
Abstract
Metastasis to the liver is common from tumors arising in various organs. Distinguishing metastatic tumors from primary hepatic tumors is important for prognosis and therapy. This chapter enumerates and discusses malignant neoplasms that commonly metastasize to the liver and examines their differential diagnoses, focusing on the histologic and immunohistochemical features that help distinguish metastases from primary hepatic tumors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Metastasis
- Adenocarcinoma
- Cholangiocarcinoma
- Hepatocellular carcinomas
- Cholangiocarcinoma
- Metastatic hepatoid carcinoma
- Sarcoma
- Lymphoma
15.1 Introduction
The liver is the one of the most common organs involved by metastases, due to a variety of factors including its location, dual blood supply, and anatomy. Autopsy studies have shown that up to 40 % of patients with extrahepatic malignant tumors have liver metastases [1]. In fact, metastatic tumors are the most common malignant neoplasms of the liver in North America, Europe, and Japan. Most tumors metastasize to the liver via the hematogenous route but occasionally they may also spread to the liver via the lymphatics or peritoneal fluid.
15.2 Definition
Malignant neoplasm that originates from an extrahepatic organ and involves the liver via hematogenous or lymphatic dissemination.
15.3 Primary Sites of Origin
The two most frequent tumors that metastasize to the liver are carcinomas and melanoma. Lymphomas and sarcomas metastasize to the liver less commonly. Within the carcinoma group, breast, lung, colon, gastric, and pancreatic carcinomas frequently metastasize to the liver [1].
15.4 Clinical Features
Patients with liver metastases may present with abdominal pain, jaundice, ascites, or weight loss. However, many patients are asymptomatic. Sometimes patients with functioning neuroendocrine tumors that are metastatic to the liver can present with carcinoid syndrome. The carcinoid syndrome has varying degrees of skin flushing that can last from a few minutes to hours, flushing that is triggered by various activities, ranging from exercising to stress, though many cases will have no obvious trigger. Other components of the carcinoid syndrome include diarrhea, rapid heartbeat, and asthma-like difficulty breathing.
Transaminases and alkaline phosphatase levels are often nonspecifically elevated in patients with hepatic metastases.
15.5 Gross Findings
Metastatic tumors are typically seen in non-cirrhotic livers; tumors in cirrhotic livers are less likely to be metastases. Metastases most often form multiple nodules of varying sizes, scattered throughout the hepatic parenchyma, often involving both lobes. Metastasis less commonly presents as a solitary hepatic lesion. Sometimes gross examination may provide a clue about the tumor type. For instance, melanomas may be black or brown in color, mucinous adenocarcinomas may appear as gelatinous glistening masses, and squamous cell carcinomas may be white and granular, while colorectal carcinoma may have an umbilicated appearance.
15.6 Approach to Working Up a Liver Tumor
When working up a liver tumor, knowing the clinical history can be helpful in making an accurate diagnosis. The presence of advanced fibrosis or cirrhosis increases the chance that a tumor is a primary hepatic carcinoma; however, metastatic tumors can rarely be seen in cirrhotic livers (Figs. 15.1, 15.2, and 15.3). In addition, the presence of a single extrahepatic tumor with multiple hepatic lesions would favor metastasis, while the presence of a single hepatic tumor without identifiable lesions elsewhere in the body would favor a primary hepatic tumor. Furthermore, if the patient has a known past history of any malignancy, such as breast carcinoma or melanoma, or even a recent clinical history that suggests extrahepatic malignancy, such as diffuse thickening of the gastric wall on imaging or a colon mass on endoscopy, then combining this information with the tumor histology can be very useful in ordering the appropriate immunohistochemical stains to make an accurate diagnosis. Knowing the clinical information about elevated serum tumor markers may also be useful while approaching a liver tumor (Table 15.1).

Cirrhotic liver with metastatic breast carcinoma. Tumor cells are seen within the fibrous septa and in the cirrhotic nodule

Cirrhotic liver with metastatic breast carcinoma. High-power view showing the metastatic tumor cells

Cirrhotic liver with metastatic breast carcinoma. Mammaglobin immunostain is positive within the tumor
While immunohistochemical stains are essential in working up a liver tumor, the morphological features seen on the H&E stain should not be neglected. Using them both together is the quickest and most accurate way to get the correct diagnosis. Morphology needs be taken into account when interpreting immunostain results because making a diagnosis based only on the results of the immunostains can lead to an erroneous diagnosis. Sometimes, repeating a special stain or an immunohistochemical stain can be helpful if the results do not correlate well with the morphology.
If a tumor is both poorly differentiated and no useful clinical information is available, then the first round of immunostains should be directed at correctly identifying the broad lineage of the neoplasm, i.e., whether it is a carcinoma, sarcoma, melanoma, or lymphoma. This can be done by ordering a broad panel of immunohistochemical stains that includes markers for carcinoma (such as cytokeratin AE1/AE3, Cam5.2, and CK903), sarcoma (desmin, CD34, and CD117), melanoma (S100, Melan-A, and HMB-45), and lymphoma (CD3, CD20, and CD45). Once the broad lineage of the tumor has been identified, more specific immunostains can be ordered for further tumor subclassification and eventual accurate diagnosis.
On the other hand, if the tumor is well-differentiated and its overall lineage is evident based on the H&E findings (e.g., gland forming and mucin producing adenocarcinoma), then the immunohistochemical workup should be directed at extending the H&E findings rather than establishing the broad tumor lineage. For example, a gland forming tumor could be evaluated with CK7/CK20 and specific markers for lung, GI, breast, or prostate origin. A carcinoma with a solid or trabecular growth pattern could be worked with markers for hepatic, adrenal, renal, and neuroendocrine differentiation.
Finally, remember that immunostains that work well in a given author’s experience may be different than the ones that work best for you, depending on the availability of the stains in your laboratory, their quality, and your overall familiarity with the stains. Every laboratory has its own somewhat unique experience with a given stain, based partly on antibodies, antigen retrieval, and other local technical practices. Therefore, the published literature should be interpreted in conjunction with direct experience.
15.7 Mimickers of Hepatocellular Carcinomas
Certain tumors can histologically mimic hepatocellular carcinoma, including epithelioid angiomyolipomas, renal cell carcinomas, adrenal cortical carcinomas, neuroendocrine tumors, and melanoma. These tumors can show a trabecular or acinar or solid growth pattern that can closely resemble hepatocellular carcinoma. In addition, the tumor cells in these cases can show cytological features that further suggest hepatocellular differentiation, including eosinophilic and granular or clear cytoplasm.
Most angiomyolipomas are distinguished from hepatocellular carcinoma by their triphasic nature, but epithelioid angiomyolipomas, especially in biopsy specimens, can be difficult to distinguish from a well-differentiated hepatocellular neoplasm. Immunohistochemical stains are helpful here, as angiomyolipomas are positive for smooth muscle actin, HMB-45 and Melan-A, but negative for cytokeratin, HepPar1, and arginase-1 (Figs. 15.4, 15.5, and 15.6).

Epithelioid angiomyolipoma. Epithelioid tumor cells with clear cytoplasm are seen

Epithelioid angiomyolipoma. Smooth muscle actin immunostain is positive within the tumor cells

Epithelioid angiomyolipoma. HMB-45 immunostain is positive within the tumor cells
Both clear cell and chromophobe renal cell carcinoma can be mistaken for hepatocellular neoplasms. A history of renal malignancy or the presence of a renal mass can help reach the correct diagnosis. Furthermore, some clear cell hepatocellular carcinomas have areas of more typical non-clear morphology, which can help distinguish it from metastatic clear cell renal cell carcinoma. Immunohistochemical stains are very helpful in the differential diagnosis; clear cell renal cell carcinomas are usually positive for vimentin while most hepatocellular carcinomas are either negative or show patchy staining (90 %), with the exception of poorly differentiated or spindle cell hepatocellular carcinomas which can show more diffuse reactivity for vimentin [2]. RCC antigen is negative in hepatocellular carcinoma, but RCC antigen has a lower sensitivity and specificity for metastatic renal cell carcinoma and should be interpreted cautiously [3]. On the other hand, the PAX8 immunostain is positive in the majority of metastatic clear cell renal cell carcinomas [4, 5]. However, a recent publication has shown that up to 20 % of clear cell hepatocellular carcinomas can also be positive for PAX8 [6], so other markers for hepatic differentiation also need to be examined. Clear cell renal cell carcinomas are negative for HepPar1, polyclonal CEA (canalicular pattern), and arginase-1 [7–9]. Chromophobe renal cell carcinoma, a close mimicker of hepatocellular neoplasms, is positive for PAX8 and CD117 and negative HepPar1 and arginase-1 (Figs. 15.7, 15.8, 15.9, and 15.10); this immunoprofile helps distinguish it from hepatocellular neoplasms. Of note, glypican-3 is not helpful in this differential diagnosis, as a subset of chromophobe renal cell carcinomas is positive.

Metastatic chromophobe renal cell carcinoma. The tumor cells have eosinophilic cytoplasm and prominent nucleoli

Metastatic chromophobe renal cell carcinoma. A PAX8 immunostain shows nuclear positivity

Metastatic chromophobe renal cell carcinoma. A CD117 immunostain showing membranous staining

Metastatic chromophobe renal cell carcinoma. An arginase immunostain is negative
Adrenal cortical carcinomas can involve the liver by metastasis or direct extension and can be difficult to differentiate morphologically from hepatocellular carcinoma (Fig. 15.11). Their immunoprofile, however, is distinct from hepatocellular carcinoma; adrenal cortical carcinomas are often positive for inhibin and Melan-A and are typically negative for HepPar1 (about 5–10 % of cases can be positive), polyclonal CEA (canalicular pattern), and arginase-1 [8–11].

Metastatic adrenal carcinoma. The growth pattern and cytology raises the possibility of a hepatocellular carcinoma on the H&E. Benign hepatocytes are seen in the lower portion of the image
Neuroendocrine tumors can resemble hepatocellular carcinoma. Some cases may have prominent clear cell morphology, while others will have ordinary cytology but mimic hepatocellular carcinoma with trabecular or acinar growth patterns. Neuroendocrine tumors, however, are strongly and diffusely positive for chromogranin and/or synaptophysin while they are negative for HepPar1 and arginase-1 (Figs. 15.12, 15.13, 15.14, and 15.15) [8, 9]. Hepatocellular carcinomas can show also focal neuroendocrine differentiation [12], especially when cholestatic, but will also be positive for markers of hepatic differentiation. Interestingly, neuroendocrine tumors metastatic to the liver that produce insulin can have a very distinctive feature, characterized by a marked steatosis involving only a rim of hepatocytes surrounding the neuroendocrine tumor (Figs. 15.16 and 15.17) [13].

Metastatic neuroendocrine tumor. This neuroendocrine carcinoma has a macrotrabecular growth pattern that mimics hepatocellular carcinoma

Metastatic neuroendocrine. Eosinophilic tumor cells show acinar and trabecular growth patterns

Metastatic neuroendocrine tumor. A chromogranin immunostain is positive (same case as Fig. 15.13)

Metastatic neuroendocrine tumor. A synaptophysin immunostain is positive (same case as Fig. 15.13)

Metastatic neuroendocrine tumor. An insulinoma metastatic to the liver shows a rim of marked fatty change in the liver parenchyma surrounding the lesion. Notice that the liver parenchyma away from the lesion shows no significant steatosis

Metastatic neuroendocrine tumor. An insulinoma metastatic to the liver shows a rim of marked fatty change in the liver parenchyma surrounding the lesion. Notice that the liver parenchyma away from the lesion shows no significant steatosis (higher power of the same case in Fig. 15.16)
Finally, melanomas can mimic hepatocellular carcinoma. A history of melanoma can often guide the pathologist to the correct diagnosis. Immunohistochemistry is invaluable in this setting, as melanoma is positive for S100, Melan-A, and HMB-45 and negative for HepPar1, polyclonal CEA, and arginase-1 (Figs. 15.18, 15.19, 15.20, and 15.21). Glypican-3, however, is usually not helpful in this setting as glypican-3 is frequently positive in melanoma [14].

Metastatic melanoma. Tumor cells showing eosinophilic cytoplasm, eccentrically located nuclei and prominent nucleoli

Metastatic melanoma. A Melan-A immunostain is positive

Metastatic melanoma. An HMB-45 immunostain is positive

Metastatic melanoma. A CD117 immunostain is positive
There are several excellent potential panels of immunohistochemical stains, which can be useful in differentiating hepatocellular carcinoma from its metastatic morphological mimickers. If a well to moderately differentiated hepatocellular carcinoma is in the differential, than one useful approach would be to perform an immunostain for hepatic differentiation, such as HepPar-1 or arginase-1. If they are negative, then additional follow-up stains can be used to further classify the tumor. Depending on the morphology and the clinical findings, these additional stains might include PAX-8, inhibin, vimentin, S100, HMB-45, Melan-A, SMA, CD-117, polyclonal CEA, and CAM5.2 (Table 15.2). As discussed previously, an effective approach for poorly differentiated tumors is a first round of stains to determine lineage (carcinoma, sarcoma, melanoma, lymphoma), followed by additional stains to help identify the most likely site of origin.
15.8 Distinguishing Cholangiocarcinoma and Metastatic Adenocarcinoma
Cholangiocarcinomas can assume many of the histological patterns of metastatic adenocarcinomas. However, if the bile ducts near the adenocarcinoma show high-grade biliary intraepithelial neoplasia (BilIN-3), this provides strong morphological evidence that the tumor is a primary cholangiocarcinoma rather than a metastasis. Other precursor lesions include mucinous cystic neoplasms and intraductal papillary neoplasms. However, precursor lesions are not identified in most cases. Furthermore, it is important to remember that some metastatic adenocarcinomas, such as colorectal adenocarcinomas, can have a prominent intrabiliary ductal growth pattern (“cancerization of the bile ducts”), which can closely mimic high-grade biliary intraductal neoplasia (BilIN-3).
A panel of immunostains is often required to distinguish cholangiocarcinoma from metastatic adenocarcinoma. Morphologically, adenocarcinomas arising from the upper gastrointestinal tract, pancreas, and biliary tract appear very similar to intrahepatic cholangiocarcinoma. Adenocarcinomas originating from all of these sites can be composed of small tubular or tubulopapillary structures embedded in a fibrous stroma. Therefore, distinction between intrahepatic carcinoma and metastases from upper gastrointestinal or pancreatobiliary sources is difficult, if not impossible, based on morphologic grounds alone. Furthermore, there are currently no immunohistochemical stains available in routine practice that can accurately distinguish between an intrahepatic cholangiocarcinoma and metastatic adenocarcinoma from upper gastrointestinal or pancreatic origin. In current practice, such distinctions rely first on ruling out other possible metastatic tumors and, when the morphology and immunostains are consistent with a biliary, pancreas, or upper gastrointestinal primary. When this is done, a final determination then relies on correlation with the imaging and endoscopic findings to identify the most likely site of origin. The lack of positive, affirmative immunostains or molecular assays that identifies biliary differentiation is a major weakness in our diagnostic armamentarium, one that will be hopefully rectified in the future.
15.8.1 Colorectal Adenocarcinoma
Metastatic colorectal adenocarcinoma probably has one of more easily recognizable histologic patterns, which is characterized by neoplastic glands lined by tall columnar cells that also have abundant dirty necrosis inside the glandular lumens. Besides their unique morphology, colorectal adenocarcinomas have an immunoprofile distinct from that of cholangiocarcinoma; cholangiocarcinomas are typically positive for CK7 and CK19 and show variable expression of CK20, whereas most colorectal adenocarcinomas are positive for CK20 and negative for CK7 and CK19 (Figs. 15.22, 15.23, and 15.24) [2]. Nuclear positivity for CDX2 is also typically seen in colorectal adenocarcinomas, where it is usually strong and diffuse. Cholangiocarcinomas can also show nuclear staining for CDX2, especially hilar tumors, though it is often patchy [15, 16]. Nevertheless, there are important caveats. In particular, colorectal adenocarcinomas with microsatellite instability due to defective DNA mismatch repair (MSI-high tumors) often show reduced expression of CK20 and CDX2 as well as increased expression of CK7 [17–19]. Identifying DNA mismatch repair in these tumors can be accomplished by an immunohistochemical battery comprising MLH1, MSH2, PMS2, and MSH6. Immunohistochemical evidence of DNA mismatch repair would generally favor a colorectal primary, but it is not definitive evidence, as microsatellite instability can rarely occur in cholangiocarcinoma, with loss of nuclear staining for mismatch repair proteins [20–22].

Metastatic colon adenocarcinoma. The neoplastic glands show characteristic dirty necrosis within the glandular lumens

Metastatic colon adenocarcinoma. A CK20 immunostain is positive

Metastatic colon adenocarcinoma. A CDX2 immunostain shows nuclear positivity
There have been several studies that have examined histological and molecular findings in resection specimens from colorectal metastases for indicators of prognosis. KRAS mutations are found in about 30 % of resected colorectal metastases and they are a predictor of worse prognosis [23]. BRAF mutations in colorectal metastases are less common, found in about 2 % of cases, and the prognosis is less clear [23]. The adenocarcinoma interface with the non-neoplastic liver can vary, showing a broad pushing border, a pseudocapsule, or an infiltrative border. One study reported an infiltrative border has a worse prognosis [24].
The background liver is also available for analysis in many resection specimens for colorectal metastases and should be evaluated for chronic liver disease including fatty liver disease, fibrosis, and other vascular injury to the sinusoids, called sinusoidal obstructive syndrome. There is some correlation with the type of changes seen in the background liver and chemotherapy regiments. Oxaliplatin use is associated with marked sinusoidal dilatation of the background liver and, in some cases, with nodular regenerative hyperplasia [25–27]. The sinusoidal dilatation and congestion can have a zone 3 distribution and in some cases shows “bridging congestion” (Fig. 15.25). The zone 3 hepatocytes will often be atrophic. There may be very mild nonspecific inflammation with occasional acidophil bodies. In longer standing cases, the Kupffer cells can have mild iron accumulation. Also depending on the timeframe since the chemotherapy, the central veins can show partial or complete obliteration by loose and finely reticulated collagen. In severe cases, central vein scarring can be seen in time. Irinotecan is also associated with moderate or marked fatty liver disease, and with steatohepatitis [26, 27].

Oxaliplatin associated liver injury. There is moderate “bridging” sinusoidal congestion throughout the background liver
15.8.2 Lung Adenocarcinoma
Metastatic lung adenocarcinoma is typically positive for TTF-1 and/or Napsin-A, while cholangiocarcinomas are negative for these markers. However, this finding is not true for extrahepatic cholangiocarcinomas, including the gallbladder, where close to a third of extrahepatic cholangiocarcinomas are positive for TTF-1 and about 10 % are also Napsin-A positive [28].
15.8.3 Breast Adenocarcinoma
Metastatic breast carcinomas are often positive for estrogen receptor, gross cystic fluid protein-15 (GCDFP-15) and mammaglobin (Figs. 15.26, 15.27, 15.28, and 15.29). Estrogen receptor positivity is generally seen in about 70 % of breast ductal carcinomas and almost all lobular carcinomas, but can also be seen in about two-thirds of hilar cholangiocarcinomas [29]. Progesterone receptor expression is not useful in identifying breast primaries, due to poor sensitivity and specificity [28]. Mammaglobin and GCDFP-15 are better markers of breast carcinoma and are expressed in about 50 % and 25 % of breast cancers, respectively. Cholangiocarcinomas are usually negative for mammaglobin and GCDFP-15 [29, 30].

Metastatic breast carcinoma. The tumor cells show some glandular architecture

Metastatic breast carcinoma. A CK7 immunostain is strongly and diffusely positive

Metastatic breast carcinoma. An estrogen receptor immunostain shows nuclear positivity

Metastatic breast carcinoma. A GCDFP-15 immunostain is positive
15.8.4 Prostate Adenocarcinoma
Prostate adenocarcinomas usually express prostate-specific antigen (PSA) and/or prostate-specific acid phosphatase (PSAP), whereas cholangiocarcinomas are negative for both markers. Of note, prostate adenocarcinomas treated with androgen deprivation therapy can show neuroendocrine differentiation [31]. Hence, when prostate adenocarcinoma metastasizes to the liver following androgen deprivation therapy, they are more frequently positive for neuroendocrine markers such as chromogranin and synaptophysin. This is often accompanied by decreased reactivity for prostatic markers such as PSA and PSAP.
15.9 Other Carcinomas Metastasizing to the Liver
Small cell carcinoma from the lung or from extrapulmonary sites can metastasize to the liver and are characterized by the typical morphological features of tumor cells growing in sheets, ribbons, and clusters, with small to medium sized tumor cells showing minimal cytoplasm, hyperchromatic nuclei with indistinct nucleoli, nuclear molding and smudging, and brisk mitotic activity (Fig. 15.30). Small cell carcinoma typically shows positive staining for TTF-1, chromogranin, and synaptophysin. It is important to remember that small cell carcinomas originating in sites other than the lung (extrapulmonary small cell carcinomas) are also frequently TTF-1 positive [32, 33], so TTF-1 positivity in this setting does not suggest a lung primary. Also of note, small cell carcinoma can rarely originate in the liver, either in isolation, or in combination with hepatocellular carcinoma or cholangiocarcinoma.

Small cell carcinoma. This metastasis from the lung shows the typical cytological findings
Urothelial carcinoma and squamous cell carcinoma from various sources can also metastasize to the liver, but are usually relatively easy to differentiate from primary hepatocellular neoplasms. Metastatic squamous and urothelial carcinomas, however, can be difficult to recognize when poorly differentiated. In this setting, immunohistochemistry can be helpful; both urothelial and squamous carcinomas are positive for CK5/6, p63, and/or p40, and are negative for hepatocellular markers (Figs. 15.31, 15.32, 15.33, 15.34, and 15.35). If no primary source is found for a squamous cell carcinoma in the liver, the possibility of a primary cholangiocarcinoma with squamous differentiation (pure squamous cell carcinoma or adenosquamous carcinoma) should be considered.

Metastatic urothelial carcinoma. The tumor cells show a nested appearance

Metastatic urothelial carcinoma. A p63 immunostain showing nuclear positivity

Metastatic urothelial carcinoma. A CK5/6 immunostain is positive

Metastatic squamous cell carcinoma. Basaloid squamous cell carcinoma showing a keratin pearl (arrow)

Metastatic squamous cell. A p63 immunostain shows nuclear positivity
Rarely, germ cell tumors metastasize to the liver (Fig. 15.36), but clinical history usually helps lead to the correct diagnosis. Most germ cell tumors express placental alkaline phosphatase (PLAP). Other helpful markers include human chorionic gonadotropin (HCG), which stains choriocarcinoma, and CD30, which stains embryonal carcinoma. Glypican-3 is not helpful in distinguishing germ cell tumors from hepatocellular carcinoma, as germ cell tumors are frequently positive. Likewise, alpha-fetoprotein is positive in yolk sac tumor and is therefore not helpful in the differential diagnosis with hepatocellular carcinoma. Germ cell tumors also often express epithelial markers including keratin stains and epithelial membrane antigen (EMA). Thyroid carcinomas are positive for TTF-1 and thyroglobulin and are negative for hepatocellular markers. Medullary carcinoma also expresses calcitonin.

Metastatic choriocarcinoma. This case was originally diagnosed as poorly differentiated hepatocellular carcinoma because of “canalicular” CD10 staining, but was negative for all hepatic markers and strongly positive for human chorionic gonadotropin
15.10 Metastatic Hepatoid Carcinomas
Hepatoid carcinomas can arise from a number of extrahepatic organs, such as lung, esophagus, stomach, gall bladder, and pancreas, and they can metastasize to the liver. These carcinomas can look like hepatocellular carcinoma on H&E and stain like hepatocellular carcinoma. They can be positive for HepPar1, arginase-1, glypican-3, and albumin-in-situ hybridization and can also have a canalicular staining pattern on pCEA or CD10 (Figs. 15.37, 15.38, 15.39, 15.40, 15.41, and 15.42).

Hepatoid carcinoma. This tumor originated in the pancreas and morphologically appears similar to hepatocellular carcinoma

Hepatoid carcinoma. Patchy positive staining for HepPar1 is seen (same tumor as in Fig. 15.37)

Hepatoid carcinoma. Patchy positive staining for arginase-1 is seen (same tumor as in Fig. 15.37)

Hepatoid carcinoma. Glypican-3 is positive (same tumor as in Fig. 15.37)

Hepatoid carcinoma. Albumin-in-situ hybridization is also positive (same tumor as in Fig. 15.37). A red chromogen was used on this stain

Hepatoid carcinoma. Showing a canalicular staining pattern for pCEA (same tumor as in Fig. 15.37)
Furthermore, about 5 % of hepatocellular carcinomas can also be focally positive for CDX2, so this stain would also not fully assist in distinguishing a metastatic gastrointestinal hepatoid carcinoma from a hepatocellular carcinoma. Nonetheless, there are some findings that can be very helpful. First, the presence of advanced fibrosis strongly favors a primary liver tumor. Second, a tumor elsewhere in the body, either by endoscopic findings or imaging findings, needs to be sampled to help rule out a metastatic hepatoid carcinoma. Third, some metastatic hepatoid carcinomas may have a mixed morphology that includes areas that do not look or stain like hepatocellular carcinoma, and this can be a very helpful clue.
15.11 Diagnostic Pitfalls
Some of these pitfalls are discussed above, or in other chapters, but are included here for convenience. These pitfalls are some of the recurrent themes seen in general surgical pathology and amongst consult practices.
-
1.
The morphology of a tumor has to be fully considered when making a final diagnosis. A fair number of cases are misclassified because of the result of one immunostain result, and a particular diagnosis was made on that basis alone, despite having a morphology that is inconsistent or very unusual for that diagnosis.
-
2.
When interpreting a stain for hepatic differentiation, make sure that any positive staining, especially when patchy, is not entrapped hepatocytes.
-
3.
No stain for hepatic differentiation is perfect. All have their diagnostic pitfalls (see Chap. 7). Nonetheless, of these, glypican-3 is the most promiscuous and glypican-3 staining in the absence of other positive stains for hepatic differentiation should be interpreted carefully.
-
4.
CD10 and or pCEA canalicular staining is a weaker form of evidence for hepatic differentiation. If HepPar1 and arginase-1 stains are negative in a poorly differentiated tumor, then any “canalicular staining” by pCEA or CD10 is probably not an important diagnostic clue, but instead a diagnostic pitfall.
-
5.
Pancreatic acinar cell carcinomas are synaptophysin positive and are often misclassified as neuroendocrine carcinomas (Figs. 15.43 and 15.44). A trypsin stain will be positive in pancreatic acinar cell carcinomas (Fig. 15.45).
Fig. 15.43 
Metastatic acinar cell carcinoma. This case mimicked a neuroendocrine carcinoma and had gland like structures that also raised the possibility of an adenocarcinoma
Fig. 15.44 
Metastatic acinar cell carcinoma. This poorly differentiated tumor was synaptophysin positive and submitted for consultation as possible neuroendocrine carcinoma. Strong diffuse trypsin staining helped clarify the diagnosis
Fig. 15.45 
Metastatic acinar cell carcinoma. Strong diffuse trypsin staining is seen (same case shown in Fig. 15.44)
-
6.
Well-differentiated neuroendocrine carcinomas are often misclassified as hepatocellular carcinomas.
-
7.
Poorly differentiated neuroendocrine carcinomas can have very limited morphological clues to their neuroendocrine origin, and immunostains are often the only way to pick them up.
-
8.
Metastatic renal cell carcinoma is often mistaken for hepatocellular carcinoma (Fig. 15.46).
Fig. 15.46 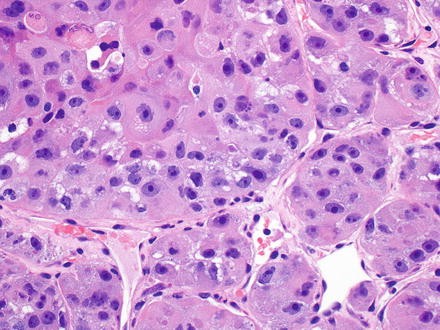
Metastatic renal cell carcinoma. The carcinoma closely mimics hepatocellular carcinoma in both architecture and cytology
-
9.
Epithelioid angiomyolipomas are often mistaken for hepatocellular carcinoma.
-
10.
Angiosarcomas are often mistaken for carcinoma (Fig. 15.47), especially when cytokeratin positive.
Fig. 15.47 
Metastatic angiosarcoma. This angiosarcoma was keratin positive and initially mistaken for a carcinoma
-
11.
Epithelioid hemangioendotheliomas are often misdiagnosed as carcinomas, especially when cytokeratin positive (Figs. 15.48 and 15.49).
Fig. 15.48 
Epithelioid hemangioendothelioma. The morphology can suggest cholangiocarcinoma
Fig. 15.49 
Epithelioid hemangioendothelioma, CK7. The tumor cells are strongly CK7 positive
-
12.
Some lymphomas, including diffuse large B cell lymphomas, can be p63 positive (Figs. 15.50 and 15.51).
Fig. 15.50 
Diffuse large B cell lymphoma. The original diagnosis considered was carcinoma
Fig. 15.51 
Diffuse large B cell lymphoma. The strong P63 staining is a potential diagnostic pitfall (same case as shown in Fig. 15.50)
-
13.
CKIT staining does not always indicate a tumor is a gastrointestinal stromal tumor (GIST); a number of different types of carcinomas as well as melanomas are CKIT positive.
-
14.
Melanomas can be epithelioid, and sometimes rhabdoid (Fig. 15.52). Pigment is present in some cases (Fig. 15.53), but not all. Melanomas will have varying staining patterns, including cases that are S100 negative, and a panel is often needed to fully exclude melanoma (e.g., keratins as negative markers, however, few melanomas can show patchy positivity for keratins; Mel-A, HMB45, microphthalmia transcription factor (MITF) as affirmative markers). Spindle cell melanomas tend to be S100 positive but negative for the other markers.
Fig. 15.52 
Metastatic melanoma. A metastatic ocular melanoma
Fig. 15.53 
Metastatic melanoma. This metastatic melanoma shows pigmented tumor cells
-
15.
Metastatic (and primary) colon adenocarcinomas from the right side of the colon are often CK20 negative, or have only focal staining, especially those with microsatellite instability (MSI-high).











15.12 Metastatic Sarcomas and Lymphomas
GIST and uterine leiomyosarcoma are the two most common sarcomas that show liver metastasis [34]. Both have spindle cell morphology and can be distinguished from primary hepatic tumors by H&E findings in most cases (Fig. 15.54). However, GISTs are not always spindled in their growth and can be epithelioid (Figs. 15.55 and 15.56). Immunostains, however, are usually indicated to determine the tumor phenotype. GISTs are positive for CD117 (Fig. 15.57), DOG-1, CD34 (70 % of cases) and often smooth muscle actin (30 % of cases), and only rarely for desmin (1 % of cases). In contrast, leiomyosarcomas are positive for desmin (100 % of cases) and smooth muscle actin; and negative for CD117 and DOG-1 (Figs. 15.58 and 15.59). Of note, primary leiomyosarcomas can rarely arise from the intrahepatic course of the inferior vena cava and extend secondarily to involve the hepatic parenchyma. Lymphomas, leukemias, and myeloproliferative disorders may also involve the liver [35] and can either form a mass lesion within the liver or produce diffuse portal and/or sinusoidal infiltrates. These lesions are covered in detail in Chap. 12.

Metastatic gastrointestinal stromal tumor. The tumor shows a spindled growth pattern

Metastatic gastrointestinal stromal tumor. The tumor resembles a poorly differentiated carcinoma

Metastatic gastrointestinal stromal tumor. The tumor is epithelioid and was submitted in consultation as probably a hepatocellular carcinoma

Metastatic gastrointestinal stromal tumor. A CKIT stain is strongly positive (same case in Fig. 15.56)

Metastatic leiomyosarcoma. Spindle-shaped tumor cells with pale eosinophilic cytoplasm

Metastatic leiomyosarcoma. A smooth muscle actin stain is positive
15.13 Prognosis of Metastatic Tumors
In most patients, liver metastasis indicates advanced stage disease, which precludes surgical treatment and the possibility for cure of disease is low. Hence, most patients with liver metastasis die within the first 2 years of diagnosis. However, patients with colon carcinoma metastatic to the liver now frequently undergo liver metastasectomy, with 5- and 10-year survival rates that are up to 40 % and 20 %, respectively [36].
References
Disibio G, French SW. Metastatic patterns of cancers: results from a large autopsy study. Arch Pathol Lab Med. 2008;132:931–9.
Geller SA, Dhall D, Alsabeh R. Application of immunohistochemistry to liver and gastrointestinal neoplasms: liver, stomach, colon, and pancreas. Arch Pathol Lab Med. 2008;132:490–9.
Pan CC, Chen PC, Tsay SH, Ho DM. Differential immunoprofiles of hepatocellular carcinoma, renal cell carcinoma, and adrenocortical carcinoma: a systemic immunohistochemical survey using tissue array technique. Appl Immunohistochem Mol Morphol. 2005;13:347–52.
Sangoi AR, Fujiwara M, West RB, Montgomery KD, Bonventre JV, Higgins JP, et al. Immunohistochemical distinction of primary adrenal cortical lesions from metastatic clear cell renal cell carcinoma: a study of 248 cases. Am J Surg Pathol. 2011;35:678–86.
Tong GX, Yu WM, Beaubier NT, Weeden EM, Hamele-Bena D, Mansukhani MM, et al. Expression of PAX8 in normal and neoplastic renal tissues: an immunohistochemical study. Mod Pathol. 2009;22:1218–27.
Mentrikoski MJ, Wendroth SM, Wick MR. Immunohistochemical distinction of renal cell carcinoma from other carcinomas with clear-cell histomorphology: utility of CD10 and CA-125 in addition to PAX-2, PAX-8, RCCma, and adipophilin. Appl Immunohistochem Mol Morphol. 2014;22:635–41.
Murakata LA, Ishak KG, Nzeako UC. Clear cell carcinoma of the liver: a comparative immunohistochemical study with renal clear cell carcinoma. Mod Pathol. 2000;13:874–81.
Kakar S, Muir T, Murphy LM, Lloyd RV, Burgart LJ. Immunoreactivity of Hep Par 1 in hepatic and extrahepatic tumors and its correlation with albumin in situ hybridization in hepatocellular carcinoma. Am J Clin Pathol. 2003;119:361–6.
Yan BC, Gong C, Song J, Krausz T, Tretiakova M, Hyjek E, et al. Arginase-1: a new immunohistochemical marker of hepatocytes and hepatocellular neoplasms. Am J Surg Pathol. 2010;34:1147–54.
Renshaw AA, Granter SR. A comparison of A103 and inhibin reactivity in adrenal cortical tumors: distinction from hepatocellular carcinoma and renal tumors. Mod Pathol. 1998;11:1160–4.
Ghorab Z, Jorda M, Ganjei P, Nadji M. Melan A (A103) is expressed in adrenocortical neoplasms but not in renal cell and hepatocellular carcinomas. Appl Immunohistochem Mol Morphol. 2003;11:330–3.
Wang JH, Dhillon AP, Sankey EA, Wightman AK, Lewin JF, Scheuer PJ. ‘Neuroendocrine’ differentiation in primary neoplasms of the liver. J Pathol. 1991;163:61–7.
Atwell TD, Lloyd RV, Nagorney DM, Fidler JL, Andrews JC, Reading CC. Peritumoral steatosis associated with insulinomas: appearance at imaging. Abdom Imaging. 2008;33:571–4.
Nakatsura T, Kageshita T, Ito S, Wakamatsu K, Monji M, Ikuta Y, et al. Identification of glypican-3 as a novel tumor marker for melanoma. Clin Cancer Res. 2004;10:6612–21.
Jinawath A, Akiyama Y, Yuasa Y, Pairojkul C. Expression of phosphorylated ERK1/2 and homeodomain protein CDX2 in cholangiocarcinoma. J Cancer Res Clin Oncol. 2006;132:805–10.
Chu PG, Schwarz RE, Lau SK, Yen Y, Weiss LM. Immunohistochemical staining in the diagnosis of pancreatobiliary and ampulla of Vater adenocarcinoma: application of CDX2, CK17, MUC1, and MUC2. Am J Surg Pathol. 2005;29:359–67.
Hinoi T, Tani M, Lucas PC, Caca K, Dunn RL, Macri E, et al. Loss of CDX2 expression and microsatellite instability are prominent features of large cell minimally differentiated carcinomas of the colon. Am J Pathol. 2001;159:2239–48.
McGregor DK, Wu TT, Rashid A, Luthra R, Hamilton SR. Reduced expression of cytokeratin 20 in colorectal carcinomas with high levels of microsatellite instability. Am J Surg Pathol. 2004;28:712–8.
Gurzu S, Jung I. Aberrant pattern of the cytokeratin 7/cytokeratin 20 immunophenotype in colorectal adenocarcinomas with BRAF mutations. Pathol Res Pract. 2012;208:163–6.
Liu D, Momoi H, Li L, Ishikawa Y, Fukumoto M. Microsatellite instability in thorotrast-induced human intrahepatic cholangiocarcinoma. Int J Cancer. 2002;102:366–71.
Limpaiboon T, Krissadarak K, Sripa B, Jearanaikoon P, Bhuhisawasdi V, Chau-in S, et al. Microsatellite alterations in liver fluke related cholangiocarcinoma are associated with poor prognosis. Cancer Lett. 2002;181:215–22.
Liengswangwong U, Karalak A, Morishita Y, Noguchi M, Khuhaprema T, Srivatanakul P, et al. Immunohistochemical expression of mismatch repair genes: a screening tool for predicting mutator phenotype in liver fluke infection-associated intrahepatic cholangiocarcinoma. World J Gastroenterol. 2006;12:3740–5.
Karagkounis G, Torbenson MS, Daniel HD, Azad NS, Diaz Jr LA, Donehower RC, et al. Incidence and prognostic impact of KRAS and BRAF mutation in patients undergoing liver surgery for colorectal metastases. Cancer. 2013;119:4137–44.
Nielsen K, Rolff HC, Eefsen RL, Vainer B. The morphological growth patterns of colorectal liver metastases are prognostic for overall survival. Mod Pathol. 2014;27:1641–8.
Morris-Stiff G, White AD, Gomez D, Cameron IC, Farid S, Toogood GJ, et al. Nodular regenerative hyperplasia (NRH) complicating oxaliplatin chemotherapy in patients undergoing resection of colorectal liver metastases. Eur J Surg Oncol. 2014;40:1016–20.
Pawlik TM, Olino K, Gleisner AL, Torbenson M, Schulick R, Choti MA. Preoperative chemotherapy for colorectal liver metastases: impact on hepatic histology and postoperative outcome. J Gastrointest Surg. 2007;11:860–8.
Vauthey JN, Pawlik TM, Ribero D, Wu TT, Zorzi D, Hoff PM, et al. Chemotherapy regimen predicts steatohepatitis and an increase in 90-day mortality after surgery for hepatic colorectal metastases. J Clin Oncol. 2006;24:2065–72.
Surrey LF, Frank R, Zhang PJ, Furth EE. TTF-1 and Napsin-A are expressed in a subset of cholangiocarcinomas arising from the gallbladder and hepatic ducts: continued caveats for utilization of immunohistochemistry panels. Am J Surg Pathol. 2014;38:224–7.
Fan ZJ, Wu Y, Wang ZJ. Expression of estrogen receptor and progesterone receptor in hilar cholangiocarcinoma and their clinical significances. Zhonghua Yi Xue Za Zhi. 2005;85:2651–3.
Yang Z. The utility of villin and mammaglobin in the differential diagnosis between intrahepatic cholangiocarcinoma and breast cancer. Appl Immunohistochem Mol Morphol. 2015;23(1):19–25.
Hirano D, Okada Y, Minei S, Takimoto Y, Nemoto N. Neuroendocrine differentiation in hormone refractory prostate cancer following androgen deprivation therapy. Eur Urol. 2004;45:586–92. discussion 92.
Kaufmann O, Dietel M. Expression of thyroid transcription factor-1 in pulmonary and extrapulmonary small cell carcinomas and other neuroendocrine carcinomas of various primary sites. Histopathology. 2000;36:415–20.
Ordonez NG. Value of thyroid transcription factor-1 immunostaining in distinguishing small cell lung carcinomas from other small cell carcinomas. Am J Surg Pathol. 2000;24:1217–23.
Stavrou GA, Flemming P, Oldhafer KJ. Liver resection for metastasis due to malignant mesenchymal tumours. HPB (Oxford). 2006;8:110–3.
Bosman FCF, Hruban RH, Theise ND. WHO classification of tumors of the digestive system. Lyon: IARC; 2010.
Frankel TL, D’Angelica MI. Hepatic resection for colorectal metastases. J Surg Oncol. 2014;109:2–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Chandan, V.S. (2015). Metastatic Tumors. In: Mounajjed, T., Chandan, V., Torbenson, M. (eds) Surgical Pathology of Liver Tumors. Springer, Cham. https://doi.org/10.1007/978-3-319-16089-4_15
Download citation
DOI: https://doi.org/10.1007/978-3-319-16089-4_15
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-16088-7
Online ISBN: 978-3-319-16089-4
eBook Packages: MedicineMedicine (R0)