
Abstract
Arthroscopy of the elbow is a relatively recent surgical procedure. Although the first experience described in the literature dates back to the 80s, it is only in the last 15 years that a real and increasing interest can be seen with the inclusion of series of patients [1] and case reports that describe the research for new indications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
8.1 Introduction
Arthroscopy of the elbow is a relatively recent surgical procedure. Although the first experience described in the literature dates back to the 80s, it is only in the last 15 years that a real and increasing interest can be seen with the inclusion of series of patients [1] and case reports that describe the research for new indications.
Intra-articular fractures, by their definition, should be anatomically reduced with extreme accuracy besides being fixed in a stable manner. Arthroscopy has already shown its usefulness in all the joints, by improving the visual field of the joint surface with a minimally-invasive surgical approach.
Besides several case reports in the literature on single fractures, in 2010 Peden et al. [2] performed the first overview on this innovative elbow arthroscopy technique.
The literature shows little scientific evidence about the various indications for arthroscopy of the elbow [3]. These indications include fractures of the radial head, capitellum, trochlea and coronoid.
This chapter addresses the various articular fractures of the elbow, where arthroscopy can nowadays be considered to be a real help. The most important technical aspects are summarized in the light of the literature and the authors’ personal experience.
8.2 Fractures of the Capitulum Humeri and Trochlea (Shear Fracture)
Fractures of the capitulum humeri and trochlea are rare fractures that alter the joint considerably. Even when they are not the result of high energy trauma, they produce severe stiffness and instability in the elbow, if they are not immediately recognized and treated adequately [4].
Various classifications try to group the various morphologies and determine correct treatment algorithms [4–7]. Anatomical reduction is necessary to restore the joint anatomy and the correct tension of the external ligament compartment.
8.2.1 In the Literature
Only a few cases have been described. Feldmann [8] reported two cases of fracture with thin osteochondral fragments (Type 2 fracture, Regan and Morrey). Having ascertained the absence of combined joint instability, this author decided for the simple removal of the fragments by arthroscopy using two approaches, anteromedial and anterolateral.
In 2002 Hardy et al. [9] described reduction and fixation of a Hahn-Steinthal fracture (Type I, Regan and Morrey) achieved arthroscopically, by three different anterolateral approaches. The metal screw, in the subchondral bone must be tilted from lateral to medial on the frontal plane, to avoid the radial nerve.
In 2009 Mitani et al. [10] published a new clinical case with interesting practical advice. By two simple anteromedial and anterolateral portals he used the arthroscope together with the probe to reduce the displaced osteochondral fragment; maintaining the reduction with the probe from the anterolateral portal, he performed fixation with two metal screws in a postero-anterior direction.
The following year Kuriyama et al. [11] went a step further by attempting arthroscopic reduction and fixation (ARIF) of two more complex cases (Type IIIA Dubberley) through two portals (anterolateral and midlateral). In one of the two cases the operation was transformed into open surgery, with an incision of only a few centimeters.
8.2.2 Surgical Technique in Our Experience
From 2000 to 2012 about 48 type I or type II shear fractures were treated in our department by open reduction and internal fixation in 43 cases and by miniopen technique in 5 cases. Our experience with arthroscopic treatment started in 2004 with 3 type III fractures in which we performed fragment removal. In the last 2 years our indications were widened to include strictly selected type I and type II fractures (5 cases).
All the patients underwent preoperative CT of the elbow that is essential to define the fracture morphology and to find medial fracture lines directed towards the trochlea or impacted fractures with osteochondral fragments deformity (so-called elbow Hill-Sachs lesions) which can make the reduction more difficult.
In open surgery, the Kocher approach extended proximally (Extensile Kocher approach) with posterolateral subluxation maneuvers, enables easy control over both the anterior articular compartment (with access to the medial trochlea) and the posterior one (to treat impacted lesions).
The capitellum and trochlea fractures that come to our attention are apparently simple injuries. The CT nearly always shows more medial fracture lines (towards the trochlea) or impact lesions with deformation of the osteochondral fragments (elbow Hill Sachs lesions) that make reduction difficult. In arthroscopic surgery, the fracture must be well visualized in the anterior compartment and the posterolateral gutter (Fig. 8.1). Therefore, if arthroscopic treatment is selected, it is not sufficient in our opinion to perform only the anterior or posterolateral portals, but it is necessary to move the arthroscope several times, before performing fixation, which is a very complex procedure.

Impacted capitellum fracture. Patient aged 36, right elbow. CT scan image of a rare impacted fracture of the posterior face of the capitellum before (a, b) and after (c, d) reduction and fixation. Illustration (e) of the arthroscopic portals used to perform ARIF of the fracture. Exploration of the anterior joint compartment enabled the tip of the intraarticular fractured coronoid to be removed. In order to see the fracture it was necessary to reach the posterolateral gutter placing the scope in the posterolateral portal (f). After reducing the fracture by a probe through the mid-lateral portal (g), fixation has been performed by a temporary percutaneous K-wire (h) and by a resorbable pin (h, i) (RSB implant, hit medica, lima corporate)
It is common to find an intraoperative lesion of the external collateral ligament complex, which, in open surgery can be repaired.
Another aspect to take into consideration is the direction of the fixation. We strongly advocate anterograde fixation, with screws and pins made of polylactic acid. In this direction compression fixation can be performed by sinking the screws under the cartilage plane, perpendicularly to the fracture lines. If the ARIF technique is chosen screws that enter posteriorly are needed in order to avoid risks to the radial nerve.
These reasons suggest restricting arthroscopic treatment of capitellum and trochlea fractures to rare cases that fulfill the following criteria:
-
Type I fractures (Hahn-Steinthal) without posterior depression
-
Type III fractures
-
absence of combined ligament lesions
For the recommended surgical technique the patient is placed in a lateral position. Injected sterile saline solution repeatedly to drain the are also recommended. By these three approaches appropriate joint shaving and lesion planning can be performed, by keeping the arthroscope in the medial portals and working through the two lateral portals. Some authors [12, 13] recommend placing the elbow in extension to facilitate reduction. In our opinion, extension reduces the space to work, so we prefer to keep flexion at 90° and operate with the two lateral approaches. After performing temporary reduction and fixation the fracture must be explored posterolaterally. We also recommended exploring the posterior compartment to drain the hematoma and check for any posterior loose bodies (posterolateral and poster central arthroscopic approaches). By the posterolateral portals it will be thus possible to go down posterolaterally to the posterior humero-radial joint (using the palpator and shaver through the midlateral approach). At this point, by bringing the arthroscope back anteromedially under image intensifier guidance, percutaneous fixation can be performed with cannulated screws, in a posteroanterior direction (enlarging the midlateral approach).
In our 5 cases, we preferred to end the operation in open surgery, with a small incision that joins the anteromedial portal to the midlateral one (ideally following the incision by the Kocher approach). This miniopen surgery enabled us to perform fixation with resorbable screws and pins, in an anteroposterior direction, without putting the radial nerve at risk.
Treatment was completely arthroscopic with fragments removal in 3 type III cases. Also in these cases we deem mandatory to explore by the arthroscope all the joint compartments, after having accurately examined the fracture comminution by CT scan, in order to reduce the risk of leaving debris.
The last case, apart from the presented series, is a rare impacted fracture of the capitellum combined with a coronoid tip fracture (Fig. 8.1). By arthroscopy it was possible to remove the coronoid fragment (working in the anterior compartment), to raise the impacted osteochondral fragment and fix it with resorbable pins (working in the posterolateral gutter). In this case arthroscopy displayed all of its efficacy, reducing surgical aggressiveness at a minimum.
At the end of fixation or debridement, articular stability is evaluated (possible also arthroscopically [13]). Faced with doubt about the stability, we recommend exploring, and possibly repairing, the lateral collateral ligament.
8.3 Coronoid Fractures
The coronoid plays a key role in elbow joint stability. Fractures were classified into 3 types according to their size by Regan and Morrey [14] in 1989 and only recently have new more complex classifications been devised [15, 16] to include possible morphologies of the fragments connected to the type of injury that can produce them.
Larger fractures are caused by a direct posterior injury, whereas a posterolateral or posteromedial distortion mechanism has been identified for fractures of the apex and medial surface respectively (sublime tubercle insertion site of the anterior bundle of the medial collateral ligament) [16].
Reduction and fixation of coronoid fractures is necessary to restore the anterior and medial elbow stability that was lost with the injury.
When combined with fractures of the radial head, which require prosthetic replacement, after radial head excision the coronoid fracture can be reached through Kocher’s lateral approach. Conversely, when the fracture is isolated, reaching and exposing the coronoid requires wide approaches (anterior, anteromedial or medial), which are aggressive and not simple to perform [17].
8.3.1 In the Literature
There are only two articles in the literature
Liu et al. [18] in 1996 showed two cases of coronoid tip fracture, which after conservative treatment produced pain and joint stiffness. Arthroscopic removal of the fracture fragment is decisive.
But the first real experience was described by Adams et al. [19] in 2007. Two of the seven fractures described had fragments that were too small to be fixed. In 4 cases arthroscopically-assisted fixation (ARIF) was performed, whereas in one case open surgery was needed to perform a stronger fixation, by dedicated plate. In 3 of the seven cases reconstruction of the lateral collateral ligament (LUCL) was needed.
8.3.2 Surgical Technique in Our Experience
As for capitellum fractures, coronoid fractures are very rarely isolated. Mostly, they are combined with radial head or olecranon fractures. In these cases, open surgery, necessary to treat combined fractures, cannot be replaced by arthroscopic treatment of the coronoid.
Conversely, isolated fractures of the coronoid can be treated arthroscopically. From January 2000 to July 2012, 5 of the 8 isolated coronoid fractures treated by the authors were treated arthroscopically. Two cases were treated with reduction and fixation with wires alone, two with cannulated screws as well as K wires, and one case with osteosuture combined with K wires.
With the patient in a lateral position, and after having washed repeatedly with needle and saline solution, the anterior arthroscopic portals are made (anteromedial, anterolateral and anteromedial or lateroproximal). Having removed the hematoma the arthroscope is inserted into the anterolateral portal to assess the fracture well. With a motorized instrument and thermal ablator the surfaces of the fragments are exposed. The retractor in the proximal anterior portal (medial or lateral) is fundamental in this phase to keep the joint space open, thus permitting working with a lower inflow pressure. The joint capsule is constantly lacerated and retracted, together with the fragment/s of the fracture. A high pressure of infusion will lead to an early extra-articular swelling, making surgery gradually more difficult and dangerous.
Through the ‘combined effect’ of the retractor (from the proximal portal) and the probe (from the anteromedial portal) the larger articular fragments are put back in place, thus maintaining the capsular insertion (Fig. 8.2g), whereas the smaller ones can be removed. At this point it is useful to expose the dorsal surface of the ulna with a small incision, so that the skin and the subcutaneous tissue do not interfere with the instruments required for the fixation.

Coronoid fracture. ARIF of a coronoid fracture: a, b, c—Illustration of the anteromedial, anterolateral and proximal anterolateral arthroscopic portals. Red shows the direction of the percutaneous fixation (advisable to perform a small skin incision so as not to interfere with placing the K-wires); d—CT scan of the fracture performed routinely to assess the morphology of the fracture and plan surgery; e, f—intraoperative radiographic checks of the temporary K-wire fixation and definitive fixation with K-wire and cannulated screw; i–n intraoperative images: with the arthroscope in the anterolateral portal, the retractor in the proximal anterolateral portal and the shaver in the anteromedial one the fracture is exposed (i); at least two K-wires are inserted out-in under the fracture fragments (h); while keeping the fracture reduced, the wires are pushed forward past the fragment (h) protecting the tip (i) to avoid lesions to the vascular and neural structures. Depending on the size of the fragments, fixation can be strengthened by placing one or more cannulated screws on the wires (l, m, n)
According to the size of the fragments, two different fixation techniques can be used:
-
cannulated screws and/or K wires
-
osteosuture.
Cannulated screws and/or K wires: (Fig. 8.2). After redislocating the intraarticular fracture with the lever from the proximal portal, K wires are drilled from the posterior cortex of the ulna, keeping the arthroscope in the anterolateral portal and checking its exit from the base of the fractured coronoid (Fig. 8.2h). This action is made safer and repeatable by the use of an aiming device for cruciate ligament surgery; a small-sized tip device must be used, because it has to enter through the anteromedial portal, and a bulky tip might impinge in the brachial muscle. The intraoperative radiographic checking is useful to evaluate the direction of the wires, especially if the freehand technique is chosen.
Having placed the first K wire, the others are placed (at least two to achieve rotational stability of the fixation).
After slightly retracting the wires, until the tip goes into the medullary bone, the fracture is reduced with the lever by the proximal portal, and with an arthroscopic grasper by the anteromedial portal.
While maintaining reduction, the wires are pushed forward again, checking that they come out anteriorly to the fragments (Fig. 8.2i).
When the size of the fragment allows, a cannulated screw, 3.5 mm in diameter, can be placed on one of the K wires. It is cautious to hold the tip of the intra-articular K wire firm with a Kocher, while inserting the cannulated drill and the screw, to prevent the wire from being pushed anteriorly, crossing dangerously the anterior brachial muscle (Fig. 8.2l, m, n).
Osteosuture: this is chosen when the fragments are too small and numerous to be fixed. This fixation will not be as stable as the previous one, but it enables the correct tension of the anteromedial joint capsule to be maintained, while scarring takes place. Often this technique also enables small bone fragments to consolidate.
To contain the joint capsule with suture thread, the suture passer commonly used for suturing rotator cuff lesions is extremely useful (Fig. 8.3d). The work portal is always anteromedial, whereas the arthroscope one remains anterolateral. Once again the retractor through the accessory proximal portal plays a fundamental role.

Osteosuture of a coronoid fracture. The portals to perform osteosuture are the same as those used for fixation with K-wires/screws fixation (a, b). The preoperative CT scan (c) shows a displaced fracture. Osteosuture can be performed arthroscopically with the anterolateral arthroscope (d–k) as described in the text, possibly reinforced by k_wires (l)
The vector suture is replaced by a reinforced double-zero suture (Orthocord, Depuy-Mitek or Hi-Fi Conmed Linvatec or Fiberwire Arthrex…) (Fig. 8.3e).
Having placed the suture thread through the joint capsule (immediately behind the fragments of the coronoid tip), the first out-in hole is made at the base of the coronoid with a K wire 1.4 mm in diameter. Having removed the thread, a spinal needle (18 GA 3.50 IN/1.2 * 90 mm spinal needle) (Fig. 8.3f) is inserted by which a vector thread (single-filament 1 mm in diameter), which having been recovered from the anteromedial portal (Fig. 8.3g), will take the first head of the osteosuture through the ulna, posteriorly (Fig. 8.3h). By inserting the second head using the same technique, the osteosuture can be closed on the posterior cortex, guiding the fracture fragments with the probe (Fig. 8.3).
Regardless of the ARIF technique chosen, the fixation must be stable upon palpation and flexion–extension tests of the elbow, to reduce the period of postoperative immobilization to a minimum. Therefore, in our cases we always supplemented screw fixation or osteosuture by K wiring (Figs. 8.2f, 8.3k, l).
8.4 Radial Head Fractures
Radial head fractures, extremely common, are classified into 4 types by Mason and Johnston and divided further into simple and complex, according to possible combined lesions [19, 20]. The option of conservative or surgical treatment depends on the number of fragments, their displacement, whether the fracture involves the olecranon and/or coronoid and if there are ligament lesions. When surgery is the choice, the surgeon has to decide among radial head excision, reduction and fixation of the fracture, or prosthetic replacement. It has been shown that ORIF or the prosthetic replacement of the radial head enables a better recovery of articular stability [21] and therefore will certainly be the best choice when there is a combined lesion of the medial collateral ligament. Conversely, an isolated fracture of the radial capitellum can be treated by the simple excision of the fragments (if they interfere with the passive joint range) or by full radial head excision (if more than 50 % of the surface is involved).
8.4.1 In the Literature
The first arthroscopic treatment was described in 2004 [22] for a fracture of the surgical neck of the proximal radius of a child, which was reduced by a manual maneuver and fixed by percutaneous wiring.
In 2006 Rolla et al. [23] published a short series of 6 fractures of the radial head (II, III and IV types according to Mason) reduced and fixed with a percutaneous screw. The author used his own surgical technique, and recommended reducing the fracture by working in the anterior compartment, and moving in the posterolateral gutter for arthroscopic fixation.
Fourteen cases were collected by Michels et al. [24] the following year, all Mason type II with a mean follow-up of 5.6 years and results ranging from good to excellent, matching those of open surgery. For this series the author managed ARIF by the use of only two portals (anterolateral and posterolateral) besides a small incision to insert the screws.
8.4.2 Surgical Technique in Our Experience
In our center arthroscopic treatment of isolated fractures of the radial head began in 2007. Until now 21 cases have been treated arthroscopically (7 ARIF, 8 partial removals of the fragments, 3 radial head excisions and 3 simple reductions, without fixation).
-
1.
Arthroscopic Reduction Internal Fixation (Arif) for Mason type II fractures
The first stage consists of removing the intra-articular hematoma and visualizing the fracture in the anterior compartment. We perform 3 approaches routinely: anteromedial (for the arthroscope) anterolateral (for the tools) and proximal anterolateral (for the retractor). The fracture is reduced by using alternately the probe from the anterolateral portal and proximal anterolateral, by pronosupination movements. Having achieved reduction, the fragments must be stabilized with K wires, after choosing the position in pronosupination to hold for fixation.
The working position to perform screw fixation may vary. In our experience we divided the fractures according to the position of the fracture fragment/s in relation to the safe zone (part of the radial head that does not come in contact with the small sigmoid notch). Dividing the radial head ideally into two halves in neutral pronosupination we have the lateral half (which contains the Safe Zone) and the medial one (Fig. 8.4).
Fig. 8.4 
Cadaver specimen. Radial head in full supination, in neutral position and in full pronation. Fractures that involve the half of the radial head opposite to the safe zone, are more difficult to be fixed by the direct lateral portal
Fractures of the lateral half can be fixed by holding the position used for reduction, by placing the forearm in pronation. The retractor and the probe hold reduction and keep the workspace open. An accessory lateral portal is directed at the radial head and a small 5 mm cannula is placed in the joint. The cannula is important to protect the soft tissues from the rotating tools (K wire, drill, screwdriver) as well as to prevent the thin K wire, used to insert the screw, from bending or breaking. The K wire is inserted through the cannula. If the fracture appears to be stable the fixation procedure is performed (measurement, drilling, screw), otherwise other percutaneous K wires should be placed (outside the cannula) to hold the fragment still while the drill produces the hole for the screw (Fig. 8.5f–j).
Fig. 8.5 

Various fixation methods for radial head fractures: in the posterolateral gutter (a–e) and anterior compartment (f–j) for radial head fractures that involve the lateral half, fixation is performed through a direct accessory portal (in red); in the anterior compartment (k–r) for fractures of the medial side of the radial head, fixation is performed through the anteromedial portal (in red)
Fractures of the lateral half can also be fixed by working in the posterolateral gutter [23] by opening the posterolateral and midlateral portals to place alternately the arthroscope and the work tools. The forearm will have to be progressively placed in supination, until the fracture can be visualized. The procedure for the fixation is the same as that seen in the previous position (Fig. 8.5a–e).
Conversely, when the fracture involves the medial half of the radial head (Fig. 8.5k–r) pronosupination cannot put the fragment to be fixed in the correct place. In this case arthroscopic fixation can be performed by the anteromedial portal by placing the arthroscope in the anterolateral one. The work cannula is even more important to protect the soft tissues.
The ARIF described is certainly more difficult than fixation in open surgery, but offers the numerous advantages of arthroscopy. For example in 4 of the 7 cases treated surgically we found small loose osteochondral fragments not visible by preoperative CT that certainly would not be found in open surgery.
However, choosing the length of the screws is more difficult because it is not easy to perform an intraoperative radiographic check with the tools in place; Generally, the screws range from 14 to 18 mm long and in case of doubt it is better to choose a shorter screw and check at the end of fixation, without risking a loss of reduction or bending the K wires in an attempt to get a satisfactory radiographic view.
The instruments should be chosen carefully so that the drill and the screwdriver of the 2.5 mm diameter screws are not too short, especially when fixation is performed by the anteromedial portal. If these tools are not available, the arthroscopic cannula can be cut on the serving table, before inserting it inside the joint.
-
2.
Simple Arthroscopic Reduction
In three cases of Mason fracture type II, after debriding the fracture, reduction was easy. The reduced fragment on the remaining intact part of the radial head was firmly kept in place by the annular ligament, which the arthroscopic technique leaves intact.
After several stability tests we decided to avoid further surgical steps; all cases had a favorable outcome and full, swift recovery.
-
3.
Arthroscopic Fragment Removal
In fractures with more comminution, when more than 50 % of the radial head is still in site, fixation is not reliable and prosthetic replacement can be excessive.
In these cases, arthroscopic exploration enables removal of the fragments and ample joint debridement, without invalidating articular stability with the surgical approach. It is performed in the anterior compartment (by anteromedial, anterolateral, and proximal anterolateral approaches) or in the posterolateral gutter (by the posterolateral and midlateral approaches).
Arthroscopy can also be used to assess the articular stability of the ulno-humeral joint [12], which is important in decision-making about radial head prosthesis.
-
4.
Arthroscopic Radial Head Removal
When the comminution does not enable fixation, the elbow is stable, and the patient is not so young, resection of the radial head is indicated, which can be performed by arthroscopy.
After removing the fragments in the anterior compartment, resection of the radial head is precise and easy by inserting the burr through the midlateral portal while the arthroscope is still in the anteromedial portal. The radial head is cut at the level of the superior margin of the intact annular ligament. Shortening the proximal radius as little as possible without impairing the annular ligament helps to hold the tension of the lateral collateral compartment (Fig. 8.6).
Fig. 8.6 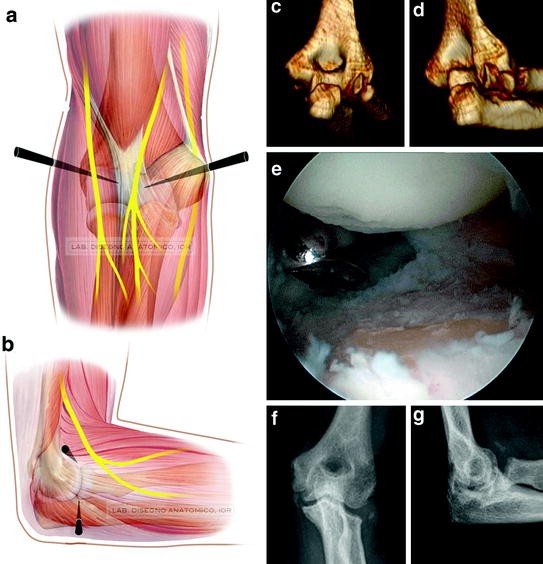
Radial head removal. Illustration (a, b) of the anteromedial, anterolateral and midlateral approaches to perform radial head excision; (c, d) comminuted fracture of the radial head in an elderly woman where radial head excision is indicated. Intraoperative image (e) with the arthroscope in the anteromedial portal monitoring the excision of the radial head performed at the height of the annular ligament by a burr through the midlateral portal. Radiographic check of the radial head excision (f, g)




8.5 Combined Radial Head and Coronoid Fractures
We treated only one case of combined radial head and coronoid fracture arthroscopically. This small-sized radial head fracture was widely displaced; the anterior joint capsule was lacerated and raised with a large fragment of the coronoid. By arthroscopy we followed carefully the path of the radial head fracture, removing the fragments, and performed an ARIF of the coronoid. At the end of the operation the elbow was deemed stable by dynamic tests. Rehabilitation of the patient was begun the day after surgery. Unfortunately, at one-month follow-up, anterior bridge ossifications had formed, with a complete loss of passive movement (Fig. 8.7).

Terrible triad of the right elbow in a 28 years old patient. Tridimensional and two-dimensional CT reconstruction (a, b, c) of the radial head fracture and coronoid fracture. d intraoperative x-ray after arthroscopic removal of the radial head fragments and reduction and internal fixation of the coronoid. e, f radiographic follow-up at 4 months shows the massive anterior bridging ossification
8.6 Complications
No neurological or vascular lesions were recorded.
There were two cases of postoperative stiffness. One Manson II fracture occurred with extension deficit, which was treated again after 9 months by soft tissue release and arthroscopic removal of the screw. The screw was in place, the fracture healed and the stiffness was connected to the reactive fibrosis of the anterior capsule. The soft tissue release enabled the full recovery. The second is the case of heterotopic ossifications as a sequela of the terrible triad treated by arthroscopy.
8.7 Conclusions
The indications for arthroscopic surgery are have become wider and more perfected, over the last two decades, and provide new tools to better address various diseases: one example is the joint fracture treatment which has witnessed the move from surgical debridement to arthroscopic reduction and fixation (ARIF).
The impetus to strive for this difficult but interesting evolution comes from the need to reduce the surgical trauma caused by exposing and reducing articular fractures, which even now give high sequela rates over time.
If 10 years ago ARIF was a future possibility, today it is becoming a reality which, with its advantages and limits (see Table 8.1), is on a par with open surgery.
In this chapter we have tried to summarize the state of the art in the light of our experience. The various surgical techniques described are still not perfectly reproducible, and the surgeon must adapt them to suit each patient. If the feeling is that of a promising road to go down, the two complications that we have highlighted teach us that arthroscopy is also not exempt from the risk of postoperative stiffness. The number of cases is still too small and more in-depth studies are required to assess the real cost/benefit relationship of arthroscopic treatment of articular fractures.
A strict selection of the surgical indication is indispensable; currently we can indicate the following conditions for arthroscopic treatment:
-
Fractures of the radial head: Mason type 2–3 fractures (no combined ligament lesions)
-
Isolated fractures of the coronoid
-
Fractures of the capitulum humeri (no combined ligament lesions)
Only case reports are found for the arthroscopic treatment of combined fractures of the radial capitellum and coronoid, other articular fractures (inter or supra-condyloid) or lesions of the lateral collateral ligament [2, 13]. These cases are to be left in the hands of more expert surgeons of the sector, while waiting for further technical development and significant results.
References
Kelly EW, Morrey BF, O’Driscoll SW (2001) Complications of elbow arthroscopy. J B J S Am 83:1
Peden JP, Savoie FH, Field LD (2010) Arthroscopic treatment of elbow fractures. In: Saunders (ed) The elbow and wrist—AANA advanced artrhoscopy, Chap. 17, pp 136–143
Yeoh KM, King GJW, Faber KJ, Glazebrook MA, Athwal GS (2012) Systematic review. Evidence-based indications for elbow arthroscopy. Arthroscopy 28(2):272–282
Ring D, Jupiter J, Gulotta L (2003) Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 85:232–238
Bryan RS, Morrey BF (1985) Fractures of the distal humerus. In: Morrey BF (ed) The elbow and its disorders. WB Saunders, Philadelphia, pp 325–333
McKee MD, Jupiter JB, Bamberger HB (1996) Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 78:49–54
Dubberley JH, Faber KJ, Macdermid JC, Patterson SD, King GJ (2006) Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 88(1):46–54
Feldman MD (1997) Arthroscopic excision of type II capitellar fractures. Arthroscopy 13(6):743–748
Hardy P, Menguy F, Guillot S (2002) Arthroscopic treatment of capitellum fracture of the humerus. Arthroscopy 18(4):422–426
Mitani M, Nabeshima Y, Ozaki A, Mori H, Issei N, Fujii H, Fujioka H, Doita M (2009) Arthroscopic reduction and percutaneous cannulated screw fixation of a capitellar fracture of the humerus: a case report. J Shoulder Elbow Surg 18(2):e6–e9 Epub 2008 Nov 25
Kuriyama K, Kawanishi Y, Yamamoto K (2010) Arthroscopic-assisted reduction and percutaneous fixation for coronal shear fractures of the distal humerus: report of two cases. J Hand Surg Am 35(9):1506–1509 Epub 2010 Aug 21
Hsu JW, Gould JL (2009) The emerging role of elbow arthroscopy in chronic use injuries and fracture care. Hand Clin 25:305–321
Holt MS, Savoie FH III, Field LD, Ramsey JR (2004) Arthroscopic management of elbow trauma. Hand Clin 20:485–495
Regan NM, Morrey BF (1992) Classification and treatment of coronoid process fractures. Orthopaedics 15(7):345–353
O’Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MG (2003) Difficult elbow fractures: pearls and pitfalls. Instuc Course Lect 52:113–134
Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King GJW (2009) The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am 91(6):1448–1458
Cheung EV, Steinmann SP (2009) Surgical approaches to the elbow. Am Acad Orthop Surg 17:325–333
Liu SH, Henry M, Bowen R (1996) Complications of type I coronoid fractures in competitive athletes: report of two cases and review of the literature. J Shoulder Elbow Surg 5(3):223–227
Adams JE, Merten SM, Steinmann SP (2007) Arthroscopic-assisted treatment of coronoid fractures. Arthroscopy 23(10):1060–1065
Van Riet RP, Van Glabbeek F, Morrey BF (2009) Radial head fracture. In: Morrey BF (ed) The elbow and its disorders, 4th edn. Saunders Elsevier, Philadelphia, PA, pp 359–381
Pike JM, Athwal GS, Faber KJ, King GJW (2009) Radial head fractures-an update. J Hand Surg 34A:557–565
Dawson FA, Inostroza F (2004) Arthroscopic reduction and percutaneous fixation of a radial neck fracture in a child. Arthroscopy 20(Suppl 2):90–93
Rolla PR, Surace MF, Bini A, Pilato G (2006) Arthroscopic treatment of fractures of the radial head. Arthroscopy 22(2):233.e1–233.e6
Michels F, Pouliart N, Handelberg F (2007) Arthroscopic management of Mason type 2 radial head fractures. Knee Surg Sports Traumatol Arthrosc 15(10):1244–1250 Epub 2007 Jul 17
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 ISAKOS
About this chapter
Cite this chapter
Guerra, E., Marinelli, A., Bettelli, G., Cavaciocchi, M., Rotini, R. (2013). Arthroscopic Treatment of Elbow Fractures. In: Pederzini, L. (eds) Elbow Arthroscopy. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-38103-4_8
Download citation
DOI: https://doi.org/10.1007/978-3-642-38103-4_8
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-38102-7
Online ISBN: 978-3-642-38103-4
eBook Packages: MedicineMedicine (R0)