
Abstract
Human beings are the only living organisms that consciously and deliberately kill themselves. Moreover, suicide is present in all societies, and internationally nearly one in ten humans will consider suicide at some point during their lives. This has left many of us asking, “What is it about being human that causes so many people to consider killing themselves?” On the surface, the answer is not a simple one. There is not one clear pathway that leads to suicide. Suicide is associated with a broad array of stressors, mental illnesses, and demographic characteristics. Acceptance and Commitment Therapy (ACT) is a transdiagnostic psychosocial treatment approach grounded in a model of psychological (in)flexibility. ACT offers a compelling explanation for why suicide is uniquely human and heterogeneous in etiology, but has been understudied in regard to its applicability to suicide prevention. In the proposed chapter, we delineate the etiology of suicidal thoughts and behaviours according to the ACT model of psychological (in)flexibility. Further, we review and synthesize the extant literature relevant to this etiological model. Topics of focus include inflexible attention, experiential avoidance, cognitive fusion, attachment to a conceptualized self, and disruption of valued living. We discuss implications for suicide risk assessment and key considerations for using ACT to manage suicide risk (e.g. how to promote the acceptance of suicidal ideation, without encouraging suicidal behaviour and ways to identify new valued directions for taking action that strengthen protective factors). Case material is presented to illustrate how ACT can be used with suicidal individuals to help them build a life they deem worth living.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others

Keywords
- Acceptance and commitment therapy
- Psychological rigidity
- Experiential avoidance
- Fostering emotional willingness
- Value-driven life
Humans are bony terrestrial bipeds with inferior physical capabilities relative to many other faster, stronger, more resilient animals. Nonetheless, humans have been fantastically successful as a species. Over the past century, the global average life expectancy has more than doubled! We have developed unparalleled technology for controlling our environment, protecting against predators and infectious disease, travelling, and transporting knowledge and goods. Humans now inhabit virtually all geographic regions of our planet. This phenomenal success is uniquely human. However, humans are also the only living organisms that consciously and deliberately kill themselves (Hayes, Strosahl, & Wilson, 2012a, b). Suicide is present in all societies and, internationally, nearly one in ten humans will consider suicide at some point during their lives (Nock et al., 2008a, b). In 2012, over 800,000 people died by suicide (World Health Organization, 2016). This has left many asking, “What is it about being human that causes so many people to consider killing themselves?” On the surface, the answer is not simple. Suicide is associated with a broad array of stressors, illnesses, and demographics. There is not one clear pathway that uniformly leads to suicide (Hayes, Pistorello, & Biglan, 2008).
Acceptance and Commitment Therapy (ACT) is a transdiagnostic psychosocial treatment approach grounded in a model of psychological flexibility (Hayes, Pistorello, & Levin, 2012). ACT offers a compelling explanation for why suicide is uniquely human and heterogeneous in etiology (Hayes et al., 2008, 2012), but has been understudied in its applicability to conceptualizing and preventing suicide. In this chapter, we articulate the unique abilities of humans that can also facilitate suicidal thoughts and behaviours, and subsequently delineate the etiology of suicidal thoughts and behaviours according to the ACT model of psychological flexibility, while considering extant empirical support. We conclude by presenting an overview of how ACT can help individuals at risk of suicide build a life worth living.
“What Is It About Being Human that Causes So Many People to Consider Killing Themselves?”
The critical abilities that have made humans so successful are also responsible for causing some to desire death. The development of humans’ capacity for symbolic activity (e.g. language) and derived relations (e.g. A > B and B > C; therefore, A must > C) unleashed a cascade of cultural and technological innovations that continue at an unprecedented rate (Harris, 2009). These abilities allow us to learn indirectly and to vastly increase our knowledge via derived relations. Furthermore, through these cognitive abilities, symbols take on the properties of the actual objects/phenomena they represent (e.g. salivating as you imagine your favourite food).
Yet there is a dark side to these cognitive abilities. The same capacity for symbolic thought, abstract reasoning, and introspection that has made humans so successful is also the source of profound suffering (Hayes et al., 2012). Just as we can reflect on past successes, we can ruminate about our failures. For example, if you think about the first time you fell in love, you probably will experience some of the same emotions and physical sensations that you had at the time. However, you can also reflect on the experience of being rejected or losing a loved one. Simply recalling such experiences often produces a nearly palpable sense of psychological pain. Just as we can look forward to future experiences, we can become entrenched in intense anxiety and hopelessness when our reasoning suggests that the future will be painful. These big brains of ours give us the unique capacity to produce psychological suffering in the absence of any aversive environmental stimuli. We can hurt anywhere anytime. Furthermore, our effective problem-solving skills often backfire when applied to internal experiences; for example, attempts to avoid unwanted thoughts and emotions may lead to isolation and loss of meaningful activities and relationships. ACT was built upon the realization that humans’ cognitive abilities lead to our achievements and misery (Hayes et al., 2012). The ACT model of psychological flexibility, presented below, further explains the processes that lead to human suffering and suicidal desire.
Applying the ACT Model of Psychological Flexibility to Suicidal Self-Directed Violence
The ACT model is defined in terms of six core processes (acceptance, defusion, being present, a noticing self, values, and committed action) that revolve around a single-core concept: psychological flexibility. Psychological flexibility can be defined as “contacting the present moment as a conscious human being, fully and without defense, as it is and not as what [the mind] says it is, and persisting or changing one’s own behaviour in the service of chosen values” (Hayes, Levin, Plumb-Vilardaga, Villatte, & Pistorello, 2013). This is the central mechanism of change in ACT, and the six core processes together create psychological flexibility.
The ACT model of psychological flexibility has been used to understand a variety of psychiatric conditions. Nonetheless, a strength of ACT is that it provides a unified transdiagnostic model for understanding and implementing behaviour change. Thus, the ACT model can be particularly useful for understanding and treating complex transdiagnostic problems and behaviours, including suicidal self-directed violence (SDV).
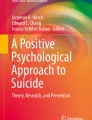
Although suicide is complex and multi-faceted, the pathways to suicidal SDV share a common element: they all involve some form of unwanted emotional or physical pain that is difficult, if not impossible, to control. Thus, suicidal SDV, according to ACT, emerges as an extreme attempt to control psychological and/or physical pain; yet herein lies the fundamental problem. Pain in and of itself is normal and inherent to being human. It is our attempts to control pain that are problematic, as such efforts often contribute to prolonged, unnecessary suffering. As shown in Fig. 26.1, each core process that contributes to psychological flexibility has a corresponding inverse process that contributes to psychological rigidity, which can be used to understand suicide.

Source Adapted from Hayes, Luoma, Bond, Masuda, and Lillis (2006)
ACT model of psychological rigidity.
The concept at the centre of the model is psychological inflexibility or rigidity. At the most basic level, suicidal SDV is conceptualized as an ineffective problem-solving method, motivated by a strong desire to escape pain and suffering (i.e. experiential control) that undermines value-driven behaviour (i.e. behavioural restriction). The six core processes that contribute to psychological rigidity and their application to suicidal SDV are described in Table 26.1.
Empirical Support for the ACT Conceptualization of Suicidal SDV
Psychological Rigidity
Research examining psychological rigidity broadly (assessed via executive functioning and neurocognitive tests) has demonstrated that mental inflexibility is, in fact, associated with suicidal thoughts and behaviours (Keilp et al., 2001; Marzuk, Hartwell, Leon, & Portera, 2005; Williams & Broadbent, 1986). For example, among depressed patients, those with current suicidal ideation (SI) performed more poorly on a measure of mental inflexibility (Marzuk et al., 2005). Additionally, adolescents who had recently attempted suicide demonstrated rigid thinking, compared to controls (Wilson et al., 1995). However, post-crisis, individuals who have made a suicide attempt (SA), do not remain inflexible, suggesting that rigidity associated with suicidal thoughts is a correlate of stress (Perrah & Wichman, 2010). Such research supports the conceptualization of psychological rigidity leading to suicidal SDV.
Experiential Avoidance
Experiential avoidance plays a key role in suicidal SDV. In a meta-analysis by Hayes, Luoma, Bond, Masuda, and Lillis (2006), experiential avoidance accounted for 16 to 25% of the variance in behavioural health problems generally and those identified as risk factors for suicidality. Additionally, greater psychological flexibility (i.e. less experiential avoidance) is associated with a lower likelihood of experiencing suicidal thoughts and behaviours (Bryan, Ray-Sannerud, & Heron, 2015). Bahraini et al. (2016) recently examined the association between experiential avoidance and SI among post-9/11 combat veterans. Experiential avoidance was positively associated with SI, adjusting for SA history and psychiatric symptoms. These findings also extend to inpatient populations; in a study by Ellis and Rufino (2016), hospitalized adults who reported decreased experiential avoidance also reported significant decreases in SI, independent of depression severity and hopelessness.
Avoidant coping styles are also associated with SDV (Guerreiro et al., 2013; Josepho & Plutchik, 1994), further supporting the assertion that avoidance is associated with risk for suicide. Moreover, although experiential avoidance involves attempts to avoid a variety of internal experiences (e.g. thoughts, emotions, sensations), substantial research has focused on attempts to suppress unwanted thoughts. The desire to suppress disturbing thoughts may seem natural; yet doing so paradoxically increases the unwanted thoughts (c.f. Wegner, 1994). In a series of studies in undergraduate and clinical samples, Pettit et al. (2009) demonstrated that a greater tendency to suppress suicidal thoughts was associated with higher levels of concurrent SI. Moreover, individuals who endorsed greater baseline tendencies to suppress suicidal thoughts displayed an increase in the severity of SI over time. Furthermore, ineffective attempts to suppress unwanted aspects of emotional experiences may generate additional negative beliefs about the emotional material itself or about one’s ability to control emotions (Salters-Pedneault, Tull, & Roemer, 2004). Such non-acceptance of emotional experiences is correlated with self-reported difficulties in emotion regulation and impulsive behaviours, including self-harm (Gratz & Roemer, 2004). These findings suggest that suppressing internal experiences (including suicidal thoughts) actually increases the presence of associated internal states (e.g. SI) and interferes with adaptive responding in the face of threatening stimuli. Thus, accepting that suicidal thoughts will occur may decrease emotional distress and also decrease SI, although research is needed to examine this directly. In sum, these results support the ACT conceptualization of experiential avoidance as a core process leading to SI and SA.
Fusion
Although sparse research has examined the association between fusion and suicidal SDV, a robust literature has demonstrated that hopelessness and dichotomous thinking are associated with suicidal thoughts and behaviours (Beck, Steer, Kovacs, & Garrison, 1985; Neuringer & Lettieri, 1971). Most extant research has focused on the presence of maladaptive thoughts as they relate to suicidality, rather than assessing fusion with those thoughts per se. Such research has supported a link between negative thoughts and SI, even when accounting for depression (Chioqueta & Stiles, 2007; Coleman & Casey, 2007). Thus, although certain types of thoughts are associated with SI and SDV, empirical studies are needed to examine whether fusion with such thoughts actually leads to SI and SDV.
Values
Cross-sectional research also suggests that identifying more values as important and perceiving success acting consistently with one’s values are both associated with being less likely to report recent SI (Bahraini et al., 2013). These findings suggest that helping patients to clarify values that are important to them and to increase value-consistent behaviour may help to decrease SI. In addition, the extent to which individuals report caring about specific values (e.g. relationships) moderates the association between known risk factors for suicide (i.e. thwarted belongingness) and SI (Monteith, Pease, Forster, Homaifar, & Bahraini, 2015), further underscoring the important role of personal values and committed action in regard to SI.
Mindfulness
Mindfulness, or present-focused, curious, open, accepting awareness (Bishop et al., 2004), can also be described as a combination of four processes of psychological flexibility: contact with the present moment, acceptance, cognitive defusion, and self as context (Luoma & Villatte, 2012). Mindfulness is inversely associated with SI (Chesin & Jeglic, 2016; Lamis & Dvorak, 2014; Serpa, Taylor, & Tillisch, 2014). Chesin et al. (2016) recently reviewed the literature and found that mindfulness-based interventions are well suited to target SI and specific deficits associated with SA, such as attentional dyscontrol. Additionally, trait mindfulness mediates the association between symptom severity and suicidal probability (Mohammadkhani, Khanipour, Azadmehr, Mobramm, & Naseri, 2015). Whereas mindfulness appears to be protective against SI, rumination (particularly ruminative brooding) and anxiety (e.g. generalized anxiety, social phobia) appear to be risk factors for SI (Cougle, Keough, Riccardi, & Sachs-Ericsson, 2009; Miranda, Valderraman, Tsypes, Gadol, & Gallagher, 2013; Morrison & O’Connor, 2011; Norton, Temple, & Pettit, 2008); notably, these processes involve diverting one’s attention away from the present and focusing instead on the past (i.e. rumination) or the future (i.e. anxiety).
In a randomized controlled trial comparing mindfulness meditation and relaxation training, Jain et al. (2007) found that mindfulness significantly decreased ruminative thoughts. Indeed, participants of mindfulness-based cognitive therapy (MBCT) demonstrate significant decreases in SI (Chesin et al., 2015; Forkmann et al., 2014), and decreases in worry are associated with decreases in SI among individuals participating in MBCT (Forkmann et al., 2014). Notably, certain aspects of mindfulness, such as the ability to observe internal experiences happening in the present, appear to be more protective against SI (Chesin & Jeglic, 2016). Furthermore, the ability to observe internal experiences is associated with less severe SI (Chesin & Jeglic, 2016). Taken together, findings from cross-sectional and interventional research suggest that past and future dominance is associated with SDV, whereas the converse (i.e. mindfulness) is inversely associated with SDV.
ACT Interventions
Research demonstrates that the different ACT processes are interconnected, and that success in one area optimizes success in others. For example, cognitive fusion and experiential avoidance interact, such that associations between cognitive fusion and psychiatric symptoms (e.g. depression, PTSD, anxiety) are strongest at higher levels of experiential avoidance (Bardeen & Fergus, 2016). In addition, psychological rigidity is a barrier to engaging in value-consistent behaviour (Plumb, Stewart, Dahl, & Lundgren, 2009). Research with individuals suffering from chronic pain indicates that the values component of ACT is more effective than focusing exclusively on acceptance (Branstetter-Rost, Cushing, & Douleh, 2009). These findings highlight the potential utility of each ACT domain for decreasing patients’ suffering.
ACT has been shown to be effective at reducing SI among depressed Veterans (Walser et al., 2015) and among a sample of individuals with a recent SA (Ducasse et al., 2014). Case study reports have also shown promising results for ACT interventions with suicidal individuals (Luoma & Villatte, 2012). However, further research is needed to examine the impact of ACT on SI and SDV.
Assessment According to the ACT Conceptualization of Suicidal SDV
Many assessment instruments have been developed to measure the processes involved in psychological flexibility. The ability to operationalize these processes is critical both to advancing ACT research and understanding how ACT can prevent suicidal SDV. Furthermore, assessment can help inform treatment targets and monitor progress. Such assessments are most consistent with ACT when done collaboratively and with an inquisitive, supportive, and open-minded approach. Below we describe assessment instruments for measuring each process associated with psychological rigidity/flexibility.
Fusion
ACT differs from other therapeutic modalities in that the presence of SI is not necessarily seen as problematic in and of itself. Rather, how individuals respond to suicidal thoughts or urge determines whether such experiences are considered problematic—for example, if a patient is fused with suicidal thoughts, such that they attach meaning to them or act on such thoughts with SDV, these latter processes and actions would be considered targets for intervention. Thus, assessing fusion with suicidal thoughts is an important component of case conceptualization and treatment when working with suicidal patients. We are not aware of any measures that assess fusion with suicidal thoughts specifically, and research on the association between cognitive fusion and SI is lacking.
However, considering that cognitive fusion is associated with several indices of psychological distress and PTSD (Bardeen & Fergus, 2016), assessing fusion more generally is important and can be accomplished with the Cognitive Fusion Questionnaire (Gillanders et al., 2014), a brief 7-item self-report measure that has evidenced reliability, validity and sensitivity to treatment with different samples. Alternately, the Thought-Action Fusion Revised Scale (Shafran, Thordarson, & Rachman, 1996) is a self-report measure which assesses different components of fusion, including the belief that thinking about an event increases: (1) the likelihood of it occurring; and (2) is equated to acting on the thought. Additional measures have been developed to assess how much individuals believe specific thoughts, such as negative thoughts (e.g. Stigmatizing Attitudes—Believability; Hayes et al., 2004), anxious thoughts and feelings (e.g. Believability of Anxious Feelings and Thoughts Questionnaire; Herzberg et al., 2012), and depressogenic automatic thoughts (e.g. Automatic Thoughts Questionnaire—Believability subscale; Zettle & Hayes, 1986). The Experiences Questionnaire (Fresco et al., 2007) measures decentering, which (similar to defusion) is defined as the ability to observe one’s thoughts and feelings as temporary, objective events in the mind. As suicidal thoughts and behaviours are common across many symptoms and disorders, the Cognitive Fusion Questionnaire (Gillanders et al., 2014) provides the most flexibility in terms of operationalization, item content, and psychometric properties to date.
Experiential Avoidance
Experiential avoidance can be assessed with the 7-item Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011; Hayes et al., 2006), which assesses willingness to approach (versus avoid) aversive internal experiences. The AAQ-II correlates with SI (Bahraini et al., 2016) and decreases in AAQ-II scores (i.e., increased willingness) during the course of ACT have been associated with lower odds of SI across time (Walser et al., 2015). In addition, disorder and syndrome-specific measures of experiential avoidance have been found to correlate more strongly with actual behaviours. Thus, when working with patients at risk for suicide, assessing experiential avoidance of suicide-related thoughts specifically may be warranted and may be achieved with the suicide-specific version of the White Bear Suppression Inventory (WBSI-SI; Williams, Duggan, Crane, & Hepburn, 2011).
Values
Assessing patients’ values and their perceived success living consistently with those values is essential to understanding risk for suicide and intervening with ACT. Several questionnaires have been developed specifically for this purpose, including the Valued Living Questionnaire (Wilson, Sandoz, Kitchens, & Roberts, 2010); the Bull’s Eye Values Survey, which assesses values attainment, discrepancy between stated values and behaviour, perceived barriers to valued living, and behavioural persistence (Lundgren, Luoma, Dahl, Strosahl, & Melin, 2012); the Personal Values Questionnaire (Blackledge & Ciarrochi, 2006); and the Survey of Life Principles (Ciarrochi & Bailey, 2008), which also assesses number of values put into play recently and pressure to endorse different values. For clinicians seeking to utilize more experiential and interactive methods of helping their patients to identify values, several values/life principles card sort exercises can be used (e.g. Ciarrochi & Bailey, 2008). Additionally, some research has shown that writing about important values, followed by word selection from the writing sample, is a valuable way to help patients identify values (Sandoz & Hebert, 2015).
Multiple Core Processes
In addition to measures that focus specifically on a single process of psychological flexibility/rigidity, there are many measures that capture a combination of several different ACT processes. As noted, mindfulness can be described as a combination of four processes of psychological flexibility: contact with the present moment, acceptance, cognitive defusion, and self as context (Luoma & Villatte, 2012). Mindfulness can be assessed through a variety of different self-report instruments, such as the Five Facet Mindfulness Questionnaire (FFMQ; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006), Mindful Attention Awareness Scale (MAAS; Brown & Ryan, 2003), and Philadelphia Mindfulness Scale (Cardaciotto, Herbert, Forman, Moitra, & Farrow, 2008). These measures range from 15 (MMAS) to 39 items (FFMQ). The lengthier assessments (e.g. FFMQ) provide information regarding specific mindfulness skills, such as individuals’ ability to observe and describe their experiences, act with awareness, and be non-judgmental and non-reactive to such internal experiences (Baer et al., 2006, 2008).
Suicidal Self-Directed Violence
Lastly, given the focus in ACT on actual behaviour (e.g. SA, preparatory behaviour), rather than internal experiences (e.g. SI), assessing suicidal SDV or preparatory behaviour is particularly important. There are a number of structured interviews which can aid this, including the Self-Injurious Thoughts and Behaviours Interview (SITBI; Nock, Holmber, Photos, & Michel, 2007), Scale for Suicidal Ideation (SSI; Beck, Kovacs, & Weissman, 1979), Lifetime Suicide Attempt Self-Injury Interview (L-SASI; Linehan & Comtois, 1996), Self-Harm Behaviour Questionnaire (SHBQ; Gutierrez, Osman, Barrios, & Kopper, 2001), and Columbia-Suicide Severity Rating Scale (C-SSRS; Posner et al., 2011).
Treatment Considerations for Using ACT to Prevent Suicidal Self-Directed Violence and Build Lives Worth Living
ACT interventions are particularly well suited for helping individuals who engage in or are at risk for suicidal SDV. ACT is a flexible treatment modality that allows clinicians to tailor interventions to the individual patient and target the unique drivers of their desire for death. Just as there is no single pathway that leads to suicide, there is no single set of ACT exercises, metaphors, or other techniques that are the way to use ACT to help patients build lives worth living. Future research should seek to optimize the use of ACT for suicide prevention and assess its efficacy for assisting these patients in building lives worth living. Below we draw from our clinical experience, Chiles and Strosahl’s (2005) treatment model for the repetitiously suicidal patient, and nascent literature on using ACT with patients who are suicidal (e.g. Ducasse et al., 2014; Hayes et al., 2008; Luoma & Villatte, 2012) to describe how ACT can be used to address suicide risk. However, we caution the reader against applying these techniques without previous training and experience in ACT. We use ACT in four fundamental ways to address suicide risk: (1) Framing suicide as part of the unworkable agenda of control; (2) Fostering emotional willingness as the alternative to control; (3) Targeting the fusion, impulsivity, and reactivity of suicidal thinking; and (4) Developing and strengthening a value-driven life.
Framing Suicide as Part of the Unworkable Agenda of Control
Treatment begins by joining with the patient in a non-judgmental, empathic way to help them assess what has been keeping them stuck. The clinician can normalize the patient’s attempts to get rid of unwanted thoughts and emotions, and ultimately guide the patient in using past experience to conclude that the control agenda is unworkable (i.e. creative hopelessness). It is not that the patient is incompetent or has not been trying hard enough, but rather that the strategy he has been taught is flawed. There are many different ways to evoke creative hopelessness. A focused interviewing approach (Hayes, Strosahl, & Wilson, 2012; Strosahl, Robinson, & Gustavsson, 2012) can be used by asking the patient: (1) What are you seeking?, (2) What have you tried?, (3) How has it worked?, and (4) What has it cost you?.
In responding to the questions What are you seeking? or How will you know therapy has worked?, patients typically respond with versions of wanting their pain to go away (i.e. unwanted thoughts, emotions, sensations). These questions often elicit important details of the patient’s reasons for dying and rationale for considering suicide, which can become treatment targets (I can’t take this anxiety and depression). Responses to this question can also provide information about the patient’s values and goals that the clinician can explore more fully later in therapy (If I could just get rid of this anxiety and depression, I’d finally be a decent father and do stuff with my son again).
The question of What have you tried? (asked in a curious non-judgmental way) helps gauge the extent of the patient’s experiential avoidance and suicide-related cognitions. The extent of client’s avoidance strategies often includes behaviours like using substances and social isolation which can be explored and reflected as risk factors that frequently lead people to increased suicidal thinking. Patients often then identify suicide as an ultimate strategy they have tried or considered. If suicide is not mentioned, the clinician can gently ask, “Would it be safe to say that your recent attempt (or thinking about ways) to end your own life was another way to try and fix this problem?”.
The final two questions allow the patient to get in touch with the reality that their strategies to get rid of pain not only are not working, but are ultimately causing them to lose control over their life as they have led to the sacrifice of valued life activities (i.e. reasons for living/protective factors). Promoting hopelessness in a person who is already feeling suicidal and hopeless about life may seem like a counterintuitive and daunting task. A critical distinction is that the goal is to illustrate the hopelessness of the control agenda, NOT hopelessness about life. Many patients who feel quite hopeless about life cling to the notion that control and avoidance of pain must be the only viable strategy for getting unstuck—this typically underpins the continued consideration of suicide. As the clinician and patient examine the results of the focused interview, it is important to emphasize suicide as yet another example of the ineffective control strategy that has led them to sacrifice what they value most in life, while also acknowledging that it is perfectly understandable that they have been considering suicide as a solution to their problem. Our society labels certain feelings as negative (e.g. fear, anxiety, sadness) and sends the message that one should not express or feel these things (e.g. don’t worry, be happy). Many people caught up in the struggle label their feelings and thinking as bad, but are unable to get rid of them. Humans then naturally start labelling the whole of themselves as bad. Society’s control agenda teaches us that we should get rid of things that are bad or broken and cannot be fixed. This control strategy tends to be very successful for external things like spoiled milk and markers that have run out of ink, so the notion of applying the same rule and solving the problem by trying to get rid of oneself is not that surprising. Who would blame us for trying to use the same strategy for bad stuff in our heads when it pays off in so many ways outside our minds? Who would blame us for doing things like using substances and withdrawing from others when it reinforces us with initial relief from the discomfort? BUT the patient’s experience shows that the control strategy does not work in the long run and can come at a high price.
Thought suppression (e.g. don’t think of a white bear; Wegner, 1994) and experiential exercises (e.g. Tug of War with Monster; Hayes et al., 2012) can be used to further illustrate that emotional avoidance is ineffective. The patient and clinician should explicitly reach the conclusion that trying to control the pain is the problem, not the solution to living a life worth living. Once patients buy into the hopelessness of the control agenda, they can be encouraged to place the solution of suicide on the shelf while they partner with the therapist in exploring alternative coping skills based on acceptance and a new strategy for building a life worth living (see below). The patient’s ability to realistically abstain from engaging in SDV can be increased by completing a Safety Plan for how they will cope with suicidal crises (c.f. Stanley & Brown, 2012). As patients master new ACT coping techniques and identify adaptive-valued activities, these can be added to the safety plan in place of activities focused purely on distraction.
Fostering Emotional Willingness as the Alternative to Control
After undermining suicidal patients’ beliefs in the efficacy of the control agenda, it is critical to assist them in beginning to explore an alternative way of living and instil hope for their future. This alternative approach begins with willingness, a value-based choice to expose oneself to unpleasant thoughts, emotions, sensations, or feared situations/content in order to engage in meaningful activities and relationships. Patients considering suicide are often suffering immensely, so simply suggesting that they confront and accept their distress is unlikely to be effective. Experiential work (i.e. metaphors, analogies, and exercises) is necessary to assist the patient in exploring the possibility of willingness and acceptance (Hayes et al., 2012) and clarifying the values and value-consistent behaviours this willingness would be in service of.
It is vital to understand what types of unwanted thoughts, emotions, and sensations drive the patient’s desire for death, so that over time the patient can develop the willingness and capacity to hold the internal experiences they are trying to get rid of.
The nature of prolonged emotional avoidance is such that patients may begin to lose contact with their emotions. Using a feeling wheel (Fig. 26.2), the therapist and patient can identify feelings the patient is unwilling to experience. Conversations about the relationships between different feelings (how we know of joy because we have felt despair) can be useful. A coin metaphor can be used to illustrate how we cannot get rid of sadness (heads) unless we also get rid of happiness (tails).

Source Cloitre’s (2013) Skills Training in Affective and Interpersonal Regulation (STAIR) https://www.ptsd.va.gov/apps/STAIR/Session2/docs/Session2Handout_FeelingsWheelColor.pdf
Feeling wheel.
Assisting the patient in personifying and physicalizing thoughts and emotions can be an effective way to further describe unwanted experiences and objectively label these thoughts and emotions when they show up in session (e.g. Here comes failure Frank again). Additionally, the personifications can be worked into experiential exercises like the “passengers on the bus” metaphor (Hayes et al., 2012) to illustrate the necessity of willingness. In the metaphor, the patient is driving a bus in a valued direction (e.g. towards independence), but the bus is full of personified unwanted thoughts and emotions. Failure Frank and his cronies threaten to hurt the patient, unless he drives in the direction they demand (e.g. away from independence). When he veers off course, they quiet down, but he is not living the life he wants to live. Although the passengers are unpleasant, based on the patient’s experience, he knows that thoughts and emotions cannot physically hurt him. The patient must be willing to listen to the threats of the passengers in order to drive the bus towards independence.
It is important to note that it takes time to develop the ability to consistently meet difficult experiences with willingness because the control agenda has been well practiced. Clinician disclosures that they also get stuck in avoidance/control strategies are useful because it normalizes the patient’s experience. Such disclosures also send an important message that this is not a problem reserved for people in therapy or with mental health diagnoses, but for all humans who live in cultures that reinforce the notion that one is only normal if they are happy. The patient and clinician can work to minimize barriers to willingness and value-based behaviour, such as fusion, impulsivity, and reactivity of suicidal thoughts and behaviours.
Targeting the Fusion, Impulsivity, and Reactivity of Suicidal Thinking
ACT includes a host of techniques to facilitate patients’ ability to experience distress without needing to react to it or avoid it. Similarly, ACT techniques can be used to undermine the control of rigidly held beliefs and suicidal thinking (e.g. “I can’t keep living with this pain”, “killing myself is the only way out of this problem”). This work can free the patient from engaging in the control agenda, create the opportunity for flexible thinking, and facilitate more meaningful volitional behaviour. ACT targets avoidant/reactive behaviour and unhelpful cognitions by teaching patients how to practice mindful self-observation. Patients learn how to stay focused on the present moment and observe their thoughts, allowing a thought to just be a thought, rather than necessarily an accurate reflection of reality. This can give patients the ability to pause and choose their actions instead of simply reacting. Thus, mindfulness exercises are typically engaged in every session and assigned as daily home practice.
When working with patients who are considering suicide, it is particularly important to directly target thinking and conditional rules the patient associates with reasons for dying. These thoughts should be identified and objectified when they arise to create a new posture of noticing thoughts as mental events rather than necessarily believing them. One method is to use objectifying language throughout therapy. ACT therapists often respond to the patient with phrases like: “You can thank your mind for that”, “So your mind is saying…”, “Is that your everything-is-hopeless thought creeping up again?”. If patients struggle with continuing to view thoughts as literal truths, it can be powerful to pull from patients’ experiences of times their minds were wrong despite a sense of certainty (e.g. about where they left their keys or predictions that others were mad at them) to create the possibility that their mind might also be wrong when it says suicide is the only answer.
Suicide-related cognitions can also be targeted in defusion exercises. For example, therapists can have patients write suicide-related thoughts on index cards and then manipulate the way the patient is holding the cards to illustrate the different relationships or stances we can take when interacting with these thoughts (e.g. becoming engrossed in them and pulled away from present-moment-valued activities that would usually serve as protective factors or holding them lightly on the lap and continuing to engage in meaningful conversation even though they are there in the background). The way the patient reads the thoughts can also be manipulated (e.g. comparing the impact of reading the thoughts as written versus adding “I notice I’m having the thought that….”; see Harris, 2009).
Developing and Strengthening a Value-Driven Life
Identifying values and setting goals for committed action in accordance with those values enhances protective factors. This part of ACT work is powerful for suicide prevention because of its focus on engaging in new adaptive behaviours and constructing a meaningful life, rather than merely getting rid of things that death could functionally get rid of too (e.g. depression, substance use, thoughts about suicide). For example, one patient observed that living his value of health by going to the gym regularly led to meeting other people interested in their own health who then invited him to join the group for a baseball game. The protective factor of social support and belonging continued to grow from value-based behaviour.
There are many techniques for identifying core values and enhancing committed action (see values assessment section). Key questions to ask the client in identifying values include “What would you like your life to stand for?” “Can you name some things you care about that I could not pay you enough to stop caring about?” ACT clinicians use metaphors and imaginal exercises to really flesh this out. For example, the 80th birthday party exercise asks the client to imagine hearing a speech from someone they care about who knows them well. The patient is encouraged to imagine this person saying whatever it is that the patient would most love to hear them say about who the patient is and what the patient stands for. Clinicians can point out that people rarely note what a nice car someone drives or how much money they earn, but are more likely to describe being a loving family member, a life-long learner, lover of nature, etc. (Harris, 2009).
The rubber meets the road when people put values into action. Examples include showing you care about others by treating them with kindness and compassion; working out to bring alive the value of personal health; reading to enact the value of personal growth, etc. Collaboratively assigning action homework between sessions allows the clinician to guide the patient in learning how to identify and commit to valued actions, and to foresee potential barriers (e.g. unwanted emotions) and work around them.
ACT clients develop a new way of guiding their everyday behaviour: asking themselves if their next action serves their values or serves the control agenda. Their internal compass that used to be bounded by psychological rigidity and guide them to experiential avoidance is now freed by psychological flexibility to guide them towards core values and a life worth living. Once clients have learned how to hold unwanted experiences while continuing to move in valued directions, they can build a life they will want to live and suicide will no longer be a viable option.
References
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45.
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., … Williams, J. M. G. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and non-meditating samples. Assessment, 15(3), 329–342.
Bahraini, N. H., Devore, M. D., Monteith, L. L., Forster, J. E., Bensen, S., & Brenner, L. A. (2013). The role of value importance and success in understanding suicidal ideation among Veterans. Journal of Contextual Behavioral Science, 2(1), 31–38.
Bahraini, N. H., Gerber, H. R., Monteith, L. L., Forster, J. E., Hostetter, T. A., & Brenner, L. A. (2016). Experiential avoidance and suicidal ideation among veterans exposed to combat Trauma. Manuscript in preparation.
Bardeen, J. R., & Fergus, T. A. (2016). The interactive effect of cognitive fusion and experiential avoidance on anxiety, depression, and posttraumatic stress symptoms. Journal of Contextual Behavioral Science, 5(1), 1–6.
Beck, A. T., Kovacs, M., & Weissman, A. (1979). Assessment of suicidal intention: The scale for suicide ideation. Journal of Consulting and Clinical Psychology, 47(2), 343–352.
Beck, A. T., Steer, R. A., Kovacs, M., & Garrison, B. (1985). Hopelessness and eventual suicide: a 10-year prospective study of patients hospitalized with suicidal ideation. American Journal of Psychiatry, 142(5), 559–563.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., Segal, Z. V., Abbey, S. … Devins, G. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241.
Blackledge, J. T., & Ciarocchi, J. (2006). Personal values questionnaire. Wollongong, Australia: Department of Psychology, University of Wollongong, Australia.
Bond, F. W., Hayes, S. C., Baer, R. A., Carpenter, K. M., Guenole, N., Orcutt, H. K., … Zettle, R.D. (2011). Preliminary psychometric properties of the acceptance and action questionniare-II: A revised measure of psychological flexibility and experiential avoidance. Behavior Therapy, 42(4), 676–688.
Branstetter-Rost, A., Cushing, C., & Douleh, T. (2009). Personal values and pain tolerance: Does a values intervention add to acceptance? The Journal of Pain, 10(8), 887–892.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848.
Bryan, C. J., Ray-Sannerud, B. R., & Heron, E. A. (2015). Psychological flexibility as a dimension of resilience for posttraumatic stress disorder, depression, and risk for suicidal ideation among Air Force personnel. Journal of Contextual Behavioral Science, 4(4), 263–268.
Cardaciotto, L., Herbert, J. D., Forman, E. M., Moitra, E., & Farrow, V. (2008). The assessment of present-moment awareness and acceptance: The Philadelphia mindfulness scale. Assessment, 15(2), 204–223.
Chesin, M. S., Interian, A., Kline, A., Benjamin-Phillips, C., Latorre, M., & Stanley, B. (2016). Reviewing mindfulness-based interventions for suicidal behaviour. Archives of Suicide Research, 20(4), 507–527.
Chesin, M. S., & Jeglic, E. L. (2016). Factors associated with recurrent suicidal ideation among racially and ethnically diverse college students with a history of suicide attempt: The role of mindfulness. Archives of Suicide Research, 20(1), 29–44.
Chesin, M. S., Sonmez, C. C., Benjamin-Phillips, C. A., Beeler, B., Brodsky, B. S., & Stanley, B. (2015). Preliminary effectiveness of adjunct mindfulness-based cognitive therapy to prevent suicidal behaviour in outpatients who are at elevated suicide risk. Mindfulness, 6(6), 1345–1355.
Chiles, J. A., & Strosahl, K. D. (2005). Clinical manual for assessment and treatment of suicidal patients. Arlington, VA: American Psychiatric Publishing.
Chioqueta, A. P., & Stiles, T. C. (2007). Dimensions of the dysfunctional attitude scale (DAS-A) and the automatic thoughts questionnaire (ATQ-30) as cognitive vulnerability factors in the development of suicide ideation. Behavioural and Cognitive Psychotherapy, 35(05), 579–589.
Ciarrochi, J., & Bailey, A. (2008). A CBT-practitioner’s guide to ACT: How to bridge the gap between cognitive behavioral therapy and acceptance and commitment therapy. Oakland, CA: New Harbinger Publications Inc.
Cloitre, M. (2013, August). Skills Training in Affect and Interpersonal Regulation (STAIR). Retrieved from https://www.ptsd.va.gov/professional/continuing_ed/STAIR_online_training.asp.
Coleman, D., & Casey, J. T. (2007). Therapeutic mechanisms of suicidal ideation: The influence of changes in automatic thoughts and immature defenses. Crisis, 28(4), 198–203.
Cougle, J. R., Keough, M. E., Riccardi, C. J., & Sachs-Ericsson, N. (2009). Anxiety disorders and suicidality in the national comorbidity survey-replication. Journal of Psychiatric Research, 43(9), 825–829.
Ducasse, D., René, E., Béziat, S., Guillaume, S., Courtet, P., & Olié, E. (2014). Acceptance and Commitment Therapy for management of suicidal patients: A pilot study. Psychotherapy and Psychosomatics, 83(6), 374–376.
Ellis, T. E., & Rufino, K. A. (2016). Change in experiential avoidance is associated with reduced suicidal ideation over the course of psychiatric hospitalization. Archives of Suicide Research, 20(3), 426–437.
Forkmann, T., Wichers, M., Geschwind, N., Peeters, F., van Os, J., Mainz, V., & Collip, D. (2014). Effects of mindfulness-based cognitive therapy on self-reported suicidal ideation: Results from a randomized controlled trial in patients with residual depressive symptoms. Comprehensive Psychiatry, 55(8), 1883–1890.
Fresco, D. M., Moore, M. T., van Delmen, M. H. M., Segal, Z. V., Ma, S. H., Teasdale, J. D., & Williams, J.M.G. (2007). Initial psychometric properties of the experiences questionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38(3), 234–246.
Gillanders, D. T., Bolderston, H., Bond, F. W., Dempster, M., Flaxman, P. E., Campbell, L., … Remingotn, B. (2014). The development and validation of the cognitive fusion questionnaire. Behavior Therapy, 45(1), 83–101.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54.
Guerreiro, D. F., Cruz, D., Frasquilho, D., Santos, J. C., Figueira, M. L., & Sampaio, D. (2013). Association between deliberate self-harm and coping in adolescent: A critical review of the last 10 years’ literature. Archives of Suicide Research, 17(2), 91–105.
Gutierrez, P. M., Osman, A., Barrios, F. X., & Kopper, B. A. (2001). Development and initial validation of the Self-Harm Behavior Questionnaire. Journal of Personality Assessment, 77(3), 475–490.
Harris, R. (2009). The house of ACT. In C. Honeychurch (Ed.), ACT made simple (pp. 33–39). Oakland, CA: New Harbinger Publications Inc.
Hayes, S. C., Bissett, R., Roget, N., Padilla, M., Kohlenberg, B. S., Fisher, G., … Niccolls, R. (2004). The impact of acceptance and commitment training and multicultural training on the stigmatizing attitudes and professional burnout of substance abuse counselors. Behavior Therapy, 35(4), 821–835.
Hayes, S. C., Levin, M. E., Plumb-Vilardaga, J., Villatte, J. L., & Pistorello, J. (2013). Acceptance and Commitment Therapy and contextual behavioural science: Examining the progress of a distinctive model of behavioral and cognitive therapy. Behavior Therapy, 44(2), 180–198.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: Model, processes and outcomes. Behavior Research and Therapy, 44(1), 1–25.
Hayes, S. C., Pistorello, J., & Biglan, A. (2008). Acceptance and commitment therapy: Model, data, and extension to the prevention of suicide. Brazilian Journal of Behavioral and Cognitive Therapy, 10(1), 81–102.
Hayes, S. C., Pistorello, J., & Levin, M. E. (2012a). Acceptance and commitment therapy as a unified model of behavior change. The Counseling Psychologist, 40(7), 976–1002.
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2012b). Acceptance and commitment therapy: The process and practice of mindful change (2nd ed.). New York, NY: The Guilford Press.
Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., & Strosahl, K. (1996). Experiential avoidance and behavioural disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152–1168.
Herzberg, K. N., Sheppard, S. C., Forsyth, J. P., Credé, M., Earleywine, M., & Eifert, G. H. (2012). The Believability of Anxious Feelings and Thoughts Questionnaire (BAFT): A psychometric evaluation of cognitive fusion in a nonclinical and highly anxious community sample. Psychological Assessment, 24(4), 877–891.
Jain, S., Shapiro, S. L., Swanick, S., Roesch, S. C., Mills, P. J., Bell, I., & Schwartz, G. E. (2007). A randomized controlled trial of mindfulness meditation versus relaxation training: Effects on distress, positive states of mind, rumination, and distraction. Annals of Behavioral Medicine, 33(1), 11–21.
Josepho, S. A., & Plutchik, R. (1994). Stress, coping, and suicide risk in psychiatric in patients. Suicide and Life Threatening Behavior, 24(1), 48–57.
Keilp, J. G., Sackheim, H. A., Brodsky, B. S., Oquendo, M. A., Malone, K. M., & Mann, J. J. (2001). Neuropsychological dysfunction in depressed suicide attempters. American Journal of Psychiatry, 158(5), 735–741.
Lamis, D. A., & Dvorak, R. D. (2014). Mindfulness, nonattachment, and suicide rumination in college students: The mediating role of depressive symptoms. Mindfulness, 5(5), 487–496.
Linehan, M. M., & Comtois, K. (1996). Lifetime parasuicide history. Seattle, WA: University of Washington. Unpublished work.
Lundgren, T., Luoma, J. B., Dahl, J., Strosahl, K., & Melin, L. (2012). The bull’s eye values survey: A psychometric evaluation. Cognitive and Behavioral Practice, 19(4), 518–526.
Luoma, J. B., & Vilatte, J. L. (2012). Mindfulness in the treatment of suicidal individuals. Cognitive and Behavioral Practice, 19(2), 265–276.
Marzuk, P. M., Hartwell, N., Leon, A. C., & Portera, L. (2005). Executive functioning in depressed patients with suicidal ideation. Acta Psychiatrica Scandinavica, 112(4), 294–301.
Miranda, R., Valderrama, J., Tsypes, A., Gadol, E., & Gallagher, M. (2013). Cognitive inflexibility and suicidal ideation: Mediating role of brooding and hopelessness. Psychiatry Research, 210(1), 174–181.
Mohammadkhani, P., Khanipour, H., Azadmehr, H., Mobramm, A., & Naseri, E. (2015). Trait mindfulness, reasons for living, and general symptom severity as predictors of suicide probability in males with substance abuse or dependence. Iranian Journal of Psychiatry, 10(1), 56–63.
Monteith, L. L., Pease, J. L., Forster, J. E., Homaifar, B. Y., & Bahraini, N. H. (2015). Values as moderators of the association between interpersonal-psychological constructs and suicidal ideation among veterans. Archives of Suicide Research, 19(4), 122–134.
Morrison, R., & O’Connor, R. C. (2011). A systematic review of the relationship between rumination and suicidality. Suicide and Life Threatening Behavior, 38(5), 523–538.
Neuringer, C., & Lettieri, D. J. (1971). Cognition, attitude, and affect in suicidal individuals. Suicide and Life Threatening Behavior, 1(2), 106–124.
Nock, M. K., Borges, G., Bromet, E. J., Alonso, J., Angermeyer, M., Beautrais, A., … Williams, D. (2008a). Cross-national prevalence and risk factor for suicidal ideation, plans, and attempts. British Journal of Psychiatry, 192(2), 98–105.
Nock, M. K., Borges, G., Bromet, E. J., Cha, C. B., Kessler, R. C., & Lee, S. (2008b). Suicide and suicidal behaviour. Epidemiologic Reviews, 30(1), 133–154.
Nock, M. K., Holmberg, E. B., Photos, V. I., & Michel, B. D. (2007). Self-injurious thoughts and behaviours interview: Development, reliability, and validity in an adolescent sample. Psychological Assessment, 19(3), 309–317.
Norton, P. J., Temple, S. R., & Pettit, J. W. (2008). Suicidal ideation and anxiety disorders: Elevated risk or artifact of comorbid depression? Journal of Behavior Therapy and Experimental Psychiatry, 39(4), 515–525.
Perrah, M., & Wichman, H. (2010). Cognitive rigidity in suicide attempters. Suicide and Life Threatening Behavior, 17(3), 251–255.
Pettit, J. W., Temple, S. R., Norton, P. J., Yaroslavsky, B. S., Grover, K. E., Morgan, S. T., & Schatte, D.J. (2009). Thought suppression and suicidal ideation: Preliminary evidence in support of a robust association. Depression and Anxiety, 26(8), 758–763.
Plumb, J. C., Stewart, I., Dahl, J., & Lundgren, T. (2009). In search of meaning: Values in modern clinic behaviour analysis. The Behavior Analyst, 32(1), 85–103.
Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K. V., Oquendo, M. A., … Mann, J. J. (2011). The columbia-suicide severity rating scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 168, 1266–1277.
Salters-Pedneault, K., Tull, M. T., & Roemer, L. (2004). The role of avoidance of emotional material in the anxiety disorders. Applied Preventive Psychology, 11(2), 95–114.
Sandoz, E. K., & Hebert, E. R. (2015). Meaningful, reminiscent, and evocative: An initial examination of four methods of selecting idiographic values-relevant stimuli. Journal of Contextual Behavioral Science, 4(4), 277–280.
Serpa, G. J., Taylor, S. L., & Tillisch, K. (2014). Mindfulness-based stress reduction (MBSR) reduces anxiety, depression, and suicidal ideation in veterans. Medical Care, 52(12), 19–24.
Shafran, R., Thordarson, D. S., & Rachman, S. (1996). Thought action fusion in obsessive-compulsive disorder. Journal of Anxiety Disorders, 10(5), 379–391.
Stanley, B., & Brown, G. K. (2012). Safety planning intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioral Practice, 19(2), 256–264.
Strosahl, K., Robinson, P., & Gustavsson, T. (2012). Brief interventions for radical change: Principles and practice of focused acceptance and commitment therapy. Oakland, CA: New Harbinger Publications.
Walser, R. D., Garvert, D. W., Karlin, B. E., Trockel, M., Ryu, D. M., & Taylor, C. B. (2015). Effectiveness of acceptance and commitment therapy in treating depression and suicidal ideation in veterans. Behaviour Research and Therapy, 74, 25–31.
Wegner, D. M. (1994). Ironic processes of mental control. Psychological Review, 101(1), 34–52.
Williams, M. J. G., & Broadbent, K. (1986). Distraction by emotional stimuli: Use of a stroop task with suicide attempters. British Journal of Clinical Psychology, 25(2), 101–110.
Williams, M. J. G., Duggan, D. S., Crane, C., & Hepburn, S. (2011). Modes of mind in suicidal processes: The potential role of mindfulness in changing minds. In R. C. O’Connor, S. Platt, & J. Gordon (Eds.), International handbook of suicide prevention: Research, policy, and practice (pp. 401–418). Oxford, UK: Wiley.
Wilson, K. G., Sandoz, E. K., Kitchens, J., & Roberts, M. E. (2010). The valued living questionnaire: Defining and measuring valued action within a behavioral framework. The Psychological Record, 60(2), 249–272.
Wilson, K. G., Stelzer, J., Bergman, J. N., Kral, M. J., Inayatullah, M., & Elliott, C. A. (1995). Problem solving, stress, and coping in adolescent suicide attempts. Suicide and Life Threatening Behavior, 25(2), 241–252.
World Health Organization (WHO). (2016). “Suicide Data”. Retrived June 22, 2016 from http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/.
Zettle, R. D., & Hayes, S. C. (1986). Dysfunctional control by client verbal behavior: The context of reason giving. The Analysis of Verbal Behavior, 4, 30–38.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Nature Singapore Pte Ltd.
About this chapter
Cite this chapter
Barnes, S.M., Smith, G.P., Monteith, L.L., Gerber, H.R., Bahraini, N.H. (2017). ACT for Life: Using Acceptance and Commitment Therapy to Understand and Prevent Suicide. In: Kumar, U. (eds) Handbook of Suicidal Behaviour. Springer, Singapore. https://doi.org/10.1007/978-981-10-4816-6_26
Download citation
DOI: https://doi.org/10.1007/978-981-10-4816-6_26
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-4815-9
Online ISBN: 978-981-10-4816-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)