
Abstract
Refractory secretory otitis media, without improvement after conservative treatments, such as antibiotics, eustachian tube inflation or previous tympanostomy alone.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Facial Nerve
- Tympanic Membrane
- External Auditory Canal
- Chronic Suppurative Otitis Medium
- Ossicular Chain
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Tympanostomy Tubes
Indications
-
1.
Refractory secretory otitis media, without improvement after conservative treatments, such as antibiotics, Eustachian tube inflation or previous tympanostomy alone.
-
2.
Glue ear or severe atelectasis.
-
3.
Severe conductive hearing loss due to negative middle ear pressure and having an effect on language development.
-
4.
Recurrent acute otitis media.
-
5.
Abnormal patency of Eustachian tube.
-
6.
Hyperbaric oxygen therapy.
Contraindications
Systemic conditions with patient not suitable for local or general anesthesia.
Operative Procedures
-
1.
Remove cerumen, then sterilize EAC with 0.1 % thimerosal solution.
-
2.
Tympanic membrane is incised full-thickness under the operating microscope. The length of the incision is about 2–4 mm, and should match the diameter of the inner flange of ventilating tube. Considering manubrium of malleus as vertical axis, umbo of tympanic membrane as horizontal axis, tympanic membrane can be divided into four quadrants, anterior-superior, anterior-inferior, posterior-superior and posterior-inferior. The incision is usually located in the anterior-inferior quadrant of the membrane for better drainage.
-
3.
Drainage of middle ear fluid, and lavage the cavity with the mixed solution of dexamethasone and α chymotrypsin.
-
4.
Tympanostomy tube in position.
Special Comments
-
1.
It is necessary to inspect the tympanic membrane under the microscope preoperatively. A blue or red color of the membrane may indicate a high jugular bulb (more common on right side) or glomus tumor. One should also look for pulsation behind the tympanic membrane.
-
2.
It is better to use a ventilating tube made of Teflon for less infection and less occlusion. Caution: a silicone tube may result in the formation of granulation tissue after prolonged intubation. Shepard and Armstrong Grommets are suitable for most cases, while Goode T Grommet have an increased risk of residual tympanic membrane perforation after long term use ventilation.
-
3.
The incision should avoid the posteriorsuperior quadrant of the drum in order to protect the ossicular chain. In case of long-term intubation, it is better to place the incision in front of the malleus handle.
-
4.
The incision should not be too close to the tympanic annulus or umbo of tympanic membrane for most stable placement.
-
5.
The incision should be made and the drainage tube should be placed in a healthy segment of the tympanic membrane.
-
6.
The EAC should be kept dry. The ear should be reviewed regularly. Avoid any kind of fluid, and apply antibiotic ear drops for infection or apply heparin if the tube is occluded.
Complications
-
1.
Injury of ossicular chain: this is uncommon if the ventilating tube is placed in the antero-inferior quadrant under operating microscope.
-
2.
Otorrhea after tympanostomy tube placement: Avoid infection by sterilizing the operating field carefully and lavaging the external canal with a solution containing antibiotics and glucocorticoid. Otorrhea may occur in some children despite these measures. If otorrhea occurs, apply antibiotic ear drops. Refractory otorrhea requires regular cleaning of the external canal and aspiration of middle ear fluid.
-
3.
A residual perforation following tube removal may take 1 or 2 years to fully heal spontaneously.
-
4.
Tube displaced into the tympanic cavity: this may be caused by an oversized incision or drum atrophy. If this occurs, the tube may be removed via the original or an extended incision.
-
5.
Bleeding from high jugular bulb: A high bulb appears as a dark red structure beneath the tympanic membrane and should be identified before tympanostomy, to avoid injury. If bleeding occurs, stop the operation immediately and pack the canal with gelfoam and antibiotic gauze for hemostasis.

Exposure of tympanic membrane
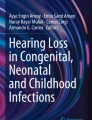
Remove cerumen from the external canal, sterilize the operation field with 0.1 % thimerosal solution. Expand external canal by otoscope or nasoscope, expose tympanic membrane under operating microscope. The tympanic membrane has lost it’s normal gloss and appears yellow. A dilated capillary can be seen on the pars tensa, and the tympanic cavity contains fluid

Myringotomy
The myringotomy is carried out with a myringotomy knife in the anteroinferior quadrant of the drum, remaining 3 mm away from the tympanic annulus. The length of the incision should match the diameter of the inner flange of the ventilating tube. In cases of atelectasis, the myringotomy should be made over the deepest possible region of the hypotympanum

Drainage of middle ear effusion
After the effusion is aspirated using the smallest possible suction tubes, the inner wall of tympanic cavity is exposed. If the secretion is viscous, an adjuvant incision may be performed at the posteroinferior quadrant to aid aspiration

Tympanic cavity irrigation
Irrigate and aspirate the tympanic cavity with a mixed solution of dexamethasone and α chymotrypsin gently and repeatedly

Placement of the ventilating tube
A ventilating tube is introduced into the external auditory canal carefully with a specialized tympanic cavity tubing pusher. One side of the tube is inserted into the incision first, then it is rotated into the tympanic cavity. Finally, adjust the position of the ventilating tube with a 1.5 mm, 45° hook

Check the position of the ventilating tube
After the placement of the ventilating tube, its position and stability should be checked. In this case, there is some clear liquid in the tube lumen, the length of the incision is appropriate, and the tube is correctly positioned

Adjust the position of the ventilating tube
Aspirate blood and liquid from around the ventilating tube, and adjust the position of the tube if necessary. If the tube is displaced into the tympanic cavity, grasp the blue strap on the tube and remove it using a large straight alligator forceps, then reposition the tube correctly
Myringoplasty
Indications
-
1.
The conducting function of ossicular chain is normal.
-
2.
The size of the perforation is medium or large
-
3.
Small perforation but the residual drum is atrophic
-
4.
The edges of the perforation are infolded.
-
5.
Persisting perforation despite cautery and application of ointment
-
6.
The ossicular chain should be evaluated when a pre-operative patch test fails to improve hearing.
Contraindications
-
1.
Middle ear cholesteatoma.
-
2.
Acute suppurative otitis media.
-
3.
Acute infection or active chronic suppurative otitis media.
-
4.
Ear Pseudomonas aeruginosa infection disease in diabetes mellitus patients.
-
5.
Patient unfit for surgery.
Operative Procedures
-
1.
Anesthesia: General or local anesthesia is used in adults, and general anesthesia is used in children. The local anesthesia is injected in four quadrants just lateral to the bone external canal and 2 % tetracaine solution is instilled in the tympanic cavity for surface anesthesia during surgery.
-
2.
The preparation of the graft: the temporalis fascia is harvested from the side of the affected ear. A horizontal incision approximately 2.5 cm long is made, 2–3 cm above the auricle. After separating the subcutaneous tissue, the tough white fascia close to the temporal muscle is exposed. The fascia is separated from the underlying muscle. The graft has a diameter of 1.5–2 cm. The graft is spread on a block and any excess fat and muscle are removed. The fascia is placed in the 75 % alcohol until it is used.
-
3.
The first skin incision starts from the 12 o’clock position of EAC and carried down to the bone. It is extended laterally between the tragus and the crus of helix for about 1.0 cm.
-
4.
The second incision is semi-circumferential and performed just medial to the bony-cartilaginous junction. It starts from the 6 o’clock position of EAC, and remains 5 mm lateral to the tympanic annulus along the posterior meatal wall in an ascending spiral fashion to meet the first incision. The edges of the perforation are freshened with a straight needle before the tympanomeatal flap is elevated.
-
5.
Elevation of meatal skin flap: An articulated retractor is introduced to expose the operating field. The skin and periosteum of EAC are separated from the underlying bone to the level of the tympanic annulus. The overhanging suprameatal spine is removed using a diamond burr or osteotome.
-
6.
The epithelial layer of the tympanic membrane remnant is separated from the fibrous layer, superiorly, anteriorly and inferiorly in sequence. This prepares the bed for the total overlay grafting technique. However if one edge of the perforation is close to the tympanic annulus, the tympanomeatal flap is raised lifting the annulus to enter tympanic cavity for the combined underlay grafting technique.
-
7.
In the combined underlay grafting procedure, one should inspect the tympanic cavity and ossicular chain after the tympanomeatal flap is elevated when an ossicular problem is suspected. Care should be taken to protect the chorda tympani nerve when separating the fibrous tympanic annulus.
-
8.
The long process of the incus and the incudostapedial joint are exposed with removal of some bone from the postero-superior canal wall.
-
9.
After aspiration of blood, the condition of the tympanic cavity and the mobility of the ossicular chain are examined. Any infected material is removed. Gelfoam pledgets soaked in antibiotic solution are placed in the tympanic cavity.
-
10.
The temporalis fascia is introduced between the epithelial and the fibrous layer of the tympanic membrane remnant (for the total overlay grafting technique); or placed between the tympanomeatal flap and the bony canal wall. If there is little or no anterior tympanic membrane remnant, the graft is inserted against the anterior wall of the tympanic cavity and pledgets of gelfoam are placed in the middle ear to support it. The graft is placed lateral to the malleus handle.
-
11.
Repositioning the meatal skin flap: the meatal skin flap and tympanic membrane remnant are replaced in their original position, covering the fascia. The graft should not extend beyond the external canal incision. The fascia is adjusted to cover the perforation.
-
12.
The external canal is packed with gelfoam and a strip of iodoform gauze.
-
13.
Incision closure.
Special Comments
-
1.
The condition of the middle ear should be explored in cases with a marginal perforation.
-
2.
The epithelial layer of the drum must be preserved during its elevation. If this is not achieved, the combined underlay grafting technique will be used.
-
3.
Removal of epithelial remnants: after the tympanomeatal flap is elevated, care must be taken to remove any residual epithelial remnants on the surface of the fibrous layer of the tympanic membrane to prevent inclusion under the graft.
-
4.
Protection of the chorda tympani nerve: The chorda tympani nerve should be preserved while elevating the posterior tympanomeatal flap and separating the tympanic annulus. The nerve is identified as a cord-like structure along the tympanic sulcus. It should be carefully dissected free from the sulcus and the bone.
-
5.
Care should be taken not to damage the ossicular chain.
-
6.
Ensure that the graft covers the perforation completely. Gentle even pressure should be used when filling the external canal with the gelfoam and gauze.
Complications
-
1.
Incomplete closure of the perforation: this complication may result from the inadequate separation of the epithelial layer from the fibrous layer of the tympanic membrane remnant. The local anesthetic should be injected deep to the epithelial layer to make the separation easier. One must ensure a strict intraoperative aseptic technique. The ear canal packing should be removed within 2 weeks of surgery.
-
2.
Formation of Cholesteatoma deep to the repaired tympanic membrane: this complication occurs when remnants of epidermis have been left on the margin of perforation. The growth of these remnants leads to the formation of the new cholesteatoma lateral to the fibrous layer of the tympanic membrane.
-
3.
Retraction pocket: this complication results from the inadequate Eustachian tube function or tympanic membrane adhering to the medial wall of the middle ear. This complication can be avoided by placing gelfoam pledgets soaked in the antibiotic solution in the tympanic cavity.
-
4.
Thick tympanic membrane: this complication occurs if the graft is too thick. Excess fat and muscle tissue must be removed from the fascia prior to its insertion.
-
5.
Blunting of the anterior tympanomeatal angle: This can occur due to the inadequate fixation of the anteroinferior graft by gelfoam pledgets.
Incomplete fusion of the drum to the manubrium of malleus: this complication is often seen in the total overlay grafting procedure, and occurs when the graft shrinks and becomes detached from the malleus handle.
-
6.
Stenosis of the external auditory canal: this complication can occur due to extensive injury to the canal skin, postoperative infection and proliferation of granulation tissue.
Surgery 1: Myringoplasty

Endaural incision
The fascia is harvested from the temporal muscle above the affected ear and dried in 75 % ethanol. The first skin incision is made at the 12 o’clock position of EAC just lateral to the bony-cartilaginous junction and carried down to the bone. An outward prolongation of about 1.0 cm in length is made between the tragus and the crus of helix, and then under the operating microscope the first incision is extended inward to a point about 0.8–1.0 cm lateral to the tympanic annulus. The second incision starts from the 6 o’clock position of EAC, and remains 5 mm lateral to the tympanic annulus along the posterior meatal wall in an ascending spiral (or curved) fashion to meet the first incision. The soft tissue in the junction of these two incisions often needs to be cut with a sharp knife

Elevation of the meatal skin flap and the epithelial layer of the posterior tympanic membrane
Remove the overhanging suprameatal spine using a diamond burr or chisel. Separate the skin of EAC to the level of the tympanic annulus and elevate the epithelial layer of the remnant tympanic membrane across the tympanic sulcus. Expose the lateral process of malleus by separating the epithelial layer from the fibrous layer covering this process

Separate the epithelial layer from the inferior remnant of tympanic membrane
Separate the epithelial layer from the fibrous layer of the tympanic membrane postero-inferiorly, inferiorly and antero-inferiorly, respectively. Then, the epithelial layer is separated from the fibrous layer totally and the tympanomeatal flaps are elevated anteriorly like a swinging door

Elevation of the tympanomeatal flaps
After the meatal portion and the tympanic portion of the flap are raised totally, the tympanomeatal flap is completed. Preserve the pedicle including the skin of the anterior wall of the external canal. This will prepare the bed to accept the graft. A posterosuperior tympanomeatal flap is raised, exposing the full-view of the fibrous layer and perforation edges, including the calcified plaque in the fibrous layer of the tympanic membrane in this case

Removal of calcified plaque in the fibrous layer of the tympanic membrane
Pierce around the margin of the calcified plaque in the tympanic membrane remnant and remove the plaque intact

Expose the manubrium of malleus after removing the calcified plaque
Remove the calcified plaque in front of the manubrium of the malleus to expose it completely. Care should be taken to avoid altering the position of the normal fibrous layer

Inspecting the incudostapedial joint
After removing the sclerosis of the fibrous layer, the incudostapedial joint is exposed. The mobility and integrity of the ossicular chain is tested and no abnormality was found in this case

Introduction of the temporal fascia
The graft is cut with scissors to the appropriate size to cover the perforation. The graft is introduced between the tympanomeatal flaps and the fibrous layer of the tympanic membrane. Care should be taken to ensure that the posterior edge of the graft does not protrude posterior to the line of the second incision. The fascia should be placed flat, without folds, bulges or indentations

Repositioning the meatal skin flap and the epithelial layer of the drum
The tympanomeatal flaps are repositioned, keeping the fascia in contact with the tympanic annulus and between the epithelial layer and fibrous layer of the drum

Placing the gelfoam on the surface of the drum
Gelfoam pledgets soaked in antibiotic solution are placed in the external acoustic meatus, on the lateral surface of the tympanic membrane and covering the second incision

Packing the external meatus with a strip of iodoform gauze and closing the wound
The external canal is packed with 0.5–1.0 cm strip of iodoform gauze, and the incision is closed
Surgery 2: Myringoplasty

Endaural incision
The fascia is harvested from the temporal muscle above the affected ear and is dried in 75 % ethanol. The skin incision is made between the tragus and the crus of helix and an inward extension is made to a point about 0.8–1.0 cm lateral to the tympanic annulus. The second incision starts from the 6 o’clock position of EAC, and remains 5 mm lateral to the tympanic annulus along the posterior meatal wall in an ascending spiral fashion to meet the inner part of the first incision

Excising the perforation margins
The edges of the perforation are freshened with a hooked needle 3 mm away from its margin. Care must be taken to remove all epithelial remnants from the rim of the perforation

Separate the posterior epithelial layer of the tympanic membrane
Remove the overhanging suprameatal spine using a sharp diamond burr or chisel. Separate the meatal skin flap as far as the tympanic annulus and elevate the epithelial layer from the posterior remnant of the tympanic membrane across the tympanic sulcus. Then separate the epithelial layer from the fibrous layer of the tympanic membrane anteriorly to the manubrium of malleus

Separate the epithelial layer from the anterior part of tympanic membrane
The epithelial layer is separated from the fibrous layer, then the edges of the tympanic membrane perforation are excised

Remove the calcified plaque
Remove a calcified plaque in the fibrous layer posterior to the malleus

Repositioning the epithelial layer of the tympanic membrane
The transplant bed of tympanic membrane is created, and the epithelial layer of the tympanic membrane is repositioned. Inspect the edges of the perforation again

Check the extent of separation of two layers of the tympanic membrane
Use micro spatula to check separation of the epithelial layer and fibrous layer of the tympanic membrane remnant

Inspecting the tympanic cavity
The postero-superior part of fibrous annulus is raised from the tympanic sulcus, and the excess bone of the posterosuperior meatus is removed. The tympanic cavity and part of ossicular chain are visible. Pierce around the edge of the calcified plaque in the tympanic membrane remnant successively and remove the calcified plaque. Take care to preserve the normal fibrous layer as much as possible

Exposure of the chorda tympani nerve
The chorda tympani nerve is identified between the manubrium of malleus and the long process of the incus, along the line of the tympanic sulcus.Take care to separate the nerve along the tympanic sulcus to protect it from injury

Checking the auditory ossicles
After the excess bony overhang of the posterosuperior meatal wall is removed, the integrity of the incudostapedial joint and the mobility of the ossicular chain are tested (or inspected). They are both normal in this case

Introducing the temporal fascia graft
The graft is introduced between the fibrous layer of the tympanic membrane and the epithelial tympanomeatal flap

Repositioning the tympanic membrane
The tympanic membrane is placed in its original position. Care is taken to ensure the temporal fascia graft fully covers the perforation

Packing the ear canal
Placing the gelfoam on the surface of the drum, packing the external canal with a strip of iodoform gauze, and closing the incision
Tympanoplasty
Indications
-
1.
Tympanoplasty can be used in Chronic otitis media and mastoiditis patients (including cholesteatoma), but only when middle ear infection is controlled, the Eustachian tube is not obstructed and there is good cochlear function.
-
2.
Traumatic ossicular chain discontinuity
-
3.
Congenital middle ear malformation
-
4.
Ossicular erosion or fixation or tympanosclerosis from chronic otitis media
Contraindications
-
1.
Poor cochlear function
-
2.
Malignancy of the middle or external ear (combined with radiation therapy)
-
3.
Pseudomonal infection in diabetic patients
-
4.
Otogenic intracranial complications
-
5.
Patient unfit for surgery
Operative Procedures
-
1.
Anesthesia: Local anesthesia can be used in adults. General anesthesia is used for children. Local anesthetic solution is injected into the skin of the wall of the external auditory canal. Cotton wool soaked with 2 % decicaine is placed on the surface of the tympanic membrane around the perforation for additional surface anesthesia.
-
2.
Graft preparation: Temporalis fascia is harvested. A 2.5 cm long horizontal skin incision is made parallel to the hairline at the top of ear. After division of the subcutaneous tissue the white and tough fascia can be identified over the temporalis muscle. A circular fascial graft of 1.5–2.0 cm in diameter is taken. The graft is cleaned of muscle and loose connective tissue. It is placed in 75 % alcohol solution until use.
-
3.
The first incision: A longitudinal incision is made at the top of EAC, with a 1.0 cm lateral extension along anterior border of crus of helix.
-
4.
The second incision: Make a semicircular incision at bony part of auditory canal, which extends from 6 o’clock up to the inner end of first incision along the posterior wall 0.5 cm away from the tympanic annulus.
-
5.
Elevation of the EAC skin flaps: Elevate the skin and periosteum of EAC towards the tympanic annulus. Curette away the spine of Henle if is prominent.
-
6.
The epithelial layer of the tympanic membrane is separated from the fibrous layer in an anterior direction to form the bed for the graft in the inlay technique.
The drum remnant is elevated as one layer in the underlay technique.
-
7.
Once the tympanomeatal flap is prepared for the inlay technique, if exploration of the middle ear and ossicular chain is needed, the tympanic annulus can be elevated from the postero-superior part of the tympanic sulcus (right side from 9 to 12 o’clock position, left side from 12 to 3 o’clock position), whilst paying attention to protect the chorda tympani nerve.
-
8.
Part of the postero-superior wall of the external auditory canal can be removed with a curette or chisel to expose the long process of the incus and the incudostapedial joint.
-
9.
After entering the tympanic cavity, blood and any debris is suctioned to allow inspection of the ossicular chain and clearance of any disease associated with it.
-
10.
Placement of temporalis fascia: the fascia is inserted between the outer epithelial layer and fibrous inner layer of the tympanic membrane (inlay technique), or inserted under the drum and between the tympanomeatal flap and auditory canal bony wall. If there is no residual rim of the tympanic membrane anteriorly, the fascia is placed right to the anterior wall of the middle ear and a small extension is placed over the annulus to anchor the graft. The anterior and inferior middle ear space is well packed with gelfoam to ensure it stays in contact with the under surface of the drum remnant.
-
11.
If ossicular chain reconstruction is needed, the temporalis fascial graft is reflected forward with the tympanic membrane remnant to expose the middle ear space. Suitable materials and methods for reconstruction are selected depending on the status of ossicular chain.
-
12.
Repositioning the EAC skin flap: Replace the tympanomeatal flap with the graft that has been inserted. Ensure that the graft covers the perforation and does not extend laterally beyond the edge of the skin flap.
-
13.
Fill the EAC with gelatin sponge and then iodoform gauze.
-
14.
Suture the incision.
Special Comments
-
1.
Inject local anesthetic solution under the skin to cause blanching but avoid excessive swelling, bruising or disruption of the canal skin.
-
2.
Carefully dissect the tympanic membrane and handle of malleus, to avoid injury. The incudostapedial joint can be separated temporarily if necessary to prevent injury to the inner ear with consequent tinnitus, or even irreversible sensorineural hearing loss.
-
3.
Ensure the gelfoam placed in the middle ear is only lightly moistened with normal saline
-
4.
If an autograft incus is used to reconstruct the ossicular chain, ensure that it is healthy and does not contain cholesteatoma.
-
5.
Make sure the attic lateral wall is intact at the end of the procedure, with any defect repaired
Complications
-
1.
Perforation of ear drum: this may happen if the fascial graft is too small and does not cover the perforation completely, or if it is too large and does not lie correctly to make good contact with the recipient bed and develop a good blood supply.
-
2.
Lateral healing of the tympanic membrane: this is mostly caused by inappropriate graft placement and packing, either by excessive separation of anterior edge skin of the recipient bed or loss of and blunting of the acute angle between the tympanic membrane and the anterior EAC wall.
-
3.
Cholesteatoma: a small cholesteatoma or epidermoid can be seen frequently on the surface of tympanic membrane, or on the EAC recipient bed due to implantation of squamous epithelium. When this occurs, it can be removed simply in the clinic without harmful effects. This should be done early to avoid ingrowth of Cholesteatoma to the middle ear.
-
4.
Inner ear injury: dissection of disease or tympanosclerosis from the ossicular chain may cause inner ear damage if it is not done delicately. The stapes can even be dislocated, leading to inner ear injury and creating a pathway for infection to spread to the inner ear. Inner ear damage is seen more frequently in the aged and those with poor inner ear function.
-
5.
EAC stenosis: excessive trauma to the skin of the EAC, infection and proliferation of granulation can cause EAC stenosis.
Widening of the bony ear canal and repair of any areas skin loss with full-thick skin grafts will help prevent this.
-
6.
Tympanic membrane retraction pocket: when extensive removal of the postero-superior bony canal wall is required, a retraction pocket can occur even in the presence of normal Eustachian tube function. Bone defects in this area should be repaired with a cartilage composite graft to prevent formation of a retraction pocket which may progress to cholesteatoma.
-
7.
Facial palsy: facial nerve damage mostly occurs at the second genu, in the postero-superior region of the tympanic cavity, where dissection may be blind and the bony facial nerve canal is likely to be deficient leaving the nerve exposed and possibly herniating.
Chemicals (such as acetaldehyde and peroxyacetic acid) contained in the gelatin sponge used to pack the tympanic cavity may cause facial nerve protein denaturation.
Surgery 1: Tympanoplasty, ossiculoplasty

Endaural incision
A longitudinal incision is made at the top of EAC, and extended about 1.0 cm along anterior border of the crus of helix. The inner end of the incision stops 0.8–1.0 cm lateral to the pars flaccida of the tympanic membrane. The second incision is circumferential and made 0.5 cm behind the tympanic annulus. It extends from the 6 o’clock position, over the posterior EAC wall to meet the inner end of the first incision

Elevation of EAC Skin flap
The skin and periosteum of the EAC is elevated from the second incision inwards to the tympanic annulus. The dissection is carried out over a broad front avoid too much elevation in one area alone. The dissector is kept tightly on the bone and a fine bore sucker is used to avoid trauma to the flap which is often quite thin

Elevation of superior EAC skin flap
The posterior and inferior skin flap of the EAC is elevated, then the superior skin flap is reflected to the anterior wall. The anterior superior spine of bone is exposed and removed if it is too prominent.
This picture shows the bony part of superior wall of EAC to be eroded leading to expansion of the EAC. The inner end of the EAC skin has turned a yellow-white color due to inflammation

The tympanic membrane is elevated to expose the tympanic cavity.
After the skin flap of the EAC was elevated to the tympanic annulus, a large tympanic membrane perforation could be seen with no posterior residual rim. Part of the postero-superior bony EAC wall, between the 9 o’clock and 12 o’clock positions, was eroded, exposing the chorda tympani nerve. Part of the lateral attic wall is also missing and the ossicles were surrounded by granulation tissue. The pars flaccida was carefully elevated

The residual epithelial and fibrous layers of the tympanic membrane were separated from the lamina propria
In this case, there was no postero-superior residual rim of the tympanic membrane. The residual posterior and inferior epithelial layer of the tympanic membrane was separated from the fibrous layer. A calcified plaque can be seen on the surface of the inferior fibrous layer of the tympanic membrane

The recipient bed for repairing the tympanic membrane is prepared
The residual epithelial layer of the anterior tympanic membrane is elevated. Dissection should advance evenly from the antero-superior and antero – inferior walls of the EAC and converge on the incisions. The epithelial layer of the tympanic membrane is then replaced to check its integrity. It must be separated completely from the fibrous layer in the area where the fascial graft is to be placed

Exposure of the ossicles
The microscope is adjusted to look superiorly. The attic was partly open due to erosion of its lateral wall. Granulation tissue surrounding the ossicular chain was cleaned up. The malleus was absent and the incus long process was mostly missing. The stapes is surrounded by swollen mucous membrane binding it to the surface of the promontory. This picture shows the incus in the process of being removed

Tympanic membrane is replaced
EAC tympanic membrane flap is replaced. The tympanomeatal flap is totally separated from the bony wall and the residual fibrous layer of the tympanic membrane, making the recipient bed for repairing the tympanic membrane

Transplanted temporalis fascia is positioned for repair of the tympanic membrane
The temporalis fascia is inserted between the epithelial and fibrous layers of the tympanic membrane. The size of fascia is important and should not be folded over, but in direct contact with the residual fibrous layer of tympanic membrane and bony wall near the tympanic sulcus. The graft should cover the perforation completely to prevent a recurrent membrane defect

The incus has been removed and the stapes superstructure is seen
The tympanomeatal flap with the embedded temporalis fascia is reflected forwards to expose the tympanic cavity. After the incus is taken out, the stapes superstructure is seen to be intact. The anterior and inferior tympanic cavity is filled with erythromycin soaked gelatin sponge to support the temporalis fascial graft

Artificial ossicle (PORP) is positioned
After cleaning the disease from around the stapes, its mobility was checked and seen to be good. The ossicular prosthesis (PORP) was positioned on the stapes head. As there was a good fit between the cup of the prosthesis and the stapes head, no additional support was necessary to hold it in correct position

A cartilage graft was inserted between the lateral face of the prosthesis and the temporalis fascia
In order to prevent extrusion of the prosthesis a cartilage graft is taken from the crus of helix and inserted between the lateral face of the prosthesis and the temporalis fascia. A rectangular curved cartilage graft is also used to repair the deficient postero-superior bony EAC wall in the 9–12 o’clock position to prevent retraction of the repaired tympanic membrane

Transplanted fascia
The fascial graft is used to cover the surface of the ossicular prosthesis and the two cartilage grafts, making sure they remain in their correct position

Iodoform gauze is used to pack the EAC
The tympanomeatal flap is replaced and positioned with a dissector
Care is taken to ensure the fascia covers the perforation and does not extend beyond the lateral end of the skin flap. Gelatin sponge is used to cover the lateral surface of the drum and iodoform gauze pieces are placed to pack the EAC
Surgery 2: Tympanoplasty

Local anesthetic is injected
10 ml of local anesthetic solution in normal saline is mixed with 10 drops of 0.1 % epinephrine and injected as local infiltration anesthesia. The injection is performed at three to four points along the junction of the cartilage and bony parts of the EAC. The needle is inserted through the lateral skin on to the EAC bone and the infiltration is performed slowly to blanch the skin and anesthetize the skin

The first incision
A longitudinal incision is made at the top of EAC, and extended about 1.0 cm along anterior border of the crus of helix. Any bleeding vessels are coagulated with bipolar diathermy. The inner end of the incision stops 0.8–1.0 cm lateral to the pars flaccida of the tympanic membrane. The second incision is circumferential and made 0.5 cm behind the tympanic annulus. It extends from the from the 6 o’clock position, over the posterior EAC wall to meet the medial end of the first incision

The second incision
The second incision is made over the posterior bony auditory canal wall from the 6 o’clock position, 0.5 cm away from the tympanic annulus, to join the inner end of the first incision. The large perforation at the center of the pars tensa and the residual tympanic membrane can be seen

Elevation of EAC skin flaps
The skin and periosteum of the EAC are elevated from the bony wall along incisional margin to the tympanic annulus. The anterior skin flap is elevated and the anterior superior spine is exposed with sharp and blunt dissection. Any prominent anterior superior spine is removed. This is an important part of the procedure to expose the anterior part of the tympanic membrane and of the middle ear

Remnant epithelial layer and fibrous layer of the tympanic membrane are separated
The skin flap of the EAC is elevated to the tympanic annulus and whole remnant epithelial layer of the tympanic membrane is separated carefully upwards, forwards and downwards. The fibrous layer of the tympanic membrane is left in situ

Repositioning of EAC skin flap
After replacing the tympanomeatal flap, the integrity of the epithelial layer of tympanic membrane is checked to ensure that it is completely separated from the lamina propria. Any areas of adhesion are identified and separated. The site and size of the ear drum perforation are also assessed. The epithelial layer of the tympanic membrane is preserved as far as possible

A segment of the lateral bony wall of postero-superior tympanic cavity is chiseled off
If exploration of the ossicular chain or attic is required, the remaining base layer of the tympanic membrane (right side from 9 to 11 o’clock) is elevated from the tympanic sulcus. Bone can be removed delicately in small pieces to extend the exposure as required, avoiding injury to the chorda tympani and the ossicular chain

The long process of incus and incudostapedial joint are exposed
In order to explore the integrity and mobility of the ossicular chain, bone of the postero-superior EAC wall can be removed to expand the field of vision. This picture shows the lamina propria, chorda tympani nerve, long process of incus and stapes. The ossicular chain is seen to be intact and mobile

Relation between chorda tympani nerve and lamina propria
Zoom in with the microscope; identify the lamina propria extending from the tympanic sulcus. The chorda tympani nerve sits under the lamina propria lateral to the long process of the incus. The handle of the malleus and remaining lamina propria surrounding it are seen in the front of the field of vision

Repair of tympanic membrane; replacement of tympanomeatal flap.
Harvest the temporalis fascia at the beginning of the operation and stiffen it in 75 % alcohol solution. Lay it between the epithelial layer of tympanic membrane and the lamina propria, covering the perforation completely. Replace the lateral and tympanomeatal flaps, ensuring the fascia is well seated and fully covers the perforation, and does not extend lateral to the end of the tympanomeatal flap
Reconstruction of Ossicular Chain/Ossiculoplasty
Indications
-
1.
Chronic suppurative otitis media
-
2.
Abnormality of ossicular chain
-
3.
Traumatic ossicular chain disruption
-
4.
Otospongiosis (Otosclerosis)
-
5.
Tympanosclerosis
-
6.
Congenital cholesteatoma
Note: Chronic suppurative otitis media is the most common indication.
Contraindications
-
1.
Patients unfit for the operation
-
2.
Dysfunction of Eustachian tube
-
3.
Residual cholesteatoma in the tympanic cavity
-
4.
Perforation of ear drum with persistent discharge
-
5.
Acute otitis externa and otitis media
Operative Procedures
Different reconstructive methods and materials are used in various approaches to ossiculoplasty depending on the disease status and ossicular status (continuity and mobility). If possible, it is the best to make full use of autologous ossicles to reconstruct hearing. Maintaining the tympanic cavity and continuity and stability of the ossicular chain are two key points in ossiculoplasty.
-
1.
Incision: an endaural or a postauricular incision can be used, depending on the middle ear pathology and the preference of the surgeon
-
2.
The tympanomeatal flap, consisting of the tympanic membrane and the posterior external auditory canal skin are carefully elevated to expose the tympanic cavity adequately.
-
3.
Expose the lateral wall of epitympanic recess and explore the malleus.
-
4.
Open the epitympanic recess to completely remove cholesteatoma, and explore the incus and malleus.
-
5.
The antrum and mastoid should be opened until normal air cells and mucosa are reached.
-
6.
Evaluate the status and mobility of the residual ossicles and prepare available autologous ossicle(s) for further use.
-
7.
Select the type of ossicle to be transplanted, measure the length required, shape the ossicle for ossicular reconstruction.
-
8.
Reconstruction of ossicular chain: there are different types of reconstruction according to the status of the residual ossicular chain.
A. Manubrium of malleus -Head of stapes: this is applicable for ossicular chain disruption due to a missing incus, attic fixation of the malleus head or incus body, tympanosclerosis and so on. B. Manubrium of malleus-Footplate of stapes: this is applicable for the lesions where the incus and the stapes superstructure are damaged and the malleus and footplate of stapes are intact. C. Manubrium of malleus-Oval window: it is applicable for the lesions where the incus and stapes superstructure are absent and the malleus is intact. The oval window may need to be sealed with tissue (perichondrium, fascia or vein). D. Tympanic membrane-Head of stapes: this is applicable for lesions where the incus and malleus are absent and the stapes is intact. A partial ossicular substitute (PORP) can be used to bridge the gap between the tympanic membrane and head of stapes. E. Tympanic membrane- Footplate of stapes: this is applicable for lesions including absence of the malleus, incus and superstructure of stapes, but the footplate of stapes present and mobile. A total ossicular substitute (TORP) may be used to connect the tympanic membrane and footplate of stapes.
-
9.
The stabilization of reconstructed ossicular chain: there are a number of techniques used for stabilizing the ossicular chain, including residual manubrium of malleus, homogenous cartilage/perichondrium tissue and chorda tympani nerve, either used alone or in combination according to the actual situation. The chorda tympani nerve should be preserved for ossicular stabilization as far as possible.
-
10.
Reconstruction and packing of the external auditory canal.
Note: Many materials may be used for reconstruction of the ossicular chain: A. Autologous grafts: including residual ossicles, cortical bone and cartilage. B. Allogeneic grafts: including auditory ossicles, and nasal septum cartilage. C. Artificial ossicles: They are more commonly used and can be made of Teflon, silicone, ceramics, titanium, etc. Transplanted materials must meet the following criteria: no residual tissue antigen, no inflammatory or foreign body response in the middle ear, easy to shape, conducive to establishing a stable connection.
Special Comments
-
1.
Remove all disease and promote good ventilation of the new tympanic cavity.
-
2.
Assess the residual ossicular chain thoroughly.
-
3.
Retain or re-use healthy autologous materials as far as possible, such as ossicles and the tympanic membrane remnant.
-
4.
Various tissues and materials can be used to stabilize the reconstructed ossicular, such as manubrium of malleus, homogenous cartilage, chorda tympani nerve, fibrin glue, gelatin sponge and so on.
-
5.
Confirm the structural integrity and mobility of the stapes: a mobile footplate is required for successful ossicular reconstruction. Stapedectomy or stapedotomy may be considered at a second stage if the footplate is fixed. If the stapes arch is missing or disconnected, a direct connection to the footplate may be considered.
-
6.
Care should be taken not to damage the chorda tympani nerve or the tendon of the tensor tympani muscle when severing the neck of the malleus and removing the incus. The chorda tympani and the tensor tympani tendon can be used for fixing implanted ossicles or prostheses. (Disease processes often exist in the epitympanic recess, necessitating removal of the malleus. This favours ventilation and drainage of the epitympanic recess).
-
7.
Carefully measure the length of transplanted ossicles to prevent displacement or protrusion of ossicle, and to prevent fracture of the stapes arch or footplate.
-
8.
The external auditory canal should be carefully packed after myringoplasty and ossicular chain reconstruction, taking care not to deform the tympanic membrane or the reconstructed chain.
Complications
-
1.
Fixation of ossicles: Both residual lesions in the tympanic cavity or improper position of ossicles can lead to fixation of ossicles. The implanted ossicle or prostheses should be positioned in the center of the stapes footplate in order to acheive maximum hearing gain and avoid poor conduction.
-
2.
Displacement of ossicles: Implanted ossicles or prostheses that are too short can often result in displacement of ossicles. The best part of the tympanic membrane to connect with the reconstructed chain is the postero-superior quadrant.
-
3.
Ossicles protruding: A small disc of cartilage should be laid between the tympanic membrane and ossicular prosthesis in order to prevent it extruding. Re-perforation of the tympanic membrane may occur when implanted ossicles or prostheses are too long and apply excessive pressure to the repaired tympanic membrane.
-
4.
Fracture of stapes arch or footplate: This may occur when the implanted ossicles or prostheses are too long or too heavy.
-
5.
Transplanted ossicles may be absorbed.
Surgery 1: Mastoidectomy with reconstruction of external auditory canal and ossicular chain

Endaural incision and removal of the overhanging suprameatal spine
The first skin incision is made at the 12 o’clock position of EAC just lateral to the bony-cartilaginous junction and carried down to the bone, and then under the operating microscope the first incision is extended inward to a point about 0.8–1.0 cm lateral to the tympanic annulus. The second incision starts from the 6 o’clock position of EAC, and remains 6–8 mm lateral to the tympanic annulus along the posterior meatal wall in an ascending spiral (or curved) fashion to meet the first incision. The overhanging suprameatal spine can be removed by a small burr or chisel for good exposure

Elevation of the meatal skin flap
The meatal skin flap of posterio-superior part of the external auditory canal is elevated and cholesteatoma is seen in the notch of Rivinus in this case

Expose the tympanic cavity and the lateral wall of the epitympanic recess
The fibrous annulus of the tympanic membrane is dissected and separated from the posterior tympanic sulcus. The meatal skin flap and tympanic membrane are raised anteriorly to the level of short process of malleus. The tympanic cavity is thus exposed and the cholesteatoma in the postero-superior part of tympanic cavity can be seen. Care should be taken not to injure the chorda tympani nerve during the procedure

Remove cholesteatoma from the tympanic cavity
Remove part of the lateral wall of epitympanic recess. The chorda tympani nerve and cholesteatoma in the epitympanic recess are clearly exposed

Open the epitympanic recess
The attic is opened with an electric drill to expose the anterior border of attic to the same level as the anterior wall of external auditory canal. When the attic is partially opened, the extent of the cholesteatoma in the attic cavity can be determined, including any extension to the mastoid antrum

Expose the cholesteatoma of epitympanic recess completely
Continue to remove the lateral wall of epitympanic recess with a drill to expose epitympanic recess adequately. The epitympanic recess is filled with the cholesteatoma, which is seen extending to the aditus ad antrum

Expose the cortex of mastoid
Make an outward prolongation of the original incision and separate the periosteum from the mastoid surface. Replace the self-retaining retractor to adequately expose the upper part of mastoid cortex

Expose the disease in the tympanic antrum and mastoid cavity
An electric drill is used to open the antrum and mastoid to fully expose the cholesteatoma. Inflammatory granulation is seen in the aditus ad antrum after removal of cholesteatoma at this site. Surgical exposure should extended beyond the disease to see normal air cells and mucosa

Eradicate all disease from the mastoid
Disease in the antrum and mastoid cavity is removed totally and the walls of mastoid cavity are polished with a diamond burr. The upper wall of surgical cavity is the thin bony plate of the middle fossa. The lateral semicircular canal and facial nerve which are partially covered by the cholesteatoma can be seen at this point

Remove the head of malleus and cholesteatoma from the epitympanic recess
The cholesteatoma can also be hidden medial to the head of malleus. In order to eradicate all cholesteatoma, the head of malleus is removed. The superstructure of stapes is absent, but the footplate of the stapes is present and mobile

Reconstruction of the ossicular chain
A groove is drilled in the bone of the anterior and posterior arch of the epitympanic recess and opened mastoid cavity. The tympanic membrane was intact and the ossicular prosthesis (TORP, Spiggle & Theis, total titanium ossicle replacement prosthesis) is positioned to connect the tympanic membrane and footplate of stapes. It is important to place a small piece of cartilage between the tympanic membrane and the prosthesis to prevent later extrusion through the tympanic membrane

Reconstruction of external auditory canal and obliteration of operation cavity
The superior and partial posterior walls of external auditory canal are repaired with tragal cartilage and the mastoid cavity is closed off. After the reconstruction of the ossicular chain and the repair of tympanic membrane, the surgical cavity should be carefully filled by small pieces of absorbable gelatin sponge to prevent adhesion and displacement of reconstructed ossicles and transplanted cartilage

Packing of external auditory canal
The pedicled temporalis muscle is put in the defect of mastoid to support the reconstructed external canal wall. It is important to pack the external auditory canal carefully with the iodoform gauze to prevent canal stenosis and displacement of reconstructed ossicular chain
Surgery 2: The tympanoplasty and ossiculoplasty

Examine the tympanic membrane
The external auditory canal and tympanic membrane are carefully examined under the microscope. In this case, there is a small perforation in the pars tensa of the tympanic membrane, with a calcified plaque in the residual tympanic membrane

Elevate the tympanic membrane to enter the tympanic cavity
The underlay grafting technique is used for tympanoplasty in this case. The skin incision is made between the tragus and the root of helix, and an inward extension is made to a point about 1.0 cm lateral to the tympanic annulus. The second incision starts from the 6 o’clock position of the EAC, and remains 6–8 mm lateral to the tympanic annulus along the posterior meatal wall in an ascending spiral fashion to meet the inner part of the first incision. The tympanomeatal flap is elevated anteriorly to expose the tympanic cavity

Examine the incus and stapes
The excess bone of the postero-superior canal is removed. The incus and stapes are visible. There is hyperplastic fibrous tissue between the malleus and the incus. The cochleariform process is whitish, which is a sign of tympanosclerosis

Removal of the incus
The incus is taken out due to its fixation. The epitympanic recess is exposed sufficiently and the mobility of the stapes is evaluated carefully. The stapes and malleus are seen to have good mobility after removal of the incus

Dissect the chorda tympani nerve
Dissect the chorda tympani nerve from the tympanic sulcus and expose the mesotympanum and hypotympanum. The mucosa of the tympanic cavity is normal and smooth, and there is no obstructive lesion in the round window niche

Repair of the tympanic membrane
The temporalis fascia was fixed in 75 % alcohol and trimmed to a suitable size, then placed under the internal surface of the residual tympanic membrane

Reconstruction of the ossicular chain with autologous incus
Raise the temporalis fascia again. The sculptured autologous incus long process is implanted to connect the head of stapes and manubrium of malleus. Fibrinogen glue can be used to support the connections of the reconstructed ossicular chain. The preserved chorda tympani nerve is also helpful in stabilization of the reconstructed ossicles

Repositioning the tympanomeatal flap and the temporalis fascia
At the end of the procedure, the temporalis fascia and the tympanomeatal flap with tympanic membrane remnant are returned to its natural position. Several pieces of gelatin sponge are placed in the anteroinferior part of tympanic cavity to support the implanted fascia. Then pack the external auditory canal with gelatin sponge and iodoform gauze
Mastoidectomy (Open Cavity)
Indications
-
1.
When there is no ability of reconstructing the ossicular chain due to extensive erosion by cholesteatoma or severe bone erosion in chronic purulent mastoiditis.
-
2.
Uncertainty of complete removal of cholesteatoma, or patients who have a completely squamous epithelial lined medial wall of the middle ear with permanent loss of Eustachian tube function.
-
3.
Chronic suppurative otitis media with intracranial complications, petrous bone inflammation, suppurative labyrinthitis, facial paralysis, etc., that are not suitable for hearing reconstruction.
-
4.
Tuberculous otitis media with bone destruction or sequestrum formation.
-
5.
Benign tumor, such as facial never neurinoma, glomus tumor.
Contraindications
-
1.
Simple chronic suppurative otitis media.
-
2.
Allergic otitis media.
-
3.
Secretory otitis media.
-
4.
Acute purulent otitis media.
-
5.
Tuberculosis of the middle ear or mastoid without destruction of bone or sequestrum.
Operative Procedures
-
1.
Incision: usually endaural but may be postauricular incision. Postauricular incision is used in cases of otogenic complications, middle ear and mastoid tuberculosis, middle ear tumors etc.
-
2.
Mastoid cortex exposure, show the landmarks: suprameatal spine, suprameatal triangle and temporal line.
-
3.
Suprameatal triangle is used as a guide to the mastoid antrum, remove disease in the mastoid, then drill out the mastoid cavity.
-
4.
Remove posterior wall of EAC and the bone bridge, lower the facial ridge as much as possible for unobstructed drainage.
-
5.
Open anterior attic fully, remove all disease and remnants of the malleus and incus, leaving only the stapes.
-
6.
Scarify the mucosa of tympanic opening of Eustachian tube and fill the entrance with muscle.
-
7.
EAC skin flap is used to cover mastoid cavity. A meatoplasty is fashioned later.
-
8.
Fill operating cavity with iodoform gauze, then close the skin incision and apply a dressing.
Special Comments
-
1.
Fully open and clean the anterior attic to ensure complete removal of cholesteatoma.
-
2.
Lower the facial nerve ridge as much as possible to improve drainage: no higher than lateral semicircular canal superiorly and at level of the EAC inferiorly.
Pay particular attention to the vertical segment of the facial nerve.
-
3.
When dealing with middle ear disease, take care to avoid injury to the horizontal segment of facial nerve which is exposed.
-
4.
It is also important to remove all the deceased tissue from posterior tympanic cavity.
-
5.
A wide open external auditory meatus is important to ensure a long term dry ear.
Complications
-
1.
Facial paralysis.
-
2.
Sensorineural hearing loss, due to inner ear injury caused by stapes or lateral semicircular canal injury at operation.
-
3.
Sigmoid sinus or dural laceration.
-
4.
Wet ear with persistent suppuration postoperatively.
-
5.
EAC stenosis or auricular perichondritis.
Surgery1: Mastoidectomy (Open Cavity)

Open mastoid antrum through Macewen’s triangle.
Lempert endaural incision has been made and the tympanomeatal flap prepared, then exposure of the mastoid cortex, using Macewen’s triangle as a landmark to the antrum, then opening antrum tympani and mastoid cavity. Cholesteatoma can be seen

Part of the attic is exposed
An extensive cholesteatoma is shown. It was necessary to enlarge the mastoid cavity from the open antrum and to the attic, to expose the cholesteatoma which was filling it

Opening of the attic
Enlarge the cavity, open the air cells forward into the root of zygoma, skeletonize bone tegmen of mastoid and attic superiorly. At the same time, drill bone cover of the sigmoid sinus posteriorly as thin as possible, and open the mastoid inferiorly. Gradually remove the posterior wall of EAC

Surgical cavity skeletonization
Continue the cavity skeletonization until attic, antrum and mastoid form a single cavity

Remove disease completely
Open the attic until it is flush with anterior wall of EAC, expose the anterior attic fully. An almost completely skeletonized cavity can be seen. Next, remove the cholesteatoma matrix in continuity from front to back

Remove the bony bridge
Further medial bone erosion can be seen after most of the cholesteatoma was removed. Remove the bridge, expose the middle ear, lower the posterior buttress and facial nerve ridge as much as possible: no higher than lateral semicircular canal superiorly, and about the same height as the EAC floor inferiorly. Complete skeletonization of the cavity

Posterior EAC flap incision
Incise tympano-meatal flap at 12 o’clock, ensure the flap can cover the mastoid cavity posteriorly

Mastoid cavity covered with flap
Turn the flap back into mastoid cavity, pars tensa perforation and tympanic membrane remnant can be seen, tympanic mucous membrane was partly epithelized

Removal of cholesteatoma and cavity skeletonization
Remove all cholesteatoma and granulation tissue, polish all cavity walls with diamond or finishing bur to smooth them out, leaving no covered space or bone ridge which can block drainage. At completion, the bony ear canal, middle ear, attic and mastoid form a single open space

Meatoplasty and cavity closure
Excise conchae cartilage to enlarge the EAC opening, fill the surgical cavity with iodoform gauze in layers. Note: the EAC flap should be placed on to the surface of the bone. Close the wound with three to four stiches
Surgery 2: Mastoidectomy (Open Cavity)

Make lempert endaural incision and enlarge surgical field by displacing the EAC flap forward
Make Lempert endaural incision, elevate the EAC flap to widen the surgical field. The area should expose the zygomatic arch and temporal line superiorly, most of mastoid posteriorly, the anterior wall of EAC and temporomandibular joint in front. In this case, bone medial to the spine of Henle has been eroded by cholesteatoma

Tympanic antrum opening
Drill marker lines along temporal line and posterior wall of EAC. Drill the mastoid cortex of this triangle to expose the antrum, then proceed to locate the tympanic attic and mastoid. In this case, cholesteatoma can be seen when drilling the mastoid

Stepwise opening of the mastoid cavity
Progressively open the mastoid cavity around the exposed cholesteatoma. The cortex of mastoid in this case was markedly thinned by the large cholesteatoma

Removal of the bony bridge
Enlarge surgical cavity around the cholesteatoma which can be seen filling the middle ear and attic. Remove the posterior wall of EAC (bone bridge) which can be seen to be eroded by disease in this case

Cholesteatoma removal
Completely elevate the cholesteatoma along its upper and lower borders. Take care in removal of disease form the facial ridge. Risk to the facial nerve can be reduced with use of a facial nerve monitor, particularly by less experienced surgeons. Always work along the long axis of the nerve to minimize trauma

Facial ridge exposure
After removal of cholesteatoma the facial ridge is exposed. In this case, an abnormal facial ridge can be seen due to bone erosion

Open attic fully
Continue drilling until the anterior wall of attic is flush with the anterior wall of EAC, in order to ensure complete removal of cholesteatoma in this region

Complete the surgical cavity
Clear disease from anterior attic, lower the facial ridge, and skeletonize the middle and posterior fossa dural plates until mastoid cavity, antrum and middle ear form a single cavity, which will drain well. Ensure the mastoid cavity walls are drilled smooth without any bony overhangs

Incise the canal wall flap
Incise the EAC flap at 12 o’clock, and complete the flap

Meatoplasty
Turn the flap back into mastoid cavity and fashion the meatoplasty
Modified Radical Mastoidectomy
Indications
-
1.
Chronic otitis media with cholesteatoma
-
2.
Persistent purulent secretion, unsuitable for tympanoplasty.
-
3.
Provide easy access for long term follow-up
-
4.
No surgical contraindication
Contraindications
-
1.
Poor systemic condition
-
2.
Acute upper respiratory infection
-
3.
Unable to resect cholesteatoma thoroughly with this technique
-
4.
Atresia of oval window and round window, mucosa of tympanic cavity is epithelized entirely
-
5.
Hearing aid is important postoperative
-
6.
Women in menstrual phase
Operative Procedures
-
1.
Terminal sulcus (endaural) incision or postauricular incision. By using terminal sulcus incision, the meatoplasty with removal of conchal cartilage must be performed at the same time, and meatal stenosis can be prevented. The meatoplasty also facilitates drainage, ventilation and epithelization of the operative cavity. The better exposure ensures easy cleaning and care of the cavity.
Alternatively, the operative field is well exposed by a postauricular incision, and the meatoplasty should be performed at the end of the operation to prevent meatal stenosis.
-
2.
Incise the skin, subcutaneous tissue and periosteum. Expose the mastoid cortex, the posterior and superior wall of external auditory meatus, tympanic notch, tympanic ring, temporal line and suprameatal spine.
-
3.
Drill the mastoid cortex and cells from cribriform area and open the mastoid antrum.
-
4.
Open the attic, find the short process of the incus.
-
5.
Saucerize the mastoid cavity. The cavity is bound by the posterior wall of the external acoustic meatus, perpendicular part of facial nerve, sigmoid sinus, tegmen mastoideum, sinodural angle, and mastoid tip. Thin the bone of the posterior wall of the external auditory meatus, preserve the facial nerve canal and protect the sigmoid sinus. Fill the mastoid tip with bone dust or other soft tissue at the end of the procedure for easier to drainage.
-
6.
Open the attic, expose the anterior and superior walls and drill down the lateral wall.
-
7.
Resect the bridge by removing the bony postero-superior wall and clear the mesotympanum.
-
8.
Separate the incudo-stapedial joint. Shear the superior ligament of the malleus. Take out of the defective malleus and incus.
-
9.
Identify the position of the cochleariform process, the horizontal part of the facial nerve and the prominence of the lateral semicircular canal. Remove the lateral and posterior-inferior walls. Lower the facial ridge. Smooth the cavity walls to assist with easy drainage.
-
10.
Implant the ossicular prosthesis to rebuild the ossicular chain. Use a PORP if the stapes superstructure is intact, or a TORP if the superstructure is missing.
-
11.
Fashion the plastic meatal flaps, making a flap with an inferior pedicle. Incise the subcutaneous tissue and cartilage of the external acoustic meatus. Fold the flap inferiorly to cover the mastoid cavity. With the postauricular incision, make a circumferential incision along the terminal sulcus, extend the incision to the point between root of the helix and tragus, then make plastic meatal flaps.
-
12.
Fashioning the meatoplasty. Excise a semilunar segment of conchal cartilage without perichondrium from the endaural incision, cut the skin flaps transversely into two to three small ones along the free edge of cavity of concha skin, and use these at the end of the procedure to cover the mastoid cavity.
-
13.
Repair the tympanic membrane with air dried temporalis fascia.
-
14.
Reflect the fascia, fill the cavity with absorbable hemostatic gauze or erythromycin-soaked gelatin sponge.
-
15.
Place a cartilage disc with periosteum between the ossicular prosthesis and the fascia. Reset the temporalis fascia and skin flap to cover the facial ridge.
-
16.
Place erythromycin-soaked gelatin sponge or absorbable hemostatic gauze over the tympanic membrane, pack the external auditory meatus by using iodoform gauze to secure the flap.
-
17.
Suture the incision using an interrupted silk suture, cover the incision with a sterile dressing.
Special Comments
-
1.
Clear the mastoid cavity, aditus ad antrum and attic thoroughly to avoid recurrent disease.
-
2.
Preserve the structure of mesotympanum and hypotympanum to give the best possibility of tympanoplasty and ossicular chain reconstruction.
-
3.
Protect the integrity of ossicular chain as far as possible.
-
4.
Protect the facial nerve and semicircular canal to prevent facial palsy and perilymph leak.
-
5.
Preserve the mucosa of the tympanic cavity as far as possible.
Complications
-
1.
Hemorrhage and infection. Use aseptic operative technique, good hemostasis and postoperative antibiotics. Avoid injury to the sigmoid sinus and jugular bulb.
-
2.
Deafness or severe hearing loss. Avoid excessive stapes manipulation and injury to the inner ear.
-
3.
Facial paralysis. Pay attention to facial nerve position and the state of its bony canal. Decompress the facial nerve immediately if it is injured during surgery or peripheral facial paralysis is apparent immediately after the operation.
-
4.
Leakage of cerebrospinal fluid. Avoid injury to the dura and repair it immediately if it is injured during operation.
-
5.
Perilymph leak. Avoid opening the horizontal semicircular canal. Dissect cholesteatoma carefully.
-
6.
Persistent purulent secretion post operation. Resect disease thoroughly and drill the facial ridge as low as possible. Ensure adequate drainage of the attic and mastoid cavity.
Surgery 1: Modified radical mastoidectomy and Tympanoplasty

Postauricular incision, exposure of the mastoid cortex
A sterile operation towel is spread over the skin after the external auditory canal and the skin around the ear is sterilized. The incision of the skin, the subcutaneous tissue and the periosteum is made behind the ear, the mastoid cortex is then exposed. Separate the meatal flaps from the subcutaneous tissue

Cholesteatoma exposure though cribriform area approach
After exposing the posterior wall of the external auditory canal, the mastoid cavity is contoured though a cribriform area approach to the mastoid antrum. The cholesteatoma is then exposed

Shaping of mastoid cavity
After the mastoid cavity is fashioned, the cholesteatoma is exposed in the mastoid antrum and attic, and then the mastoid tip and the sinodural angle are exposed thoroughly. The exposure includes the posterior wall of external auditory meatus, perpendicular part of facial nerve, sigmoid sinus, tegmen mastoideum, sinodural angle, and mastoid tip. Open the attic and expose the anterior and superior walls

Disease in mastoid and tympanic cavity are exposed via a combined approach
After adjusting the amplification of the microscope, the tympano-meatal flap is elevated to expose the tympanic cavity containing cholesteatoma. The residual tympanic membrane is also visible

Removal of the bridge
The surgical bridge is taken down because of extensive cholesteatoma. The cholesteatoma which is surrounding the head of malleus and covering the medial wall of the tympanic cavity is removed carefully

Full view of operation cavity
The full view of operation cavity is shown clearly. The attic is opened fully. Its anterior wall is further forward than that of the external auditory canal. The tegmen mastoideum is drilled as thin as possible. The sinodural angle is exposed thoroughly. The facial ridge is made lower than the lateral semicircular canal. Contouring of the sigmoid sinus, mastoid tip and high riding jugular bulb region is completed. The mesotympanic cholesteatoma is cleaned and the mucous membrane of medial wall of tympanic cavity is left intact

Lower the facial ridge and remove the disease
After the facial ridge is lowered, the cholesteatoma over horizontal part of facial nerve and oval window is removed thoroughly. The stapes superstructure is absent, the stapes footplate is mobile and the mucosa is healthy. The horizontal part of facial nerve, the prominence of the lateral semicircular canal and the cochleariform process are exposed after the cholesteatoma is cleared

Ossicular prosthesis implantation
Underlay the tympanic membrane with temporalis fascia that has previous been air dried. Turn the fascia back and fill the tympanic cavity with absorbable non-adhesive gauze to support the graft and prevent post-operative adhesions. The prosthesis (TORP) is cut to the appropriate length and placed on the stapes footplate

Place the cartilage disc
A cartilage disc with attached perichondrium is taken from the auricle and inserted over the TORP. The temporalis fascia graft is placed over this under the tympano-meatal flap

Placement of fascia
Reposition the temporalis fascia and skin flap over the facial ridge, TORP and tympanic cavity

Mastoid cavity packing
The absorbable non-adhesive gauze is placed over the tympanic membrane

Mastoid cavity packing
The iodoform gauze is packed into the external auditory meatus to hold the flap

Wound closure
The incision and the meatoplasty of auricular concha is performed to enlarge the external auditory meatus. Close the wound with interrupted silk sutures. Cover the wound with a sterile dressing to complete the operation
Surgery 2: Modified radical mastoidectomy and Tympanoplasty

Make Lempert endaural incision
A sterile operation towel is spread over the skin after the external auditory canal and the skin around the ear is sterilized. Make Lempert endaural incision, the mastoid cortex is then exposed. Perform a mastoidectomy via a cribriform area approach

Contour the mastoid cavity
The mastoid cavity is fashioned via a cribriform area approach to expose the sigmoid sinus, the tegmen mastoideum and the cholesteatoma in the antrum and mastoid

Open attic
The cholesteatoma in the attic and mesotympanum is exposed after the attic is opened. The middle ear space also contains disease

Removal of the bridge
The bridge is removed because of the extensive cholesteatoma in the middle ear and around the ossicles which will be difficult to remove otherwise

Removal of the facial ridge
The head of malleus is taken out after the bridge is removed. The facial ridge is then lowered to expose the cholesteatoma in the mesotympanum and over the prominence of the lateral semicircular canal. The horizontal part of the facial nerve is also exposed due to erosion of its covering bony canal

Removal of the cholesteatoma
The cholesteatoma is removed from tympanic cavity, attic and over the lateral semicircular canal leaving the healthy mucosa. The anterior-inferior remnant of the pars tensa and the handle of the malleus are exposed. Fistulization of the lateral semicircular canal is suspected, so removal of any overlying disease should be done with great care

Removal of disease
The cholesteatoma over the horizontal part of the facial nerve and oval window is removed thoroughly. The eroded head, crura and footplate of the stapes and the horizontal part of facial nerve are exposed. The stapes is mobile and the covering mucosa is healthy. Part of the head of the stapes is eroded, but the crura and footplate are normal

Removal of the cholesteatoma
The cholesteatoma is removed thoroughly. It can be seen that part of lateral semicircular duct is eroded by cholesteatoma. This is superficial and an osseous fistula has not been created

Incise the flap
Cut the flap at the 12 o’clock point, then drape the external part of the cavity and the facial ridge with the flap

Spread the fascia
Repair the tympanic membrane with temporalis fascia that has been air dried. Spread the fascia on the surface of the mastoid cavity and deep to the flap. Ensure the size of the fascial graft is adequate to repair the drum and cover the bone of the cavity

Ossicular prosthesis implantation
The fascia is elevated; the TORP is cut to the appropriate length and implanted on the stapes footplate

Position the cartilage disc
Place a cartilage disc taken with perichondrium from the auricle between the TORP and the fascia to prevent tympanic membrane erosion and extrusion of the prosthesis

Re-position the fascia
Cover the facial ridge by replacing the temporalis fascia and the skin flap. Place absorbable hemostatic gauze over the tympanic membrane. The external auditory canal and mastoid cavity are packed with iodoform gauze to fix the flap. The incision is closed with interrupted silk sutures. Cover the wound with a sterile dressing to complete the operation
Mastoidectomy (Closed Cavity)
Indications
-
1.
Chronic otitis media with persistent otorrhea or other symptoms including ear pain and external canal bleeding despite routine medical therapy.
-
2.
Cholesteatoma in middle ear and mastoid, especially involving attic and mastoid antrum; where any disease in the mesotympanum and hypotympanum is able to be controlled.
-
3.
The tumors involving the attic or middle ear.
-
4.
Refractory middle ear effusions unresponsive to conservative measures.
Contraindications
-
1.
Non-functioning Eustachian tube or erosion of the inner ear.
-
2.
Significant erosion of the posterior bony EAC wall.
-
3.
A small sclerotic mastoid, a low-lying middle cranial fossa and an anteriorly positioned sigmoid sinus will limit surgical exposure and may necessitate removal of the canal wall.
-
4.
Irreversible disease in the middle ear.
-
5.
The large area dura mater defects which can lead to cerebrospinal otorrhea or cerebral hernia.
-
6.
Patient unfit for surgery.
Operative Procedures
-
1.
Incision: Under local or general anesthesia, the procedure is usually carried out through a postauricular incision which is 0.5–1.0 cm behind the posterior sulcus. The incision is carried down to the mastoid cortex, and the postauricular flap is elevated anteriorly and inferiorly to expose the mastoid cortex and outer attic wall.
-
2.
Opening the mastoid antrum: The cortex of the mastoid is removed in the cribriform area using a large cutting bur. The mastoid antrum is directly deep to this area. The bone should be widely removed with bevelling of the margins to give adequate exposure of the cavity.
(PS:If the disease is only limited to the attic and mastoid antrum, atticoantrostomy may be used).
In this procedure the lateral wall of the attic is exposed by elevating the skin and periosteum of the external auditory canal. Bone is removed progressively from the margin of the tympanic notch to the antrum until all disease is exposed. The short process of incus, incudal fossa and prominence of lateral semicircular canal can be seen with this approach. (In this technique the posterior EAC wall is mostly preserved and the sigmoid sinus is not exposed.)
-
3.
Fashioning of mastoid cavity: The surgical field is expanded from the antrum. The epitympanum is opened to expose the short process of incus by drilling anteriorly. The mastoid is then drilled to identify and skeletonize the sigmoid sinus, the middle cranial fossa dural plate, the digastric ridge, the lateral semicircular canal.
-
4.
Thinning of posterior EAC wall: The bony EAC must be thinned to allow access for the facial recess dissection and eventual visualization of the most posterior mesotympanic structures, such as the round window and the stapedius tendon.
-
5.
Opening the attic: The lateral wall of the attic is removed to expose the incudo-malleal joint drilling from the temporal line to the zygomatic root. The incus may need to be removed depending on the disease. Removal of the ossicles will improve the communication of middle ear and mastoid cavity.
-
6.
Opening the facial recess: Facial recess is a variably pneumatized triangle bounded anteriorly by the chorda tympani, posteriorly by the second genu and descending portion of the facial nerve and superiorly by the bone of the fossa incudis (incus buttress). When opened it forms a posterior tympanotomy exposing the pyramid, the round window and oval window.
-
7.
Eradication of disease: Disease can now be cleared from the attic, the mastoid cavity, the facial recess and the mesotympanum. Cholesteatoma matrix should be completely removed from the mastoid working from posterior to anterior. The malleus head should be removed if it is eroded by cholesteatoma. This will allow exposure of the supratubal recess and assist in eradicating the disease from both anterior attic and upper part of the EAC. Whether an open or closed approach is used, the areas that are most difficult to be seen are the posterior recesses of the middle ear, including the area below the pyramid and tympanic sinus. These areas are located between and behind the oval and round windows, where the cholesteatoma epithelium is easily hidden, especially in cases of marginal tympanic membrane perforations. If the stapes superstructure and stapedial muscle are missing, the pyramid and the surrounding bone should be drilled to assist in eradicating the disease thoroughly.
-
8.
Tympanoplasty: The annulus is elevated via an EAC approach, and tympanoplasty is performed based on the status of ossicular chain.
-
9.
Closing: A drainage tube is placed in the mastoid cavity and the wound is closed in layers.
Special Comments
-
1.
The mastoid cavity should be saucerized to allow better visualization and prevent injury to important structures.
-
2.
Any overhang of the posterior bony EAC wall should be removed in order to fully visualize the drum and middle ear.
-
3.
Care should be taken in clearing disease from the mastoid antrum in order to avoid injury to the facial nerve or lateral and posterior semicircular canals.
-
4.
When removing of lateral wall to the attic, the bone over the incus should be thinned with a diamond bur then gently removed with a curette to avoid injury to the stapes and inner ear.
-
5.
Any defect of the scutum must be identified. These should be repaired. Large defects may be best treated with open cavity surgery. Failure to deal with bony wall defects will allow pars flaccida retraction post operatively leading to recurrent disease.
-
6.
The air cells of the sinodural angle must be removed in order to clear the area behind the semicircular canals.
-
7.
During the careful skeletonization of the facial nerve and chorda tympani a diamond bur is used and liberal irrigation is necessary to avoid thermal injury to the nerve. The tympanic segment of the facial nerve is commonly exposed, either congenitally or by disease. Care needs to be taken to avoid injury to the nerve when dissecting in this area.
-
8.
When working in the region of the anterior part of the lateral semicircular canal, care needs to be taken with the incus and the facial nerve which is covered with only thin bone here. One needs to be certain of clearing all disease from the canal and irrigation will assist with this.
-
9.
Care needs to be taken with the chorda tympani when working at the anterior margin of the facial recess.
-
10.
The facial recess needs to be opened widely for good access and with due care to the facial nerve when working posteriorly.
-
11.
The bone is removed gently in performing the posterior tympanotomy, without undue pressure which may cause accidental injury to the stapes.
Complications
-
1.
Facial paralysis: If the facial nerve is injured, swelling may occur deep to its sheath causing excessive pressure and paralysis. If this occurs, bone should be removed for 5–6 mm from each side of the exposed portion of the facial nerve and the sheath should be incised to relieve the pressure
-
2.
Vertigo: Caused by semicircular canal injury. It is possible to injure the semicircular canals in a sclerosed mastoid or when dealing with inflamed granulation tissue. Any opening in the labyrinth that occurs should be sealed immediately with bone wax and the area covered with temporalis fascia.
-
3.
Sensorineural hearing loss and tinnitus: These can be caused by a direct injury to any of the semicircular canals or cochlea, or indirectly via trauma to the incus or stapes, especially when opening the posterior tympanotomy.
-
4.
Residual and recurrent cholesteatoma: due to incomplete eradication of cholesteatoma, insufficient opening of attic, inflammation, and so on.
-
5.
Hemorrhage: (1) sigmoid sinus injury: It may bleed immediately after being abraded. Bleeding can be suppressed to stop with pieces of cotton for a few minutes. A larger defect can be sutured with 4–0 lines or be repaired with a muscle flap. The packing materials should be sutured with the surrounding tissues in order to avoid embolism caused by displacement in to the vessel. (2) Jugular bulb Bleeding: Bleeding may come from air cells and bone marrow covering the jugular bulb. They are sealed with bone wax, and then use cotton pieces to press bone wax into air cell for more effective hemostasis.
Surgery 1: Intact Canal Wall Mastoidectomy and myringoplasty with maintaining Ossicular Chain intact

Post-auricular incision and mastoid exposure
The incision is carried down to the temporalis fascia. The superior periosteal incision was at the level of the temporal line and a second incision extends inferiorly to the mastoid tip over the posterior mastoid. The periosteal flap is elevated in the direction of the EAC

Opening the mastoid antrum
The bone is drilled from a triangle made up of the temporal line above, one parallel to the postero-superior EAC wall anteriorly and a vertical line tangential to the posterior curve of the EAC. This bone overlies the mastoid antrum. The bone is “saucerised” to give wide exposure to the antrum and the disease it contains

Exposure of the incus and fashioning of mastoid cavity with preservation of the posterior wall of EAC
The attic has been opened antero-superior to the mastoid antrum. Some bone was eroded. The ossicular chain is surrounded by cholesteatoma. After the short process of incus has been exposed, the mastoid cavity is fashioned by drilling posteriorly towards the sigmoid sinus and inferiorly to the mastoid tip. Care needs to be taken with vertical portion of the facial nerve as it runs inferiorly and slightly laterally from the level of the horizontal semi-circular canal

Thinning the posterior EAC wall and opening the attic
The key point of Intact Canal Wall Mastoidectomy is to preserve the posterior wall of EAC, whilst thinning the bony wall as much as possible to expose the operative field
In order to see all disease, the anterior attic should be fully exposed by drilling the anterior and superior walls, leaving a thin postero-superior EAC wall. This figure shows the incudo-malleal joint. Cholesteatoma has been removed from lateral to the ossicles but is still to be cleared from the anterior and medial attic

Opening the attic and eradicating the disease
Further opening of the anterior attic allows access to clear the disease. The malleus head and incus body are seen to be intact

Elevation of the EAC flap
The skin flap of EAC is very thin and care needs to be taken to keep it intact, with gentle dissection along its whole width

Exploration of the tympanic cavity via a post-auricular approach
Remove the suprameatal spine to enlarge the operative field. Elevate the tympano-meatal flap to enter the middle ear. The cholesteatoma has been partially removed from Prussak’s space via the EAC

Eradication of attic cholesteatoma
The cholesteatoma has been completely removed from the attic and Prussak’s space with combined dissection from the attic above and the EAC below. Ensure no cholesteatoma is left medial to the posterosuperior wall of EAC

Thinning of the posterior wall of EAC and exposure of the facial recess
A facial recess approach needs to be performed to expose the middle ear and lower part of the ossicular chain and remove any disease present. Firstly, the posterior wall of EAC is further thinned over the facial recess which lies inferior to the incus and lateral semicircular canal

Opening the facial recess
The facial recess is a triangular area bounded superiorly by the bone of incudal fossa, posteriorly by the facial nerve and antero-inferiorly by the chorda tympani. The recess is initially opened superiorly, near to but not touching the incus. This gives the best exposure of the posterior middle ear in intact canal wall mastoidectomy

Exploration of the posterior tympanic cavity via the facial recess approach
Exploration via the facial recess revealed mild mucosal edema around the stapes. The incudo-stapedial joint was seen to be intact and the stapes was mobile

The operative cavity with complete eradication of disease
The operative cavity is seen after complete removal of disease from the attic (both lateral and medial to the ossicles), the antrum and the posterior tympanic cavity (seen via the facial recess approach). The middle ear structures were normal. The pars tensa of the tympanic membrane was intact in this case and the perforation of parts flaccida was repaired with a small piece of fascia
Surgery 2: Intact Canal Wall Mastoidectomy, myringoplasty, and ossiculoplasty with prosthesis

Opening the mastoid antrum
This is a diploic mastoid and a small amount of inflammatory granuloma is seen in the aditus ad antrum

Opening the attic and fashioning the mastoid cavity
In a diploic or poorly developed mastoid the tegmen mastoideum, tegmen tympani and postero-superior wall of EAC all need to be thinned down maximally to obtain the best exposure. The anterior position of the sigmoid sinus and the attic cholesteatoma can be seen

Exploration of the attic
The ossicles are surrounded by cholesteatoma in the attic. This must be completely removed from the ossicles in a posterior and superior direction using a delicate technique to minimize trauma to the ossicular chain

Exploration of the anterior epitympanic recess
After separation of the incudo-stapedial joint, the incus is removed. The neck of the malleus is then cut and the head is removed. This allows removal of cholesteatoma from medial to the malleus in the middle ear and attic

Exploration of the middle ear via EAC.
Elevate the skip flap of EAC to the annulus then elevate the tympanic membrane to enter the mesotympanum. Using this approach, the chorda tympani nerve can be usually preserved and the mesotympanum and hypotympanum can be explored for disease

Exposure of the posterior tympanic cavity via a facial recess approach
The posterior tympanic cavity cannot be adequately explored via the EAC. A facial recess approach with removal of the incus buttress was used to widely expose the area. Cholesteatoma and inflammatory granuloma were seen to extend down from the attic

Exploration of the posterior tympanic cavity
The posterior arch (incus buttress) has been removed completely to aid visualization of the oval window and posterior tympanic cavity. Bone over the facial nerve has been removed more inferiorly to expose the round window niche and hypotympanum. This allowed removal of cholesteatoma from these areas and exposure of the stapes

Tympanoplasty
The mucosa on the medial wall of mesotympanum was seen to be intact after removal of all cholesteatoma. The cochleariform process was identified. The stapes was seen to be intact and mobile. The tympanic membrane (TM) defect was then repaired with fascia
Reconstruction of the ossicular chain: The incus and malleus were absent whilst the stapes was intact and mobile. The distance from the head the stapes to the TM was measured. A PORP was trimmed to the correct length and placed on the stapes, with the cup-shaped end on the stapes head and the disc-shaped top under the TM

Operative cavity of intact wall mastoidectomy with tympanoplasty
The intact wall mastoidectomy with tympanoplasty is almost complete. The mastoidectomy cavity extends anteriorly to the anterior epitympanic recess, posteriorly to the sinodural angle and inferiorly to the mastoid tip. The eradication of disease and repair of the tympanic membrane and ossicular chain have been accomplished by using the combined-approach through the EAC and facial recess approach via the mastoid

Placement of cartilage disc between TM and prosthesis
A small disc of cartilage has been taken from the tragus. This is placed between the prosthesis and the TM to prevent later extrusion. It also assists in maintaining stability of the PORP

Placement of cartilage disc between TM and prosthesis (High power)
The cartilage should be well-sized and must cover the entire top of the PORP
Surgery 3: Intact Canal Wall Mastoidectomy with preservation of the intact Ossicular Chain

Exposure of the incus and fashioning the mastoid cavity
Intact canal wall mastoidectomy is usually used in cases of limited attic, middle ear or mastoid disease without erosion the ossicular chain. In this case, the attic lesion has been removed while a small amount of cholesteatoma was seen in Prussak’s space

Exploration of the tympanic cavity via a post-auricular approach
This surgery usually requires exploration of the tympanic cavity. The TM has been elevated anteriorly to show the intact pars tensa and separated chorda tympani. The diseases in the pars flaccida and Prussak’s space can be eradicated by a combined approach through EAC and attic

Exploration of the posterior tympanic cavity through facial recess
Exploration via the facial recess identified no disease in the posterior tympanic cavity. The ossicular chain was shown to be intact and mobile
Mastoid Obliteration, Canal Wall Reconstruction and Tympanoplasty
Indications
-
1.
To avoid cholesteatoma recurrence and maintain an adequate middle ear space post-operatively;
-
2.
To avoid the formation of a mastoid cavity which requires regular cleaning and may have other problems such as vertigo with temperature stimulation;
-
3.
To enable hearing reconstruction either at the first or a second stage operation.
-
4.
Patient must undergo long term follow-up and be prepared for a second look operation if there is concern of cholesteatoma recurrence;
-
5.
Patient wishes to expose ear to water. Patient wants a normal appearing ear;
Contraindications
-
1.
Inability to ensure complete clearance of cholesteatoma;
-
2.
Patients are not able to undergo long term follow-up. Patients are not concerned about hearing.
-
3.
Extensive disease or severe complication identified pre-operatively.
-
4.
Patient unable to tolerate multiple procedures.
Operative Procedures
-
1.
Make incision in the hair line, harvest a generous piece of temporalis fascia and place it in alcohol for dehydration. Periosteum from the tragus or conchal cartilage can be used as an alternative;
-
2.
A posterior or endaural incision can be used, with the soft tissues dissected from the surface of the mastoid;
-
3.
Bone can be removed via the antrum or by enlarging the postero-superior part of the EAC. Care must be taken to avoid facial nerve injury;
-
4.
The middle ear cleft is exposed and cholesteatoma is removed thoroughly. The cholesteatoma must be cleared completely from surface of bone or mucous membrane. This is done by dissecting from above down and from below up to the oval window, finally clear disease around the stapes. Care must be taken to avoid opening the inner ear. Healthy mucous membrane is preserved.
-
5.
The lateral wall of the attic is removed to expose the ossicular chain. If the incudo-stapedial joint is intact, it is separated to avoid inner ear injury. The operated cavity should extend from the anterior attic wall, along the tegmen tympani without exposure of the middle cranial fossa (MCF) dura to the mastoid cavity behind.
-
6.
Fashioning the mastoid cavity. Under the microscope, all involved mastoid air cells are exenterated with reducing drills size until all cholesteatoma has been removed. Copious irrigation is used to cool the bone and keep the operative field clear for drilling. The tegmen should be smoothed above without exposure of the MCF dura. The sigmoid sinus is skeletonized posteriorly. The anterior wall is the EAC wall in a closed mastoidectomy, or the EAC if the wall is eroded or needs to be removed. When creating the mastoid cavity one may encounter Koerner’s septum before exposing the antrum. The facial nerve and the lateral semicircular canal must be protected when drilling, using a diamond bur and copious irrigation when working near them.
-
7.
The EAC wall is removed if necessary to clear all disease. If it can be preserved, the facial recess must be opened. The upper margin of the recess is the fossa incudis, its anterior border is the chorda tympanic and its posterior border is the vertical segment of the facial nerve. Once the facial recess has been adequately opened, cholesteatoma can be removed from the posterior middle ear cavity
-
8.
Reconstruction of the lateral attic wall or external auditory canal wall: Use free cartilage, pedicled cartilage or artificial material to rebuild the attic lateral wall and/or the external canal wall to keep an adequate middle ear space. Cholesteatoma is thoroughly cleared around the stapes;
-
9.
The temporalis fascia is laid under the tympanic membrane, the ossicular chain is reconstructed as is the external auditory canal wall. Gelfoam is placed in the middle ear and mastoid to support the grafts.
-
10.
The patient’s incus or malleus (if present) or a PORP can be used to rebuild the ossicular chain.
If the stapes footplate is fixed, it is not opened or removed at this stage. A secondary procedure will be necessary.
-
11.
The tympano-meatal flap is re-positioned and supported with gelfoam in the external canal as well. The canal is packed with iodoform gauze. The external meatus can be enlarged if necessary. The incisions are sutured.
Special Comments
-
1.
Cholesteatoma must be cleared thoroughly. The attic and posterior tympanic cavity must be thoroughly checked to avoid recurrence after the operation;
-
2.
Materials used to reconstruct the external auditory canal wall must be stable to avoid cholesteatoma recurrence and to maintain an open middle ear cavity;
-
3.
Any free bone grafts or artificial material must be covered to avoid sequestrum formation or extrusion;
-
4.
Long term regular review is required post-operatively. A temporal bone CT or MRI scan may also be helpful in identifying recurrence. A second operation should be undertaken promptly when a recurrence is found early or a long time after the original surgery;
Complications
-
1.
Facial paralysis: this I more likely if the anatomic landmarks are not clear or when anatomical anomalies are present. The nerve needs to be clearly identified to avoid intra-operative injury;
-
2.
Medial displacement of the reconstructed external auditory canal wall: ensure the transplant material used o reconstruct the wall is firmly fixed to prevent displacement;
-
3.
Cholesteatoma recurrence: this can be due to inadequate initial clearance. Collapse of the reconstructed wall may also allow recurrence of cholesteatoma. Good initial surgery and long term regular follow-up are necessary.
Surgery 1: Closed mastoidectomy with tympanoplasty and reconstruction of the external auditory canal

Attic exposure
If cholesteatoma is limited in the attic or the mastoid is diploic, the attic can be opened directly from the external auditory canal. The tympanomeatal flap is elevated. The postero-superior external auditory canal, the cribriform area and mastoid cortex are exposed. The lateral wall of the attic is drilled away to expose the cholesteatoma. The tympanic antrum is also opened out posteriorly

Clearance of attic cholesteatoma and exposure of ossicular chain
Thorough clearance of attic cholesteatoma. The pars tensa is elevated to expose the middle ear contents. The malleus and incus are absent but the stapes is intact and mobile. The middle ear mucosa was normal and the tympanic opening of the Eustachian tube was free of disease

Insertion of PORP and reconstruction of the tympanic membrane
A slot is drilled in the external auditory canal wall to hold the cartilage flap. The PORP is positioned between the head of stapes and temporalis fascial graft. A cartilage disc is placed between the top of the PORP and the fascia

Reconstruct lateral attic and superior external auditory canal walls
The cartilage flap is placed in the bone slot made in external auditory canal and fill the attic with gelfoam. Temporalis fascia covers this and the tympano-meatal flap is re-positioned. The external canal is packed with iodoform gauze. The incision is then sutured
Surgery 2: Closed mastoidectomy with tympanoplasty and reconstruction of external auditory canal

Incision
The endaural incision is extended into the external canal. The subcutaneous tissues are extensively removed

Exposure of the middle ear cavity
Remove the soft tissues from the back of the meatal flaps, in order to expose mastoid cortex, the root of the zygoma, the cribriform area and mastoid tip clearly. The perforation of tympanic membrane was in the postero-superior quadrant with epithelium extending to the attic and mastoid

Attic opening
On drilling away the lateral attic wall, cholesteatoma is seen to fill the attic. The mastoid antrum has been opened posteriorly to identify the incus and erosion of the mastoid

Fashioning of mastoid cavity
The mastoid cavity is created with drilling of air cells and complete clearance of cholesteatoma

Removal of incus and exposure of stapes
The incus is removed to expose the stapes. The stapes was intact and mobile. The middle ear cavity, attic and mastoid were seen to be free of cholesteatoma

Repair of tympanic membrane with temporalis fascia
The temporalis fascia is used to completely cover the tympanic membrane perforation on its medial side

Repair tympanic membrane with temporalis fascia
Perforation of tympanic membrane was repaired by temporalis fascia, and it’s better to cover part of cartilage graft that was used for external ear canal reconstruction

Reconstruction of external auditory canal
Bone slots are drilled anteriorly between the attic and anterior wall of the ear canal and posteriorly on the upper part of the facial ridge to place the cartilage graft

Rebuilding the ossicular chain
Drill the autologous ossicle to fit between the head of the stapes and the tympanic membrane. Position the ossicle and ensure it is stable

Rebuild the lateral wall of the attic and the superior wall of the EAC
Place the free cartilage graft in the bone slots. Pack gelfoam into the attic and mastoid cavity. The cartilage graft is then covered with fascia and the tympanomeatal flap

Reposition meatal flaps
Cover with gelfoam then place iodoform gauze in the external auditory canal

Packing of external auditory canal
Pack iodoform gauze into external auditory canal and replace the flaps

Suturing the incision
After suturing the incision, the operation is complete
Surgery 3: Closed mastoidectomy with tympanoplasty and reconstruction of external auditory canal

Incision
The endaural incision is extended in to the external canal. The subcutaneous tissues are extensively removed

Elevation of meatal flaps
Make the endaural incision, reflect the helix and subcutaneous tissues posteriorly to expose the posterior wall of the external auditory canal, the cribriform area and the mastoid cortex

Opening the attic
Elevate the meatal flaps and tympanic membrane anteriorly. Drill down the lateral wall of the attic and expose it clearly. The attic here is filled with cholesteatoma

Exposure of mastoid antrum and tympanic cavity
Expose the attic, the antrum and tympanic cavity thoroughly. The tympanic membrane is intact but retracted

Clear the cholesteatoma and elevate the tympanic membrane to expose the ossicular chain
Clear the cholesteatoma from the attic and mastoid antrum completely, elevate the tympanic membrane to expose the mesotympanum. The incus is absent and the stapes was normal. All cholesteatoma was removed

Rebuild the superior wall of external auditory canal with cartilage graft
Place the free tragal cartilage graft in the bone slots to rebuild the external auditory canal wall

Repair the tympanic membrane
Reconstruct the tympanic membrane with temporalis fascia

Rebuild the ossicular chain
Lift the fascial graft, trim the PORP to the correct length to fit between the head of stapes and the new tympanic membrane and rebuild the ossicular chain. Place the cartilage graft between the PORP and fascia

Reconstruct the external auditory canal
Rebuild the external auditory canal wall with the free cartilage graft after the PORP has been positioned

Reposition the meatal flaps
Place the temporalis fascia on the canal side of the free cartilage graft and cover it with the meatal flap

Pack the external auditory canal and suture the incision
Place gelfoam into attic and mastoid cavity. Pack iodoform gauze into external auditory canal and suture the incision
Ossicular Chain Reconstruction for Congenital Deformity or Trauma
Indications
-
1.
Conductive hearing loss present at birth with normal tympanic membrane (usually symmetrical hearing loss)
-
2.
Conductive hearing loss with intact tympanic membrane after minor trauma;
-
3.
Conductive hearing loss with ossicular chain abnormality on CT scan.
Contraindications
-
1.
Major round window malformation
-
2.
Eustachian tube malformation or stenosis;
-
3.
Patient unfit for operation.
Operative Procedures
-
1.
Incise the skin in front of the helical crus. Carefully elevate a tympanomeatal flap to expose the middle ear. Bone may need to be curetted from the postero-superior wall to expose all of the oval window niche.
-
2.
Assess the state of the ossicular chain and its mobility, with particular attention to the incus, the incudostapedial joint and stapes footplate.
-
3.
Reconstruction of ossicular chain and choice of technique. If the stapes is present and mobile, the incus and head of malleus can be removed. Either the incus or a PORP can be positioned between the stapes head and tympanic membrane to reconstruct the chain. Where a PORP is used, a disc of cartilage should be placed between it and the drum to prevent extrusion. If the stapes footplate is fixed, stapedotomy or stapedectomy can be performed. If the incus long process is absent, the stapes prosthesis must be attached to the malleus handle. A small fat graft should be used to seal around the stapedotomy. If the oval window cannot be accessed, a fenestration of the lateral canal can be considered.
-
4.
The tympanomeatal flap is repositioned. If the operation is done under local anesthesia, the improvement in hearing can be checked before packing the ear canal.
Special Comments
-
1.
Take care not to damage the tympanomeatal flap. When a prosthesis is used, place a cartilage disc between it and the tympanic membrane to prevent secondary perforation and extrusion;
-
2.
Ensure good mobility of the reconstructed chain;
-
3.
Aspirate blood from the middle ear to reduce the formation of adhesions after operation;
-
4.
Avoid injury of the mucous membrane around the Eustachian tube;
-
5.
Check for a perilymph leak after stapedotomy or stapedectomy;
-
6.
If the middle ear malformation is too severe, ossicular chain reconstruction may not be possible.
Complications
-
1.
Facial paralysis: One should identify the position of the facial nerve clearly to avoid injury;
-
2.
Sensorineural hearing loss: Care should be taken when drilling the stapes footplate and inserting the prosthesis of correct length to minimise trauma to the inner ear.
-
3.
Cerebrospinal fluid otorrhea: This may occur if there is an abnormal communication between the inner ear and the subarachnoid space (“Gusher”).
-
4.
Perforation of tympanic membrane: Care should be taken to avoid perforation of the tympanic membrane. If it does occur it should be repaired immediately. Prostheses should not be placed in direct contact with the drum.
Surgery 1: ossiculoplasty of incus malformation (PORP)

Endaural incision
Incise the skin anterior to the helical crus and into the upper external auditory canal, elevate the tympanomeatal flap and tympanic membrane forward

Opening the tympanic cavity
Elevate the tympanomeatal flap and tympanic membrane to expose the tympanic cavity

Expose incudostapedial joint
Observe the chorda tympani nerve crossing the mesotympanum from back wall of external auditory canal. Adjust the angle of view of the microscope to display the incudostapedial joint. The long process of the incus is seen to be abnormal and separate from incus body

Check for abnormalities
The ossicular chain malformation is shown under high power. The separate incus process, both stapes crura, the facial nerve canal and the footplate can be seen

Remove abnormal incus
Use a hook to remove the abnormal incus process from head of stapes, check mobility of stapes

Check status of stapes
The stapes was intact and mobile. The chorda tympani should be preserved if possible. It can, sometimes be used to support the reconstructed ossicular chain

PORP
The cupped end sits on the stapes head, and the disc end sits under the tympanic membrane. The connecting bar between the two ends can be trimmed to correct length

Rebuilding ossicular chain
Once its shaft is trimmed to the correct length, the PORP can be placed between the stapes head and tympanic membrane. The shaft must be of optimal length for best hearing result

Cover prosthesis with cartilage graft
Place the cartilage graft between PORP and tympanic membrane to prevent secondary perforation of tympanic membrane

Reposition tympanomeatal flap
Reposition the tympanic membrane and meatal flap in original position

Packing and closure
Pack iodoform gauze into external auditory canal and to sew up the incision. Cover the ear with an sterile dressing
Surgery 2: ossiculoplasty of incus malformation (autogenous ossicle)

Elevation of the tympanic membrane and exposure of the tympanic cavity
After the EAC incisions are made, the meatal flaps and tympanic membrane are elevated to expose the tympanic cavity. The promontory and round window niche are exposed

Assessment of the ossicular chain
With adjustment of the microscope angle of view, the chorda tympani is seen to cross the tympanic cavity and the incus is noted to be markedly deformed

Examination of abnormal ossicular chain
The abnormal ossicular chain is assessed. There was only a segment of the abnormal long process of the incus on the head of stapes which did not connect with incus body. The stapes had a near normal shape but the crura were both thinner than normal

Remove abnormal incus
Remove the abnormal segment of incus from the stapes head. The stapes mobility was seen to be normal

Reconstruct the ossicular chain
Place the re-shaped autogenous ossicle between the stapes head and the tympanic membrane
Ensure that the grafted ossicle makes good contact with the stapes and is free of contact from all bony walls of the middle ear

Replace tympanic membrane
Reposition the plastic meatal flaps and tympanic membrane in their correct position

Pack the external auditory canal and sew up the incision
Replace the plastic meatal flaps and tympanic membrane. Pack iodoform gauze into the external auditory canal and to sew up the incision. Cover the operation field with an aseptic dressing
Suggested Reading
Tympanostomy Tubes
Jiang S-C, Gu R, Zheng-Min W. Otorhinolaryngology – otology. 2nd ed. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2002a. p. 754–75.
Kong WJ. Otorhinolaryngology head and neck surgery. Beijing: People’s Medical Publishing House; 2005. p. 460–4.
Qian Y-Z, Fan Z, Li P-H. Otorhinolaryngology head and neck surgery manual. Beijing: People’s Military Medical Press; 2000a. p. 26–31.
Zheng-Min W. Microsurgery of the ear. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2004a. p. 125–41.
Myringoplasty
Jiang S-C, Gu R, Zheng-Min W. Otorhinolaryngology – otology. 2nd ed. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2002b. p. 754–75.
Qian Y-Z, Fan Z, Li P-H. Otorhinolaryngology head and neck surgery manual. Beijing: People’s Military Medical Press; 2000b. p. 26–31.
Zheng-Min W. Microsurgery of the ear. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2004b. p. 125–41.
Tympanoplasty
Huang X-Z, Wang J-B, Kong W-J. Practice of otorhinolaryngology head and neck surgery. 2nd ed. Beijing: People’s Medical Publishing House; 2008a. p. 888–965.
Jiang S-C, GU R, Zheng-Min W. Otorhinolaryngology – otology. 2nd ed. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2002c. p. 754–75.
Zheng-Min W. Microsurgery of the ear. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2004c. p. 125–41.
Reconstruction of Ossicular Chain/Ossiculoplasty
Huang X-Z, Wang J-B, Kong W-J. Practice of otorhinolaryngology head and neck surgery. 2nd ed. Beijing: People’s Medical Publishing House; 2008b.
Javia LR, Ruckenstein MJ. Ossiculoplasty. Otolaryngol Clin North Am. 2006;39(6):1177–89.
McGee M, Hough JV. Ossiculoplasty. Otolaryngol Clin North Am. 1999;32(3):471–88.
Samy RN, Pensak ML. Revision ossiculoplasty. Otolaryngol Clin North Am. 2006;39(4):699–712.
Yang W-Y, Zhai S-Q. Head-neck dissection and temporal surgery. Beijing: People’s Military Medical Press; 2002.
Yu Y-J, Dai P, Liu Z. Stereo anatomical and surgical atlas of temporal bone. Beijing: People’s Military Medical Press; 2006a.
Mastoidectomy (Open Cavity)
Huang X-Z, Wang J-B, Kong W-J. Practice of otorhinolaryngology head and neck surgery. 2nd ed. Beijing: People’s Medical Publishing House; 2008c.
Jiang S-C, Gu R, Zheng-Min W. Otorhinolaryngology – otology. 2nd ed. Shanghai: Shanghai Scientific and Technological Education Publishing House; 2002d.
Jiang S.-C, Yang W.-Y, Gu R. Operative surgery of otorhinolaryngology head and neck department. In: The complete works of operative surgery. 2nd ed. Beijing: People’s Military Medical Press; 2005.
Modified Radical Mastoidectomy
Huang X-Z, Wang J-B, Kong W-J. Practice of otorhinolaryngology head and neck surgery. 2nd ed. Beijing: People’s Medical Publishing House; 2008d.
Jiang S.-C, Yang W.-Y, Gu R. Operative surgery of otorhinolaryngology head and neck department. In: The complete works of operative surgery. 2nd ed. Beijing: People’s Military Medical Press; 2005.
Sanna M, et al. The temporal bone a maunal for dissection and surgical apporaches. New York: Thieme; 2005.
Yu Y-J, Dai P, Liu Z. Stereo anatomical and surgical atlas of temporal bone. Beijing: People’s Military Medical Press; 2006b.
Mastoidectomy (Closed Cavity)
Coker NJ, Jenkins HA. Atlas of otologic surgery. Philadelphia: Saunders; 2001.
Jiang S.-C, Yang W.-Y, Gu R. Operative surgery of otorhinolaryngology head and neck department. In: The complete works of operative surgery. 2nd ed. Beijing: People’s Military Medical Press; 2005.
Yu Y-J, Dai P, Liu Z. Stereo anatomical and surgical atlas of temporal bone. Beijing: People’s Military Medical Press; 2006c.
Mastoid Obliteration, Canal Wall Reconstruction and Tympanoplasty
Della Santina CC, Lee SC. Ceravital reconstruction of canal wall down mastoidectomy: long-term results. Arch Otolaryngol Head Neck Surg. 2006;132(6):617–23.
Ni Y, Hirsch BE, Da-zhang Y, et al. Outcome analysis of 40 ossiculoplasty cases. Chinese J Otol. 2005;3(2):100–3.
Ucar C. Canal wall reconstruction and mastoid obliteration with composite multifractured osteoperiosteal flap. Eur Arch Otorhinolaryngol. 2006;263(12):1082–6.
Ossicular Chain Reconstruction for Congenital Deformity or Trauma
Bahmad Jr F, Merchant SN. Histopathology of ossicular grafts and implants in chronic otitis media. Ann Otol Rhinol Laryngol. 2007;116(3):181–91.
Brackmann D, Shelton C, Arriaga MA. Otologic surgery. 2nd ed. Philadelphia: Saunders; 2001.
Caldart AU, Terruel I, Enge Jr DJ, Kurogi AS, Buschle M. Adriana Sayuri Kurogi, Maurício Buschle. Stapes surgery in residency – the ufpr clinical hospitalexperience. Braz J Otorhinolaryngol. 2007;73(5):647–53.
Elsheikh MN, Elsherief H, Elsherief S. Physiologic reestablishment of ossicular continuity during excision of retraction pockets: use of hydroxyapatite bone cement for rebridging the incus. Arch Otolaryngol Head Neck Surg. 2006;132(2):196–9.
Fenli X, Keli C. Clinical study of congenital middle ear malformations. J Clin Otorhinol. 2004;18(10):586–9.
Hu U, Qiu-ju W, Dong-yi H. Clinical classification and relationship with conductive deafness of congenital middle ear malformations. Chinese J Otorhinol Head Neck Surg. 2005;40(12):893–5.
Lesinskas E, Vainutiene V. Closed tympanoplasty in middle ear cholesteatoma surgery. Medicina (Kaunas). 2004;40(9):856–9.
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media Singapore and People's Medical Publishing House
About this chapter
Cite this chapter
Dai, P. et al. (2017). Mastoid and Middle Ear Surgery. In: Dai, P., Han, Dy., Cousins, V., Song, Ys. (eds) Stereo Operative Atlas of Micro Ear Surgery. Springer, Singapore. https://doi.org/10.1007/978-981-10-2089-6_2
Download citation
DOI: https://doi.org/10.1007/978-981-10-2089-6_2
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-2088-9
Online ISBN: 978-981-10-2089-6
eBook Packages: MedicineMedicine (R0)