dextran, mannitol, and albumin were used for volume expansion as a routine measure in the past. However, there was mounting evidence that hypervolemia and hemodilution were not be of much benefit [113, 114] with convincing evidence to suggest harmful effects of hemodilution [115, 116]. Hence induced hypertension, to maintain a high mean arterial pressure (MAP), remains one of the efficacious components of the regime, which is followed routinely in most of the centers [115]. Maintaining a high level of hemoglobin has also been seen to have contributed to better outcomes [116]. Since cerebral perfusion is guided by a balance between the intracranial pressure and the MAP there remains a role of anti-edema measures through pharmacological means as well as ventilation. Mannitol, which is a commonly used drug to reduce ICP, was also popular because of its volume expansion effect. However, there remains a concern in long-term use of mannitol due to its effect on blood rheology through serum osmolality changes, electrolyte imbalance, and rebound rise in ICP after its withdrawal. ICP reduction, in order to improve cerebral perfusion, is therefore better managed through controlled ventilation.
2.7.1.5 Calcium Channel Antagonists
Calcium channel blockers are known to act on the “slow calcium” channels and hence have a relaxing effect on vascular smooth muscles and cardiac muscles without any effect on skeletal muscle. Apart from their action on smooth muscle vasculature they are known to play a significant role in blood rheology, calcium entry in ischemic cells, dilation of collateral leptomeningeal vessels, and platelet aggregation [117,118,119].
2.7.1.6 Nimodipine
Dihydropyridine calcium antagonists are known to reduce spasm of vascular smooth muscles and amongst them nimodipine has been proved to have class I evidence to be efficacious in significant number of cases, more so, if it is prophylactically started on the day of SAH [78, 95, 113, 120, 121]. Nimodipine has been shown to also improve outcomes in DCI as it demonstrates a neuroprotective effect through a reduction in the degree of apoptosis by decreasing Ca influx and antiplatelet aggregation properties and also by improving collateral channels and blood rheology. Results of the British aneurysm nimodipine trial substantiate these facts with a significant reduction in incidence infarction and improvement in outcome [122, 123]. The treatment with nimodipine has shown to be cost-effective also with nominal side effects [124].
Nimodipine is administered by oral or intravenous route, ideally in an ICU setting, and the recommended dose is 60 mg every 4 hourly. In case this dose interferes with maintenance of desired MAP, required for sustained cerebral perfusion, a revised dose of 30 mg every 2 to 4 hourly may be administered under strict monitoring.
2.7.2 Strategies to Reduce Blood Load in Subarachnoid Space
2.7.2.1 Lumbar Drain
Since free blood remains the main spasmogenic source in the subarachnoid space (SAS) studies were conducted to reduce the blood load around the vessels in order to attenuate the harmful effect of blood or its products. The EARLY DRAIN Trial (Early Lumbar Cerebrospinal Fluid Drainage in Aneurysmal Subarachnoid Haemorrhage Trial) [125] and the LUMAS trial (Lumbar Drainage in Subarachnoid Haemorrhage Trial) [126] were instituted to look for decrease in the incidence of DCI and improved early clinical outcome. Both the studies were found to be safe and showed a reduction in the incidence of DCI with improvement in early clinical outcomes. However, the long-term clinical outcome did not reveal any significant improvement. Even then, the use of lumbar drain and removal of blood load in the basal cisterns during open surgery is still practiced by many clinicians with disputed claims of achieving lower incidence of ischemia and vasospasm [78]. However, one needs to be cautious as too much drainage of CSF is found to be associated with shunt dependency [126].
2.7.2.2 Cisternal Lavage and Local Thrombolytics
Studies conducted to look for efficacy of cisternal and ventricular lavage, mechanical agitation (kinetic therapy), and use of local thrombolytics were analyzed to see for reduction in DCI and improvement in outcome. The studies definitely suggest improvement in early outcome and reduced incidence of vasospasm in the group who are subjected to cisternal and/or ventricular lavage with added kinetic therapy. However, there are limitations of these procedures as it involves potential risk of infection and is a subject of logistic debate in patients who are treated purely be radiological intervention.
2.7.3 Intrathecal Treatment Options
2.7.3.1 Intrathecal Thrombolysis
Early and quick resolution of blood in subarachnoid space seems to be an attractive alternative to clear the blood from the thecal space. Several studies were undertaken using intracisternal thrombolysis using urokinase or tissue plasminogen activator to lyse the clot from the cisternal/intraventricular space. Recent meta-analysis suggests a clear advantage of intrathecal fibrinolysis showing improved functional outcome with lower mortality risk and lesser incidence of hydrocephalus [127, 128]. Despite claims of efficacy in this management, issues related to inconsistency of technical aspects cast a doubt on safety and side effects, infection and hemorrhage being of serious concern. A prospective randomized control trial on intraventricular thrombolysis is already underway to answer these important issues [129].
2.7.3.2 Intrathecal Nicardipine
Nicardipine, a calcium channel blocker which is used to treat hypertension and chronic angina, has been tried to treat vasospasm after SAH [130, 131]. The drug was used as a slow-release loaded polymer for local release which demonstrated promising results. However, the problems of logistics in delivery and its efficacy in the distant vascular tree, especially with thick load of blood clot in subarachnoid space around the vessel precluded it from coming into regular use.
2.7.4 Endovascular Intervention for Vasospasm
Endovascular treatment options for vasospasm are considered when the other options do not yield encouraging response to the clinician, even though they are not bereft of side effects and complications. The options include the use of intra-arterial drug infusions and balloon angioplasty [132, 133].
2.7.5 Role of Intra-arterial Pharmacotherapy
2.7.5.1 Intra-arterial Nimodipine
Since nimodipine is considered to be of proven efficacy as a calcium channel blocker its role in preventing and reversing vasospasm has been very much tried in various studies with reasonable success in controlling and reversing vasospasm specifically when it is in mild or moderate form. However, its efficacy in severe vasospasm with advanced DCI is not very well established. In a single-center study conducted in the recent past using intra-arterial nimodipine for vasospasm the outcome was good in 73.8% of patients [134].
2.7.5.2 Papaverine
Papaverine (a nonspecific phosphodiesterase inhibitor) which is a potent vasodilator was initially considered a useful agent for intra-arterial use. Though good vasodilation was achieved, the effect of the drug was short-lasting [135]. Moreover, intra-arterial papaverine did not last the test of time because of issues of unpredictable complications, e.g., systemic hypotension, brainstem function depression, seizures [136]. A comparison of intra-arterial papaverine and nimodipine was studied to see for the efficacy of each agent. Though papaverine has a diffuse effect on all the vessels in comparison to nimodipine (83%), there was no demonstrable difference in perfusion at the capillary level [137].
2.7.5.3 Milrinone
Milrinone, a phosphodiesterase III inhibitor, is widely used to treat patients with acute cardiac failure having a dual role of vasodilation and inotropic effect. This therapy has shown significant improvement in the patients of vasospasm including refractory vasospasm in patients of poor grade SAH [138]. Safety and efficacy of milrinone are being assessed in MilriSpasm Trial (Safety of Intravenous Milrinone for the Treatment of Subarachnoid Hemorrhage-induced Vasospasm) is due to complete in early 2021. The drug seems to hold a promise in reversing vasospasm through chemical angioplasty.
2.7.5.4 Balloon Angioplasty
Balloon angioplasty remains an important option for refractory vasospasm when pharmacotherapy fails. Though it gives relief from focal vasospasm it may not be very useful in diffuse vasospasm particularly if it involves distal vessels. More so, this therapy is ideally to be implemented in centers which are equipped with the facility and expertise. The procedure is not without any risk or failures and hence may need to be repeated several times during the phase of acute vasospasm. The controversy remains in the timing of mechanical balloon dilation where studies have shown the procedure to be effective if performed within the first 2 h of onset of vasospasm in contrast to that performed within 24 h [132, 139].
If normal or supranormal diameter of the vessel is achieved at initial angioplasty then subsequent need for angioplasty can be obviated in contrast to a subnormal dilatation where repeat dilations may be necessary [140]. The main limitation of mechanical angioplasty is in its effectiveness mainly in short segment vasospasm and it remains technically difficult to exploit its role in vasospasm involving long arterial segments or distal vessels. Hence, a combination of intra-arterial mechanical dilation and infusion using nimodipine was found to be more effective than isolated use of individual modalities and the effect was most pronounced on ICA and BA [141]. However, the procedure of mechanical angioplasty needs to be done with caution as there are reported complications which include perforation and rupture of vessels, occlusion, stroke, dissection, displacement of aneurysm clips. 144. Attempts for prophylactic dilation of major vessels to prevent vasospasm did not yield the desired outcome of preventing delayed ischemia of the brain [132].
The Invasive Diagnostic and Therapeutic Management of Cerebral Vasospasm After Aneurysmal Subarachnoid Haemorrhage trial (IMCVS) to sort out the optimal treatment modality has not been able to provide a defined guideline for treatment in individual cases [142]. However, endovascular treatment for vasospasm remains an effective alternative in situations of refractory vasospasm with comparatively better functional outcome [143].
2.8 Conclusion
Vasospasm, which is an important cause of morbidity and mortality, remains a major challenge in patients of SAH. Over the decades there is a definite improvement in outcome because of better perioperative management using aggressive treatment and prevention protocols. Understanding of the pathophysiological changes after SAH and identification of various substrates involved in its genesis has helped in formulating management guidelines yielding better outcome. The identity of primary trigger spasmogenic molecules remains illusive, and the cascading events initiated by activation of various biochemical pathways starting from release of oxyhemoglobin to oxygen free radicals and their consequences are yet to be precisely understood. In comparison to the past, the molecular changes and their impact are now better revealed but there has been no breakthrough in countering their impact on the brain. As various trials to date have failed to come out with a panacea the age-old concept of augmentation of cerebral perfusion, creation of an optimal milieu for the brain parenchyma still remains an important strategy for ICU management. Nimodipine is the only drug with proven efficacy but it fails to ameliorate all stages of vasospasm especially the refractory group. Hence, the emerging concept of “Early Brain Injury” and its prevention remains a major target for timely institution of treatment strategies in such patients.
References
Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis the Lancet. Neurology. 2011 Jul;10(7):626–36. https://doi.org/10.1016/S1474-4422(11)70109-0.
Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors: a prospective Finnish Cohort Study. Stroke. 2014;45:1958–63. https://doi.org/10.1161/STROKEAHA.114.005318.
Mensing LA, Greving JP, Verhoeff TA, Rinkel GJE, Ruigrok YM. Comparison of rupture risk of intracranial aneurysms between familial and sporadic patients. Stroke. 2019;50:1380–3. https://doi.org/10.1161/STROKEAHA.118.023783.
Karenberg A, Moog FP. Die Apoplexieimmedizinischen Schrifttum der Antike. Apoplexy in Ancient Medical Writings. Fortschritte der Neurologie-Psychiatrie. 1997;65(11):489–503. https://doi.org/10.1055/s-2007-996355.
Lawton MT, Vates GE. Subarachnoid hemorrhage. New Engl J Med. 2017;377:257–66. https://doi.org/10.1056/NEJMcp1605827.
Macdonald RL, Kassell NF, Mayer S, Ruefenacht D, Schmiedek P, Weidauer S, et al. Clazosentan to overcome neurological ischemia and infarction occurring after subarachnoid hemorrhage (CONSCIOUS-1): randomized, double-blind, placebo-controlled phase 2 dose-finding trial. Stroke. 2008 Nov;39(11):3015–21. https://doi.org/10.1161/STROKEAHA.108.519942.
Macdonald RL, Higashida RT, Keller E, Mayer SA, Molyneux A, Raabe A, et al. Clazosentan, an endothelin receptor antagonist, in patients with aneurysmal subarachnoid haemorrhage undergoing surgical clipping: a randomised, double-blind, placebo-controlled phase 3 trial (CONSCIOUS-2). Lancet Neurol. 2011 Jul;10(7):618–25. https://doi.org/10.1016/S1474-4422(11)70108-9.
Dorsch N. Therapeutic approaches to vasospasm in subarachnoid hemorrhage. Curr Opin Crit Care. 2002 Apr;8(2):128–33. https://doi.org/10.1097/00075198-200204000-00007.
Ecker A, Rimenschneider P. Arteriographic demonstration of spasm of the intracranial arteries with special reference to saccular arterial aneurysms. J Neurosurg. 1951 Nov;8(6):660–7. https://doi.org/10.3171/jns.1951.8.6.0660.
Weir B, Grace M, Hansen J, et al. Time course of vasospasm in man. J Neurosurg. 1978 Feb;48(2):173–8. https://doi.org/10.3171/jns.1978.48.2.0173.
Nornes H. The role of intracranial pressure in the arrest of hemorrhage in patients with ruptured intracranial aneurysms. J Neurosurg. 1973;39:226–34. https://doi.org/10.3171/jns.1973.39.2.0226.
Trojanowski T. Blood Elsevier brain barrier changes after experimental subarachnoid hemorrhage. Acta Neurochirurgica (Wien). 1982;60(1–2):45–54. https://doi.org/10.1007/BF01401749.
Baldwin ME, Loch Macdonald R, Huo D, Novakovia RL, Goldenberg FD, Frank JI, Rosengart AJ. Early vasospasm on admission angiography in patients with aneurysmal subarachnoid hemorrhage is a predictor for in-hospital complications and poor outcome. Stroke. 2004 Nov;35(11):2506–11. https://doi.org/10.1161/01.STR.0000144654.79393.cf.
Dreier JP, Ebert N, Priller J, Megow D, Lindauer U, Klee R, Reuter U, Imai Y, Einhäupl KM, Victorov I, Dirnagl U. Products of hemolysis in the subarachnoid space inducing spreading ischemia in the cortex and focal necrosis in rats: a model for delayed ischemic neurological deficits after subarachnoid hemorrhage? J Neurosurg. 2000 Oct;93(4):658–66. https://doi.org/10.3171/jns.2000.93.4.0658.
Ostrowski RP, Colohan AR, Zhang JH. Molecular mechanisms of early brain injury after subarachnoid hemorrhage. Neurol Res. 2006 Jun;28(4):399–414. https://doi.org/10.1179/016164106X115008.
Geraghty JR, Testai FD. Delayed cerebral ischemia after subarachnoid hemorrhage: beyond vasospasm and towards a multifactorial pathophysiology. Curr Atheroscler Rep. 2017 Oct 23;19(12):50. https://doi.org/10.1007/s11883-017-0690-x.
Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389:655–66.
Fujii M, Yan J, Rolland WB, Soejima Y, Caner B, Zhang JH. Early brain injury, an evolving frontier in subarachnoid hemorrhage research. Transl Stroke Res. 2013 Aug;4(4):432–46. https://doi.org/10.1007/s12975-013-0257-2.
Seifert V, Löffler B-M, Zimmermann M, Roux S, Stolke D. Endothelin concentrations in patients with aneurysmal subarachnoid hemorrhage: correlation with cerebral vasospasm, delayed ischemic neurological deficits and volume of hematoma. J Neurosurg. 1995 Jan;82(1):55–62. https://doi.org/10.3171/jns.1995.82.1.0055.
Zuccarello M, Bonasso C, Lewis A, Sperelakis N, Rapoport RM. Relaxation of subarchnoid hemorrhage-induced spasm of rabbit basilar artery by the K+ channel activator cromakalim. Stroke. 1996 Feb;27(2):311–6. https://doi.org/10.1161/01.str.27.2.311.
Sehba F, Bederson J. Mechanisms of acute brain injury after subarachnoid hemorrhage. Neurol Res. 2006 Jun;28(4):381–98. https://doi.org/10.1179/016164106X114991.
Cahill WJ, Calvert JH, Zhang JH. Mechanisms of early brain injury after subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2006 Nov;26(11):1341–53. https://doi.org/10.1038/sj.jcbfm.9600283.
Turner C, Bergeron M, Matz P, et al. Heme oxygenase-1 is induced in glia throughout brain by subarachnoid hemoglobin. J Cereb Blood Flow Metab. 1998 Mar;18(3):257–73. https://doi.org/10.1097/00004647-199803000-00004.
Vikman P, Beg S, Khurana T, Hansen-Schwartz J, Edvinsson L. Gene expression and molecular changes in cerebral arteries following subarachnoid hemorrhage in the rat. J Neurosurg. 2006 Sep;105(3):438–44. https://doi.org/10.3171/jns.2006.105.3.438.
Dietrich H, Dacey R. Molecular keys to the problems of cerebral vasospasm. Neurosurgery. 2000 Mar;46(3):517–30. https://doi.org/10.1097/00006123-200003000-00001.
Clark JF, Sharp FR. Bilirubin oxidation products (BOXes) and their role in cerebral vasospasm after subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2006 Oct;26(10):1223–33. https://doi.org/10.1038/sj.jcbfm.9600280.
Sharkey J, Butcher SP, Kelly JS. Endothelin-1 induced middle cerebral artery occlusion: pathological consequences and neuroprotective effects of MK801. J Auton Nerv Syst. 1994 Sep;49(Suppl):S177–85. https://doi.org/10.1016/0165-1838(94)90109-.
Gaetani P, Rodriguez y Baena R, Grignani G, Spanu G, Pacchiarini L and Paoletti P. Endothelin and aneurysmal subarachnoid haemorrhage: a study of subarachnoid cisternal cerebrospinal fluid. J Neurol Neurosurg Psychiatry. 1994;57:66–72.
Hansen-Schwartz J, Hoel NL, Zhou M, Xu CB, Svendgaard NA, Edvinsson L. Subarachnoid hemorrhage enhances endothelin receptor expression and function in rat cerebral arteries. Neurosurgery. 2003 May;52(5):1188–94.
Rothoerl RD, Ringel F. Molecular mechanisms of cerebral vasospasm following aneurysmal SAH. Neurol Res. 2007 Oct;29(7):636–42. https://doi.org/10.1179/016164107X240224.
Grassie ME, Moffat LD, Walsh MP, MacDonald JA. The myosin phosphatase targeting protein (MYPT) family: a regulated mechanism for achieving substrate specificity of the catalytic subunit of protein phosphatase type 1delta. Arch Biochem Biophys. 2011 Jun 15;510(2):147–59.
Miao L, Dai Y, Zhang J. Mechanism of RhoA/Rho kinase activation in endothelin-1-induced contraction in rabbit basilar artery. Am J Physiol Heart Circ Physiol. 2002 Sep;283(3):H983–9. https://doi.org/10.1152/ajpheart.00141.2002.
Kikkawa Y, Matsuo S, Kameda K, Hirano M, Nakamizo A, Sasaki T, Hirano K. Mechanisms underlying potentiation of endothelin-1-induced myofilament Ca(2+) sensitization after subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2012 Feb;32(2):341–52. https://doi.org/10.1038/jcbfm.2011.132.
Nakamura K, Koga Y, Sakai H, Homma K, Ikebe M. cGMP-dependent relaxation of smooth muscle is coupled with the change in the phosphorylation of myosin phosphatase. Circ Res. 2 Aug 2007;(101):712–22. https://doi.org/10.1161/CIRCRESAHA.107.153981.
Zhou C, Yamaguchi M, Kusaka G, Schonholz C, Nanda A, Zhang JH. Caspase inhibitors prevent endothelial apoptosis and cerebral vasospasm in dog model of experimental subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2004 Apr;24(4):419–31. https://doi.org/10.1097/00004647-200404000-00007.
Zubkov AY, Ogihara K, Bernanke DH, Parent AD, Zhang J. Apoptosis of endothelial cells in vessels affected by cerebral vasospasm. Surg Neurol. 2000 Mar;53(3):260–6. https://doi.org/10.1016/s0090-3019(99)00187-1.
Kimura H, Gules I, Meguro T, Zhang JH. Cytotoxicity of cytokines in cerebral microvascular endothelial cell. Brain Res. 2003 Nov 14;990(1–2):148–56. https://doi.org/10.1016/s0006-8993(03)03450-4.
Iseda K, Ono S, Onoda K, Satoh M, Manabe H, Nishiguchi M, Takahashi K, Tokunaga K, Sugiu K, Date I. Antivasospastic and antiinflammatory effects of caspase inhibitor in experimental subarachnoid hemorrhage. J Neurosurg. 2007 Jul;107(1):128–35. https://doi.org/10.3171/JNS-07/07/0128.
Satoh S, Suzuki Y, Harada T, Ikegaki I, Asano T, Shibuya M, Sugita K, Saito A. The role of platelets in the development of cerebral vasospasm. Brain Res Bull. 1991 Nov;27(5):663–8. https://doi.org/10.1016/0361-9230(91)90042-i.
Takeuchi H, Tanabe M, Okamoto H, Yamazaki M. Effects of thromboxane synthetase inhibitor (RS-5186) on experimentally-induced cerebral vasospasm. Neurol Res. 1999 Jul;21(5):513–6.
Fassbender K, Hodapp B, Rossol S, Bertsch T, Schmeck J, Schutt S, Fritzinger M, Horn P, Vajkoczy P, Wendel-Wellner M, Ragoschke A, Kuehl S, Brunner J, Schurer L, Schmiedeck P, Hennerici M. Endothelin-1 in subarachnoid hemorrhage: an acute-phase reactant produced by cerebrospinal fluid leukocytes. Stroke. 2000 Dec;31(12):2971–5. https://doi.org/10.1161/01.str.31.12.2971.
Polin RS, Bavbek M, Shaffrey ME, Billups K, Bogaev CA, Kassell NF, Lee KS. Detection of soluble E-selectin, ICAM-1, VCAM-1, and L-selectin in the cerebrospinal fluid of patients after subarachnoid hemorrhage. J Neurosurg. 1998 Oct;89(4):559–67. https://doi.org/10.3171/jns.1998.89.4.0559.
Bavbek M, Polin R, Kwan AL, Arthur AS, Kassell NF, Lee KS. Monoclonal antibodies against ICAM-1 and CD18 attenuate cerebral vasospasm after experimental subarachnoid hemorrhage in rabbits. Stroke. 1998 Sep;29(9):1930–5. https://doi.org/10.1161/01.str.29.9.1930.
Prunell GF, Svendgaard NA, Alkass K, Mathiesen T. Inflammation in the brain after experimental subarachnoid hemorrhage. Neurosurgery. 2005 May;56(5):1082–92.
Allen BG, Walsh MP. The biochemical basis of the regulation of smooth-muscle contraction. Trends Biochem Sci. 1994 Sep;19(9):362–8. https://doi.org/10.1016/0968-0004(94)90112-0.
Hoffman WE, Wheeler P, Edelman G, Charbel FT, Torres NJ, Ausman JI. Hypoxic brain tissue following subarachnoid hemorrhage. Anesthesiology. 2000 Feb;92(2):442–6. https://doi.org/10.1097/00000542-200002000-00026.
Park S, Yamaguchi M, Zhou C, Calvert JW, Tang J, Zhang JH. Neurovascular protection reduces early brain injury after subarachnoid hemorrhage. Stroke. 2004;35(2412–2417) https://doi.org/10.1161/01.STR.0000141162.29864.e9.
Jan Claassen J, Carhuapoma R, Kreiter KT, Du EY, Sander Connolly E, Mayer SA. Global cerebral edema after subarachnoid hemorrhage: frequency, predictors, and impact on outcome. Stroke. 2002;33:1225–32. https://doi.org/10.1161/01.STR.0000015624.29071.1F.
Semenza GL. Regulation of oxygen homeostasis by hypoxia-inducible factor 1. Physiology (Bethesda, MD). 2009 Apr;24:97–106. https://doi.org/10.1152/physiol.00045.2008.
Schmidt-Kastner R, Aguirre-Chen C, Kietzmann T, Saul I, Busto R, Ginsberg MD. Nuclear localization of the hypoxia-regulated pro-apoptotic protein BNIP3 after global brain ischemia in the rat hippocampus. Brain Res. 2004 Mar 19;1001(1–2):133–42. https://doi.org/10.1016/j.brainres.2003.11.065.
Yan J, Chen C, Lei J, Yang L, Wang K, Liu J, Zhou C. 2-methoxyestradiol reduces cerebral vasospasm after 48 hours of experimental subarachnoid hemorrhage in rats. Exp Neurol. 2006;202(2):348–56.
Cahill J, Calvert JW, Solaroglu I, Zhang JH. Vasospasm and p53-induced apoptosis in an experimental model of subarachnoid hemorrhage. Stroke. 2006 Jul;37(7):1868–74. https://doi.org/10.1161/01.STR.0000226995.27230.96.
Cahill J, Calvert JW, Marcantonio S, Zhang JH. p53 may play an orchestrating role in apoptotic cell death after experimental subarachnoid hemorrhage. Neurosurgery. 2007 Mar;60(3):531–45. https://doi.org/10.1227/01.NEU.0000249287.99878.9B.
Pearl JD, Macdonald RL. Vasospasm after aneurysmal subarachnoid hemorrhage: need for further study. Acta Neurochir Suppl. 2008;105:207–10.
Guney O, Erdi F, Esen H, Kiyici A, Kocaogullar Y. N-acetylcysteine prevents vasospasm after subarachnoid hemorrhage. World Neurosurg. 2010 Jan;73(1):42–9. https://doi.org/10.1016/j.surneu.2009.06.003.
Munakata A, Ohkuma H, Shimamura N. Effect of a free radical scavenger, edaravone, on free radical reactions: related signal transduction and cerebral vasospasm in the rabbit subarachnoid hemorrhage model. Acta Neurochir Suppl. 2011;110(Pt 2):17–22. https://doi.org/10.1007/978-3-7091-0356-2_4.17-22.
Hofmann F. The biology of cyclic GMP-dependent protein kinases. J Biol Chem. 2005 Jan;280(1):1–4. https://doi.org/10.1074/jbc.R400035200.
Kehl F, Cambj-Sapunar L, Maier KG, Miyata N, Kametani S, Okamoto H, Hudetz AG, Schulte ML, Zagorac D, Harder DR, Roman RJ. 20-HETE contributes to the acute fall in cerebral blood flow after subarachnoid hemorrhage in the rat. Am J Physiol Heart Circ Physiol. 2002 Apr;282(4):H1556–65. https://doi.org/10.1152/ajpheart.00924.200.
Kim DE, Suh YS, Lee MS, Kim KY, Lee JH, Lee HS, Hong KW, Kim CD. Vascular NAD(P)H oxidase triggers delayed cerebral vasospasm after subarachnoid hemorrhage in rats. Stroke. 2002 Nov;33(11):2687–91. https://doi.org/10.1161/01.str.0000033071.99143.9e.
Zheng JS, Zhan RY, Zheng SS, Zhou YQ, Tong Y, Wan S. Inhibition of NADPH oxidase attenuates vasospasm after experimental subarachnoid hemorrhage in rats. Stroke. 2005 May;36(5):1059–64. https://doi.org/10.1161/01.STR.0000163102.49888.b7.
Pyne-Geithman GJ, Caudell DN, Prakash P, Clark JF. Glutathione peroxidase and subarachnoid hemorrhage: implications for the role of oxidative stress in cerebral vasospasm. Neurol Res. 2009 Mar;31(2):195–9. https://doi.org/10.1179/174313209X393906.
Pluta RM, Hansen-Schwartz J, Dreier J, et al. Cerebral vasospasm following subarachnoid hemorrhage: time for a new world of thought. Neurol Res. 2009 Mar;31(2):151–8. https://doi.org/10.1179/174313209X393564.
Andresen J, Shafi NI, Bryan RM Jr. Endothelial influences on cerebrovascular tone. J Appl Physiol. 2006 Jan;100(1):318–27. https://doi.org/10.1152/japplphysiol.00937.2005.
Kolias AG, Sen J, Belli A. Pathogenesis of cerebral vasospasm following aneurysmal subarachnoid hemorrhage: putative mechanisms and novel approaches. J Neurosci Res. 2009 Jan;87(1):1–11. https://doi.org/10.1002/jnr.21823.
Leao AA. Spreading depression of activity in the cerebral cortex. J Neurophysiol. 1944;7:359–90.
Leao AA. Further observations on the spreading depression of activity in the cerebral cortex. J Neurophysiol. 1947 Nov;10(6):409–14. https://doi.org/10.1152/jn.1947.10.6.409.
Dreier JP, Woitzik J, Fabricius M, Bhatia R, Major S, Drenckhahn C, Lehmann T-N, Sarrafzadeh A, Willumsen L, Hartings JA, Sakowitz OW, Seemann JH, Thieme A, Lauritzen M, Strong AJ. Delayed ischaemic neurological deficits after subarachnoid haemorrhage are associated with clusters of spreading depolarizations. Brain. 2006 Dec;129(Pt 12):3224–37. https://doi.org/10.1093/brain/awl297.
Sotero RC, Trujillo-Barreto NJ. Biophysical model for integrating neuronal activity, EEG, fMRI and metabolism. Neuroimage. https://doi.org/10.1016/j.neuroimage.2007.08.001.
Filosa JA. Vascular tone and neurovascular coupling: considerations toward an improved in vitro model. Front Neuroenergetics. 2010;2:16. https://doi.org/10.3389/fnene.2010.00016.
Gardner-Medwin AR. Analysis of potassium dynamics in mammalian brain tissue. J Physiol. 1983 Feb;335:393–426. https://doi.org/10.1113/jphysiol.1983.sp014541.
Orellana JA, Sáez PJ, Shoji KF, Schalper KA, Palacios-Prado N, Velarde V, Giaume C, Bennett MVL, Sáez JC. Modulation of brain hemichannels and gap junction channels by pro-inflammatory agents and their possible role in neurodegeneration. Antioxid Redox Signal. 2009;11:369–99.
Lindauer U, Kunz A, Schuh-Hofer S, Vogt J, Dreier JP, Dirnagl U. Nitric oxide from perivascular nerves modulates cerebral arterial pH reactivity. Am J Physiol Heart Circ Physiol. 2001 Sep;281(3):H1353–63. https://doi.org/10.1152/ajpheart.2001.281.3.H1353.
Horiuchi T, Dietrich HH, Hongo K, Goto T, Dacey RG Jr. Role of endothelial nitric oxide and smooth muscle potassium channels in cerebral arteriolar dilation in response to acidosis. Stroke. 2002;33:844–9. https://doi.org/10.1161/hs0302.104112.
Lindauer U, Vogt J, Schuh-Hofer S, Dreier JP, Dirnagl U. Cerebrovascular vasodilation to extraluminal acidosis occurs via combined activation of ATP-sensitive and Ca2+-activated potassium channels. J Cereb Blood Flow Metab. 2003;23:1227–38.
Celotto AC, Capellini VK, Baldo CF, Dalio MB, Rodrigues AJ, Evora PRB. Effects of acid-base imbalance on vascular reactivity. Braz J Med Biol Res. 2008 Jun;41(6):439–45. https://doi.org/10.1590/s0100-879x2008005000026.
Kleeberg J, Petzold GC, Major S, Dirnagl U, Dreier JP. ET-1 induces cortical spreading depression via activation of the ETA receptor/phospholipase C pathway in vivo. Am J Physiol Heart Circ Physiol. 2004;286:H1339–46.
Yufu K, Itoh T, Edamatsu R, Mori A, Hirakawa M. Effect of hyperbaric oxygenation on the Na+, K(+)-ATPase and membrane fluidity of cerebrocortical membranes after experimental subarachnoid hemorrhage. Neurochem Res. 1993;18:1033–9.
Mortimer AM, Steinfort B, Faulder K, Bradford C, Finfer S, Assaad N, Harrington T. The detrimental clinical impact of severe angiographic vasospasm may be diminished by maximal medical therapy and intensive endovascular treatment. J Neurointerv Surg. 2015 Dec;7(12):881–7. https://doi.org/10.1136/neurintsurg-2014-011403.
Chugh C, Agarwal H. Cerebral vasospasm and delayed cerebral ischemia: Review of literature and the management approach. Neurol India. 2019;67(1):185–200. https://doi.org/10.4103/0028-3886.253627.
Treggiari MM. Hemodynamic management of subarachnoid hemorrhage. Neurocrit Care. 2011 Sep;15(2):329–35. https://doi.org/10.1007/s12028-011-9589-5.
Lindegaard KF, Nornes H, Bakke SJ, Sorteberg W, Nakstad P. Cerebral vasospasm after subarachnoid hemorrhage investigated by means of transcranial Doppler ultrasound. Acta Neurochir Suppl (Wien). 1988;42:81–4. https://doi.org/10.1007/978-3-7091-8975-7_16.
Meyer R, Deem S, Yanez ND, Souter M, Lam A, Treggiari MM. Current practices of triple-H prophylaxis and therapy in patients with subarachnoid hemorrhage. Neurocrit Care. 2011 Feb;14(1):24–36. https://doi.org/10.1007/s12028-010-9437-z.
Soustiel JF, Shik V, Shreiber R, Tavor Y, Goldsher D. Basilar vasospasm diagnosis. Stroke. 2002;33:72–8.
Kassell NF, Haley EC Jr, Apperson-Hansen C, Alves WM. Randomized, double-blind, vehicle-controlled trial of tirilazad mesylate in patients with aneurysmal subarachnoid hemorrhage: a cooperative study in Europe, Australia, and New Zealand. J Neurosurg. 1996 Feb;84(2):221–8. https://doi.org/10.3171/jns.1996.84.2.0221.
Pollock DM, Keith TL, Highsmith RF. Endothelin receptors and calcium signaling. FASEB J. 1995 Sep;9(12):1196–204. https://doi.org/10.1096/fasebj.9.12.7672512.
Macdonald RL, Higashida RT, Keller E, Mayer SA, Molyneux A, Raabe A, Vajkoczy P, Wanke I, Frey A, Marr A, Roux S, Kassell NF. Preventing vasospasm improves outcome after aneurysmal subarachnoid hemorrhage: rationale and design of CONSCIOUS-2 and CONSCIOUS-3 trials. Neurocrit Care. 2010 Dec;13(3):416–24. https://doi.org/10.1007/s12028-010.
Tseng MY. Summary of evidence on immediate statins therapy following aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2011 Sep;15(2):298–301. https://doi.org/10.1007/s12028-011-9596-6.
Kirkpatrick PJ, Turner CL, Christopher Smith PJ, Hutchinson PG, Murray D. Simvastatin in aneurysmal subarachnoid haemorrhage (STASH): a multicentre randomised phase 3 trial. Lancet. 2014;13:666–75.
Kruuse C, Gupta S, Nilsson E, Kruse L, Edvinsson L. Differential vasoactive effects of sildenafil and tadalafil on cerebral arteries. Eur J Pharmacol. 2012 Jan 15;674(2–3):345–51. https://doi.org/10.1016/j.ejphar.2011.10.037.
Mukherjee KK, Singh SK, Khosla VK, Mohindra S, Salunke P. Safety and efficacy of sildenafil citrate in reversal of cerebral vasospasm: a feasibility study. Surg Neurol Int. 2012;3:3. https://doi.org/10.4103/2152-7806.92164.
Fathi AR, Bakhtian KD, Pluta RM. The role of nitric oxide donors in treating cerebral vasospasm after subarachnoid hemorrhage. Acta Neurochir Suppl. 2011;110(Pt 1):93–7. https://doi.org/10.1007/978-3-7091-0353-1_17.
Pathak A, Mathuriya SN, Khandelwal N, Verma K. Intermittent low dose intrathecal sodium nitroprusside therapy for treatment of symptomatic aneurysmal SAH-induced vasospasm. Br J Neurosurg. 2003 Aug;17(4):306–10. https://doi.org/10.1080/02688690310001601180.
Fathi AR, Pluta RM, Bakhtian KD, Qi M, Lonser RR. Reversal of cerebral vasospasm via intravenous sodium nitrite after subarachnoid hemorrhage in primates. J Neurosurg. 2011 Dec;115(6):1213–20. https://doi.org/10.3171/2011.7.JNS11390.
Iseri LT, French JH. Magnesium: nature’s physiologic calcium blocker. Am Heart J. 1984;108:188–93.
Castanares-Zapatero D, Hantson P. Pharmacological treatment of delayed cerebral ischemia and vasospasm in subarachnoid hemorrhage. Ann Intens Care. 2011;1:12. https://doi.org/10.1186/2110-5820-1-12.
Suarez JI. Magnesium sulfate administration in subarachnoid hemorrhage. Neurocrit Care. 2011 Sep;15(2):302–7. https://doi.org/10.1007/s12028-011-9603-y.
Wong GK, Poon WS, Chan MT, Boet R, Gin T, Ng SC, Zee BC. Intravenous magnesium sulphate for aneurysmal subarachnoid hemorrhage (IMASH): a randomized, double-blinded, placebo-controlled, multicenter phase III trial. Stroke. 2010 May;41(5):921–6. https://doi.org/10.1161/STROKEAHA.109.571125.
Vergouwen MD. Magnesium sulfate for aneurysmal subarachnoid hemorrhage: the end of the road or more trials? Crit Care (London, Engl). 2011;15(2):140. https://doi.org/10.1186/cc10055.
Benedict CR, Loach AB. Sympathetic nervous system activity in patients with subarachnoid hemorrhage. Stroke. 1978;9(3):237–44. https://doi.org/10.1161/01.str.9.3.237.
Ogura T, Satoh A, Ooigawa H, Sugiyama T, Takeda R, Fushihara G, et al. Characteristics and prognostic value of acute catecholamine surge in patients with aneurysmal subarachnoid hemorrhage. Neurol Res. 2012 Jun;34(5):484–90. https://doi.org/10.1179/1743132812Y.0000000033.
Hall A, O’Kane R. The extracranial consequences of subarachnoid hemorrhage. World Neurosurg. 2018 Jan;109:381–92. https://doi.org/10.1016/j.wneu.2017.10.016.
Fernandez A, Schmidt JM, Claassen J, Pavlicova M, Huddleston D, Kreiter KT, Ostapkovich ND, Kowalski RG, Parra A, Sander Connolly E, Mayer SA. Fever after subarachnoid hemorrhage: risk factors and impact on outcome. Neurology. 2007 Mar 27;68(13):1013–9. https://doi.org/10.1212/01.wnl.0000258543.45879.f5.
Kramer CL, Pegoli M, Mandrekar J, Lanzino G, Rabinstein AA. Refining the association of fever with functional outcome in aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2017 Feb;26(1):41–7. https://doi.org/10.1007/s12028-016-0281-7.
Schubert GA, Poli S, Schilling L, Heiland S, Thomé C. Hypothermia reduces cytotoxic edema and metabolic alterations during the acute phase of massive SAH: a diffusion-weighted imaging and spectroscopy study in rats. J Neurotrauma. 2008;25:841–52.
Török E, Klopotowski M, Trabold R, Thal SC, Plesnila N, Schöller K. Mild hypothermia (33 °C) reduces intracranial hypertension and improves functional outcome after subarachnoid hemorrhage in rats. Neurosurgery. 2009;65:352–9.
Badjatia N, Fernandez L, Schmidt JM, Lee K, Claassen J, Connolly ES, Mayer SA. Impact of induced normothermia on outcome after subarachnoid hemorrhage: a case-control study. Neurosurgery. 2010;66(4):696–700. https://doi.org/10.1227/01.NEU.0000367618.42794.AA.
Kuramatsu JB, Kollmar R, Gerner ST, Madzar D, Pisarcikova A, Staykov D, et al. Is hypothermia helpful in severe subarachnoid hemorrhage? An exploratory study on macro vascular spasm, delayed cerebral infarction and functional outcome after prolonged hypothermia. Cerebrovasc Dis (Basel, Switzerland). 2015;40(5–6):228–35. https://doi.org/10.1159/000439178.
Choi W, Kwon SC, Lee WJ, CheolWeon Y, Choi B, Lee H, Park ES, Ahn R. Feasibility and safety of mild therapeutic hypothermia in poor-grade subarachnoid hemorrhage: prospective pilot study. J Kor Med Sci. 2017 Aug;32(8):1337–44. https://doi.org/10.3346/jkms.2017.32.8.1337.
Okazaki T, Hifumi T, Kawakita K, Shishido H, Ogawa D, Okauchi M. Atsushi Shindo, Masahiko Kawanishi, Takashi Tamiya, Yasuhiro Kuroda. Target serum sodium levels during intensive care unit management of aneurysmal subarachnoid hemorrhage. Shock. 2017 Nov;48(5):558–63. https://doi.org/10.1097/SHK.0000000000000897.
Shah K, Turgeon RD, Gooderham PA, Ensom MHH. Prevention and treatment of hyponatremia in patients with subarachnoid hemorrhage: a systematic review. World Neurosur. 2018;109:222–9.
Beseoglu K, Etminan N, Steiger HJ, Hanggi D. The relation of early hypernatremia with clinical outcome in patients suffering from aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 2014 Aug;123:164–8. https://doi.org/10.1016/j.clineuro.2014.05.022.
Spatenkova V, Bradac O, de Lacy P, Skrabalek P, Suchomel P. Dysnatremia as a poor prognostic indicator in patients with acute subarachnoid hemorrhage. J Neurosurg Sci. 2017 Aug;61(4):371–9. https://doi.org/10.23736/S0390-5616.16.03411-1.
Rabinstein AA, Lanzino G, Wijdicks EF. Multidisciplinary management and emerging therapeutic strategies in aneurysmal subarachnoid haemorrhage. Lancet Neurol. 2010 May;9(5):504–19. https://doi.org/10.1016/S1474-4422(10)70087-9.
Wolf S. Routine management of volume status after aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2011 Jul;10(7):626–36. https://doi.org/10.1016/S1474-4422(11)70109-0.
Diringer MN, Bleck TP, Claude Hemphill J, Menon D, Shutter L, Vespa P, Bruder N, Connolly ES Jr, Citerio G, Gress D, Hanggi D, Hoh BL, Lanzino G, Le Roux P, Rabinstein A, Schmutzhard E, Stocchetti N, Suarez JI, Treggiari M, Tseng MY, Vergouwen MD, Wolf S, Zipfel G. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care. 2011;15:211–40.
Chittiboina P, Conrad S, McCarthy P, Nanda A, Guthikonda B. The evolving role of hemodilution in treatment of cerebral vasospasm: a historical perspective. World Neurosurg. 2011;75(5–6):660–4. https://doi.org/10.1016/j.wneu.2011.02.019.
Schanne FA, Kane AB, Young EE, Farber JL. Calcium dependence of toxic cell death: a final common pathway. Science (New York, NY). 1979 Nov 9;206(4419):700–2. https://doi.org/10.1126/science.386513.
Auer LM. Pial arterial vasodilation by intravenous nimodipine in cats. Arzneimittelforschung. 1981;31(9):1423–5.
Dale J, Landmark KH, Myhre E. The effects of nifedipine, a calcium antagonist, on platelet function. Am Heart J. 1983 Jan;105(1):103–5. https://doi.org/10.1016/0002-8703(83)90285-5.
Allen GS, Ahn HS, Preziosi TJ, Battye R, Boone SC, Boone SC. Cerebral arterial spasm: A controlled trial of nimodipine in patients with subarachnoid hemorrhage. New Engl J Med. 1983 Mar 17;308(11):619–24. https://doi.org/10.1056/NEJM198303173081103.
Mees SMD, Rinkel GJE, Feigin VL, Algra A, van den Bergh WM, Vermeulen M, van Gijn J. Calcium antagonists for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev. 2007 Jul 18;2007(3):CD000277. https://doi.org/10.1002/14651858.CD000277.
Pickard JD, Murray GD, Illingworth R, Shaw MD, Teasdale GM, Foy PM, Humphrey PR, Lang DA, Nelson R, Richards P. Effect of oral nimodipine on cerebral infarction and outcome after subarachnoid haemorrhage: British aneurysm nimodipine trial. BMJ. 1989 Mar 11;298(6674):636–42. https://doi.org/10.1136/bmj.298.6674.636.
Murray GD. Surgical bleeding and calcium antagonists. British aneurysm nimodipine trial reported improved clinical outcome with nimodipine. Br Med J. 1995; https://doi.org/10.1136/bmj.311.7001.388c.
Karinen P, Koivukangas P, Ohinmaa A, Koivukangas J, Ohman J. Cost-effectiveness analysis of nimodipine treatment after aneurysmal subarachnoid hemorrhage and surgery. J Neurosurg. 1988 Nov;69(5):683–6. https://doi.org/10.3171/jns.1988.69.5.0683.
Bardutzky J, Witsch J, Juttler E, Schwab S, Vajkoczy P, Wolf S. EARLYDRAIN- outcome after early lumbar CSF-drainage in aneurysmal subarachnoid hemorrhage: study protocol for a randomized controlled trial. Randomized Controlled Trials. 2011;12:203.
Al-Tamimi YZ, Bhargava D, Feltbower RG, Hall G, Goddard AJ, Quinn AC. Lumbar drainage of cerebrospinal fluid after aneurysmal subarachnoid hemorrhage: a prospective, randomized, controlled trial (LUMAS). Stroke. 2012 Mar;43(3):677–82. https://doi.org/10.1161/STROKEAHA.111.625731.
Yamamoto T, Esaki T, Nakao Y, Mori K. Efficacy of low-dose tissue-plasminogen activator intracisternal administration for the prevention of cerebral vasospasm after subarachnoid hemorrhage. World Neurosurg. 2010;73:675–82. https://doi.org/10.1016/j.wneu.2010.04.002.
Lu X, ChengyuanJi JW, You W, Wang W, Wang Z, Chen G. Intrathecal fibrinolysis for aneurysmal subarachnoid hemorrhage: evidence from randomized controlled trials and Cohort studies. Front Neurol. 2019;10:885. https://doi.org/10.3389/fneur.2019.00885.
Gaberel T. Intraventricular Fibrinolysis for Aneurysmal Subarachnoid Hemorrhage (FIVHeMA). Available online https://clinicaltrials.gov/ct2/show/NCT03187405. Accessed 01 February 2019.
Kasuya H, Onda H, MikihikoTakeshita YO, Hori T. Efficacy and safety of nicardipine prolonged-release implants for preventing vasospasm in humans. Stroke. 2002 Apr;33(4):1011–105. https://doi.org/10.1161/01.str.0000014563.75483.22.
Kasuya H, Onda H, Sasahara A. Application of nicardipine prolonged-release implants: analysis of 97 consecutive patients with acute subarachnoid hemorrhage. Neurosurgery. 2005 May;56(5):895–902.
Rosenwasser RH, Armonda RA, Thomas JE, Benitez RP, Gannon PM, Harrop J. Therapeutic modalities for the management of cerebral vasospasm: timing of endovascular options. Neurosurgery. 1999;44:975–9.
Zwienenberg-Lee M, Hartman J, Rudisill N, Madden LK, Smith K, Eskridge J. Effect of prophylactic transluminal balloon angioplasty on cerebral vasospasm and outcome in patients with Fisher grade III subarachnoid hemorrhage: results of a phase II multicenter, randomized, clinical trial. Stroke. 2008;39:1759–65.
Narayan V, Pendharkar H, Devi BI, Bhat DI, Shukla DP. Aggressive management of vasospasm with direct intra-arterial nimodipine therapy. Neurol India. 2018;66(2):416–22.
Vajkoczy P, Horn P, Bauhuf C, Munch E, Hubner U, Ing D, Thome C, Poeckler-Schoeninger C, Roth H, Schmiedek P. Effect of intra-arterial papaverine on regional cerebral blood flow in hemodynamically relevant cerebral vasospasm. Stroke. 2001;32:498–50. https://doi.org/10.1161/01.STR.32.2.498.
Firlik KS, Kaufmann AM, Firlik AD, Jungreis CA, Yonas H. Intra-arterial papaverine for the treatment of cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Surg Neurol. 1999 Jan;51(1):66–74. https://doi.org/10.1016/s0090-3019(97)00370-4.
Kerz T, Boor S, Beyer C, Welschehold S, Schuessler A, Oertel J. Effect of intraarterial papaverine or nimodipine on vessel diameter in patients with cerebral vasospasm after subarachnoid hemorrhage. Br J Neurosurg. 2012 Aug;26(4):517–24. https://doi.org/10.3109/02688697.2011.6507373.
Abulhasan YB, Jimenez JO, Teitelbaum J, Simoneau G, Angle MR. Milrinone for refractory cerebral vasospasm with delayed cerebral ischemia. J Neurosurg. 134(3):971–82.
Bejjani GK, Bank WO, Olan WJ, Sekhar LN. The efficacy and safety of angioplasty for cerebral vasospasm after subarachnoid hemorrhage. Neurosurgery. 1998;42:979–86.
Miley JT, Tariq N, Souslian FG, Qureshi N, Suri MF, Tummala RP. Comparison between angioplasty using compliant and noncompliant balloons for treatment of cerebral vasospasm associated with subarachnoid hemorrhage. Neurosurgery. 2011 Dec;69(2 Suppl):ons161-8. https://doi.org/10.1227/NEU.0b013e31822a8976.
Kerz T, Boor S, Ulrich A, Beyer C, Hechtner M, Mueller-Forell W. Endovascular therapy for vasospasm after aneurysmatic subarachnoid hemorrhage. Br J Neurosurg. 2016 Oct;30(5):549–53. https://doi.org/10.3109/02688697.2016.1173193.
The invasive diagnostic and therapeutic management of cerebral vasospasm after aneurysmal subarachnoid haemorrhage trial (IMCVS) as cited by Chandril Chugh, Himanshu Agarwal in Cerebral vasospasm and delayed cerebral ischemia: Review of literature and the management approach. Neurol India. 2019; 67(1):185–200.
Sokolowski JD, Chen C-J, Ding D, Buell TJ, Raper DM, Ironside N, Taylor DG, Starke RM, Liu K. Endovascular treatment for cerebral vasospasm following aneurysmal subarachnoid hemorrhage: predictors of outcome and retreatment. J Interv Surg. 2018;10(4):367–74. https://doi.org/10.1136/neurintsurg-2017-013363.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Pathak, A. (2022). Aneurysmal SAH Induced Vasospasm: Pathogenesis and Management. In: Lv, X. (eds) Endovascular Surgery of Cerebral Aneurysms. Springer, Singapore. https://doi.org/10.1007/978-981-16-7102-9_2
Download citation
DOI: https://doi.org/10.1007/978-981-16-7102-9_2
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-7101-2
Online ISBN: 978-981-16-7102-9
eBook Packages: MedicineMedicine (R0)