
Abstract
The definitive treatment of early stage prostate cancer with radiation therapy has progressed dramatically over the past two decades primarily due to the development and implementation of intensity-modulated radiation therapy (IMRT) techniques and better definition of the role of androgen deprivation therapy (ADT). IMRT has permitted the escalation of radiotherapy dose to the target tissues, namely, the prostate and proximal seminal vesicles, in an effort to improve tumor cell killing and local tumor control, while also reducing dose to nearby organs at risk (OARs) including the bladder, rectum, bowel, femoral heads, and penile bulb. Advances in image-guided radiotherapy (IGRT) have improved the accuracy of the delivery of IMRT, reduced PTV margins, and consequently decreased acute and long-term side effects. This chapter will review the clinical evidence for the use of IMRT for early stage, clinically localized (T1–2N0M0) prostate cancer and will outline the processes involved in designing and implementing a safe and effective IMRT treatment plan.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Risk classifications
- Androgen deprivation therapy
- Interfraction motion
- Intrafraction motion
- Image-guided treatment delivery
1 Introduction
The definitive treatment of early stage prostate cancer with radiation therapy has progressed dramatically over the past two decades primarily due to the development and implementation of intensity-modulated radiation therapy (IMRT) techniques and better definition of the role of androgen deprivation therapy (ADT). IMRT has permitted the escalation of radiotherapy dose to the target tissues, namely, the prostate and proximal seminal vesicles, in an effort to improve tumor cell killing and local tumor control, while also reducing dose to nearby organs at risk (OARs) including the bladder, rectum, bowel, femoral heads, and penile bulb. Advances in image-guided radiotherapy (IGRT) have improved the accuracy of the delivery of IMRT, reduced PTV margins, and consequently decreased acute and long-term side effects. This chapter will review the clinical evidence for the use of IMRT for early stage, clinically localized (T1–2N0M0) prostate cancer and will outline the processes involved in designing and implementing a safe and effective IMRT treatment plan.
2 Staging/Risk Classifications
Prostate cancer is the leading cause of non-skin cancer in the US adult male population [1] and is the second most common cause of cancer mortality in American men according to the Centers for Disease Control and Prevention. The American Joint Committee on Cancer (AJCC) anatomic staging system for prostate cancer is outlined in Table 19.1 and the prognostic grouping based on TNM stage, PSA, and Gleason score in Table 19.2. Men with early stage, localized prostate cancer who are candidates for primary therapy most commonly fall into the low-risk (group I: cT1–2a, Gleason 6, PSA <10) and intermediate-risk (group IIa: cT2b and/or Gleason 7 and/or PSA 10–20) categories, which are similar to the NCCN risk groups, the main difference being that cT2c is considered high risk in the AJCC grouping (IIb) and intermediate risk in the NCCN grouping.
3 Treatment Options
The most established treatment options for favorable to intermediate-risk prostate cancer include radical prostatectomy, external beam radiotherapy, or brachytherapy. There are no published contemporary phase III randomized trials that have directly compared these treatment options to determine which therapy, if any, is superior with regard to outcome and toxicity, and such comparisons may not be feasible [2].
4 Historical Review of RT Treatment Options and Outcomes
Conventional 2D RT was initially used to treat early stage prostate cancer, but efficacy at ≤70 Gy was found to be less than previously thought when PSA became available for assessing duration of response [3]. When using 2D techniques to achieve doses >70 Gy, the genitourinary and gastrointestinal side effects increase considerably [4]. However, several retrospective analyses indicated that the delivery of doses higher than 70 Gy improved local control of the tumor [5–7]. Further technological innovations introduced CT-based 3D conformal radiotherapy (3D CRT) delivery systems. These 3D systems enabled radiation oncologists to more safely escalate radiotherapy to doses >70 Gy before reaching the upper limit of acceptable bladder and rectal toxicities [8]. An early study utilizing 3D CRT for the prostate boost portion of treatment demonstrated on DVH analysis that the volume of bladder and rectum receiving the prescribed dose could be reduced to nearly one half of the volume treated with 2D RT delivery [9]. Eade et al. described the dose response for over 1,500 men treated with 3D conformal or IMRT at Fox Chase Cancer Center from 1998 to 2002, demonstrating that there are continued gains of approximately 2.2 % freedom from biochemical failure (FFBF) for every 1 Gy increase, even beyond 80 Gy using either the nadir + 2 or ASTRO definitions of biochemical failure [10].
Several randomized, controlled trials also compared higher dose radiotherapy (>70 Gy) to conventionally dosed radiotherapy (70 Gy) with respect to outcomes in men with prostate cancer [11–15]. In a randomized dose escalation trial of 301 patients, Kuban et al. found an improvement in freedom from biochemical or clinical failure at a median follow-up of 8.7 years of 78 % in the group receiving 78 Gy compared to 59 % in patients receiving 70 Gy [11]. However, gastrointestinal toxicity of grade 2 or greater occurred in 26 % of patients in the high-dose 78 Gy arm compared to 13 % in the conventional 70 Gy arm in treatment delivered by 3D CRT. A meta-analysis that included 7 trials found a significant FFBF benefit for dose escalation when all of the trials (p < 0.0001) were considered [16]. This benefit was significant for NCCN low-risk (p = 0.007), intermediate-risk (p < 0.0001), and high-risk (p < 0.0001) groups, although no difference was found for overall survival (p = 0.69) or disease-specific survival (p = 0.41). All of the trials had less than 10 years of follow-up, which is not sufficient for survival endpoints.
5 Clinical Evidence for IMRT
While the 3D CRT prostate cancer dose escalation trials were accruing, intensity-modulated radiotherapy (IMRT) was introduced, revolutionizing the radiation treatment of numerous tumor types, including prostate cancer. In 1996, Ling et al. published one of the first descriptions of prostate cancer inversely planned intensity-modulated photon beams using dynamic multi-leaf collimation [17]. The ability to collimate the treatment fields in a dynamic way during the delivery of radiation resulted in more conformal dose distributions with the potential to reduce toxicity.
When compared directly to 3D CRT plans in dosimetric studies, IMRT proved superior in target volume coverage at the prescribed dose and at reducing the volume of normal tissues treated to specified constraint doses [18–22]. Ailleres reported that 95 % of the PTV1 received 5 Gy more with IMRT when compared to 3D CRT planning without compromising dose limits on the bladder and rectal walls [23]. Using an endorectal balloon for prostate immobilization, Ashman compared sequential IMRT plans to 3D CRT in delivering whole pelvic radiotherapy and found that IMRT reduced the volume of bowel receiving 45 Gy by 60 % when compared to 3D CRT delivery [21]. Without placing intentional constraints on the penile bulb dose, Kao designed IMRT and 3D CRT plans to deliver 74 Gy to the target for ten patients with clinically organ-confined prostate cancer; IMRT reduced the mean penile bulb dose, the percentage of bulb receiving >40 Gy, and the dose received by >95 % of the penile bulb; however, the maximum penile bulb dose was higher to a very small volume [22]. Subsequent studies have confirmed the reduction in dose to critical structures including the penile bulb with IMRT while achieving improved coverage to target structures including the pelvic lymph nodes [24, 25].
Investigators at Memorial Sloan Kettering Cancer Center were leaders in the application of IMRT to prostate cancer. Zelefsky et al. [26] described the early experience where 61 men with localized disease were treated with 3D CRT and 171 with IMRT to a prescribed dose of 81 Gy. When comparing the plans of 20 randomly selected patients, IMRT showed a significant improvement in the coverage of the clinical target volume (CTV) to the prescribed dose while lowering the volume of the bladder and rectal walls that received this dose. The analysis also demonstrated a reduction in the 2-year risk of rectal bleeding from 10 % with 3D CRT to 2 % for IMRT [26]. In a larger analysis, Zelefsky analyzed 1,100 patients with cT1c–T3N0 prostate cancer treated with 3D CRT or IMRT and reported statistically significant improvements in the 5-year PSA relapse-free survival in the favorable, intermediate, and unfavorable risk groups. For the patients who received a prescription dose of 81 Gy, IMRT resulted in significantly less late grade 2 rectal toxicity (14 % vs. 2 %) with no impact on GU toxicity [27]. In the Dutch randomized dose escalation trial CKVO 96-10, a subset analysis comparing the toxicities for patients who received 78 Gy via sequential 3D CRT or via simultaneous integrated boost, with IMRT, IMRT resulted in significantly lower acute grade 2+ GI toxicity (61 % vs. 20 %), while the rates of 5-year FFBF were comparable in both groups (61 % vs. 70 %). Acute GU and late GI and GU toxicities were similar in both groups [28]. Several other reports confirmed that IMRT is a safer delivery method for high-dose RT to the prostate [18, 23, 29], which eventually resulted in the adoption of IMRT as the standard of care.
IMRT is associated with an increased volume of low-dose radiation to normal tissues as a result of the multiple gantry angles by which IMRT is delivered to create the highly conformal dose distribution to target structures. Kry reported that IMRT required 3.5–4.9 times more monitor units (MU) when compared to more conventional treatments. According to the analysis, the calculated conservative maximal lifetime risk of fatal radiation-induced malignancy was 1.7 % for conventional RT, 2.1 % for IMRT with 10-MV X-rays, and 5.1 % for IMRT using 18-MV X-rays [30]. There are conflicting data on the observed risk of second malignancies after prostate cancer radiotherapy [31–35], and the overwhelming majority of clinical and dosimetric evidence support IMRT as the standard of care over 3D CRT.
6 IMRT Technique
Close collaboration between physicians, nurses, radiation therapists, dosimetrists, and medical physicists facilitates coordination that can reduce uncertainties in IMRT treatment delivery. In our institution, prior to diagnostic/planning MRI and CT simulation, the patient receives instructions on bowel and bladder preparation. Table 19.3 outlines the simulation technique and sequence that is utilized at the University of Miami.
All patients who are candidates for an MRI with contrast undergo diagnostic 3.0 T MRI of the prostate and pelvis using a body coil. Multiparametric MRI that includes T2w, T1 non-contrast, T1 dynamic contrast-enhanced (DCE)-MRI, and diffusion-weighted imaging (DWI) sequences (our standard sequences), as well as MR proton spectroscopy (MRS), has been shown to improve the sensitivity and specificity of tumor localization [36–39]. T2w-MRI provides an excellent depiction of prostate and pelvic anatomy with regions of healthy peripheral zone prostate tissue demonstrating higher signal intensity than prostate cancer. The observed reduction in MRI image signal intensity is due to a loss of the normal glandular (ductal) morphology in regions of prostate cancer. However, other benign pathologies such as inflammation, benign prostatic hyperplasia (BPH), blood, and prior radiation treatment also cause a loss of ductal morphology and low signal intensity on T2w-MRI. Additionally, infiltrating prostate cancer does not always cause a reduction in normal glandular morphology and therefore may not be hypointense on T2w-MRI. Due to these confounding factors, T2w-MRI alone can localize cancer larger than 0.5 cm3 in volume with only a 65–74 % sensitivity and low specificity [40]. Other studies also report quite variable sensitivity (50–83 %) and specificity (21–88 %). Utilizing an endorectal coil improves MRI’s sensitivity to 78 %, but the specificity still remains poor (55 %).
MRS, DWI, and DCE-MRI have been used to improve the sensitivity and specificity of MRI and to determine tumor location and extent. Localization accuracies of above 80 % may be achieved by combining these methods [41]. Each has shown promise when combined with T2w-MRI. DWI is sensitive to random thermal movement of water molecules and provides a determination of stiffness. DWI is used to calculate apparent diffusion coefficient (ADC) values, which are significantly lower in tumor than in normal prostate due to the restriction of water displacement. Lower ADC values are associated with Gleason 7 or above disease [42].
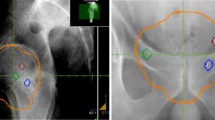
DCE-MRI also discriminates between normal and cancerous tissues [43, 44]. Greater and earlier enhancement with washout over time is seen in tumor tissue vs. delayed enhancement in normal tissue. DCE-MRI is a measure of tissue vascularity and angiogenesis. Specificity has been notably high at close to or over 90 % in a number of studies [45, 46], while sensitivity has been 65 to >80 %. At the University of Miami, we routinely use DCE-MRI combined with DWI (and ADC maps) and T2w-MRI in our assessments and planning of radiotherapy. These sequences aid in the determination of tumor location and extraprostatic extension, thereby informing the CTV. In addition, there is an emerging literature on delivering higher daily doses using dose painting to the dominant prostatic lesion(s) based on MRI criteria [47–54], and we are testing this approach in clinical trials (Fig. 19.1). In some high-risk patients with well-defined MRI lesions, we have boosted the dominant intraprostatic lesion(s) slightly (2.15 Gy per fraction to 86 Gy) if not a candidate for a clinical trial.

Dose distribution on a single axial slice for a dose-painting IMRT plan prescribing a boost to dominant intraprostatic lesion(s) on multiparametric MRI for patient on an inhouse (UM) clinical trial
Patients are given bowel preparation and bladder filling instructions for the diagnostic MRI to mimic treatment bladder and rectal filling. If possible, the MRI is performed on a flat tabletop to most accurately reproduce the patient’s treatment position. After the MRI, 3–4 gold fiducial markers are implanted transrectally in the prostate at a distance of 1 cm apart [55], to reduce interfraction setup error [56–59]. Seed migration is not a major issue [57, 58, 60, 61]. We typically wait a week after fiducial marker placement before simulation to allow for the stabilization of fiducial position.
Gold seed fiducials are currently the most commonly employed method to correct for interfraction motion. Although patients do require an extra outpatient procedure, they tolerate the insertion well [62]. The most frequent reported side effects are hematuria (15 %) and rectal bleeding (4 %) [63]. Patients report their pain is less than that of diagnostic biopsy, even without local anesthesia. Daily fiducial marker alignment prior to each treatment via orthogonal portal imaging, cone beam CT, or in-room CT reduces uncertainties from interfraction motion [56], allowing for reduced margins [58, 59, 64, 65].
Daily alignment to gold seed fiducials reduces the subjectivity of the alignment process over cone beam CT (CBCT) alone. With fiducial correction for interfraction motion and arc-based therapy that typically takes <5 min (2–3 arcs), we use a PTV expansion of 5 mm everywhere, except posteriorly where the margin is 3–4 mm. Langen et al. have shown that the chance for prostate displacement increases over time during patient setup [66]; arc-based therapy reduces the chance of a portion of the CTV falling outside the PTV.
Real-time tracking of fiducials using fluoroscopy, electromagnetic transponders, or transperineal ultrasound [67] limits effects from intrafraction motion, which takes on considerable importance. When using transponders, three are placed in the prostate to define prostate position [68]. The system continuously monitors and compares the triangulated center of mass of the transponders to the planned isocenter. This information is used to stop the treatment if a predetermined threshold is exceeded [69]. The threshold that has been used in our institution is 3 mm. Of note, transponders result in significant artifacts on MRI that preclude assessments of tumor location or recurrence in the prostate.
After waiting 7 days to allow for fiducial marker position to stabilize, CT simulation with 2 mm slices is performed throughout the pelvis in supine position with arms on chest and legs supported or in an immobilization device such as a Vac-LokTM. On the same day, a limited 2.5 mm slice thickness MRI simulation using T1, DWI, T2*, and T2w sequences has been used for patients on protocols in which a GTV boost is administered in order to facilitate more accurate MRI-CT fusion based on the position of the implanted markers. While the simulation MRI is of value in fusing the diagnostic MRI to the planning CT, it is not usually reimbursed.
Bladder and rectal volumes should be thoroughly analyzed prior to approval of the CT simulation for IMRT planning. At our institution, we have a low threshold for repeating the CT simulation after the patient has adjusted the bladder filling or rectal emptying if these normal organs do not conform to our preferred volume and anatomic orientation. The smaller the rectal volume at simulation, the more the plan will reflect a worst case dosimetric assessment during planning.
7 Contouring of Target and Normal Anatomy
The IMRT planning process begins with the fusion of the CT and MRI images followed by delineation of the target structures and normal tissue volumes by the treating radiation oncologist. As background, the prostate is an exocrine gland that surrounds the prostatic urethra. The normal adult gland measures approximately 4×3×3 cm (transverse, AP, craniocaudal) and weighs 15–20 g [70]. The size of the prostate generally increases with age, and according to Zackrisson et al., up to 85 % of healthy males older than 40 years have prostate volumes higher than 20 cm3 [71]. Five anatomical prostatic zones are recognized: (1) anterior fibromuscular stroma, (2) periurethral glandular tissue, (3) transition zone, (4) central zone, and (5) peripheral zone [70].
Inconsistencies in CT contouring are the result of poor definition of the prostate relative to adjacent structures and wide variation in anatomic position relative to the pelvic bones [72]. The prostate tends to blend in with muscle, making it unclear where the prostate borders are located relative to the levator ani muscle, the rectum (particularly inferiorly near the prostatic apex), and the bladder wall superiorly. The inferior aspect of the prostatic apex is not recognizable on CT. The rectum blends into the apex posteriorly, and the urogenital diaphragm blends into the apex inferiorly. These structures are more clearly visualized on T2w-MRI [73]. Using CT alone, the apex location may be estimated to be about 1.0–1.5 cm superior to the bulb of the penis. It is best to overestimate the inferior location of the apex in the absence of MRI. MRI considerably resolves these boundaries and makes accurate contouring of the prostate more consistent [74, 75]. MRI prostate volumes are more aligned with ultrasound volumes [76]; CT prostate volumes are about 30–40 % larger than MRI volumes [77, 78]. However, current planning algorithms are based on CT, making CT-MR fusion the best approach to define the prostate, seminal vesicles, and pelvic lymph node regions.
CT-MR fusion is fraught with potential problems that could lead to significant errors if not performed appropriately. The CT should be used primarily and the MRI only used as a reference because of the inherent problems with the accuracy of CT-MR fusion. The position of the prostate on MRI may be substantially different from the CT because of bladder and rectal filling. These differences are accentuated when the MRI is being performed at a different time (not in sequence with the CT) and on a concave tabletop (instead of a flat table on the CT simulator). Patients should be given instructions on diet to minimize gas and should perform an enema before going for both the MRI and CT. Ideally, a radiation simulation therapist will be present at the MRI to confirm optimal bladder and bowel filling at the time of MRI. An MRI equipped with lasers to ensure accuracy of patient positioning will also help to optimize the subsequent CT-MR fusion. If there are considerable differences in bladder and rectal filling, the fusion will be inaccurate. The random error for CT-MR registration along the three spatial directions was estimated to be on the order of 0.5 mm and around 0.4° in rotation (standard deviation) for each axis [79]. Fusion error is minimized when a second limited MRI simulation (T1, DWI, T2, and T2* MRI sequences) with fiducials in place on the same day of CT simulation is performed and the fiducial markers are considered in the fusion process [54].
The seminal vesicles (SV) are paired organs located in the connective tissue lodged between the urinary bladder and the rectum lateral to the ampulla of the vas deferens. Seminal vesicles can vary in size, and differences in dimension between the right and left seminal vesicle have been reported [80, 81]. According to surgical specimen reports, the length is about 31 ± 10.3 mm [80], which is concordant with reported results on ultrasound [71]. The angle between the seminal vesicles and the horizontal plane (normally 50 to 60°) changes with bladder and rectal filling [82]. Seminal vesicle contouring, similar to that of prostate contouring, is better delineated on MRI because of enhanced anatomic detail [83]. We include the proximal SVs in the CTV with the prostate.
The bulb of the penis is formed by the elongation of the corpus spongiosum after the separation of the corpora cavernosa to form the crura of the penis. The bulb of the penis is attached superiorly to the inferior surface of the urogenital diaphragm [84]. The penile bulb is best visualized on T2w-MRI as an oval-shaped, hyperintense midline structure [25, 84]. Although the penile bulb can also be identified on CT imaging and transverse transrectal ultrasound, MRI is best for the superior and inferior aspects. Contouring should stop inferiorly when the bulb loses the lateral bulging aspects of the corpus spongiosum. As summarized by Van der Wielen et al. [85], the sparing of the penile bulb, corporal bodies, and neurovascular structures has sometimes been associated with increased preservation of erectile function, but results have been mixed [25, 86]. IMRT reduces the dose received by the penile bulb, as shown by some authors and reported above [22, 87]. Regarding the relationship between the penile bulb dose and the development of erectile dysfunction, some studies have not shown any significant association [88], whereas Merrick et al. have [89]. Roach et al. advocate keeping the penile bulb dose to <52.5 Gy [90].
8 IMRT Planning and Dosimetry
Table 19.4 outlines common dose constraints utilized in IMRT planning for prostate cancer. Figure 19.2 demonstrates a typical IMRT treatment plan with corresponding dose-volume histograms when prescribing 80 Gy in 40 fractions to the PTV, the standard dose used at the University of Miami. At the University of Miami, particular attention is paid to the 30 Gy isodose line, and optimization structures are created to ensure that this line is anterior to the posterior rectal wall, as well as excluding the lateral rectal wall as much as possible (Fig. 19.3). The bladder volume at 30 Gy is also reduced by designing a plan that pulls in dose tightly in the anterior. The resultant optimization of dose across the rectal and bladder is accomplished using optimization structures that result in an increase in doses to the lateral soft tissues and femoral heads while still maintaining constraints to the femoral heads (Fig. 19.4).


Dose distribution and DVH for a typical IMRT plan prescribing 80 Gy in 40 fractions to the PTV

Example of optimization structure (shaded blue) utilized to pull dose in anteriorly to spare the rectum and posteriorly to better spare the bladder while pushing out lower dose regions into lateral soft tissues. The optimized plan is on the left

Dose distribution and DVH comparison at multiple axial slices for a typical optimized IMRT plan (left) compared to an initial IMRT plan (right). Attention is given to the 30 Gy isodose line, which is pushed well within the rectum
9 IMRT Delivery Methods
Two common treatment delivery techniques include standard fixed gantry IMRT, otherwise known as step-and-shoot, and volumetric modulated arc therapy (VMAT). The step-and-shoot technique results in increased treatment time compared to VMAT as the gantry must be repositioned between the deliveries of each small, irregularly shaped field. The VMAT technique typically requires 2–3 arcs for the delivery of one standard daily fraction. VMAT reduces the overall treatment time on average by 1.5–3 min for each 2 Gy fraction by delivering the dose during a continuous gantry rotation and also reduces the calculated monitor units by approximately 50 % [91]. Treatment time is reduced more significantly when the pelvic lymph nodes are treated for high-risk disease. Additionally, VMAT may offer dosimetric advantages over IMRT in some cases, especially in high-dose regions [92]. Another variant of continuous rotational treatment is TomoTherapy®, which offers at least equivalent, if not slightly improved, dose distributions [93].
10 Image-Guided Treatment Delivery (IGRT): Interfraction Motion
Interfraction motion occurs during the daily setup of patients and can result in decreased dose to the PTV and increased toxicity due to increased dose to normal tissues. Uncertainties in prostate position are related to both setup error and prostate motion between daily fractions. Setup error could be systematic or random. Systematic errors do not change, are reproducible, and always occur in the same direction and magnitude. Random errors vary daily and are not reproducible [94].
The prostate is not a fixed organ, and its location can vary significantly from day to day [95–99]. The mean prostate shift was found to be 1.0 + 1.5 mm in the lateral direction, 0.9 + 2.1 mm in the AP, and 1.9 + 2.1 mm in the craniocaudal direction in an Italian study. After DVH recalculation, CTV coverage was maintained despite organ motion, whereas rectal DVHs were often dramatically different [95]. The amount of prostate motion varies from patient to patient, and the reproducibility of daily prostate positioning has become increasingly important with decreased PTV margins and dose escalation permitted by IMRT.
The impact of rectal distension on prostate target volume variability, treatment dose, and patient outcomes has been well studied [100–104]. The effects of rectal distension at simulation described by de Crevoisier et al. [103] can be mitigated by the use of daily image guidance [105]. There are many methods to correct the observed interfraction motion. These methods are daily CT bony pelvis alignment, daily cone beam CT or ultrasound soft tissue alignment, definitive isocenter calculation, and daily online fiducial correction. If gold seed markers are not placed within the prostate, daily CT localization using bony anatomy could be used with reasonable results [98]. The increase in PTV margin would consist of the uncertainty of the location of the prostate with respect to the bone in addition to intrafractional motion. Hanna et al. also described how centrally located intraprostatic calcifications (IPC) can be used as natural fiducials with similar pattern of displacement compared to implanted fiducials [106]. The use of IPC in IGRT for prostate cancer can eliminate an invasive procedure to implant fiducials which comes with both financial cost and unnecessary morbidity when IPCs are identified.
Cone beam CT (CBCT) 3D volume reconstruction images have improved over the years and are often used for correction of prostate interfraction motion. The measures obtained by the use of CBCT are highly accurate, with the greatest displacement usually observable in the AP axis [107, 108].
CBCT appears to be associated with less variability than ultrasound [109]. However, therapists must still make subjective decisions concerning prostate anatomy. We combine daily fiducial marker assessment with CBCT to reduce the subjectiveness of the alignment and assess bladder and rectal filling. A broad comparison of MV CBCT with other imaging modalities was performed by Bylund et al. [108], who found a similar measurement of interfraction motion when comparing their results with other published studies that used electromagnetic transponders, ultrasound, fiducial seed marker implants, and CT on rails as image guidance methods [110, 111]. A study performed by Moseley et al. retrospectively compared the patient adjustments based on kV CBCT compared to two orthogonal MV portal images and confirmed that there was a high correlation for the measured isocenter shifts between these systems [98].
Advances in ultrasound technology have resulted in noninvasive and non-ionizing methods of daily prostate localization that do not require the implantation of fiducial markers. Boda-Heggemann et al. demonstrated that transabdominal ultrasound improved the daily repositioning accuracy compared to the use of skin marks or bony anatomy [112]. The development of 3D ultrasound imaging modalities has improved IGRT via ultrasound by providing physicians with data regarding the daily changes in the target dimensions and location, while automatically calculating geometric beam coverage to ensure the accuracy of the treatment delivery.
11 Image-Guided Treatment Delivery (IGRT): Intrafraction Motion
Real-time tracking of the prostate via fiducials using fluoroscopy, electromagnetic transponders, or transperineal ultrasound [67] limits effects from intrafraction motion, which takes on considerable importance for hypofractionation. Alonso-Arrizabalaga et al. [64] found that the margins can be reduced with correction for interfraction and intrafraction prostate motion. Compared to daily online correction, there was a PTV increase of 40 % for definitive isocenter and 80 % for bony anatomy image guidance. The overlap of PTV with the rectum approximately doubles for each of these increases.
Kupelian et al. [110] reported the use of a 4D localization system for continuous, intrafraction three-dimensional isocenter tracking via electromagnetic detection of three implanted beacon transponders. In this study, 41 patients with clinical stage I–III prostate cancer treated per institutional preference had transponder setup compared to traditional laser and skin markings performed pretreatment and between beams for all patients, and during delivery for 35 of 41 patients (6 patients had large anteroposterior torso dimensions precluding tracking due to geometric constraints). Transponder stability after implantation was demonstrated with a mean standard deviation of the intertransponder distance of 0.8 mm. The study identified a seemingly random continuous motion ≥3 mm and ≥5 mm for durations exceeding 30 s in 41 % and 15 % of fractions, respectively. This intrafraction motion could have significant effects with respect to coverage, especially when treatment margins of as small as 5 mm are not uncommon.
12 Dose Escalation: Beyond 80 Gy
As previously discussed, IMRT has allowed the safe delivery of higher doses in the 74–80 Gy range, which has resulted in improved outcomes. Under investigation now is even further dose escalation beyond 80 Gy. Eade et al. [10] described a dose response beyond 80 Gy, the data of which were used as a rationale for the Fox Chase dose escalation hypofractionation trial described by Pollack et al. [113]. A phase II study from Memorial Sloan Kettering Cancer Center described the treatment of 1,002 patients treated to 86.4 Gy in 48 fractions from 1997 to 2008 with a median follow-up of 5.5 years; 86 % of patients were clinical stage T1–T2N0. The PTV consisted of the prostate, entire seminal vesicles, and a 10 mm circumferential margin, except posteriorly, where it was reduced to 6 mm. Weekly port films were used to verify patient positioning. Fifty-nine percent of patients received ADT. Seven-year biochemical recurrence-free survival rates based on the nadir plus 2 ng/mL definition were 98.8 %, 85.6 %, and 67.9 % (p < 0.001) for low-, intermediate-, and high-risk patients, respectively. Seven-year actuarial distant metastasis-free survival rates were 99.4 %, 94.1 %, and 82.0 % (p < 0.001) for low-, intermediate-, and high-risk patients, respectively. Seven-year prostate cancer-specific mortality rates using competing risk analysis were 0 %, 3.3 %, and 8.1 % (p = 0.008), for low-, intermediate-, and high-risk patients, respectively. Late grade 3 gastrointestinal and genitourinary toxicities at 7 years were experienced by 0.7 % and 2.2 % of patients, respectively [114]. Although this was a retrospective study with modest follow-up of a median of 5.5 years, further dose escalation beyond 80 Gy demonstrated excellent tumor control and relatively low rates of toxicity. More recently, Spratt et al. [115] described that the combination of brachytherapy plus external beam RT was superior to 86.4 Gy of external beam RT alone, illustrating the potential benefit of further dose escalation. These findings are complicated by changes in (better IGRT) methods over the period of the study and patient selection bias. Nonetheless, such data lend support for further dose escalation using IMRT to dominant tumor regions defined on MRI [54, 116], since these seem to be at the greatest risk of persistent disease [117].
13 Androgen Deprivation Therapy
A group of patients with early stage prostate cancer fall into the intermediate-risk prognostic group as a result of their specific PSA and/or Gleason score. In studies of primarily intermediate-risk patients, two main randomized trials support the addition of short-term ADT to RT when standard doses of RT were used (about 70 Gy). D’Amico et al. compared 6 months of ADT with RT versus RT alone in 206 men with AJCC clinical stage T1b–T2bN0M0 adenocarcinoma of the prostate with at least 1 unfavorable prognostic factor (PSA > 10 ng/mL, GS 7–10, radiographic evidence of extracapsular extension, and/or seminal vesicle invasion on MRI) who were treated between 1995 and 2001. All patients in the combined treatment arm received 3D conformal RT and ADT (consisting of a luteinizing hormone-releasing hormone (LHRH) agonist and the antiandrogen flutamide beginning 2 months prior to RT). With a median follow-up of 7.6 years, the 8-year overall survival was 74 % in the combined RT-ADT arm and 61 % in the RT alone arm (p = 0.01). In addition, RT alone resulted in an increased risk of prostate cancer-specific mortality (HR 4.1; 95 % CI, 1.4–12.1; p = 0.01), as well as all-cause mortality (HR 1.8; 95 % CI, 1.1–2.9; p = 0.01) compared to RT-ADT. An unplanned post-randomization subgroup analysis revealed that the increased risk in all-cause mortality in men randomized to RT alone was only found in those with no or minimal comorbidity (31 vs. 11 deaths; HR 4.2; 95 % CI, 2.1–8.5; p < 0.001) [118].
RTOG 94-08 compared 4 months of ADT with RT versus RT alone in 1979 men with AJCC stage T1b–T2bN0M0 adenocarcinoma of the prostate with a PSA level ≤20 ng/ml who were treated between 1994 and 2001. ADT consisted of an LHRH agonist and an antiandrogen beginning 2 months prior to RT and continued during RT. With a median follow-up of 9.1 years, the 10-year overall survival was 62 % in the combined arm and 57 % in the RT alone arm (HR 1.17; 95 % CI, 1.01–1.35; p = 0.03). The 10-year disease-specific mortality was 4 % in the combined arm and 8 % in the RT alone arm (HR 1.87; 95 % CI, 1.27–2.74; p = 0.001). The 10-year cumulative incidence of distant metastasis was 6 % in the combined arm and 8 % in the RT alone arm (HR 1.45; 95 % CI, 1.03–2.06; p = 0.04). Of note, multivariate analysis revealed Gleason score of 7 or higher to be a negative prognostic factor for overall survival, disease-specific survival, distant metastasis, and biochemical failure. Further subgroup analysis revealed that the overall survival and disease-specific mortality benefits were greatest in the intermediate-risk category patients and were not significant in the low-risk patient group [119].
Both trials used standard RT doses of about 70 Gy and were conducted in the pre-IGRT/IMRT era. RTOG 08-15 is currently examining the role of 6 months of ADT in addition to dose-escalated RT for patients with intermediate-risk prostate cancer. Lastly, practical factors such as patient age, comorbidities including a history of congestive heart failure or prior myocardial infarction, MRI stage, and extent of tumor on diagnostic biopsies help inform whether ADT should be added to definitive RT in intermediate-risk, early stage (T1a–2bN0M0) prostate cancer patients.
References
Siegel R, Naishadham D, Jemal A (2012) Cancer statistics, 2012. CA Cancer J Clin 62(1):10–29
Eccles BK et al (2013) SABRE 1 (Surgery Against Brachytherapy – a Randomised Evaluation): feasibility randomised controlled trial (RCT) of brachytherapy vs radical prostatectomy in low-intermediate risk clinically localised prostate cancer. BJU Int 112(3):330–337
Kuban DA et al (2003) Long-term multi-institutional analysis of stage T1-T2 prostate cancer treated with radiotherapy in the PSA era. Int J Radiat Oncol Biol Phys 57(4):915–928
Pilepich MV et al (1987) Correlation of radiotherapeutic parameters and treatment related morbidity in carcinoma of the prostate–analysis of RTOG study 75–06. Int J Radiat Oncol Biol Phys 13(3):351–357
Hanks GE, Martz KL, Diamond JJ (1988) The effect of dose on local control of prostate cancer. Int J Radiat Oncol Biol Phys 15(6):1299–1305
Valicenti R et al (2000) Survival advantage from higher-dose radiation therapy for clinically localized prostate cancer treated on the Radiation Therapy Oncology Group trials. J Clin Oncol 18(14):2740–2746
Zelefsky MJ et al (2008) Influence of local tumor control on distant metastases and cancer related mortality after external beam radiotherapy for prostate cancer. J Urol 179(4):1368–1373; discussion 1373
Leibel SA et al (1994) The biological basis and clinical application of three-dimensional conformal external beam radiation therapy in carcinoma of the prostate. Semin Oncol 21(5):580–597
Ten Haken RK et al (1989) Boost treatment of the prostate using shaped, fixed fields. Int J Radiat Oncol Biol Phys 16(1):193–200
Eade TN et al (2007) What dose of external-beam radiation is high enough for prostate cancer? Int J Radiat Oncol Biol Phys 68(3):682–689
Kuban DA et al (2008) Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys 70(1):67–74
Zietman AL et al (2005) Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. J Am Med Assoc 294(10):1233–1239
Peeters ST et al (2006) Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol 24(13):1990–1996
Dearnaley DP et al (2007) Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT01 randomised controlled trial. Lancet Oncol 8(6):475–487
Beckendorf V et al (2011) 70 Gy versus 80 Gy in localized prostate cancer: 5-year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys 80(4):1056–1063
Viani GA, Stefano EJ, Afonso SL (2009) Higher-than-conventional radiation doses in localized prostate cancer treatment: a meta-analysis of randomized, controlled trials. Int J Radiat Oncol Biol Phys 74(5):1405–1418
Ling CC et al (1996) Conformal radiation treatment of prostate cancer using inversely-planned intensity-modulated photon beams produced with dynamic multileaf collimation. Int J Radiat Oncol Biol Phys 35(4):721–730
Marchal C et al (2004) Preliminary results of the assessment of intensity modulated radiotherapy (IMRT) for prostatic and head and neck tumors (STIC 2001). Cancer Radiother 8(Suppl 1):S121–S127
Nutting CM et al (2000) Reduction of small and large bowel irradiation using an optimized intensity-modulated pelvic radiotherapy technique in patients with prostate cancer. Int J Radiat Oncol Biol Phys 48(3):649–656
Vlachaki MT et al (2005) IMRT versus conventional 3DCRT on prostate and normal tissue dosimetry using an endorectal balloon for prostate immobilization. Med Dosim 30(2):69–75
Ashman JB et al (2005) Whole pelvic radiotherapy for prostate cancer using 3D conformal and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys 63(3):765–771
Kao J et al (2004) Sparing of the penile bulb and proximal penile structures with intensity-modulated radiation therapy for prostate cancer. Br J Radiol 77(914):129–136
Ailleres N et al (2004) Pilot study of conformal intensity modulated radiation therapy for localized prostate cancer. Cancer Radiother 8(2):59–69
Wang-Chesebro A et al (2006) Intensity-modulated radiotherapy improves lymph node coverage and dose to critical structures compared with three-dimensional conformal radiation therapy in clinically localized prostate cancer. Int J Radiat Oncol Biol Phys 66(3):654–662
Perna L et al (2009) Sparing the penile bulb in the radical irradiation of clinically localised prostate carcinoma: a comparison between MRI and CT prostatic apex definition in 3DCRT, Linac-IMRT and Helical Tomotherapy. Radiother Oncol 93(1):57–63
Zelefsky MJ et al (2000) Clinical experience with intensity modulated radiation therapy (IMRT) in prostate cancer. Radiother Oncol 55(3):241–249
Zelefsky MJ et al (2001) High dose radiation delivered by intensity modulated conformal radiotherapy improves the outcome of localized prostate cancer. J Urol 166(3):876–881
Al-Mamgani A et al (2009) Role of intensity-modulated radiotherapy in reducing toxicity in dose escalation for localized prostate cancer. Int J Radiat Oncol Biol Phys 73(3):685–691
De Meerleer G et al (2004) Intensity-modulated radiotherapy as primary treatment for prostate cancer: acute toxicity in 114 patients. Int J Radiat Oncol Biol Phys 60(3):777–787
Kry SF et al (2005) The calculated risk of fatal secondary malignancies from intensity-modulated radiation therapy. Int J Radiat Oncol Biol Phys 62(4):1195–1203
Brenner DJ et al (2000) Second malignancies in prostate carcinoma patients after radiotherapy compared with surgery. Cancer 88(2):398–406
Brenner DJ (2006) Induced second cancers after prostate-cancer radiotherapy: no cause for concern? Int J Radiat Oncol Biol Phys 65(3):637–639
Nieder AM, Porter MP, Soloway MS (2008) Radiation therapy for prostate cancer increases subsequent risk of bladder and rectal cancer: a population based cohort study. J Urol 180(5):2005–2009; discussion 2009–10
Singh AK et al (2010) Increasing age and treatment modality are predictors for subsequent diagnosis of bladder cancer following prostate cancer diagnosis. Int J Radiat Oncol Biol Phys 78(4):1086–1094
Kendal WS et al (2006) Prostatic irradiation is not associated with any measurable increase in the risk of subsequent rectal cancer. Int J Radiat Oncol Biol Phys 65(3):661–668
Isebaert S et al (2013) Multiparametric MRI for prostate cancer localization in correlation to whole-mount histopathology. J Magn Reson Imaging 37(6):1392–1401
Sciarra A et al (2011) Advances in magnetic resonance imaging: how they are changing the management of prostate cancer. Eur Urol 59(6):962–977
Hegde JV et al (2013) Multiparametric MRI of prostate cancer: an update on state-of-the-art techniques and their performance in detecting and localizing prostate cancer. J Magn Reson Imaging 37(5):1035–1054
Vargas HA et al (2011) Diffusion-weighted endorectal MR imaging at 3 T for prostate cancer: tumor detection and assessment of aggressiveness. Radiology 259(3):775–784
Coakley FV et al (2002) Prostate cancer tumor volume: measurement with endorectal MR and MR spectroscopic imaging. Radiology 223(1):91–97
Mazaheri Y et al (2008) Prostate cancer: identification with combined diffusion-weighted MR imaging and 3D 1H MR spectroscopic imaging–correlation with pathologic findings. Radiology 246(2):480–488
Hambrock T et al (2011) Relationship between apparent diffusion coefficients at 3.0-T MR imaging and Gleason grade in peripheral zone prostate cancer. Radiology 259(2):453–461
Padhani AR et al (2000) Dynamic contrast enhanced MRI of prostate cancer: correlation with morphology and tumour stage, histological grade and PSA. Clin Radiol 55(2):99–109
Turnbull LW et al (1999) Differentiation of prostatic carcinoma and benign prostatic hyperplasia: correlation between dynamic Gd-DTPA-enhanced MR imaging and histopathology. J Magn Reson Imaging 9(2):311–316
Girouin N et al (2007) Prostate dynamic contrast-enhanced MRI with simple visual diagnostic criteria: is it reasonable? Eur Radiol 17(6):1498–1509
Schmuecking M et al (2009) Dynamic MRI and CAD vs. choline MRS: where is the detection level for a lesion characterisation in prostate cancer? Int J Radiat Biol 85(9):814–824
Singh AK et al (2007) Simultaneous integrated boost of biopsy proven, MRI defined dominant intra-prostatic lesions to 95 Gray with IMRT: early results of a phase I NCI study. Radiat Oncol 2:36
Fonteyne V et al (2008) Intensity-modulated radiotherapy as primary therapy for prostate cancer: report on acute toxicity after dose escalation with simultaneous integrated boost to intraprostatic lesion. Int J Radiat Oncol Biol Phys 72(3):799–807
Ippolito E et al (2012) Intensity-modulated radiotherapy with simultaneous integrated boost to dominant intraprostatic lesion: preliminary report on toxicity. Am J Clin Oncol 35(2):158–162
Aluwini S et al (2013) Stereotactic body radiotherapy with a focal boost to the MRI-visible tumor as monotherapy for low- and intermediate-risk prostate cancer: early results. Radiat Oncol 8:84
Riches SF et al (2014) Effect on therapeutic ratio of planning a boosted radiotherapy dose to the dominant intraprostatic tumour lesion within the prostate based on multifunctional MR parameters. Br J Radiol 87(1037):20130813
Murray LJ et al (2014) Prostate stereotactic ablative radiation therapy using volumetric modulated arc therapy to dominant intraprostatic lesions. Int J Radiat Oncol Biol Phys 89(2):406–415
Bauman G et al (2013) Boosting imaging defined dominant prostatic tumors: a systematic review. Radiother Oncol 107(3):274–281
van Lin EN et al (2006) IMRT boost dose planning on dominant intraprostatic lesions: gold marker-based three-dimensional fusion of CT with dynamic contrast-enhanced and 1H-spectroscopic MRI. Int J Radiat Oncol Biol Phys 65(1):291–303
Shinohara K, Roach M 3rd (2008) Technique for implantation of fiducial markers in the prostate. Urology 71(2):196–200
Gauthier I et al (2009) Dosimetric impact and theoretical clinical benefits of fiducial markers for dose escalated prostate cancer radiation treatment. Int J Radiat Oncol Biol Phys 74(4):1128–1133
Chung PW et al (2004) On-line aSi portal imaging of implanted fiducial markers for the reduction of interfraction error during conformal radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys 60(1):329–334
Schallenkamp JM et al (2005) Prostate position relative to pelvic bony anatomy based on intraprostatic gold markers and electronic portal imaging. Int J Radiat Oncol Biol Phys 63(3):800–811
Beltran C, Herman MG, Davis BJ (2008) Planning target margin calculations for prostate radiotherapy based on intrafraction and interfraction motion using four localization methods. Int J Radiat Oncol Biol Phys 70(1):289–295
Kupelian PA et al (2005) Intraprostatic fiducials for localization of the prostate gland: monitoring intermarker distances during radiation therapy to test for marker stability. Int J Radiat Oncol Biol Phys 62(5):1291–1296
Poggi MM et al (2003) Marker seed migration in prostate localization. Int J Radiat Oncol Biol Phys 56(5):1248–1251
Gill S et al (2012) Patient-reported complications from fiducial marker implantation for prostate image-guided radiotherapy. Br J Radiol 85(1015):1011–1017
Igdem S et al (2009) Implantation of fiducial markers for image guidance in prostate radiotherapy: patient-reported toxicity. Br J Radiol 82(983):941–945
Alonso-Arrizabalaga S et al (2007) Prostate planning treatment volume margin calculation based on the ExacTrac X-Ray 6D image-guided system: margins for various clinical implementations. Int J Radiat Oncol Biol Phys 69(3):936–943
Nederveen AJ et al (2003) Comparison of megavoltage position verification for prostate irradiation based on bony anatomy and implanted fiducials. Radiother Oncol 68(1):81–88
Langen KM et al (2008) Observations on real-time prostate gland motion using electromagnetic tracking. Int J Radiat Oncol Biol Phys 71(4):1084–1090
Abramowitz M (2012) Noninvasive real-time prostate tracking using a transperineal ultrasound approach. Int J Radiat Oncol Biol Phys 84(3):1
Noel C et al (2009) Prediction of intrafraction prostate motion: accuracy of pre- and post-treatment imaging and intermittent imaging. Int J Radiat Oncol Biol Phys 73(3):692–698
Bittner N et al (2010) Electromagnetic tracking of intrafraction prostate displacement in patients externally immobilized in the prone position. Int J Radiat Oncol Biol Phys 77(2):490–495
Coakley FV, Hricak H (2000) Radiologic anatomy of the prostate gland: a clinical approach. Radiol Clin N Am 38(1):15–30
Zackrisson B, Hugosson J, Aus G (2000) Transrectal ultrasound anatomy of the prostate and seminal vesicles in healthy men. Scand J Urol Nephrol 34(3):175–180
McLaughlin PW et al (2010) Radiographic and anatomic basis for prostate contouring errors and methods to improve prostate contouring accuracy. Int J Radiat Oncol Biol Phys 76(2):369–378
Villeirs GM, De Meerleer GO (2007) Magnetic resonance imaging (MRI) anatomy of the prostate and application of MRI in radiotherapy planning. Eur J Radiol 63(3):361–368
Debois M et al (1999) The contribution of magnetic resonance imaging to the three-dimensional treatment planning of localized prostate cancer. Int J Radiat Oncol Biol Phys 45(4):857–865
Milosevic M et al (1998) Magnetic resonance imaging (MRI) for localization of the prostatic apex: comparison to computed tomography (CT) and urethrography. Radiother Oncol 47(3):277–284
Smith WL et al (2007) Prostate volume contouring: a 3D analysis of segmentation using 3DTRUS, CT, and MR. Int J Radiat Oncol Biol Phys 67(4):1238–1247
Roach M 3rd et al (1996) Prostate volumes defined by magnetic resonance imaging and computerized tomographic scans for three-dimensional conformal radiotherapy. Int J Radiat Oncol Biol Phys 35(5):1011–1018
Rasch C et al (1999) Definition of the prostate in CT and MRI: a multi-observer study. Int J Radiat Oncol Biol Phys 43(1):57–66
van Herk M et al (1998) Automatic registration of pelvic computed tomography data and magnetic resonance scans including a full circle method for quantitative accuracy evaluation. Med Phys 25(10):2054–2067
Gofrit ON et al (2009) The dimensions and symmetry of the seminal vesicles. J Robot Surg 3:29–33
Banner MP, Hassler R (1978) The normal seminal vesiculogram. Radiology 128(2):339–344
Secaf E et al (1991) MR imaging of the seminal vesicles. AJR Am J Roentgenol 156(5):989–994
Villeirs GM et al (2005) Interobserver delineation variation using CT versus combined CT + MRI in intensity-modulated radiotherapy for prostate cancer. Strahlenther Onkol 181(7):424–430
Wallner KE et al (2002) Penile bulb imaging. Int J Radiat Oncol Biol Phys 53(4):928–933
van der Wielen GJ, Mulhall JP, Incrocci L (2007) Erectile dysfunction after radiotherapy for prostate cancer and radiation dose to the penile structures: a critical review. Radiother Oncol 84(2):107–113
Buyyounouski MK et al (2004) The radiation doses to erectile tissues defined with magnetic resonance imaging after intensity-modulated radiation therapy or iodine-125 brachytherapy. Int J Radiat Oncol Biol Phys 59(5):1383–1391
Brown MW et al (2007) An analysis of erectile function after intensity modulated radiation therapy for localized prostate carcinoma. Prostate Cancer Prostatic Dis 10(2):189–193
Macdonald AG et al (2005) Predictive factors for erectile dysfunction in men with prostate cancer after brachytherapy: is dose to the penile bulb important? Int J Radiat Oncol Biol Phys 63(1):155–163
Merrick GS et al (2005) Erectile function after prostate brachytherapy. Int J Radiat Oncol Biol Phys 62(2):437–447
Roach M et al (2004) Penile bulb dose and impotence after three-dimensional conformal radiotherapy for prostate cancer on RTOG 9406: findings from a prospective, multi-institutional, phase I/II dose-escalation study. Int J Radiat Oncol Biol Phys 60(5):1351–1356
Poon DM et al (2013) Dosimetric advantages and superior treatment delivery efficiency of RapidArc over conventional intensity-modulated radiotherapy in high-risk prostate cancer involving seminal vesicles and pelvic nodes. Clin Oncol (R Coll Radiol) 25(12):706–712
Kopp RW et al (2011) VMAT vs. 7-field-IMRT: assessing the dosimetric parameters of prostate cancer treatment with a 292-patient sample. Med Dosim 36(4):365–372
Iori M et al (2008) Dose-volume and biological-model based comparison between helical tomotherapy and (inverse-planned) IMAT for prostate tumours. Radiother Oncol 88(1):34–45
Korreman S et al (2010) The European Society of Therapeutic Radiology and Oncology-European Institute of Radiotherapy (ESTRO-EIR) report on 3D CT-based in-room image guidance systems: a practical and technical review and guide. Radiother Oncol 94(2):129–144
Landoni V et al (2006) A study of the effect of setup errors and organ motion on prostate cancer treatment with IMRT. Int J Radiat Oncol Biol Phys 65(2):587–594
Alasti H et al (2001) Portal imaging for evaluation of daily on-line setup errors and off-line organ motion during conformal irradiation of carcinoma of the prostate. Int J Radiat Oncol Biol Phys 49(3):869–884
Vigneault E et al (1997) Electronic portal imaging device detection of radioopaque markers for the evaluation of prostate position during megavoltage irradiation: a clinical study. Int J Radiat Oncol Biol Phys 37(1):205–212
Moseley DJ et al (2007) Comparison of localization performance with implanted fiducial markers and cone-beam computed tomography for on-line image-guided radiotherapy of the prostate. Int J Radiat Oncol Biol Phys 67(3):942–953
Roeske JC et al (1995) Evaluation of changes in the size and location of the prostate, seminal vesicles, bladder, and rectum during a course of external beam radiation therapy. Int J Radiat Oncol Biol Phys 33(5):1321–1329
Zelefsky MJ et al (1999) Quantification and predictors of prostate position variability in 50 patients evaluated with multiple CT scans during conformal radiotherapy. Radiother Oncol 50(2):225–234
Antolak JA et al (1998) Prostate target volume variations during a course of radiotherapy. Int J Radiat Oncol Biol Phys 42(3):661–672
Beard CJ et al (1996) Analysis of prostate and seminal vesicle motion: implications for treatment planning. Int J Radiat Oncol Biol Phys 34(2):451–458
de Crevoisier R et al (2005) Increased risk of biochemical and local failure in patients with distended rectum on the planning CT for prostate cancer radiotherapy. Int J Radiat Oncol Biol Phys 62(4):965–973
Heemsbergen WD et al (2007) Increased risk of biochemical and clinical failure for prostate patients with a large rectum at radiotherapy planning: results from the Dutch trial of 68 GY versus 78 Gy. Int J Radiat Oncol Biol Phys 67(5):1418–1424
Kupelian PA et al (2008) Impact of image guidance on outcomes after external beam radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 70(4):1146–1150
Hanna SA et al (2012) Role of intra- or periprostatic calcifications in image-guided radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys 82(3):1208–1216
Ryan D et al (2009) Prostate positioning errors associated with two automatic registration based image guidance strategies. J Appl Clin Med Phys 10(4):3071
Bylund KC et al (2008) Analysis of interfraction prostate motion using megavoltage cone beam computed tomography. Int J Radiat Oncol Biol Phys 72(3):949–956
Gayou O, Miften M (2008) Comparison of mega-voltage cone-beam computed tomography prostate localization with online ultrasound and fiducial markers methods. Med Phys 35(2):531–538
Kupelian P et al (2007) Multi-institutional clinical experience with the Calypso System in localization and continuous, real-time monitoring of the prostate gland during external radiotherapy. Int J Radiat Oncol Biol Phys 67(4):1088–1098
Scarbrough TJ et al (2006) Comparison of ultrasound and implanted seed marker prostate localization methods: implications for image-guided radiotherapy. Int J Radiat Oncol Biol Phys 65(2):378–387
Boda-Heggemann J et al (2008) Accuracy of ultrasound-based (BAT) prostate-repositioning: a three-dimensional on-line fiducial-based assessment with cone-beam computed tomography. Int J Radiat Oncol Biol Phys 70(4):1247–1255
Pollack A et al (2013) Randomized trial of hypofractionated external-beam radiotherapy for prostate cancer. J Clin Oncol 31(31):3860–3868
Spratt DE et al (2013) Long-term survival and toxicity in patients treated with high-dose intensity modulated radiation therapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 85(3):686–692
Spratt DE et al (2014) Comparison of high-dose (86.4 Gy) IMRT vs combined brachytherapy plus IMRT for intermediate-risk prostate cancer. BJU Int 114(3):360–367
Pickett B et al (1999) Static field intensity modulation to treat a dominant intra-prostatic lesion to 90 Gy compared to seven field 3-dimensional radiotherapy. Int J Radiat Oncol Biol Phys 44(4):921–929
Pucar D et al (2007) Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor: magnetic resonance imaging and step-section pathology evidence. Int J Radiat Oncol Biol Phys 69(1):62–69
D’Amico AV et al (2008) Androgen suppression and radiation vs radiation alone for prostate cancer: a randomized trial. J Am Med Assoc 299(3):289–295
Jones CU et al (2011) Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med 365(2):107–118
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Japan
About this chapter
Cite this chapter
Scott, M., Orman, A., Pollack, A. (2015). Early Prostate Cancer (T1–2N0M0). In: Nishimura, Y., Komaki, R. (eds) Intensity-Modulated Radiation Therapy. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55486-8_19
Download citation
DOI: https://doi.org/10.1007/978-4-431-55486-8_19
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55485-1
Online ISBN: 978-4-431-55486-8
eBook Packages: MedicineMedicine (R0)