
Abstract
Coronary Heart Disease (CHD) is one of the major causes of morbidity and mortality in many developing countries, including Bangladesh. A stratified random sampling with proportional allocation technique was used to collect data from elderly people from urban, rural, and ethnic areas of the Sylhet region. A total of 230 (110 women and 120 men) people aged 60 years or above from the above mentioned areas were included in this study. A multiple logistic regression model was used to evaluate major risk factors associated with CHD for this sample group. The prevalence of CHD was higher for males than females, at 47.80% and 52.20% for females and males, respectively. Elderly people in urban areas were significantly (AOR = 4.03; 95% CI: 1.22–3.29) more likely to have CHD as compared to elderly persons living in rural areas. Elderly persons of ethnic origin were found to be less likely to suffer from CHD (AOR = 0.04, 95% CI: 0.01–0.17514.69) in comparison to urban elderly. The risk factors smoking (44.8%) and hypertension (51.3%) were also positively associated with CHD. Elderly persons who reported to exercise regularly were found to have 89% (AOR = 0.11, 95% CI: 0.03–0.50) less risk of suffering from CHD as compared to those who did not exercise regularly. The findings of this study further indicated that factors such as a high BMI (overweight/obese), high sugar intake, high soft drink consumption, diabetes, and mental stress have a significant influence on CHD.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Background
Coronary heart disease (CHD) is one of the most prevalent of chronic diseases of our modern era [1, 2]. Known as a ‘silent killer’ due to its lack of easily observable symptoms, CHD has become one of the leading causes of death globally [3]. Over 80% of all reported cases of CHD have been registered in low- or middle-income countries in 2005 [4]. Further, the prevalence of CHD is predicted to continue to increase in low- and middle-income countries due to lifestyle conversions associated with increasing urbanization, economic development, and globalization. Significant risk factors associated with CHD include age, family history, gender, hypertension, high cholesterol, diabetes, smoking, obesity, excessive alcohol intake, excessive stress, and physical inactivity [5]. Obesity, among the various risk factors associated with the onset of CHD [6], has nearly tripled since 1975. It is estimated that approximately 2 billion people worldwide are overweight or obese; of these, over 650 million are obese [7, 8]. Of the above factors significantly associated with CHD, obesity, intake of processed foods (associated with increased prevalence of high blood pressure), and physical in activity are known to increase in populations undergoing urbanization. It is well established that the risk of dying from CHD increases substantially with age [9]. As a chronic disease, CHD is the largest contributor to mortality in individuals >60 years [10], being responsible for 17% of all deaths [11]. The average percentage of CHD is 73.3% between age 60 and 79 [12].
Although Bangladesh has the highest rates of coronary artery disease among all Asian countries, it is an issue that remains severely understudied [13]. Bangladesh is a densely populated country with population of over 160 million [14]. In 1981, the percentage of the elderly population was 11.35%, and in 2011, 16.57%. While no official census has been carried out since 2011, population estimates by the United Nations (UN) predict this number to have further increased. In Bangladesh, approximately 99.6% of males and 97.9% of females are endangered to at least one of the risks of cardiovascular disease at a younger age [15]. By 2020, 85% of the global CH disease burden is expected to be borne by developing nations, and the increase in coronary artery disease (CAD) mortality in developing countries between 1990 and 2020 is projected to be 120% in women and 137% in men [16, 17]. In recent years, factors such as rapid urbanization, increased life expectancy, unhealthy dietary habits, and lifestyle changes have led to an increase in the rate of CHD in Bangladesh [18]. A recent report has highlighted CHD as a significant, urgent medical and public health concern in Bangladesh due to its alarmingly increased impact on national mortality rates. In the advent of the new millennium, factors such as poor dietary habits, excess saturated and trans-fat consumption, high salt intake, and low levels of physical activity have been identified as major contributors towards the increased onset of this chronic disease in Bangladesh [5]. Bangladesh has been experiencing a rough epidemiological transition due to the limited availability of resources and strategies for prevention of these chronic diseases in low-income areas [19]. Moreover, better healthcare accessibility for elderly people (aged over 60 years) is a significant issue of concern in the context of Bangladesh, as studies have revealed that lack of access to healthcare significantly increases the risk of death among elderly people [20] and speeds up the longevity of health to access health care service [21]. CHD has become a major burden of disease for people of this country. Day by day, the mortality rate of CHD increases; today, it bears responsibility for approximately 75% of all deaths reported in the past few years in Bangladesh [22]. showed that weighted pooled prevalence of overall CHD in the Bangladeshi population was higher in urban areas (8%) compared to rural areas (2%) but there is no study has been conducted based on ethnic people and sylhet region. In this study, we have estimated the effect of factors such as socioeconomic status, dietary habits, and traditionally CHD-associated risk factors (hypertension, diabetes, smoking etc.) on the prevalence rate of this disease in Bangladesh.
2 Methods
2.1 Study Design
A stratified random sampling with proportional allocation technique was used to collect survey locations, number of respondents and the data. In order to capture the socioeconomic and demographic conditions as well as the ethnicity distribution of the Sylhet region, the total study area was divided into three strata, namely an urban area, a rural area, and an ethnic minority area. From the above strata, a ward in an urban area, a union in a rural area, and an ethnic community were randomly selected and surveyed. Data from elderly people (age 60 years or above) at the household level was collected with the use of a structured questionnaire. Three randomly selected areas were considered from three strata. The recognized sample size determination formula for these strata was n = z 2[p(1 − p)/d 2] * D eff; where p is the indicator percentage, Z is the value of normal variate with a 95% confidence interval, and D eff is the design effect. Attained values were calculated on the basis of 50% indicator percentage (proportion of households having elderly person), 95% confidence interval, 0.10p relative precision, and highest response distribution with an assumed design effect of 2.00. Using this design, a total of 230 households were calculated as the substantial number sample for strata. A total 230 elderly people were successfully interviewed. The sylhet region was selected purposely so as to capture data from elderly persons from an ethnic community.
In stratified random sampling, the allocation of a given sample of size n to different strata is done in proportion to their sizes:
\( \hspace*{140pt}\displaystyle{n}_i=\frac{nN_i}{N}\vspace*{6pt} \)
Where N i is the total number of units in the ith stratum. The sampling fraction is equal to the sample size divided by the population size. Using this formula, a total of 90, 100, and 40 elderly persons belonging to urban, rural, and ethnic communities, respectively, were interviewed.
2.2 Response Variable
A prior CHD diagnosis was selected as the dependent variable in this study. An elderly person was considered to suffer from heart disease if they had been diagnosed with CHD prior to data collection. The CHD variable was coded as 1 if the elderly suffered from heart disease, and as 0 if otherwise.
2.3 Predictor Variables
Predictor variables considered for this study included socioeconomic factors such as income, occupation, wealth index, and education, as well as variables such as age, gender, residence (strata), and marital status. Risk factors such as hypertension, diabetes, respiratory, obesity (measured as body mass index, BMI), mental stress and smoking were also considered as predictor variables. Lastly, factors related to dietary and fitness habits, such as food consumption, level of exercise, sugar intake, red meat consumption, use of cooking oil, use of salt, soft drink consumption, and fast food consumption, were also considered as possible predictor variables on the basis of previous studies.
2.4 Statistical Analyses
A complex multiple logistic regression model was used to identify risk factors associated with CHD in the elderly population of the Sylhet region. Variables were selected in two stages so as to assure the final model was correctly specified. In the first stage of variable selection, a chi-square test was carried out to assess the statistical significance of all variables considered as possible predictor variables. Based on the chi-square test, only 18 variables were statistically significant with respect to the CHD variable at a 95% level of significance. Variables with a p-value >0.05 were excluded from the model. A stepwise (forward) logistic regression was next carried out, further narrowing down the variables to 11. Lastly, a multiple logistic regression was carried out with the selected predictor variables. The final adjusted model included the independent variables: sex, residence, education, occupation, BMI, exercise, sugar intake, cooking oil, smoking habit, mental stress, and hypertension. The hosmer and lemeshow goodness-of-fit test was used to assess the overall fit of the final model. Statistical analysis and data management for this study were carried out using R and SPSS (IBM SPSS 25).
3 Results
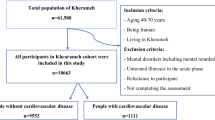
A total of 230 elderly generated as a sample. Among them, 43.50%, 39.10% and 17.00% elderly were included from rural, urban and ethnic, respectively (Fig. 16.1). Among 230 elderly, 52.20% were male and 47.80% were female (Fig. 16.2). From (Fig. 16.3), it was depicted that the percentage of CHD in the elderly were high in urban and it was gradual decreases in urban and ethnic.

Percentage of elderly by residence/strata

Percentage of elderly by sex

Percentage of elderly by residence and coronary heart disease
3.1 Socio-economic Status
From the Table 16.1 it can be said that 27.0% female elderly and 37.4% male elderly had CD. Among all of the elderly people 72.2% were illiterate and 27.8% were literate. Most of the elderly (43.5%) lived in rural areas. Among all, 42.6% were employed others were unemployed. About all of the elderly, 83.9% reported their yearly income was less than 50,000 TK. From the BMI status who had CHD, 35.7% of them were overweight, 5.2% were normal weight and 23.5% were underweight.
3.2 Food Consumption
Table 16.2 represents the association of food consumption of elderly and their CHD. More than one third, 34.8% elderly had reported to take sugar and had CHD. Most of the elderly (32.8%) who had CHD and used to eat red meat. Again, 43.9% elderly people had CHD and used to have soft drinks and above half of the elderly (50.4%) had CHD who used to eat fast food. From this food consumption table, it can be assured that sugar intake, meal intake (three or two times a day), cooking oil, taking extra salt in meal, fast food, drinking water have some correlation with CHD whether taking red meat and soft drinks do not have that correlation with heart disease.
3.3 Risk Factors
Table 16.3 indicates the risks of other diseases related with CHD. In this table, 47.0% people had CHD and also had diabetes, 17.4% people had CHD but they were free from diabetes. Elderly people who had smoking habit (44.8%) suffering from CHD where 16.1% elderly were not suffering from CHD who did not use to in habit of smoking. 48.7% elderly were suffering from mental stress with CHD. Elderly who were suffering from hypertension (51.3%) also had CHD. The results also indicate that diabetes, smoking, chest pain, mental stress and hypertension have clear relation with heart disease. Only respiratory did not show any relation with CHD.
3.4 Multiple Logistic Regression Model
Table 16.4 shows that there were significant differences in CHD and residence of elderly when the socio-economic factors, food consumption and other risk factors was adjusted. For instance, female elderly was 93% (AOR = 0.07; 95% CI: 0.02–0.26) less likely to have CHD as compared with male elderly. Elderly in ethnic were a 96% (AOR = 0.04; 95% CI: 0.01–0.175) lower chance to have CHD compared to rural elderly people. It is worthwhile to mention that people of the elderly of urban areas were 4.03 times more likely (AOR = 4.03, 95% CI: 1.22–13.29) to hold CHD compared to rural elderly people when other factors were adjusted. The odds ratio for the employed elderly had 98% (AOR = 0.02, 95% CI: 0.01–0.12) lower chance compare to who had not involvement in job. The odds of underweight elderly and normal-weight elderly affected by CHD were 33% (AOR = 0.77, 95% CI: 0.02–0.33) and 39% (AOR = 0.71, 95% CI: 0.02–0.31) less likely than those elderly who were overweight. Elderly people who were exercise regularly had 89% (AOR = 0.11, 95% CI: 0.03–0.50) less risk to develop CHD compared to those elderly who were not involve in regular exercise.
Elderly who reported take sugar were (AOR = 4.32, 95% CI: 1.35–13.81) more likely to have CHD compared to the people who were not take soft drinks. After adjusting for the risk factors, we found that smoke had 11.68 times (AOR = 11.68, 95% CI: 3.06–44.57) higher odds of CHD compared to people who had not smoked. On the other hand, the likelihood of mental stress and blood pressure had increased 5.50 times higher the risk [95% CI: 1.69–17.90] and 4.59 times higher the risk [95% CI: 1.36–15.55] of having CHD in comparison to the elderly had no mental stress and no hypertension.
3.5 Hosmer and Lemeshow Goodness of Fit Test
Hosmer and Lemeshow goodness of fit test has been given in Table 16.5.
So, the Hosmer-Lemeshow test does not gives us significant evidence of good fit on 36% of occasions.
4 Discussion
This study shows that rural communities have lower risk factors of heart diseases than urban westernized populations. Another study reveals that this difference may be attributable to a low fat (15–20 g per day) diet based on whole grain (400 g per day) combined with physically demanding occupations [23] which is similar to our results. A recent report published that the prevalence of stroke of elderly people (aged >30 years) in rural population has been found to be 0.94% in general, 1.45% in male and 0.45% in female [24]. In Bangladesh, year of 2014, non-communicable diseases (NCDs) represented 59% of the total deaths; CHD was the single-most important contributor, being responsible for 17% of total death [25]. Recent studies suggest that socio-economic statuses, as assessed by occupation, education and income level [26] is closely related with the quality of diet though differences in the amount of food or in nutrient intake among social classes are often small [27, 28]. Occupation is considered as an important marker of socio-economic status which gives the economic condition of people and income ranges. Income provides access to goods and services, including quality education and medical care, which may protect against disease [29]. This study concludes that unemployed people have higher chance of heart diseases compared with the employed people and normally people of urban areas are more sufferer than the rural people [30]. Sitting for prolonged periods would also cause the loss of opportunity for cumulative energy expenditure resulting from the thousands of intermittent muscular contractions throughout the 16-h period that people are awake. This may have chronic effects on the propensity to become overweight [31]. And this study also reveals that people who are inactive are being attacked by heart diseases more often than the people who’re physically active. Male are suffering from heart diseases than the female and BMI Index is another most important risk factor for heart disease. A study shows that Body mass index (BMI), waist to hip ratio, obesity, independent fat distribution and weight gain since age 21 are associated with an increased risk of coronary heart disease and is getting stronger day by day [32]. Along with the previous studies, this study also reveals that people who are overweight they are in higher risk of attacked by heart diseases than the people who have normal weight and underweight. There is an inverse relation between education and long-term risk of coronary heart disease, this study indicates that heart diseases rarely vary from literate to illiterate people. But practically literate people are more conscious about the nutrition value of food [33, 34]. In an absolutely theoretical basis, the higher educational level could be related with more stressed occupation, less available time for cooking and consequently with a bigger trend for consumption of ready-to eat food or fast-food habits [35]. Food consumption is most important risk factors for heart diseases. People who are used to fast foods, intake extra salt and sugar, soft drinks, polyunsaturated fat foods are in higher risk of heart diseases. Heart disease is significantly associated with a lower intake of saturated fat and higher intakes of polyunsaturated fat, alcohol, folate, vitamin C, and vitamin E [36]. Healthy nutrient food consumption, proper meals every day and quitting smoking can reduce the risk of heart disease. In Bangladesh people are used to tobacco consumption i.e. smoking which is a risk factor for heart disease. From this heart disease people are attacked with many diseases like diabetes, hypertension, chest pain, back pain etc. which make people more inactive. Diabetes has long been recognized as one of the most important major cardiovascular risk factors, and in particular from cardiovascular disease diabetic subjects have a risk of early death [37].
5 Conclusion
In this study, we found that there is a wide range of factors, which are significantly associated with CHD among elderly (age > 60 years). The finding demonstrates that the primary risk factors for cardiovascular disease are smoking, hypertension, sedentary lifestyle, and diabetes. Moreover, a significant proportion of the elderly men and women are not aware of the consequence of this disease, and a small proportion of them are taking healthy dietary. Exercise is vital to reduce risk of heart disease. Health professionals have a crucial role in influencing lifestyle decisions. However, most health care delivery in south Asia is through formally and informally trained and traditional health professionals, who should become part of prevention strategies for CHD to obtain the maximum effect. CHD can be included cost effectively in existing training programs for these health professionals.
Declaration
-
Conception, Design, Writing, Review and Edit: KFF
-
Review and Edit: AAK
-
Analysis: MNH
-
Writing: TI
References
Cassar, A., et al.: Chronic coronary artery disease: diagnosis and management. Mayo Clin. Proc. 84(12), 1130–1146 (2009)
Iyngkaran, P., et al.: Risk stratification for coronary artery disease in multi-ethnic populations: are there broader considerations for cost efficiency? World J. Methodol. 9(1), 1–19 (2019)
Benjamin, E.J., et al.: Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation 137(12), e67–e492 (2018)
WHO (World Health Organization).: Cardiovascular Diseases (CVDs). http://www.whoint/mediacentre/factsheets/fs317/en/index.html. Last accessed 2015/01
Saquib, N., et al.: Cardiovascular diseases and type 2 diabetes in Bangladesh: a systematic review and meta-analysis of studies between 1995 and 2010. BMC Public Health. 12(1), 434 (2012)
Lim, S.S., et al.: A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 380(9859), 2224–2260 (2012)
The, G.B.D.O.C, et al.: Global, regional and national prevalence of overweight and obesity in children and adults 1980-2013: a systematic analysis. Lancet. 384(9945), 766–781 (2014)
WHO (World Health Organization).: Obesity and Overweight (2014)
Castelli, W.P.: Epidemiology of coronary heart disease: the Framingham study. Am. J. Med. 76, 4–12 (1984)
WHO.: The Atlas of Heart Disease and Stroke. WHO, Geneva, (2004)
WHO.: Noncommunicable Diseases (NCD) Country Profiles. Bangladesh, http://apps.who.int/iris/bitstream/10665/128038/1/9789241507509_eng.pdf?ua=1 (2014). Last accessed 14 Dec 2014
Nag, T., Ghosh, A.: Cardiovascular disease risk factors in Asian Indian population: a systematic review. J. Cardiovasc. Dis. Res. 4(4), 222–228 (2013)
Islam, A.K.M.M., Majumder, A.A.S.: Coronary artery disease in Bangladesh: a review. Indian Heart J. 65(4), 424–435 (2013)
Bangladesh Bureau of Statistics (BBS).: http://www.bbs.gov.bd/Home.aspx (2016). Last accessed 16 Nov 2016
Sameh E. S., Zunaid, A.K., Tarcey, Michel. M. E.: Tackling Noncommunicable Diseases in Bangladesh: Now Is the Time. Directions in Development – Human Development. The World Bank 136 (2013)
Bulato, R.A., Stephens, P.W.: Global Estimates and Projections of Mortality by Cause. Population, Health and Nutrition Department, Washington, DC. World Bank 1007 (1992)
Reddy, K.S., Yusuf, S.: Emerging epidemic of cardiovascular disease in developing countries. Circulation. 97, 596–601 (1998)
Joshi, P., et al.: Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA. 297(3), 286–294 (2007)
Gaziano, T.A., et al.: Laboratory-based versus non-laboratory-based method for assessment of cardiovascular disease risk: the NHANES I follow-up study cohort. Lancet. 371(9616), 923–931 (2008)
Abdullah, J.M., Ahmad, M.M., Saqib, S.E.: Understanding accessibility to healthcare for elderly people in Bangladesh. Dev. Pract. 28(4), 552–561 (2018)
Gu, D., Zhang, Z., Zeng, Y.: Access to healthcare services makes a difference in healthy longevity among older Chinese adults. Soc. Sci. Med. 68(2), 210–219 (2009)
Chowdhury, M.Z.I., et al.: Prevalence of cardiovascular disease among Bangladeshi adult population: a systematic review and meta-analysis of the studies. Vasc. Health Risk Manag. 14, 165–181 (2018)
Singh, R.B., et al.: Prevalence of coronary artery disease and coronary risk factors in rural and urban populations of North India. Eur. Heart J. 18(11), 1728–1735 (1997)
Zaman, M.M.A.C., et al.: Prevalence of stroke in a rural population of Bangladesh. Glob. Heart. 10, 333–334 (2015)
World Health Organization.: Noncommunicable Diseases (NCD) Country Profiles, 2014,Bangladesh. Available from: http://apps.who.int/iris/bitstream/10665/128038/1/9789241507509_eng.pdf?ua=1 (2014)
Krieger, N., Williams, D.R., Moss, N.E.: Measuring social class in US Public Health Research: concepts, methodologies, and guidelines. Annu. Rev. Public Health. 18(1), 341–378 (1997)
Galobardes, B., Morabia, A., Bernstein, M.S.: Diet and socioeconomic position: does the use of different indicators matter? Int. J. Epidemiol. 30(2), 334–340 (2001)
Groth, M.V., Fagt, S., Brøndsted, L.: Social determinants of dietary habits in Denmark. Eur. J. Clin. Nutr. 55, 959–966 (2001)
Psaltopoulou, T., et al.: Socioeconomic status and risk factors for cardiovascular disease: impact of dietary mediators. Hell. J. Cardiol. 58(1), 32–42 (2017)
Fatema, K., et al.: Prevalence of risk factors for cardiovascular Diseases in Bangladesh: a systematic review and meta-analysis. PLoS One. 11(8), e0160180 (2016)
Hamilton, M.T., Hamilton, D.G., Zderic, T.W.: Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes. 56(11), 2655–2667 (2007)
Rimm, E.B., et al.: Body size and fat distribution as predictors of coronary heart disease among middle-aged and older US men. Am. J. Epidemiol. 141(12), 1117–1127 (1995)
Patterson, R.E., et al.: Is there a consumer backlash against the diet and health message? J. Am. Diet. Assoc. 101(1), 37–41 (2001)
Wardle, J., Parmenter, K., Waller, J.: Nutrition knowledge and food intake. Appetite. 34(3), 269–275 (2000)
Kirkpatrick, S.T.V.: The relationship between low income and household food expenditure patterns in Canada. Public Health Nutr. 6, 589–597 (2003)
van Dam, R.M., et al.: Patterns of food consumption and risk factors for cardiovascular disease in the general Dutch population. Am. J. Clin. Nutr. 77(5), 1156–1163 (2003)
The, D.S.G: Glucose tolerance and mortality: comparison of WHO and American Diabetes Association diagnostic criteria. Diabetes epidemiology: collaborative analysis of diagnostic criteria in Europe. Lancet. 617-621, 354 (1999)
Acknowledgement
We would like to thank SUST research center for funding this research.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Ferdushi, K.F., Kamil, A.A., Hasan, M.N., Islam, T. (2020). Factors Associated with Coronary Heart Disease among Elderly People in Different Communities. In: Rahman, A. (eds) Statistics for Data Science and Policy Analysis. Springer, Singapore. https://doi.org/10.1007/978-981-15-1735-8_16
Download citation
DOI: https://doi.org/10.1007/978-981-15-1735-8_16
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-1734-1
Online ISBN: 978-981-15-1735-8
eBook Packages: Mathematics and StatisticsMathematics and Statistics (R0)