
Abstract
The discovery of stem cells was followed by the discovery of stem cells with the highest numbers in the fat layer, known as adipose-derived stem and progenitor cells. Adult stem cells are undifferentiated, long-lived cells that have the capacity to self-renew and give rise to a differentiated progeny. The author discusses the therapeutic uses of autologous fat and stem cell transfer, the surgical steps of lipotransfer, stem cell use in natural breast augmentation, the therapeutic uses of stem cells, stem cell use in orthopedic surgery, stem cell use in wound healing, stem cells in cardiovascular disease, and FDA recommendations and guidelines.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Stem Cell
- Vascular Endothelial Growth Factor
- Stem Cell Therapy
- Human Dermal Fibroblast
- Stromal Vascular Fraction
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Research into the clinical therapeutic uses of adipose-derived stem cells (ASCs) has skyrocketed in the past 5 years: the discovery that the majority of our stem cells reside not in the bone marrow but in the adipose layer, that the ASCs can be harvested more rapidly with greater quantities, that new cellular technological advancements have become clinically available, and that the understanding of stem and regenerative cell interactions with the tissue microenvironment has made this scientific advancement possible. The previous chapter reviewed the optimal steps in harvesting, processing, purifying, and storing of stem cells. Some of the therapeutic uses of stem cells will be elucidated here.
2 Historical Perspective
Since ASCs reside in the deep adipose layers, extraction (harvesting), processing (preparation), and grafting (administration) of stem cells became closely associated with adipocytes and autologous fat transfer (Fig. 24.1). In 2001, an adipose-derived stem cell harvesting technique was first described by Zuk et al. [1]. Adult stem cells may be isolated from adipose tissue, bone marrow, embryonic tissue, and the blood. The adipose-derived stem cells have the potential for mesodermal, ectodermal, and endodermal differentiation. The adipose tissue contains not only adipogenic progenitor cells but also multipotent stem cells, which can differentiate into fat, bone, cartilage, and types of tissue [1–3]. This ability of stem cells to differentiate into probably any cell in the human body has opened up treatment options. The ability to isolate, purify, and store stem cells as well as grow them and differentiate them in culture makes stem cells the potential therapeutic “magic bullet.”

Microscopy of a population of mature adipocytes
3 Therapeutic Uses of Autologous Fat and Stem Cell Transfer
Autologous fat grafting is used for aesthetic soft tissue volume replacement and for reconstruction of soft tissue defects. Yoshimura et al. revealed that the addition of stem cells to fat prior to transplantation, termed cell-assisted lipotransfer (CAL), has improved fat survival during autologous fat grafting (Fig. 24.2) [4]. The therapeutic uses for CAL include all areas of soft tissue volume replacement that one may consider standard autologous fat transfer:

Cell-assisted lipotransfer converts ASC-poor aspirated fat to ASC-rich fat, which increases the concentration of ASCs by 43 %, improving fat graft survival (From Yoshimura et al. [4])
-
1.
Facial rejuvenation (Fig. 24.3) [5, 6]
Fig. 24.3 
Facial fat grafting using autologous fat transfer with 45 mL total volume replacement with follow-up at 12 months. (a) Preoperative. (b) Postoperative (Courtesy of Robert J Troell, MD, FACS)
-
2.
Facial lipodystrophy [7]
-
3.
Natural breast augmentation (Fig. 24.4) [4, 8–11]
Fig. 24.4 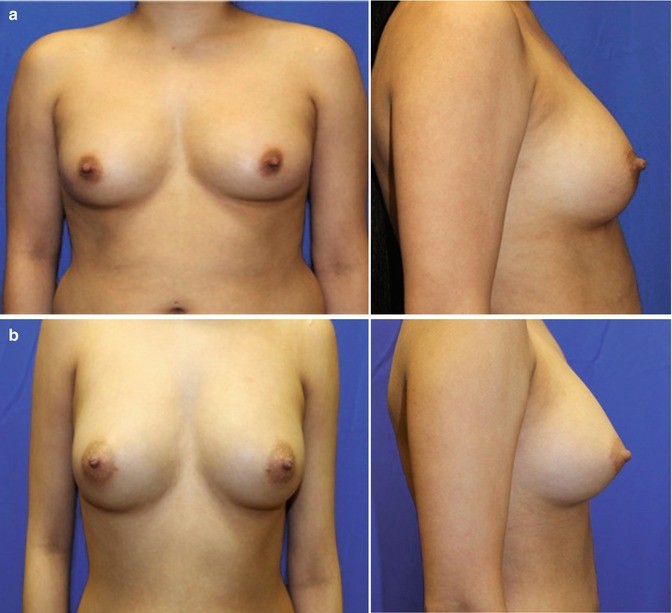
(a) Preoperative. (b) Postoperative after natural breast augmentation using autologous fat and stem cells with 145 mL to right breast and 125 mL to left breast (Courtesy of Robert J Troell, MD, FACS)
-
4.
Breast defect reconstruction [12]
- 5.
-
6.
Gluteal reshaping and augmentation (Fig. 24.5) [15–17]
Fig. 24.5 
(a) Preoperative 29-year-old woman, 67 in., 125 lb. (b) Twelve months postoperative following 650 mL total liposuction fat removal from inner and outer thigh, lower back, abdomen and flanks, gluteal sculpting, and augmentation using autologous fat transfer with 350 mL total volume replacement to central and medial buttock area (Courtesy of Robert J Troell, MD, FACS)
- 7.
-
8.
Liposuction indentation repair
-
9.
Cellulite indentation repair



4 Stem Cell Lipotransfer: Surgical Steps
Autologous fat and stem cell grafting to any face or body part is performed with similar steps (Fig. 24.6):


Autologous facial fat grafting procedural steps: (a) Patient marking. (b) Local anesthesia injection. (c) Incision options (#11 knife blade v. dermal punch). (d) Incision with skin tension. (e) Wetting solution administration. (f) Fat-harvesting instrumentation using LipoKit (MediKan). (g) Closed-syringe harvesting method with suction. (h) Syringe post-centrifugation (3,500 rpms for 4 min). (i) Infranatant removal. (j) Transfer to fat injection syringe. (k) One mm punch for facial incision and supraperiosteal dissection in tear trough area. (l) Subcutaneous injection throughout face (except tear trough). (m) Immediate posttreatment appearance. (n) Four months post-procedure (Courtesy of Robert J Troell, MD, FACS)
-
1.
Anesthesia: general anesthesia, oral sedation with or without intravenous sedation. Facial fat grafting may also use trigeminal sensory nerve blocks.
-
2.
Anatomical donor site and recipient site skin marking.
-
3.
Prepping and sterile draping.
-
4.
Superwet or tumescent technique of wetting solution administration. Options include 60 mL syringe manual technique or powered infiltrators (preferred).
-
5.
Ultrasound energy delivery, VASER mode at 60 % (if desired).
-
6.
Fat harvesting (closed fat collection container or harvesting syringe).
-
7.
Fat processing (washing, filtering, and/or centrifugation).
-
8.
Stem cell isolation and purification from harvested fat (steps dependent on processing system employed).
-
9.
Combining fat cells with stem cells, also possibly, adding platelet-rich plasma (PRP).
-
10.
Fat graft (combined with stem cell and/or PRP) injection.
-
11.
Dressing and compression garment placement.
The discussion of autologous fat transfer to all areas of the body is outside the scope of this chapter. However, since there has been some controversy with fat transfer to the breast and that this has been one of the main areas of clinical research with cell-assisted lipotransfer, a more detailed review will be presented.
5 Stem Cell Use in Natural Breast Augmentation
The area of natural breast augmentation using autologous fat transfer, with or without the addition of stem cells, was certainly delayed by the American Society of Plastic Surgery (ASPS) policy statements: [21]
-
1987: “The committee is unanimous in deploring the use of autologous fat injection in breast augmentation.”
-
1992: “furthermore, women who seek the procedure for breast enlargement are sometimes not informed that much of the injected fat will die, causing scar tissue and calcifications…In a worst case scenario may force exploratory surgery.”
-
2007: “Patients considering breast augmentation need to know that fat grafting for this indication is not recommended at this time.”
-
2009: Investigative committee panel on breast fat grafting – “further studies and consideration warranted.”
-
2012: “autologous fat grafting is an effective option in breast reconstruction following mastectomy while demonstrating moderate to significant aesthetic improvement.”
These policy statements on autologous fat transfer to the breast had some scientific basis, however, in my humble opinion, seemed to be more based on fear of competition from other specialties performing natural breast augmentation versus breast implant placement, where plastic surgeons have dominance. For instance, the most recent policy statement does not mention the indication of natural breast augmentation solely for an aesthetic standpoint in woman desiring to avoid breast implant surgery with its known risk profile. The medical literature and the author’s personal experience regarding procedural risks and revision rates are far greater with breast implant surgery compared to autologous fat transfer. Coleman assisted in lobbying for the use of autologous fat grafting for aesthetic breast augmentation and has published his own experience on the subject [8].
The cause of the breast autologous fat grafting controversy was due to the lower than optimal fat survival rates observed during grafting (fat survival Bircoll, 50 %; Alexander, 65 %; Fulton, 73 %; Ueberreiter, 76 %; Khouri, 90 %). Early breast autologous fat transfer studies resulted in the formation of microcalcifications from fat necrosis (Bircoll, 1.4 %; Miller, 12.5 %; Mitnick, 24.3 %; Khouri 20 %). With improvements in cell transfer viability, the incidence of microcalcifications has diminished.
Additionally, radiologists today can clearly differentiate neoplastic radiologic properties from fat necrosis. The natural breast augmentation technique nearly always places the fat around the breast mound and not into the breast glandular tissue. The multiple views of a mammogram and the 3-dimensional views of breast magnetic resonance imaging make the diagnosis more accurate. Additionally, the improvement in fat viability also has reduced the incidence in microcalcifications.
Rubin et al. [22] compared mammographic changes following fat grafting to the breast with changes seen after breast reduction. Women were treated with fat grafting to the breast (n = 27), including admixing of autologous adipose stem cells with the fat graft, for cosmetic augmentation. Additionally, postsurgical mammograms from reduction mammaplasty patients (n = 23) were compared. Mammograms were performed 12 months after surgery. Eight academic breast-imaging radiologists reviewed each mammogram in a blinded fashion.
Differences in interpretation among individual radiologists were consistently observed; however, differences in abnormality rates were not significant for oil cysts, benign calcifications, and calcifications warranting biopsy. Scarring and masses requiring biopsy were more common in the breast reduction group. Breast-imaging reporting and data system scores were higher after breast reduction.
Compared with reduction mammaplasty, fat grafting to the breast produces fewer radiographic abnormalities with a more favorable breast-imaging reporting and data system score and less aggressive follow-up recommendations by trained and experienced breast radiologists [22]. The results of this study reveal that fat cell transfer to the breast, with or without stem cells, has little risk of causing confusion during mammogram surveillance. It is a good idea to recommend patients seeking natural breast augmentation, and breast implant surgery for that matter, to undergo a preoperative baseline mammogram.
Since fat transfer has been confirmed not to interfere with standard mammogram cancer surveillance, one can concentrate on the outcomes of fat along with stem cell use in cosmetic breast augmentation as well as in breast defect and cancer reconstruction.
A study was designed to evaluate the safety and efficacy of stem cells in breast reconstruction following partial mastectomy and radiation therapy [23]. Twenty-one women were treated with stem cells at least 12 months after radiation therapy was completed. The study concluded the following:
-
1.
The procedure was safe and well tolerated.
-
2.
There was no rejection or adverse immune response.
-
3.
High patient satisfaction rate (79 %).
-
4.
Statistically significant increase in average breast tissue thickness.
-
5.
No change in the breast tissue thickness from 1 month to the end of follow-up.
The first prospective, multicenter clinical trial (RESTORE 2) [24] evaluated ASC enhanced fat used for breast defect reconstruction in patients with T2NoMo invasive breast carcinoma after undergoing breast conservation therapy with or without radiation therapy who were in remission for at least 12 months. Seven clinical sites participated within the European Union including Spain (2), United Kingdom (2), Belgium (2), and Italy (1) with 71 patients treated with ≤150 mL of fat for their breast defects.
Fat harvesting was performed with a syringe collection technique and processed using a closed automated system isolating ASCs and then augmenting using the CAL injection technique. One fraction of the lipoaspirate was added to the Celution® system (Cytori Therapeutics; San Diego, CA) to make the ASC-enriched fat graft. Breast injections were performed using the Celbrush® (Cytori Therapeutics; San Diego, CA), which consists of a stainless steel thumb-controlled syringe adapter designed to provide microdroplet dispersion of graft. Twenty-four patients elected to undergo a second fat and stem cell transfer to the defect area after a 6-month follow-up.
The outcome measures were patient and physician satisfaction, magnetic resonance imaging (MRI) volumetric increase in breast tissue thickness, and an evaluation of side effects/complications. The RESTORE 2 study investigators reported satisfaction with 57 out of 67 patients [24], and 54 out of the 65 patients reported improvement in the breast contour based on blinded MRI anatomical assessment. There were no reported local cancer recurrences and no serious adverse events associated with the ASC-enriched fat transfer procedure; however, cysts were noted in ten patients. This prospective trial demonstrated the safety and efficacy of the treatment of breast cancer conservative treatment defects utilizing ASC-enriched fat transfer.
The availability of tissue banks for the storage of fat and stem cells may change the future of soft tissue augmentation with a transition to ASCs to be used alone as the primary method and/or used for “touch-up” soft tissue volume replacement. The use of cryopreservatives, controlled rates of freezing, and storage in liquid nitrogen has been confirmed to maintain adipocyte and ASC viability [25]. However, most storage banks recommend using the stored adipocytes within 1 year of harvesting, while there appears to be no limit on stem cells.
ASCs have valuable qualities that make ASCs an important avenue for long-term engraftment: a robust cellular nature, the ability for adipogenic differentiation (Fig. 24.7), the ability to differentiate into vascular endothelial and probably vascular mural cells, and the ease to grow and expand extensively in culture. Because of these qualities, current methods of fat transfer for soft tissue augmentation may transition to the combining ASCs in most fat transfer cases. The regenerative cells in adipose tissue are so abundant that the need for culture expansion to reach a therapeutic dose is not necessary; however, stem cells still need to be harvested, processed, and concentrated from the lipoaspirate [26].

Differentiation of a stem cell to adipocyte
ASCs can differentiate into adipocytes in vitro; the younger adipocytes are smaller during their first 2 months after differentiation than mature cells and are more robust, which may allow less traumatic implantation through smaller cannulas. Using this tissue engineering approach for fat transfer may heighten the reliability of grafts with improved aesthetic appearance and lowering the incidence of touch-up procedures.
And with the addition of platelet-rich plasma, ASCs have the flexibility to be injected into the dermis for a combined synergy in skin rejuvenation. If microdermabrasion and dermal microneedling are performed initially, the rejuvenation treatment could be done with only the topical application of ASCs and PRP, saving the patient injections.
A joint task force of the American Society for Aesthetic Plastic Surgery (ASAPS) and the American Society of Plastic Surgeons (ASPS) formatted a position statement on the use of “stem cells” in aesthetic surgery [27]. This policy statement was based on a systematic review of the peer-reviewed literature and concluded that “while there is tremendous potential for the future use of stem cells in aesthetic surgical procedures, the scientific evidence and other data are very limited in terms of assessing the safety or efficacy of stem cell therapies in aesthetic medicine.” The remaining part of this manuscript will touch on only a fraction of the current peer-reviewed journal articles published in the medical literature regarding the use of stem cells and their mechanism of action in a multitude of fields of medicine.
Based on the current state of knowledge, the task force made the following recommendations to ASAPS/ASPS members and their patients:
-
Terms such as “stem cell therapy” or “stem cell procedure” should be reserved to describe those treatments or techniques where the collection, concentration, manipulation, and therapeutic action of the stem cells are the primary goal, rather than a passive result, of the treatment. For example, standard fat grafting procedures that do transfer some stem cells naturally present within the tissue should be described as fat grafting procedures, not stem cell procedures.
-
The marketing and promotion of stem cell procedures in aesthetic surgery are not adequately supported by clinical evidence at this time.
-
While stem cell therapies have the potential to be beneficial for a variety of medical applications, a substantial body of clinical data to assess plastic surgery applications still needs to be collected. Until further evidence is available, stem cell therapies in aesthetic and reconstructive surgery should be conducted within clinical studies under Institutional Review Board approval, including compliance with all guidelines for human medical studies.
-
The collection and reporting of data on outcomes and safety by any physician performing stem cell therapies are strongly encouraged in order to advance the knowledge and science of stem cells.
-
Stem cell-based procedures should be performed in compliance with FDA regulatory guidelines. If devices are employed that are subject to regulation by the FDA, surgeons should use these devices with appropriate approval in place, especially when used for investigational purposes.
-
Patients are advised to seek consultation for aesthetic procedures by a surgeon certified by the American Board of Plastic Surgery. These physicians are able to properly evaluate a patient’s concerns and offer a wide range of safe solutions. Extreme caution should be exercised when a physician is promising results from any treatment that sound too good to be true.
These recommendations are from two societies and are not considered dictum. Physicians promoting stem cell augmented autologous fat transfer or stem cell administration alone, many wish to follow some or all of these recommendations. Scientific laboratory and clinical research will guide the future of therapeutic indications for stem cell use.
6 Therapeutic Uses of Stem Cell
A number of clinical trials using freshly isolated or cultured ASCs are ongoing in more than ten countries, most in Europe and Asia.
The therapeutic uses of stem cells include:
-
1.
Treatments for bone defects (autologous fresh ASCs) [28]
-
2.
Rectovaginal fistula (autologous cultured ASCs) [29]
-
3.
Graft-versus-host disease (non-autologous ASCs) [30]
-
4.
General orthopedic surgery (fractures and articular joint disease) [31–34]
- 5.
-
6.
Breast reconstruction s/p partial mastectomy and radiation therapy [25]
-
7.
Radiation necrosis
-
8.
Wrinkle treatment
-
9.
Acute myocardial infarction and chronic cardiovascular disease [38, 39].
-
10.
Liver insufficiency
-
11.
Nonalcoholic chronic liver disease
-
12.
Stress urinary incontinence
-
13.
Renal ischemia
7 Stem Cell Use in Orthopedic Surgery
In the 1990s, stem cells were combined in processes for the repair of cartilage, bone, tendon, muscle, and other connective tissues. The field of stem cells in orthopedic surgery has expanded to nearly every aspect of the specialty.
Bone matrix (BM) is an acellular, cross-linked cancellous bone graft, often porcine derived. Because it is a biologic tissue, it has advantages over synthetic materials. Arca et al. evaluated the potential for BM to support the growth and differentiation of human mesenchymal stem cells (ASCs) in vitro [31]. Long-term growth analysis by confocal imaging and histology demonstrated ASCs survived on the bone matrix scaffold in culture. The authors conclusion was that bone matrix had osteo-inductive capabilities and when supplemented with osteogenic stimulants (growth factors) supported osteogenesis by ASCs.
ASCs’ influence in fracture healing was studied in an immunodeficient rat femur nonunion fracture model [32]. Local transplantation of human ASCs in a rat femur fracture revealed both radiographic and histological evidence promoting fracture healing with significant improvement of biomechanical function at the fracture site compared with local transplantation of human fibroblasts. Histological capillary density and laser Doppler blood perfusion imaging were significantly greater in the stem cell group compared to the human fibroblast-treated group. These findings suggest stem cells augmented angiogenesis and bone tissue formation.
Rat growth factors (bone morphogenetic protein-2 (BMP-2), vascular endothelial growth factor (VEGF), and angiopoietin-1) in the tissue surrounding the fracture were most upregulated in the human ASC group. They also showed that the presence of BMP-2 or VEGF activated the proliferation and migration of ASCs in vitro. These results indicate that human ASCs interacted with resident cells stronger than other cells and promoted fracture healing more effectively. Additionally, human-specific antibody immunohistochemistry revealed direct differentiation of human ASCs into osteoblasts and endothelial cells in the newly formed rat callus. They deduced that the grafting of ASCs into fractures may become a useful strategy for cell-based bone regeneration [32].
This data revealed that growth factors stimulated stem cell function. ASCs could differentiate into vascular endothelial cells promoting increase tissue blood supply and ASCs differentiate into osteoblasts, which produce new bone formation. The bone formation requires a scaffold or bone matrix, growth factors, and stem cells themselves for this process to occur.
Atesok et al. [33] evaluated the effects of a type of stem cell, the local endothelial progenitor cell (EPC), on bone regeneration. A segmental bone defect was created in a rat femur and fixed with a mini-plate in both the stem cell and control group with the animals sacrificed at 1, 2, 3, and 10 weeks postoperatively. Healing was evaluated with radiographic, histological, and quantitative microcomputed tomography (micro-CT) scans. At 10 weeks, all the animals in the EPC-treated group had complete union, while none in the control group achieved union. Histological evaluation revealed that specimens from EPC-treated animals had abundant new bone and vessel formation compared to that in controls. Micro-CT assessment showed significantly improved parameters of bone volume, bone volume density, trabecular number, thickness, and spacing, bone surface, and bone-surface-to-bone-volume ratio in the EPC group. Atesok et al. [33] concluded that there was significantly enhanced bone regeneration with the presence of the local endothelial progenitor cells.
In a follow-up study [34], the same group evaluated the effects of the local endothelial progenitor cell (EPC) on the microarchitecture and biomechanical properties of a segmental bone defect in a rat model. New bone formation was assessed with radiographs, microcomputed tomography, and biomechanical testing. They showed that stem cells significantly enhanced fracture healing with superior radiographic bone formation [34].
These studies confirm the importance of a subset of stem and progenitor cells that differentiate into blood vessels. Another subset of stem cells can differentiate into other tissues cells, such as osteoblasts, in a specific cellular environment with local cellular and growth factor influences.
8 Stem Cell Use in Wound Healing
Dermal wound healing is a highly coordinated process, where fibroblasts interact with surrounding cells and produce extracellular matrix (ECM), glycoproteins, and various cytokines. After tissue injury, fibroblasts migrate into the initial fibrin-based matrix and proliferate and begin the production of ECM and collagen. Wound edges reapproximate through the wounds contractile properties.
Histological features of photo-aged skin show marked alterations of ECM composition. The collagenous component of dermal ECM is responsible for the strength and resiliency of skin and is a key factor involved in sun-induced skin pathologic changes. In photo-aged human skin, the precursors of type I and III collagen are significantly reduced in the papillary dermis and their reduction has been shown to correlate with the clinical severity of photo-aging. This reduction results from a combination of reduced pro-collagen biosynthesis and increased actions of cellular collagenase, also known as matrix metalloproteinase (MMP), involved in the breakdown of extracellular matrix.
Few studies have researched the effects of ASCs on fibroblasts, which play a key role in wound healing, scar formation, and solar skin damage. Kim et al. [35] investigated the possible roles of ASCs in the skin wound-healing process, specifically related to human dermal fibroblast (HDF) activation with cellular migration, proliferation, and collagen synthesis. In addition, secretion of type I collagen was examined by measuring messenger ribonucleic acid (mRNA) levels of ECM proteins and the effect on the migration activity of HDFs was tested in an in vitro wound-healing model. They also studied the effect of ASCs on wound size and skin re-epithelialization in an animal model. The results revealed that ASCs promoted human dermal fibroblast (HDF) proliferation, not only by cell-to-cell direct contact, but also by paracrine activation through secretory factors. Interestingly, this proliferative effect was completely abolished by boiling, suggesting that it was due to a specific receptor/ligand interaction [37]. In this study, ASCs were superior to HDFs in promoting HDF proliferation and in upregulation of type I collagen secretion by fibroblasts. ASC enhanced HDF proliferation in a dose-dependent manner. ASCs enhanced the secretion of type I collagen in HDFs by regulating the mRNA levels of extracellular matrix (ECM) proteins: upregulation of collagen type I, type III, and fibronectin and downregulation of the MMP-1 collagenase enzyme. The concentrations of type I collagen and fibronectin were found to be at least 1,000-fold higher than those of other growth factors. In an animal model, ASCs significantly reduced the wound size and accelerated the re-epithelialization from the wound edge.
Kim et al. [36] noted that ASCs were found to produce various growth factors, such as platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), and keratinocyte growth factor (KGF), in addition to the previously reported growth factors: fibroblast growth factor (bFGF), transforming growth factor (TGF-β), hepatocyte growth factor (HGF), and vascular endothelial growth factor (VEGF). These cytokines operate in concert with other regulatory proteins. For fibroblasts, the main implicated cytokines are PDGF, TGF-β1, FGF, as well as interleukins (IL)-1β, 6, and 10. Among these, PDGF and TGF-β1 may play a key role in the wound-healing process. The conclusions of this study were that ASCs promote dermal fibroblast proliferation by cell-to-cell contact and by paracrine activation through secretory factors. ASCs enhanced the secretion of type I collagen in fibroblasts and stimulated the migration of fibroblasts. Additionally, ASCs significantly reduced the wound size accelerating re-epithelialization [35]. This data suggests that ASCs can be used for the treatment of solar-damaged skin and can be used to improve wound healing.
Amazingly, stem cells can influence adjacent cells, in this case fibroblasts, to migrate, proliferate, and secrete substances. The cellular influence is from both direct cellular contact and by growth factor secretion.
Blanton et al. [36] examined the efficacy of ASCs, when supplied either alone or along with platelet-rich plasma, to improve wound healing. A porcine full-thickness wound model was used to compare six topical treatments: platelet-poor plasma, platelet-rich plasma, autologous adipose stem cells plus platelet-poor plasma, autologous adipose stem cells plus platelet-rich plasma, allogeneic adipose stem cells containing green fluorescent protein plus platelet-poor plasma, and saline (control). There was no significant difference in the re-epithelialization rate; however, treatments containing ASCs demonstrated increased capillary densities. Wound cosmesis was improved with the combination of ASCs with platelet-rich plasma. ASC samples had approximately seven-fold higher levels of vascular endothelial growth factor. Transgenic green fluorescent protein combined with ASCs became incorporated near new blood vessels [36]. They concluded that ASCs enhanced the healing process in association with growth factors present in platelet-rich plasma. Additionally, the perivascular ASC localizations suggest a function in enhancing blood supply through providing physical and paracrine support to newly forming vessels. This study reiterates that the improved blood supply in the presence of stem cells is directly related to vascular endothelial growth factor secretion.
The inflammatory response in wound areas induces oxygen deficiency. The objectives of the study by Lee et al. [37] were as follows: (1) does hypoxia alter the wound-healing function of adipose-derived stem cells and (2) what are the factors responsible for wound healing? Hypoxia enhanced the proliferation of ASCs. The conditioned medium of ASCs harvested under hypoxic conditions significantly promoted collagen synthesis and the migration of human dermal fibroblasts, compared with the cellular milieu from a normal oxygen environment. Hypoxia upregulated angiogenic growth factors, including vascular endothelial growth factor (VEGF), and basic fibroblast growth factor (bFGF) as determined by mRNA and protein measurements. To test the effects of the growth factors in the healing wounds in an animal model, their effects were inhibited by using neutralizing antibodies to VEGF and bFGF. This reversed the migration of human dermal fibroblasts. In summary, these study results infer that hypoxia increases the proliferation of ASCs and the hypoxia enhances the wound-healing function of ASCs by upregulating the secretion of VEGF and bFGF [37].
9 Stem Cells in Cardiovascular Disease
Knowledge of the mechanisms of cardiac cell regeneration is critical for the identification of medical treatment strategies aimed at restoring function and structural integrity of an acutely injured heart as with acute myocardial ischemia or a chronic failing heart as in congestive heart failure. Although a mass of research has been compiled, there is still debate on the role of stem cells from the bone marrow and in the heart itself in terms of both normal cellular regeneration as well as healing mechanisms from injury. However, most believe that the heart is no longer considered a postmitotic organ, but it’s a continually self-renewing organ. Anversa et al. [40] has published an excellent review of the data and controversies regarding the status of stem cells and the heart.
There is a debate over how rapid cardiac cells are turned over. Studies support both low levels of myocyte turnover [41–45] as well as those revealing a high rate of myocyte renewal [46–52]. Myocyte apoptosis in the normal human heart involves at least an estimated 1 in 100,000 cells [53], and since this apoptosis lasts about 4 h to completion, it is calculated that 0.006 % of myocytes are lost per day for a decrease of 2.2 % of myocytes per year. This myocyte apoptosis increases linearly with age. It is estimated that over 30 years, approximately 95 % of the original ventricular myocytes are regenerated due to this cellular loss [52].
The other debate is the source or origin of new cardiomyocytes. They are suggested to be from (1) cardiac stem cells (CSC), (2) bone marrow or hematopoietic stem cells (HSC), or (3) dedifferentiation of myocytes. The dedifferentiated myocytes have been shown to acquire an immature cell phenotype and then reenter the cell cycle and divide [54–57].
The heart harbors multipotent c-kit-positive cardiac stem cells [58, 59] and other progenitor cell classes [60–62] capable of differentiating into cardiomyocytes and coronary vessels. There is a significant amount of data to support the conclusion that the adult heart possesses a class of c-kit-positive CSCs that modulate organ homeostasis and they are also involved in tissue repair. During physiological myocardial aging in humans, it appears that differentiation of c-kit-positive CSCs replaces the entire myocyte compartment approximately 12 times [52].
There are numerous populations of cardiac stem cells that have been discovered: (1) c-kit-positive CSCs [15], (2) ISL-1 progenitors (restricted to the embryonic fetal heart), (3) epicardial progenitors, (4) side population progenitors, (5) seal progenitors, (6) progenitor-generating cardiospheres, and (7) mesenchymal stem cells [59–61]. However, instead of being resident stem cells in the heart, others suggest that the undifferentiated stem cells may reside in distant organs, mainly the bone marrow. It is postulated by some that they continuously translocate to the adult heart, where they assume specific functions, leading to the preservation of tissue homeostasis.
Bone marrow stem cells have been shown to differentiate into (1) cardiomyocytes, (2) vascular endothelial cells, and (3) smooth muscle cells, presumably of the vascular wall. The bone marrow has numerous classes of stem cells, including the c-kit-positive HSCs as well as mononuclear bone marrow cells. HSCs may play a role in cardiomyocytes and coronary vessels regeneration following injury [63, 64].
Activation and myocyte differentiation of c-kit-positive CSCs occur in response to myocardial infarction (MI) and chronic aortic stenosis in humans [47, 49, 50]. The argument against the presence of resident CSCs and their role to differentiate into myocytes is that spontaneous cardiac repair does not occur after infarction and that necrotic tissue is not restored by intact myocardium, instead the healing process results in a thick scar [65].
Different classes of hematopoietic stem cells have been used in phase 1 and phase 2 clinical trials, which yielded positive results. This prompted the current European phase III ongoing trial using HSCs in patients with acute and chronic ischemic cardiomyopathy [38, 39]. The exact cellular and growth factor interaction that results in cardiomyocyte and coronary vessel growth is unknown. However, some believe that HSCs secrete cytokines that activate endogenous progenitors, which are actually responsible for the repair process [66]. Conversely, others suggest that HSCs acquire the myocyte lineage and differentiate into functionally competent cardiomyocytes [63, 64].
Endothelial progenitor cells, mononuclear bone marrow cells, mesenchymal stromal cells, and CD34-positive cells have been administered to patients suffering from acute myocardial infarction or chronic ischemic cardiomyopathy [38, 39]. Based on meta-regression analyses, these interventions have had positive outcomes, documenting the safety and the beneficial effects on cardiac function. An average significant increase in ejection fraction of 3 % points has been reported [38, 39], although studies have also been published that indicate no changes in ejection fraction [66–71].
Aging causes a progressive decrease in the number of CSCs with high regenerative potential and an increase in the pool of stem cells with minimal or no differentiation potential [52, 72]. The loss of CSC function with aging is suspected to be due to an imbalance between factors promoting growth and survival and factors enhancing oxidative stress, telomere attrition, and apoptosis [40].
Insulin-like growth factor (IGF-1) receptor system and the renin-angiotensin system (RAS) have a critical role in CSC replication, differentiation, and death. The IGF1/IGF1 receptor induces CSC division, upregulates telomerase activity, maintains telomere length, hinders replicative senescence, and preserves the population of functionally competent CSCs in animals [73] and humans [72]. The expression of IGF-1 receptors and the synthesis of IGF-1 are decreased in aging CSCs, possibly diminishing the ability of IGF-1 to activate cell proliferation and interfere with oxidative damage and telomeric shortening [74].
Experimentally, remarkable levels of myocardial regeneration after infarction have been obtained with c-kit-positive HSCs [63, 64], but not with mononuclear bone marrow cells [75]. Presently, it is unknown if CSCs have the same effectiveness as HSCs in reconstituting the necrotic and scarred tissue or whether limitations exist in CSC growth and HSC transdifferentiation, resulting in inadequate restoration of the damaged myocardium.
Administration of freshly isolated adipose-derived regenerative cells immediately after an acute myocardial infarction (AMI) improves left ventricular (LV) function and myocardial perfusion in animal models [76, 77]. The postulated mechanism of stem cell therapy in AMI is through paracrine release of antiapoptotic, immunomodulatory, and angiogenic factors. These factors stimulate angiogenesis in the infarct border zone and also stimulate cardiomyocyte salvage. These cellular and growth factor interactions result in reduced infarct scar formation and adverse cardiac remodeling [76–78].
Lipoaspirates contain numerous types of cells, with the stem cells being the most significant in this discussion:
-
Adipocytes
-
Adult mesenchymal stem cells
-
Endothelial cells
-
Endothelial progenitor cells
-
Vascular smooth muscle cells
-
Perivascular cells
-
Tissue resident macrophages
-
Lymphocytes
The amount of mesenchymal stem cells in freshly isolated adipose tissue lipoaspirate is about 2,500-fold greater than that of freshly aspirated bone marrow, which makes cell culture unnecessary to generate therapeutically sufficient cells [79]. Approximately 20–40 million cells can be isolated from a typical lipoaspirate (200 g of fat) and prepared for reinjection within 2 h [80]. This allows adipose-derived stem cell therapy to be a viable treatment option in AMI patients, since the harvesting, processing, and administration of the stem cells can be carried out within hours of the ischemic injury.
The APOLLO trial is a randomized, double-blind, placebo-controlled, phase I/IIa study sponsored by Cytori Therapeutics designed to assess the treatment safety, feasibility, and efficacy of intracoronary infusion of ASCs in the acute phase of a large ST-segment elevation acute myocardial infarction (STEMI) [80]. Patients underwent a liposuction procedure of the periumbilical region, after which ASCs were isolated using the Cytori Celution device (Cytori Therapeutics Inc., San Diego, California). ASCs were infused into the coronary occluded vessel within 24 h of presentation while being carefully monitored for coronary flow-related side effects.
Feasibility endpoints were defined as the change in left ventricular ejection fraction (LVEF), infarct size as determined by delayed enhancement-cardiac magnetic resonance imaging, and perfusion defect as assessed by sestamibi-single-photon emission computed tomography (MIBI-SPECT) with follow-up clinically and angiographically at 6 months posttreatment. Patients (n = 14) were randomized 3:1 to receive an intracoronary infusion of either 20 million ASCs (n = 10) or placebo solution (n = 4) in the occluded coronary artery.
The observations of the APOLLO trial at the 6-month follow-up were the following: (1) liposuction to harvest ASCs in the acute phase of an AMI is safe and feasible; (2) intracoronary infusion of freshly isolated ASCs is safe and did not result in an alteration of coronary flow; (3) no serious adverse effects were related to the ASC therapy; and (4) ASC infusion resulted in a trend toward improved cardiac function with an improved LVEF by 4 %, an improvement of the perfusion defect by 6 %, and a 52 % reduction of myocardial scar formation (Fig. 24.8).

Infarct size and perfusion defect in APOLLO patients (From Houtgraaf et al. [80]). (a) The percentage of the left ventricle (LV) infarcted improved significantly in adipose tissue-derived regenerative cell (ADRC)-treated patients from baseline (open column) to the 6-month follow-up time point (solid column; example to the right, red arrows depict (top right) infarct at baseline and (bottom right) 6-month follow-up), with no improvement in placebo patients. (b) A significant improvement of the perfusion defect was seen in ADRC-treated patients (right, red arrows) from baseline (open column) to the 6-month follow-up time point (solid column) compared with a deterioration in placebo patients
There is an ongoing ADVANCE study, initiated in 2011 that is a multicenter, prospective, randomized, placebo-controlled phase IIb/III clinical trial that will assess the safety and efficacy of an intracoronary infusion of two doses of ASC in up to 375 patients with an STEMI. Personal communication with Cytori Therapeutics gives the estimated completion of the study some time after the summer of 2014. Hopefully, the results of this study will mimic the positive cardiac function outcomes observed with stem cell therapy like the APOLLO study.
Tissue regeneration and healing requires an adequate blood supply. Improved tissue blood supply is almost certainly from perivascular ASCs providing physical and paracrine support to newly forming vessels [36]. The improved blood supply in the presence of stem cells is directly related to vascular endothelial growth factor (VEGF) secretion. Other studies have shown that stem cells actually differentiate into vascular endothelial cells and probably vascular mural cells [81, 82]. Additionally, hypoxia increases the proliferation of ASCs and enhances the wound-healing function of ASCs by upregulating the secretion of VEGF and bFGF [37, 83, 84].
10 Federal Food and Drug Administration (FDA) Recommendations and Guidelines
The harvesting, processing, and administration of “autologous” fat or stem cell-enhanced fat grafting using collagenase from a patient at a “single” procedure do “not” require FDA approval. However, the clinical use of stem cells may be regulated by the FDA. The main determinant to be regulated is “if the fat is more than minimally manipulated.” FDA (21 CFR Parts 16; 1,270; and 1,271) regards cells cultured as more than minimally manipulated cells. Cultured ASCs are known to show a distinct phenotype to freshly isolated ASCs [30]. If the FDA determines that the fat is more than minimally manipulated before replantation or injection, then it classifies the stem cell graft as a drug with the same guidelines and regulations of any medication.
The specific government guidelines are from § 1271.10 and answer a number of specific questions. Are my human cells, tissue, and cellular-based products (HCT/Ps) regulated under section 361 of the PHS Act and the regulations in this part, and if so what must I do?
-
(a)
An HCT/P is regulated solely under section 361 of the PHS Act and the regulations in this part if it meets all of the following criteria:
-
1.
The HCT/P is minimally manipulated;
-
2.
The HCT/P is intended for homologous use only, as reflected by the labeling, advertising, or other indications of the manufacturer’s objective intent;
-
3.
The manufacture of the HCT/P does not involve the combination of the cells or tissues with another article, except for water, crystalloids, or the sterilizing, preserving, or storage agent, provided that the addition of water, crystalloids, or the sterilizing, preserving, or storage agent does not raise new clinical safety concerns with respect to the HCT/P; and
-
4.
Either:
-
(i)
The HCT/P does not have a systemic effect and is not dependent upon the metabolic activity of living cells for its primary function; or
-
(ii)
The HCT/P has a systemic effect or is dependent upon the metabolic activity of living cells for its primary function, and
-
(a)
Is for autologous use;
-
(b)
Is for allogeneic use in a first-degree or second-degree blood relative; or
-
(c)
Is for reproductive use.
-
(a)
-
(i)
-
1.
-
(b)
If you are a domestic or foreign establishment that manufactures an HCT/P described in paragraph (a) of this section:
-
1.
You must register with the FDA; 1
-
2.
You must submit to FDA a list of each HCT/P manufactured; and
-
3.
You must comply with the other requirements contained in this part. [66 FR 5466, Jan, 19, 2001, as amended at 69 FR 68681, Nov. 24, 2004]
-
1.
The key for those performing stem cell clinical and research use in the United States are the following exceptions, since cases are usually performed on one patient as an autologous procedure at one setting and procedure location:
§ 1271.15 Are there any exceptions from the requirements of this part?
- (a)
You are not required to comply with the requirements of this part if you are an establishment that uses human cells, tissue and cellular and tissue-based products (HCT/Ps) solely for nonclinical scientific or educational purposes.
- (b)
You are not required to comply with the requirement of this part is you are an establishment that removes HCT/Ps from an individual and implants such HCY/Ps into the same individual during the same surgical procedure.
- (c)
You are not required to comply with the requirements of this part is you are a carrier who accepts, receives, carries, or delivers HCT/Ps in the usual course of business as a carrier..
- (d)
You are not required to comply with the requirement of this part is you are an establishment that does not recover, screen, test, process, label…
The following is a list of FDA guidelines or recommendations to be followed with stem cell harvesting, processing, and administration, which concentrates on current good tissue practice (cGTP) and current good manufacturing practices (cGMP).
-
1.
Validate and document aseptic operating processes and procedures to prevent microbiological contamination of the stromal vascular fraction (SVF) protocols to prevent contamination.
-
2.
The drug product (SVF) requires the identity, strength, quality, and purity to be represented.
-
3.
Document how the reagent, in this case coagulase, is prepared and used.
-
4.
Note previous studies using the same technique for fat and stem cell harvesting, separation, and proving cellular viability.
-
5.
Document resting or waiting time from fat harvesting until administration.
-
6.
Document specific harvesting techniques, such as the type and size of ultrasonic probe and the ultrasound settings, to include amount of energy delivered and length of time for ultrasonic cavitation.
-
7.
Document fat processing times and settings, for instance, the revolutions per minute (RPMs) or G forces and time of centrifuging specimen.
-
8.
Note amount of any solutions added to the fat during harvesting or processing.
-
9.
Note time between adding a reagent and further processing or administration of the sample.
-
10.
Validation and established working parameters for the flow cytometer for cell counting.
-
11.
Quality control analysis, perhaps using another laboratory to corroborate the results.
-
12.
Before reinjection, describe the process of receipt of the sample, noting the sample identification, storage and handling technique, and length of time stored.
-
13.
Record lot numbers of operating room and laboratory supplies and equipment used in the harvesting and processing steps.
-
14.
Noting the specific technique of injection or method of combining fat, stem cells, and platelet-rich plasma and any other additives.
-
15.
Follow-up actions for the postoperative patient to ensure no complications as well as assessing outcome measures.
-
16.
Document temperature of surgical procedure room and the temperature of any processing or storage.
-
17.
Records of maintenance, cleaning, sanitizing, and inspection of surgical and processing equipment.
11 Conclusions
The discovery of stem cells was followed by the discovery of stem cells with the highest numbers in the fat layer, known as adipose-derived stem and progenitor cells. Adult stem cells are undifferentiated, long-lived cells that have the capacity to self-renew and give rise to a differentiated progeny. The complex interaction of stem cells with fibroblasts, leukocytes and endothelial cells, the microenvironments healing processes with growth factors and cytokines signaling local and distant cells, stem cells dividing and differentiating as well as conducting this symphony of cells are substances working in wonderful ways for the end goal of organism survival.
The upcoming years will be most exciting with the growing knowledge of how to harvest our own body’s miraculous healing powers using stem cells and growth factors in therapeutic uses in all fields of medicine.
References
Zuk PA, Zhu M, Mizuno H, Huang J, Futrell JW, Katz AJ, Benhaim P, Lorenz HP, Hedrick MH. Multi-lineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng. 2001;7(2):211–28.
Zuk PA, Zhu M, Ashjian P, De Ugarte DA, Huang JI, Mizuno H, Alfonso ZC, Fraser JK, Benhaim P, Hedrick MH. Human adipose tissue is a source of multi-potent stem cells. Mol Biol Cell. 2002;13(12):4279–95.
Panetta N, Gupta D, Kwan M, Wan DC, Commons GW, Longaker MT. Tissue harvest by means of suction-assisted or third-generation ultrasound-assisted lipoaspiration has no effect on osteogenic potential of human adipose-derived stromal cells. Plast Reconstr Surg. 2009;124(1):65–73.
Yoshimura K, Sato K, Aoi N, Kurita M, Hirohi T, Harii K. Cell-assisted lipotransfer for cosmetic breast augmentation supportive use of adipose-derived stem/stromal cells. Aesthetic Plast Surg. 2008;32(1):48–55.
Coleman SR. Facial recontouring with lipostructure. Clin Plast Surg. 1997;24(2):347–67.
Guerrerosantos J, Haidar F, Paillet JC. Aesthetic facial contour augmentation with microlipofilling. Aesthet Surg J. 2003;23(4):239–47.
Serra-Renom JM, Fontdevila J. Treatment of facial fat atrophy related to treatment with protease inhibitors by autologous fat injection in patients with human immunodeficiency virus infection. Plast Reconstr Surg. 2004;114(2):551–5.
Coleman SR, Saboeiro AP. Fat grafting to the breast revisited: safety and efficacy. Plast Reconstr Surg. 2007;119(3):775–85.
Spear SL, Newman MK. Fat grafting to the breast revisited: safety and efficacy. Plast Reconstr Surg. 2007;119(3):786–7 (Discussion).
Illouz YG, Sterodimas A. Autologous fat transplantation to the breast: a personal technique with 25 years of experience. Aesthetic Plast Surg. 2009;33(5):706–15.
Ueberreiter K, et al. BEAULI™– a new and easy method for large-volume fat grafts. Handchir Mikrochir. 2010;42(6):379–85.
Spear SL, Wilson HB, Lockwood MD. Fat injection to correct contour deformities in the reconstructed breast. Plast Reconstr Surg. 2005;116(5):1300–5.
Coleman SR. Hand rejuvenation with structural fat grafting. Plast Reconstr Surg. 2002;110(7):1731–44.
Butterwick KJ. Lipoaugmentation for aging hands: a comparison of the longevity and aesthetic results of centrifuged versus noncentrifuged fat. Dermatol Surg. 2002;28(11):987–91.
Cárdenas-Camarena L, Arenas-Quintana R, Robles-Cervantes JA. Buttocks fat grafting: 14 years of evolution and experience. Plast Reconstr Surg. 2011;128(2):545–55.
Roberts 3rd TL, Toledo LS, Badin AZ. Augmentation of the buttocks by micro fat grafting. Aesthet Surg J. 2001;21(4):311–9.
Cardenas Restrepo JC, Muñoz Ahmed JA. Large-volume lipoinjection for gluteal augmentation. Aesthet Surg J. 2002;22(1):33–8.
Veber Jr M, Mojallal A. Calf augmentation with autologous tissue injection. Plast Reconstr Surg. 2010;125(1):423–4; author reply 424–5.
Mojallal A, Veber M, Shipkov C, Ghetu N, Foyatier JL, Braye F. Analysis of a series of autologous fat tissue transfer for lower limb atrophies. Ann Plast Surg. 2008;61(5):537–43.
Erol OO, Gürlek A, Agaoglu G. Calf augmentation with autologous tissue injection. Plast Reconstr Surg. 2008;121(6):2127–33.
American Society of Plastic Surgeons (ASPS) website, Policy statements, 2012.
Rubin JP, Coon D, Zuley M, Toy J, Asano Y, Kurita M, Aoi N, Harii K, Yoshimura K. Mammographic changes after fat transfer to the breast compared with changes after breast reduction: a blinded study. Plast Reconstr Surg. 2012;129(5):1029–38.
Kitamura K, Mori M, Sugimachi K. Stem cell augmented reconstruction: a new hope for reconstruction after breast conservative therapy, 2007. 30th annual San Antonio breast cancer symposium (poster presentation), San Antonio, 13–17 Dec 2007.
Pérez-Cano R, Vranckx JJ, Lasso JM, Calabrese C, Merck B, Milstein AM, Sassoon E, Delay E, Weiler-Mithoff EM. Prospective trial of adipose-derived regenerative cell (ADRC)-enriched fat grafting for partial mastectomy defects: the RESTORE-2 trial. Eur J Surg Oncol. 2012;38(5):382–9.
Moscatello DK, Dougherty M, Narins RS, Lawrence N. Cryopreservation of human fat for soft tissue augmentation: viability requires use of cryoprotectant and controlled freezing and storage. Dermatol Surg. 2005;31(11 Pt 2):1506–10.
Fraser J, Wulur I, Alfonso Z, Hedrick M. Fat tissue: an underappreciated source of stem cells for biotechnology. Trends Biotechnol. 2006;24(4):150–4.
American Society of Aesthetic Plastic Surgery (ASAPS) website, policy statement on stem cells, 2012
Eto H, Suga H, Aoi N, Kato H, Araki J, Doi K, Higashino T, Yoshimura K. Adipose injury-associated factors activate adipose stem/stromal cells, induce neo-angiogenesis, and mitigate hypoxia in ischemic tissues. Am J Pathol. 2013;178(5):2322–32.
Eto H, Suga H, Matsumoto D, Inoue K, Aoi N, Kato H, Araki J, Yoshimura K. Characterization of adipose tissue structure and cellular components: differences between aspirated adipose tissue and excised adipose tissue. Plast Reconstr Surg. 2009;124(4):1087–97.
Fan Y, Bergmann A. Apoptosis-induced compensatory proliferation. The cell is dead. Long live the cell! Trends Cell Biol. 2008;18(10):467–73.
Arca T, Proffitt J, Genever P. Generating 3D tissue constructs with mesenchymal stem cells and a cancellous bone graft for orthopaedic applications. Biomed Mater. 2011;6(2):025006.
Shoji T, Ii M, Mifune Y, Matsumoto T, Kawamoto A, Kwon SM, Kuroda T, Kuroda R, Kurosaka M, Asahara T. Local transplantation of human multipotent adipose-derived stem cells accelerates fracture healing via enhanced osteogenesis and angiogenesis. Lab Invest. 2010;90(4):637–49.
Atesok K, Li R, Stewart DJ, Schemitsch EH. Endothelial progenitor cells promote fracture healing in a segmental bone defect model. J Orthop Res. 2010;28(8):1007–14.
Li R, Atesok K, Nauth A, Wright D, Qamirani E, Whyne CM, Schemitsch EH. Endothelial progenitor cells for fracture healing: a microcomputed tomography and biomechanical analysis. J Orthop Trauma. 2011;25(8):467–71.
Kim WS, Park BS, Sung JH, Yang JM, Park SB, Kwak SJ, Park JS. Wound healing effect of adipose-derived stem cells: a critical role of secretory factors on human dermal fibroblasts. J Dermatol Sci. 2007;48(1):15–24.
Blanton MW, Hadad I, Johnstone BH, Mund JA, Rogers PI, Eppley BL, March KL. Adipose stromal cells and platelet-rich plasma therapies synergistically increase revascularization during wound healing. Plast Reconstr Surg. 2009;123(2 Suppl):56S–64.
Lee EY, Xia Y, Kim WS, Kim MH, Kim TH, Kim KJ, Park BS, Sung JH. Hypoxia-enhanced wound-healing function of adipose-derived stem cells: increase in stem cell proliferation and up-regulation of VEGF and bFGF. Wound Repair Regen. 2009;17(4):540–7.
Abdel-Latif A, Bolli R, Tleyjeh IM, Montori VM, Perin EC, Hornung CA, Zuba-Surma EK, Al-Mallah M, Dawn B. Adult bone marrow-derived cells for cardiac repair: a systematic review and meta-analysis. Arch Intern Med. 2007;167(10):989–97.
Kang S, Yang YJ, Li CJ, Gao RL. Effects of intracoronary autologous bone marrow cells on left ventricular function in acute myocardial infarction: a systematic review and meta-analysis for randomized controlled trials. Coron Artery Dis. 2008;19(5):327–35.
Anversa P, Kajstura J, Rota M, Leri A. Regenerating new heart with stem cells. J Clin Invest. 2013;123(1):62–70.
Rubart M, Field LJ. Cardiac regeneration: repopulating the heart. Annu Rev Physiol. 2006;68:29–49.
Bergmann O, Bhardwaj RD, Bernard S, Zdunek S, Barnabé-Heider F, Walsh S, Zupicich J, Alkass K, Buchholz BA, Druid H, Jovinge S, Frisén J. Evidence for cardiomyocyte renewal in humans. Science. 2009;324(5923):98–102.
Laflamme MA, Murry CE. Heart regeneration. Nature. 2011;473(7347):326–35.
Vunjak-Novakovic G, Lui KO, Tandon N, Chien KR. Bioengineering heart muscle: a paradigm for regenerative medicine. Annu Rev Biomed Eng. 2011;13:245–67.
Xu H, Yi BA, Chien KR. Shortcuts to making cardiomyocytes. Nat Cell Biol. 2011;13(3):191–3.
Kajstura J, Leti A, Finato N, Di Loreto C, Beltrami CA, Anversa P. Myocyte proliferation in end-stage cardiac failure in humans. Proc Natl Acad Sci U S A. 1998;95(15):8801–5.
Beltrami AP, Urbanek K, Kajstura J, Yan SM, Finato N, Bussani R, Nadal-Ginard B, Silvestri F, Leri A, Beltrami CA, Anversa P. Evidence that human cardiac myocytes divide after myocardial infarction. N Engl J Med. 2001;344(23):1750–7.
Quaini F, Urbanek K, Beltrami AP, Finato N, Beltrami CA, Nadal-Ginard B, Kajstura J, Leri A, Anversa P. Chimerism of the transplanted heart. N Engl J Med. 2002;346(1):5–15.
Urbanek K, Quaini F, Tasca G, Torella D, Castaldo C, Nadal-Ginard B, Leri A, Kajstura J, Quaini E, Anversa P. Intense myocyte formation from cardiac stem cells in human cardiac hypertrophy. Proc Natl Acad Sci U S A. 2003;100(18):10440–5.
Urbanek K, Torella D, Sheikh F, De Angelis A, Nurzynska D, Silvestri F, Beltrami CA, Bussani R, Beltrami AP, Quaini F, Bolli R, Leri A, Kajstura J, Anversa P. Myocardial regeneration by activation of multi potent cardiac stem cells in ischemic heart failure. Proc Natl Acad Sci U S A. 2005;102(24):8692–7.
Kajstura J, Urbanek K, Perl S, Hosoda T, Zheng H, Ogórek B, Ferreira-Martins J, Goichberg P, Rondon-Clavo C, Sanada F, D’Amario D, Rota M, Del Monte F, Orlic D, Tisdale J, Leri A, Anversa P. Cardiomyogenesis in the adult human heart. Circ Res. 2010;107(2):305–15.
Kajstura J, Gurusamy N, Ogórek B, Goichberg P, Clavo-Rondon C, Hosoda T, D’Amario D, Bardelli S, Beltrami AP, Cesselli D, Bussani R, del Monte F, Quaini F, Rota M, Beltrami CA, Buchholz BA, Leri A, Anversa P. Myocyte turnover in the aging human heart. Circ Res. 2010;107(11):1374–86.
Olivetti G, Abbi R, Quaini F, Kajstura J, Cheng W, Nitahara JA, Quaini E, Di Loreto C, Beltrami CA, Krajewski S, Reed JC, Anversa P. Apoptosis in the failing human heart. N Engl J Med. 1997;336(16):1131–41.
Engel FB, Schebesta M, Duong MT, Lu G, Ren S, Madwed JB, Jiang H, Wang Y, Keating MT. p38 MAP kinase inhibition enables proliferation of adult mammalian cardiomyocytes. Genes Dev. 2005;19(10):1175–87.
Kuhn B, del Monte F, Hajjar RJ, Chang YS, Lebeche D, Arab S, Keating MT. Periostin induces proliferation of differentiated cardiomyocytes and promotes cardiac repair. Nat Med. 2007;13(8):962–9.
Berseli K, Arab S, Haring B, Kühn B. Neuregulin l/ErbB4 signaling induces cardiomyocyte proliferation and repair of heart injury. Cell. 2009;138(2):257–70.
Kubin T, Pöling J, Kostin S, Gajawada P, Hein S, Rees W, Wietelmann A, Tanaka M, Lörchner H, Schimanski S, Szibor M, Warnecke H, Braun T. Oncostatin M is a major mediator of cardiomyocyte dedifferentiation and remodeling. Cell Stem Cell. 2011;9(5):420–32.
Beltrami AP, Barlucchi L, Torella D, Baker M, Limana F, Chimenti S, Kasahara H, Rota M, Musso E, Urbanek K, Leri A, Kajstura J, Nadal-Ginard B, Anversa P. Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell. 2003;114(6):763–76.
Bearzi C, Leri A, Lo Monaco F, Rota M, Gonzalez A, Hosoda T, Pepe M, Qanud K, Ojaimi C, Bardelli S, D’Amario D, D’Alessandro DA, Michler RE, Dimmeler S, Zeiher AM, Urbanek K, Hintze TH, Kajstura J, Anversa P. Identification of a coronary vascular progenitor cell in the human heart. Proc Natl Acad Sci U S A. 2009;106(37):15885–90.
Oh H, Bradfute SB, Gallardo TD, Nakamura T, Gaussin V, Mishina Y, Pocius J, Michael LH, Behringer RR, Garry DJ, Entman ML, Schneider MD. Cardiac progenitor cells from adult myocardium: homing, differentiation, and fusion after infarction. Proc Natl Acad Sci U S A. 2003;100(21):12313–8.
Bu L, Jiang X, Martin-Puig S, Caron L, Zhu S, Shao Y, Roberts DJ, Huang PL, Domian IJ, Chien KR. Human ISL1 heart progenitors generate diverse multipotent cardiovascular cell lineages. Nature. 2009;460(7251):113–7.
Chong JJ, Chandrakanthan V, Xaymardan M, Asli NS, Li J, Ahmed I, Heffernan C, Menon MK, Scarlett CJ, Rashidianfar A, Biben C, Zoellner H, Colvin EK, Pimanda JE, Biankin AV, Zhou B, Pu WT, Prall OW, Harvey RP. Adult cardiac-resident MSC-like stem cells with a proepicardial origin. Cell Stem Cell. 2011;9(6):527–40.
Rota M, Kajstura J, Hosoda T, Bearzi C, Vitale S, Esposito G, Iaffaldano G, Padin-Iruegas ME, Gonzalez A, Rizzi R, Small N, Muraski J, Alvarez R, Chen X, Urbanek K, Bolli R, Houser SR, Leri A, Sussman MA, Anversa P. Bone marrow cells adopt the cardiomyogenic fate in vivo. Proc Natl Acad Sci U S A. 2007;104(45):17783–8.
Kajstura J, Rota M, Whang B, Cascapera S, Hosoda T, Bearzi C, Nurzynska D, Kasahara H, Zias E, Bonafé M, Nadal-Ginard B, Torella D, Nascimbene A, Quaini F, Urbanek K, Leri A, Anversa P. Bone marrow cells differentiate in cardiac cell lineages after infarction independently of cell fusion. Circ Res. 2005;96(1):127–37.
Steinhauser ML, Lee RT. Regeneration of the heart. EMBO Mol Med. 2011;3(12):701–12.
Loffredo FS, Steinhauser ML, Gannon J, Lee RT. Bone marrow-derived cell therapy stimulates endogenous cardiomyocyte progenitors and promotes cardiac repair. Cell Stem Cell. 2011;8(4):389–98.
Lunde K, Solheim S, Aakhus S, Arnesen H, Abdelnoor M, Egeland T, Endresen K, Ilebekk A, Mangschau A, Fjeld JG, Smith HJ, Taraldsrud E, Grøgaard HK, Bjørnerheim R, Brekke M, Müller C, Hopp E, Ragnarsson A, Brinchmann JE, Forfang K. Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N Engl J Med. 2006;355(12):1199–209.
Meyer GP, Wollert KC, Lotz J, Steffens J, Lippolt P, Fichtner S, Hecker H, Schaefer A, Arseniev L, Hertenstein B, Ganser A, Drexler H. Intracoronary bone marrow cell transfer after myocardial infarction: eighteen months’ follow-up data from the randomized, controlled BOOST (BOne marrOw transfer to enhance ST-elevation infarct regeneration) trial. Circulation. 2006;113(10):1287–94.
Beitnes JO, Hopp E, Lunde K, Solheim S, Arnesen H, Brinchmann JE, Forfang K, Aakhus S. Long-term results after intracoronary injection of autologous mononuclear bone marrow cells in acute myocardial infarction: the ASTAMI randomised, controlled study. Heart. 2009;95(24):1983–9.
Traverse JH, Henry TD, Ellis SG, Pepine CJ, Willerson JT, Zhao DX, Forder JR, Byrne BJ, Hatzopoulos AK, Penn MS, Perin EC, Baran KW, Chambers J, Lambert C, Raveendran G, Simon DI, Vaughan DE, Simpson LM, Gee AP, Taylor DA, Cogle CR, Thomas JD, Silva GV, Jorgenson BC, Olson RE, Bowman S, Francescon J, Geither C, Handberg E, Smith DX, Baraniuk S, Piller LB, Loghin C, Aguilar D, Richman S, Zierold C, Bettencourt J, Sayre SL, Vojvodic RW, Skarlatos SI, Gordon DJ, Ebert RF, Kwak M, Moyé LA, Simari RD, Cardiovascular Cell Therapy Research Network. Effect of intracoronary delivery of autologous bone marrow mononuclear cells 2 to 3 weeks following acute myocardial infarction on left ventricular function: the LateTIME randomized trial. JAMA. 2011;306(19):2110–9.
Hatzopoulos AK, Gee AP, Taylor DA, Cogle CR, Smith D, Westbrook L, Chen J, Handberg E, Olson RE, Geither C, Bowman S, Francescon J, Baraniuk S, Piller LB, Simpson LM, Loghin C, Aguilar D, Richman S, Zierold C, Bettencourt J, Sayre SL, Vojvodic RW, Skarlatos SI, Gordon DJ, Ebert RF, Kwak M, Moyé LA, Simari RD, Cardiovascular Cell Therapy Research Network (CCTRN). Effect of transendocardial delivery of autologous bone marrow mononuclear cells on functional capacity, left ventricular function, and perfusion in chronic heart failure: the FOCUSCCTRN trial. JAMA. 2012;307(16):1717–26.
D’Amario D, Cabral-Da-Silva MC, Zheng H, Fiorini C, Goichberg P, Steadman E, Ferreira-Martins J, Sanada F, Piccoli M, Cappetta D, D’Alessandro DA, Michler RE, Hosoda T, Anastasia L, Rota M, Leri A, Anversa P, Kajstura J. Insulin-like growth factor- 1 receptor identifies a pool of human cardiac stem cells with superior therapeutic potential for myocardial regeneration. Circ Res. 2011;108(12):1467–81.
Gonzalez A, Rota M, Nurzynska D, Misao Y, Tillmanns J, Ojaimi C, Padin-Iruegas ME, Müller P, Esposito G, Bearzi C, Vitale S, Dawn B, Sanganalmath SK, Baker M, Hintze TH, Bolli R, Urbanek K, Hosoda T, Anversa P, Kajstura J, Leri A. Activation of cardiac progenitor cells reverses the failing heart senescent phenotype and prolongs lifespan. Circ Res. 2008;102(5):597–606.
Torella D, Rota M, Nurzynska D, Musso E, Monsen A, Shiraishi I, Zias E, Walsh K, Rosenzweig A, Sussman MA, Urbanek K, Nadal-Ginard B, Kajstura J, Anversa P, Leri A. Cardiac stem cell and myocyte aging, heart failure, and insulin-like growth factor- 1 overexpression. Circ Res. 2004;94(4):514–24.
Ziebart T, Yoon CH, Trepels T, Wietelmann A, Braun T, Kiessling F, Stein S, Grez M, Ihling C, Muhly-Reinholz M, Carmona G, Urbich C, Zeiher AM, Dimmeler S. Sustained persistence of transplanted proangiogenic cells contributes to neovascularization and cardiac function after ischemia. Circ Res. 2008;103(11):1327–34.
Valina C, Pinkernell K, Song YH, Bai X, Sadat S, Campeau RJ, Le Jemtel TH, Alt E. Intracoronary administration of autologous adipose tissue-derived stem cells improves left ventricular function, perfusion, and remodeling after acute myocardial infarction. Eur Heart J. 2007;28(21):2667–77.
Meliga E, Strem BM, Duckers HJ, Serruys PW. Adipose-derived cells. Cell Transplant. 2007;16(9): 963–70.
Madonna R, Geng YJ, De Caterina R. Adipose tissue-derived stem cells: characterization and potential for cardiovascular repair. Arterioscler Thromb Vasc Biol. 2009;29(11):1723–9.
Fraser J, Schreiber R, Strem B, Zhu M, Alfonso Z, Wulur I, Hedrick MH. Plasticity of human adipose stem cells toward endothelial cells and cardiomyocytes. Nat Clin Pract Cardiovasc Med. 2006;3 Suppl 1:S33–7.
Houtgraaf J, den Dekker W, van Dalen B, Springeling T, de Jong R, van Geuns RJ, Geleijnse ML, Fernandez-Aviles F, Zijlsta F, Serruys PW, Duckers HJ. First experience in humans using adipose tissue–derived regenerative cells in the treatment of patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2012;59(5):539–40.
Miranville A, Heeschen C, Sengenes C, Curat CA, Busse R, Bouloumié A. Improvement of postnatal neovascularization by human adipose tissue-derived stem cells. Circulation. 2004;110(3):349–55.
Planat-Benard V, Silvestre JS, Cousin B, André M, Nibbelink M, Tamarat R, Clergue M, Manneville C, Saillan-Barreau C, Duriez M, Tedgui A, Levy B, Pénicaud L, Casteilla L. Plasticity of human adipose lineage cells toward endothelial cells: physiological and therapeutic perspectives. Circulation. 2004;109(5):656–63.
Rehman J, Traktuev D, Li J, Merfeld-Clauss S, Temm-Grove CJ, Bovenkerk JE, Pell CL, Johnstone BH, Considine RV, March KL. Secretion of angiogenic and antiapoptotic factors by human adipose stromal cells. Circulation. 2004;109(10):1292–8.
Kondo K, Shintani S, Shibata R, Murakami H, Murakami R, Imaizumi M, Kitagawa Y, Murohara T. Implantation of adipose-derived regenerative cells enhances ischemia-induced angiogenesis. Arterioscler Thromb Vasc Biol. 2009;29(1):61–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Troell, R.J. (2014). Current Therapeutic Uses of Adipose-Derived Stem and Regenerative Cells. In: Shiffman, M., Di Giuseppe, A., Bassetto, F. (eds) Stem Cells in Aesthetic Procedures. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-45207-9_24
Download citation
DOI: https://doi.org/10.1007/978-3-642-45207-9_24
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-45206-2
Online ISBN: 978-3-642-45207-9
eBook Packages: MedicineMedicine (R0)