
Abstract
Lung cancer is the principal cause of cancer death worldwide; overall, 5-year survival of patients even with limited disease and resectable tumor is 35–40 %, making lung cancer one of the most important public health problems. Majority of patients die within 2 years of diagnosis. At the time of diagnosis, frequently, the disease is found to have spread beyond the primary site. Early localized lung cancer is treated with surgery with or without adjuvant chemotherapy; patients with positive ipsilateral mediastinal lymphadenopathy are treated with neoadjuvant chemotherapy followed by surgery, while more advanced cases are treated with palliative chemotherapy with or without radiotherapy.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Lung Cancer
- Carcinoid Tumor
- Recurrent Laryngeal Nerve Palsy
- Solitary Pulmonary Nodule
- Atypical Carcinoid
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Lung cancer is the principal cause of cancer death worldwide; overall, 5-year survival of patients even with limited disease and resectable tumor is 35–40 %, making lung cancer one of the most important public health problems. Majority of patients die within 2 years of diagnosis. At the time of diagnosis, frequently, the disease is found to have spread beyond the primary site. Early localized lung cancer is treated with surgery with or without adjuvant chemotherapy; patients with positive ipsilateral mediastinal lymphadenopathy are treated with neoadjuvant chemotherapy followed by surgery, while more advanced cases are treated with palliative chemotherapy with or without radiotherapy.
Clinical Problems
Tumor Diagnosis in Solitary Pulmonary Nodule (SPN)
Morphological images can detect a nodule or mass but cannot determine its benign or malignant nature in a conclusive fashion. Nonspecificity of anatomic imaging management depends upon invasive diagnostic procedures, which are associated with complications and have morbidity of 1–10 % depending on technique, the patient’s medical status, and experience of the operator.
Pretreatment Staging in a Diagnosed Case of Lung Carcinoma
Defining the extent of disease, both locoregional and at distant sites, is key to choosing the appropriate therapeutic option. Anatomical imaging demonstrates substantial discordance in the tumor stage as determined preoperatively with conventional techniques and at surgery. Hence, FDG PET/CT has been investigated for the sensitive detection of tumor extent and disease spread to reduce futile surgery, without sacrificing specificity of diagnosis (Figs. 12.1, 12.2, 12.3, 12.4, and 12.5).

Case record: A 55-year-old male biopsy-proven adenocarcinoma, diagnosed of left upper lobe mass with no locoregional lymph nodes by conventional contrast-enhanced CT scan, sent for whole-body PET–CT scan for staging. PET–CT revealed FDG-avid large cavitating pulmonary mass with irregular speculated margins in the upper lobe of the right lung, measuring 7.1 × 6.8 × 6.8 cm (SUVmax 12.5 g/ml). FDG-avid multiple subcentimeter bilateral hilar, right peribronchial, and subcarinal nodes (SUVmax 4.8 g/ml)

Case record: A 55-year-old male biopsy-proven adenocarcinoma, diagnosed of well-defined soft tissue mass lesion 11.9 × 5.9 cm in the left lobe extending from the apex to the mediastinum abutting the adjoining mediastinum with no locoregional nodes by conventional contrast-enhanced CT scan, sent for whole-body PET–CT scan for staging. PET–CT lung window revealed marked heterogeneous FDG uptake in the large pulmonary mass involving almost the entire left lung (SUVmax 7.93 g/ml) with evidence of areas of necrosis, abutting the adjoining mediastinum arch of aorta with left hilar, subcarinal nodes (SUVmax 6.5 g/ml) and multiple thoracodorsal vertebrae, multiple ribs, right scapula (SUVmax 5.36 g/ml), right ischium, and sacrum with lytic component

Case record: A 50-year-old male presented with change in voice and left-sided chest pain; chest X-ray revealed a large mass in the upper and middle lobe of the left lung, thus was referred for PET–CT scan for staging, which revealed FDG-avid large cavitating pulmonary mass with irregular margins in the upper and middle lobe of the left lung, measuring 9.1 × 7.8 × 8.8 cm, SUV max 16.54 g/ml. FDG-avid multiple lytic and sclerotic skeletal metastases involving the skull, D3, D9, L2 vertebrae, right acetabulum, and sacrum (SUVmax 9.84 g/ml). Diffuse FDG uptake was noted in both lobes of the thyroid gland consistent with thyroiditis. No FDG uptake was noted in the left vocal cord as a result of left recurrent laryngeal nerve palsy from a left lung tumor, whereas benign intense FDG uptake was noted in the right vocal cord secondary to the compensatory hypertrophy

Case record: A 65-year-old female presented with dry cough and breathlessness, diagnosed by CT chest as harboring dense pulmonary soft tissue of size approximately 3.5 × 2.5 cm in the left lower lobe and a single 1.7 × 1.6 cm left paraesophageal lymph node. FDG PET–CT revealed heterogeneous FDG concentrating lesion noted in the lower lobe of the left lung with area of central necrosis (SUVmax 9.59)



(a–c) Case record: A 69-year-old male patient of biopsy-proven adenocarcinoma of the left lung. CT chest revealed mildly enhancing soft tissue mass with speculated margins (4.6 × 3.4 cm) involving perihilar region of anterior segment of the left upper lobe and left hilum abutting the mediastinum medially and pushing the left pulmonary artery, partial obliteration of the left upper lobe anterior segment bronchus and partial volume loss. Staging PET–CT (a–c) revealed FDG-avid soft tissue mass with spiculated margins (4.6 × 3.4 cm) involving perihilar region of anterior segment of the left upper lobe and left hilum (SUVmax 11.14). Low-grade FDG-avid subcentimeter parenchymal nodule along the fissure in the left lung upper lobe (SUVmax 3.88), and subpleural nodule in the left lung upper lobe (SUVmax 3.36) is seen; FDG uptake noted in the multiple foci in the left pleura, FDG-avid lytic lesion in the right ilium (SUVmax 6.61). FDG uptake in the right lobe of thyroid gland was also observed
Message
FDG PET/CT when compared to the baseline diagnostic contrast-enhanced CT scan revealed contralateral hilar nodes, which changed the staging from operable to inoperable.
Message
PET–CT when compared to the baseline diagnostic contrast-enhanced CT scan upstaged the patient to stage IV and revealed additional hypermetabolic left hilar and subcarinal nodes and multiple bone metastases. CECT chest was unable to detect the metastases to the right scapula, multiple ribs, and dorsal vertebrae.
Message
PET–CT-based disease upstaging is further demonstrated in this case, where disease is upstaged to stage IV. The asymmetry of FDG uptake in the vocal cord is also noteworthy, an indirect feature of recurrent laryngeal nerve palsy secondary to involvement.
Message
FDG PET/CT-based disease characterization of tumor heterogeneity is an area of major interest in recent times, which can highlight tumor biology with various novel tracers too. This has implications for selecting patients for appropriate treatment options.
Message
This case highlights that PET–CT can clearly demarcate pleural involvement and the single lytic skeletal lesion that upstaged the disease. PET–CT aided in evaluating the abnormal FDG uptake in the right lobe of the thyroid gland, in which poorly differentiated thyroid carcinoma (synchronous second primary) with papillary thyroid carcinoma background which was proven by biopsy.
Assessment of Treatment Efficacy
Posttreatment detection of residual or recurrent tumor is an important clinical question, where functional imaging with FDG-PET has potential advantages (Fig. 12.6). Structural changes produced by radiotherapy and/or surgery further reduce the accuracy of anatomical imaging modalities.


(a, b) Case record: a 52-year-old male patient, biopsy-proven poorly differentiated squamous cell carcinoma, stage IIIb at presentation. Baseline CECT revealed heterogeneously enhancing spiculated mass lesion in the anterior segment of the right upper lobe causing cutoff of the upper lobe bronchus with areas of consolidation and volume loss (T2N2M0); patient received neoadjuvant chemotherapy and 3DCRT 60 Gy/30 # in 45 days with 5 # of weekly cisplatin and was referred for residual disease evaluation after 6 weeks of completion of EBRT. FDG PET/CT scan (a, b) revealed FDG-avid residual disease in the right upper lobe in the paratracheal region with central photopenia (SUVmax 4.36) with CT evidence of patchy fibrosis surrounding the lesion. FDG-avid residual right tracheobronchial, pretracheal, subcarinal, and left hilar nodes are evident (b)
Identification of metabolic abnormalities of lung cancer was the first non-CNS oncologic application of FDG-PET to be reported. Differentiating malignant from nonmalignant nodules was the first oncologic indication for FDG-PET to be established, leading the way for later advances in staging, therapy assessment, and follow-up, so the use of PET is now generally accepted for the management of lung cancer.
The most common staging system used is the TNM (tumor, node, metastases); this will be familiar to most readers.
Case Record
A 52-year-old male patient, biopsy-proven poorly differentiated squamous cell carcinoma, stage IIIb at presentation. Baseline CECT revealed heterogeneously enhancing spiculated mass lesion in the anterior segment of the right upper lobe causing cutoff of the upper lobe bronchus with areas of consolidation and volume loss (T2N2M0); patient received neoadjuvant chemotherapy and 3DCRT 60 Gy/30 # in 45 days with 5 # of weekly cisplatin and was referred for residual disease evaluation after 6 weeks of completion of EBRT. FDG PET/CT scan (Fig. 12.6a, b) revealed FDG-avid residual disease in the right upper lobe in paratracheal region with central photopenia (SUVmax 4.36) with CT evidence of patchy fibrosis surrounding the lesion. FDG-avid residual right tracheobronchial, pretracheal, subcarinal, and left hilar nodes are evident (Fig. 12.6b).
Message
This case highlights the role of FDG PET/CT in the evaluation of posttreatment residual disease assessment when CECT is inconclusive.
Classification and Evaluation of Lung Cancer
Histological Classification of Non-small-Cell Lung Cancers
The new World Health Organization/International Association for the Study of Lung Cancer histologic classification of non-small-cell lung cancers.
-
1.
Squamous cell carcinoma
-
Papillary
-
Clear cell
-
Small cell
-
Basaloid
-
-
2.
Adenocarcinoma
-
Acinar
-
Papillary
-
Bronchioloalveolar carcinoma
-
Non-mucinous
-
Mucinous
-
Mixed mucinous and non-mucinous or indeterminate cell type
-
Solid adenocarcinoma with mucin
-
Adenocarcinoma with mixed subtypes variants
-
Well-differentiated fetal adenocarcinoma
-
Mucinous (“colloid”) adenocarcinoma
-
Mucinous cystadenocarcinoma
-
Signet ring adenocarcinoma
-
Clear cell adenocarcinoma
-
-
3.
Large cell carcinoma variants
-
Large cell neuroendocrine carcinoma
-
Combined large cell neuroendocrine carcinoma
-
Basaloid carcinoma
-
Lymphoepithelioma-like carcinoma
-
Clear cell carcinoma
-
Large cell carcinoma with rhabdoid phenotype
-
-
4.
Adenosquamous carcinoma
-
5.
Carcinomas with pleomorphic, sarcomatoid, or sarcomatous elements
-
Carcinomas with spindle and/or giant cells
-
Spindle cell carcinoma
-
Giant cell carcinoma
-
Carcinosarcoma
-
Pulmonary blastoma
-
-
6.
Carcinoid tumor
-
Typical carcinoid
-
Atypical carcinoid
-
-
7.
Carcinomas of salivary gland type
-
Mucoepidermoid carcinoma
-
Adenoid cystic carcinoma
-
Others
-
-
8.
Unclassified carcinoma
TNM Classification and Stage Grouping
Primary tumor (T) | |
TX | Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging or bronchoscopy |
T0 | No evidence of primary tumor |
Tis | Carcinoma in situ |
T1 | Tumor 3 cm or less in greatest dimension, surrounded by lung or visceral pleura, without bronchoscophic evidence of invasion more proximal than the lobar bronchusa, (i.e., not in the main bronchus) |
T2 Tumor with any of the following features of size or extent | |
More than 3 cm in greatest dimension | |
Involves main bronchus, 2 cm or more distal to the carina | |
Invades the visceral pleura | |
Associated with atelectasis or obstructive pneumonitis that extends to the hilar region but does not involve the entire lung | |
T3 Tumor of any size that directly invades any of the following | |
Chest wall (including superior sulcus tumors), diaphragm, mediastinal pleura, parietal pericardium; or tumor in the main bronchus less than 2 cm distal to the carina, but without involvement of the carina; or associated atelectasis or obstructive pneumonitis of the entire lung | |
T4 Tumor of any size that invades any of the following | |
Mediastinum, heart, great vessels, trachea, esophagus, vertebral body, carina; or separate tumor nodules in the same lobe; or tumor with malignant pleural effusionb | |
Regional lymph nodes (N) | |
NX | Regional lymph nodes cannot be assessed |
N0 | No regional lymph node metastasis |
N1 | Metastasis to ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension of the primary tumor |
N2 | Metastasis to ipsilateral mediastinal and/or subcarinal lymph nodes(s) |
N3 | Metastasis to contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph nodes(s) |
Distant metastasis (M) | |
MX | Distant metastasis cannot be assessed |
M0 | No distant metastasis |
M1 | Distant metastasis present |
Stage Grouping
Occult carcinoma TX N0 M0 | |
Stage 0 | Tis N0 M0 |
Stage IA | T1 N0 M0 |
Stage IB | T2 N0 M0 |
Stage IIA | T1 N1 M0 |
Stage IIB | T2 N1 M0 |
T3 N0 M0 | |
Stage IIIA | T1 N2 M0 |
T2 N2 M0 | |
T3 N1 M0 | |
T3 N2 M0 | |
Stage IIIB | Any T N3 M0 |
T4 Any N M0 | |
Stage IV | Any T any N M1 |
Conventional Staging
Conventional staging of lung cancer usually involves contrast-enhanced computed tomography (CECT) scan of the thorax and upper abdomen, a radionuclide bone scan, and a magnetic resonance imaging (MRI) scan of the brain.
Patterns of FDG Uptake in Lung Cancer
In general, lung cancer is very FDG avid.
Two lung tumors, pulmonary carcinoid and bronchioloalveolar cell cancer, are well known to be less FDG avid and are frequently listed as causes of false-negatives on FDG-PET.
Although it is important to remember that these tumors may be a cause of false-negative scans, many of them are positive on FDG-PET.
Bronchioloalveolar cell lung cancers with a prominent solid component on CT are more likely to be FDG avid.
Atypical carcinoid tumors are more likely to be FDG avid than typical carcinoid tumors. Thus, FDG uptake should not be used to exclude either of these tumors.
The FDG avidity of lung cancer is a valuable prognostic factor: the more FDG avid the cancer, the worse the prognosis.
A recent study showed that FDG uptake correlated with tumor proliferation as measured by Ki-67 immunostaining in lung cancers. Comparison of FDG uptake with F-18-fluorothymidine (FLT) showed that FDG had higher mean uptake as measured by SUV, while the FLT had a better correlation with tumor proliferation. Studies of FLT as a prognostic indicator have not yet been done. These two PET tracers may provide different insight into cancer metabolism.
Potential Role of PET–CT in Lung Cancer
-
Assessment of the solitary pulmonary nodule (SPN)
-
Staging of non-small-cell lung cancer (NSCLC)
-
Assessment of mediastinal lymphadenopathy
-
Identification of distant metastatic disease
-
Detection of recurrent disease
-
Radiotherapy planning
-
Response to therapy assessment
-
As a prognostic indicator
-
Possible role in staging small-cell lung cancer
-
Detecting lung carcinoma as the unknown primary with metastatic presentations (Figs. 12.7a, b and 12.8) with simultaneous disease staging
Fig. 12.7 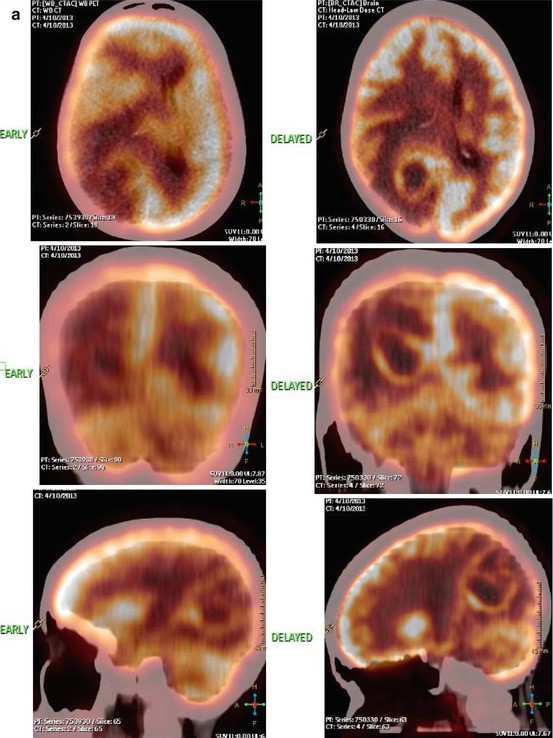

(a, b) Case record: a 49-year-old female diagnosed of multiple ring-enhancing lesions with irregular margins and varying sizes at the gray-white junction in the supratentorial parenchyma and the left cerebellum suggesting multiple brain metastases was referred for a whole-body PET/CT scan (a, b) to search for unknown primary tumor. PET/CT revealed an intense and homogenous FDG uptake in the large well-defined mass in the upper lobe of the left lung abutting the arch of aorta with no definite infiltration, measuring 2.9 × 2.7 × 4.5 cm (SUVmax 10.82 g/ml). FDG-avid multiple nodes noted in the ipsilateral mediastinum involving the prevascular (largest measuring 1.6 cm, SUVmax 4.77 g/ml), aortopulmonary window, and subcarinal and left hilar region. Multiple FDG-avid skeletal metastases were noted in the distal end of the right clavicle, manubrium sternum, proximal ends of the left humerus, and the right femur. The known brain metastases were not appreciable in the early scan (postinjection one hour), which were well delineated in the dedicated delayed brain image (a)
Fig. 12.8 
Case record: a 50-year-old male patient, biopsy-proven poorly differentiated adenocarcinoma from the abdominal nodes; baseline CECT revealed soft tissue density in the right lower lobe-medial basal segment of size 2.5 × 2.1 × 1.6 cm. USG abdomen revealed portal, peripancreatic, and paraaortic nodes. Staging FDG PET/CT revealed FDG-avid soft tissue mass, measuring 2.0 × 1.5 cm in the lower lobe of the right lung (SUVmax 7.74) and FDG-avid left supraclavicular, pretracheal, subcarinal, and right hilar node( SUVmax 8.88). FDG-avid conglomerulated nodal mass in the multiple peripancreatic, preaortic, and paraaortic nodes (SUVmax 13.0). FDG-avid single right lobe of liver (SUVmax 7.43)



Case Record
The 49-year-old female diagnosed of multiple ring-enhancing lesions with irregular margins and varying sizes at the gray-white junction in the supratentorial parenchyma and the left cerebellum suggesting multiple brain metastases was referred for a whole-body PET–CT scan (Fig. 12.7a, b) to search for unknown primary tumor. PET–CT revealed an intense and homogenous FDG uptake in the large well-defined mass in the upper lobe of the left lung abutting the arch of aorta with no definite infiltration, measuring 2.9 × 2.7 × 4.5 cm (SUVmax 10.82 g/ml). FDG-avid multiple nodes noted in the ipsilateral mediastinum involving the prevascular (largest measuring 1.6 cm, SUVmax 4.77 g/ml), aortopulmonary window, and subcarinal and left hilar region. Multiple FDG-avid skeletal metastases were noted in the distal end of the right clavicle, manubrium sternum, proximal ends of the left humerus, and the right femur. The known brain metastases were not appreciable in the early scan (postinjection 1 h), which were well delineated in the dedicated delayed brain image (Fig. 12.7a).
Message
FDG PET/CT can serve as a one-stop shop for detecting the site of primary in patients with brain metastases; most frequently, they are encountered in the lungs. A whole-body FDG PET/CT would also provide disease staging in the same go in such a patient. The scan highlights the importance of delayed brain imaging in FDG-PET to identify and clearly delineate brain metastases.
Case Record
A 50-year-old male patient, biopsy-proven poorly differentiated adenocarcinoma from the abdominal nodes; baseline CECT revealed soft tissue density in the right lower lobe-medial basal segment of size 2.5 × 2.1 × 1.6 cm. USG abdomen revealed portal, peripancreatic, paraaortic nodes. Staging FDG PET/CT (Fig. 12.8) revealed FDG-avid soft tissue mass, measuring 2.0 × 1.5 cm in the lower lobe of the right lung (SUVmax 7.74), and FDG-avid left supraclavicular, pretracheal, subcarinal, and right hilar node, (SUVmax 8.88). FDG-avid conglomerulated nodal mass in the multiple peripancreatic, preaortic, and paraaortic nodes (SUVmax 13.0). FDG-avid single right lobe of liver (SUVmax 7.43).
Message
This is another example of the role of FDG PET/CT in detecting and delineating the primary lesion in a patient with presentation of abdominal nodes from unknown primary and also to do a whole-body disease assessment in a single go.
Assessment of the Solitary Pulmonary Nodule (SPN)
Solitary pulmonary nodule (SPN) is defined as a single spherical lesion of 3 cm or less in diameter completely surrounded by lung parenchyma without any associated atelectasis or lymphadenopathy.
Imaging characteristics favoring benign or malignant nature of the nodule has important implications for patient management.
Findings Favoring a Benign Lesion
Conventional Imaging with chest X-Ray or CT Scan
-
Size less than 2 cm.
-
Stable appearance (since 2 years).
-
Smooth margin.
-
Diffuse calcification (“popcorn” calcification) is typical of hamartomas, and central calcification is typical of granulomas.
-
If cavitation is present, smooth, thin walls (4 mm or less) favor benign.
-
Satellite nodules seen at the periphery of a dominant smooth nodule suggest infectious granuloma.
-
Nodule enhancement <15 HU.
Imaging with FDG-PET
-
SUVmax <2.5 or visually less metabolically active than mediastinal blood pool (for nodules >1 cm), though considerable overlap exists
Findings Favoring a Malignant Lesion
Conventional Imaging with chest X-Ray or CT Scan
-
Size greater than 3 cm.
-
Interval change, that is, increase in size.
-
Spiculated, irregular, or lobulated margin.
-
Stippled or eccentric calcification.
-
Cavitation with irregular thick walls (>15 mm) favors malignancy.
-
Malignant lesions are relatively hypervascular.
Imaging with FDG-PET
-
SUVmax >2.5 or visually more metabolically active than mediastinal blood pool (for nodules >1 cm)
False-Positive SPN
-
Granulomatous conditions
-
Sarcoidosis
-
Inflammation
-
Infection
-
Adenomas
-
Hamartomas
-
Neurofibromas
-
Pulmonary fibrosis
False-Negative SPN
-
Bronchoalveolar cancer
-
Scar adenocarinoma
-
Carcinoid tumors
-
Neuroendocrine tumors
-
Lesions that are too small (<1 cm)
-
Well-differentiated lesions
PET scanning has a sensitivity of 91–97 % and a specificity of 78–88 % for predicting the pathologic nature of SPN.
Integrated PET–CT permits anatomic definition to be added to help resolve metabolic ambiguity. The improved localization with PET–CT also allows radiologists and nuclear physicians to differentiate areas of normal physiological uptake from abnormal areas of increased uptake. Integrated FDG PET/CT has been found to be more useful in characterizing SPN with better sensitivity, specificity, and accuracy. Semiquantitative analysis of glucose metabolism (SUVmax) is also frequently performed, in addition to visual assessment, because of observer independence and reproducibility.
Competing Methods for Evaluating a Single Pulmonary Nodule
A histological sample may be obtained from the nodule by transthoracic needle aspiration, by bronchoscopy with direct biopsy, transbronchial needle aspiration (TBNA), or bronchoalveolar lavage (BAL) or by surgical excision.
Advantage of All of These Methods
They provide histological samples.
A peripheral lesion, which is adherent to the chest wall, is ideal for transthoracic biopsy.
An endobronchial lesion is ideal for bronchoscopy.
A highly suspicious peripheral lesion, which is to be resected regardless of the findings on FDG, considered primarily for resection.
Disadvantages of These Methods
There is moderate morbidity from each of the aforementioned procedures. Transthoracic needle aspiration is associated with pneumothorax, hemoptysis, and rarely air embolism. Methods using bronchoscopy are associated with hemoptysis, infection, and pneumothorax.
Biopsy methods also suffer from sampling error.
The complications associated with surgical excision depend on the method—video-assisted thoroscopic surgery (VATS) or thoracotomy. Depending upon the exact location of the lesion, a biopsy may be more or less dangerous. However, the advantage of all of these methods is that they provide a histological sample.
Comparison with Conventional Imaging
In a large fraction of cases, FDG PET/CT will be the method of choice for characterizing a single pulmonary nodule and follow-up CT to assure 2-year stability in size. If there are other smaller nodule(s), then it is important to follow-up these nodules.
Staging of Non-small-Cell Lung Cancer (NSCLC)
T Staging
CT is a satisfactory method for the assessment of the size and location of a primary pulmonary lesion, but it is less successful in the characterization of mediastinal nodes. For the assessment of T stage, the combined PET–CT has increased the accuracy of tumor detection, chest wall, and mediastinal infiltration as compared to PEt alone. One potential advantage of PET over conventional imaging is the evaluation of extension of the primary tumor to involve the pleura with a high positive and negative predictive value for the evaluation of malignant pleural effusions. Also, FDG-PET is more accurate than CT in determining the size of primary tumor (T1 and T2) when there is adjacent collapse or consolidation.
N Staging
Conventional imaging modalities (CT/MRI), using only dimensional criteria (>1 cm) to detect nodal involvement, have poor accuracy in differentiating benign from malignant nodal disease (sensitivity, 60–83 %; specificity, 77–82 %). The standard radiological practice is that the mediastinal nodes greater than 1 cm in diameter are considered abnormal and, therefore, more likely to represent metastatic disease. Small nodes may contain malignant cells and large nodes are often only reactive in nature; CT can therefore under- or overstage up to 40 % of cases (Fig. 12.1); thus, the accuracy of such a system is only approximately 60–79 %. Studies have shown that up to 75 % of metastatic nodes were within nodes considered to be of normal size. FDG PET/CT is reported to have a higher diagnostic accuracy than either CT or PEt alone for the N staging. A recent multicenter study has shown that FDG PET/CT has very high negative predictive value (91 %) and specificity (83 %), but limited positive predictive value (29 %).
The use of mediastinoscopy is reserved for those patients considered suitable for surgery by CT staging but who have enlarged mediastinal nodes that require evaluation. The procedure has its risks and may have a false-negative rate of up to 10 %.
Transbronchial needle biopsy can have a very high specificity; it has a poor sensitivity of not much more than 50 % and in turn can have a significant morbidity. Many studies concluded that nodal size is a poor determinant of metastatic involvement. A recent study examined lymph nodes of all sizes, in known lung cancer patients, and found that in those nodes with metastatic deposits, the nodal size was “normal” in 74 %. However, PET findings cannot replace histological confirmation of FDG-positive lesions by mediastinoscopy. FDG PET/CT cannot obviate the need for invasive procedures. PET–CT virtual mediastinoscopy has also been found to be a useful adjunct.
Teaching Point
-
Without the aid of PET–CT, it can be difficult to distinguish active tumor from collapsed lung or necrotic tissue.
-
The conventional staging of nodes by size criteria alone can often lead to the wrong conclusion. Metabolic imaging stages mediastinal nodes with much greater accuracy than CT alone. The highest diagnostic accuracy has been with combined PET–CT with a generally accepted figure of approximately 90 % for mediastinal nodal involvement.
-
PET has consistently been shown to be accurate in the distinction between N2 (operable) and N3 (inoperable) nodal disease.
-
Not only is PET–CT superior than other noninvasive methods for mediastinal staging, it also has the advantage that whole-body images are obtainable, and therefore, an assessment can be made of potential distant metastatic disease.
-
PET–CT has a higher accuracy for mediastinal nodal involvement compared to PET scan alone.
M Staging
Detection of a distant site of disease means the patient is stage IV and palliative chemotherapy is indicated. The common sites of metastases from NSCLC are to the adrenal glands, liver, bone, and brain.
Adrenal
PET and PET–CT are accurate in the assessment of metastatic disease to the adrenal glands. Evidence suggests that the removal of a solitary adrenal deposit at the time of resection of the lung primary results in an increased life expectancy.
Liver
FDG-PET appears more accurate than CT in detecting liver metastases because of its better specificity.
Bone
Lytic osseous metastases appear to have a greater uptake of FDG and as such are more readily detected (Fig. 12.2). PET–CT is both more sensitive and specific than bone scanning in lesion detection in lung cancer. Metastatic lesions start in marrow and FDG is positive much before bone scan becomes positive. In a recent meta-analysis, it was shown that the pooled sensitivity and specificity for the detection of bone metastasis in lung cancer using FDG PET/CT, FDG-PET, MRI, and bone scan were 92, 87, 77, and 86 %; and 98, 94, 92, and 88 %, respectively.
Brain
FDG-PET due to high physiological brain parenchymal uptake has its limitation in the detection of brain metastases. MRI brain is thus mandatory in the staging of lung cancer to rule out brain metastases.
Comparison with conventional imaging: Liver, adrenal, brain, and bony deposits are common with lung cancer, but many of the lesions are undetected in the course of conventional staging.
Anatomic imaging is often important in helping make important distinctions about issues such as invasion of structures, but FDG-PEt also has an important role.
Accurate staging is very important since it has such a major impact on both therapy and prognosis.
A meta-analysis of studies comparing FDG-PET and CT evaluation of mediastinal lymph nodes showed that FDG-PET had a sensitivity of 85 % and a specificity of 90 %, whereas CT had a sensitivity of 61 % and a specificity of 79 %. FDG-PET was more sensitive but less specific in enlarged lymph nodes (sensitivity of 100 %, specificity of 78 %) than in normal-sized nodes (sensitivity of 82 %, specificity of 93 %).
Integrated PET–CT improves the diagnostic accuracy of the staging of non-small-cell lung cancer.
Radiation Treatment Planning
FDG-PET may have an important role in radiation treatment planning in lung cancer.
In addition to determining if radiation therapy is appropriate and whether therapy will be given with curative or palliative intent, FDG-PET is useful for determining therapy ports. It can be used both to limit ports to spare normal tissue and to include additional involved regions. Treatment plans that include all the FDG-avid lesions or the FDG-avid portions of a complex mass will result in more effective local control with less unnecessary tissue being treated. PET–CT should be used for RT planning in NSCLC because it more accurately images tumor extent than CT alone. PET–CT imaging can improve the accuracy of target volume delineation using anatomic biological contour (ABC) and determined directly on PET–CT images. PET–CT imaging has another positive effect on tumor volume delineation: Significantly reduced interobserver and intraobserver variability for tumor volume delineation.
Recurrent Laryngeal Nerve Palsy
The recurrent laryngeal nerves, especially the left recurrent laryngeal nerve, may be involved with lung cancer, causing recurrent laryngeal nerve palsy. In this case, the involved vocal cord does not function. The non-involved vocal cord must work harder than normal in order to make up for the loss in function of the involved vocal cord.
Consequently, the ipsilateral vocal cord will not show any FDG uptake, and the contralateral vocal cord will show increase uptake, which can be quite intense (Fig. 12.3).
Unilateral FDG uptake in the vocal cord region, especially with an appropriately placed mass, can be used to suggest the diagnosis of recurrent laryngeal nerve palsy. It should not be misinterpreted as spread of disease.
Monitoring Response to Therapy
FDG-PET is playing an increasing role in monitoring therapy for lung cancer.
A decrease in FDG uptake after therapy is very encouraging, although with lung cancer, one often has to settle for stable findings. One of the major theoretical advantages of FDG-PET compared with structural imaging techniques is that there is usually a more rapid change in cellular metabolism than in tumor size (Fig. 12.6).
A new region of uptake indicates that therapy is not effective or no longer effective. The level of FDG uptake as measured by the SUV is a prognostic factor both before and during therapy.
Remember that when comparing quantitative measures on sequential studies, the details of the analysis become even more important. Quantitative measurement should be made at the same time after injection, and when monitoring therapy with FDG-PET, it is important to recognize the confounding effects of radiation therapy. In the area of radiation change, there is typically low-level FDG uptake. Occasionally, there can be avid FDG uptake, especially when there is frank radiation pneumonitis. The FDG uptake often returns to normal after 6 months, but radiation change may persist for a longer period of time. There can be increased uptake in both the lung and the chest wall after radiation therapy. A local region with the radiation port with more marked FDG uptake, or a region with increasing uptake, especially if it is associated with a mass on anatomic imaging, should be considered suspicious for recurrence. Mild to moderate uptake in a region corresponding to typical radiation changes does not suggest recurrence. FDG PET/CT has been shown to be useful in monitoring response to the EGFR kinase inhibitor erlotinib in few studies.
Prognosis
The primary purpose of staging is to identify patients who may benefit from different therapies.
Staging is also a potent prognostic indicator. The 5-year survival for patients with non-small-cell lung cancer is 61 % if they have stage I disease and only 5 % if they have stage IIIB disease. Since FDG imaging allows for more accurate staging, it should make TNM staging an even more accurate predictor of prognosis.
In addition to staging, the FDG avidity of the tumor is an independent prognostic factor. It has been shown that FDG uptake correlates with tumor growth rate and FDG uptake correlates with Ki-67 immunostaining, a marker of tumor proliferation. It has been found that patients with an SUV greater than or equal to 7 had 6.3 times the 5-year mortality of those with an SUV less than 7. In a larger prospective study, a metabolic response to chemoradiation, as assessed by visual analysis of FDG-PET, was also much more powerfully correlated with survival than the response on CT determined from WHO criteria.
Most of the information about prognosis has dealt with non-small-cell lung cancer. But SUV may also provide prognostic information in small-cell lung cancer.
Detection of Recurrent Disease
PET–CT scan should not be carried out in less than 3 months after the therapy to allow any metabolically active macrophage activity within inflammatory lung to resolve preventing a false-positive report.
At least 3 months is suggested to allow postoperative change to improve.
FDG uptake correlates with the tumor growth and proliferation rates as well as the degree of tumor differentiation.
PET–CT in Therapy Response and Radiotherapy Planning
FDG uptake relates well to tumor growth and proliferation rates, thus, allows us to quantify the metabolic response of therapy within the tumor.
Results as early as 1 week after initiation of chemotherapy accurately reflect response, but imaging 6 weeks after chemotherapy has finished and at least 3 months after radiotherapy is generally regarded as more accurate. This helps avoid the problems with false-positive reports due to radiation-induced pneumonitis.
Tumors with higher pretherapy FDG uptake respond better to radiotherapy than those with low uptake, and additionally, persisting uptake after therapy is predictive of relapse.
Comparison with Conventional Imaging
PET–CT has been shown to be better than CT at assessing accurate tumor volume.
PET–CT is excellent at delineating tumor from distal atelectasis.
Small-Cell Lung Cancer and Mesothelioma
Diagnosis of small-cell lung cancer equates to a diagnosis of disseminated disease. This, however, is not always the case.
Principle role of staging in small-cell lung cancer is to determine if localized radiotherapy can be used in addition to chemotherapy.
The role of PET–CT in this instance is still under evaluation, but evidence suggests PET can be used to accurately upstage presumed limited disease and has been shown to be useful in the detection of paraneoplastic-associated small-cell lung cancers. The potential role of FDG-PET to assess early therapeutic response and disease prognostification has also been demonstrated.
In comparison with conventional imaging, PET–CT has been shown to be more sensitive in the detection of mesothelioma, in active pleural plaques. Circumferential pleural uptake of FDG is characteristic of this disease.
FDG PET/CT in Lung Cancer Restaging
As a rule, for lesions that are greater than 1 cm, an SUV greater than or equal to 2.5 and a visual intensity greater than that within the mediastinal blood pool are accepted criteria for malignancy.
Limitations
Lesion size is an important factor when a patient is undergoing FDG-PET evaluation for lung cancer. The threshold for lesion detection for most FDG-PET scanners currently in use is between 6 and 8 mm.
False-negative FDG-PET scans are seen in well-differentiated cancers such as bronchioloalveolar carcinoma (BAC), slow-growing neuroendocrine tumors such as bronchial carcinoid, and mucinous neoplasms.
Recurrent Lung Cancer/Second Primary
There may be considerable postoperative and postradiation therapy anatomic changes. These changes can make early detection of recurrent cancer a problem on anatomic imaging.
In patients who have been successfully treated for lung cancer, an important cause of mortality is the development of a second lung primary. In both recurrent and new primary lung cancer, FDG-PET imaging is valuable for detection of disease. Early detection is important, since new primaries are treated similarly to the initial primary and salvage therapies exist for localized recurrent lung cancer. A recent study revealed that the FDG-PET scan resulted in a major management change in 63 % of patients. Both the presence and the extent of disease were important prognostic factors.
Cost-Effectiveness
FDG PET/CT is a one-shop stop for staging with brain MRI, identification of distant metastatic disease, detection of recurrent disease, radiotherapy planning, response to therapy assessment, and as a prognostic indicator.
Newer Directions: Tracers Beyond FDG
FDG PET/CT is now an established modality in the management of lung cancer. A host of newer radiopharmaceuticals that target different aspects of tumor biology are being explored in lung cancers. These include the proliferation tracer 18F-fluorothymidine, which has been evaluated in few studies and found to be useful. Other tracers that provide information regarding hypoxia (18F-FMISO, 64Cu-ATSM), angiogenesis (RGD peptides), amino acid metabolism (11C-methionine), and choline metabolism (11C-choline, 18F-fluorocholine) have also been evaluated. An evolving area is the noninvasive assessment of epidermal growth factor receptor (EGFR) and EGFR tyrosine kinase overexpression in tumors by PET imaging that has the potential for in vivo a priori determination of EGFR-targeted drug efficacy. These agents might give better insight into tumor behavior, aggressiveness, and therapy-related toxicity, thereby helping in the formulation of individualized treatment strategies with targeted agents. However, substantial prospective assessment is needed before these agents come into routine use.
Concluding Remarks
Diagnosis, staging, and restaging of lung cancer are among the most extensively studied applications of FDG-PET. With the exception of bronchioloalveolar cell cancer and carcinoid, lung cancer is FDG avid. Lung cancer is one of the most commonly employed indications for FDG PET/CT in clinical practice, and the modality has a substantial impact on the management of lung cancer.
For Further Reading
Bradley J, Thorstad WL, Mutic S, Miller TR, Dehdashti F, Siegel BA, et al. Impact of FDG-PET on radiation therapy volume delineation in non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004;59:78–86.
Buck AK, Herrmann K, Schreyögg J. PET-CT for staging lung cancer: costly or cost-saving? Eur J Nucl Med Mol Imaging. 2011;38:799–801.
De Wever W, Ceyssens S, Mortelmans L, Stroobants S, Marchal G, Bogaert J, et al. Additional value of PET-CT in the staging of lung cancer: comparison with CT alone, PET alone and visual correlation of PET and CT. Eur Radiol. 2007;17:23–32.
Kim SK, Allen Auerbach M, Goldin J, Fueger BJ, Dahlbom M, Brown M, et al. Accuracy of PET-CT in characterization of solitary pulmonary lesions. J Nucl Med. 2007;48:214–20.
Lynch TB. Textbook of PET-CT in clinical practice. Springer-Verlag, Berlin/Heidelberg/New York; 2007. p. 16–47.
Mac Manus MP, Hicks RJ. Impact of PET on radiation therapy planning in lung cancer. Radiol Clin North Am. 2007;45:627–38.
Nahmias C, Wahl LM. Reproducibility of standardized uptake value measurements determined by 18F-FDG PET in malignant tumors. J Nucl Med. 2008;49:1804–8.
Yamamoto Y, Kameyama R, Murota M, Bandoh S, Ishii T, Nishiyama Y. Early assessment of therapeutic response using FDG PET in small cell lung cancer. Mol Imaging Biol. 2009;11:467–72.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer India
About this chapter
Cite this chapter
Sonavane, S., Basu, S. (2015). PET–CT Imaging of Lung Cancer: The Current Status and Future Potentials. In: Das, B. (eds) Positron Emission Tomography. Springer, New Delhi. https://doi.org/10.1007/978-81-322-2098-5_12
Download citation
DOI: https://doi.org/10.1007/978-81-322-2098-5_12
Published:
Publisher Name: Springer, New Delhi
Print ISBN: 978-81-322-2097-8
Online ISBN: 978-81-322-2098-5
eBook Packages: MedicineMedicine (R0)