
Abstract
Oxidative stress is a pathophysiologic mechanisms implicated in various medical conditions. In this chapter, we discuss oxidative stress and key components of the body’s anti-oxidation system. We summarize the evidence supporting the role of oxidative stress in disease, concentrating on various psychiatric disorders. We also describe the molecular pharmacology of N-acetylcysteine (NAC) and explain the role of NAC in decreasing oxidative stress in psychiatric disorders.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Oxidative stress has been postulated as one of the pathophysiologic mechanisms implicated in various medical conditions, including neurologic and psychiatric disorders. In this chapter, we will start with the definition of oxidative stress, sources of cellular oxidative stress, and key components of the anti-oxidation system in the body. Then, we will summarize the evidence supporting the role of oxidative stress in various psychiatric disorders. We will also describe the molecular pharmacology of N-acetylcysteine (NAC), a medication that has been shown to reduce oxidative stress. Finally, we will conclude by explaining the role of NAC in decreasing oxidative stress in psychiatric disorders.
2 Oxidative Stress and the Anti-oxidation System
2.1 Oxidative Stress
Oxidative stress is defined as an imbalance between the levels of prooxidants and antioxidants. This phenomenon is known to result in damage to macromolecules (i.e., proteins and DNA) and activation of redox-sensitive signals. The reactions to macromolecules are generally caused by prooxidant reactive chemicals containing oxygen or nitrogen and are called reactive oxygen species (ROS) and reactive nitrogen species (RNS), respectively.
One main source of ROS is the nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) complexes in cell membranes and other cell organelles including mitochondria, peroxisomes, and endoplasmic reticulum. Mitochondria convert energy for the cell into a usable form, adenosine triphosphate (ATP), by oxidative phosphorylation. This process involves reduction of oxygen to water. However, this process does not occur perfectly all the time. A small percentage of oxidative phosphorylation will reduce the oxygen prematurely and form superoxide radical (O2 −•). The superoxide radical can then initiate lipid peroxidation. The lipid hydroperoxide will then be transformed to lipid radicals, which can further cause damage in cell membranes and even trigger a cascade of events leading to apoptosis. Other examples of ROS include singlet oxygen (1O2), hydroperoxyl radical (HO2 •), hydrogen peroxide (H2O2), hydroxyl radical (HO•), hydroxyl anion (OH−), peroxyl radical (ROO•), lipid peroxyl radical (LOO•), hypochlorous acid (HOCl), hypobromous acid (HOBr), and hypothiocyanous acid (HOSCN) (Moniczewski et al. 2015). In regard to RNS, the key source is nitric oxide (NO•). Other examples of RNS include nitrogen dioxide (NO2 •), peroxynitrite (ONOO−), nitrite (NO2 −), nitrate (NO3 −), and nitronium ion (NO2 +). Nitrite is often used as a marker of NO activity. In addition to endogenous sources, ROS and RNS can also come from exogenous sources such as medications and environmental toxicants.
2.2 Antioxidant Systems in the Body
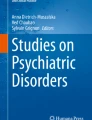
Under normal physiologic conditions, the body can neutralize ROS and RNS by anti-oxidation systems before significant cellular damage occurs. These systems can reverse oxidative damage by supplying electrons to ROS, RNS, proteins, and electrophilic xenobiotics, thereby maintaining redox balance. Superoxide radicals are typically transformed to hydrogen peroxide by superoxide dismutase (SOD). The resulting hydrogen peroxide is then converted to water by either catalase (CAT) or glutathione peroxidase (GPX). The glutathione system is the predominant antioxidant system in our body. Glutathione exists in two forms: reduced glutathione (GSH) and oxidized glutathione (GSSG) (see Fig. 4.1). The biotransformation between the two forms is central to the regulation of redox balance in the brain. The oxidation of GSH to GSSG is catalyzed by GPX, the same enzyme that converts hydrogen peroxide to water. This GSH→GSSG reaction is key in protecting proteins by coupling with the reduction of thiol groups in proteins via glutaredoxins (GRXs). The reduction of GSSG back to GSH is catalyzed by glutathione reductase (GR), which uses NADPH as a cofactor. In addition to the above biochemical functions, GSH plays a key role in neutralizing electrophilic xenobiotic compounds by conjugating to them via glutathione-S-transferases (GSTs). Other endogenous antioxidants include vitamin E and vitamin C, which convert lipid peroxyl radicals to stable vitamin radicals. Collectively, the anti-oxidation system plays a key role in cellular redox homeostasis and has special relevance to pathophysiology of several psychiatric disorders (e.g., schizophrenia and autism) and neurologic diseases (e.g., Alzheimer’s disease and Parkinson’s disease).

Anti-oxidation systems of the body involving glutathione and the role of N-acetylcysteine (NAC) in restoring glutathione
2.3 Biomarkers of Oxidative Stress
The level of oxidative stress can be assessed peripherally by measuring the concentrations of GSH and GSSG using high-performance liquid chromatography (HPLC) and fluorimetric assays and in the central nervous system using proton magnetic resonance spectroscopy (1H MRS). Other common biomarkers of oxidative stress include the enzyme activities of CAT, GPX, and SOD. In addition to oxidative stress, downstream processes such as lipid peroxidation, oxidative protein damage, and oxidative DNA damage can also be monitored. Aconitase activity has been employed as a biomarker of mitochondrial superoxide production. Thiobarbituric acid reactive substances (TBARS) are common biomarkers for lipid peroxidation. 3-nitrotyrosine (3-NT) has been used to assess oxidative protein damage. 8-oxo-deoxyguanosine (8-oxo-dG) is a biomarker of oxidative DNA damage. 3-chlorotyrosine (3-CT) is an established biomarker of a chronic inflammatory response.
2.4 Oxidative Stress in the Developing Brain
Neurons are highly susceptible to oxidative damage due to high levels of ROS and RNS production, relatively low amounts of antioxidant enzymes, the high brain’s lipid content and metabolic rate, and the non-regenerative nature of neurons. Of particular interest is the developing brain that has a high metabolic rate. When low levels of antioxidants and high levels of heavy metal ions are present, ROS levels will become elevated. The developing brain at an early age is sensitive to even small changes to redox balance, which can affect the signaling pathways and processes involved in neurogenesis, neuronal differentiation, and myelination. Therefore, oxidative stress is associated with neuronal injury in the developing brain when subjected to hypoxia, ischemia, and traumatic brain injury. Consequently, these insults may derail brain development and result in neurodevelopmental disorders such as autism spectrum disorder (ASD) and schizophrenia.
3 Oxidative Stress and Psychiatric Disorders
Oxidative stress has been implicated in various psychiatric disorders including ASD, schizophrenia, bipolar disorder, and major depressive disorder (MDD). Here we will summarize the evidence of oxidative stress in these disorders (Table 4.1).
3.1 Oxidative Stress and Autism Spectrum Disorder
3.1.1 Peripheral Biomarkers of Redox Balance in ASD
ASD is characterized by deficits in socio-communicative abilities, stereotypic behaviors, restricted interests, cognitive inflexibility, and sensory aberrations. Like schizophrenia, many investigators in the field of autism have studied oxidative stress. Han et al. reported that GSH levels as well as the GSH/GSSG ratio showed significantly lower values in children with ASD compared to control subjects (Han et al. 2015). Other investigators showed that children with ASD had lower levels of plasma GSH but higher levels of GSSG than typically developing children (Geier et al. 2009; James et al. 2006). Furthermore, homocysteine and GSSG levels were significantly higher in children with ASD (Han et al. 2015). Finally, homocysteine levels were found to correlate positively with Childhood Autism Rating Scale (CARS) scores in children with ASD. The associations between other oxidative stress parameters and ASD have not been consistent. The SOD activity was either increased in erythrocytes (Al-Gadani et al. 2009; Zoroglu et al. 2004) or decreased in plasma and erythrocytes (Meguid et al. 2011; Yorbik et al. 2002). The CAT activity was reduced in erythrocytes (Zoroglu et al. 2004) but unchanged in plasma (Al-Gadani et al. 2009). The GPX activity was reduced in plasma (El-Ansary and Al-Ayadhi 2012; Laszlo et al. 2013) and erythrocytes (Meguid et al. 2011) but increased in plasma (Al-Gadani et al. 2009).
Ghezzo et al. evaluated oxidative stress parameters in children with ASD and neurotypical controls. While some oxidative stress biomarkers including TBARS, urinary isoprostane, and hexanoyl-lysine adduct levels in RBC were found to be elevated in ASD, many others (RBC SOD and CAT activities, urinary 8-oxo-dG, plasma radical absorbance capacity, and carbonyl groups) were not different between the two groups (Ghezzo et al. 2013). Interestingly, Na+/K+-ATPase activity and RBC membrane fluidity were found to be reduced in ASD compared to TD (Ghezzo et al. 2013). Furthermore, fatty acid membrane profile was altered in ASD; children with ASD demonstrated an increase in monounsaturated fatty acids, decrease in eicosapentaenoic acid (EPA), decrease in docosahexaenoic acid (DHA)-ω3, and increase in the ω6/ω3 ratio as compared to controls (Ghezzo et al. 2013).
Existing evidence is not consistent and small sample sizes and effects limit many studies. Frustaci and his colleagues, who completed a recent systematic review and meta-analyses of oxidative stress-related biomarkers in autism, recognized this problem. This meta-analysis showed the children with autism consistently demonstrated decreased blood levels of reduced GSH, GPX, methionine, and cysteine and increased concentrations of GSSG relative to controls across multiple studies, whereas SOD, homocysteine, and cystathionine were not consistently different between ASD and controls across published studies (Frustaci et al. 2012).
Building on the above findings, Frye and his colleagues studied the connection between oxidative stress and mitochondrial dysfunction in children with ASD. Compared to typically developing controls, children with ASD [with or without comorbid mitochondrial disease (MD)] showed lower GSH and GSH/GSSG. Compared to children with ASD only, children with ASD + MD were found to have significantly higher GSH/GSSG and lower levels of GSSG. Furthermore, the authors demonstrated that signs of chronic inflammation were present in both groups of children with ASD, as evidenced by higher levels of 3-chlorotyrosine (3-CT). Finally, children with ASD + MD were found to have lower scores on the daily living skill and communication subscales of the Vineland Adaptive Behavior Scale (VABS) despite having similar language and ASD symptoms. This study suggested that different subgroups of children with ASD have different abnormalities in their redox balance, which may arise from different etiologies.
3.1.2 Evaluation of Brain GSH Levels in Individuals with ASD by 1H MRS
Using 1H MRS, no difference in brain GSH was found in either basal ganglia or dorsomedial prefrontal cortex in adults with ASD (Durieux et al. 2016).
3.1.3 Assessing Redox Balance from Postmortem Brain Samples of Individuals with ASD
Using postmortem brain samples of individuals with ASD, central nervous system levels of oxidative stress biomarkers were measured (Rose et al. 2012). Consistent with previous studies on plasma and immune cells, the oxidative stress biomarkers GSH and GSH/GSSG, as measured by HPLC, were significantly decreased in both ASD cerebellum and temporal cortex as compared to controls.
A significant increase in 3-NT, a biomarker of oxidative protein damage, in the cerebellum and temporal cortex was found in ASD (Rose et al. 2012). Similarly, 8-oxo-dG, a biomarker of oxidative DNA damage, was elevated in cerebellar and temporal cortices in individuals with ASD in comparison to controls and was inversely correlated with GSH/GSSG in the cerebellum (Rose et al. 2012). An increase in levels of 3-CT, a biomarker of chronic inflammatory response, in both brain regions was also observed. Finally, the activity of aconitase, a biomarker of mitochondrial superoxide production, was significantly decreased in cerebellar tissue of individuals with ASD cerebellum and was negatively correlated with GSH/GSSG (Rose et al. 2012). Together, these results indicate that decreased GSH/GSSG redox/antioxidant capacity and increased oxidative stress in the brain tissue from individuals with ASD may have functional consequence in terms of a chronic inflammatory response, increased mitochondrial superoxide production, and oxidative protein and DNA damage. Finally, in a similar study, cerebellar tissues from individuals with ASD were examined, and the activities of GSH-related enzymes GPX, GST, GR, and glutamate-cysteine ligase (GCL) were measured (Gu et al. 2013). Compared to that of the control group, the activities of GPX, GST, and GCL were significantly decreased in ASD.
3.1.4 Oxidative Stress and Mitochondrial Dysfunction in ASD
The relationship of oxidative stress and mitochondrial dysfunction was also demonstrated in a subset of individuals with ASD (Rose et al. 2014, 2015). Using lymphoblastoid cell lines (LCLs) derived from children with ASD, Rose et al. reported that this subset of ASD children had an abnormal mitochondrial reserve capacity before and after exposure to ROS. LCLs from a subset of children with ASD displayed high reserve capacity at baseline but a precipitous drop in reserve capacity when challenged with ROS. In a recent study, this group demonstrated that this metabolic phenotype was related to worse repetitive and stereotyped behaviors (Rose et al. 2017). Interestingly, in this ASD LCL subgroup, pretreatment with NAC prevented this sharp decline of anti-oxidation reserve capacity and improved GSH metabolism, suggesting a role for altered GSH metabolism associated with this type of mitochondrial dysfunction (Rose et al. 2015). Collectively, these results suggested that a subgroup of children with ASD might have alterations in mitochondrial function, which could cause increased vulnerability to prooxidants.
3.2 Oxidative Stress and Schizophrenia
3.2.1 Peripheral Biomarkers of Redox Balance in Schizophrenia
Schizophrenia is a psychiatric disorder characterized by hallucinations, delusions, and cognitive dysfunction. This disorder has been viewed as a neurodevelopmental disorder due to the known risk factors of early life insult and genetic loading. Redox regulation has been hypothesized as one of the components of a “central hub” in the pathophysiology of schizophrenia (Steullet et al. 2010). Redox dysregulation, NMDA hypofunction, and neuroinflammation were hypothesized as the three components of this hub, which mediates the impairment of microcircuits and macrocircuits, thereby causing aberrations in circuit connectivity and psychopathologic findings in schizophrenia (Steullet et al. 2010). Peripheral (blood and plasma) GSH levels in patients with schizophrenia have been found to be lower than in healthy volunteers (Altuntas et al. 2000; Mico et al. 2011; Raffa et al. 2009, 2011). Further, blood GSSG concentrations were found to be higher in patients with schizophrenia (Raffa et al. 2009, 2011). GSH levels correlated positively with the Scale for the Assessment of Positive Symptoms (SAPS) (Raffa et al. 2011).
In addition to GSH and GSSG levels, the disorder was found to be associated with aberrations in other oxidative stress parameters based on a recent meta-analysis of oxidative stress of 44 studies involving individuals with schizophrenia (Flatow et al. 2013). Compared to control subjects, serum or plasma total antioxidant status (TAS) levels were significantly lower in patients who underwent first episodes of psychosis (FEP). However, TAS levels were found to be significantly higher in patients who have been treated with antipsychotic medications after acute exacerbations of psychosis. Similarly, cross-sectional studies revealed that red blood cell (RBC) CAT and plasma nitrite were significantly decreased in FEP and significantly increased in stable outpatients. Based on these results, the authors concluded that plasma or serum TAS, plasma nitrite, and RBC CAT were state-related biomarker of oxidative stress in individuals with schizophrenia. In contrast, compared to control subjects, RBC SOD was found to be lower in FEP, acutely relapsed inpatients, and stable outpatients, and therefore, SOD appeared to be a trait-related biomarker for schizophrenia. Collectively, these findings supported that abnormalities in oxidative stress in FEP might be independent of antipsychotic medications.
One genetic factor that has been reported to influence GSH concentrations in the systemic circulation is the GAG trinucleotide repeat (TNR) polymorphism in the gene coding for the catalytic subunit of glutamate-cysteine ligase (GCL), the rate-limiting enzyme for GSH synthesis. Importantly, polymorphism of this catalytic subunit of GCL (GCLC) was associated with schizophrenia in two case-control studies. As compared with GCLC low-risk genotypes, GCLC high-risk genotypes were more frequent in patients with schizophrenia and were associated with lower GCLC protein expression, GCL activity, and GSH levels in fibroblasts when challenged with oxidative stress conditions. In their recent studies in patients with early psychosis, Xin et al. found that glutamate concentrations in the mPFC as measured by MRS were lower in patients with low-risk GCLC genotypes, but this was not the case for patients with high-risk genotypes (Xin et al. 2016). Furthermore, the authors revealed that the GSH levels in the mPFC, as measured by 1H MRS, correlated negatively with GPX levels in RBC in patients with schizophrenia. In contrast to individuals with early psychosis, GSH levels in the mPFC of healthy volunteers correlated positively with GPX levels in RBC (Xin et al. 2016).
3.2.2 Evaluation of Brain GSH Levels in Individuals with Schizophrenia by 1H MRS
Regarding GSH levels in the brain, Do and her colleagues found that the GSH concentrations in cerebrospinal fluid (CSF) of inpatients with schizophrenia or schizophreniform disorder were lower than those of age- and gender-matched healthy controls (Do et al. 2000). They examined the prefrontal cortex (PFC) of these participants by proton magnetic resonance spectroscopy (1H MRS), which revealed the GSH levels in the PFC to be lower in patients with schizophrenia than healthy volunteers (Do et al. 2000). This finding was replicated by 1H MRS of the frontal cortex in patients with schizophrenia (Matsuzawa and Hashimoto 2011).
Despite the consistent findings of reduced GSH in the frontal cortex, decreased GSH levels were not found in other areas of the brain. For example, a 1H MRS study detected no changes in GSH levels in the anterior cingulate (Terpstra et al. 2005) and posterior medial frontal cortex (Matsuzawa et al. 2008), whereas GSH concentrations in the medial temporal lobe were increased in patients with their first episode of schizophrenia (Wood et al. 2009). Collectively, these results suggested that perturbation in the GSH levels may be regionally specific in schizophrenia.
3.2.3 Assessing Redox Balance from Postmortem Brain Samples of Individuals with Schizophrenia
According to postmortem studies, the concentrations of GSH in the prefrontal cortex (Gawryluk et al. 2011) and striatum (Yao et al. 2006) of schizophrenic patients were lower than controls. Such decreases were linked with lowered activity of related enzymes, such as GPX, GSH-R, and GSH-S-transferase mu isoform (Gawryluk et al. 2011; Yao et al. 2006). Furthermore, increased oxidation and nitration was also found in the postmortem PFC samples of patients with schizophrenia (Kim et al. 2014).
Among brain cells, oligodendrocytes are known to be highly vulnerable to oxidative stress. Monin and his colleagues investigated the interplay between glutathione and myelin (Monin et al. 2015). In control subjects, a positive association was found between mPFC GSH levels as assessed by MRS and both fractional anisotropy (FA) and resting-state functional connectivity along the cingulum bundle. In contrast, in early psychosis patients, mPFC GSH levels were correlated only with FA measures. Therefore, redox regulation has a critical role in myelination processes and white matter maturation in the mPFC of patients with schizophrenia.
3.2.4 Oxidative Stress and Other Pathophysiologic Mechanisms of Schizophrenia
On one hand, oxidative stress can cause damage in the cellular machinery for neurotransmission. On the other hand, abnormalities in the neurotransmission system can trigger changes in oxidative stress. For example, hypofunction of the NMDA receptor (NMDAR) can trigger the downregulation of antioxidant genes, leading to ROS generation through the activation of NADPH oxidase (NOX). NMDAR hypofunction can also result in circuit-level disinhibition of cortical networks. These events cause GSH depletion, which in turn can further repress NMDAR activity. Consequently, during brain development, oxidative stress and GSH deficits caused by NMDAR hypofunction can cause cellular impairment of specific neurons including parvalbumin-expressing interneurons (PVIs), leading to excitation-inhibition (E/I) imbalance (Do et al. 2015; Morishita et al. 2015). The E/I imbalance may lead to the alterations in sensory processing, cognition, and behavior in individuals with schizophrenia.
3.3 Oxidative Stress and Bipolar Disorder
3.3.1 Peripheral Biomarkers of Redox Balance in Bipolar Disorder
Bipolar disorder is a mood disorder characterized by discrete episodes of manic and depressive symptoms. The findings on redox status are mixed and are mostly from data obtained from studies of adult individuals with bipolar disorder. Rosa et al. found that bipolar patients had significantly lower plasma levels of GSH and higher levels of GSSG, compared to controls (Rosa et al. 2014). This investigation also revealed a correlation between total GSH levels and age of illness onset, so that lower plasma levels of GSH were associated with later onset of disease, not length of illness. Interestingly, Tuncel et al. however could not replicate the difference in plasma GSH levels between bipolar patients and control subjects (Tuncel et al. 2015). Additionally, the activity of SOD was found to be similar between bipolar patients and healthy volunteers (Tuncel et al. 2015; Tsai and Huang 2015). Serum GPX activity in bipolar patients was found to be significantly lower than that of control subjects and correlated negatively with severity of manic symptoms as measured by the Young Mania Rating Scale (YMRS) (Tsai and Huang 2015). No difference in CAT activity was found between bipolar patients and control subjects. However, serum CAT activity was associated positively with YMRS (Tsai and Huang 2015).
Tuncel et al. also examined other oxidation markers of lipid peroxidation, protein oxidation, and total oxidized guanine species, in adult bipolar patients during manic and euthymic episodes (Tuncel et al. 2015). Significant increase in the level of lipid peroxidation was found in the bipolar disorder manic episode group compared to the control group. Furthermore, the level of total oxidized guanine species was statistically higher in bipolar groups compared to the control group. Tsai and colleagues replicated the increased lipid peroxidation (Tsai and Huang 2015). Serum levels of TBARS in bipolar patients in a manic phase were significantly higher than those of healthy volunteers. Furthermore, these authors found significantly decreased changes in TBARS levels only in bipolar manic patients after treatment, suggesting that TBARS levels might be a state biomarker of oxidative stress in bipolar patients (Tsai and Huang 2015).
Brown et al. conducted a meta-analysis of studies that examined markers of oxidative stress in bipolar patients compared to healthy volunteers (Brown et al. 2014). Bipolar disorder patients were found to have significantly higher markers of lipid peroxidation and DNA/RNA damage, as compared to healthy controls. While the effect size for lipid peroxidation was very high, GPX, SOD, and CAT in bipolar patients were not different from that of healthy volunteers.
The evidence of oxidative stress appears to persist into later life in individuals with bipolar disorder (Andreazza et al. 2015). Andreazza et al. compared the levels of oxidative damage to proteins and lipids in plasma from 110 euthymic older patients with bipolar disorder (mean age, 62 years) and found that these patients showed higher levels of lipid hydroperoxide (LPH) and 4-hydroxynonenal (4-HNE) than age-matched healthy volunteers. However, no significant differences for PC, 3-NT, and 4-HNE were found between the two groups. These results support the persistent effect of oxidative stress in patients with bipolar disorder into later life.
3.3.2 Brain GSH Levels in Individuals with Bipolar Disorder by 1H MRS
GSH levels were assessed in prefrontal (Godlewska et al. 2014), anterior cingulate (Soeiro-de-Souza et al. 2016; Lagopoulos et al. 2013), and occipital (Godlewska et al. 2014) cortices of patients with euthymic bipolar disorder. No difference in GSH levels between bipolar participants and controls was found. Similarly, participants showed no difference from controls in other measured cortical metabolites including GABA, glutamate, and NAA. Although no difference in GSH levels was found in the brain regions studied, lactate levels in the dorsal anterior cingulate cortex were found to be higher in bipolar disorder patients, as compared to healthy controls. Interestingly, lactate and GSH levels in the dorsal anterior cingulate cortex correlated positively in euthymic bipolar patients only (Soeiro-de-Souza et al. 2016). While no alterations of markers of the oxidative system were observed in euthymic individuals with bipolar disorder, it remains to be determined whether abnormalities in this system might be observed during active clinical activities, either manic or depressive.
3.3.3 Assessing Redox Balance from Postmortem Brain Samples of Individuals with Bipolar Disorder
Pathologic studies have also examined the antioxidant system in individuals with bipolar disorder. Andreazza et al. examined the postmortem PFC samples from patients with bipolar disorder and isolated mitochondria, synaptosomes, and myelin (Andreazza et al. 2013). They found decreased complex I subunit levels in bipolar subjects compared with healthy volunteers, but no difference in complex III subunits. Additionally, carbonylation was increased in synaptosomes from the bipolar group, while 3-NT was increased in mitochondria from the bipolar group. These results suggest that mitochondrial proteins in the PFC of bipolar patients are more susceptible to potentially reversible nitrosative damage, while more long-standing oxidative damage occurs to synaptic proteins.
Kim et al. found increased oxidation of dopamine transporter (DAT)-immunoreactive regions and decreased nitration of tyrosine hydroxylase (TH)-immunoreactive regions in the PFC of patients with bipolar disorder (Kim et al. 2014). On the other hand, these authors found increased global levels of oxidation in patients with bipolar disorder. (Kim et al. 2014) These findings suggest alterations in levels of protein oxidation and nitration in DA-rich regions of the prefrontal cortex in patients with bipolar disorder.
3.4 Oxidative Stress and Major Depressive Disorder
3.4.1 Peripheral Biomarkers of Redox Balance in Major Depressive Disorder (MDD)
Major depressive disorder is a psychiatric disorder characterized by discrete episodes of low mood, sadness, and hopelessness accompanied by vegetative symptoms of depression involving alterations of sleep and appetite. Several lines of evidence support that the redox balance in patients with MDD is perturbed. However, findings of oxidative stress parameters are mixed. While various studies revealed that systemic levels of GPX (Ozcan et al. 2004; Kodydkova et al. 2009), CAT (Ozcan et al. 2004; Wei et al. 2009), and SOD (Wei et al. 2009; Selek et al. 2008) were lower in MDD patients than healthy volunteers, opposite results were also published. Some reports indicated the rise of activities of GR (Kodydkova et al. 2009; Andreazza et al. 2009) and GST (Andreazza et al. 2009) in the late stage of MDD, without alteration in GPX activity (Andreazza et al. 2009; Galecki et al. 2009). Higher levels of SOD activities were also found in serum and erythrocytes of patients with MDD (Kodydkova et al. 2009; Khanzode et al. 2003; Sarandol et al. 2007; Bilici et al. 2001).
3.4.2 Evaluation of Brain GSH Levels in Individuals with Major Depressive Disorder by 1H MRS
GSH concentration in the occipital cortex of patients with MDD was determined by 1H MRS (Lapidus et al. 2014; Godlewska et al. 2015). Patients with MDD were found to have lower GSH levels in the occipital cortex than control participants; however, GABA and glutamate levels between MDD patients and controls were similar (Godlewska et al. 2015). Furthermore, the severity of anhedonia was found to correlate negatively with occipital GSH levels (Lapidus et al. 2014). Effects of the selective serotonin reuptake inhibitor, escitalopram, on GSH levels were also examined in one study. After a 6-week escitalopram treatment, brain levels of GSH, GABA, and glutamate in the occipital cortex remained unchanged (Godlewska et al. 2015).
Oxidative stress and depressive symptoms were investigated in one study of older adults at risk for depression (Duffy et al. 2015). Compared to age-matched controls, the elderly “at-risk” individuals had increased GSH levels in the anterior cingulate cortex (ACC). Additionally, the increased GSH levels were associated with greater symptoms of depression and worse cognitive performance.
3.4.3 Assessing Redox Balance from Postmortem Brain Samples of Individuals with MDD
A limited number of studies examined the redox balance in postmortem brain tissue in individuals with MDD. In one study, the concentration of SOD was found to be increased in the prefrontal cortex, but not in the hippocampus in postmortem brain samples of individuals with depression in comparison to controls (Michel et al. 2007).
3.5 Summary
While several investigations have assessed the antioxidant defense system in neuropsychiatric disorders, findings have not been very consistent. Additional studies are warranted to examine large sample sizes in a developmental approach and longitudinally to determine the stability of some of the observations over time and the effect of age and treatment on the abnormalities observed. Using a multimodal approach is also needed where markers of oxidative system are examined peripherally and centrally by innovative imaging methodologies.
4 Pharmacology of N-Acetylcysteine
N-acetylcysteine (NAC) is a well-known antidote against acetaminophen overdose, which works by increasing the concentrations of GSH through supplementation of cysteine. Cysteine can also be oxidized to cystine, which is a substrate for the glutamate-cystine antiporter. In exchange of the cystine taken by the glial cells, the antiporter transports glutamate into the extracellular space. The non-vesicular glutamate released into the extracellular space activates the type 2/3 metabotropic glutamate receptors, which inhibit the release of vesicular glutamate, thereby decreasing glutamatergic neurotransmission.
NAC has been shown to prevent oxidative damage in animal models, such as the Gclm knockout mice which have impaired synthesis of GSH (Cabungcal et al. 2013). Without supplementation of NAC, the redox dysregulation in the Gclm knockout mice was found to cause oxidative stress in the brain. In particular, parvalbumin (PV)-containing GABAergic interneurons, but not GABAergic interneurons containing calbindin or calretinin, were found to be especially vulnerable to oxidative damage. This effect was revealed to persist into adulthood of the Gclm knockout mice and could be prevented with NAC.
5 Role of NAC in Relieving Oxidative Stress in Patient Population
NAC has been tested as adjunctive treatments for patients with ASD (Hardan et al. 2012; Dean et al. 2016), schizophrenia (Berk et al. 2008a; Farokhnia et al. 2013; Lavoie et al. 2008), bipolar disorder (Berk et al. 2008b, 2012), depression (Berk et al. 2014), and other psychiatric disorders. While many of these studies found that NAC resulted in behavioral improvements, only one study had confirmed the mechanism of action of NAC in patient populations (Lavoie et al. 2008). Here we will summarize the evidence for the modulation of the redox system in the brain as demonstrated by clinical trials of NAC.
As discussed above, redox dysregulation and NMDA hypofunction have been demonstrated in patients with schizophrenia. Based on these pathophysiologic mechanisms of schizophrenia, several investigators had conducted randomized, double-blind trials of NAC. Lavoie et al. performed the only study to date that measured the GSH levels in the systemic circulation (Lavoie et al. 2008). After a 6-week treatment of NAC, the mean concentration of GSH in whole blood was 0.89 μmol/mL, which was significantly higher than the mean GSH concentration after placebo treatment (0.81 μmol/mL).
One study has also been completed to examine the effect of NAC on the antioxidant system in mood disorders. Das and her colleagues conducted a multicenter, randomized, double-blind, placebo-controlled study of MDD patients treated with NAC (Das et al. 2013). Participants (n = 76) from one site completed 1H MRS of the ACC at the end of treatment (12 weeks). MR spectra from the ACC yielded absolute concentrations of glutamate (Glu), glutamate+glutamine (Glx), N-acetyl-aspartate (NAA), and myoinositol (mI), but not GSH. Binary logistic regression analysis was performed to determine whether metabolite profiles could predict NAC versus placebo group. While controlling for the severity of depression and gender, the regression model including concentrations of Glx, NAA, and mI resulted in 75% accuracy in predicting group outcome (NAC or placebo). The finding of higher Glx and NAA levels being predictive of the NAC group provides preliminary support for the putative anti-oxidative role of NAC in MDD. The authors stated that the links between Glx and GSH synthesis (Dodd et al. 2008) and between NAA and GSH levels (Heales et al. 1995) would support that GSH levels were likely elevated by NAC.
Despite the overwhelming evidence of GSH depletion in multiple psychiatric disorders, monitoring of brain levels of GSH before and after oral NAC treatment has not been conducted to date. The closest attempt to this strategy was performed by Holmay et al., who showed that a single-dose, intravenous administration of NAC resulted in an increase in GSH in the occipital cortices of patients with Gaucher and Parkinson diseases (Holmay et al. 2013). Clearly, the use of 1H MRS is at its infancy.
6 Future Directions
The evidence supporting the role of the antioxidant system in the pathophysiology in neuropsychiatric disorders is mounting. Treatment studies examining the effect of NAC on behavioral improvement are of interest to many investigators, and attempts are being made to replicate existing findings in larger trials. More importantly, there is a dire need to examine the direct effect of NAC on the antioxidant system either peripherally or centrally. Therefore, measuring GSH concentrations in the brain before and after NAC treatment is essential not only important to confirm the mechanism of action of NAC but also provide a potential avenue to develop biomarkers that can track disease progression and predict response to treatment. This strategy will be facilitated by the development of advanced MRS methodologies to allow the reliable measurement of GSH in the brain using acquisition sequences that are of short duration to facilitate the participation of individuals with severe neuropsychiatric disorders.
References
Al-Gadani Y, El-Ansary A, Attas O, Al-Ayadhi L (2009) Metabolic biomarkers related to oxidative stress and antioxidant status in Saudi autistic children. Clin Biochem 42(10–11):1032–1040. https://doi.org/10.1016/j.clinbiochem.2009.03.011
Altuntas I, Aksoy H, Coskun I, Caykoylu A, Akcay F (2000) Erythrocyte superoxide dismutase and glutathione peroxidase activities, and malondialdehyde and reduced glutathione levels in schizophrenic patients. Clin Chem Lab Med 38(12):1277–1281. https://doi.org/10.1515/CCLM.2000.201
Andreazza AC, Kapczinski F, Kauer-Sant’Anna M, Walz JC, Bond DJ, Goncalves CA, Young LT, Yatham LN (2009) 3-Nitrotyrosine and glutathione antioxidant system in patients in the early and late stages of bipolar disorder. J Psychiatry Neurosci 34(4):263–271
Andreazza AC, Wang JF, Salmasi F, Shao L, Young LT (2013) Specific subcellular changes in oxidative stress in prefrontal cortex from patients with bipolar disorder. J Neurochem 127(4):552–561. https://doi.org/10.1111/jnc.12316
Andreazza AC, Gildengers A, Rajji TK, Zuzarte PM, Mulsant BH, Young LT (2015) Oxidative stress in older patients with bipolar disorder. Am J Geriatr Psychiatry 23(3):314–319. https://doi.org/10.1016/j.jagp.2014.05.008
Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Judd F, Katz F, Katz P, Ording-Jespersen S, Little J, Conus P, Cuenod M, Do KQ, Bush AI (2008a) N-acetyl cysteine as a glutathione precursor for schizophrenia--a double-blind, randomized, placebo-controlled trial. Biol Psychiatry 64(5):361–368. https://doi.org/10.1016/j.biopsych.2008.03.004
Berk M, Copolov DL, Dean O, Lu K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Bush AI (2008b) N-acetyl cysteine for depressive symptoms in bipolar disorder--a double-blind randomized placebo-controlled trial. Biol Psychiatry 64(6):468–475. https://doi.org/10.1016/j.biopsych.2008.04.022
Berk M, Dean OM, Cotton SM, Gama CS, Kapczinski F, Fernandes B, Kohlmann K, Jeavons S, Hewitt K, Moss K, Allwang C, Schapkaitz I, Cobb H, Bush AI, Dodd S, Malhi GS (2012) Maintenance N-acetyl cysteine treatment for bipolar disorder: a double-blind randomized placebo controlled trial. BMC Med 10:91. https://doi.org/10.1186/1741-7015-10-91
Berk M, Dean OM, Cotton SM, Jeavons S, Tanious M, Kohlmann K, Hewitt K, Moss K, Allwang C, Schapkaitz I, Robbins J, Cobb H, Ng F, Dodd S, Bush AI, Malhi GS (2014) The efficacy of adjunctive N-acetylcysteine in major depressive disorder: a double-blind, randomized, placebo-controlled trial. J Clin Psychiatry 75(6):628–636. https://doi.org/10.4088/JCP.13m08454
Bilici M, Efe H, Koroglu MA, Uydu HA, Bekaroglu M, Deger O (2001) Antioxidative enzyme activities and lipid peroxidation in major depression: alterations by antidepressant treatments. J Affect Disord 64(1):43–51
Brown NC, Andreazza AC, Young LT (2014) An updated meta-analysis of oxidative stress markers in bipolar disorder. Psychiatry Res 218(1–2):61–68. https://doi.org/10.1016/j.psychres.2014.04.005
Cabungcal JH, Steullet P, Kraftsik R, Cuenod M, Do KQ (2013) Early-life insults impair parvalbumin interneurons via oxidative stress: reversal by N-acetylcysteine. Biol Psychiatry 73(6):574–582. https://doi.org/10.1016/j.biopsych.2012.09.020
Das P, Tanious M, Fritz K, Dodd S, Dean OM, Berk M, Malhi GS (2013) Metabolite profiles in the anterior cingulate cortex of depressed patients differentiate those taking N-acetyl-cysteine versus placebo. Aust N Z J Psychiatry 47(4):347–354. https://doi.org/10.1177/0004867412474074
Dean OM, Gray KM, Villagonzalo KA, Dodd S, Mohebbi M, Vick T, Tonge BJ, Berk M (2016) A randomised, double blind, placebo-controlled trial of a fixed dose of N-acetyl cysteine in children with autistic disorder. Aust N Z J Psychiatry 51(3):241–249. https://doi.org/10.1177/0004867416652735
Do KQ, Trabesinger AH, Kirsten-Kruger M, Lauer CJ, Dydak U, Hell D, Holsboer F, Boesiger P, Cuenod M (2000) Schizophrenia: glutathione deficit in cerebrospinal fluid and prefrontal cortex in vivo. Eur J Neurosci 12(10):3721–3728
Do KQ, Cuenod M, Hensch TK (2015) Targeting oxidative stress and aberrant critical period plasticity in the developmental trajectory to schizophrenia. Schizophr Bull 41(4):835–846. https://doi.org/10.1093/schbul/sbv065
Dodd S, Dean O, Copolov DL, Malhi GS, Berk M (2008) N-acetylcysteine for antioxidant therapy: pharmacology and clinical utility. Expert Opin Biol Ther 8(12):1955–1962. https://doi.org/10.1517/14728220802517901
Duffy SL, Lagopoulos J, Cockayne N, Hermens DF, Hickie IB, Naismith SL (2015) Oxidative stress and depressive symptoms in older adults: a magnetic resonance spectroscopy study. J Affect Disord 180:29–35. https://doi.org/10.1016/j.jad.2015.03.007
Durieux AM, Horder J, Mendez MA, Egerton A, Williams SC, Wilson CE, Spain D, Murphy C, Robertson D, Barker GJ, Murphy DG, McAlonan GM (2016) Cortical and subcortical glutathione levels in adults with autism spectrum disorder. Autism Res 9(4):429–435. https://doi.org/10.1002/aur.1522
El-Ansary A, Al-Ayadhi L (2012) Lipid mediators in plasma of autism spectrum disorders. Lipids Health Dis 11:160. https://doi.org/10.1186/1476-511X-11-160
Farokhnia M, Azarkolah A, Adinehfar F, Khodaie-Ardakani MR, Hosseini SM, Yekehtaz H, Tabrizi M, Rezaei F, Salehi B, Sadeghi SM, Moghadam M, Gharibi F, Mirshafiee O, Akhondzadeh S (2013) N-acetylcysteine as an adjunct to risperidone for treatment of negative symptoms in patients with chronic schizophrenia: a randomized, double-blind, placebo-controlled study. Clin Neuropharmacol 36(6):185–192. https://doi.org/10.1097/WNF.0000000000000001
Flatow J, Buckley P, Miller BJ (2013) Meta-analysis of oxidative stress in schizophrenia. Biol Psychiatry 74(6):400–409. https://doi.org/10.1016/j.biopsych.2013.03.018
Frustaci A, Neri M, Cesario A, Adams JB, Domenici E, Dalla Bernardina B, Bonassi S (2012) Oxidative stress-related biomarkers in autism: systematic review and meta-analyses. Free Radic Biol Med 52(10):2128–2141. https://doi.org/10.1016/j.freeradbiomed.2012.03.011
Galecki P, Szemraj J, Bienkiewicz M, Florkowski A, Galecka E (2009) Lipid peroxidation and antioxidant protection in patients during acute depressive episodes and in remission after fluoxetine treatment. Pharmacol Rep 61(3):436–447
Gawryluk JW, Wang JF, Andreazza AC, Shao L, Young LT (2011) Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int J Neuropsychopharmacol 14(1):123–130. https://doi.org/10.1017/S1461145710000805
Geier DA, Kern JK, Garver CR, Adams JB, Audhya T, Geier MR (2009) A prospective study of transsulfuration biomarkers in autistic disorders. Neurochem Res 34(2):386–393. https://doi.org/10.1007/s11064-008-9782-x
Ghezzo A, Visconti P, Abruzzo PM, Bolotta A, Ferreri C, Gobbi G, Malisardi G, Manfredini S, Marini M, Nanetti L, Pipitone E, Raffaelli F, Resca F, Vignini A, Mazzanti L (2013) Oxidative stress and erythrocyte membrane alterations in children with autism: correlation with clinical features. PLoS One 8(6):e66418. https://doi.org/10.1371/journal.pone.0066418
Godlewska BR, Yip SW, Near J, Goodwin GM, Cowen PJ (2014) Cortical glutathione levels in young people with bipolar disorder: a pilot study using magnetic resonance spectroscopy. Psychopharmacology 231(2):327–332. https://doi.org/10.1007/s00213-013-3244-0
Godlewska BR, Near J, Cowen PJ (2015) Neurochemistry of major depression: a study using magnetic resonance spectroscopy. Psychopharmacology 232(3):501–507. https://doi.org/10.1007/s00213-014-3687-y
Gu F, Chauhan V, Chauhan A (2013) Impaired synthesis and antioxidant defense of glutathione in the cerebellum of autistic subjects: alterations in the activities and protein expression of glutathione-related enzymes. Free Radic Biol Med 65:488–496. https://doi.org/10.1016/j.freeradbiomed.2013.07.021
Han Y, Xi QQ, Dai W, Yang SH, Gao L, Su YY, Zhang X (2015) Abnormal transsulfuration metabolism and reduced antioxidant capacity in Chinese children with autism spectrum disorders. Int J Dev Neurosci 46:27–32. https://doi.org/10.1016/j.ijdevneu.2015.06.006
Hardan AY, Fung LK, Libove RA, Obukhanych TV, Nair S, Herzenberg LA, Frazier TW, Tirouvanziam R (2012) A randomized controlled pilot trial of oral N-acetylcysteine in children with autism. Biol Psychiatry 71(11):956–961. https://doi.org/10.1016/j.biopsych.2012.01.014
Heales SJ, Davies SE, Bates TE, Clark JB (1995) Depletion of brain glutathione is accompanied by impaired mitochondrial function and decreased N-acetyl aspartate concentration. Neurochem Res 20(1):31–38
Holmay MJ, Terpstra M, Coles LD, Mishra U, Ahlskog M, Oz G, Cloyd JC, Tuite PJ (2013) N-acetylcysteine boosts brain and blood glutathione in Gaucher and Parkinson diseases. Clin Neuropharmacol 36(4):103–106. https://doi.org/10.1097/WNF.0b013e31829ae713
James SJ, Melnyk S, Jernigan S, Cleves MA, Halsted CH, Wong DH, Cutler P, Bock K, Boris M, Bradstreet JJ, Baker SM, Gaylor DW (2006) Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am J Med Genet B Neuropsychiatr Genet 141B(8):947–956. https://doi.org/10.1002/ajmg.b.30366
Khanzode SD, Dakhale GN, Khanzode SS, Saoji A, Palasodkar R (2003) Oxidative damage and major depression: the potential antioxidant action of selective serotonin re-uptake inhibitors. Redox Rep 8(6):365–370. https://doi.org/10.1179/135100003225003393
Kim HK, Andreazza AC, Yeung PY, Isaacs-Trepanier C, Young LT (2014) Oxidation and nitration in dopaminergic areas of the prefrontal cortex from patients with bipolar disorder and schizophrenia. J Psychiatry Neurosci 39(4):276–285
Kodydkova J, Vavrova L, Zeman M, Jirak R, Macasek J, Stankova B, Tvrzicka E, Zak A (2009) Antioxidative enzymes and increased oxidative stress in depressive women. Clin Biochem 42(13-14):1368–1374. https://doi.org/10.1016/j.clinbiochem.2009.06.006
Lagopoulos J, Hermens DF, Tobias-Webb J, Duffy S, Naismith SL, White D, Scott E, Hickie IB (2013) In vivo glutathione levels in young persons with bipolar disorder: a magnetic resonance spectroscopy study. J Psychiatr Res 47(3):412–417. https://doi.org/10.1016/j.jpsychires.2012.12.006
Lapidus KA, Gabbay V, Mao X, Johnson A, Murrough JW, Mathew SJ, Shungu DC (2014) In vivo (1)H MRS study of potential associations between glutathione, oxidative stress and anhedonia in major depressive disorder. Neurosci Lett 569:74–79. https://doi.org/10.1016/j.neulet.2014.03.056
Laszlo A, Novak Z, Szollosi-Varga I, Hai du Q, Vetro A, Kovacs A (2013) Blood lipid peroxidation, antioxidant enzyme activities and hemorheological changes in autistic children. Ideggyogy Sz 66(1–2):23–28
Lavoie S, Murray MM, Deppen P, Knyazeva MG, Berk M, Boulat O, Bovet P, Bush AI, Conus P, Copolov D, Fornari E, Meuli R, Solida A, Vianin P, Cuenod M, Buclin T, Do KQ (2008) Glutathione precursor, N-acetyl-cysteine, improves mismatch negativity in schizophrenia patients. Neuropsychopharmacology 33(9):2187–2199. https://doi.org/10.1038/sj.npp.1301624
Matsuzawa D, Hashimoto K (2011) Magnetic resonance spectroscopy study of the antioxidant defense system in schizophrenia. Antioxid Redox Signal 15(7):2057–2065. https://doi.org/10.1089/ars.2010.3453
Matsuzawa D, Obata T, Shirayama Y, Nonaka H, Kanazawa Y, Yoshitome E, Takanashi J, Matsuda T, Shimizu E, Ikehira H, Iyo M, Hashimoto K (2008) Negative correlation between brain glutathione level and negative symptoms in schizophrenia: a 3T 1H-MRS study. PLoS One 3(4):e1944. https://doi.org/10.1371/journal.pone.0001944
Meguid NA, Dardir AA, Abdel-Raouf ER, Hashish A (2011) Evaluation of oxidative stress in autism: defective antioxidant enzymes and increased lipid peroxidation. Biol Trace Elem Res 143(1):58–65. https://doi.org/10.1007/s12011-010-8840-9
Michel TM, Frangou S, Thiemeyer D, Camara S, Jecel J, Nara K, Brunklaus A, Zoechling R, Riederer P (2007) Evidence for oxidative stress in the frontal cortex in patients with recurrent depressive disorder—a postmortem study. Psychiatry Res 151(1-2):145–150. https://doi.org/10.1016/j.psychres.2006.04.013
Mico JA, Rojas-Corrales MO, Gibert-Rahola J, Parellada M, Moreno D, Fraguas D, Graell M, Gil J, Irazusta J, Castro-Fornieles J, Soutullo C, Arango C, Otero S, Navarro A, Baeza I, Martinez-Cengotitabengoa M, Gonzalez-Pinto A (2011) Reduced antioxidant defense in early onset first-episode psychosis: a case-control study. BMC Psychiatry 11:26. https://doi.org/10.1186/1471-244X-11-26
Moniczewski A, Gawlik M, Smaga I, Niedzielska E, Krzek J, Przegalinski E, Pera J, Filip M (2015) Oxidative stress as an etiological factor and a potential treatment target of psychiatric disorders. Part 1. Chemical aspects and biological sources of oxidative stress in the brain. Pharmacol Rep 67(3):560–568. https://doi.org/10.1016/j.pharep.2014.12.014
Monin A, Baumann PS, Griffa A, Xin L, Mekle R, Fournier M, Butticaz C, Klaey M, Cabungcal JH, Steullet P, Ferrari C, Cuenod M, Gruetter R, Thiran JP, Hagmann P, Conus P, Do KQ (2015) Glutathione deficit impairs myelin maturation: relevance for white matter integrity in schizophrenia patients. Mol Psychiatry 20(7):827–838. https://doi.org/10.1038/mp.2014.88
Morishita H, Cabungcal JH, Chen Y, Do KQ, Hensch TK (2015) Prolonged period of cortical plasticity upon redox dysregulation in fast-spiking interneurons. Biol Psychiatry 78(6):396–402. https://doi.org/10.1016/j.biopsych.2014.12.026
Ozcan ME, Gulec M, Ozerol E, Polat R, Akyol O (2004) Antioxidant enzyme activities and oxidative stress in affective disorders. Int Clin Psychopharmacol 19(2):89–95
Raffa M, Mechri A, Othman LB, Fendri C, Gaha L, Kerkeni A (2009) Decreased glutathione levels and antioxidant enzyme activities in untreated and treated schizophrenic patients. Prog Neuro-Psychopharmacol Biol Psychiatry 33(7):1178–1183. https://doi.org/10.1016/j.pnpbp.2009.06.018
Raffa M, Atig F, Mhalla A, Kerkeni A, Mechri A (2011) Decreased glutathione levels and impaired antioxidant enzyme activities in drug-naive first-episode schizophrenic patients. BMC Psychiatry 11:124. https://doi.org/10.1186/1471-244X-11-124
Rosa AR, Singh N, Whitaker E, de Brito M, Lewis AM, Vieta E, Churchill GC, Geddes JR, Goodwin GM (2014) Altered plasma glutathione levels in bipolar disorder indicates higher oxidative stress; a possible risk factor for illness onset despite normal brain-derived neurotrophic factor (BDNF) levels. Psychol Med 44(11):2409–2418. https://doi.org/10.1017/S0033291714000014
Rose S, Melnyk S, Pavliv O, Bai S, Nick TG, Frye RE, James SJ (2012) Evidence of oxidative damage and inflammation associated with low glutathione redox status in the autism brain. Transl Psychiatry 2:e134. https://doi.org/10.1038/tp.2012.61
Rose S, Frye RE, Slattery J, Wynne R, Tippett M, Pavliv O, Melnyk S, James SJ (2014) Oxidative stress induces mitochondrial dysfunction in a subset of autism lymphoblastoid cell lines in a well-matched case control cohort. PLoS One 9(1):e85436. https://doi.org/10.1371/journal.pone.0085436
Rose S, Frye RE, Slattery J, Wynne R, Tippett M, Melnyk S, James SJ (2015) Oxidative stress induces mitochondrial dysfunction in a subset of autistic lymphoblastoid cell lines. Transl Psychiatry 5:e526. https://doi.org/10.1038/tp.2015.29
Rose S, Bennuri SC, Wynne R, Melnyk S, James SJ, Frye RE (2017) Mitochondrial and redox abnormalities in autism lymphoblastoid cells: a sibling control study. FASEB J 31(3):904–909. https://doi.org/10.1096/fj.201601004R
Sarandol A, Sarandol E, Eker SS, Erdinc S, Vatansever E, Kirli S (2007) Major depressive disorder is accompanied with oxidative stress: short-term antidepressant treatment does not alter oxidative-antioxidative systems. Hum Psychopharmacol 22(2):67–73. https://doi.org/10.1002/hup.829
Selek S, Savas HA, Gergerlioglu HS, Bulbul F, Uz E, Yumru M (2008) The course of nitric oxide and superoxide dismutase during treatment of bipolar depressive episode. J Affect Disord 107(1-3):89–94. https://doi.org/10.1016/j.jad.2007.08.006
Soeiro-de-Souza MG, Pastorello BF, Leite Cda C, Henning A, Moreno RA, Garcia Otaduy MC (2016) Dorsal anterior cingulate lactate and glutathione levels in euthymic bipolar I disorder: 1H-MRS study. Int J Neuropsychopharmacol 19(8):pyw032. https://doi.org/10.1093/ijnp/pyw032
Steullet P, Cabungcal JH, Kulak A, Kraftsik R, Chen Y, Dalton TP, Cuenod M, Do KQ (2010) Redox dysregulation affects the ventral but not dorsal hippocampus: impairment of parvalbumin neurons, gamma oscillations, and related behaviors. J Neurosci 30(7):2547–2558. https://doi.org/10.1523/JNEUROSCI.3857-09.2010
Terpstra M, Vaughan TJ, Ugurbil K, Lim KO, Schulz SC, Gruetter R (2005) Validation of glutathione quantitation from STEAM spectra against edited 1H NMR spectroscopy at 4T: application to schizophrenia. MAGMA 18(5):276–282. https://doi.org/10.1007/s10334-005-0012-0
Tsai MC, Huang TL (2015) Thiobarbituric acid reactive substances (TBARS) is a state biomarker of oxidative stress in bipolar patients in a manic phase. J Affect Disord 173:22–26. https://doi.org/10.1016/j.jad.2014.10.045
Tuncel OK, Sarisoy G, Bilgici B, Pazvantoglu O, Cetin E, Unverdi E, Avci B, Boke O (2015) Oxidative stress in bipolar and schizophrenia patients. Psychiatry Res 228(3):688–694. https://doi.org/10.1016/j.psychres.2015.04.046
Wei YC, Zhou FL, He DL, Bai JR, Hui LY, Wang XY, Nan KJ (2009) The level of oxidative stress and the expression of genes involved in DNA-damage signaling pathways in depressive patients with colorectal carcinoma. J Psychosom Res 66(3):259–266. https://doi.org/10.1016/j.jpsychores.2008.09.001
Wood SJ, Berger GE, Wellard RM, Proffitt TM, McConchie M, Berk M, McGorry PD, Pantelis C (2009) Medial temporal lobe glutathione concentration in first episode psychosis: a 1H-MRS investigation. Neurobiol Dis 33(3):354–357. https://doi.org/10.1016/j.nbd.2008.11.018
Xin L, Mekle R, Fournier M, Baumann PS, Ferrari C, Alameda L, Jenni R, Lu H, Schaller B, Cuenod M, Conus P, Gruetter R, Do KQ (2016) Genetic polymorphism associated prefrontal glutathione and its coupling with brain glutamate and peripheral redox status in early psychosis. Schizophr Bull 42(5):1185–1196. https://doi.org/10.1093/schbul/sbw038
Yao JK, Leonard S, Reddy R (2006) Altered glutathione redox state in schizophrenia. Dis Markers 22(1–2):83–93
Yorbik O, Sayal A, Akay C, Akbiyik DI, Sohmen T (2002) Investigation of antioxidant enzymes in children with autistic disorder. Prostaglandins Leukot Essent Fatty Acids 67(5):341–343
Zoroglu SS, Armutcu F, Ozen S, Gurel A, Sivasli E, Yetkin O, Meram I (2004) Increased oxidative stress and altered activities of erythrocyte free radical scavenging enzymes in autism. Eur Arch Psychiatry Clin Neurosci 254(3):143–147. https://doi.org/10.1007/s00406-004-0456-7
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Fung, L., Hardan, A. (2019). Oxidative Stress in Psychiatric Disorders. In: Frye, R., Berk, M. (eds) The Therapeutic Use of N-Acetylcysteine (NAC) in Medicine. Adis, Singapore. https://doi.org/10.1007/978-981-10-5311-5_4
Download citation
DOI: https://doi.org/10.1007/978-981-10-5311-5_4
Published:
Publisher Name: Adis, Singapore
Print ISBN: 978-981-10-5310-8
Online ISBN: 978-981-10-5311-5
eBook Packages: MedicineMedicine (R0)