
Abstract
Congenital heart defects are uncommon among people with NF1, but pulmonic stenosis and coarctation of the aorta appear to occur more often than expected. Double outlet right ventricle (the characteristic cardiac defect in Nf1 −/− mouse models) and other complex cardiac malformations are rare in people with NF1.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Congenital Heart Defect
- Malignant Peripheral Nerve Sheath Tumor
- Neointima Formation
- Noonan Syndrome
- Congenital Heart Defect
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Most people with NF1 vasculopathy have involvement of multiple arteries in a spotty distribution. NF1 vasculopathy is usually asymptomatic, although the first clinical manifestation may be a life-threatening or fatal event. Vascular lesions in NF1 patients may occur anywhere but are most often identified in the renal arteries, usually in association with hypertension. Cerebrovascular disease typically produces stenosis of the internal carotid artery, middle cerebral artery, or anterior cerebral artery and is often associated with moyamoya.
No cohort of NF1 patients has been systematically screened for vasculopathy of any site, and the overall prevalence among people with NF1 is unknown. Vasculopathy is an unexpectedly frequent cause of death among people with NF1 who die in childhood, adolescence, or early adulthood.
Most of our understanding of the role that neurofibromin plays in cardiovascular system development comes from studies in targeted mouse mutants. Spontaneous cardiovascular disease is not seen in heterozygous Nf1 +/− mice, but Nf1 −/− mutants die in mid-gestation as a result of double outlet right ventricle, membranous ventricular septal defect, and enlarged endocardial cushions. Studies in lineage-restricted homozygous knockout mice demonstrate critical involvement of endothelial cells in the pathogenesis of these cardiac malformations, with pERK activation leading to hyperproliferation of the endocardial cushions.
Murine models show a normal phenotype and normal function for heterozygous Nf1 +/−endothelial cells, but these cells exhibit an exaggerated response to environmental changes and growth factors. Adult humans with NF1 have normal numbers of endothelial colony-forming cells in their peripheral blood, but these cells exhibit increased ERK activation and increased proliferation and migration in response to angiogenic growth factors.
Hyperproliferative potential has been demonstrated in each of the cell types that comprise the vascular wall—endothelial cells, vascular smooth muscle cells (VSMCs), and pericytes. The characteristic lesions of NF1 vasculopathy in humans are intima hyperplasia and neointima formation, and analogous proliferation of intima VSMCs has been demonstrated in murine models using a variety of techniques. Studies in lineage-restricted knockout mice indicate that Ras–Mek–ERK signaling is amplified in VSMCs, and this appears to play an important role in neointima formation. Experiments using adoptive bone marrow transplantation indicate that heterozygous inactivation of Nf1 in the marrow is also required for neointima formation in response to injury. A key factor may be stimulation of VSMC proliferation by cytokines produced by marrow-derived macrophages.
Although cardiovascular abnormalities have been recognized as a feature of NF1 for over 65 years (Reubi 1945; Feyrter 1949), the frequency and natural history of these lesions are still incompletely understood. Nevertheless, recent research has provided important insights into the molecular pathogenesis of the congenital heart defects and vasculopathy that occur in some people with NF1.
23.1 Congenital Heart Defects
The prevalence of clinically apparent congenital heart defects (CHD) ranges from 0.4 % to 6.4 % in published series of NF1 patients (Lin et al. 2000). Differences in ascertainment, patient age, and diagnostic criteria for cardiac defects probably account for the wide variation in reported frequencies. Tedesco et al. (2002) performed two-dimensional echocardiograms and color Doppler studies on 48 unselected children and adolescents with NF1 and found cardiovascular disease in four (8 %): one case of pulmonic stenosis, one case of aortic coarctation, and two cases of hypertrophic cardiomyopathy. No abnormalities were found in a control group of 30 children of comparable age.
The strongest evidence that NF1 and CHD are, in fact, associated is the extraordinarily high proportion of these patients in whom the CHD is pulmonic stenosis, usually of the valvar type. Pulmonic stenosis accounts for approximately one-quarter of all CHD among NF1 patients (Lin et al. 2000) and is a recognized feature of three clinical subtypes of NF1-Watson syndrome, NF1-Noonan syndrome, and individuals with large deletions of the NF1 gene (Lin et al. 2000). Valvar pulmonic stenosis is also a common feature in patients with Noonan syndrome, LEOPARD syndrome, or cardio–facio–cutaneous syndrome, conditions that, like NF1, are genetic disorders that produce dysregulation of the Ras/MAPK pathway (Zenker 2011).
Coarctation of the aorta has been reported repeatedly in patients with NF1 (Lin et al. 2000), although the narrowing in these patients is usually of a long fusiform type. This differs anatomically from the abrupt segmental constriction that is most often seen in other patients with coarctation of the aorta. Hypertrophic cardiomyopathy has also been reported in several NF1 patients, but this appears to be an infrequent occurrence (Friedman et al. 2002).
Double outlet right ventricle, a conotruncal defect, occurs in homozygous Nf1 “knockout” mouse embryos (Brannan et al. 1994; Jacks et al. 1994) but appears to be quite rare in people with NF1. In fact, the small number of NF1 patients who have been reported to have complex CHD of any kind is striking (Lin et al. 2000; Friedman et al. 2002).
23.2 NF1 Vasculopathy
NF1 vasculopathy may affect arteries that range in size from small arterioles to the proximal aorta. The systemic circulation is affected much more often than the pulmonary arteries, although the latter may also be involved. The outflow tract of the heart or the veins may also be affected. Most NF1 patients with vasculopathy have involvement of multiple vessels (Friedman et al. 2002; Oderich et al. 2007).
NF1 vasculopathy is usually asymptomatic, and the first clinical manifestation may be a life-threatening or fatal event. Sudden death has been reported as a result of rupture of a major artery, cerebral ischemia or hemorrhage, or myocardial infarction in young patients with NF1 vasculopathy (Friedman et al. 2002). Pathological consequences of NF1 vasculopathy may include arterial stenosis, occlusion, aneurysm, pseudoaneurysm, and rupture or fistula formation. The condition is sometimes progressive, with lesions becoming more severe with time or recurring after treatment that initially appeared to be effective (Criado et al. 2002; Rea et al. 2009; Ghosh et al. 2012).
Vascular lesions in NF1 patients are most often identified in the renal arteries: 1–5 % of people with NF1 have renal artery disease (Friedman et al. 2002). High blood pressure may occur as a result of proximal renal artery stenosis, intraparenchymal renal arterial abnormalities, or both. Renovascular hypertension in NF1 usually presents in childhood, adolescence, or early adulthood; it is sometimes recognized as eclampsia or accelerated hypertension during pregnancy (Dugoff and Sujansky 1996).
Cerebrovascular abnormalities in people with NF1 usually result from stenosis or occlusion of the internal carotid artery, middle cerebral artery, or anterior cerebral artery (Friedman et al. 2002). Small telangiectatic vessels may form around the area of the stenosis and look like a puff of smoke on cerebral angiography. Patients with NF1 appear to be unusually prone to this finding, which is called “moyamoya,” in response to cerebral hypoxia (Wu et al. 2006) or radiation damage (Ullrich et al. 2007; Milewicz et al. 2010).
23.3 Prevalence of NF1 Vasculopathy, Morbidity, and Mortality
No population-based cohort of NF1 patients has been systematically screened for vasculopathy, but a few studies have assessed various aspects of vascular disease among clinical series. Fifteen (3.8 %) of 398 children with NF1 who underwent MRI were found to have stenosis or occlusion of an intracranial artery or moyamoya in one series (Ghosh et al. 2012). Rosser et al. (2005) examined brain MRIs of 316 unselected children with NF1 and found that 8 (2.5 %) had cerebrovascular abnormalities. In another series, 7 (4.9 %) of 144 patients with NF1 who had undergone head MRI were found to have dysplasia of the cerebral arteries (Cairns and North 2008). The arterial lesions were asymptomatic in most of the patients studied.
Seventeen (6.4 %) of 266 children with NF1 who underwent MRI in another series had stenosis of one or more intracranial arteries, moyamoya, or aneurysms (Rea et al. 2009). Most of these patients were imaged because of central nervous system symptoms. Fifteen of the 17 affected patients also had optic gliomas, but no information is provided regarding radiotherapy.
Patients who have had radiation therapy for intracranial tumors are at increased risk of developing moyamoya (Milewicz et al. 2010), and this is especially frequent among patients with NF1 (Ullrich et al. 2007). The pathogenic basis for this association is unknown, but possibilities include increased vascular damage, abnormal vascular repair, or increased neovascular proliferation in response to radiation injury in NF1 patients.
Fossali et al. (2000) screened 27 unselected children with NF1 and found hypertension in three (11 %) and borderline hypertension in another two. Thirteen of these patients had venous digital subtraction angiography, and renal artery stenosis was seen in seven and aortic coarctation in one. 24-h blood pressure monitoring has been performed in two series of young NF1 patients, which included 20 and 73 subjects, respectively (Fossali et al. 2000; Tedesco et al. 2005). Abnormal 24-h blood pressure measurements were observed in 40 % of the smaller series and in 16 % of the larger series. Some of the cases with abnormal 24-h monitoring had normal basal blood pressure measurements.
Pulmonary hypertension may also occur in NF1, although it is much less frequent than arterial hypertension (Stewart et al. 2007; Montani et al. 2011). Unlike arterial hypertension, pulmonary hypertension is rarely seen in NF1 patients under 50 years of age, and it is often associated with parenchymal lung disease.
Vasculopathy appears to be an unexpectedly frequent cause of death among people with NF1 who die in childhood, adolescence, or early adulthood (Rasmussen et al. 2001). There is a large excess of deaths before 50 years of age among people with NF1 (Rasmussen et al. 2001). Most of this excess mortality is attributable to neoplasms, especially malignant peripheral nerve sheath tumors, but deaths associated with vascular disease also occur more often than expected among young adults with NF1 (Sørensen et al. 1986; Rasmussen et al. 2001; Evans et al. 2011).
In an unselected autopsy series, Salyer and Salyer (1974) found histological lesions of vasculopathy in 8 of 18 NF1 patients who died at a median age of 24 years (range, 4–69 years). Only one of these patients died of vascular disease; the vasculopathy was asymptomatic in the other seven affected patients. The kidneys were involved in six of the eight NF1 patients, but multiple arteries were affected, including those of the heart, pancreas, thyroid, ileum, spleen, and meninges.
23.4 Embryology
Neurofibromin plays a critical role in embryogenesis and cardiovascular development. In animal models, cardiovascular malformations result from substantial or complete loss of neurofibromin activity and constitutive Ras stimulation of aberrant proliferation within key cardiovascular lineages in the embryo (Viskochil 2002). However, the role of haploinsufficiency for neurofibromin in heart development and function is not yet well understood.
Most of our understanding of the in utero role of NF1 has come from animal studies, principally targeted mouse mutants and more recently zebra fish results (Brannan et al. 1994; Jacks et al. 1994; Gitler et al. 2003; Ismat et al. 2006; Xu et al. 2007; Padmanabhan et al. 2009). Somewhat surprisingly, Nf1 heterozygous mice are viable postnatally and do not exhibit any in utero cardiovascular abnormalities. The reason underlying the disconnect between the mouse and human NF1 heterozygous cardiovascular developmental phenotypes remains unclear but may be due to the inbred nature of mouse genetic backgrounds used or the lack of sophisticated experimental tools to analyze and map partially penetrant phenotypes.
However, systemic Nf1 null mutants exhibit mid-gestation lethality and outflow tract septation defects (double outlet right ventricle/membranous ventricular septal defect) and concomitant enlarged endocardial cushions (Brannan et al. 1994; Jacks et al. 1994). Although the precise cause of the Nf1 null mid-gestation lethality remains unclear, significant anasarca of the embryo suggests either poor cardiac function or abnormal regurgitant blood flow, and diastolic dysfunction may cause in utero death (Conway et al. 2003; Phoon et al. 2004).
Given the demonstrated role of the neural crest within both NF1 tumor formation and the pathogenesis of outflow tract septation defects, as well as the fact that neural crest-derived cells in the peripheral nervous system have the highest neurofibromin expression levels, these cardiovascular defects were presumed to have a cardiac neural crest cell origin (Kirby et al. 1983; Daston and Ratner 1992; Zhu et al. 2002; Hutson and Kirby 2003; Snider et al. 2007; Yang et al. 2008). Nevertheless, more recent lineage-restricted mouse knockout approaches surprisingly revealed that tissue-specific inactivation within the endothelial lineage using Tie2–Cre-mediated Nf1 inactivation reproduced the in utero Nf1 null cardiac abnormalities, although neural crest-restricted inactivation resulted in overgrowth of peripheral nervous tissue (Gitler et al. 2003; Ismat et al. 2006).
Moreover, these transgenic mice showed that loss of Nf1 in the embryonic endocardium, a precursor of the heart valves, is directly linked to an increase in activated GTP-bound Ras. The resulting stimulation of MAPK signaling resulted in abnormal enlargement of the outflow tract septum. Restoration of the neurofibromin GTPase-activating protein (GAP)-related domain in endothelial cells is sufficient to regulate Ras activity and rescue the CHDs observed in Nf1 null embryos (Ismat et al. 2006).
Although these elegant transgenic data suggest a cell-autonomous role for NF1 within the embryonic endothelium and may also provide potential therapeutic targets, it should be noted that the Tie2 promoter used in these studies is expressed throughout the embryonic and extraembryonic endothelial lineage and is also known to be active in hematopoietic stem cells (Forde et al. 2002). Thus, given the myeloproliferative features of NF1 and the importance of the haploinsufficient hematopoietic microenvironment to NF1 disease progression, the precise role of the cardiovascular endothelium within NF1-deficient CHD pathogenesis remains to be verified. Similarly, the potential modifying role and in utero effects of the Nf1-deficient hyperplastic neural crest lineage and its interactions with adjacent endocardial and endothelial lineages during cardiovascular morphogenesis also remain unknown (Gitler et al. 2002; Wang et al. 2005).
Consistent with neurofibromin’s function as a regulator of the Ras pathway and the demonstration of ERK hyperactivation, parallels have been drawn with Noonan syndrome (Mangues et al. 1998; Friedman et al. 2002; Araki et al. 2004; Lasater et al. 2008). Noonan syndrome is an autosomal dominant condition characterized by short stature, facial abnormalities, heart defects, and possibly increased risk of leukemia (Araki et al. 2004). Mutations of PTPN11 occur in approximately 50 % of individuals with Noonan syndrome and lead to pulmonary stenosis, hypertrophic cardiomyopathy, atrial septal defect, tetralogy of Fallot, aortic coarctation, and anomalies of the mitral valve (Marino et al. 1999). In addition to exhibiting similar range of cardiovascular phenotypes, mouse models of both NF1 and Noonan syndrome have enlarged endocardial cushions with increased expression of ERK coincident with double outlet right ventricle and hyperplastic outflow tract cushions (Araki et al. 2004). Moreover, there is a recent report of a child who died early in infancy with severe cardiovascular defects and who was found to carry both an NF1 missense mutation and a pathogenic mutation of the PTPN11 gene (Prada et al. 2011).
Thus, the in utero cardiovascular manifestations of Nf1 null mice appear to result from a pathway mediating CHDs in which endothelially driven hyperproliferation of the endocardial cushions occurs in association with pERK activation. How this mechanism relates to the pathogenesis of CHD in haploinsufficient NF1 patients remains to be seen, but CHD in humans is likely also to involve multiple cell lineages responding in gene dosage-dependent and pathway-selective manners.
23.5 Angiogenesis
Vessel formation and proliferation is a critical component of solid tumor growth and has become an important target for cancer treatment. The ability to form discrete, independent vascular networks, termed “angiogenic switch,” is necessary for tumor propagation and has been demonstrated in a variety of NF1-related tumors. Schwann cells, the primary cell type in neurofibromas, have been shown to undergo angiogenic switch in a number of animal models and human tumor samples (Sheela et al. 1990; Kim et al. 1997; Mashour et al. 1999; Munchhof et al. 2006). Using tumor samples from NF1 patients, Sheela et al. (1990) first demonstrated the ability of neurofibromas to stimulate vascular development independent of additional growth factors. Incubation of single cell colonies on chorioallantoic membranes (CAM) of developing chick embryos showed that wild-type (WT) Schwann cells, fibroblasts, and tumor fragments from non-NF1 patients failed to induce an angiogenic response. However, fragments of tumor from NF1 patients stimulated a robust proliferation of new blood vessels that were easily visualized by 48 h and highly prevalent by 10 days. Addition of fibroblast growth factor (bFGF), a known angiogenic growth factor, greatly enhanced this response. Application of single cell lines of Schwann cells and fibroblasts from neurofibromas demonstrated that Schwann cell-enriched cultures were highly angiogenic and often invaded the mesoderm of the CAM, while fibroblasts, another common cell population within neurofibromas, failed to induce vessel formation (Sheela et al. 1990).
Examination of conditioned media from NF1−/− Schwann cell cultures demonstrated an alteration in the balance of angiogenic growth factors to favor proliferation. Thrombospondin-1, platelet-derived growth factor beta, and midkine mRNA expression were elevated in NF1−/− Schwann cell-conditioned media compared to WT-conditioned media (Mashour et al. 2001). In addition, incubation of endothelial cells (ECs) with NF1−/− Schwann cell-conditioned media produced a hyperproliferative endothelial cell phenotype similar to that seen with stimulation by vascular endothelial growth factor (VEGF) or fibroblast growth factor-2 (FGF-2). This response is mediated through hyperactivation of Ras–Mek–ERK signaling and is abrogated with use of a specific inhibitor of Mek–ERK signaling in vivo (Munchhof et al. 2006). This is a critical observation because alteration in endothelial cell phenotype has been observed in several models of tumor angiogenesis. The contribution of each or all of these growth factors in promoting angiogenesis within the developing neurofibroma and the mechanism through which angiogenic switch occurs to promote tumor growth remains an area for future study.
Although early experiments focused on mutant cell lines with homozygous loss of Nf1, a growing body of evidence suggests that haploinsufficiency of stromal cells has important implications for NF1 tumor propagation and angiogenesis. Murine models of neovascularization have demonstrated an exaggerated proliferation of heterozygous endothelial cells, pericytes, and abnormal neovascular networks in response to hypoxia, which are not present in littermate controls in a normoxic environment (Wu et al. 2006; Ozerdem 2004). Furthermore, Nf1 +/− mice showed markedly increased neovascularization and endothelial proliferation and migration in response to corneal implantation of micropellets impregnated with bFGF or VEGF compared to controls (Munchhof et al. 2006; Wu et al. 2006).
Importantly, Nf1 −/− Schwann cell-conditioned media, which contain increased concentrations of several proangiogenic peptides, further amplify angiogenesis through amplification of Ras–Mek–ERK signaling in heterozygous mice when compared to WT controls (Mashour et al. 2001; Munchhof et al. 2006). Of particular interest, Wu et al. (2006) noted a nearly fivefold increase in the number of macrophages and a significant mast-cell infiltration in the neovascular zone of Nf1 +/− corneas compared to controls. This is an important observation since macrophages and mast cells play a critical role in tumor growth and neoangiogenesis. These studies, when taken together, demonstrate a normal phenotype and function for heterozygous endothelial cells but an exaggerated response to environmental changes and growth factors as compared to wild-type controls.
Overall, there are significant murine and human data that demonstrate an increased angiogenic potential in neurofibromas. Additionally, circulating progenitor cells, which are important in vascular development and angiogenesis, are sensitive biomarkers in several tumor types. Specifically, endothelial progenitor cells can be isolated from adult peripheral blood and contain a novel population of endothelial colony-forming cells (ECFCs) with proliferative potential and the ability to form vessels de novo (Ingram et al. 2004). Although they have normal numbers of ECFCs in the peripheral blood, NF1 patients exhibit increased proliferation and migration in response to angiogenic growth factors VEGF and bFGF compared to age and sex-matched controls. Also, ECFCs isolated from NF1 patients demonstrate increased ERK activation, but their proliferative potential is reduced to non-NF1 levels when incubated with a specific inhibitor of Mek–ERK signaling. This is similar to in vitro and in vivo studies using transduced human cell lines and provides validation to previous model systems.
23.6 Models of NF1 Cardiovascular Disease
Expression of neurofibromin, the gene product of NF1, has been demonstrated in each cell type that composes the vascular wall, including endothelial cells, vascular smooth muscle cells (VSMCs), and pericytes (Norton et al. 1995; Ozerdem 2004; Li et al. 2006; Munchhof et al. 2006). The hyperproliferative potential of each of these cell lines, along with circulating bone marrow-derived cells, which contribute growth factors and cytokines that maintain vessel wall homeostasis, has been demonstrated using in vitro assays (Ozerdem 2004; Li et al. 2006; Munchhof et al. 2006; Xu et al. 2007). However, murine models of subtle or preclinical NF1-related cardiovascular disease have proved difficult because of the lethality of the homozygous mutant mouse (Friedman et al. 2002). In addition, homozygous loss of NF1 is an inaccurate representation of arterial disease in humans because it is likely that homozygous loss of NF1 in patients would result in overt, rather than subtle, disease. Therefore, focus on murine models utilizing heterozygous backgrounds and lineage-restricted inactivation of Nf1 provide more feasible and accurate representations for investigation.
The characteristic phenotype of NF1-related cardiovascular disease is arterial stenosis resulting from intima hyperplasia (or neointima formation) (Hamilton and Friedman 2000; Friedman et al. 2002). Proliferation of VSMCs in the intima layer using murine models has been demonstrated using a variety of techniques. Two mechanisms of injury, endothelial denudation using a beaded guidewire and ligation of the common carotid artery proximal to the bifurcation, have been particularly useful in studies of NF1 neointima formation. In addition, the use of lineage-restricted transgenic mice provides a tractable platform to test the contribution of heterozygous and homozygous loss of neurofibromin to vascular remodeling in a cell-specific manner.
To generate the initial model of neointima hyperplasia, Xu et al. (2007) crossbred alpha-smooth muscle cre (SM22α-Cre) mice and Nf1 fl/− mice (heterozygous mice with a single floxed allele) to generate offspring with lineage-restricted homozygous deletion of Nf1 in VSMCs superimposed on an Nf1 haploinsufficient background. These mice were born at the expected Mendelian ratio, were phenotypically normal at birth, and developed appropriately (Xu et al. 2007). Examination of the cardiovascular system revealed phenotypically normal large arteries, similar to wild-type mice (Xu et al. 2007). In response to ligation of the carotid artery, Nf1 fl/−;SM22α-Cre mice displayed a 2.5-fold increase in intima thickening and intima-to-media ratio compared to WT mice, signifying that proliferation was restricted to the intima layer without simultaneous proliferation of the medial layer (Xu et al. 2007). Smooth muscle cells were the most common cell type in the neointima and demonstrated a profound increase in number and proliferative index compared to WT controls (Xu et al. 2007). However, the phenotype produced in this model was only evident on a haploinsufficient background, suggesting the role of another cell lineage as the primary effector of NF1 vasculopathy.
The accumulation of VSMCs in the neointima suggests that NF1 plays a critical role in VSMC proliferation, migration, and survival (Li et al. 2006; Xu et al. 2007). Several studies have demonstrated marked increases in murine and human VSMC proliferation and migration compared to WT and in response to growth factor (Xu et al. 2007; Munchhof et al. 2006; Li et al. 2006; Lasater et al. 2010). Interestingly, stimulation of Nf1 haploinsufficient murine VSMCs with PDGF-BB, which excites both the Ras–ERK and PI-3 kinase-AKT pathways, resulted in a twofold increase in proliferation and fourfold increase in migration compared to WT VSMCs. These phenotypic changes are probably mediated through Ras–ERK signaling in as much as use of a specific Mek inhibitor and restoration of the Nf1 GAP-related domain resulted in demonstrable ERK inactivation and restoration of Nf1 heterozygous VSMCS proliferation and migration to that of WT controls.
Examination of the neointimas from Nf1 fl/−;SM22α-Cre mice showed significantly more pERK-positive cells than WT mice, indicating that Ras–Mek–ERK signaling was amplified and probably plays an important role in neointima formation and vascular repair (Xu et al. 2007). In addition, restoration of the Nf1 GAP-related domain reduced neointima formation to that of WT mice (Xu et al. 2007). These observations are intriguing and provide insights into the evolution of NF1 vasculopathy because mice harboring genetic mutations that increase signaling through the PDGF-BB–Ras–ERK axis develop exaggerated neointima formation and arterial occlusion, reminiscent of patients with NF1 vasculopathy (Jin et al. 2000; Zhang et al. 2008).
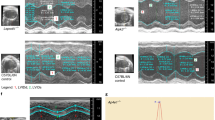
To examine the role of Nf1 heterozygosity alone, Lasater et al. (2008) performed endothelial denudation via a guidewire of the common carotid artery in Nf1 +/− and WT mice. In response to injury, Nf1 +/− mice had a significant increase in intima area and intima-to-media ratio similar to other models and to patients with NF1 vasculopathy (Fig. 23.1). As in previous reports, proliferating VSMCs accounted for more than 75 % of the cells in the neointima, and significant pERK staining was noted (Lasater et al. 2008). Interestingly, pretreatment with Gleevec, an inhibitor of PDGF signaling, prior to injury, completely reduced neointima formation in Nf1 +/−, signifying that neointima formation or, more specifically, VSMC proliferation may be mediated through the Ras–Mek–ERK signaling pathway (Lasater et al. 2008). This is an important model of cardiovascular disease and demonstrates that manifestations of abnormal vascular remodeling may be present in asymptomatic NF1 patients without known risk factors.

Histological and morphometric analysis of injured carotid arteries from WT and Nf1 +/− mice. (a) Representative photomicrographs of carotid arteries from WT (top panels) and Nf1 +/− (bottom panels). Red arrows indicate boundary of neointima. (b) Neointima area of uninjured and injured carotid artery cross sections from WT and Nf1 +/− mice. (c) I/M ratio of uninjured and injured carotid artery cross sections from WT and Nf1 +/− mice. (d) Percentage of carotid artery stenosis 21 days following injury in WT and Nf1 +/− mice
To further define the role of neurofibromin in vessel wall homeostasis and remodeling, Lasater et al. (2010) generated mice with loss of a single Nf1 allele in ECs and VSMCs alone. In response to carotid artery ligation, Nf1 fl/+ ;Tie2Cre (ECs) mice, Nf1 fl/+ ;SM22Cre mice (VSMCs), and Nf1 fl/+ ;Tie2;SM22Cre mice (ECs and VSMCs) had similar neointima formation to WT mice, and intima proliferation in these genotypes was greatly reduced when compared to Nf1 +/− mice, providing evidence that neointima formation and VSMC proliferation are not primarily mediated through heterozygous loss of Nf1 within the vessel wall itself (Lasater et al. 2010). However, using adoptive hematopoietic stem cell transfer techniques, Nf1 +/− mice reconstituted with WT bone marrow showed a tenfold reduction in neointima area and a ninefold reduction in I/M ratio compared to Nf1 +/− mice reconstituted with Nf1 +/− bone marrow (Lasater et al. 2010) (Fig. 23.2). Further, WT mice transplanted with Nf1 +/− bone marrow had increased neointima formation, comparable to Nf1 +/− mice transplanted with Nf1 +/− bone marrow (Lasater et al. 2010) (Fig. 23.2).

Histological and morphometric analysis of WT and Nf1 +/− mice transplanted with WT and Nf1 +/− bone marrow. (a) Representative hematoxylin and eosin-stained cross sections of uninjured and injured carotid arteries from WT and Nf1 +/− mice transplanted with WT or Nf1 +/− bone marrow. Red arrows indicate boundaries of neointima. Scale bars: 50 μm. (b and c) Quantification of neointima area (b) and I/M ratio (c) of uninjured and injured carotid arteries from WT or Nf1 +/− recipients transplanted with WT or Nf1 +/− marrow
These experiments using adoptive bone marrow transplantation strongly indicate that heterozygous inactivation of Nf1 in the bone marrow plays a critical role in neointima formation in response to injury (Lasater et al. 2010). As noted in previous studies of vascular remodeling, macrophages were the most common bone marrow-derived hematopoietic cell identified within the neointima (Wu et al. 2006; Lasater et al. 2010). This is an important observation because macrophages within the neointima produce cytokines that stimulate VSMC proliferation and generate metalloproteases, which are required for extracellular matrix remodeling in neointima formation (Bendeck et al. 1994).
Mouse modeling has made important contributions to our understanding of the pathogenesis of NF1 cardiovascular disease, although important questions remain unanswered. The primary bone marrow-derived hematopoietic cell involved in VSMC proliferation and neointima formation has yet to be identified formally. Lineage-restricted transgenic mice will continue to play a central role in the identification of this primary cell in as much as macrophages, mast cells, and lymphocytes have all been implicated as significant contributors to vascular remodeling (Strom et al. 2007; Swirski et al. 2007).
The nature of the signaling pathway mediating VSMC proliferation within the neointima remains poorly understood. ERK staining is significantly increased in neointimas, and cell culture experiments suggest that Ras–Mek–ERK signaling is an important mediator of VSMC proliferation and migration, although inactivation of ERK signaling through molecular therapeutics or the use of transgenic mice has yet to be demonstrated in vivo. These experiments are needed for understanding disease pathogenesis, rational design of biomarkers, and developing potential therapeutic strategies for patients with NF1 vasculopathy.
References
Araki T, Mohi MG, Ismat FA et al (2004) Mouse model of Noonan syndrome reveals cell type- and gene dosage-dependent effects of Ptpn11 mutation. Nat Med 10:849–857
Bendeck MP, Zempo N, Clowes AW et al (1994) Smooth muscle cell migration and matrix metalloproteinase expression after arterial injury in the rat. Circ Res 75:539–545
Brannan CI, Perkins AS, Vogel KS et al (1994) Targeted disruption of the neurofibromatosis type-1 gene leads to developmental abnormalities in heart and various neural crest-derived tissues. Genes Dev 8:1019–1029
Cairns AG, North KN (2008) Cerebrovascular dysplasia in neurofibromatosis type 1. J Neurol Neurosurg Psychiatry 79:1165–1170
Conway SJ, Kruzynska-Frejtag A, Kneer PL et al (2003) What cardiovascular defect does my prenatal mouse mutant have, and why? Genesis 35:1–21
Criado E, Izquierdo L, Luján S, Puras E, del Mar Espino M (2002) Abdominal aortic coarctation, renovascular, hypertension, and neurofibromatosis. Ann Vasc Surg 16:363–367
Daston MM, Ratner N (1992) Neurofibromin, a predominantly neuronal GTPase activating protein in the adult, is ubiquitously expressed during development. Dev Dyn 195:216–226
Dugoff L, Sujansky E (1996) Neurofibromatosis type 1 and pregnancy. Am J Med Genet 66:7–10
Evans DG, O’Hara C, Wilding A et al (2011) Mortality in neurofibromatosis 1: in North West England: an assessment of actuarial survival in a region of the UK since 1989. Eur J Hum Genet 19:1187–1191
Feyrter F (1949) Über die vasculäre Neurofibromatose, nach Untersuchungen am menschlichen Magen-Darmschlauch. Virchow Arch Pathol Anat 317:221–265
Forde A, Constien R, Grone HJ, Hammerling G, Arnold B (2002) Temporal Cre-mediated recombination exclusively in endothelial cells using Tie2 regulatory elements. Genesis 33:191–197
Fossali E, Signorini E, Intermite RC et al (2000) Renovascular disease and hypertension in children with neurofibromatosis. Pediatr Nephrol 14:806–810
Friedman JM, Arbiser J, Epstein JA et al (2002) Cardiovascular disease in neurofibromatosis 1: report of the NF1 Cardiovascular Task Force. Genet Med 4:105–111
Ghosh PS, Rothner AD, Emch TM, Freidman NR, Moodley M (2012) Cerebral vasculopathy in children with neurofibromatosis type 1. J Child Neurol (in press)
Gitler AD, Brown CB, Kochilas L et al (2002) Neural crest migration and mouse models of congenital heart disease. Cold Spring Harb Symp Quant Biol 67:57–62
Gitler AD, Zhu Y, Ismat FA et al (2003) Nf1 has an essential role in endothelial cells. Nat Genet 33:75–79
Hamilton SJ, Friedman JM (2000) Insights into the pathogenesis of neurofibromatosis 1 vasculopathy. Clin Genet 58:341–344
Hutson MR, Kirby ML (2003) Neural crest and cardiovascular development: a 20-year perspective. Birth Defects Res C Embryo Today 69:2–13
Ingram DA, Mead LE, Tanaka H et al (2004) Identification of a novel hierarchy of endothelial progenitor cells using human peripheral and umbilical cord blood. Blood 104:2752–2760
Ismat FA, Xu J, Lu MM, Epstein JA (2006) The neurofibromin GAP-related domain rescues endothelial but not neural crest development in Nf1 mice. J Clin Invest 116:2378–2384
Jacks T, Shih TS, Schmitt EM et al (1994) Tumour predisposition in mice heterozygous for a targeted mutation in Nf1. Nat Genet 7:353–361
Jin G, Chieh-Hsi Wu J et al (2000) Effects of active and negative mutants of Ras on rat arterial neointima formation. J Surg Res 94:124–132
Kim HA, Ling B, Ratner N (1997) Nf1-deficient mouse Schwann cells are angiogenic and invasive and can be induced to hyperproliferate: reversion of some phenotypes by an inhibitor of farnesyl protein transferase. Mol Cell Biol 17:862–872
Kirby ML, Gale TF, Stewart DE (1983) Neural crest cells contribute to normal aorticopulmonary septation. Science 220:1059–1061
Lasater EA, Bessler WK, Mead LE et al (2008) Nf1+/− mice have increased neointima formation via hyperactivation of a Gleevec sensitive molecular pathway. Hum Mol Genet 17:2336–2344
Lasater EA, Li F, Bessler WK et al (2010) Genetic and cellular evidence of vascular inflammation in neurofibromin-deficient mice and humans. J Clin Invest 120:859–870
Li F, Munchhof AM, White HA et al (2006) Neurofibromin is a novel regulator of RAS-induced signals in primary vascular smooth muscle cells. Hum Mol Genet 15:1921–1930
Lin AE, Birch PH, Korf BR et al (2000) Cardiovascular malformations and other cardiac abnormalities in neurofibromatosis 1 (NF1). Am J Med Genet 95:108–117
Mangues R, Corral T, Lu S et al (1998) NF1 inactivation cooperates with N-ras in in vivo lymphogenesis activating ERK by a mechanism independent of its Ras-GTPase accelerating activity. Oncogene 17:1705–1716
Marino B, Digilio MC, Toscano A et al (1999) Congenital heart diseases in children with Noonan syndrome: an expanded cardiac spectrum with high prevalence of atrioventricular canal. J Pediatr 135:703–706
Mashour GA, Wang HL, Cabal-Manzano R et al (1999) Aberrant cutaneous expression of the angiogenic factor midkine is associated with neurofibromatosis type-1. J Invest Dermatol 113:398–402
Mashour GA, Ratner N, Khan GA et al (2001) The angiogenic factor midkine is aberrantly expressed in NF1-deficient Schwann cells and is a mitogen for neurofibroma-derived cells. Oncogene 20:97–105
Milewicz DM, Kwartler CS, Papke CL et al (2010) Genetic variants promoting smooth muscle cell proliferation can result in diffuse and diverse vascular diseases: evidence for a hyperplastic vasculomyopathy. Genet Med 12:196–203
Montani D, Coulet F, Girerd B et al (2011) Pulmonary hypertension in patients with neurofibromatosis type I. Medicine (Baltimore) 90:201–211
Munchhof AM, Li F, White HA et al (2006) Neurofibroma-associated growth factors activate a distinct signaling network to alter the function of neurofibromin-deficient endothelial cells. Hum Mol Genet 15:1858–1869
Norton KK, Xu J, Gutmann DH (1995) Expression of the neurofibromatosis I gene product, neurofibromin, in blood vessel endothelial cells and smooth muscle. Neurobiol Dis 2:13–21
Oderich GS, Sullivan TM, Bower TC et al (2007) Vascular abnormalities in patients with neurofibromatosis syndrome type I: clinical spectrum, management, and results. J Vasc Surg 46:475–484
Ozerdem U (2004) Targeting neovascular pericytes in neurofibromatosis type 1. Angiogenesis 7:307–311
Padmanabhan A, Lee JS, Ismat FA et al (2009) Cardiac and vascular functions of the zebrafish orthologues of the type I neurofibromatosis gene NFI. Proc Natl Acad Sci USA 106:22305–22310
Phoon CK, Ji RP, Aristizabal O et al (2004) Embryonic heart failure in NFATc1−/− mice: novel mechanistic insights from in utero ultrasound biomicroscopy. Circ Res 95:92–99
Prada CE, Zarate YA, Hagenbuch S et al (2011) Lethal presentation of neurofibromatosis and Noonan syndrome. Am J Med Genet A 155A:1360–1366
Rasmussen SA, Yang Q, Friedman JM (2001) Mortality in neurofibromatosis 1: an analysis using U.S. death certificates. Am J Hum Genet 68:1110–1118
Rea D, Brandsema JF, Armstrong D et al (2009) Cerebral arteriopathy in children with neurofibromatosis type 1. Pediatrics 124:e476–e483
Reubi F (1945) Neurofibromatose et lésions vasculaires. Schweiz Med Wochenschr 75:463–465
Rosser TL, Vezina G, Packer RJ (2005) Cerebrovascular abnormalities in a population of children with neurofibromatosis type 1. Neurology 64:553–555
Salyer WR, Salyer DC (1974) The vascular lesions of neurofibromatosis. Angiology 25:510–519
Sheela S, Riccardi VM, Ratner N (1990) Angiogenic and invasive properties of neurofibroma Schwann cells. J Cell Biol 111:645–653
Snider P, Olaopa M, Firulli AB, Conway SJ (2007) Cardiovascular development and the colonizing cardiac neural crest lineage. ScientificWorldJournal 7:1090–1113
Sørensen SA, Mulvihill JJ, Nielsen A (1986) Long-term follow-up of von Recklinghausen neurofibromatosis: survival and malignant neoplasms. N Engl J Med 314:1010–1015
Stewart DR, Cogan JD, Kramer MR et al (2007) Is pulmonary arterial hypertension in neurofibromatosis type 1 secondary to a plexogenic arteriopathy? Chest 132:798–808
Strom A, Wigren M, Hultgardh-Nilsson A et al (2007) Involvement of the CD1d-natural killer T cell pathway in neointima formation after vascular injury. Circ Res 101:e83–e89
Swirski FK, Libby P, Aikawa E et al (2007) Ly-6Chi monocytes dominate hypercholesterolemia-associated monocytosis and give rise to macrophages in atheromata. J Clin Invest 117:195–205
Tedesco MA, Di Salvo G, Natale F et al (2002) The heart in neurofibromatosis type 1: an echocardiographic study. Am Heart J 143:883–888
Tedesco MA, Di Salvo G, Natale F, Graziano L, Grassia C, Calabrò R, Lama G (2005) Early cardiac morphologic and functional changes in neurofibromatosis type 1 hypertensives: an echocardiographic and tissue Doppler study. Int J Cardiol 101:243–247
Ullrich NJ, Robertson R, Kinnamon DD et al (2007) Moyamoya following cranial irradiation for primary brain tumors in children. Neurology 68:932–938
Viskochil D (2002) Genetics of neurofibromatosis 1 and the NF1 gene. J Child Neurol 17:562–570, discussion 71–72, 646–651
Wang Y, Nicol GD, Clapp DW, Hingtgen CM (2005) Sensory neurons from Nf1 haploinsufficient mice exhibit increased excitability. J Neurophysiol 94:3670–3676
Wu M, Wallace MR, Muir D (2006) Nf1 haploinsufficiency augments angiogenesis. Oncogene 25:2297–2303
Xu J, Ismat FA, Wang T et al (2007) NF1 regulates a Ras-dependent vascular smooth muscle proliferative injury response. Circulation 116:2148–2156
Yang FC, Ingram DA, Chen S et al (2008) Nf1-dependent tumors require a microenvironment containing Nf1+/−- and c-kit-dependent bone marrow. Cell 135:437–448
Zenker M (2011) Clinical manifestations of mutations in RAS and related intracellular signal transduction factors. Curr Opin Pediatr 23:443–451
Zhang LN, Parkinson JF, Haskell C, Wang YX (2008) Mechanisms of intimal hyperplasia learned from a murine carotid artery ligation model. Curr Vasc Pharmacol 6:37–43
Zhu Y, Ghosh P, Charnay P et al (2002) Neurofibromas in NF1: Schwann cell origin and role of tumor environment. Science 296:920–922
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Stansfield, B.K., Ingram, D.A., Conway, S.J., Friedman, J.M. (2012). Molecular Basis of Cardiovascular Abnormalities in NF1. In: Upadhyaya, M., Cooper, D. (eds) Neurofibromatosis Type 1. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-32864-0_23
Download citation
DOI: https://doi.org/10.1007/978-3-642-32864-0_23
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-32863-3
Online ISBN: 978-3-642-32864-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)