
Abstract
Metastatic tumors are the most common type of malignancy in the liver, far exceeding primary tumors of the liver. The distinction between a primary tumor and a metastatic tumor in the liver has both therapeutic and prognostic significance. Knowledge of the primary tumor site and its morphology, if available, is important in evaluating and comparing it to its metastasis. Among tumor types, adenocarcinoma, neuroendocrine tumor, and lymphoma are the most common. Common primary sites include the colon (adenocarcinoma), pancreas (adenocarcinoma and pancreatic neuroendocrine tumor), stomach and small intestine (adenocarcinoma, neuroendocrine and gastrointestinal stromal tumor), lung (adenocarcinoma, small-cell and large-cell neuroendocrine carcinoma, and squamous cell carcinoma), breast, skin (melanoma), and kidney (renal cell carcinoma).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
18.1 Introduction
Metastatic tumors are the most common type of malignancy in the liver, far exceeding primary tumors of the liver. The distinction between a primary tumor and a metastatic tumor in the liver has both therapeutic and prognostic significance. Knowledge of the primary tumor site and its morphology, if available, is important in evaluating and comparing it to its metastasis. Among tumor types, adenocarcinoma, neuroendocrine tumor, and lymphoma are the most common. Common primary sites include the colon (adenocarcinoma), pancreas (adenocarcinoma and pancreatic neuroendocrine tumor), stomach and small intestine (adenocarcinoma, neuroendocrine and gastrointestinal stromal tumor), lung (adenocarcinoma, small-cell and large-cell neuroendocrine carcinoma, and squamous cell carcinoma), breast, skin (melanoma), and kidney (renal cell carcinoma).
18.2 Clinical and Pathological Features
Besides the evaluation of morphologic features of the tumor, immunohistochemical stains or additional studies—such as flow cytometry or molecular studies—are often necessary in the diagnosis and treatment of metastatic tumors. For example, colonic adenocarcinomas, the most common type of metastasis of the liver, often demonstrate fairly well-formed glands with tall columnar cells and “dirty” necrotic debris in the glandular lumen. Further immunohistochemical stains, such as cytokeratin profile (CK7 negative and CK20 positive) or marker for enteric differentiation (CDX-2), are used to confirm or exclude other sites of origin with similar morphology. Molecular studies are often performed for identification of specific mutations and predicting response to antigrowth factor therapies. For the diagnosis of lymphoma, flow cytometry can be performed in addition to immunohistochemical stains. Table 18.1 provides a list of immunohistochemical stains for various metastatic tumors.
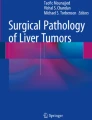
Image analysis of metastatic tumors to the liver almost always shows hypovascularity, except for liver metastasis from carcinoids/neuroendocrine tumors which are hypervascular [1]. Diffuse metastatic lesions may not be detected by ultrasonography, computed tomography, or magnetic resonance imaging [2]. Therefore, laparoscopy with liver biopsy or, more commonly, radiology-guided fine needle aspiration (FNA) may be required for diagnosis, molecular pathology tissue procurement, and clinical trial/research protocol eligibility determination. Peritoneoscopy is helpful to visualize multiple metastatic nodules on the liver surface (Fig. 18.1), and central depression is often seen in metastatic nodules due to central necrosis as the result of insufficient blood supply.

Metastatic liver tumor. Peritoneoscopy shows multiple metastatic nodules with central excavation
On occasion, biopsy may miss the target metastatic lesion, yielding benign liver parenchyma with histological changes due to compression and local obstruction of bile duct and blood flow. In this case, histological changes show a triad, consisting of focal sinusoidal dilatation and congestion, ductular reaction, and neutrophils in edematous portal tracts [3].
18.3 Differentiation from Benign Liver Lesion
Benign liver lesions are frequently encountered during workups for metastatic lesions and should be in the differential diagnoses of these lesions. Simple biliary cyst, cavernous hemangioma, and focal fatty change can be distinguished from solid metastatic lesions with relative ease in imaging studies. Liver abscess can be difficult to differentiate from an extensively necrotic metastatic tumor but is usually accompanied by other constitutional symptoms such as fever. Inflammatory pseudotumor often requires biopsy to confirm the absence of malignant cells and the presence of chronic inflammation and storiform fibrosis.
Benign hepatocellular tumors, including focal nodular hyperplasia and hepatocellular adenoma, are not uncommon incidental findings. Focal nodular hyperplasia usually shows characteristic imaging features as a result of a prominent central scar containing large dystrophic vessels. The absence of an obvious central scar or the presence of steatosis in these lesions may render an atypical appearance in imaging studies. Hepatocellular adenoma, usually encountered in young and middle-aged females with a history of oral contraceptive use or males with anabolic steroid use, requires complete resection because of its risk of bleeding and its slight risk of recurrence and malignant transformation.
Liver capsule or subcapsular nodules are often sampled during unrelated operations (gastric reduction surgery, pancreatoduodenectomy (whipple), etc.). Biliary hamartoma (von Meyenburg complex) is the most common non-malignant cause of such nodules. On frozen section biliary hamartoma can be mistaken for well-differentiated adenocarcinoma but is usually readily apparent as a benign process. This lesion typically presents as a subcapsular cluster of angulated glands with surrounding fibrous reaction +/− neutrophilic inflammatory reaction. The epithelial cells themselves are typically bland with a low cuboidal morphology and smooth round-to-ovoid nuclei without nucleoli.
18.4 Case
Case 18.1
A patient presented with enlargement of the right submandibular gland and multiple small space-occupying lesions in the liver by ultrasonography. Computed tomography (CT) with contrast medium showed multiple low-density areas (Fig. 18.2). Peritoneoscopy showed small tumor nodules on the liver surface (Fig. 18.3). Echo-guided liver biopsy showed clusters of small neoplastic cells with hyperchromic nuclei, which were also positive for carcinoembryonic antigen. In this case, adenocarcinoma of the submandibular gland was diagnosed from metastatic lesions of the liver (Fig. 18.4).

Metastatic liver tumor. CT with contrast medium shows multiple low-density nodules

Metastatic liver tumor. Peritoneoscopy shows nodular and granular liver surface

Metastatic liver. (a) Small neoplastic cells at the upper two thirds of the picture are arranged in solid sheets with anisonucleosis and high nuclear cytoplasmic ratio. The lower third of the picture shows compressed non-tumoral hepatocytes in trabecular arrangement with low nuclear cytoplasmic ratio. (b) Carcinoembryonic antigen immunoreactivity is seen in neoplastic cells
Case 18.2
A 55-year-old female complained of epigastric pain and diarrhea, and gastrointestinal fiberscope showed duodenal ulcers. Liver function tests revealed AST 136 IU/L, ALT 89 IU/L, LDH 336 IU/L, ALP 628 IU/L, GGT 189 IU/L, and AFP 570 ng/mL. The L3 fraction of AFP was 84.2% and serum gastrin was 6400 pg/mL. CT with contrast medium in the arterial phase showed multiple high-density areas in the liver and low density in the center. A low-density area in the pancreas was observed. High-density areas in the liver became low in the venous phase (Fig. 18.5). Biopsy of the liver tumor showed neoplastic cells with anisonucleosis in comparison to normal hepatocytes; the neoplastic cells did not form a trabecular structure, and trabecular formation was preserved in non-tumoral area (Fig. 18.6). The tumor cells were positive for synaptophysin, CD56, chromogranin A, and AFP (Fig. 18.7). Serum test showed high values of gastrin and AFP. Image analysis revealed multiple hypervascular tumors in the liver and a hypovascular tumor of the pancreas. Histologically, neuroendocrine tumor was diagnosed from biopsy of liver metastasis. The pancreas was the suspected primary site. The tumor cells presumably produce gastrin and AFP. The elevation of serum AFP and human chorionic gonadotrophin-beta pertains to worse prognosis in patients with a neuroendocrine tumor [4].

Liver metastasis of neuroendocrine tumor. (a) CT with contrast medium shows multiple high-density areas with low density in the center at arterial phase. (b) CT shows low-density tumors at venous phase

Histological features of tumor area and non-tumor area. (a) Pleomorphic neoplastic cells in solid sheets. (b) Hepatocytes preserve the trabecular architecture in non-tumoral area. (c) Reticulin stain shows no trabecular arrangement of neoplastic cells. (d) Hepatocytes show trabecular arrangement


Expression of synaptophysin, CD56, chromogranin A, and AFP immunoreactivity of the neoplastic cells. (a) Synaptophysin-immunoreactivity of the neoplastic cells. (b) CD56-immunoreactivity on the membrane of neoplastic cells. (c) Chromogranin A-immunoreactivity of some neoplastic cells (arrow). (d) Alpha-fetoprotein-immunoreactivity of some neoplastic cells (arrow)
Case 18.3
A 68-year-old female had a mastectomy for breast cancer, and a localized recurrence was found in the residual mammary gland 1 year later. General malaise and anorexia developed, and liver function tests showed TBIL 4.97 mg/dL, AST 219 IU/L, ALT 240 IU/L, ALP 1826 IU/L, and LDH 810 IU/L. CT by contrast medium showed heterogeneous enhancement in the liver at the arterial phase, but it decreased at the venous phase (Fig. 18.8). Peritoneoscopy showed enlarged liver with wavy surface and diffused white maculae (Fig. 18.9). Liver biopsy showed microthrombus of neoplastic cells in the portal veins and invasion beyond the portal tract, and the portal tract was edematous (Fig. 18.10). She was treated with systemic chemotherapy but died of acute liver failure due to diffuse invasion and proliferation of neoplastic cells. Breast cancer often metastasizes to the liver and produces multiple hypovascular tumors. In this patient, tumor cells invaded and proliferated diffusely in the peripheral portal veins. Hence, mass lesions were not detected in the liver, and heterogeneous density was seen on CT. The development of diffuse metastasis and portal thrombus caused acute liver failure [5].

CT of metastatic liver. (a) Heterogeneous density at arterial phase with contrast medium. (b) Heterogeneous density is decreased at venous phase

Peritoneoscopic findings of metastatic liver. Large excavation and many white maculae are seen on liver surface

Histological findings of metastatic liver. (a) Neoplastic cells proliferate in the portal tract with thrombi in the vessel (arrow) and invasion of the periportal area. (b) Portal tract is edematous with neoplastic thrombus (arrow) in the portal vein
Abbreviations
- AFP:
-
Alpha-fetoprotein
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- CK:
-
Cytokeratin
- CT:
-
Computed tomography
- GGT:
-
Gamma-glutamyl transferase
- LDH:
-
Lactate dehydrogenase
- TBIL:
-
Total bilirubin
References
De Santis M, Santini D, Alborino S, Carubbi F, Romagnoli R. Liver metastasis from carcinoid: diagnostic imaging. Radiol Med. 1996;92:594–9.
Borja ER, Hori JM, Pugh RP. Metastatic carcinomatosis of the liver mimicking cirrhosis: case report and review of the literature. Cancer. 1975;35:445–9.
Gerber MA, Thung SN, Bodenheimer HC Jr, Kapelman B, Schaffner F. Characteristic histologic triad in liver adjacent to metastatic neoplasm. Liver. 1986;6:85–8.
Shah T, Srirajaskanthan R, Bhogal M, Toubanakis C, Meyer T, Noonan A, et al. Alpha-fetoprotein and human chorionic gonadotrophin-beta as prognostic markers in neuroendocrine tumour patients. Br J Cancer. 2008;99:72–7.
Athanasakis E, Mouloudi E, Prinianakis G, Kostaki M, Tzardi M, Georgopoulos D. Metastatic liver disease and fulminant failure: presentation of a case and review of the literature. Eur J Gastroenterol Hepatol. 2003;15:1235–40.
Acknowledgement
Prof. Alex Y. Chang was a coauthor of the first edition of this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Vaickus, L.J., Suriawinata, A.A., Iwai, M. (2019). Metastatic Liver Tumors. In: Hashimoto, E., Kwo, P., Suriawinata, A., Tsui, W., Iwai, M. (eds) Diagnosis of Liver Disease. Springer, Singapore. https://doi.org/10.1007/978-981-13-6806-6_18
Download citation
DOI: https://doi.org/10.1007/978-981-13-6806-6_18
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-6805-9
Online ISBN: 978-981-13-6806-6
eBook Packages: MedicineMedicine (R0)