
Abstract
The purpose of this study was to investigate the effects of a concurrent, strength, and endurance training program on metabolic syndrome risk factors among obese females. Fifty-two obese females (mean ± SD: age 22.71 ± 1.53 years; body mass index 33.96 ± 3.36 kg m−2) were randomly assigned into four groups (n = 13; concurrent (CE), endurance exercise (EE), resistance exercise (RE) programs, and control (C). All the intervention groups completed an 8-week intervention period that consisted of either an endurance exercise (EE: aerobic exercise intensity level started at 40% of training heart rate at week 1 and increased to 60% of training heart rate at week 8), resistance exercise (six to eight resistance exercises using machine at 50–70% of predicted 1RM), or concurrent exercise (CE: 25-min running plus six to eight resistance exercises at 50–70% of predicted 1RM). Resistance exercise was focused on upper body, lower body, and abdominal muscles. Before and after the intervention, subjects completed an incremental treadmill run and maximal isometric strength tests. The baseline values for waist circumference, TRI, HDL, fasting blood glucose, and blood pressure were identical in all groups. Significant interaction (time x intervention) were found in WC, systolic blood pressure, and blood glucose, but not in TRI and HDL. However, no significant differences were found between the groups in all outcome measures. The results suggest no significant difference in benefits of an 8-week of endurance, resistance and concurrent exercises on WC, TRI, HDL, fasting blood glucose, and blood pressure among obese female adults maybe because of an insufficient sample size or a short intervention period.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Obesity is generally associated with excessive body weight which is caused from excessive fat in the body due to an imbalance between energy intake and energy expenditure. Metabolic syndrome (MetS) is a group of risk factors which increases the heart disease and health problems. The five risk factors are large waist circumference (WC), high triglyceride (TRI) and low high-density lipoprotein (HDL) levels, high fasting blood sugar, and blood pressure (BP). Metabolic syndrome is becoming very common due to an increase in obesity rate in adults. Having metabolic syndrome will increase the risk of developing cardiovascular disease and diabetes. Presence of 3–5 risk factors constitutes the diagnosis of metabolic syndrome [1]. Malaysia has been noted to have a high prevalence of MetS when compared to other Asian countries [2].
Prevalence of metabolic syndrome are more evident in women as compared to men [3]. Evidences have shown that in most cases of obesity are more related to low energy expenditure. Weight training or resistance exercise shows many advantages, which is a powerful stimulus to increase mass, strength, muscular power and helps to preserve the integrity the musculature.
Literatures have shown that resistance training is a safe training method and significantly help to improve body weight, reducing waist circumference, increasing muscular strength and improve physical performance [4, 5]. Endurance exercise helps reduce cardiovascular risk by reducing body weight, improving blood lipid profiles [6]. There is evidence to show that the combined resistance exercise and aerobic activity improve blood lipid profiles better than either exercise performed independently [7]. However, there are evidences showing that combining the exercises may compromise the gains from weight exercise as compared to when conducting it alone due to the interference effect. Concurrent exercise is defined as the integration of endurance and weight training in a periodized exercise regime [8]. The purpose of this study was to evaluate the effect of endurance, resistance, and concurrent training on metabolic risk factors among obese female adults.
2 Method
2.1 Participants
A total of 52 participants who met the inclusion criteria were recruited via advertisement. Participants were adults obese female volunteers aged between 20 and 26 years old and underwent two screening processes. Criteria for inclusion were: females having Body Mass Index (BMI) ranged from 30.0 to 39.9 kg/m2, body fat percentage ranged between 35 and 45%, and free from any chronic diseases (diabetes mellitus, hypertension, any cancer disease, and any of heart diseases and endocrine disorder). Volunteers with musculoskeletal injuries, physically impaired, under medication or drugs or both, and having abnormal menstruation were excluded. Participants were required to pass a Physical Activity Readiness Questionnaire (PAR-Q), health status examination and ECG tests prior to participation. Participants gave their consent upon arriving at the lab. The study was approved by UiTM Ethics Committee in accordance to the Helsinki Declaration.
Participants were randomly assigned based on age, BMI, body fat percentage, and non-fasting blood glucose into four groups: aerobic exercise (AE), resistance exercise (RE), concurrent exercise (CE), and control. Participants’ characteristics are as shown in Table 4. All participants successfully completed the intervention, and no injuries due to the intervention were reported. Outcome measures were measured for the pre- and post-intervention.
2.2 Intervention
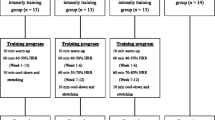
All exercise groups engaged with the exercise program for 8 weeks, 3 times per week, and 1 h per session. Participants warmed up for 5 min prior to exercise and cooled down for 5 min after the conditioning phase. Earlier, participants were taught to perform carotid palpation to measure their resting heart rate upon wake up from sleep in the morning. Carotid palpation was used to calculate the training heart rate for aerobic exercise group.
Aerobic exercise (AE)—The prescribed aerobic exercise intensity level started at 40% of the training heart rate at week 1 and increased to 60% of training heart rate at week 8 of the intervention. Aerobic exercise phase began with a brisk walk to slow jog (Table 1).
Resistance exercise (RE)—Resistance exercise group were asked to perform six to eight resistance exercises using machine at 50–70% of predicted one repetition maximum (1-RM) with rest interval between 1 and 2 min between set [9]. The exercises were focused on upper body, lower body and abdominal muscles (Table 2).
Concurrent exercise (CE)—For concurrent exercise group, the participants had to perform aerobic exercise for 25 min followed by resistance exercise in one session at the same intensity with aerobic and resistance exercise. Participants in concurrent group were trained half of the volume of resistance exercise (Table 3).
-
Control
The control group did not follow any exercise program but maintained a normal daily activity throughout the exercise duration.
Participants were advised to maintain to their normal diet throughout the exercise program. Three days food record was collected from the participants to ensure they were keeping to the normal diet.
2.3 Outcome Measures
-
Anthropometry measurements
Height and weight were measured using stadiometer and weighing machine (Tanita). Body mass index is calculated using mass formula (kg) divided by height × height (m2).
-
Waist circumference
WC was measured at the end of several consecutive natural breaths, at the level parallel to the floor, midpoint between the top of the iliac crest and the lower margin of the last palpable rib in midaxillary line [10]. The data were analyzed using cutoffs points for Caucasians and Asians (80 cm in women) [11].
-
Triglyceride and high-density lipoprotein
Venous blood samples were taken by a doctor and analyzed for lipid profile and fasting glucose. Triglycerides were measured based on an enzymatic procedure. The Abell–Kendall method was used to measure high-density lipoprotein.
-
Fasting blood sugar
Fasting serum glucose was assayed enzymatically by using the VISTA kit analyzer (SIEMENS, USA). The process involves in sampling the blood specimens, reagent delivery, mixing procedures, and chemical processing were automatically performed by Dimension Vista software operating system (2008).
-
Blood pressure
This systolic and diastolic blood pressure measurement was using manual desk mercury sphygmomanometer. The measurement was taken at the left arm after participants sit at backrest chair for 10 min. The values of systolic and diastolic were recorded in mmHg. Reliability for systolic was reported at r = .89 and diastolic was reported at r = .83 [12].
2.4 Data Analysis
This study utilized a mixed within-between subjects analysis of variance (ANOVA) to determine the significant interaction and main effects of the interventions on the outcome measures between pre- and post-intervention. Data are reported as mean ± SD. The statistical significance level was set at 0.05. Statistical Package for Social Science version 21.0 was used to analyze the data. Tukey’s post hoc test was further used to determine the differences.
3 Results and Discussion
3.1 Participants’ Characteristics
Participants were not significantly different in age, weight, height, WC, TRI, HDL, and blood glucose at baseline. Table 4 shows the participants’ characteristics.
3.2 Effects of Intervention on WC
Significant interaction between intervention type and time was found for WC, Wilks’ Lambda = .597, F (3, 48) = 10.81, p < .05, partial eta squared = .043, with all groups showing reduction in WC. The main effect for time, Wilks’ Lamda = .615, F (1, 48) = 30.02, p < .05, partial eta squared = .385, with three groups showing reduction in WC across two observations. The main effect comparing the types of training was not significant, F (1, 48) = 1.669, p = .186, partial eta squared = .094, suggesting no difference in the effectiveness of the three interventions.
This study supported earlier findings [13] which indicate that all types of exercise induce positive changes to WC, in which high WC measurement is a risk factor of metabolic syndrome which leads to cardiovascular disease [14]. Most of the studies which reported the changes were mostly conducted at a longer duration (12 weeks), while in the present study, it was conducted only in 8 weeks.
3.3 Effects of Intervention on TRI and HDL
No significant interaction between intervention (aerobic, resistance, concurrent, and control) and time on TRI, Wilks’ Lambda = .957, F (3, 48) = 1.481, p = .231, partial eta squared = .085. There was no main effect for time, Wilks’ Lambda = .925, F (1, 48) = 3.893, p = .054, partial eta squared = .075. The main effect when comparing the types of training also showed no significant difference, F (3, 48) = .714, p = .548, partial eta squared = .048, which suggests no difference in the effectiveness of all interventions in triglycerides.
A significant interaction between interventions (aerobic, resistance, concurrent, and control) and time in HDL is noted, Wilks’ Lambda = .844, F (3, 48) = 2.956, p = .042, partial eta squared = .156. There was no main effect for time, Wilks’ Lambda = .975, F (1, 48) = 1.236, p = .272, partial eta squared = .025. The main effect when comparing the types of training showed no significant difference, F (3, 48) = .644, p = .591, partial eta squared = .039, which suggests no difference in the effectiveness of all interventions in high density lipoprotein.
Although some studies have shown improvement in TRI and HDL following 8 weeks of concurrent and endurance training [15], this study however did not show any improvement in TRI and HDL, but changes in body weight and fat mass were found. This is probably due to the difference in the exercise intensity and volume which did not exert any changes in the activities of some lipid-regulating enzymes [16]. For future study, it is suggested that to determine the adequate volume and intensity, cortisol level is to be measured.
3.4 Effects of Intervention on Fasting Blood Glucose
No significant interaction were found between training types and time in blood glucose, Wilks Lamda = .854, F (3, 48) = 2.739, p = .054, partial eta squared = .146. A substantial main effect for time, Wilks Lamda = .888, F (1, 48) = 6.051, p = .018, partial eta squared = .112, with all intervention groups shows reduction in blood glucose. The main effect when comparing the three interventions showed no significant difference, F (3, 48) = .865, p = .466, partial eta squared = .051, which indicates no difference in the effectiveness of all interventions in blood glucose level.
This study supported earlier study [16] which indicated improvement in blood glucose among obese nondiabetic subjects following endurance and concurrent training. This finding is further supported by improvement in WC. Improvement in blood glucose is associated with improved in insulin sensitivity [16].
3.5 Effects of Intervention on Resting Blood Pressure
Significant interaction between interventions and time were noted, Wilks’ Lambda = .851, F (3, 48) = 2.805, p = .050, partial eta squared = .149. There was substantial main effect for time, Wilks’ Lambda = .756, F (1, 48) = 15.487, p = .000, partial eta squared = .244. The aerobic, resistance, and concurrent groups showed a reduction in systolic blood pressure, but an increment of systolic blood pressure is shown in the control group. However, the main effect when comparing aerobic, resistance, concurrent, and control groups showed no significant difference, F (3, 48) = 1.821, p = .156, partial eta squared = .102, which suggests that there is no difference in the effective of all interventions in reducing systolic blood pressure.
Several studies have shown the improvement in systolic blood following endurance, resistance, and concurrent training [17]. The reduction in systolic blood pressure is probably due to the reduction in peripheral vascular resistance [18], alteration of sympathetic nervous system function and vasculature responsiveness, and baroreflex action in lowering the blood pressure [18].
No significant interaction between and time on diastolic pressure was found, Pillai’s Trace = .028, F (3, 48) = .460, p = .711, partial eta squared = .028. No main effect for time, Pillai’s Trace = .024, F (1, 48) = 1.181, p = .283, partial eta squared =.024. In addition, the main effect when comparing aerobic, resistance, concurrent, and control groups showed no significant difference, F (3, 48) = .281, p =.839, partial eta squared = .017, which suggests that there is no difference in the effectiveness of all interventions in diastolic blood pressure (Table 5).
4 Conclusion
It can be concluded that these exercise interventions do not show clear superiority and definite adaptations in metabolic risk factors among obese female adults, however, it is proven that exercise intervention do induce positive changes in improving the metabolic risk factors. Further studies are, therefore, necessary to which include a larger sample size, different gender, and a longer intervention period.
References
Alberti, K. G. M. M., Eckel, R. H., Grundy, S. M., Zimmet, P. Z., Cleeman, J. I., Donato, K. A., et al. (2009). Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Taskforce on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity.
Beigh, S. H., & Jain, S. (2012, July). Prevalence of metabolic syndrome and gender differences. Bioinformation, 8(13), 613–616.
Mohamud, W. N., Ismail, A. A., Sharifuddin, A., Ismail, I. S., Musa, K. I., Kadir, N. A., et al. (2011, February). Prevalence of metabolic syndrome and its risk factors in adult Malaysians: Results of a nationwide survey. Diabetes Research and Clinical Practice, 9(2), 239–245.
Jan Mohamed, H. J., Mitra, A. K., Zainuddin, L. R., Leng, S. K., & Wan Muda, W. M. (2013). Women are at a higher risk of metabolic syndrome in rural Malaysia. Women and Health, 53(4), 335–348.
Mekary, R. A., Grøntved, A., Despres, J.-P., De Moura, L. P., Asgarzadeh, M., Willett, W. C., et al. (2015). Weight training, aerobic physical activities, and long-term waist circumference change in men. Obesity, 23, 461–467.
Mann, S., Beedie, C., & Jimeniz, A. (2014). Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: Review, synthesis and recommendations. Sports Medicine, 44, 211–221.
Wescott, W. L. (2012). Resistance training is medicine: Effects of strength training on health. Current Sport Medicine Report, 11(4), 209–216.
Pitsavos, C., Panagiotakos, D. B., Tambalis, K. D., et al. (2009). Resistance exercise plus aerobic activities is associated with better lipids profile among healthy individuals: The ATTIICA study. QJM, 102, 609–616.
Fyfe, J. J., Bishop, D. J., & Stepto, N. K. (2014). Interference between concurrent resistance and endurance exercise: Molecular bases and the role of individual training variables. Sports Medicine, 44(6), 743–762.
Kraemer, W. J., & Ratamess, N. A. (2004). Fundamentals of resistance training: Progression and exercise prescription. Medicine and Science in Sports and Exercise, 36(4), 674–688.
World Health Organization (WHO). (2008). Waist circumference and waist-hip ratio. Report of WHO Expert Consultation. Geneva: World Health Organization.
Beam, W., & Adams, G. (2008). Exercise physiology manual (7th ed.).
Norfazilah Ahmad, A., SamiaI, I. M. A., Azmawati, M. N., Mohd Rohaizat, H., & Hasanain Faisal, G. (2016). Abdominal obesity indicators: Waist circumference or waist-to-hip ratio in Malaysian adults population. International Journal of Preventive Medicine, 7, 82.
Adegbija, O., Hoy, W., & Wang, Z. (2015). Prediction of cardiovascular disease risk using waist circumference among Aboriginals in a remote Australian community. BMC Public Health, 15, 57.
Ali-Mohamadi, M., Abbaspoor, M., Rahimi, R., & Hakimi, M. (2014). The influence of order execution components of the strength and endurance in the concurrent training on lipid profile and body composition in overweight females. World Applied Sciences Journal, 29(7), 946–953.
da Silva Medeiros, N., de Abreu, F. G., Colato, A. S., de Lemos, L. S., Ramis, T. R., Dorneles, G. P., et al. (2015). Effects of concurrent training on oxidative stress and insulin resistance in obese individuals. Oxidative Medicine and Cellular Longevity, 2015.
Dias, I., Farinati, P., De Souza, M. G., Manhanini, D. P., Balthazar, E., Dantas, D. L., et al. (2015, December). Effects of resistance training on obese adolescents. Medicine and Science in Sports and Exercise, 47(12), 2636–2644.
Delavar, S. H., & Faraji, H. (2011). Effect of different concurrent training methods on post-exercise hypotension in borderline hypertensive women. Middle-East Journal of Scientific Research, 9(4), 456–461.
Acknowledgements
The authors would like to express gratitude to all participants participated in this study and staff of Faculty of Sports Science and Recreation, Universiti Teknologi MARA Shah Alam, Selangor for their support.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this paper

Cite this paper
Md. Yusof, S., Mohd Idris, N.I., Aiman, S., Abd Kadir, Z. (2019). Effects of Concurrent, Strength, and Endurance Training on Metabolic Syndrome Risk Factors Among Obese Females. In: Sulaiman, N., Ismail, S., Adnan, R. (eds) Proceedings of the 3rd International Colloquium on Sports Science, Exercise, Engineering and Technology. ICoSSEET 2016. Springer, Singapore. https://doi.org/10.1007/978-981-10-6772-3_4
Download citation
DOI: https://doi.org/10.1007/978-981-10-6772-3_4
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-6771-6
Online ISBN: 978-981-10-6772-3
eBook Packages: EngineeringEngineering (R0)