
Abstract
After the onset of an ischemic stroke, every minute is important for reducing ischemic brain injury. Patients with suspected ischemic stroke require rapid and efficient evaluation to identify those who are eligible for time-sensitive reperfusion therapies. Establishing the exact time of stroke onset is of utmost importance. After taking the history of the patient, a rapid physical and neurologic examination including stroke scale is necessary. In patients with stable vital signs, emergent non-contrast-enhanced computed tomography (NECT) should be performed to exclude intracerebral hemorrhage. If NECT is interpreted as an ischemic stroke, immediately obtaining a computed tomography angiography (CTA) and perfusion CT may aid in making therapeutic decisions for intra-arterial thrombectomy without time delay. Laboratory and cardiac evaluations should also be performed as soon as possible to exclude conditions that mimic strokes by examining metabolic abnormalities and to confirm exclusion criteria for intravenous thrombolysis. To ensure timely treatment after arrival to the emergency department, the cooperation of the stroke teams, including emergency medical physicians, neurologists, intervention team, nursing staff, and medical technicians, is important. Since intra-arterial thrombectomy has been successful in patients with middle cerebral artery or internal carotid artery occlusion, reducing the time from door to groin puncture is another key component of acute treatment for ischemic stroke. This chapter emphasizes the rapid management of patients with suspected ischemic stroke and focuses on what physicians should do during this stage. Additional medical management techniques specific to the emergency department will be discussed briefly.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


The first few hours after the onset of stroke symptoms provide a crucial intervention window to prevent permanent disability or death. The major goal in this hyperacute stage is to reduce infarct volume and to minimize neurologic deficits. If the occluded vessels are successfully recanalized, the patients will improve and penumbral zones will be normalized. With no recanalization, penumbral tissues will turn into areas of permanent infarction with severe symptoms persisting. Because earlier recanalization results in a better outcome, a systematic approach to reduce time delay should be emphasized in this stage by the collaboration of stroke teams. A consensus panel convened by the National Institutes of Neurological Disorders and Stroke (NINDS) established goals for time frames in the evaluation of stroke patients in the emergency department (Table 5.1) [1]. However, stroke teams may not satisfy to meet the recommended time frame and should make every effort to reduce time delays.
1 Establishing Time of Stroke Onset and History Taking
If stroke symptoms are recognized by emergency physicians, “stroke code” should be activated immediately. In some well-developed areas, emergency medical service (EMS) personnel are trained to identify stroke symptoms, and the stroke team could be alerted on the way to the hospital. Following stroke code activation, the exact time of symptom onset should be determined because time-dependent treatments are performed based on this information. Physicians should ask patients when the stroke symptoms began. However, the patient may not be able to talk about their symptoms or onset status due to neurologic deficits or comorbidities. In this situation, obtaining a detailed history from family members, witnesses who observed the onset of the stroke, and emergency medical personnel can provide valuable information. In addition, any observations of the patient during daily activities might be evaluated with cautious history taking, as a patient’s daily routine may aid in providing a stroke onset time. Cellular phone recordings could also verify the normal status of the patient. Because therapeutic intervention in this stage carries risk and requires rapid decision, the physician may contact responsible family members or a legally authorized representative to discuss the possible risks or benefits of the intervention.
Additional history about the patient should also be obtained quickly. Risk factors such as hypertension, diabetes mellitus, dyslipidemia, and cardiac disease, as well as migraine, seizure, trauma, drug abuse, alcohol abuse, pregnancy, and previous stroke history, should be noted. Medication history including the use of antithrombotics should be obtained. Intravenous thrombolysis exclusion criteria should be assessed in a timely manner. In addition, the patient’s weight is needed to determine the dose of recombinant tissue plasminogen activator (rtPA).
2 Physical Examination
After the airway, breathing, and circulation of the patient have been assessed and vital signs including blood pressure, heart rate, oxygen saturation, and temperature have been recorded, a more detailed physical examination should be performed. Ageneral physical examination is important to identify possible etiologic factors for ischemic stroke as well as possible complications and coexisting comorbidities. Examination of the face and head may reveal signs of trauma. Auscultation of the neck and chest may reveal carotid bruits and cardiac murmurs, arrhythmias, and rales, respectively. Skin and extremity examination may reveal a few signs specific to coagulopathies, platelet disorders, trauma, or embolic lesions. Because acute comorbidities may influence the selection of an acute treatment, a thorough but brief examination is necessary.
3 Neurologic Examination and Stroke Scales
The neurological evaluation of an acute stroke patient must be brief and efficient. An experienced neurologist should immediately assess the level of consciousness and breathing patterns. If patients are alert and able to respond to verbal stimuli, neurological examinations should be performed based on common stroke scales, such as the National Institutes of Health Stroke Scale (NIHSS) (Table 5.2). The scales have demonstrated their utility and can be administered by a broad spectrum of health providers [2]. Use of a standard stroke scale helps quantify the degree of neurological deficits and facilitate communication among stroke teams. When a patient’s consciousness is impaired, neurologists should uncover localizing and lateralizing signs. Deviation of the eyes or head, air-escaping pattern of the face, asymmetric withdrawal response to noxious stimuli, asymmetric brainstem reflexes, and asymmetric pathologic reflexes are examples of brain damage. A thorough neurological examination is necessary in patients who are unconscious to rule out conditions that may mimic stroke. Although intravenous rtPA use in stroke mimics does not show harmful effects, thrombolytic treatment of stroke mimics should be under 3% based on non-contrast-enhanced computed tomography (NECT) alone [3].
4 Emergency Management of Stroke Patients
4.1 Brain and Vascular Imaging
Imaging of the brain with NECT is crucial to confirm the diagnosis of cerebral hemorrhage, which appears as an area of high density. It is widely used in almost all hospitals because it is inexpensive, noninvasive, and easily accessible. It is the single most important imaging modality because a decision of intravenous thrombolysis can be easily made, and it can also reveal brain tumors, which would be a contraindication to thrombolysis. NECT may show early signs of infarction such as a loss of gray-white matter interface among the nuclei of the basal ganglia and insular cortex. Cortical swelling by cerebral ischemia may produce sulcal effacement, and early arterial occlusion may show signs of a hyperdense vessel. When these signs of early infarct are present, the degree of ischemia will be more profound and the outcome will be poor [4].
Diffusion-weighted imaging (DWI) of the brain is the most sensitive and specific imaging for acute infarct even in the early stages of a stroke. It can differentiate an old infarction from a recent infarction and detect relatively small lesions in the brainstem, which are poorly visualized with NECT. In the hyperacute stage of ischemic stroke, visible diffusion lesions will include both regions of irreversible infarctions with more severe apparent diffusion coefficient (ADC) changes and regions of salvageable penumbra with less severe ADC changes. Standard MRI sequences (T1-weighted, T2-weighted, fluid-attenuated inversion recovery [FLAIR]) are relatively insensitive to acute stroke but may be useful to diagnose stroke mimics such as seizure and metabolic abnormalities. DWI/FLAIR mismatch has been recently suggested, especially in patients with unclear onset or wake-up stroke. It is a concept based on DWI changes beginning with the onset of stroke and FLAIR changes that are apparent after 3 h. However, it should only be used in specific conditions and on an individual basis [5]. Susceptibility-weighted imaging (SWI) and gradient echo imaging (GRE) are able to detect very small amounts of deoxyhemoglobin and intracerebral hemorrhages and microbleeds. Based on these MRI findings, they could be used as an initial imaging modality to evaluate acute stroke patients. However, if MRI scans are not readily available for 24 h, as in most hospitals, time should not be wasted waiting for MRI results.
Vascular imaging in the state of hyperacute stroke is an emerging field because intra-arterial thrombectomy of middle cerebral artery (MCA) or internal carotid artery (ICA) occlusions has been associated with improved functional outcomes and higher rates of recanalization without the increase of symptomatic intracranial hemorrhage [6]. Helical CT angiography (CTA) is a quick, noninvasive method to evaluate the intracranial and extracranial vasculature in the acute stroke stage with high sensitivity and specificity. Since a CTA could be acquired immediately after NECT and lasts less than 5 min, a time-saving decision could be made to perform a CTA while in the CT room. In the presence of large artery occlusions such as MCA or ICA, an intervention team alert for endovascular thrombectomy is necessary at this time. MR angiography (MRA) or Doppler ultrasound can also evaluate intracranial vasculature. However, important limitations include a long acquisition time and less accuracy. Conventional angiography is rarely required during the hyperacute phase of stroke evaluation. It should be reserved for situations where intra-arterial thrombectomy is required.
Perfusion CT or MRI that reveal parenchymal perfusion of the patient may provide additional information to identify potentially salvageable brain tissue. This will better identify those patients who are most likely to benefit from reperfusion therapy, which is especially useful in patients with an unclear stroke onset. Brain perfusion imaging provides information about regional cerebral hemodynamics such as cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), and time to peak (TTP). It can delineate an infarct core and penumbral tissue by using CBF-CBV mismatched areas on a perfusion imaging. On the other hand, the penumbra is indicated as DWI-perfusion-weighted imaging in mismatched areas on a perfusion MRI. There is a growing body of reports that those mismatched areas are potentially salvageable and are an ideal target for neuroprotection or reperfusion therapies [7]. However, the acquisition of additional imaging should not delay treatment with intravenous thrombolysis and should be performed only in a hospital where rapid processing is possible. Recent advances in CT machines and software enable angiography and perfusion imaging to be obtained simultaneously after NECT (Fig. 5.1).

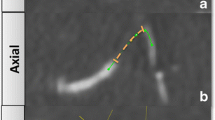
CT and MRI images from a 55-year-old man with the sudden onset of dysarthria and left-sided weakness 60 min earlier. NECT appears normal without early ischemic changes (a). Perfusion CT was immediately obtained after NECT and shows CBF (b) and CBV (c) mismatch (arrows). Reconstructed angiography based on perfusion CT shows obstruction of the internal carotid artery (d). Intravenous rtPA was administered and patient symptoms subsided except for mild dysarthria. Brain MRI was performed 24 h after initial symptoms. DWI (e) and FLAIR (f) show permanent infarction (arrows), and TOF-MRA (g) shows recanalization of internal carotid artery. Contrast-enhanced MRA showed severe stenosis at the proximal internal carotid artery (arrow) (h). CT computed tomography, MRI magnetic resonance image, NECT non-contrast-enhanced computed tomography, CBF cerebral blood flow, CBV cerebral blood volume, rtPA recombinant tissue plasminogen activator, DWI diffusion-weighted image, FLAIR fluid-attenuated inversion recovery, TOF-MRA time-of-flight magnetic resonance angiography
After an intravenous rtPA is administered based on the CT or MRI, patients with large artery occlusions (MCA, ICA) should perform conventional angiography. In this situation, a conventional angiography with intra-arterial thrombectomy should be readied by interventional teams. If the conventional angiography still shows a large artery occlusion, mechanical thrombectomy with Solitaire or Trevo should be used to recanalize the occluded artery [6]. When intravenous thrombolysis is contraindicated in a patient, intra-arterial thrombectomy can be performed independently. Detailed methods and evidence will be dealt with in subsequent chapters.
4.2 Ancillary Laboratory Tests
A few laboratory tests are routinely required during the initial evaluation of patients who have a suspected stroke. The results of these tests may provide information about serious comorbid diseases and conditions that can mimic stroke and possible stroke etiology. These tests may assist with therapeutic decision-making, especially to identify if intravenous thrombolysis is contraindicated. This is extremely valuable when the patient’s history is vague or inconclusive. Routine laboratory tests should include blood glucose, electrolytes with renal function tests, complete blood count with platelet count, liver function tests, prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (aPTT), and cardiac enzymes (creatine kinase (CK), CK-MB, troponin). In addition, a chest radiograph should be obtained in all stroke patients. It may show a widened mediastinum indicative of an aortic dissection that can mimic stroke, cardiomegaly, or pulmonary edema, which is indicative of heart failure. An electrocardiogram (ECG) should also be performed in all patients to determine the cause of the stroke and to optimize immediate and long-term management. Due to the close association between stroke and cardiac abnormalities, it is important to assess the cardiovascular status of patients presenting with acute stroke. Baseline ECG, chest radiograph, and cardiac biomarkers may identify concurrent myocardial ischemia or cardiac arrhythmias. These routine laboratory tests might be performed in the emergency department setting, if possible, so as not to delay administration of intravenous rtPA.
Some laboratory tests are not routine during a hyperacute stroke evaluation but may be considered in certain patients. Due to the increasing number of patients who are using direct thrombin inhibitors (dabigatran) and direct factor Xa inhibitors (rivaroxaban, apixaban, and edoxaban), it is important to understand what studies may assist in determining anticoagulant effects. The PT/INR is not helpful in determining the anticoagulant effect of those types of medicines. A thrombin time (TT) and ecarin clotting time (ECT) may demonstrate direct thrombin activity. However, it takes a long time to obtain the results [8]. Unfortunately, there is no specific assay for direct factor Xa inhibitor. In young patients, toxicology screening for sympathomimetic drugs (cocaine, methamphetamine, etc.) may identify the underlying cause of the stroke. In women of childbearing age, a pregnancy test is needed because it can affect overall management protocols.
Because time is critical, a limited number of essential diagnostic tests are recommended. Stroke protocols and critical pathways should be clearly defined in all hospitals (Fig. 5.2). Mandatory and selected laboratory tests are described in Table 5.3.

Example for stroke protocol and critical pathway. Algorithm for initial diagnosis and treatment should be clearly defined in all acute stroke care hospitals
5 General Medical Managements in Hyperacute Stage of Ischemic Stroke
In the hyperacute stages of ischemic stroke, management should be focused on reperfusion within the critical period. However, physicians should not neglect management of life-threatening comorbid conditions. Initial assessment of the airway, breathing, and circulation is necessary in the emergency department, and a constant reassessment is required to avoid oxygen desaturation, respiratory compromise, and hypotension. Because patients often suffer a fall after a stroke, the physician should look for traumatic injuries and the neck should be stabilized. In addition, temperature, blood pressure, and blood glucose should be managed properly in the hyperacute stage.
5.1 Airway and Oxygen
Hypoxia frequently occurs after stroke. Common causes of hypoxia are partial airway obstruction, hypoventilation, aspiration, atelectasis, and pneumonia. Patients with a severe stroke presenting with diminished levels of consciousness or brainstem dysfunction may have an increased risk of airway compromise due to impaired oropharyngeal mobility and sensation and loss of protective reflexes. Patients with these conditions or with frequent vomiting may need intubation to protect the airway from aspiration of gastric contents. In addition, prior to the swallowing evaluation, strict avoidance of oral intake is imperative. However, in patients with mild to moderate stroke, routine oxygen supplementation did not show beneficial effects [9]. If patients have less than 94% oxygen saturation, noninvasive oxygen therapy with nasal cannula or with a Venturi mask is recommended [1]. Patients can better maintain oxygen saturation and cerebral perfusion when lying flat in a supine position.
5.2 Intravenous Fluids
Patients with acute ischemic stroke are sometimes hypovolemic, especially those with severe stroke. Hypovolemia should be avoided because it may predispose them to cerebral hypoperfusion and exacerbate brain edema, increased myocardial stress, and renal impairments. Therefore, maintaining iso-osmolar and euvolemic states with isotonic solutions, such as 0.9% saline, is required for patients with acute ischemic stroke. Hypotonic solutions, such as 5% dextrose or 0.45% saline, may distribute into the intracellular spaces and may exacerbate ischemic brain edema. In addition, dextrose-containing fluid may also exacerbate ischemic brain injury. In some patients who have a predisposed vulnerability to intravascular volume overload, such as renal or heart failure, volume replacement should be performed cautiously.
5.3 Temperature
Hyperthermia (above 37.6 °C) is observed in about one third of acute stroke patients. It is associated with stroke severity, infarct size, mortality rate, and a worsened outcome [10]. Thus, lowering the temperature with antipyretics may be beneficial to acute stroke patients. In some situations with occult infections, such as pneumonia, urinary tract infection (UTI), sepsis, and infective endocarditis, patients should be managed with empirical antibiotics.
5.4 Blood Pressure
Arterial blood pressure is commonly increased after an acute ischemic stroke and starts to spontaneously decrease after 90 min of stroke symptoms. Moderately increased blood pressure may augment the delivery of blood to the ischemic area and should be treated conservatively because it can be advantageous to the patient. However, extreme hypertension is clearly harmful because it leads to hypertensive encephalopathy, cardiac complications, renal insufficiency, and hemorrhagic transformation of an ischemic brain. Unfortunately, an ideal blood pressure range has not been scientifically determined. The blood pressure range during an acute ischemic stroke will depend on the stroke subtype and other patient-specific comorbidities. Some conditions, such as myocardial ischemia, aortic dissection, and heart failure, accompany acute ischemic stroke and may be exacerbated by arterial hypertension. However, most guidelines recommend that blood pressure should remain untreated unless the systolic pressure is above 220 mmHg or the diastolic above 120 mmHg. Reasonable blood pressure control should be implemented on a case-by-case basis.
Specific blood pressure management recommendations have been established for acute ischemic stroke patients being considered for thrombolysis therapy (Table 5.4) [1]. These recommendations include a gentle approach to bring the pressure below 185/110 mmHg to qualify for fibrinolytic therapy with intravenous rtPA. Once intravenous rtPA is administered, the blood pressure must be maintained below 180/105 mmHg to reduce the risk of intracerebral hemorrhage. Blood pressure control in the hyperacute stage may be performed by intravenous antihypertensive agents rather than with a single pill medication. It would be beneficial to use short-acting, titratable agents such as labetalol, nicardipine, and esmolol. In patients undergoing intra-arterial thrombectomy, blood pressure should be lowered to prevent reperfusion injury and hemorrhagic transformation. However, the proper range of blood pressure has not yet been determined.
Hypotension should also be avoided because it may decrease cerebral perfusion pressure and increase cerebral edema. To maintain cerebral perfusion, head down, intravenous fluid, inotropic agents, and vasopressors can be used. Since hypotension after an ischemic stroke is rare, physicians should explore medical causes such as myocardial infarction, gastrointestinal bleeding, aortic dissection, and sepsis.
5.5 Blood Glucose
Hypoglycemia is uncommon during the hyperacute stage of ischemic stroke and it is likely to be associated with antidiabetic medications. Hypoglycemia may cause neurological symptoms, including stroke mimics and seizures. These symptoms may be reversible if the hypoglycemia is rapidly corrected. However, severe and prolonged hypoglycemia can result in permanent brain damage. Therefore, blood glucose should be measured as soon as possible in patients with acute ischemic stroke, and low glucose lower than 60 mg/dL should be corrected immediately with a dextrose solution (50% DW).
Hyperglycemia is common during acute ischemic stroke. This increase in blood glucose levels may be associated in part with a nonfasting state and in part to a stress reaction with impaired glucose metabolism. Although a cause and effect relationship could not be determined, many observational studies have found an association between admission hyperglycemia and worsened outcome of strokes [11]. Currently there is no clear target for blood glucose levels during an acute ischemic stroke. It is best to control blood glucose levels with subcutaneous insulin below 180 mg/dL in acute stroke patients. Physicians should monitor glucose to reduce hypoglycemic events that commonly occur after normal correction of hyperglycemia.
Conclusion
A predetermined system for rapid and precise assessment is essential in patients with acute ischemic strokes. The acute stroke teams should be able to perform their own tasks in a parallel manner with minimal delay (Table 5.5). Coordination of these stroke team members in the hyperacute stage may enable them to achieve the main goal of ischemic stroke treatment, which may reduce brain damage and improve outcome.
Suggestions from Clinical Practice Guidelines
For initial evaluation of acute stroke patients, a stroke rating scale such as the National Institutes of Health Stroke Scale (NIHSS) needs to be used. Several laboratory tests including hematologic, coagulation, and biochemistry tests are helpful for emergency care, but blood glucose should be immediately analyzed using a fingertip glucose test. Hypoglycemia (blood glucose level <60 mg/dL) should be normalized by bolus injection of high-dose dextrose solution. Blood pressure is generally observed without control if not reaching 220/120 mmHg. However, if the patient is eligible for intravenous fibrinolysis, the blood pressure should be lowered slowly to <185/110 mmHg. Brain imaging is indispensable for stroke diagnosis in emergency setting. Non-enhanced brain computed tomography should be performed for initial and differential diagnosis of stroke.
References
Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44:870–947.
Lyden P, Raman R, Liu L, et al. National Institutes of Health stroke scale certification is reliable across multiple venues. Stroke. 2009;40:2507–11.
Chernyshev OY, Martin-Schild S, Albright KC, et al. Safety of tPA in stroke mimics and neuroimaging-negative cerebral ischemia. Neurology. 2010;74:1340–5.
Wardlaw JM, Mielke O. Early signs of brain infarction at CT: observer reliability and outcome after thrombolytic treatment—systematic review. Radiology. 2005;235:444–53.
Wouters A, Lemmens R, Dupont P, et al. Wake-up stroke and stroke of unknown onset: a critical review. Front Neurol. 2014;5:153.
Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular thrombectomy for acute ischemic stroke: a meta-analysis. JAMA. 2015;314:1832–43.
Scalzo F, Nour M, Liebeskind DS. Data science of stroke imaging and enlightenment of the penumbra. Front Neurol. 2015;6:8.
Blommel ML, Blommel AL. Dabigatran etexilate: a novel oral direct thrombin inhibitor. Am J Health Syst Pharm. 2011;68:1506–19.
Ronning OM, Guldvog B. Should stroke victims routinely receive supplemental oxygen? A quasi-randomized controlled trial. Stroke. 1999;30:2033–7.
Hajat C, Hajat S, Sharma P. Effects of poststroke pyrexia on stroke outcome: a meta-analysis of studies in patients. Stroke. 2010;31:410–4.
Capes SE, Hunt D, Malmberg K, et al. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426–32.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media Singapore
About this chapter
Cite this chapter
Kim, Y.S. (2017). Initial Diagnosis and Management of Acute Ischemic Stroke. In: Lee, SH. (eds) Stroke Revisited: Diagnosis and Treatment of Ischemic Stroke. Stroke Revisited. Springer, Singapore. https://doi.org/10.1007/978-981-10-1424-6_5
Download citation
DOI: https://doi.org/10.1007/978-981-10-1424-6_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-1423-9
Online ISBN: 978-981-10-1424-6
eBook Packages: MedicineMedicine (R0)