
Abstract
The role of the microcirculation is increasingly being recognized in the pathophysiology of cardiovascular disease. It is the major site of control of vascular resistance. In addition, the microcirculation is a major site of damage in most target organs of cardiovascular disease, such as the heart, brain, and kidney. In this chapter, we review the main methods used to assess the microcirculation. These methods include intravital microscopy, video capillaroscopy, Doppler flowmetry, and the use of isolated small arteries. Recently, important advances have been made in retinal microvascular imaging. These methods have led to important new insights in the role of changes in microcirculation both as a cause and a consequence of hypertension. We propose a major role for a defect in angiogenesis as a cause of microvascular rarefaction.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The hemodynamic characteristic of essential and most forms of secondary hypertension consists of elevated blood pressure (BP) and peripheral vascular resistance. BP comprises two components: a pulsatile (pulse pressure) and a steady [mean arterial pressure (MAP)] component. Pulse pressure is predominantly influenced by the elastic properties of the larger conduit arteries, whereas MAP is determined by the resistance to flow in smaller arteries and arterioles, ranging in diameter from 10 to 300 μm. The small arteries and arterioles are a continuous segment of the vascular system associated with a gradual drop in pressure. Instead of referring to specific components as resistance vessels, the entire arterial microcirculation vessels of between 10 and 300 μm should be regarded as a site of resistance, and thus MAP, control. The exact location of the pressure drop may differ in relation to tissue. In cardiac tissue, for example, the pressure drop occurs distally in the arterial tree, whereas in the mesentery it is located more proximally. The role of the microcirculation is increasingly being recognized in the pathophysiology of cardiovascular disease [1, 2]. The microcirculation is a major site of damage in most target organs of cardiovascular disease, such as the heart, brain, and kidney. Both functional and structural alterations in the small arteries, arterioles, and capillaries are the basis of target organ damage (Table 17.1).
Detailed mechanistic studies in both human and animal models of cardiovascular disease have revealed the nature of microcirculatory dysfunction. Large-scale epidemiological studies in the last two decades have identified the associations between deranged microvascular perfusion and structure, target organ damage, and subsequent cardiovascular disease [3]. Major technological developments now allow the study of the microcirculation both in mechanistic and epidemiological studies. The purpose of this brief review is to provide a critical appraisal of these developments and their particular impact on hypertension research.
2 Methods to Assess the Microcirculation
Table 17.2 provides an overview of the major methods used to assess the microcirculation. In Table 17.3, the tissues that can be studied using these methods are summarized, whereas Table 17.4 indicates the major parameters that are used to assess the microcirculation. Intravital microscopy has been used by many groups in experimental models to study microcirculatory (dys)function. It has been the primary technology underlying our present knowledge of microcirculatory function in health and disease. Originally, this technique was used in relatively transparent tissues like the bat wing, hamster cheek pouch, or rat mesentery. Later developments using trans- and epi-illumination have allowed wider access to the microcirculation of other tissues, such as skeletal muscle, the brain, and the heart. The recent introduction of molecular imaging probes now allows detailed analyses of molecular mechanisms in microcirculatory control [4].
The major advantage of intravital microscopy is that it allows direct and precise observation of the microcirculation and its dynamics in vivo. However, access to tissues usually requires surgery and anesthesia, thus limiting its application in human studies. New techniques for video microscopic examinations have been introduced in the past two decades that do not require surgery and anesthesia. These techniques are based on the use of orthogonal polarization spectral (OPS) or sidestream dark-field (SDF) imaging [5–8]. Both devices use the principle that green light illuminates the depth of a tissue and that scattered green light is absorbed by the hemoglobin of the red blood cells contained in superficial vessels [6]. These techniques have been applied in humans for the study of various tissues, but mostly the cutaneous and sublingual microcirculation. Video recordings by handheld cameras now allow microcirculatory observations to be made even in epidemiological studies. The parameters used to assess the microcirculation using OPS and SDF imaging include: total vascular density; arteriolar, venular, and capillary density; and microvascular flow and microvascular diameters. Broekhuizen and colleagues [9] have even used SDF imaging recently to study the behavior of the endothelial glycocalyx in humans. Endothelial glycocalyx perturbation contributes to increased vascular permeability and has been shown to be involved in the vascular complications of type 2 diabetes and perhaps other cardiovascular diseases [9].
3 Capillaroscopy
Until recently, nailfold capillaroscopy, using rather bulky microscopes, was the standard technique to study the microcirculation in hypertensive patients. Capillaroscopy consists of the direct in vivo observation of skin capillaries using a microscope with an epi-illumination system [10]. Nailfold capillaries are parallel to the surface of the skin, which facilitates their observation. Fluorescent tracers such as Na-fluorescein and indocyanine green have been used to improve image contrast and to study the dynamics of the microcirculation in addition to studying transcapillary diffusion. Abnormal patterns have been observed in diseases affecting the digital skin microvasculature, such as systemic sclerosis, but also in diseases like diabetes and hypertension [10, 11]. Skin capillary density has been consistently found to be 10–20 % lower in patients with untreated hypertension, when compared to normotensive controls [12–15]. This defect might be an early feature of hypertensive disease, as it was reported in borderline hypertensive subjects [16] and even in the normotensive offspring of hypertensive parents [17]. He and colleagues [18] recently showed that modest dietary salt reduction can restore capillary density in patients with mild hypertension.
4 Retinal Imaging
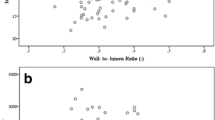
A major advantage in large-scale epidemiological studies on the pathophysiology of hypertension has been the introduction of retinal imaging methods [3, 19, 20]. Hypertensive retinopathy was first described in the nineteenth century and has been used since in the diagnosis of the severity of hypertension-induced target organ damage. However, the classical assessment of retinopathy was descriptive and gave no quantitative and mechanistic data on microcirculatory dysfunction. In the last two decades, several groups have advanced the technology of retinal microcirculatory image analysis with the use of nonmydriatic video cameras [20–22]. In particular, the advances introduced by Knudtson and colleagues [23] have allowed retinal microcirculatory analysis to become part of both mechanistic and epidemiological studies. A further, major technical advance was the introduction of scanning laser Doppler flowmetry, which allows perfusion imaging analysis [24]. This technique also allows the determination of the wall thickness and wall-to-lumen ratio of individual retinal arterioles [25].
Retinal microcirculation undergoes a series of pathophysiological changes during and after the development of hypertension. In the initial, vasoconstrictive stage, there is vasospasm and an increase in retinal arteriolar tone [20]. Persistently elevated BP leads to intimal thickening, hyperplasia of the media wall, and hyaline degeneration in the subsequent sclerotic stage. This stage corresponds to more severe areas of arteriolar narrowing and changes in the arteriolar and venular junctions (arteriovenous nicking/nipping) [20]. In an even later stage, there is disruption of the blood–retina barrier with microaneurysms, hemorrhages, necrosis of the smooth muscle and endothelial cells, and retinal ischemia.
5 Retinal Microcirculation and Cardiovascular Disease
Retinal microcirculatory imaging techniques have substantial reproducibility [26, 27] and can be used repeatedly in the same individuals for follow-up. Such longitudinal studies have shown that signs of hypertensive retinopathy can be observed already in relatively young individuals without a history of hypertension [20]. These data suggest that retinal arteriolar narrowing may precede the development of hypertension [28]. Retinal microcirculatory analysis has been used for the risk stratification of hypertensive patients since it shows a strong association with the risk to develop stroke [29], coronary heart disease [30, 31], and renal complications [32]. An autopsy study of patients with stroke showed a close correlation between retinal and cerebral arteriolar changes [33]. At an even more advanced level, retinal microcirculation imaging allows the analysis of arteriolar and venular branching patterns and retinal vascular fractal dimensions [34]. We have previously suggested that abnormal growth and branching of the vascular tree may represent an early genetic or fetal programming-related characteristic of hypertensive-prone individuals [35].
Retinal arteriolar narrowing is associated with increased aortic [36] and carotid artery [37] stiffness, whereas data from the Hoorn Study [38] did not show an independent association of retinal microvascular abnormalities with indices of large artery endothelial dysfunction and intima-media thickness. Thus, the value of retinal microvascular disease for risk stratification of future cardiovascular events needs to be further investigated [39].
6 Advanced Imaging Technologies
The (video)microscopy techniques discussed previously allow both structural and functional studies of the microcirculation. Over the past two decades, there has been a growing interest in advanced perfusion imaging technologies, such as laser Doppler flowmetry, positron emission tomography (PET), magnetic resonance imaging (MRI), and angiography. Laser Doppler flowmetry is based on the backscattering of a beam of laser light. The light undergoes changes in wavelength when it hits moving cells. The magnitude and frequency distribution of these changes in wavelength are related to the number and velocity of red blood cells [10]. Laser Doppler flowmetry assesses the blood flow of superficial tissue (i.e., skin) over a small volume and is accurate at detecting and quantifying relative changes in skin blood flow in response to a given stimulus [10]. Due to spatial variability, the reproducibility of this technique is relatively poor. The more recently developed two-dimensional laser Doppler perfusion imaging, in which a region of skin is progressively scanned, reduces spatial variability. However, it does not provide an exact linear measure of flow [10]. This makes laser Doppler mostly suited to assess microvascular reactivity instead of absolute measurement of the structure or flow of microvasculature.
PET has been used for more than 35 years as a powerful tool to study cardiac physiology [40]. Apart from studies on metabolism, it allows the assessment of myocardial perfusion in combination with molecular studies. Coronary microvascular function was conventionally assessed by studying flow changes detected by thermodilution or intracoronary Doppler flow wires [40]. The invasive nature of these technologies limits their applicability. PET has become an alternative technique to study microvascular function, although still only used in highly specialized centers. For a detailed review on PET and coronary microvascular function, readers are referred to two recent review papers [40, 41].
MRI has undergone major advances in the past years and is now used to study the structure of arteries in various organs, such as the brain and the heart. However, its resolution is still not high enough to assess the microcirculation. The same is true for angiography on the basis of computed tomography or dyes. Again, most advances are being made in the area of myocardial microvascular studies. The recent progress in MRI and angiography has been reviewed recently [42].
7 Isolated Small Arteries
All of the previously discussed methods used to study the microcirculation share an in vivo approach. Isolated small arteries have been used in the past 20 years successfully to study other aspects of microcirculatory behavior in health and disease. Small arteries have been obtained either from surgical procedures or from specific subcutaneous gluteal biopsies [43–45]. A clear advantage of the in vitro approach has been the possibility for detailed structural analyses of the small arteries both in diseased conditions and during pharmacological treatment of patients. With respect to structural alterations, small arteries remodel in hypertension with two types of remodeling. Inward eutrophic remodeling is usually found in primary forms of hypertension in humans and rats, whereas inward hypertrophic remodeling has been described in secondary hypertension and hypertension associated with diabetes [43–45]. The mechanisms of these forms of remodeling are still poorly understood, but seem to involve growth of both cellular and matrix components of the vessel wall. Low-grade inflammation of the arterial wall, and perhaps perivascular fat, also plays a role in arterial remodeling.
Park and colleagues have proposed that small-artery remodeling may be an early manifestation of target organ damage in hypertension [46]. Small-artery structure has important prognostic significance for later cardiovascular events in both hypertensive and normotensive individuals [44, 47]. Although there are limitations to the in vivo relevance of these isolated artery studies, they provide an excellent approach to the study of the molecular and cellular mechanisms of microvascular changes in hypertension and cardiovascular disease.
8 Microcirculatory Dysfunction: Cause or Consequence of Hypertension?
Microcirculatory dysfunction seems to be both a cause and consequence of elevated BP [2] (Fig. 17.1). Arteriolar and capillary rarefaction and small-artery remodeling are the early hallmarks of hypertension and have been shown to occur already before or early in the onset of primary hypertension in human or animal models [2, 45]. On the other hand, the microcirculation is a primary target of the organ damage caused by an elevated BP. Microvascular damage is now held responsible for much of the pathology related to cardiac, brain, and renal dysfunction in hypertension [48]. The microcirculation is part of a vicious cycle that initiates, maintains, and amplifies high BP if it is not treated adequately [49].

The microcirculation is part of a vicious cycle and is both the cause and consequence of hypertension
The most rigorous way to investigate the behavior of this vicious cycle is to follow the dynamics of the microcirculation throughout life in a population at risk of developing hypertension. Ideally, such a population should be followed up from birth. In animal models like the spontaneously hypertensive rat, such studies have been performed [50], but the most challenging study is, of course, a human one. A beginning of such studies has been made on the basis of retinal imaging and OPS video capillaroscopy. In 6–8-year-old children, those with the higher quartiles of BP had significantly narrower retinal arterioles [51]. Recent studies showed that low-birth-weight children, who are at risk of developing hypertension later in life, have a narrower retinal arteriolar caliber at the ages of 6 and 12 years [52, 53]. Earlier studies had already associated low birth weight with capillary rarefaction in both prepubertal children and in adults [54–57]. Surprisingly, low-birth-weight infants do not have capillary rarefaction at birth [58]. In low-birth-weight infants, capillary density may be even higher because of the relative systemic hypoxia that these infants experienced in utero [56]. Basal capillary density decreases progressively after the first week of life because of a process of pruning. It may be speculated that low-birth-weight infants undergo a process of capillary hyperpruning because of a relative hyperoxia of the extrauterine environment, together with supplemental oxygen in the postnatal period of preterm infants. Alternatively, a catch-up process, with abundant availability of nutrients, may cause capillary hyperpruning [59]. Follow-up studies on the neonatal cohort described by D’Souza and colleagues [58] have to be awaited to decide on this hypothesis.
9 Genetic Determinants of Microcirculatory Phenotypes
The genetic components of hypertensive disease have been the focus of recent, intense research efforts. Apart from several rare forms of monogenic causes, hypertension seems associated with subtle changes in a range of genes. Recent genome-wide association studies indicate that perhaps more than 30 genes can contribute—each to a small degree—to average BP values in a population [60, 61]. Since BP is a highly variable phenotype in an individual, it can be speculated that more robust underlying phenotypes, such as microvascular structure, give better correlations. With respect to the microcirculation, recent studies have focused on the genetic influence on the structure of the retinal microcirculation. There is a strong heritability for retinal arteriolar and venular caliber [62]. Genome-wide association studies have revealed several loci that were significantly associated with retinal arteriolar and venular caliber [62–64]. However, there was no overlap in the specific loci found in the three published genome-wide association studies. This may suggest a lack of power or may indicate regional differences, since the studies were based on populations from different parts of the world. Another approach in genetic studies is the candidate gene approach. Using this approach we recently found that the diameters of the retinal arterioles are associated with the +1675 G/A polymorphism in the angiotensin II receptor, type 2 (AGTR2) gene [65].
10 Conclusions
The microcirculation is both a major site of vascular resistance control and of target organ damage in hypertensive disease. Evidence from animal, clinical, and epidemiological studies has confirmed its essential role in the pathogenesis of hypertension. Major advances in technology now allow the noninvasive study of various aspects of the microcirculation in clinical and even population-based research. Such studies have revealed the major phenotypic microcirculatory changes in hypertension, such as arteriolar narrowing, capillary rarefaction, and altered branching patterns. Future research should focus on the mechanisms underlying these changes in microcirculatory phenotype as well as on how these are influenced by drug treatment.
This chapter is based upon a brief review we published earlier in Hypertension [66].
Funding
This work was performed within the framework of Dutch Top Institute Pharma, project Renin-Angiotensin System Blockade beyond Angiotensin II (T2-301).
Disclosures
None.
References
Levy BI, Schiffrin EL, Mourad JJ et al (2008) Impaired tissue perfusion: a pathology common to hypertension, obesity, and diabetes mellitus. Circulation 118:968–976
Struijker-Boudier HA, Rosei AE, Bruneval P et al (2007) Evaluation of the microcirculation in hypertension and cardiovascular disease. Eur Heart J 28:2834–2840
Strain WD, Adingupu DD, Shore AC (2011) Microcirculation on a large scale: techniques, tactics and relevance of studying the microcirculation in larger population samples. Microcirculation 19:37–46
Fukumura D, Duda DG, Munn LL, Jain RK (2010) Tumor microvasculature and microenvironment: novel insights through intravital imaging in pre-clinical models. Microcirculation 17:206–225
Awan ZA, Wester T, Kvernebo K (2009) Human microvascular imaging: a review of skin and tongue videomicroscopy techniques and analysing variables. Clin Physiol Funct Imaging 30:79–88
De Backer D, Hollenberg S, Boerma C et al (2007) How to evaluate the microcirculation: report of a round table conference. Crit Care 11:R101
Goedhart PT, Khalilzada M, Bezemer R et al (2007) Sidestream dark field (sdf) imaging: a novel stroboscopic led ring-based imaging modality for clinical assessment of the microcirculation. Opt Express 15:15101–15114
Groner W, Winkelman JW, Harris AG et al (1999) Orthogonal polarization spectral imaging: a new method for study of the microcirculation. Nat Med 5:1209–1212
Broekhuizen LN, Lemkes BA, Mooij HL et al (2010) Effect of sulodexide on endothelial glycocalyx and vascular permeability in patients with type 2 diabetes mellitus. Diabetologia 53:2646–2655
Roustit M, Cracowski JL (2011) Non-invasive assessment of skin microvascular function in humans: an insight into methods. Microcirculation 19:47–64
De Boer MP, Meijer RI, Wijnstok NJ et al (2011) Microvascular dysfunction: a potential mechanism in the pathogenesis of obesity-associated insulin resistance and hypertension. Microcirculation 19:5–18
Antonios TF, Singer DR, Markandu ND et al (1999) Structural skin capillary rarefaction in essential hypertension. Hypertension 33:998–1001
Debbabi H, Uzan L, Mourad JJ et al (2006) Increased skin capillary density in treated essential hypertensive patients. Am J Hypertens 19:477–483
Prasad A, Dunnill GS, Mortimer PS, MacGregor GA (1995) Capillary rarefaction in the forearm skin in essential hypertension. J Hypertens 13:265–268
Serne EH, Gans RO, ter Maaten JC et al (2001) Impaired skin capillary recruitment in essential hypertension is caused by both functional and structural capillary rarefaction. Hypertension 38:238–242
Antonios TF, Singer DR, Markandu ND et al (1999) Rarefaction of skin capillaries in borderline essential hypertension suggests an early structural abnormality. Hypertension 34:655–658
Antonios TF, Rattray FM, Singer DR et al (2003) Rarefaction of skin capillaries in normotensive offspring of individuals with essential hypertension. Heart 89:175–178
He FJ, Marciniak M, Markandu ND et al (2010) Effect of modest salt reduction on skin capillary rarefaction in white, black, and asian individuals with mild hypertension. Hypertension 56:253–259
Grassi G, Schmieder RE (2011) The renaissance of the retinal microvascular network assessment in hypertension: new challenges. J Hypertens 29:1289–1291
Wong TY, Mitchell P (2004) Hypertensive retinopathy. N Engl J Med 351:2310–2317
Harazny JM, Ritt M, Baleanu D et al (2007) Increased wall: lumen ratio of retinal arterioles in male patients with a history of a cerebrovascular event. Hypertension 50:623–629
Hughes AD, Martinez-Perez E, Jabbar AS et al (2006) Quantification of topological changes in retinal vascular architecture in essential and malignant hypertension. J Hypertens 24:889–894
Knudtson MD, Lee KE, Hubbard LD et al (2003) Revised formulas for summarizing retinal vessel diameters. Curr Eye Res 27:143–149
Ritt M, Harazny JM, Ott C et al (2008) Analysis of retinal arteriolar structure in never-treated patients with essential hypertension. J Hypertens 26:1427–1434
Harazny JM, Raff U, Welzenbach J et al (2011) New software analyses increase the reliability of measurements of retinal arterioles morphology by scanning laser doppler flowmetry in humans. J Hypertens 29:777–782
Couper DJ, Klein R, Hubbard LD et al (2002) Reliability of retinal photography in the assessment of retinal microvascular characteristics: the atherosclerosis risk in communities study. Am J Ophthalmol 133:78–88
Liu Y-P, Richart T, Jin Y et al (2011) Retinal arteriolar and venular phenotypes in a flemish population: reproducibility and correlates. Artery Res 5:72–79
Ikram MK, Witteman JC, Vingerling JR et al (2006) Retinal vessel diameters and risk of hypertension: the Rotterdam study. Hypertension 47:189–194
Witt N, Wong TY, Hughes AD et al (2006) Abnormalities of retinal microvascular structure and risk of mortality from ischemic heart disease and stroke. Hypertension 47:975–981
Duncan BB, Wong TY, Tyroler HA et al (2002) Hypertensive retinopathy and incident coronary heart disease in high risk men. Br J Ophthalmol 86:1002–1006
Sairenchi T, Iso H, Yamagishi K et al (2011) Mild retinopathy is a risk factor for cardiovascular mortality in japanese with and without hypertension: the ibaraki prefectural health study. Circulation 124:2502–2511
Sabanayagam C, Tai ES, Shankar A et al (2009) Retinal arteriolar narrowing increases the likelihood of chronic kidney disease in hypertension. J Hypertens 27:2209–2217
Goto I, Katsuki S, Ikui H et al (1975) Pathological studies on the intracerebral and retinal arteries in cerebrovascular and noncerebrovascular diseases. Stroke 6:263–269
Cheung CY, Tay WT, Mitchell P et al (2011) Quantitative and qualitative retinal microvascular characteristics and blood pressure. J Hypertens 29:1380–1391
le Noble FA, Stassen FR, Hacking WJ, Struijker Boudier HA (1998) Angiogenesis and hypertension. J Hypertens 16:1563–1572
Cheung N, Sharrett AR, Klein R et al (2007) Aortic distensibility and retinal arteriolar narrowing. The muti-ethnic study of atherosclerosis. Hypertension 50:617–622
Liao D, Wong TY, Klein R et al (2004) Relationship between carotid artery stiffness and retinal arteriolar narrowing in healthy middle-aged persons. Stroke 35:837–842
Van Hecke MN, Dekker JM, Nijpels G et al (2006) Are retinal microvascular abnormalities associated with large artery endothelial dysfunction and intima-media thickness? The Hoorn study. Clin Sci 110:597–604
Cuspidi C, Sala C (2012) Do microvascular retinal changes improve cardiovascular risk estimation? J Hypertens 30:682–684
Al-Mallah MH, Sitek A, Moore SC et al (2010) Assessment of myocardial perfusion and function with pet and pet/ct. J Nucl Cardiol 17:498–513
Camici PG, Crea F (2007) Coronary microvascular dysfunction. N Engl J Med 356:830–840
Porto I, Hamilton-Craig C, Brancati M et al (2010) Angiographic assessment of microvascular perfusion–myocardial blush in clinical practice. Am Heart J 160:1015–1022
Heagerty AM, Heerkens EH, Izzard AS (2010) Small artery structure and function in hypertension. J Cell Mol Med 14:1037–1043
Rizzoni D, Muiesan ML, Porteri E et al (2009) Vascular remodeling, macro- and microvessels: Therapeutic implications. Blood Press 18:242–246
Schiffrin EL (2012) Vascular remodeling in hypertension: mechanisms and treatment. Hypertension 59:367–374
Park JB, Schiffrin EL (2001) Small artery remodeling is the most prevalent (earliest?) form of target organ damage in mild essential hypertension. J Hypertens 19:921–930
Agabiti-Rosei E, Heagerty AM, Rizzoni D (2009) Effects of antihypertensive treatment on small artery remodelling. J Hypertens 27:1107–1114
Safar ME, Struijker-Boudier HA (2010) Cross-talk between macro- and microcirculation. Acta Physiol (Oxf) 198:417–430
Cohuet G, Struijker-Boudier H (2006) Mechanisms of target organ damage caused by hypertension: therapeutic potential. Pharmacol Ther 111:81–98
Struijker Boudier HA, le Noble JL, Messing MW et al (1992) The microcirculation and hypertension. J Hypertens Suppl 10:S147–S156
Mitchell P, Cheung N, de Haseth K et al (2007) Blood pressure and retinal arteriolar narrowing in children. Hypertension 49:1156–1162
Gopinath B, Baur LA, Wang JJ et al (2010) Smaller birth size is associated with narrower retinal arterioles in early adolescence. Microcirculation 17:660–668
Mitchell P, Liew G, Rochtchina E et al (2008) Evidence of arteriolar narrowing in low-birth-weight children. Circulation 118:518–524
Chapman N, Mohamudally A, Cerutti A et al (1997) Retinal vascular network architecture in low-birth-weight men. J Hypertens 15:1449–1453
Ijzerman RG, van Weissenbruch MM, Voordouw JJ et al (2002) The association between birth weight and capillary recruitment is independent of blood pressure and insulin sensitivity: a study in prepubertal children. J Hypertens 20:1957–1963
Sasongko MB, Wong TY, Wang JJ (2010) Retinal arteriolar changes: intermediate pathways linking early life exposures to cardiovascular disease? Microcirculation 17:21–31
Serne EH, Stehouwer CD, ter Maaten JC et al (2000) Birth weight relates to blood pressure and microvascular function in normal subjects. J Hypertens 18:1421–1427
D’Souza R, Raghuraman RP, Nathan P et al (2011) Low birth weight infants do not have capillary rarefaction at birth: implications for early life influence on microcirculation. Hypertension 58:847–851
Hellstrom A, Ley D, Hansen-Pupp I et al (2010) New insights into the development of retinopathy of prematurity–importance of early weight gain. Acta Paediatr 99:502–508
The International Consortium for Blood Pressure Genome Wide Association Studies (2011) Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature 478:103–109
Salvi E, Kutalik Z, Glorioso N et al (2012) Genomewide association study using a high-density single nucleotide polymorphism array and case-control design identifies a novel essential hypertension susceptibility locus in the promoter region of endothelial no synthase. Hypertension 59:248–255
Sun C, Zhu G, Wong TY et al (2009) Quantitative genetic analysis of the retinal vascular caliber: the Australian twins eye study. Hypertension 54:788–795
Ikram MK, Sim X, Jensen RA et al (2010) Four novel loci (19q13, 6q24, 12q24, and 5q14) influence the microcirculation in vivo. PLoS Genet 6:e1001184
Xing C, Klein BE, Klein R et al (2006) Genome-wide linkage study of retinal vessel diameters in the beaver dam eye study. Hypertension 47:797–802
Liu YP, Kuznetsova T, Thijs L et al (2011) Are retinal microvascular phenotypes associated with the 1675 g/a polymorphism in the angiotensin ii type-2 receptor gene? Am J Hypertens 24:1300–1305
Struijker-Boudier HA, Heijnen BF, Liu YP, Staessen JA (2012) Phenotyping the microcirculation. Hypertension 60:523–527
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer-Verlag Italia
About this chapter
Cite this chapter
Struijker-Boudier, H.A.J., Heijnen, B.F. (2012). The Microcirculation and Hypertension. In: Berbari, A., Mancia, G. (eds) Special Issues in Hypertension. Springer, Milano. https://doi.org/10.1007/978-88-470-2601-8_17
Download citation
DOI: https://doi.org/10.1007/978-88-470-2601-8_17
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-2600-1
Online ISBN: 978-88-470-2601-8
eBook Packages: MedicineMedicine (R0)