
Abstract
X-linked adrenoleukodystrophy (ALD) especially in childhood cerebral type is a metabolic degenerative disease with a severe clinical course of progressive deterioration until death involving progressive demyelination of the central nervous system caused by a defect in the ABCD1 gene at Xq28.
The frequency of hearing impairment has been reported in a rather high percentage of the patients but the other apparent deteriorating motor, mental, and visual symptoms are often concealed. Thus central auditory dysfunction is not fully recognized and it is difficult to support patients directly for their difficulties from their handicaps. These symptoms are due to the localized brain lesions but because of the character of disease, the lesions continuously and progressively expanded to the whole white matter of the brain without treatment.
The duration of apparent hearing impairment continued not so long in their natural history. Serial change could be evaluated clinically, nerophysiologically, and neurophysiologically.
There are some types of leukodystrophy but they usually progress rapidly in the brain and the lesion expansion is almost uniform. Therefore, it seems difficult to recognize symptoms based only on the localized brain lesions. Even during the clinical evaluation of an ALD patient, such symptoms may often be overlooked.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Etiology and Clinical Course of the Disease
X-linked adrenoleukodystrophy (ALD) is a metabolic degenerative disease with a severe clinical course of progressive deterioration until death involving progressive demyelination of the central nervous system, adrenal dysfunction, and accumulation of saturated very long-chain fatty acids (VLCFA) in various tissues and body fluids. It is caused by a defect in the ABCD1 gene at Xq28 which encodes for a peroxisomal membrane protein (Mosser et al. 1993).
2 Clinical Types of ALD and Their Signs and Symptoms
There are several clinical phenotypes which are usually classified as childhood cerebral type (CCALD), adolescent cerebral type (AdolCALD), adult cerebral type (ACALD), adrenomyeloneuropathy (AMN), cerebello-brainstem type (CB-BS ALD), Addison type (ALD with Addison disease), preclinical male patients (PCM), and females with apparent symptoms.
Two cerebral types of ALD (CCALD and AdolCALD) may often initially present with gait disturbances, strabismus, abnormal vision, visual dysfunction, and intellectual and/or behavioral changes around 6–10 years old.
The prognosis of CCALD is very poor and patients usually pass away within a few years after their clinical onset followed by their deterioration of their physical and intellectual abilities (Suzuki et al. 2005). The prognosis of patients with AdolCALD is somewhat better.
The survey of hospitalized patients by Suzuki et al. gave light to the natural history of ALD: the initial symptoms of childhood cerebral-type ALD were intellectual deterioration 16/46, visual signs/symptoms 11/46, gait disturbance 4/46, psychic symptoms 4/46 and hearing disorder 3/46, and adrenal insufficiency 1/46 (Suzuki et al. 2005) (Table 8.1).
Tanaka et al. also examined the initial symptoms of their ALD. They reported that hearing problems presented as the initial symptom of their patients was noted in 13% of ALD patients (Tanaka et al. 1989) (Table 8.2).
Thus, hearing problems were not a rare finding and this should be importantly considered in the diagnosis of ALD. Usually, patients’ intellectual deterioration, gait disturbance, and visual impairment are more easily detected by their family members and teachers than are their hearing disorder.
The Kaplan–Meier neurological progression evaluation in patients with ALD informs us that patients with CCALD are not symptom-free after following 1.3 years after their diagnoses of ALD and even patients with AMN show a gait disturbance within 4–5 months after their diagnosis (Suzuki et al. 2005) (Fig. 8.1).

Kaplan–Meier plot of neurological progression in patients with ALD (Suzuki et al. 2005). (a) Childhood cerebral form, (b) adrenomyeloneuropathy, (c) adult cerebral form. Vertical line shows the ratio of patients with no clinical symptom, horizontal line shows time course (years)
3 Diagnosis of ALD
The diagnosis of ALD is made by the observation of clinical signs, the determination of each patient’s symptoms, and by special testing such as MRI findings and the finding of a high concentration of very long-chain fatty acid (VLCFA) in the serum. A definitive diagnosis nowadays hinges on the confirmation of the disease from a gene mutation in the ABCD1 gene. However, it is impossible to differentiate the various clinical manifestations of the disease from the gene mutation itself or from the clinical types of the patients’ relatives, even those who are their siblings. Clinically, presence of certain symptoms and confirmation of MRI lesions are the best way to diagnose ALD. However, neuropsychological/cognitive symptoms might be present before the appearance of MRI lesions (Furushima et al. 2009; Kaga et al. 2009). The introduction of ALD as part of the neonatal screening (Vogel et al. 2015) is a recent trend in several states in the USA and some European countries. This trend will ultimately positively impact the clinical care of ALD patients before the emergence of their clinical manifestations of the disease. On another front, such patients and their parents will no longer spend peaceful lives, but they will also have agonizing length of time which will continue as long as 5–50 years before having a specific diagnosis.
4 Hearing Impairment in ALD
Hearing impairment in ALD is primarily of central origin and is not due to an inner ear or cochlear lesion. In other words, the etiology of hearing impairment in ALD arises from white matter lesions in the auditory pathway. Of course, some patients have co-existing conductive hearing impairment due to otitis media. Hearing impairment has been found to the initial symptom of ALD (Tanaka et al. 1989; Suzuki et al. 2005) (Tables 8.1 and 8.2) but the actual details of the audiometric findings of the disease have not been described. This is probably due to the rapid progression of the disease which often leads to total disability or even death (Moser 2000, 2001; Peters et al. 2004). Moser HW in 2000 reported that CCALD seems to be the most grievous type of this disease because of its rapid progress and poor prognosis which result in loss of physical function and in a short life expectancy.
5 Evaluation of Hearing in ALD
A standard hearing test for patients is pure tone audiometry. For infants, toddlers, and younger children, behavioral observation audiometry (BOA), conditioned orientation reflex audiometry (COR), and play audiometry are attempted and are used based on the patients’ chronological or developmental age. Word discrimination tests (WDC), the environmental sound discrimination, token tests, dichotic listening tests (DLT), and sound lateralization tests are designated to evaluate precisely auditory cognitive function. Objective tests of auditory function include auditory brainstem responses (ABR) and otoacoustic emissions (OAEs). At the beginning of the disease, some patients request repetitions of speech input or they simply declare that they cannot hear (Fig. 8.2). Because of this, these patients are often misdiagnosed with a psychological reaction and a hearing impairment is not considered.

Serial change of audiogram in a patient with ALD (Kaga et al. 1980)
Hearing assessment in symptomatic patients with CCALD has indicated that a significant percentage of these patients had hearing impairment to some degree (Kaga et al. 2015).
To better understand auditory agnosia in ALD patients, the author presents three ALD patients with typical auditory agnosia which was severe and was difficult to understand initially, by family members and clinicians during the early clinical course of the disease.
6 Case Reports of Japanese Patients with ALD and Auditory Agnosia (Furushima et al. 2015)
6.1 Case Histories of Three Patients
6.1.1 Patient 1
This patient was a 3-year-old boy. He began to respond poorly when called and to ask back frequently to have incoming speech to be reacted. His hearing test at school was normal. In that his hearing continued to decline, he was seen by an otolaryngologist 3 months later. His pure tone audiogram was normal at two visits to this clinic. It gradually became difficult for him to converse and he then lost the ability on the phone. He seemed not to comprehend his own hearing difficulty. This was later thought to be anosognosia. Other than his hearing problems he was completely normal. He was referred to a hospital at 13 years and 4 months of age. He was then diagnosed with CALD because of brain lesions on his MRI, elevated plasma VLCFA, and the presence of mutation of the ABCD1 gene. His adrenal function was normal.
His condition prompted further neuropsychological and neurophysiological evaluation and he was thus referred to us. At our first encounter with him, he could only answer very simple questions such as his name or his age. His corrected visual acuity was 0.1 in his left eye and 0.6 in his right eye. He was found to have a left homonymous quadrantanopia. His pupils were dilated and reacted sluggishly to light. No pyramidal, cerebellar nor sensorineural signs were evident. Left to right transport impairment of tactile sensation and positional information was intact.
6.1.2 Patient 2
This patient was an 11-year-old boy. He began to complain of difficulty and fatigue with hearing other people’s speech. He often did not respond to instructions given to him and he was thought to be absent-minded. His teacher noticed that he had poor reactions when he was called upon, he looked at his textbook upside down, he wore his gym suits backward (later it was thought to be a dressing apraxia) and he wrote confused and inaccurate letters. One year later he visited a psychiatric clinic whereupon he was referred to a university hospital. He then visited a pediatric clinic and was subsequently referred to a university hospital and he was diagnosed with CALD. The MRI showed characteristic signal changes, a high titer of VLCFA and a mutation of the ABCD1 gene. His ABR was normal. Left homonymous hemianopia was detected and he had partial adrenal insufficiency. He gradually became short-tempered. Six months after the onset of his disease, he was referred to our clinic for detailed evaluation. At the time his physical examination was normal and he had no abnormal skin pigmentation. He could only engage in short and simple conversation. His deep tendon reflexes were exaggerated on his lower extremities although his muscle tonus was normal. Response to both tactile and painful stimuli was unstable. Position and vibratory senses were impaired over his left lower limb.
His SVR and MMN findings are presented in Fig. 8.3.

MMN and SVR of a patient with ALD. 13 years old, boy
6.1.3 Patient 3
This patient was a 10-year-old boy. He did well until his 10th birthday and began to respond less and less when he was spoken to. He began to move slowly, become inactive (stagnated), and he ceased spending time with his friends. His school performance declined. Five months later his hearing was found to be normal by an otolaryngologist; however, his response to voices on the phone decreased and he often asked speakers to repeat themselves. He was consequently referred to a pediatrician who made the diagnosis of CALD based on the following findings: brain lesions on his MRI, elevated VLCFA, and intellectual deterioration. Adrenal function was normal.
At 10 years and 9 months of age, he was referred to us for further evaluation. His physical examinations were normal. He displayed emotional incontinence and marked separation anxiety from his mother. On confrontation, he had a left-sided constriction of his visual field. His Achilles tendon reflexes were exaggerated and an ankle clonus was found in his right lower limb. Tactile, positional, and vibratory senses were normal.
6.2 MRIs of the Above Patients
6.2.1 Patient 1 (Fig. 8.4a)
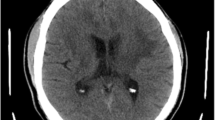
In Fig. 8.4a, axial sections of FLAIR images from patient 1 and a coronal section of enhanced T1-weighed image are shown. FLAIR images indicated signal intensity changes in the auditory pathway (bilateral brachium of the inferior colliculus to medial geniculate body with right auditory radiation) and visual pathway changes over the bilateral lateral geniculate body with right optic radiation. Material-enhanced T1-weighted images revealed enhanced activity in his left medial geniculate body.

MRI of three patients with auditory agnosia due to ALD (Furushima et al. 2015)
6.2.2 Patient 2 (Fig. 8.4b)
Axial and coronal sections of his FLAIR images are also presented. FLAIR images show signal intensity changes in his auditory pathway (bilateral trapezius body ~ lateral lemunisci ~ brachium of the inferior colliculus to the medial geniculate body ~ auditory radiation) and signal intensity changes in his visual pathway (bilateral lateral geniculate body ~ optic radiation) and the splenium of corpus callosum.
6.2.3 Patient 3 (Fig. 8.4c)
The axial and coronal sections of FLAIR images in patient 3 are presented. The flair images show signal intensity changes in the auditory pathways (bilateral brachium of the inferior colliculis to medial geniculate body to auditory radiation) and visual pathway intensity changes bilateral lateral geniculate bodies to optic radiation.
6.3 Audiograms
Pure tone audiograms and word discrimination test scores for each patient are presented in Fig. 8.5.

Audiogram of three patients with auditory agnosia due to ALD (Furushima et al. 2015). All patients showed an almost normal pure tone audiogram but markedly abnormal speech audiogram
In each case, when compared to their pure tone audiogram findings, these patients’ word discrimination scores were markedly worse. This finding delineates auditory verbal agnosia and nonverbal agnosia.
Serial change of audiogram was presented by Kaga in 1980.
6.4 ABR Findings
ABR tracings are presented in Fig. 8.6.

ABR of three patients with auditory agnosia due to ALD (Furushima et al. 2015). All patients showed normal waveform of ABR and wave V threshold. Patient 3 showed prolonged latency of wave V and central conduction
The basic waveform configurations and response thresholds were almost normal in each patient. The precise evaluation of each patient’s evoked waveforms is described below:
- Pt 1:
-
Interpeak latency of Wave I and III was prolonged on the left side. The threshold of wave V was normal.
- Pt 2:
-
Interpeak latency of Wave I and V was prolonged on the left. The threshold of wave V was normal.
- Pt 3 :
-
Interpeak latency of Wave I and V was prolonged bilaterally. The threshold of wave V was normal. Serial change of ABRs is presented by Kaga et al. in 1980 (Fig. 8.7) and Inagaki et al. in 2006 (Fig. 8.8).

Serial change of ABR in a patient with ALD (Kaga et al. 1980, altered by the author)

Serial change of ABR in a patient with ALD (Inagaki et al. 2006). The patient’s motor and mental development was normal until 8 years and 1 month old. His first symptom was a defect of the visual field. He was admitted to a hospital aged 8 years and 11 months. He gradually lost his ability and became bedridden at last. His ABR was normal in shape, latency, and amplitude after the onset of his disease (9 years and 1 month). However, interpeak latency of I–V gradually became prolonged and all waves reduced their amplitude. Three years from the onset, wave V disappeared finally.
Figures noted in blankets are the time course from his onset of the disease
6.5 SVR and MMN
The evoked N1s of the slow vertex response (SVR) and the evoked mismatch negativity (MMN) response to verbal and nonverbal stimuli are useful to evaluate the objective and unconscious cognition of verbal and nonverbal auditory stimuli. In this section, we will show the results of SVR and MMN to nonverbal (tone burst, [1KHz][2KHz]) and verbal (vowel sound, [a][æ]) stimuli. The occurence of the stimuli is 80% for the former and 20% for the latter, in each stimuli. These results point out the disparity of findings between the use of these different stimuli in patients with auditory agnosia due to ALD. This stimulus-dependent disparity between results of SVR and MMN in patient 2 is shown in Fig. 8.9.

Patient 2, ALD, boy, 11 years (Furushima et al. 2015)
Serial change of SVR was presented by Kaga (Fig. 8.10).

Serial change of SVR in a patient with ALD (Kaga et al. 1980)
7 Summary
7.1 Hearing Impairment
The frequency of hearing impairment as the initial symptom of ALD has been reported to be between 6 and 7% (childhood cerebral type 3/46 and adolescent cerebral type 1/14, Suzuki et al. 2005), 8% in childhood cerebral type N = 160 (The Metabolics & Molecular Bases of Inherited diseases, 8th edition) and 13% (childhood and adolescent cerebral type 5/38, Tanaka et al. 1989).
All three of the above-described patients had in common: (1) a severe loss of word discrimination scores compared to their relatively normal pure tone acuity, (2) good ability to recognize, understand, and respond a non-auditory route or appropriately to help that which was spoken to them by using non-auditory route, they could perform quite well, (3) no paraphasia was noted in any patient. We thus determined that these patients had auditory agnosia and not aphasia. These patients could recognize verbal and environmental sounds when they were accompanied by visual aids (presented with pictures and lip reading). Verbal stimuli coming from outside their visual field was hard to recognize for these patients. Conversations on the telephone were very difficult for them because they had no visual cues.
7.2 Auditory and Other Symptoms Caused by Localized Brain Lesions in Patients with ALD
Abnormal MRIs confirmed bilateral medial geniculate body abnormalities and unilateral or bilateral auditory radiation in all three of the above ALD patients. ALD is basically a disease of the white matter, lesions in the auditory cortex of these patients were not observed at least not in the early stage of their disease. Thus, auditory agnosia occurs due to a disconnection between the auditory cortex and the subcortical white matter. Auditory agnosia was therefore a clinical diagnosis based on finding (by MRI) localized white matter lesions each of these in these patients’ auditory pathways.
Moreover, there are some patients who showed agnosia of their disease, and apraxia while dressing. Those symptoms were considered as due to cortical lesions. However, ALD can play a role in emerging temporal, parietal, and frontal signs and symptoms based on the extensiveness of the white matter lesions when they can be tested by neurologically.
Serial change could be evaluated clinically and nerophysiologically.
There are other types of leukodystrophy such as Groboid cell leukodystrophy (Krabbe disease), metachromatic leukodystrophy, Alexander disease, and others. These disorders also present a slow progressive course with the possibility of developing emerging focal cortical lesions as seen in ALD. However, patients with these diseases rarely show symptoms caused by localized brain lesions. This is because these diseases usually progress rapidly in the brain and the lesion expansion is almost uniform. Therefore, it is very difficult to recognize symptoms based only on MRI images of localized brain lesions. Even during the clinical evaluation of an ALD patient, such symptoms may often be overlooked.
References
Furushima W, Inagaki M, Gunji A, Inoue Y, Kaga M, Mizutani S. Early signs of visual perception and evoked potentials in radiologically asymptomatic boys with X-LInked adrenoleukodystrophy. J Child Neurol. 2009;24:927−35.
Furushima W, Kaga M, Nakamura M, Gunji A, Inagaki M. Auditory agnosia as a clinical symptom of childhood adrenoleukodystrophy. Brain Dev. 2015;37:690–7.
Inagaki M, Kaga Y, Kaga M, Nihei K. Multimodal evoked potentials in patients with pediatric leukodystrophy. Suppl Clin Neurophysiol. 2006;59:251–63.
Kaga K, Tokoro Y, Tanaka Y, Ushijima H. The progress of adrenoleukodystrophy as revealed by auditory brainstem evoked responses and brainstem histology. Arch Otorhinolaryngol. 1980;228:17–27.
Kaga M, Furushima W, Inagaki M, Nakamura M. Early neuropsychological signs of childhood adrenoleukodystrophy (ALD). Brain Dev. 2009;31:558−61.
Kaga M, Nakamura M, Furushima W, Gunji A, Sakihara K, Inagaki M. Auditory function in patients with adrenoleukodystrophy. In: 11th European Paediatr Neurology Society Congress. May; Wien, AT. 2015.
Moser HW, Loes DJ, Melhem ER, Raymond GV, Bezman L, Cox CS, et al. X-linked adrenoleukodystrophy: overview and prognosis as a function of age and brain magnetic resonance imaging abnormality. A study involving 372 patients. Neuropediatrics. 2000;31:277–39.
Moser HW, Smith KD, Watkins PA, Powers J, Moser AB. X-linked adrenoleukodystrophy. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The metabolic and molecular bases of inherited disease, vol. 2. 8th ed. New York: McGraw-Hill; 2001. p. 3257–301.
Mosser J, Douar AM, Sarde CO, Kioschis P, Feil R, Moser H, et al. Putative X-linked adrenoleukodystrophy gene shares unexpected homology with ABC transporters. Nature. 1993;361:726–30.
Peters C, Charnas LR, Tan Y, Ziegler RS, Shapiro EG, DeFor T, et al. Cerebral X-linked adrenoleukodystrophy: the international hematopoietic cell transplantation experience from 1982 to 1999. Blood. 2004;104:881–8.
Suzuki Y, Takemoto Y, Shimozawa N, Imanaka T, Kato S, Furuya H, et al. Natural history of X-linked adrenoleukodystrophy in Japan. Brain Dev. 2005;27:353–7.
Tanaka K, Naruto T, Yamamoto H, Nishizawa R, Izeki E, Shimada M. Early symptoms and signs of adrenoleukodystrophy. J Jpn Pediatr Soc. 1989;93:950–5. Japanese.
Vogel BH, Bradley SE, Adams DJ, D’Aco K, Erbe RW, Fong C, Iglesias A, Kronn D, Levy P, Morrissey M, Orsini J, Parton P, Pellegrino J, Saavedra-Matiz CA, Shur N, Wasserstein M, Raymond GV, Caggana M. Newborn screening for X-linked adrenoleukodystrophy in New York State: diagnostic protocol, surveillance protocol and treatment guidelines. Mol Genet Metab. 2015;114:599–603.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2021 Springer Science+Business Media Singapore
About this chapter

Cite this chapter
Kaga, M. (2021). Adrenoleukodystrophy (ALD). In: Landau-Kleffner Syndrome and Central Auditory Disorders in Children. Modern Otology and Neurotology. Springer, Singapore. https://doi.org/10.1007/978-981-10-1479-6_8
Download citation
DOI: https://doi.org/10.1007/978-981-10-1479-6_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-1478-9
Online ISBN: 978-981-10-1479-6
eBook Packages: MedicineMedicine (R0)