
Abstract
Healthcare sector effectuates agile application to upgrade services level and competitive advantage. It states utilizing expertise ideas relating numerous managing methods in obtaining a correlation between variable. The paper begins with the idea of agility in the healthcare organization; secondly, it facilitates us in finding out the factors affecting the agility in the healthcare organization; thirdly, it explicates the interrelationship among them using Interpretive Structure Modelling (ISM) technique and MICMAC analysis. Agility being imperative for healthcare organization as it helps healthcare companies reconcile more rapidly to fluctuating customer needs, competitor feedback. This study helps in the ranking of factors influencing agility in healthcare, which finally help hospitals and healthcare organization in implementing agile system efficiently and effectively.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
To survive in the current competition of advance era of globalization, every line of work of the company is working hard to develop the best quality management parameters, tools, and strategies. Every manufacturing organization now requires effective remote sensing and degree of automation in synchronizing with Web facilities platform. Moreover, an organization needs to amalgamate environmental management into their plan so as to achieve suppleness in an agile manufacturing system. The idea of agility long last from a century, with an organization from US military to Japanese manufactures. Healthcare organization nowadays being a great center of interest and are under severe pressure to improve. It is now a challenging sector, it comprises hospitals, nursing homes, clinics, and institutions with every level of patient care. As the time passes, the demand for health care is increasing day to day, but the financial condition is becoming more worsening. Hence, there is a need for the efficient way of facilitating health care services. In this era, customer requires affordable, accessible, safe, and cost-effective health care. So it is a challenging issue for both industries and academia to how to tackle this issue? However, there are many solutions to this issue such as networking, reengineering, and high-performance organization. Variation in customer demand has left the manufacturing industries bewildered. Today customers have ample of the option to choose, so to compete in the market manufacturing industries are compelled to fulfill the desires of the customer. So there is the need to implement agile techniques in the healthcare organization. Although, lean manufacturing is implemented in health care to eliminate unnecessary motion, wastage, inventory and defects for better flow of goods, information, patients [1]. Various studies show that lean technique is already implemented in hospitals showing better impact [2, 3]. But now there is a need to implement agile techniques in every organization. Implementing agility in health care would lead to remove the complication and will improve the efficiency of the healthcare organization. Agile manufacturing refers to all process, ideas, tools, and training which respond to customer’s needs and market need maintaining cost and quality. Healthcare industry is basically divided into two parts: (a) Healthcare products manufacturing (b) Healthcare services. Healthcare product manufacturing includes health equipment manufacturers, drug manufacturers. Healthcare services include services such as consultation, exercise centers, medical software, and medical insurance. An organization can only fulfill the increasing, complex, unpredictable demand and variation in product design and services by applying agile techniques [4, 5]. The ultimate goal is to obtain development, upgradation, and refinement of the healthcare organization internationally so that quality service can be given to patients. Improving the quality with simultaneously reducing cost is a challenging task. As stated by Natarajan, that in last two decades, health care has improved a lot in the field of delivery of service, quality of care, in absentia health care (that is non-face-to-face communication) and among many others factors.
Hence, 10 factors have been recognized through various literature reviews, articles, and expertise views which are then analyzed by Interpretive Structure Modeling (ISM) technique and MICMAC analysis. ISM techniques are one of the ideal approaches to examine the interconnections between numerous factors [6–8]. With the help of ISM technique and MICMAC analysis linkage between numerous factors are obtained, the factors are then isolated as the driving factors (the main cause of others factors to occur) and dependence factors (depends on others). The segregation and examination of factors are done so that researchers can provide proper devotion and care and it also helps the managers while applying agility in their company.
The main aim behind writing this paperwork is:
-
To detect and identify the factors or elements and make changes in healthcare organization switching from conventional to the agile system.
-
With the help of ISM techniques, develop a relationship between factors.
-
Using MICMAC analysis, determine the driving and dependence power of the factors affecting AMS in health care.
-
To determine the best scope of these techniques.
The residue of this paperwork contains recognition of key factors with the help of reports and publications and expertise ideas are described in the Sects. 2 and 3. Section 4 contains a brief introduction of the ISM approach. Implementation of the ISM approach and MICMAC analysis is shown in Sect. 5. In the last, Sect. 6 has results, conclusions, and future scope.
2 Literature Review
While looking into various literatures and papers, we found numerous obstacles faced by healthcare organization during agile practices. This shows that there are various factors which affect the agility in health care or decides the upbringings and downfall of agile projects in health care. First of all, we should know what agile companies are? According to Christopher and Jultner, agility is a reply to the high level of intricacy and uncertainty in the advanced market. Naylor et al. [9] stated that “agility implies applying market understanding and utilizing chances for fast-changing market”. Agility and flexibility are inter-related to each other as discussed in the literature [10, 11]. Roots of agility lie in the flexible manufacturing system [12]. The main aim of the agile endeavor is to fulfill customer and employees satisfaction. In a competitive market where the demand of customer fluctuates rapidly, Agility is believed as the winning scheme or plan of action. According to a case study of a public health care organization in Europe by Helena Santos–Rodrigues, Joao Faria, and Desiree Cranfield focuses on finding the effect of intellectual capital on healthcare organization. On the basis of this, 68 questionnaires data were used in research which were filled by hospital managers and leaders between July and August 2011. Researchers show that there is a direct relationship between human capital and innovation. Katzenbach and Smith [13] cited that Team-based management is a highly active facilitator of organizational agility. Kidd [14] stated that improved agility requires the amalgamation of human capital, ideas and advanced technology. Various activity and effort to execute agility in an organization are sharing information among the different group, giving the power to take the decision to employees integrating technologies, design specification, product planning [15].
3 Identification of Factors Affecting Agility in Healthcare Organization
Now a day’s disease growing in the society must be considered as a priority to be dealt at every level. Evolution from a traditional or conventional approach to agile techniques is not an easy deal it requires identifying and analyzing the factors that could facilitate faster implementation of agility in healthcare organization [16]. So this paper identifies 10 crucial factors through literature and experts views from academia and industry. These factors are as follows (Table 1).
4 An Introduction of ISM Approach
Due to the availability of a large number of elements and connectivity among these elements researchers faced ample of the problem which required to be solved for obtaining an optimal solution [29]. So to solve these type of complex structures various methodology have been tested, among them ISM is the ideal and advance one. ISM was first proposed by Warfield in 1973 to solve complexly structured modeling [30]. ISM is a computer-aided forming method which enables us in joining three methodologies, i.e., words, graphics, and mathematics. It is a methodology to solve complex cases and models [31]. As stated by Attri et al. [32], ISM converts an ambiguous and complex problem to structure a well-defined problem and provides the impact of variables on decision objects. ISM is defined as a procedure which helps in supporting the user to realize what they believe and examine clearly what they don’t know [33, 34]. It is a method which converts unsystematic and unarranged models of the system into well-arranged models [32]. ISM methodology facilitates us to use expert’s ideas, knowledge to divide complex situation models into various factors or subfactors and provides a multi-level structural model. It is a structural analysis tool which helps in defining variables according to the extent they influence other factors.
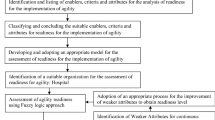
In the ISM approach, first identification of factors which affect the system and the factors that are related to each other are identified [35]. After the factors being recognized, relationship is developed between the factors which are aligned into matrix named structure self-interaction matrix (SSIM). After obtaining the SSIM matrix, reachability matrix (RM) is obtained with the help of SSIM and is checked for transitivity. After that reachability matrix is converted into conical matrix. With the help of relationship developed by reachability matrix, digraph is drawn. The digraph is now converted into ISM model [29, 30, 33, 36]. The steps are illustrated via diagram as shown in Fig. 1.

Flow diagram for ISM methodology
5 Modeling of AMS Factors with ISM Approach and MICMAC Analysis
For model making, several steps which are to be followed are:
-
Step 1 Determining relevant key factors influencing health care
The factors influencing agility healthcare organization are determined via literature survey and brainstorming with knowledgeable from academia and health care.
-
Step 2 Preparation of structural self-interactive matrix (SSIM)
In SSIM, four notation are shown to indicate inter-connection factors (i and j)
-
V indicates that factor j will be helped by factor i.
-
A indicates that factor i will be helped by factor j.
-
X indicates i and j will influence each other.
-
O indicates both are not related to each other.
The relationship between the factors has been determined and then SSIM has been developed. This SSIM is then discussed by expertise as depicted in Table 2. The symbols V, A, X, O denote the relationship between the factors (i and j) [37]
-
Notation V is used for cell (1, 9) because of factor 1 effect factor 12.
-
Notation A is used for cell (2, 10) because of factor 10 effect factors 2.
-
Notation X is used for cell (4, 7) because factor 4 and 7 affect each factor.
-
Notation O is used for cell (1, 8) because factor 1 and 8 are unrelated.
-
Step 3 Establishing reachability matrixes
After obtaining the SSIM matrix, a reachability matrix is created. In this, SSIM is transformed into a binary matrix by replacing V, A, X, O by 1, 0 as per case. The rules for substituting 1 and 0 are as follows:
-
If V is used in place of (i, j) in Table 2, then the (i, j) will have 1 and (j, i) will have 0.
-
If A is used in place of (i, j) in Table 2, then the (i, j) will have 0 and (j, i) will have 1.
-
If X is used in place of (i, j) in Table 2, then the (i, j) will have 1 and (j, i) will also have 1.
-
If O is used in place of (i, j) in Table 2, then the (i, j) will have 0 and (j, i) will have 0.
-
V is used for (1, 9), thus reachability matrix will have 1 for (i, j) and 0 for (j, i).
-
A is used for (2, 10), thus reachability matrix will have 0 for (i, j) and 1 for (j, i).
-
X is used for (4, 7), thus reachability matrix will have 1 for both (i, j) and (j, i).
-
O is used for (1, 7), thus reachability matrix will have 0 for both (i, j) and (j, i).
Final reachability matrix is calculated by integrating transitivity. Transitivity is a connection between three elements such that if a relationship holds for A and B and also the relation occurs between B and C then A and C itself comes in a relation. Table 3 depicts Final reachability matrix and 1* stands for transitivity.
-
Step 4 Partition of reachability matrix into different levels
Final reachability matrix possesses reachability and antecedent set. The horizontal factors come under reachability set and antecedent set comprises vertical factors. After that common value is obtained [38]. The factors having the same value for reachability and intersection set occurs in the first position. The first level is then eliminated from the table, and then this process repeats for the next level of a hierarchy. This process repeats until each element got its position in the pecking order. This order enables us in the modeling of the digraph. Ten factors along with the reachability set, antecedent set, intersection set, and the levels are shown in Table 4.
-
Step 5 Making of conical matrix
Conical matrix is obtained by arranging the factors according to highness of hierarchy from top to bottom. By summing a total number of ones in the rows, we get drive power and by adding in a column we get dependence power. Now, the drive power and dependence power are ranked by checking maximum no of ones in rows and column, respectively, as depicted in Table 5.
-
Step 6 Development of digraph
In the making of the digraph, the top-level factors are located at the topmost place of the digraph and then the second level is indicated in the second level of the digraph and rest follow the same till we get bottom level in the last position.
-
Step 7 Drafting ISM model
Now after obtaining digraph, an ISM model is created by exchanging nodes with their respective factors as displayed in Fig. 3. ISM model represents that multi-skill and multi-knowledgeable employees and leadership in the healthcare organization have high driving power. The employees must be provided with the best training program so that everyone has multi-skill and knowledge and flexibility to rapidly switch to a new task if required. For better agility in healthcare, proper leadership must be there as a good leader has a great impact on the worker by their personality leadership is the foundation and basic requirement in any healthcare as it imparts confidence to the team. Unlike traditional management style of control and command leadership, trust and confidence should be there. ISM model shows that factors having high driving factors as organization structure play a vital role in the execution of agile manufacturing system. They also need more attention and care as they have high driving and low dependency. Patient assumption and hospital discernment and chain management in hospitals also play a vital role in AMS. After those factors like a patient assumption and hospital discernment, technology upgrade and market awareness come in the hierarchy level after that, hence, these factors have the average drive and dependency powers. Outsourcing and supporting customers mentally have high dependency and less driving powers. These required less care as it would not have much effect.
-
Step 8 MICMAC analysis
The main idea behind the MICMAC technique is to get the driving and dependency powers of the above factors. Now these factors have been divided into four groups as described in Fig. 4.
-
Group 1: Autonomous factors;
-
Group 2: Dependent factors;
-
Group 3: Linkage factors;
-
Group 4: Driving factors.
-
Group 1: Autonomous factors—weak driving power and weak dependency is the characteristic of this group. In this group, we have four factors, i.e., organizational structure, Implementing clinical governance, technology upgrade, and outsourcing (Factors 1, 5, 6 and 8), respectively.
-
Group 2: Dependence factors—this group shows weak drive power but strong dependence. In this group, two factors have been identified, i.e., patient assumption and hospital discernment and supporting customers mentally (Factors 3 and 9), respectively.
-
Group 3: Linkage factors—No factors have been identified in this group. These groups possess both driving and dependency power strong.
-
Group 4: Driving factors—weak dependence and strong driving power is the characteristic of this group. In this group, we have four identified factors, i.e., leadership, Chain management in hospitals, market awareness, multi-skill and multi-knowledgeable employees (Factors, 2, 4, 7, and 10) respectively (Fig. 2).
Fig. 2 
Digraph for AMS factor
-

6 Results and Conclusion
This paper has identified 10 factors affecting agility in healthcare organization by reviewing several kinds of literature, research papers, and experts’ ideas. ISM analysis and MICMAC analysis have been applied to those factors to develop the contextual relationship between them. The result of above is shown in Figs. 3 and 4. The factors play a crucial role in the upliftment of healthcare services; these models show a hierarchy that which factors have a greater influence on a healthcare organization. This approach can be helpful for medical colleges, nursing homes, super specialty hospital, healthcare practitioners, and decision makers. The factors which have been identified are very recent and useful for the growth of hospitals. The Indian health care is still facing problems due to practicing traditional approach in spite of using new agile techniques. The rapid changes in the market and customer demands variation requires agile manufacturing techniques to be implemented [23]. New optimized healthcare models are required for sustainable development in healthcare organization and for that we have to choose the correct path for applying input resources.

MICMAC analysis

ISM model for AMS in healthcare
Based on the result obtained in this paper, the following points are noted as:
-
This research paper uses ISM and MICMAC approach for determining key factors that should be implemented in a healthcare organization.
-
This approach also lets us knows the relationship between the factors and type extent of influence of one factor on another factor.
-
Factors like multi-skill and multi-knowledgeable employees, leadership, organization structure have high driving factor, i.e., if these factors severely affect others factors, hence, these key factors require pure devotion and care on the priority basis.
-
This research also shows a path for an organization which still run on traditional techniques to rapidly switch over implementing new agile techniques to their organization.
The health care now is a wide sector and requires huge attention and researches to be done so that new and more innovative ideas can be implements in this sector for economic growth of the country.
References
Brandao de Souza L (2009) Trends and approaches in lean healthcare. Leadership Health Serv 22(2):121–139
Radnor Z, Osborne SP (2013) Lean: a failed theory for public services? Public Manage Rev 15(2):265–287
Sindhwani R, Malhotra V (2013) Overview and drivers of agile manufacturing system: a review. Int J Mark Technol 3(12):144
Towill D, Christopher M (2002) The supply chain strategy conundrum: to be lean or agile or to be lean and agile? Int J Logist 5(3):299–309
Sindhwani R, Malhotra V (2015) Lean and agile manufacturing system barriers. Int J Adv Res Innov 3(1):110–112
Kumar S, Sharma RK (2015) An ISM based framework for structural relationship among various manufacturing flexibility dimensions. Int J Syst Assur Eng Manage 6(4):511–521
Jain V, Raj T (2015) Modeling and analysis of FMS flexibility factors by TISM and fuzzy MICMAC. Int J Syst Assur Eng Manage 6(3):350–371
Attri R, Dev N, Sharma V (2013) Interpretive structural modelling (ISM) approach: an overview. Res J Manage Sci 2(2):3–8
Naylor JB, Naim MM, Berry D (1999) Leagility: integrating the lean and agile manufacturing paradigms in the total supply chain. Int J Prod Econ 62(1–2):107–118
Christopher M (2000) The agile supply chain: competing in volatile markets. Ind Mark Manage 29(1):37–44
Swafford PM, Ghosh S, Murthy NN (2006) A framework for assessing value chain agility. Int J Oper Prod Manage 26(2):118–140
Gosling J, Purvis L, Naim MM (2010) Supply chain flexibility as a determinant of supplier selection. Int J Prod Econ 128(1):11–21
Katzenbach JR, Smith DK (1993) The wisdom of teams: creating the high-performance organization. Harvard Business Press, Boston
Kidd PT (1995) Agile manufacturing: forging new frontiers. Addison-Wesley Longman Publishing Co., Inc, London
Gehani RR (1995) Time-based management of technology: a taxonomic integration of tactical and strategic roles. Int J Oper Prod Manage 15(2):19–35
Sindhwani R, Malhotra V (2016) Modelling the attributes affecting design and implementation of agile manufacturing system. Int J Process Manage Benchmarking 6(2):216–234
https://www.beckershospitalreview.com/human-capital-and-risk/agile-management-can-benefit-healthcare-process-improvement-projects.html, last accessed 2018/12/24
Powell L (2002) Shedding a tier: flattening organisational structures and employee empowerment. Int J Educ Manage 16(1):54–59
https://www.linkedin.com/pulse/20140915033433-34529931-leadership-impact-on-healthcare-organizational-behavior, last accessed 2018/12/24
Talib F, Rahman Z (2015) An interpretive structural modelling for sustainable healthcare quality dimensions in hospital services. Int J Qual Res Serv 2(1):28–46
Vanu SC (2004) Clinical governance: a fresh look at its definition. Clin Governance Int J 9(2):87–90
Thomson R (1998) Quality to the fore in health policy at last. Br Med J 317(7151):95–96
Mittal VK, Sindhwani R, Kalsariya V, Salroo F, Sangwan KS, Singh PL (2017) Adoption of integrated Lean-Green-Agile strategies for modern manufacturing systems. Proc CIRP 61:463–468
Feeney AR, Zairi M (1994) Best practice quality management in pathology: results of a benchmarking study. Benchmarking Qual Manage Technol 1(2):64–80
Christopher M, Towill D (2001) An integrated model for the design of agile supply chains. Int J Phys Distrib Logist Manage, 31(4):235–246
Tolf S, Nyström ME, Tishelman C, Brommels M, Hansson J (2015) Agile, a guiding principle for health care improvement? Int J Health Care Qual Assur 28(5):468–493
Guimarães CM, de Carvalho JC (2011) Outsourcing in the healthcare sector-a state-of-the-art review. Supply Chain Forum Int J 12(2):140–148
Sharp JM, Irani Z, Desai S (1999) Working towards agile manufacturing in the UK industry. Int J Prod Econ 62(1–2):155–169
Jayant A, Azhar M, Singh P (2015) Interpretive structural modelling (ISM) approach: a state of the art literature review. Int J Res Mech Eng Technol 5(1):15–21
Malhotra V (2014) Modelling the barriers affecting design and implementation of reconfigurable manufacturing system. Int J Logist Syst Manage 17(2):200–2017
Janes FR (1988) Interpretive structural modelling: a methodology for structuring complex issues. Trans Instrum Meas Control 10(3):145–154
Attri R, Grover S, Dev N, Kumar D (2013) An ISM approach for modelling the enablers in the implementation of total productive maintenance (TPM). Int J Syst Assur Eng Manage 4(4):313–326
Raj T, Shankar R, Suhaib M (2008) An ISM approach for modelling the enablers of flexible manufacturing system: the case for India. Int J Prod Res 46(24):6883–6912
Sindhwani R, Malhotra V (2017) Modelling and analysis of agile manufacturing system by ISM and MICMAC analysis. Int J Syst Assur Eng Manage 8(2):253–263
Mittal VK, Sangwan KS (2011) Development of an interpretive structural model of obstacles to environmentally conscious technology adoption in Indian industry. In: Globalized solutions for sustainability in manufacturing. Springer, Berlin, pp 383–388
Talib F, Rahman Z, Qureshi MN (2011) An interpretive structural modelling approach for modelling the practices of total quality management in service sector. Int J Model Oper Manage 1(3):223–250
Sindhwani R, Malhotra V (2016) Barriers evaluation for agile manufacturing system with fuzzy performance importance index approach. Int J Agile Syst Manag 9(4):292–301
Sindhwani R, Malhotra V (2017) A framework to enhance agile manufacturing system: a total interpretive structural modelling (TISM) approach. Benchmarking Int J 24(4):467–487
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Sindhwani, R., Singh, P.L., Iqbal, A., Prajapati, D.K., Mittal, V.K. (2019). Modeling and Analysis of Factors Influencing Agility in Healthcare Organizations: An ISM Approach. In: Shanker, K., Shankar, R., Sindhwani, R. (eds) Advances in Industrial and Production Engineering . Lecture Notes in Mechanical Engineering. Springer, Singapore. https://doi.org/10.1007/978-981-13-6412-9_64
Download citation
DOI: https://doi.org/10.1007/978-981-13-6412-9_64
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-6411-2
Online ISBN: 978-981-13-6412-9
eBook Packages: EngineeringEngineering (R0)