
Abstract
Enterococcal species are Gram-positive lactic acid bacteria that are ubiquitously present in environmental samples, plants, and gastrointestinal tracts of animals. As commensals they are known to benefit the host, but in recent years, they have earned dubious reputation as nosocomial pathogens. They are known to cause diseases like urinary tract infections, endocarditis, bacteremia, and intra-abdominal infections especially in immunocompromised patients that are subjected to prolonged antibiotic treatments. The various factors contributing to their status as nosocomial pathogens are their intrinsic and acquired resistance to various classes of antibiotics. They are known to persist on animate and inanimate surfaces for a long period of time which thus act as reservoirs for the spread of the infection in hospitals. Recent studies have shown that the nosocomial strains are genetically distinct from commensal Enterococcal strains. Thus, herein the various diseases caused by nosocomial Enterococcus spp., the problem of antibiotic resistance, and their treatment have been reviewed. Further, this chapter also discusses the various virulence factors contributing to its pathogenicity and highlights the genetic differences between pathogenic and commensal Enterococcus spp.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
From the last three decades, Enterococcus spp. have emerged as one of the important etiological agents of hospital-associated infections in immunocompromised individuals and in patients with prolonged antibiotic treatment and hospital stay (Gilmore et al. 2013). The two species Enterococcus faecalis and E. faecium out of 50 known species of enterococci are particularly pathogenic to man; for example, E. faecalis accounts for 85–90%, and E. faecium accounts for 5–10% of all Enterococcal diseases (Maki and Agger 1988). Other species that can also be pathogenic include E. gallinarum, E. casseliflavus, E. durans, and E. mundtii. In the USA and Europe, enterococci have been reported to be the second and third leading cause of nosocomial infections (Sievert et al. 2013; Zarb et al. 2012). In India, enterococci accounted for 2.3–9.7% of all nosocomial infections (Sreeja et al. 2012; Chakraborty et al. 2015; Karmarkar et al. 2004). Enterococci have immense genome plasticity, are prolific colonizers, and have the ability to persist in hospital environment for a long time owing to their sturdy nature. The various clinical manifestations of Enterococcal infection are urinary tract infections, bacteremia, endocarditis, and intra-abdominal infections (Murray 1990). Apart from E. faecalis, the incidence of nosocomial E. faecium infections is also on the rise, primarily due to antibiotic resistance in E. faecium. The ability to cause infection in E. faecium is mainly attributed to the increasing resistance to antibiotics, whereas E. faecalis has been reported to exhibit innate ability to cause infections irrespective of the antibiotic resistance (Mundy et al. 2000). To better understand the molecular mechanisms involved in the pathogenicity of Enterococcus, the whole genome sequences of various pathogenic (Qin et al. 2012) and commensal (Brede et al. 2011) Enterococcus spp. have been published and compared.
2 General Characterization of Enterococci
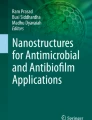
Enterococci are Gram-positive, facultative anaerobic bacteria, which are ovoid in shape and may occur in diploids, in chains, or as single cells (Fig. 15.1). They are catalase- and cytochrome c oxidase-negative. According to the classification by Sherman (1937), the bacteria belonging to Enterococcus genera possess characteristic ability to grow at 10° and 45 °C, in media containing 6.5% NaCl, and do not produce gas from glucose (Schleifer and Kilpper-Bälz 1984). Hydrolysis of L-pyrrolidonyl-3-naphthylamide and group D antisera test is also one of the characteristic features of enterococci genera. The genera fall in low GC branch of bacteria, and G + C content ranges between 37 and 45 mol%. Species-level identification of Enterococcus genera is generally done by 16S rDNA sequencing or whole cell protein analysis. Till date approximately 50 species of Enterococcus have been reported. The prominent species present in the gut of animals and humans is E. faecium followed by E. faecalis (Silva et al. 2012).

(a) Photomicrograph showing Gram-positive coccus-shaped Enterococcal cells in the pulmonary tissue. (b) Scientific classification of Enterococcus genera
3 Habitat
Enterococci are ubiquitous members of gastrointestinal tracts (GIT) of various organisms. In the 1960s and 1970s, enterococci were isolated from GIT of reptiles (85.7%), mammals (71.3%), insects (53%), and birds (31.8%) by Mundt et al. Enterococci have also been isolated from plants (Mundt 1963), soil (Mundt 1961), water, and fermented foods. It is postulated that enterococci may have been one of the earliest members of the GIT with their existence dating back from early Devonian period (Gilmore et al. 2013). Due to their role in highly evolved and extremely competitive environment of GIT, enterococci have well-adapted and reduced genomes ranging from 2.6 to 3.6 Mb. These bacteria are fastidious in nature and draw a number of vitamins and amino acids from their habitats (Niven and Sherman 1944). They have reduced their genome by eliminating genes necessary for the biosynthesis of amino acids and vitamins from simpler precursors.
4 Enterococcal Diseases
4.1 Endocarditis
Enterococcus spp. are known to cause endocarditis since 1899, when the first clinical description of the strain which was most certainly E. faecalis was published (MacCallum and Hastings 1899). Enterococci are the third main causative agents of infective endocarditis (IE) and prosthetic valve endocarditis worldwide after Streptococcus spp. and Staphylococcus spp. Worldwide approximately 10–15% IE cases are caused by enterococci (Murdoch et al. 2009). Frequency of Enterococcal IE is more in elderly debilitated patients with prior valvular damage, intracardiac devices, or a prosthetic valve. It occurs more in men than women (McDonald et al. 2005). Most common clinical findings of IE include subacute fever and the presence of a cardiac murmur. Almost half of the IE patients suffer from heart failure. Mortality rate in Enterococcal IE is significant at 9–15%, but it is lower than IE caused by other pathogens such as S. aureus (McDonald et al. 2005; Rice et al. 1991). The first report of IE by vancomycin-resistant E. faecium (VRE) appeared in the late 1990s (Vijayvargiya and Veis 1996). The risk of VRE IE increases in the patients with the history of hemodialysis and organ transplantation and presence of a central venous catheter (Stevens and Edmond 2005). The study on clinical outcomes of IE by E. faecalis and E. faecium showed high mortality rates and longer persistence of bacteremia in E. faecium IE patients (Forrest et al. 2011).
4.2 Urinary Tract Infections (UTIs)
Enterococcus spp. are the third most common pathogen isolated from catheter-associated UTIs in hospitalized patients causing approximately 15% of the UTI cases in ICU patients. UTIs occur most frequently in elderly men. Vancomycin resistance was found to be 81% in E. faecium and 6% in E. faecalis urinary isolates in catheter-associated UTI (Hidron et al. 2008)
4.3 Bacteremia
At present, enterococci are the second leading causative agent of healthcare-related bacteremia (Hidron et al. 2008). The most common route of Enterococcal bloodstream infection (EBSI) is genitourinary tract and endovascular, intra-abdominal, or soft tissue infections. Other factors like old age, liver disease, male gender, renal impairment, hematologic transplant, diabetes, prior treatment with antibiotics, and malignancy have also been associated with EBSI (Noskin et al. 1995; Gray et al. 1994). In a study on patients diagnosed with acute leukemia, it was demonstrated that the risk of EBSI increases with increase in duration of hospital stay and with administrations of carbapenes and corticosteroids, diarrhea, and severe neutropenia (Ford et al. 2015). Twenty-five percent of EBSI cases have tendency to be polymicrobial in nature (Billington et al. 2014). Mortality rate in polymicrobial EBSI is approximately two times higher than monomicrobial EBSI (McKenzie 2006). Almost 9.5% and 82.6% E. faecalis and E. faecium isolated from blood stream infections are vancomycin resistant (Lautenbach et al. 1999). Unlike S. aureus-associated bacteremia, Enterococcal bacteremia rarely causes metastatic abscesses or seeds distant organs. Some studies have reported more mortality rate in E. faecium caused by bacteremia than that caused by E. faecalis (Noskin et al. 1995). Death rates can be up to 75% in patients with serious health conditions like diabetes mellitus, transplantation, heart diseases, or malignancy.
4.4 Intra-abdominal Infections
Intra-abdominal infections (IAIs) include various pathological conditions, such as fecal peritonitis, uncomplicated appendicitis, perforated viscus, and postoperative complications (Menichetti and Sganga 2009). In a 14-year-long study on recurrent and relapsing peritonitis in patients undergoing peritoneal dialysis, enterococci were found to be common causative agents of recurrent peritonitis (Szeto et al. 2009). The data collected at 68 medical centers demonstrated that enterococci were the most commonly isolated Gram-positive bacteria from IAI patients and constituted almost 12.9% of the isolates out of which 9.2% were E. faecalis and 3.7% were E. faecium (Sartelli et al. 2014). Further, it was reported that the increased intrinsic and acquired resistance in enterococci pose great challenges in the effective treatment of the diseases.
5 Nosocomial Transmission
Nosocomial Enterococcal infections are caused by increased colonization of GIT by resistant enterococci. Prolonged exposure of hospitalized patients to antibiotics alters gut microbiota which decreases the prevalence of Gram-negative microbes in the GIT, thus facilitating colonization by resistant Gram-positive bacteria such as enterococci. The primary mode of transmission of resistant enterococci in hospital setting is through the hands of healthcare workers (Hayden 2000). Studies have shown that enterococci have the ability to persist on the hands for approximately 1 h and for 4 months on inanimate surfaces, which thus act as reservoirs for transmission in the absence of regular sanitization (Kramer et al. 2006). Medical equipments like thermometers, stethoscopes, blood pressure cuffs, intravenous fluid pumps, bed rails, gowns, bedside tables, urinals, bedpans, and bed linens are readily contaminated with high densities of VRE (Bonilla et al. 1997; Hota 2004). Other factors posing VRE colonization risk include duration of patient’s stay in hospital or intensive care unit and patient’s proximity to other VRE-colonized patients (Fig. 15.2; Tornieporth et al. 1996). Strict surveillance of health workers is required to curb the spread of nosocomial Enterococcal infections. Further, various precautions, such as proper decontamination of inanimate surfaces, use of gloves, hand sanitization, etc., should be strictly followed.

Factors affecting the transmission of vancomycin-resistant enterococci (VRE) in nosocomial settings. The close proximity to VRE-infected patient passes on the contamination to hospital staff or hospital equipments and finally to the immunocompromised patient
6 Virulence Determinants of Enterococci
Virulence of enterococci is a multifactorial process, with the participation of several genes and their products. The virulence genes are mostly known to be present on the genome in special regions which are termed pathogenicity islands (PAI). However, some virulence factors may be present on plasmids also. E. faecalis are known to carry more numbers of virulence factors as compared to E. faecium.
7 Secreted Virulence Factors
7.1 Cytolysin
Cytolysin toxin belongs to the class of lantibiotic group of bacteriocins. Cytolysin production can be chromosomally encoded by PAI or encoded by a pheromone-responsive plasmid pAD1 (Ike et al. 1990). Cytolysin consists of two components CylLL and CylLS which are secreted as pro-peptides from the cell. These pro-peptides are proteolytically activated by CylM, CylB, and CylA.
Almost 30% of E. faecalis strains produce cytolysin, and its production has been associated with increased toxicity of Enterococcal infections. Cytolysin can lyse bacterial cells, mammalian erythrocytes, and other eukaryotic cells (Cox et al. 2005). In a rabbit endocarditis model, aggregation substance and cytolysin-positive strains caused 55% mortality as compared to 15% with only aggregation substance-positive strains (Chow et al. 1993).
7.2 Gelatinase
Gelatinase (Gel) is an extracellularly secreted Zn-metalloprotease which hydrolyzes casein, collagen, fibrinogen, complement components (C) 3 and C3a, and hemoglobin. Gel has been implicated as virulence factor by animal models and epidemiological studies. Gel expression is induced by fsr quorum-sensing system in response to high cell density (Qin et al. 2000). It mediates virulence by degrading host tissue and modulating host’s immune response (Park et al. 2008). Gel can activate autolysin which is a peptidoglycan-degrading enzyme and leads to release of DNA and has a role in biofilm formation (Thomas et al. 2009).
8 Cell Surface-Associated Virulence Determinants
8.1 Aggregation Substance
Adherence to host tissue is important for pathogens to cause infection. In enterococci, aggregation substance (AS) and extracellular surface protein (esp) have been reported to play a role in adherence (Waters et al. 2004). In E. faecalis, AS is encoded by pheromone-responsive plasmid in response to pheromone (Clewell 1993). AS mediates aggregation of Enterococcal cells and facilitates transfer of plasmid during conjugation. It also has been reported to promote internalization of Enterococcal cells by intestinal cells, adhesion to renal tubular cells, and survival of E. faecalis cells inside polymorphonuclear neutrophils (Olmested et al. 1994; Kreft et al. 1992). In endocarditis model, destruction of pulmonary and myocardial tissue was found to be caused due to AS. Moreover, AS has been reported to mediate bacterial aggregation on cardiac valve resulting in increased pathogenesis in endocarditis (Schlievert et al. 1998).
8.2 Enterococcal Surface Protein
Esp is a large molecular weight protein expressed on the surface of E. faecalis. Esp is mainly associated with biofilm formation (Heikens et al. 2007) and plays a role in biofilm-associated infections such as UTI (Shankar et al. 2001), bacteremia, and endocarditis (Heikens et al. 2001) as demonstrated by studies with an esp deletion mutant. The esp gene located on PAI encodes a very large LPXTG-motif cell wall-anchored protein in both E. faecalis and E. faecium. It is widely present in E. faecalis strains, but E. faecium esp is predominantly found in hospital-associated isolates, suggesting its role in virulence.
8.3 Adhesion to Collagen Proteins
The ability of E. faecalis to adhere to extracellular matrix proteins like collagen, fibrinogen, laminin, lactoferrin, fibronectin, thrombospondin, and vitronectin has been reported in many studies (Rich et al. 1999; Nallapareddy and Murray 2008). The search for the gene encoding these adhesion molecules led to the discovery of Ace, an adhesin to collagen of E. faecalis. Most of these studies also found that only few isolates of E. faecalis exhibit adherence to extracellular matrix proteins under laboratory conditions (Woodford et al. 2001). Further experiments have found that most clinical isolates of E. faecalis do not express adherence phenotypes constitutively, but expression of these phenotypes is elicited under stress conditions or in the presence of host-derived factors (Nallapareddy and Murray 2008). The role of Ace was studied in experimental endocarditis rat model. Immunization with recombinant anti-Ace antibodies decreased endocarditis development (Singh et al. 2010).
Adherence studies showed that like E. faecalis, many isolates of E. faecium can bind to collagen following growth in brain-heart media, and the protein responsible is a cell wall-anchored Acm (adhesin to collagen of E. faecium; Nallapareddy et al. 2003). Collagen adherence of clinical isolates of E. faecium was found to be significantly more than the isolates from animal, community, or fecal origin, thus suggesting that it is an important factor responsible for infection-causing ability of E. faecium. Incorporation of acm gene in acm-negative mutants resulted in the expression of adherence phenotype. In E. faecium endocarditis mice model, acm mutant was less likely to develop endocarditis; thus it has been shown to be antigenic (Nallapareddy et al. 2008).
8.4 Endocarditis- and Biofilm-Associated Pili (ebp)
The ebp are surface-associated filamentous structures in E. faecalis. It plays a role in biofilm formation by binding to abiotic surfaces and adhering to platelets (Nallapareddy et al. 2011a). In animal models, it contributes to tissue colonization in IE and UTI (Sillanpaa et al. 2013). Deletion of the ebp locus resulted in a diminished capacity of E. faecalis OG1RF to colonize kidneys and bladders in a murine model of ascending UTI (Nallapareddy et al. 2011b) and in catheter-associated UTI (Nielsen et al. 2012).
9 Factors Contributing to Enterococcus Pathogenesis and Divergence from Commensals
Enterococci are part of normal GIT, and transition of commensals to pathogens is associated with change in ecology, acquisition of toxin genes, and mobile genetic elements carrying PAI. Comparative studies of the genomes of nosocomial and commensal strains show that nosocomial strains have acquired these virulent traits. Genome sequence analysis of V583, which is considered as representative strain of nosocomial lineage of E. faecalis, revealed that 26% of the genome comprised of mobile genetic elements, 38 insertion elements, remains of 3 integrative phages, 7 apparent phages, and 3 independently replicating plasmids (Paulsen 2003). Similar evolutionary sequences are found in case of nosocomial E. faecium strains which are found to possess large PAI carrying several IS and esp gene (Leavis et al. 2007). Further, these virulent genes synergize with each other to express the virulence phenotype; for example, in an endocarditis model, AS was found to synergize with cytolysin protein.
Further, the genome of V583 when compared with commensal strain OG1RF revealed the presence of CRISPR-cas in commensal strains which provides defense against plasmid acquisition and phage infection. The absence of CRISPR in V583 led to studies directed to find correlation between absence of CRISPR and accumulation of mobile genetic elements in nosocomial strains. Sixteen E. faecalis strains representing the deepest phylogenetic nodes were studied to identify polymorphism in location and content of CRISPR loci. Results suggested that CRISPR loci were highly conserved and influenced the movement of pheromone-responsive plasmids and phages. A complete absence of CRISPR-cas in MDR Enterococcus strains was also reported (Palmer and Gilmore 2010). Based on the whole genome data and the comparison of the 2113 core genes of the eight E. faecium strains, they were placed in two different clades. Clade A mainly comprised of nosocomial infection-causing strains, whereas clade B comprised of commensal strains. Clades A and B have similarity in the range 93.9–95.6% that shows the degree of divergence between the species. In case of E. faecalis, the commensal and nosocomial pathogens can also be similarly differentiated into different clonal complexes, but the division is overlapping in some cases (Gilmore et al. 2013).
10 Treatment
The treatment of infections caused by susceptible Enterococcus strains is mainly by using ß-lactam antibiotics. Monomicrobial Enterococcal infections that are susceptible are usually treated with ampicillin and penicillin alone. On the other hand, polymicrobial infections are treated with the combination of ampicillin and other antibiotics having broad spectrum of activity against aerobic, anaerobic, and Gram-negative bacteria. Combination drugs containing β-lactam along with β-lactamase inhibitor such as piperacillin-tazobactam or ampicillin-clavulanic acid can also be used. In case of penicillin allergies, a single agent like vancomycin or teicoplanin can be used to treat nonresistant Enterococcal infections. In case of penicillin-susceptible VRE infections like cystitis, oral application of nitrofurantoin, doxycycline, and fosfomycin can be considered (Heintz et al. 2010). Infections caused by VRE strains are mostly treated by antibiotic, linezolid, daptomycin, and quinupristin-dalfopristin (Q-D), but side effects are common in prolonged treatment. For E. faecium Q-D is not used as it is resistant. UTI and skin and soft tissue infections caused by VRE are treated by fluoroquinolones or doxycycline depending upon the susceptibility patterns (Landman and Quale 1997). Adjunct measures including drainage of abscesses and removal of infected foci can also be used wherever possible.
Treatment of IE caused by E. faecalis mainly includes combination of ß-lactams, gentamicin, and aminoglycosides. In case of IE caused by E. faecium, treatment is challenging due to higher resistance to ß-lactams and aminoglycosides. Daptomycin and ceftaroline have also been found to be effective for the treatment (Pericás et al. 2015).
11 Antibiotic Resistance
Increasing antibiotic resistance in enterococci is a matter of concern because the increase in the cases of Enterococcal infections in humans is partially due to its ability to escape the action of commonly used antibiotics. Enterococci are known to be intrinsically resistant to many antibiotics due to which they can exist in environments enriched for antibiotic resistance (Mundy et al. 2000; Murray 1998). They are known to be intrinsically resistant to semisynthetic penicillins and cephalosporins due to the presence of low-affinity penicillin-binding proteins; for example, E. faecalis expresses PBP4, and E. faecium expresses PBP5. The minimum inhibitory concentrations (MICs) for penicillins are typically 2–8 μg/ml for E. faecalis and 8–16 μg/ml for E. faecium (Sifaoui et al. 2001). They also show decreased susceptibility to penicillin, ampicillin, aminoglycosides, and clindamycin.
Among aminoglycosides, the MIC of streptomycin and kanamycin in E. faecalis is 250 μg/ml, whereas that of tobramycin and gentamycin is 8–64 μg/ml (Chow 2000). Aminoglycoside resistance is due to the inability of the aminoglycoside to enter the thick cell wall (Aslangul et al. 2006). Therefore in the presence of cell wall-inhibiting antibiotics such as β-lactams, the enterococci become susceptible to aminoglycosides. The presence of aminoglycoside-converting enzymes such as acetyltransferases, phosphotransferases, and nucleotidyl transferases in E. faecium and E. faecalis also contributes to aminoglycoside resistance (Chow 2000; Miller et al. 2014). In E. faecium chromosomally encoded genes, rRNA methyltransferase (efmM) (Galimand et al. 2011) and a 6′-N-aminoglycoside acetyltransferase (aac(6′)- Ii) (Costa et al. 1993) are associated with intrinsic resistance to tobramycin and kanamycin. Resistance to clindamycin in E. faecalis is probably due to the presence of protein product of lsa (lincosamide and streptogramin A resistance) gene, i.e., ATP-binding cassette (ABC)-efflux pumps, i.e., ABC-23 (Singh et al. 2002). Similarly, putative ABC transporter was identified in all E. faecium isolates that result in resistance to erythromycin, and chloramphenicol resistance has been linked to efflux of the antibiotic out of the cell (Aakra et al. 2010).
Enterococcus spp. are known to acquire resistance to various antibiotics such as vancomycin, chloramphenicol, erythromycin, and fluoroquinolones and high-level resistance to aminoglycosides and penicillin. Acquired antibiotic resistance in a pathogen is due to either of the two mechanisms, i.e., either by mutation of the gene or by horizontal transfer of antibiotic resistance genes. However, in Enterococcus antibiotic resistance problem mainly stems from horizontal gene transfer. Enterococci exist in complex microbial environments where they come in contact with large diversity of genetic material, and in the presence of antibiotic pressure, they tend to acquire resistance to antibiotics. For example, there is a direct relationship between exposure to parenteral antibiotics, especially cephalosporins, antibiotics for anaerobes, and high-level gastrointestinal colonization by ampicillin-resistant E. faecium (Rice et al. 2004).
Enterococci were recognized as important agents of MDR nosocomial infections after vancomycin resistance was observed. In the USA, 87% E. faecium and 14% E. faecalis isolated from nosocomial infections are vancomycin resistant (Edelsberg et al. 2014). Vancomycin acts by binding to D-alanine-D-alanine moiety of peptide chain of peptidoglycans, thus preventing cross-linking of peptidoglycans. Enterococcus strains become resistant to vancomycin by altering peptidoglycan precursors from d-alanine-d-alanine to d-Ala-d-lactate or to d-Ala-d-serine. Nine gene clusters involved in vancomycin resistance are vanA, vanB, vanD, and vanM (Xu et al. 2010) leading to the formation of d-Ala-d-Lac and vanC, vanE, vanG, vanL, and vanN catalyzing d-Ala-d-Ser formation (Boyd et al. 2008; Lebreton et al. 2011). VanA and vanB are the most relevant vancomycin-resistant determinants and are located on transposons (Courvalin 2006). In the 1970s Enterococcus acquired high level of resistance against ampicillin due to specific mutations in pbp genes, which encode for penicillin-binding proteins (Galloway-Peña et al. 2011).
12 Conclusion
The emerging problem of hospital-associated Enterococcal infections appears to be man-made due to injudicious use of antibiotics especially for non-therapeutic purposes such as avoparcin which was employed as growth promoter in the animal feed for the first time in 1975. The overuse of avoparcin led to avoparcin resistance in the gut flora of animals. The avoparcin-resistant gut flora showed cross-resistance toward vancomycin (Mudd 2000). Thus, the first VRE was isolated from the gut flora of farm animals in the 1990s. Subsequently, the use of avoparcin was banned (Casewell et al. 2003) It is hypothesized that the VRE from farm animals were acquired by humans. This is a classic case that highlights the serious repercussions of overuse of antibiotics both for therapeutic and non-therapeutic purposes. To treat Enterococcal infections, antibiotics should be selected wisely based on various factors such as the age, immunocompromised status, type and location of infection, and antibiotic sensitivity spectrum of the Enterococcal pathogen. Further, general measures to prevent the spread of Enterococcus in the hospital settings should be strictly followed such as sanitization of hospital environment and equipments.
References
Aakra A, Vebø H, Indahl U, Snipen L, Gjerstad O, Lunde M et al (2010) The response of Enterococcus faecalis V583 to chloramphenicol treatment. Int J Microbiol 2010:483048. https://doi.org/10.1155/2010/483048
Aslangul E, Massias L, Meulemans A, Chau F, Andremont A, Courvalin P et al (2006) Acquired gentamicin resistance by permeability impairment in Enterococcus faecalis. Antimicrob Agents Chemother 50:3615–3621
Billington EO, Phang SH, Gregson DB, Pitout JD, Ross T, Church DL et al (2014) Incidence, risk factors, and outcomes for Enterococcus spp. blood stream infections: a population-based study. Int J Infect Dis 26:76–82
Bonilla HF, Zervos MA, Lyons MJ, Bradley SF, Hedderwick SA, Ramsey MA et al (1997) Colonization with vancomycin-resistant Enterococcus faecium: comparison of a long-term-care unit with an acute-care hospital. Infect Control Hosp Epidemiol 18:333–339
Boyd DA, Willey BM, Fawcett D, Gillani N, Mulvey MR (2008) Molecular characterization of enterococcus faecalis N06-0364 with low-level vancomycin resistance harboring a novel D-Ala-D-Ser gene cluster, vanL. Antimicrob Agents Chemother 52:2667–2672
Brede DA, Snipen LG, Ussery DW, Nederbragt AJ, Nes IF (2011) Complete genome sequence of the commensal Enterococcus faecalis 62, isolated from a healthy Norwegian infant. J Bacteriol 193:2377–2378. https://doi.org/10.1128/JB.00183-11
Casewell M, Friis C, Marco E, McMullin P, Phillips I (2003) The European ban on growth-promoting antibiotics and emerging consequences for human and animal health. J Antimicrob Chemother 52:159–161
Chakraborty A, Pal NK, Sarkar S, Gupta MS (2015) Antibiotic resistance pattern of enterococci isolates from nosocomial infections in a tertiary care hospital in Eastern India. J Natl Sci Biol Med 6(2):394
Chow JW (2000) Aminoglycoside resistance in enterococci. Clin Infect Dis 31(2):586–589
Chow JW, Thal LA, Perri MB, Vazquez JA, Donabedian SM, Clewell DB et al (1993) Plasmid-associated hemolysin and aggregation substance production contribute to virulence in experimental Enterococcal endocarditis. Antimicrob Agents Chemother 37:2474–2477
Clewell DB (1993) Sex pheromones and the plasmid-encoded mating response in enterococcus faecalis. In: Clewell DB (ed) Bacterial conjugation. Springer, Boston
Costa Y, Galimand M, Leclercq R, Duval J, Courvalin P (1993) Characterization of the chromosomal aac (6′)-Ii gene specific for Enterococcus faecium. Antimicrob Agents Chemother 37:1896–1903
Courvalin P (2006) Vancomycin resistance in Gram-positive cocci. Clin Infect Dis 42(Supplement 1):S25–S34
Cox CR, Coburn PS, Gilmore MS (2005) Enterococcal cytolysin: a novel two component peptide system that serves as a bacterial defense against eukaryotic and prokaryotic cells. Curr Protein Pept Sci 6:77–84
Edelsberg J, Weycker D, Barron R, Li X, Wu H, Oster G et al (2014) Prevalence of antibiotic resistance in US hospitals. Diagn Microbiol Infect Dis 78:255–262
Ford CD, Lopansri BK, Haydoura S, Snow G, Dascomb KK, Asch J et al (2015) Frequency, risk factors, and outcomes of vancomycin-resistant Enterococcus colonization and infection in patients with newly diagnosed acute leukemia: different patterns in patients with acute myelogenous and acute lymphoblastic leukemia. Infect Control Hosp Epidemiol 36:47–53
Forrest GN, Arnold RS, Gammie JS, Gilliam BL (2011) Single center experience of a vancomycin resistant Enterococcal endocarditis cohort. J Infect 63:420–428
Galimand M, Schmitt E, Panvert M, Desmolaize B, Douthwaite S, Mechulam Y et al (2011) Intrinsic resistance to aminoglycosides in Enterococcus faecium is conferred by the 16S rRNA m5C1404-specific methyltransferase EfmM. RNA 17:251–262
Galloway-Pena JR, Rice LB, Murray BE (2011) Analysis of PBP5 of early US isolates of Enterococcus faecium: sequence variation alone does not explain increasing ampicillin resistance over time. Antimicrob Agents Chemother 55:3272–3277
Gilmore MS, Lebreton F, van Schaik W (2013) Genomic transition of enterococci from gut commensals to leading causes of multidrug-resistant hospital infection in the antibiotic era. Curr Opin Microbiol 16:10–16
Gray J, Marsh PJ, Stewart D, Pedler SJ (1994) Enterococcal bacteraemia: a prospective study of 125 episodes. J Hosp Infect 27:179–186
Hayden MK (2000) Insights into the epidemiology and control of infection with vancomycin-resistant enterococci. Clin Infect Dis 31:1058–1065
Heikens E, Singh KV, Jacques-Palaz KD, van Luit-Asbroek M, Oostdijk EA, Bonten MJ et al (2001) Contribution of the Enterococcal surface protein Esp to pathogenesis of Enterococcus faecium endocarditis. Microbes Infect 13:1185–1190
Heikens E, Bonten MJ, Willems RJ (2007) Enterococcal surface protein Esp is important for biofilm formation of Enterococcus faecium E1162. J Bacteriol 189:8233–8240
Heintz BH, Halilovic J, Christensen CL (2010) Vancomycin-resistant Enterococcal urinary tract infections. Pharmacother: J Hum Pharmacol Drug Ther 30:1136–1149
Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, Pollock DA et al (2008) NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect Control Hosp Epidemiol 29:996–1011
Hota B (2004) Contamination, disinfection, and cross-colonization: are hospital surfaces reservoirs for nosocomial infection? Clin Infect Dis 39:1182–1189
Ike Y, Clewell DB, Segarra RA, Gilmore MS (1990) Genetic analysis of the pAD1 hemolysin/bacteriocin determinant in Enterococcus faecalis: Tn917 insertional mutagenesis and cloning. J Bacteriol 172:155–163
Karmarkar MG, Gershom ES, Mehta PR (2004) Enterococcal infections with special reference to phenotypic characterization & drug resistance. Indian J Med Res 119:22–25
Kramer A, Schwebke I, Kampf G (2006) How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis 6:130
Kreft B, Marre R, Schramm U, Wirth R (1992) Aggregation substance of Enterococcus faecalis mediates adhesion to cultured renal tubular cells. Infect Immun 60:25–30
Landman D, Quale JM (1997) Management of infections due to resistant enterococci: a review of therapeutic options. J Antimicrob Chemother 40:161–170
Lautenbach E, Bilker WB, Brennan PJ (1999) Enterococcal bacteremia: risk factors for vancomycin resistance and predictors of mortality. Infect Control Hosp Epidemiol 20:318–323
Leavis HL, Willems RJ, Van Wamel WJ, Schuren FH, Caspers MP, Bonten MJ (2007) Insertion sequence-driven diversification creates a globally dispersed emerging multiresistant subspecies of E. faecium. PLoS Pathog 26(3):e7
Lebreton F, Depardieu F, Bourdon N, Fines-Guyon M, Berger P, Camiade S et al (2011) D-Ala-D-Ser VanN-type transferable vancomycin resistance in Enterococcus faecium. Antimicrob Agents Chemother 55:4606–4612
MacCallum WG, Hastings TW (1899) A case of acute endocarditis caused by Micrococcus zymogenes (nov. spec.), with a description of the microorganism. J Exp Med 4:521–534
Maki DG, Agger WA (1988) Enterococcal bacteremia: clinical features, the risk of endocarditis, and management. Medicine 67:248
McDonald JR, Olaison L, Anderson DJ, Hoen B, Miro JM, Eykyn S et al (2005) Enterococcal endocarditis: 107 cases from the international collaboration on endocarditis merged database. Am J Med 118:759–766
McKenzie FE (2006) Case mortality in polymicrobial bloodstream infections. J Clin Epidemiol 59:760–761
Menichetti F, Sganga G (2009) Definition and classification of intra-abdominal infections. J Chemother 21:3–4
Miller WR, Munita JM, Arias CA (2014) Mechanisms of antibiotic resistance in enterococci. Expert Rev Anti-Infect Ther 12:1221–1236
Mudd AJ (2000) Vancomycin-resistant enterococci and use of avoparcin in animal feed: is there a link? Med J Aust 172:458–459
Mundt JO (1961) Occurrence of enterococci: bud, blossom, and soil studies. Appl Microbiol 9:541–544
Mundt JO (1963) Occurrence of enterococci on plants in a wild environment. Appl Microbiol 1:141–144
Mundy LM, Sahm DF, Gilmore MS (2000) Relationships between Enterococcal virulence and antimicrobial resistance. Clin Microbiol Rev 13:513–522
Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG Jr, Bayer AS et al (2009) Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the international collaboration on endocarditis-prospective cohort study. JAMA Intern Med 169:463–473
Murray BE (1990) The life and times of the Enterococcus. Clin Microbiol Rev 3:46–65
Murray BE (1998) Diversity among multidrug-resistant enterococci. Emerg Infect Dis 4:37
Nallapareddy SR, Murray BE (2008) Role played by serum, a biological cue, in the adherence of Enterococcus faecalis to extracellular matrix proteins, collagen, fibrinogen, and fibronectin. J Infect Dis 197:1728–1736
Nallapareddy SR, Weinstock GM, Murray BE (2003) Clinical isolates of Enterococcus faecium exhibit strain-specific collagen binding mediated by Acm, a new member of the MSCRAMM family. Mol Microbiol 47:1733–1747
Nallapareddy SR, Singh KV, Murray BE (2008) Contribution of the collagen adhesin Acm to pathogenesis of Enterococcus faecium in experimental endocarditis. Infect Immun 76:4120–4128
Nallapareddy SR, Sillanpää J, Mitchell J, Singh KV, Chowdhury SA, Weinstock GM et al (2011a) Conservation of Ebp-type pilus genes among enterococci and demonstration of their role in adherence of Enterococcus faecalis to human platelets. Infect Immun 79:2911–2920
Nallapareddy SR, Singh KV, Sillanpää J, Zhao M, Murray BE (2011b) Relative contributions of Ebp pili and the collagen adhesin ace to host extracellular matrix protein adherence and experimental urinary tract infection by Enterococcus faecalis OG1RF. Infect Immun 79:2901–2910
Nielsen HV, Guiton PS, Kline KA, Port GC, Pinkner JS, Neiers F et al (2012) The metal ion-dependent adhesion site motif of the Enterococcus faecalis EbpA pilin mediates pilus function in catheter-associated urinary tract infection. MBio 3:e00177-12. https://doi.org/10.1128/mBio.00177-12
Niven CF Jr, Sherman JM (1944) Nutrition of the enterococci. J Bacteriol 47:335–342
Noskin GA, Peterson LR, Warren JR (1995) Enterococcus faecium and Enterococcus faecalis bacteremia: acquisition and outcome. Clin Infect Dis 20:296–301
Olmested S, Dunny G, Erlandsen S, Wells C (1994) A plasmid encoded surface protein on Enterococcus faecalis augments its internalization by cultured intestinal epithelial cells. J Infect Dis 170:1549–1556
Palmer KL, Gilmore MS (2010) Multidrug-resistant enterococci lack CRISPR-cas. MBio 29(1):e00227–e00210
Park SY, Shin YP, Kim CH, Park HJ, Seong YS, Kim BS et al (2008) Immune evasion of Enterococcus faecalis by an extracellular gelatinase that cleaves C3 and iC3b. J Immunol 181:6328–6336
Paulsen IT (2003) Role of mobile DNA in the evolution of vancomycin-resistant enterococcus faecalis. Science 299(5615):2071–2074
Pericás J, Zboromyrska Y, Cervera C, Castañeda X, Almela M, Garcia-De-La-Maria C et al (2015) Enterococcal endocarditis revisited. Future Microbiol 10:1215–1240
Qin X, Singh KV, Weinstock GM, Murray BE (2000) Effects of Enterococcus faecalis fsr genes on production of gelatinase and a serine protease and virulence. Infect Immun 68:2579–2586
Qin X, Galloway-Peña JR, Sillanpaa J, Roh JH, Nallapareddy SR, Chowdhury S et al (2012) Complete genome sequence of Enterococcus faecium strain TX16 and comparative genomic analysis of Enterococcus faecium genomes. BMC Microbiol 12:135
Rice LB, Calderwood SB, Eliopoulos GM, Farber BF, Karchmer AW (1991) Enterococal endocarditis: a comparison of prosthetic and native valve disease. Rev Infect Dis 13:1–7
Rice LB, Lakticová V, Helfand MS, Hutton-Thomas R (2004) In vitro anti Enterococcal activity explains associations between exposures to antimicrobial agents and risk of colonization by multi resistant enterococci. J Infect Dis 190:2162–2166
Rich RL, Kreikemeyer B, Owens RT, LaBrenz S, Narayana SV, Weinstock GM et al (1999) Ace is a collagen-binding MSCRAMM from Enterococcus faecalis. J Biol Chem 274:26939–26945
Sartelli M, Catena F, Ansaloni L, Coccolini F, Corbella D, Moore EE et al (2014) Complicated intra-abdominal infections worldwide: the definitive data of the CIAOW study. World J Emerg Surg 9:37
Schleifer KH, Kilpper-Bälz R (1984) Transfer of Streptococcus faecalis and Streptococcus faecium to the genus Enterococcus nom. rev. as Enterococcus faecalis comb. nov. and Enterococcus faecium comb. nov. Int J Syst Evol Microbiol 34:31–34
Schlievert PM, Gahr PJ, Assimacopoulos AP, Dinges MM, Stoehr JA, Harmala JW et al (1998) Aggregation and binding substances enhance pathogenicity in rabbit models of Enterococcus faecalis endocarditis. Infect Immun 66:218–223
Shankar N, Lockatell CV, Baghdayan AS, Drachenberg C, Gilmore MS, Johnson DE (2001) Role of Enterococcus faecalis surface protein Esp in the pathogenesis of ascending urinary tract infection. Infect Immun 69:4366–4372
Sherman JM (1937) The streptococci. Bacteriol Rev 1:3–97
Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J, Srinivasan A et al (2013) Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect Control Hosp Epidemiol 34:1–14
Sifaoui F, Arthur M, Rice L, Gutmann L (2001) Role of penicillin-binding protein 5 in expression of ampicillin resistance and peptidoglycan structure in Enterococcus faecium. Antimicrob Agents Chemother 45:2594–2597
Sillanpää J, Chang C, Singh KV, Montealegre MC, Nallapareddy SR, Harvey BR et al (2013) Contribution of individual Ebp pilus subunits of Enterococcus faecalis OG1RF to pilus biogenesis, biofilm formation and urinary tract infection. PLoS One 8(7):e68813. https://doi.org/10.1371/journal.pone.0068813
Silva N, Igrejas G, Gonçalves A, Poeta P (2012) Commensal gut bacteria: distribution of Enterococcus species and prevalence of Escherichia coli phylogenetic groups in animals and humans in Portugal. Ann Microbiol 62:449–459
Singh KV, Weinstock GM, Murray BE (2002) An Enterococcus faecalis ABC homologue (Lsa) is required for the resistance of this species to clindamycin and quinupristin-dalfopristin. Antimicrob Agents Chemother 46:1845–1850
Singh KV, Nallapareddy SR, Sillanpää J, Murray BE (2010) Importance of the collagen adhesin ace in pathogenesis and protection against Enterococcus faecalis experimental endocarditis. PLoS Pathog 6(1):e1000716. https://doi.org/10.1371/journal.ppat.1000716
Sreeja S, Babu PRS, Prathab AG (2012) The prevalence and the characterization of the Enterococcus species from various clinical samples in a tertiary care hospital. J Clin Diagn Res 6:1486–1488
Stevens MP, Edmond MB (2005) Endocarditis due to vancomycin resistant enterococci: case report and review of the literature. Clin Infect Dis 41:1134–1142
Szeto CC, Kwan BC, Chow KM, Law MC, Pang WF, Chung KY et al (2009) Recurrent and relapsing peritonitis: causative organisms and response to treatment. Am J Kidney Dis 54:702–710
Thomas VC, Hiromasa Y, Harms N, Thurlow L, Tomich J, Hancock LE (2009) A fratricidal mechanism is responsible for eDNA release and contributes to biofilm development of Enterococcus faecalis. Mol Microbiol 72:1022–1036
Tornieporth NG, Roberts RB, John J, Hafner A, Riley LW (1996) Risk factors associated with vancomycin-resistant Enterococcus faecium infection or colonization in 145 matched case patients and control patients. Clin Infect Dis 23:767–772
Vijayvargiya R, Veis JH (1996) Antibiotic-resistant endocarditis in a hemodialysis patient. J Am Soc Nephrol 7:536–542
Waters CM, Hirt H, McCormick JK, Schlievert PM, Wells CL, Dunny GM (2004) An amino-terminal domain of Enterococcus faecalis aggregation substance is required for aggregation, bacterial internalization by epithelial cells and binding to lipoteichoic acid. Mol Microbiol 52:1159–1171
Woodford N, Soltani M, Hardy KJ (2001) Frequency of esp in Enterococcus faecium isolates. Lancet 358:584. https://doi.org/10.1016/S0140-6736(01)05726-9
Xu X, Lin D, Yan G, Ye X, Wu S, Guo Y et al (2010) vanM, a new glycopeptide resistance gene cluster found in Enterococcus faecium. Antimicrob Agents Chemother 54:4643–4647
Zarb P, Coignard B, Griskeviciene J, Muller A, Vankerckhoven V, Weist K et al (2012) The European Centre for Disease Prevention and Control (ECDC) pilot point prevalence survey of healthcare-associated infections and antimicrobial use. Euro Surveill 17:20316
Acknowledgment
This work was supported by research grant (grant number, 42-478/2013 SR) sponsored by the University Grants Commission (UGC), New Delhi, India. Ms. Preeti Sharma is thankful to the University of Potential for Excellence scheme of UGC for the fellowship. Ms. Sumanpreet Kaur is thankful to UGC for the fellowship.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Sharma, P., Kaur, S., Kaur, S. (2018). Enterococci As Nosocomial Pathogen. In: Singh, P. (eds) Infectious Diseases and Your Health. Springer, Singapore. https://doi.org/10.1007/978-981-13-1577-0_15
Download citation
DOI: https://doi.org/10.1007/978-981-13-1577-0_15
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-1576-3
Online ISBN: 978-981-13-1577-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)