
Abstract
Since the first endoscopic thyroidectomy performed by Huscher et al. (Surg Endosc 11:877, 1997) in 1997, more than 20 different techniques of endoscopic thyroidectomy have been reported. Video-assisted minimal endoscopic thyroidectomy (Miccoli surgery) was first brought up by Miccoli et al. (J Endocrinol Invest 22:849–851, 1999), who accomplished the thyroidectomy through a 2–3 cm incision in neck with the help of endoscope. This surgery decreases the length of the incision in the neck with a better cosmetic result than traditional open surgery. After that, some different approaches of endoscopic thyroidectomy were reported. All of them shifted the incision from neck to more hidden or unexposed sites such as chest wall (Takami and Ikeda, ANZJ Surg 72:841–842, 2002), axillary (Ikeda et al., J Am Coll Surg 191:336–340, 2000) and breast (Ohgami et al., Surg Laparosc Endosc Percutan Tech 10:1–4, 2000) et al. The most obvious advantage of these surgeries is cosmesis. Although in experienced hands, the overall morbidity and mortality haven’t increased, some special complications such as seroma, metastasis along the path of tunnel was reported. Furthermore, robotic assisted endoscopic thyroidectomy was reported (Kang et al., Surgery 146:1048–1055, 2009; Kang et al., J Am Coll Surg 209:e1–e7, 2009; Lee et al., J Oncol 2012:734541, 2012). More complicated surgery such as thyroid carcinoma resection can be performed under robotic assisted endoscope due to its better flexibility. Recently, laparoendoscopic single-site thyroidectomy was reported by some authors (Youben et al., Surg Laparosc Endosc Percutan Tech 21:e192–e196, 2011; Lee et al., J Laparoendosc Adv Surg Tech A 20:839–842, 2010; Fan et al., J Laparoendosc Adv Surg Tech A 21:243–247, 2011). The indications were limited to unilateral benign lesions, such as adenoma or nodule. The procedure was partial lobectomy. Laparoendoscopic single-site thyroidectomy decreased the dissection space, which decreased the postoperative discomfort and complication, at the same time; one incision can achieve the best cosmetic results. During the procedure, the axillary approach was thought the best way although some authors reported breast approach and even trans-oral approach (Nakajo et al., Surg Endosc 27:1105–1110, 2013).So far, we have performed single incision transaxillary endoscopic thyroid lobectomy in more than ten cases with good results.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
10.1 Indications and Case Selection
A single-port totally endoscopic thyroidectomy was offered to patients according to criteria specifying young female gender, unilateral thyroid benign lesion with lesion diameter of less than 3 cm and strong desire for cosmesis.
10.2 Contraindications
-
1.
Patients with history of operation around the neck and proximal upper limbs.
-
2.
Patients with history of thyroiditis or radiation therapy.
-
3.
Patients suffer from malignancy with the thyroid.
-
4.
A lesion located in the thyroid dorsal area (especially adjacent to the tracheoesophageal groove) owing to possible injury to the trachea, esophagus, or recurrent laryngeal nerve (RLN) was also excluded.
-
5.
Patients with inability to tolerate general anesthesia.
-
6.
Patients with relatively operative contraindications.
10.3 Major Instruments or Energy Sources
-
1.
Laparoscopy System
-
2.
SILS port
-
3.
Harmonic scalpel
10.4 Team Setup, Anesthesia and Position
Under general anesthesia, the patient was placed in supine position with the neck slightly extended. The arm on the lesion side was extended to expose the axilla. The position of surgeon, assistants and nurses is shown in Fig. 10.1a, b.

Fig. 10.1
10.5 Key Steps
-
1.
Set up of the subcutaneous tunnel
-
2.
Extension of working space
-
3.
Division of Strap muscle
-
4.
Removal of the lesion of the thyroid
-
5.
Extraction of the specimen
-
6.
Irrigation and suction of working space
-
7.
The placement of drain
10.6 Surgical Techniques
-
1.
Set up of the subcutaneous tunnel
0.1 % epinephrine solution was injected subcutaneously along the operating area for vasoconstriction and hemostasis. A 3 cm incision was made along the skin fold in axilla. The working space was created subcutaneously by gentle dissection with blunt instrument. The dissection range is shown in Fig. 10.1b. Then the single-port was inserted. CO2 was insufflated up to the pressure of 6 mmHg. The 10 mm 30o laparoscopy was inserted (Fig. 10.2a–f).


Fig. 10.2
-
2.
Extension of working space
5 mm scalpel and grasp forceps were inserted through the 5 mm port. The connective tissue was sharply dissected using scalpel to extend the working space further (Fig. 10.3).

Fig. 10.3
-
3.
Division of Strap muscle
The ispilateral sternocleidomastoid muscle was identified. The medial border was dissected with strap muscle. Strap muscle was divided and ispilateral thyroid was exposed (Fig. 10.4a–d).

Fig. 10.4
-
4.
Removal of the lesion of the thyroid
The surface of the thyroid tissue was divided until the lesion was exposed. The lesion was removed with the capsule or with a little normal thyroid tissue (Fig. 10.5a–f).

Fig. 10.5
-
5.
Extraction of the specimen
The specimen was extracted from the incision. Occasionally, the specimen was placed in the bag and extracted from the incision (Fig. 10.6a–c).
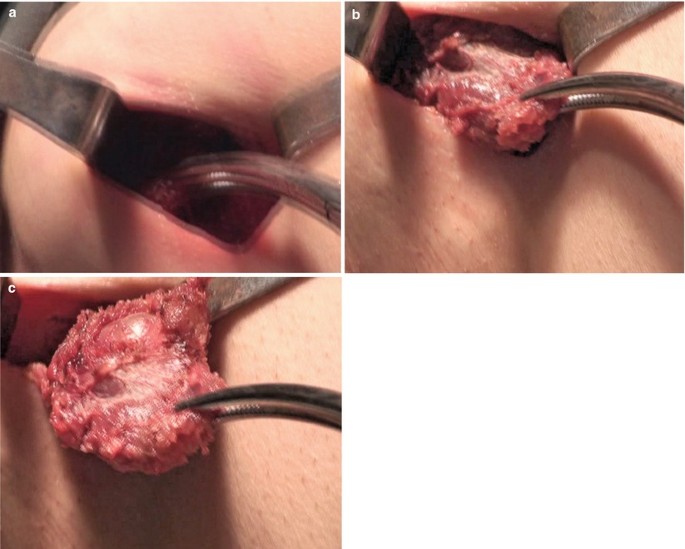
Fig. 10.6
-
6.
Irrigation and suction of working space
After complete hemostasis, the working space was irrigated and cleaned (Fig. 10.7).

Fig. 10.7
-
7.
The placement of drain
A drain was placed and extracted from the incision (Fig. 10.8a, b).

Fig. 10.8








10.7 Tips and Tricks
-
1.
The neck is slightly extended and the lesion-side arm is stretched out at 90°.
-
2.
A 2.5 cm long incision was made parallel to the skin folds on the anterior axillary line of the lesion side and a subcutaneous skin flap from the axilla to the anterior neck area is dissected over the anterior surface of the pectoralis major muscle and clavicle by electrical cautery under direct vision.
-
3.
After exposing the medial border of the sternocleidomastoid muscle, the dissection is approached bluntly through the superficial space of the sternocleidomastoid muscle to reach the surface of the strap muscle above the ipsilateral lobe of the thyroid.
-
4.
The lesion-side thyroid lobe was reached by vertical dissection of the strap muscle.
-
5.
Under endoscopic guidance, the lower pole of the thyroid lobe was drawn upward and medially using the grasper forceps, and inferior thyroid vessels were identified and individually divided.
-
6.
Careful dissection was performed to identify the middle thyroid vein, and individual division was performed by Harmonic scalpel.
-
7.
The upper pole of the thyroid was drawn downward and medially using the forceps, and superior thyroid vessels were identified and individually divided close to the thyroid gland to avoid injuring the external branch of the superior laryngeal nerve using the Harmonic scalpel.
-
8.
Usually, the thyroid tissue near the tracheoesophageal groove should be preserved to prevent injury to the RLN.
10.8 Complications Analysis and Management
-
1.
Recurrent laryngeal nerve injury
In SILS thyroid surgery, because the instruments, light and the tumor that was prepared to be removed were coaxial, the operator’s judgment regarding depth and distance would be affected. Thus, the distal part near to the trachea cannot be seen clearly. So, the recurrent laryngeal nerve may be injured. When the tumor in inferior thyroid is larger than 3 cm, the occurrence of recurrent laryngeal nerve injury may increase. To avoid the recurrent laryngeal nerve injury, the operative point should be close to the tumor surface and keep far away from the para-tracheal groove, when the side of tumor near to trachea is dissected.
-
2.
Purple and broken skin of thorax and neck
Establishing the operational space should be in strict accordance with the operation essentials to dissect the loose connective tissue between platysma and throat muscles. If the dissection is too deep, it may induce anterior superficial jugular bleeding and difficult construction of operative space. On the other hand, if the dissection is too shallow, it may form purple and broken skin of thorax and neck.
-
3.
Subcutaneous fat liquefaction
Subcutaneous fat liquefaction may be induced by situations such as the when the operational space is too shallow, large area of subcutaneous fat is destroyed, and too much tissue is coagulated by ultrasound scalpel. So, appropriate dissecting level and area may prevent this complication effectively
-
4.
Haemorrhage
Thyroid is abundant in blood. Intraoperative haemorrhage is major in thyroid gland and vessels bleeding, which are induced by incorrect use of ultrasound scalpel or large vessels injury. Low gear of ultrasound scalpel is appropriate for coagulating while cutting the thyroid gland. Do not violently tear the thyroid gland. Inferior thyroid gland vessels and middle thyroid vein can be cut off by ultrasound scalpel. But if the vessels are thicker, ligation is better.
References
Huscher CS, Chiodini S, Napolitano C, Recher A, et al. Endoscopic right thyroid lobectomy. Surg Endosc. 1997;11:877.
Miccoli P, Berti P, Conte M, Bendinelli C, Marcocci C. Minimally invasive surgery for thyroid small nodules: preliminary report. J Endocrinol Invest. 1999;22:849–51.
Takami H, Ikeda Y. Minimally invasive thyroidectomy. ANZ J Surg. 2002;72:841–2.
Ikeda Y, T akami H, Sasaki Y, Kan S, Niimi M, et al. Endoscopic neck surgery by the axillary approach. J Am Coll Surg. 2000;191:336–40.
Ohgami M, Ishii S, Arisawa Y, Ohmori T, Noga K, Furukawa T, Kitajima M. Scarless endoscopic thyroidectomy: breast approach for better cosmesis. Surg Laparosc Endosc Percutan Tech. 2000;10:1–4.
Kang SW, Lee SC, Lee SH, Lee KY, Jeong JJ, Lee YS, Nam KH, Chang HS, Chung WY, Park CS. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: the operative outcomes of 338 consecutive patients. Surgery. 2009;146:1048–55.
Kang SW, Jeong JJ, Nam KH, Chang HS, Chung WY, Park CS. Robot-assisted endoscopic thyroidectomy for thyroid malignancy using a gasless transaxillary approach. J Am Coll Surg. 2009;209:e1–7.
Lee J, Yun JH, Choi UJ, Kang SW, Jeong JJ, Chung WY. Robotic versus endoscopic thyroidectomy for thyroid cancers: a multi-institutional analysis of early postoperative outcomes and surgical learning curves. J Oncol. 2012;2012:734541.
Youben F, Bomin G, Bo W, Jie K, Fan Y, Wencai Q, Yuyao H, Qi Z. Trans-areola single-incision endoscopic thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2011;21:192–6.
Lee D, Nam Y, Sung K. Single-incision endoscopic thyroidectomy by the axillary approach. J Laparoendosc Adv Surg Tech A. 2010;20:839–42.
Fan Y, Wu SD, Kong J. Single-port access transaxillary totally endoscopic thyroidectomy: a new approach for minimally invasive thyroid operation. J Laparoendosc Adv Surg Tech A. 2011;21:243–7.
Nakajo A, Arima H, Hirata M, Mizoguchi T, Kijima Y, Mori S, Ishigami S, Ueno S, Yoshinaka H, Natsugoe S. Trans-Oral Video-Assisted Neck Surgery (TOVANS). A new transoral technique of endoscopicthyroidectomy with gasless premandible approach. Surg Endosc. 2013;27:1105–10.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Wu, S., Fan, Y., Tian, Y. (2013). Thyroid Surgery: Single-Port Access Transaxillary Totally Endoscopic Thyroidectomy. In: Wu, S., Fan, Y., Tian, Y. (eds) Atlas of Single-Incision Laparoscopic Operations in General Surgery. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6955-7_10
Download citation
DOI: https://doi.org/10.1007/978-94-007-6955-7_10
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6954-0
Online ISBN: 978-94-007-6955-7
eBook Packages: MedicineMedicine (R0)