
Abstract
This chapter presents the diagnostic criteria, treatment planning, and surgical protocols for the application of computer-assisted surgical simulation (CASS) for patients requiring TMJ total joint replacement and orthognathic surgery (C-TJR-OS). The CASS protocol decreases the preoperative workup time and increases the accuracy of model preparation and subsequent surgery.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Patients with temporomandibular joint (TMJ) pathology and coexisting dentofacial deformities can be corrected with concomitant TMJ and orthognathic surgery (C-TMJ-OS). Systematic TMJ and craniofacial analysis utilizing radiographic and clinical findings are critical in the decision-making on whether to proceed with isolated orthognathic surgery or in combination with total joint replacement (TJR). Surgical alterations utilizing C-TMJ-OS can help restore facial esthetics, improve airway and mastication function, provide a stable occlusion, and eliminate pain. C-TMJ-OS can be completed in one surgical stage or separated into two surgical stages. The two-stage approach requires the patient to undergo two separate operations (one surgery to correct the TMJ pathology and a second operation to perform the orthognathic surgery) and two general anesthetics, significantly lengthening the overall treatment time and increasing possible risks. Performing C-TMJ-OS in a single operation decreases treatment time, provides better clinical outcomes, but requires careful treatment planning and surgical proficiency in the two surgical areas.
This chapter presents the diagnostic criteria, treatment planning, and surgical protocols for the application of computer-assisted surgical simulation (CASS) for patients requiring TMJ total joint replacement and orthognathic surgery (C-TJR-OS). The CASS protocol decreases the preoperative workup time and increases the accuracy of model preparation and subsequent surgery.
2 Indications for C-TJR-OS
Temporomandibular joint (TMJ) disorders or pathology and dentofacial deformities commonly coexist. The TMJ pathology may be the causative factor of the jaw deformity or develop as a result of the jaw deformity, or the two entities may develop independent of each other. The most common TMJ pathologies that can adversely affect jaw position, occlusion, and orthognathic surgical outcome stability include (1) articular disc dislocation, (2) adolescent internal condylar resorption (AICR), (3) osteoarthritis, (4) reactive arthritis, (5) condylar hyperplasia, (6) ankylosis, (7) congenital deformation or absence of the TMJ, (8) tumors, (9) connective tissue and autoimmune diseases, (10) trauma, and (11) other end-stage TMJ pathologies [1,2,3,4]. These TMJ conditions can be associated with dentofacial deformities, malocclusion, TMJ pain, headaches, myofascial pain, TMJ and jaw functional impairment, ear symptoms, sleep apnea, etc. Patients with these conditions may benefit from corrective surgical intervention, including TMJ and orthognathic surgery. Some of the aforementioned TMJ pathologies may have the best outcome prognosis using custom-fitted total joint prostheses for TMJ reconstruction. This chapter is designed to improve the surgeon’s ability to recognize TMJ conditions that may be best treated with concomitant TMJ total joint prostheses and orthognathic surgery.
Some clinicians choose to ignore the TMJ pathology and symptoms, preferring to perform only orthognathic surgery for these types of cases. However, this treatment philosophy can result in continuation or exacerbation of the presurgical TMJ pathology and adverse outcomes. Although most TMJ patients have associated symptoms, approximately 25% of patients with significant TMJ pathology/disorders may be asymptomatic presurgically. These patients are diagnostically challenging when undergoing orthognathic surgery because the TMJ pathology may not be recognized. Failure to recognize and properly treat the TMJ pathology in symptomatic or asymptomatic patients will commonly result in poor treatment outcomes including potential redevelopment of the skeletal and occlusal deformity by continued condylar resorption or condylar overdevelopment, initiation of or worsening pain, headaches, and jaw and TMJ dysfunction, as well as other TMJ symptoms [5]. However, there are clinical and imaging factors that can indicate the presence of TMJ pathology in the asymptomatic as well as the symptomatic patient.
Approximately two-thirds of the patients requiring total joint prostheses can benefit from concomitant TMJ and orthognathic surgery for improvement in jaw function, airway and breathing capabilities, improved esthetics, and decreased or elimination of pain.
3 Disc Displacement
When determining the presence of TMJ pathology, it is important to appreciate the normal TMJ anatomy (Fig. 10.1). When discs are anteriorly displaced for an extended time period, the discs may become nonreducing, deformed with loss of the intermediate zone and thickening of the posterior and anterior bands (Fig. 10.2). Also, there may be a degenerative process developing in the discs where there is a breakdown of the cartilaginous substance with vascular invasion and degeneration. Displaced discs initiate a cascade of events that lead to TMJ arthritis. When discs are displaced and become nonreducing, the degenerative process of the disc progresses more rapidly as compared to displaced discs that reduce. When discs advance to a certain level of deformation and degeneration, they become non-salvageable requiring patient-fitted total joint prostheses to produce the most predictable and high-quality outcomes.


MRI of a normal TMJ in closed position with disc in position. The anatomical landmarks are labeled


MRI showing arthritic condyle and the articular disc are anteriorly displaced, significantly deformed, degenerated, nonreducing, and non-salvageable
4 Adolescent Internal Condylar Resorption (AICR)
Adolescent internal condylar resorption (AICR) is a condition that develops usually during pubertal growth between the ages of 11 and 15 years and predominantly in females (ratio, 8:1 females to males) [1,2,3,4, 6]. Clinically, the mandible will be noted to slowly retrude into a Class II occlusal and skeletal relationship with a tendency toward anterior open bite. These patients all have high occlusal plane angle facial morphological profiles. On the MRI, these cases present with a condyle that is slowly becoming smaller in size in all three planes of space and the disc is anteriorly displaced (Fig. 10.3). In some cases, there is significant thinning of the cortical bone on top of the condyle contributing to the inward collapse of the condylar head in this pathological process. The articular discs are anteriorly displaced and may or may not reduce on opening. Commonly, the disc become nonreducing relatively early in the pathological progression. Nonreducing discs will degenerate and deform at a more rapid rate as compared to discs that reduce. AICR stabilization may be achieved with disc repositioning if it is performed within 4 years of the onset of the disc displacement. After around 4 years from the onset of disc displacement, the discs may become non-salvageable, and condyles significantly resorbed with the indicated treatment transitioning to patient-fitted total joint prostheses to repair the TMJs and advance the mandible concomitant with orthognathic surgery.


MRI of TMJ demonstrating adolescent internal condylar resorption (AICR) with condylar resorption and an anterior displaced articular disc. These discs can become nonreducing relatively early on in the process. Note the thinness of the cortical bone on the superior surface of the condyle and amorphous tissue surrounding the condyle
5 Arthritis
Various types of arthritic pathologies including osteoarthritis, rheumatoid arthritis, and spondyloarthropathies, such as reactive arthritis, may affect the TMJs. These TMJ disorders are discussed in detail in earlier chapters, but a brief review is presented here. Osteoarthritis is the most common type of TMJ arthritis and is characterized by a progressive degeneration of articular disc leading to direct contact of the condyle with the fossa and gradual erosion. Rheumatoid arthritis is an autoimmune disease that may present as an acute onset of bilateral TMJ disease with erosion of the complex. Juvenile rheumatoid arthritis is a progressive Class II malocclusion and apertognathia due to condylar destruction and may lead to ankylosis in late stages. Medical management has decreased the need for surgical intervention [7]. Reactive arthritis is commonly caused by bacterial or viral entities [1,2,3,4, 8,9,10,11] and may show a localized area of inflammation (synovitis) with erosion of the condyle and/or fossa. It also can present as a more profuse inflammatory process through the bilaminar tissues, capsule, surrounding the disc (Fig. 10.4a), but can progress to destruction of the disc and condylar resorption (Fig. 10.4b). The most common bacteria causing reactive arthritis in the knees and TMJs are Chlamydia trachomatis and Chlamydia pneumoniae [10,11,12], as well as Mycoplasma genitalium [11]. These are non-culturable, non-motile, obligate intracellular bacteria that stimulate production of pro-inflammatory/pain mediators—TNFα, cytokines, chemokines, substance P, etc.—with subsequent breakdown of the cartilage and bone and generation of pain. Standard antibiotic therapy can be effective for urinary tract, genital, ocular, respiratory, and GI infections involving these bacteria, but are not effective for synovial infections, making it very difficult to eliminate these bacteria from joints including the TMJs [12]. Currently, there are no predictable methods to conservatively treat reactive arthritis involving these particular bacteria. However, when the infection is confined to a small portion of the synovial and bilaminar tissues in the TMJ, debridement may be indicated, but outcomes may be unpredictable. With evidence of arthritic TMJ changes and particularly with destruction of the TMJ tissues, a total joint prosthesis provides the highest predictable outcomes.


(a) T2 MRI of TMJ with relatively early initiation of reactive arthritis. The articular disc is anteriorly displaced (red arrows), and the onset of condylar resorption at anterior aspect of the condyle (yellow arrow) is noted. The synovitis appearing as “gray to white” tissue (green arrow) is surrounding the anterior condyle and superior aspect of the disc. (b) MRI of advanced reactive arthritis with the synovitis (blue arrows) filling the fossa, destruction of the articular disc, and condylar resorption (yellow arrow)
6 Perforations
Perforations can occur in the TMJ area resulting in bone-on-bone contact. Disc perforations can occur following anterior and/or medial disc displacement. Almost always these perforations are posterior to the posterior band of the articular disc or lateral to the disc, and rarely do perforations occur through the disc itself (Fig. 10.5). Clinically, crepitation will usually be present, and, on the MRI, there will be evidence of bone-on-bone contact, arthritis of the condylar head and/or fossa, as well as anteriorly and/or medially displaced disc. If the disc becomes non-salvageable, a total joint prosthesis may be indicated.


MRI of left arthritic condyle with perforation of the bilaminar tissue posterior to the anteriorly displaced disc. Bone-to-bone contact of the condyle and fossa is observed with crepitation on jaw function
7 Connective Tissue/Autoimmune Diseases
The MRI presentation of connective tissue/autoimmune diseases can be pathognomonic. In these conditions, the articular disc oftentimes is in a relatively normal position, but there is progressive condylar resorption, “mushrooming” of the remaining condyle and often resorption of the articular eminence, with slow but progressive destruction of the articular disc that is surrounded by a reactive pannus [13] (Fig. 10.6a–c). This presentation almost always indicates the requirement of total joint prostheses for jaw reconstruction to eliminate the pathologic process in the joint and develop predictable stability [1,2,3,4, 13,14,15,16,17]. The use of autogenous tissues in this scenario could result in the disease process attacking autogenous tissues placed into the joint with subsequent failure.


(a) MRI of TMJ with juvenile idiopathic arthritis (JIA). The sagittal view demonstrates that the disc is commonly in position but surrounded by a reactive pannus (gray tissue around the degenerated disc and condyle) that destroys the disc, condyle, and articular eminence. The remaining condyle has a “mushroom” appearance. (b) The condyle and disc are outlined in orange. (c) Coronal view showing the extreme narrowness of the residual condyle
8 Trauma
Traumatic injuries to the jaws may develop facial deformities, particularly those that involve the TMJs with unilateral or bilateral condylar or subcondylar fractures that are inadequately reduced. Patients may present with (1) mandible retruded or deviated toward the affected side, if unilateral, (2) pain and jaw dysfunction, (3) deficient growth on the affected side(s) in growing patients, (4) Class II skeletal and occlusal relationships, and (5) premature contact of the occlusion on the affected side(s) and open bite (Fig. 10.25a–c). Imaging features could include (1) evidence of previous condylar, mandibular, or midfacial fractures; (2) the condyle, when fractured, may be malpositioned downward, forward, and medial to the fossa; and (3) decreased vertical ramus/condyle length. MRI aids in showing the disc position and condition. At the initial presentation of the trauma, the options for treating subcondylar fractures are open reduction, closed reduction, or no treatment. The amount of displacement and the condition of the fracture(s) affect the treatment needed to fix the problem. When identified early, fractures may be best treated by open reduction for significantly displaced segments or closed reduction for minimally displaced segments to achieve a symmetric face and stable occlusion. If the condyle has healed in a minimally to moderately displaced position and the articular disc is salvageable, then orthognathic surgery could realign the jaw structures in the proper orientation. If the condyle is severely deformed and non-salvageable, then the most predictable reconstruction of the TMJ and repositioning of the mandible are using patient-fitted total joint prostheses (TMJ Concepts system) and fat grafts (see Figs. 10.21a–c and 10.22a–d). Other treatment options for TMJ reconstruction include rib grafts and sternoclavicular grafts.
9 Ankylosis
Temporomandibular joint (TMJ) heterotopic bone refers to calcifications that develop in and around areas of the joint that are normally void of the bone. The development of heterotopic bone within the confines of a joint or in the surrounding area can cause joint dysfunction, pain, and progression to ankylosis.
Temporomandibular joint ankylosis is a condition where the condyle is fused to the fossa by bony or fibrotic tissues creating a debilitating, painful condition that can interfere with jaw function, mastication, speech, oral hygiene, growth and development, breathing, and normal life activities (Fig. 10.7). There are numerous surgical techniques that have been proposed to manage heterotopic bone and TMJ ankylosis with varying outcomes reported. The most common complications following the treatment of ankylosis are limited jaw function, pain, and re-ankylosis [18, 19].


Bony ankylosis of the right TMJ is noted creating severe limitation of jaw function and opening
The formation of TMJ heterotopic bone and ankylosis is most commonly caused from trauma but can also be related to inflammation or bone growth stimulation related to various TMJ pathologies such as infection, reactive arthritis, osteoarthritis, inflammatory conditions, connective tissue/autoimmune diseases (e.g., juvenile idiopathic arthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, scleroderma, etc.), endocrine and metabolic disorders, multiply operated joints, foreign-body giant-cell reaction, repeated injections of medications into the TMJ (i.e., steroids), as well as unsuccessful previous TMJ surgeries including failed TMJ autogenous grafts and alloplastic implants. In the initial phases, heterotopic bone may be asymptomatic. However, with further progression, the excess bone can create pain, decrease range of motion, and lead to ankylosis (Fig. 10.7). A variable amount of fibrosis and reactive tissue are normally associated with heterotopic bone, thereby worsening the adverse effects.
Bleeding into a joint by trauma or a surgical procedure, the presence of dead space following extensive TMJ debridement, or reconstruction with autogenous bone or total joint prosthesis can lead to blood clot formation in the joint area, with subsequent organization. Pluripotent cells can then migrate into the area and differentiate into fibroblasts and osteoblasts, leading to deposition of collagen and then the bone. This results in the potential development of heterotopic bone and ankylosis. In excessively fibrotic joints, the tissue vascularity decreases with resultant decrease in oxygen tension in the surrounding tissue, which can lead to the transformation of fibrous tissue into the cartilage and bone with potential for ankylosis. Temporomandibular joint ankylosis can be even more devastating in growing patients resulting in a profound dentofacial deformity in addition to jaw dysfunction and malocclusion [20]. Effective and predictable treatment of ankylosis includes TMJ reconstruction with total joint prostheses and fat grafting [19].
10 Craniofacial Anomalies/Obstructive Sleep Apnea
Patients may require C-TJR-OS when treating temporomandibular joint disorders in combination with other factors such as A-P hypoplasia of the maxilla and mandible, craniofacial anomalies, decreased oropharyngeal airway, and sleep apnea issues. Patients with TMJ pathologies, particularly those with condylar resorption, may experience progressively worsening breathing and sleep apnea issues due to progressive mandibular retrusion and posterior mandibular vertical collapse. Craniofacial patients, such as Treacher Collins syndrome, Pierre Robin sequence, and hemifacial microsomia, often present with hypoplastic condyle and mandible which lead to functional (mastication and breathing) disorders. Treatment options that have been applied to these patients’ conditions include distraction osteogenesis, costochondral reconstruction, early-stage orthognathic surgery, or TMJ total joint prostheses. When these techniques are used on growing patients, secondary procedures commonly are required following growth completion. Once the patients have completed growth, definitive treatment can be implemented that may involve alloplastic TMJ reconstruction with orthognathic surgery.
Patients with sleep apnea symptoms may require further diagnostic workup including polysomnography and drug-induced sleep endoscopy. Many patients diagnosed with sleep apnea also have TMJ issues that need to be addressed at the same time or before the orthognathic surgery is performed to provide a stable and predictable outcome. Advancing the maxillary and mandibular complex with simultaneous counterclockwise rotation improves facial balance and significantly opens the oropharyngeal airway [21,22,23,24,25,26]. Double-jaw surgery with counterclockwise rotation of the maxillomandibular complex will increase the oropharyngeal airway of approximately 65–70% for the first 10 mm of mandibular advancement [27,28,29,30,31]. With 10–15 mm of advancement, the oropharyngeal airway continues to open, but at a lesser percentage ranging from 55 to 60% of the mandibular advancement. When the mandible is advanced 15–20 mm, the oropharyngeal airway continues to open but only about 40–45% of the amount of mandibular advancement. Later in this chapter, Cases 1, 2, and 3 illustrate successfully treated patient with TMJ pathology and obstructive sleep apnea utilizing the one-stage concomitant total joint replacement and orthognathic surgery.
11 Patient Evaluation
It is important to know the patient’s concerns, history, symptoms, and treatment expectations. Although previous publications further detail information on patient evaluation for orthognathic, TMJ, and sleep apnea surgery including clinical, radiographic, MRI, and dental model analyses [1,2,3,4, 32], we will briefly discuss the salient points and provide a general overview. A complete structural craniofacial analysis is carried out to determine the degree to which the individual patient varies from his or her “ideal.” This analysis demonstrates all of the maxillofacial deformities and imbalances that require orthodontic and surgical correction. The relative retrusion or protrusion of each facial third in profile and vertical and transverse excess or deficiency of the maxilla and mandible are examined. The anterior facial height is also carefully studied to delineate other skeletal and dental deformities from TMJ pathology resulting in vertical discrepancies. Wolford [33] demonstrated radiographically that the upper anterior face, measured from nasion (Na) to anterior nasal spine (ANS), constitutes 45% of the total anterior facial height and that the lower anterior facial height, measured from ANS to menton (Me), constitutes 55%. Delaire and Schendel [34,35,36] have confirmed via architectural and structural craniofacial analysis that these percentages represent constants of ideal vertical facial height.
It is imperative for the clinician to realize that patients with TMJ pathology and dentofacial deformities (often with retruded mandible) are sometimes misleading in their clinical presentation because their “natural head position” may posture their head hyperextended, resulting in the lower jaw and chin tipped upward and forward to make the chin appear more prominent and to open the oropharyngeal airway to improve their ability to breathe. If the patients are not evaluated with a properly corrected head position, the amount and degree of maxillary and mandibular retrusion and asymmetry may be missed. Therefore, it is important that the clinician evaluates the patient with the pupillary plane and ear plane parallel to the floor in the frontal view (Fig. 10.8a) and clinical Frankfort horizontal plane (a line from the tragus of the ear through the bony infraorbital rim) parallel to the floor in the profile view (Fig. 10.8b). Obviously there will be some variance in individuals, but this is a basic guide.


(a) Patients should be evaluated in the frontal view with pupillary plane and ear plane relatively parallel to the floor with understanding there are variations in symmetry in this view. (b) In profile, patients should be evaluated with clinical Frankfort horizontal plane (a line from the tragus of the ear through the bony inferior orbital rim) parallel to the floor for assessment of A-P and vertical facial balance
12 Imaging
Radiographic evaluation is critical in the diagnostic process. Various imaging modalities provide different views of the soft and hard tissues in the craniofacial complex that allows for assessment of pathological conditions and deviation of the bony relationships from the relative normal values. Imaging options include panoramic and cephalometric X-rays, TMJ tomograms, cone beam CT, traditional CT scans, bone scans, and magnetic resonance imaging.
12.1 CT Imaging
Three-dimensional (3-D) imaging with CT scan allows for analysis of the TMJ, of the positioning between the maxilla, mandible, and cranial base, and of the oropharyngeal and nasal airways. Cone beam computed tomography (CBCT) provides low-cost and low-radiation scans when compared to traditional CT scans. Either CBCT or traditional CT scans can be used as part of the diagnostic and planning process. Craniofacial data obtained from cephalometric and CT scan analysis is integrated to determine the treatment plan and simulate the surgical movements using virtual planning. 3-D modeling of the surgical movements, which provides the new position of the jaws and joints, is necessary for manufacture of patient-fitted TMJ total joint prostheses.
12.2 MRI Evaluation
Magnetic resonance imaging (MRI) is one of the most important diagnostic tools to evaluate and diagnose and treatment plan for TMJ pathology. MRI evaluates bone and soft tissue structures, TMJ disc position, morphology, mobility, extent of joint degenerative changes, inflammation, the presence of connective tissue/autoimmune diseases, and other pathologies. It aids in the diagnosis of TMJ disorders in patients with “silent joints” that may not make noise or cause pain but have presence of disc displacement and degenerative changes. If the TMJ pathology is not treated in these patients, then the diseased joints may contribute to poor outcomes when only orthognathic surgery is performed.
In general, T-1 MRIs are helpful in identifying disc position and morphology, the presence of alteration in bone and soft tissue structures, and interrelationships of the bony and soft tissue anatomy. T-2 MRIs are more helpful in identifying inflammatory responses in the TMJ, such as effusions, synovitis, etc. 1.5–3.0 T MRI machines are recommended for MRI evaluation of the TMJs. “TMJ coils” are necessary to achieve diagnostic quality images of the TMJs. The basic views that are most helpful in diagnoses include (1) sagittal views in centric relation as well as in maximum opening, (2) coronal views in centric relation, and (3) dynamic views, if available. The MRI imaging can be correlated to cone beam imaging of the TMJs for joint space evaluation and greater interpretation of bony pathology. Figure 10.1 shows a normal TMJ MRI with healthy anatomical structures and relative positioning. Later, this chapter will also discuss examples of TMJ conditions where the MRI provides guidance in determining the appropriate surgical treatment option.
12.3 Cephalometric Analysis
The lateral cephalometric analysis can determine the severity of the jaw deformity, dental alignment, and airway dimensions in the anteroposterior vector. Cephalometric analysis is an important assessment for diagnosis and treatment planning for TMJ patients because the most dominant facial type that experiences TMJ pathology is the high occlusal plane angle facial morphology with a retruded maxilla and mandible. Normal cephalometric relationships have been described in detail in previously published papers [3, 32].
One of the primary factors contributing to sleep apnea is a decreased oropharyngeal airway that is commonly seen in TMJ patients, specifically with a history of TMJ condylar resorption. The normal cephalometric A-P dimension from the posterior pharyngeal wall to the soft palate and posterior pharyngeal wall to the base of the tongue is 11 mm, plus or minus 2 mm. In patients who have a retruded maxilla and mandible, this airway may be significantly decreased. The airway size and length increase until age 20, at which time there is a variable period of stability, after which the airway at first decreases slowly in size and then, after age 50, more rapidly [37]. Accompanying these deficiencies is usually a high occlusal plane angle. The normal cephalometric angle of the occlusal plane to the Frankfort horizontal plane is 8°±4°. Cephalometric analysis depicting a significantly increased occlusal plane is commonly seen with a retruded maxilla and mandible (particularly with condylar resorption) and should be addressed in the treatment planning.
13 Comprehensive Diagnostic List and Treatment Plan
Following completion of all necessary and required evaluations, a comprehensive diagnostic list can be compiled. A definitive treatment plan can then be established to address these issues and other treatment options that may be available to allow the patient to make an informed decision as to the preferred treatment.
The following triad of factors are commonly encountered in the diagnostic list of TMJ patients: (1) A high occlusal plane angle facial morphology associated with retruded maxilla and mandible with an accompanying decreased oropharyngeal airway, (2) nasal airway obstruction related to hypertrophied turbinates and/or nasal septal deviation or spurring, and (3) TMJ pathology. A recent study evaluated 1234 consecutive patients referred for orthognathic surgery requiring at least maxillary osteotomies [36]. There were 603 patients (49%) with hypertrophied turbinates requiring partial turbinectomies and 278 patients (23%) required nasal septoplasty. For patients requiring partial turbinectomies (n = 603), 84% had maxillary hypoplasia, 72% had mandibular hypoplasia, 69% had a high occlusal plane angle, and 49% of the patients required C-TMJ-OS. Furthermore, a female predominance was seen in the data reviewed. Sixty-seven percent of the turbinectomy cases and 73% of concomitant turbinectomy and orthognathic and TMJ surgery cases involved female subjects. A strong correlation has been established between hypertrophied inferior turbinates, hypoplastic maxilla and mandible, and a steep occlusal plane. The findings of this study correlate with other studies evaluating the morphology of mouth breathing and nasally obstructed patients [38,39,40,41,42]. Therefore, patients with the high occlusal plane angle facial morphology with a retruded maxilla and mandible should be assessed for nasal airway obstruction, decreased oropharyngeal airway and sleep apnea, as well as TMJ pathology including asymptomatic patients.
14 Age for Surgical Intervention
Although there are individual variations, females usually have the majority of their facial growth (98%) complete by the age of 15 years and males by the age of 17–18 years [43]. Predictability of results and limiting corrections of the jaw and TMJ pathology related deformities to one major operation can best be achieved by waiting until growth is relatively complete if only the TMJ total joint prostheses are placed without maxillary surgery, particularly if only a unilateral prosthesis is required. However, there are definite indications for performing surgery during the growing years such as progressive TMJ deterioration, ankylosis, masticatory dysfunction, tumor removal, pain, sleep apnea, etc. Performing surgery during growth may result in the need for additional surgery at a later time to correct a resultant deformity and malocclusion that may develop. Additional surgery is a greater probability with unilateral prosthesis and a normal contralateral TMJ if surgery is performed during the growing years. In addition, some orthognathic surgical procedures, such as maxillary Le Fort 1 osteotomies, have a profound effect on subsequent facial growth and development where maxillary anterior-posterior growth is stopped. However, the vertical alveolar growth of the maxilla and mandible continues contributing to a downward and backward rotation vector of facial growth with maintenance of occlusion. Therefore, bilateral TMJ patient-fitted total joint prostheses and maxillary osteotomies can be done at an earlier age with predictable results. If repeat orthognathic surgery is required at a later time, the advancement of the mandible with the TMJ total joint prosthesis can be accomplished by one of four surgical options: (1) intraoral mandibular ramus sagittal split osteotomy; (2) extraoral mandibular ramus sagittal split osteotomy; (3) advance the mandible forward relative to the prosthesis by removing the screws from the mandibular component, separate it from the ramus, advance the mandible along the patient-fitted prosthesis, and re-fixate the prosthesis to the mandible with bone screws in its new position (can usually work for only smaller advancements); or (4) replace the mandibular component of the total joint prosthesis with a new longer custom fabricated mandibular component that would be reattached to the mandibular ramus after the mandible is moved into its new position.
Previous publications have described the effects of maxillary and mandibular orthognathic surgery on growth with guidelines for age considerations for surgical intervention [44,45,46] as well as the effects of TMJ surgery on facial growth [20] and will not be further discussed here. Later in this chapter, Case 2 illustrates successfully treated juvenile idiopathic arthritis (JIA) patient (age 16) utilizing the one-stage concomitant total joint replacement and orthognathic surgery with good functional and esthetic results without requiring secondary procedures [13]. These cases are predictable when performed at age 13 years or older in females and 15 years or older in males. However, the vector of facial growth will change in younger patients to a downward and backward direction.
15 High Occlusal Plane Facial Morphology
The common functional and esthetic characteristics of the high occlusal plane facial morphology generally include the following:
-
1.
Increased occlusal plane angulation (occlusal plane greater than 12°).
-
2.
Increased mandibular plane angulation.
-
3.
Anterior vertical maxillary hyperplasia and/or posterior vertical maxillary hypoplasia.
-
4.
Increased vertical height of the anterior mandible and/or decreased vertical height of the posterior mandible.
-
5.
Decreased projection of the chin (anteroposterior microgenia).
-
6.
Anteroposterior and vertical posterior mandibular and maxillary hypoplasia.
-
7.
Decreased angulation of maxillary incisors, although overangulation can occur.
-
8.
Increased angulation of mandibular incisors.
-
9.
Class II malocclusion is common, although Class I and Class III malocclusions also can occur.
-
10.
An anterior open bite may be accompanied by an accentuated curve of Spee in the upper arch.
-
11.
Loss of incisal guidance, loss of canine rise occlusion, and the presence of working and non-working dental interferences in the molar areas may occur in more pronounced cases in which the occlusal plane approaches the slope of the articular eminence.
-
12.
More severe cases may demonstrate moderate to severe sleep apnea symptoms as a result of the tongue base and soft palate displaced posteriorly and constricting the oropharyngeal airway (normal oropharyngeal airway space is 11 ± 2 mm).
-
13.
Nasal airway obstruction related to hypertrophied turbinates and/or septal deviation or spur.
-
14.
TMJ pathology.
16 Occlusal Plane Angle
The correction of dentofacial deformities often requires double-jaw surgery to achieve a harmonious result when addressing the function, esthetic, and airway needs. An often ignored but important cephalometric and clinical interrelationship in the diagnosis and treatment planning for the correction of dentofacial deformities is the occlusal plane angulation [32, 47,48,49]. The occlusal plane angle is formed by the Frankfort horizontal plane and a line tangent to the cusp tips of the lower premolars and the buccal groove of the second molar. The normal value for adults is 8 ± 4°. An increased (high) occlusal plane angle usually is reflected in an increased mandibular plane angle (dolicocephaly), and a decreased (low) occlusal plane angle usually correlates with a decreased mandibular plane angle (brachycephaly). Patients may benefit functionally and esthetically with surgical alteration of the occlusal plane.
17 Surgical Decrease of the Occlusal Plane
In the high occlusal plane patients, the indicated surgical correction may include a counterclockwise rotation of the maxillomandibular complex. In open bite cases, the maxillary occlusal plane and the mandibular occlusal plane may be different, and each should be evaluated independently. For illustrative purposes, a Class I case is used with the maxillary incisor edge as the center of rotation for counterclockwise rotation (Fig. 10.9). The anatomical changes that occur include the following: (1) occlusal plane angle decreases; (2) mandibular plane angle decreases; (3) maxillary incisor angulation increases (the same amount that the maxillary occlusal plane decreases); (4) mandibular incisor angulation decreases (the same amount that the mandibular occlusal plane decreases); (5) projection of the chin increases relative to the lower incisor edges; (6) posterior facial height increases; (7) vertical prominence of the mandibular angles increases; (8) maxillary incisor edges move forward relative to the perinasal area; (9) incisal guidance and canine rise occlusion improve, and posterior working and non-working interferences are eliminated; and (10) oropharyngeal airway increases.


Surgical decrease of the occlusal plane from the dotted line to solid line (counterclockwise rotation) rotates the chin forward, decreased prominence of the perinasal areas, maxillary incisor angulation increases, mandibular incisor angulation decreases, and the oropharyngeal airway increases
The center of rotation affects the esthetic relationship of the jaws with the other facial structures. In the illustrative case (Fig. 10.9), the center of rotation is at the maxillary incisor edge. Counterclockwise rotation of the maxillomandibular complex results in the perinasal area, subnasale area, and the nasal tip moving posteriorly, but the mandible and chin come forward. If rotation is around point A or higher, then the perinasal area and the nose are less affected, but the mandible, chin, and maxillary incisor edges come further forward, increasing the anteroposterior support to the upper and lower lip (Fig. 10.10). This demonstrates the significant esthetic difference that the alteration of the occlusal plane can make by rotating at different points of rotation [32, 47,48,49]. When decreasing the occlusal plane angle and advancing the mandible counterclockwise, the oropharyngeal airway increases approximately 50–70% of the mandibular advancement measured at the genial tubercles for the first 10 mm of forward movement [27,28,29,30,31].


When the point of rotation is moved upward above the maxillary osteotomy level and counterclockwise rotation of the maxillomandibular complex is completed, all structures below that point move forward including the maxilla, mandible, and teeth, with the greatest forward movement at menton
18 Concomitant TMJ Total Joint Replacement and Orthognathic Surgery (C-TJR-OS)
Treatment planning for C-TJR-OS cases is based on cephalometric and 3-D analysis, prediction tracing, clinical evaluation, and dental models, which provide the templates for movements of the upper and lower jaws to establish optimal treatment outcome in relation to function, facial harmony, occlusion, and oropharyngeal airway dimensions. For patients who require total joint prostheses, a medical-grade computed tomographic (CT) scan with 1 mm overlapping cuts is recommended of the maxillofacial region that includes the TMJs, maxilla, and mandible. The surgeon has two options for model preparation to aid in the construction of patient-fitted total joint prostheses using the TMJ Concepts system (Ventura, CA). Previously published articles have detailed the traditional protocol technique versus the computer-assisted surgical simulation (CASS) protocol. The CASS technique is also known as virtual surgical planning (VSP) [50, 51]. In this chapter, we will present only the CASS technique.
Over the past decade, CASS technology has been integrated to many maxillofacial surgical applications [52, 53], including dentofacial deformities, congenital deformities, treatment of obstructive sleep apnea, defects after tumor ablation, post-traumatic defects, reconstruction of cranial defects [54], and reconstruction of the TMJ [55]. CASS technology can improve surgical accuracy, provide intermediate and final surgical splints, and decrease the surgeon’s time input for presurgical preparation compared with traditional methods of case preparation [50, 51]. C-TJR-OS involves intricate surgical steps that must be judicially planned and executed.
19 Protocol for C-TJR-OS Using CASS
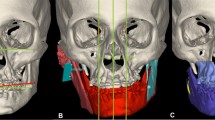
To prepare for C-TJR-OS cases using CASS, a medical-grade CT scan is obtained, and the Digital Imaging and Communications in Medicine (DICOM) data is then sent to a VSP company. The CASS technology is utilized by several different VSP companies including 3D Systems (formerly Medical Modeling), ProtoMED, Materialize, and ProPlan. The orthognathic surgery is planned using CASS technology by moving the maxilla and mandible into their final positions in a computer-simulated environment (Fig. 10.11a–c). Using the computer simulation, the anteroposterior and vertical positions, pitch, yaw, and roll are accurately finalized for the maxilla and mandible based on clinical evaluation, dental models, cephalometric analysis, prediction tracing, and computer simulation analysis.


Staged computer-aided surgical simulation (CASS). (a) Simulated preoperative position of the maxilla and mandible. (b) The maxilla and mandible in the simulated intermediate position, with the maxilla in it’s original position, but mandible in it’s final position with the mandibular surgery performed first for fabrication of the intermediate splint (red simulated splint). (c) The final position of maxilla and mandible, after counterclockwise rotation advancement of the mandible and segmented maxilla, for the production of a palatal splint
The stereolithic model is produced with the maxilla and mandible in the final position and provided to the surgeon for removal of the condyle and recontouring of the lateral rami and mandibular fossae if indicated. The stereolithic model is sent to TMJ Concepts (Ventura, CA) for the design, blueprint, and wax-up of the prostheses. Using the Internet, the design is sent to the surgeon for approval. Then, the custom-fitted total joint prostheses are manufactured (Fig. 10.12). It takes approximately 12 weeks to manufacture the total joint custom-fitted prostheses.


Stereolithic model fabricated after simulated maxillary and mandibular counterclockwise rotation advancement to the final position. Condylectomy and recontouring of the lateral rami and fossae were performed and prostheses manufactured. The basic design of the TMJ Concepts patient-fitted prosthesis is observed. The black arrow points to the mesh framework on the underside of the custom-fitted titanium shell that secures the polyethylene articulating portion of the fossa component. The yellow arrow points to the mesh on the superior surface of the fossa component that allows osseointegration with the fossa bone. The red arrow points to the posterior stop of the fossa, a necessary component for mandibular advancement and stability. The green arrow shows the bony defect in the lateral maxillary wall created from the counterclockwise rotation of the maxilla. These defects require rigid fixation and bone or synthetic bone grafting for stability of the maxilla
Approximately 2 weeks before surgery, final dental models are produced. If single piece maxillary and mandibular surgery without equilibration is planned, then only one set of models is required. Two sets of maxillary and mandibular models are required if the maxilla or mandible is to be segmented or dental equilibrations are required. One of the maxillary models is segmented if indicated, dental equilibration performed, and segments placed in the best occlusion fit with the mandibular dentition. The maxillary segments are then fixed to each other with glue, wax, or other means that the surgeon prefers. The dental models do not require mounting on an articulator. The three or four models (two maxillary and one mandibular or two mandibular models if equilibrations are done) are sent to a VSP company for scanning and simulation into the computer model. Recent advancements in direct intraoral scanning can also be utilized instead of stone casts for VSP planning. Because the authors routinely perform the TMJ reconstruction and mandibular advancement with the TMJ Concepts total joint prosthesis first, the unsegmented maxillary model is simulated into the original maxillary position, and the mandible is maintained in the final position. The intermediate splint is constructed (Fig. 10.13a–d). Then the segmented maxillary model is simulated into the computer model in its final position, with the maxilla and mandible placed into the best occlusal fit, and the final splint is fabricated (Fig. 10.14a–d). The stereolithic model, dental models, splints, and images of the computer-simulated surgery are sent to the surgeon for implementation during surgery.


(a–d) Intermediate splint is printed from the CASS model with the mandible in the final position and the maxilla in the original position


(a) The final palatal splint is printed for surgical application. (b–d) The palatal splint allows the teeth to fit together maximally and can remain in positon for several months if required for stability and the maxillary segments. If the maxilla is not segmented, then the palatal splint may not be required. It is stabilized to the maxillary arch with light gage wires securing it to the first molars and first bicuspids
19.1 Step-by-Step Methods
-
1.
CT scan of the entire mandible, maxilla, and TMJs (1 mm overlapping cuts).
-
2.
Dental models/dental scans and CT scan sent to VSP company.
-
3.
Processing of DICOM data to create a computer model in CASS environment by the VSP company.
-
4.
Correction of dentofacial deformity, including final positioning of the maxilla and mandible, with computer-simulated surgery.
-
5.
Stereolithic model constructed with jaws in final position and sent to surgeon for condylectomy and rami and fossae recontouring if indicated.
-
6.
Model sent to TMJ Concepts for prostheses design, blueprint, and wax-up.
-
7.
Surgeon evaluation and approval using the Internet.
-
8.
TMJ prostheses manufactured and sent to hospital for surgical implantation.
-
9.
Two weeks before surgery, acquisition of final dental models (two maxillary, one or two mandibular models if dental equilibrations are required); one maxillary model is segmented and models equilibrated if indicated to maximize the occlusal fit; models sent to the company performing the CASS planning.
-
10.
Models incorporated into computer-simulated surgery for construction of intermediate and final palatal splints.
-
11.
Stereolithic model, dental models, splints, and printouts of computer-simulated surgery sent to surgeon.
Using CASS technology for CTOS cases eliminates the “traditional” steps requiring the surgeon to manually set the mandible into its new final position on the stereolithic model, thus saving time and improving surgical accuracy. Although dental model surgery is necessary only if the maxilla requires segmentation or equilibration, the models do not require mounting on an articulator. This saves considerable time by eliminating the time required to mount the models, prepare the model bases for model surgery, reposition the mandible, construct the intermediate occlusal splint, and make the final palatal splint. With CASS technology, the company performing the CASS planning manufactures the splints.
19.2 Surgical Sequencing for C-TJR-OS
-
1.
Condylectomy and discectomy.
-
2.
Coronoidectomy (if mandible significantly advanced or lengthened vertically).
-
3.
Detach the masseter and media pterygoid muscles from the ramus.
-
4.
Modify rami and fossae if indicated from the stereolithic model preparation.
-
5.
Mobilize the mandible.
-
6.
Maxillomandibular fixation with intermediate surgical splint.
-
7.
Placement of total joint prostheses.
-
8.
Bilateral TMJ fat grafts harvested from the abdomen or buttock.
-
9.
Maxillary osteotomies and mobilization.
-
10.
Turbinectomies, septoplasty, etc.
-
11.
Maxillary segmentation and application of the palatal splint if indicated.
-
12.
Maxillary rigid fixation and bone grafting.
-
13.
Adjunctive procedures such as genioplasty, rhinoplasty, UPPP, facial augmentation, etc.
The TMJ Concepts prostheses use design principles and materials that are proven highly successful and are the gold standard in orthopedic joint reconstruction for hip and knee replacements. The prosthesis consists of a fossa component with a commercially pure titanium framework covered with a mesh and an ultra-high-molecular-weight polyethylene functional component fused to the mesh on the bottom side of the framework. The fossa component is attached to the lateral rim of the fossa with four 2-mm-diameter screws. The mandibular component is composed of a titanium alloy shaft with a cobalt-chromium alloy head with the prosthesis secured to the mandibular ramus with seven to nine 2-mm-diameter bicortical screws. The fossa and mandibular components osseointegrate with the fossa and ramus, respectively.
20 Surgical Procedure
-
1.
After surgical prepping including the face, neck, mouth, ears, ear canals, nose, endotracheal tube, and abdomen, the abdomen and the face and neck are draped, and the mouth and nose are isolated by application of a Tegaderm film dressing (Fig. 10.15a), and the ear canal is gently packed with cotton or Xeroform.
-
2.
The TMJs are approached through an endaural (Fig. 10.16) or preauricular incision to perform the condylectomy, discectomy, joint debridement, and coronoidectomy (Fig. 10.17a) (when the mandible is significantly advanced or vertically lengthened). The condylectomy and debridement of the joint are performed first, and then the coronoidectomy is preformed through the endaural incision using a reciprocating saw cutting from the anterior aspect of the coronoid and coursing horizontally across the ramus 5 mm inferior to the sigmoid notch. Using a medial retractor or packing Surgicel or Gelfoam medial to the coronoid will protect the vessels and other soft tissue structures while the cut is made. The coronoidectomy may also be performed after the submandibular approach to the ramus to allow for access to the external carotid artery for urgent ligation in case uncontrollable bleeding is encountered from the maxillary artery and branches. The bone from the condylectomies and coronoidectomies is saved for use in grafting the bone defects that may be associated with the maxillary osteotomies.
Risks associated with this part of the surgery include facial nerve injury and bleeding as the facial nerve branches and maxillary artery and branches are in close proximity. Facial nerve involvement can be minimized by understanding the anatomy, employ small incisions, use of a nerve stimulator when appropriate, careful surgery, and avoid heavy-handed inferior retraction toward earlobe as this can cause damage to the main branch of the nerve. Bleeding may be prevented by using retractors that surround the medial side of the condyle and neck at the time of the condylectomy. Traditionally, reciprocating saw is used for the condylectomy and coronoidectomy. Packing Surgicel or Gelfoam around the medial side of the condylar neck and medial to the ramus, sigmoid notch area, and coronoid will help prevent encountering the major vessels in the area by placing a physical barrier between the bone cuts and the vessels. Using Piezo technology can also be of benefit. For example, the use of the ultrasonic BoneScalpel in TMJ reconstruction results in less blood loss when compared to surgeries employing the use of the conventional reciprocating saw (Fig. 10.17b, c) for completing osteotomies and is now being used more widely in TMJ and orthognathic surgery [56].
Next, the fossa is debrided and recontoured if indicated according to the preparation on the stereolithic model. Generally, 20 mm of space is required between the fossa and the top of the ramus when the mandible is placed in its new position. Be sure to remove an adequate amount of the bone to accommodate the prosthesis; otherwise there could be interferences that won’t allow the prosthesis components to be properly seated.
-
3.
Submandibular incisions (Fig. 10.16) are used to access the ramus to reflect off the masseter and medial pterygoid muscles (if angle significantly advanced or vertically elongated), to recontour the lateral aspect of the ramus if indicated, as well as to mobilize the mandible in a downward and forward direction. Potential risk factors include facial nerve damage and bleeding. The use of a nerve stimulator during dissection to the angle area will help identify the nerve branches and prevent damage. After cutting through the platysma muscle, blunt dissection to the pterygoid-masseteric sling will avoid vascular injury. The lateral aspect of the ramus is prepared by duplicating the alterations on the stereolithic model.
-
4.
The mandibular mobilizer device (KLS Martin, Jacksonville, FL) (Fig. 10.18a) is inserted through the submandibular incision and hooked around the sigmoid notch/condyle area and pulled downward and forward to facilitate vertical lengthening and advancement of the mandibular ramus (Fig. 10.18b, c).
-
5.
The oral cavity is isolated by draping with sterile towels and is exposed by cutting through the Tegaderm from commissure to commissure (Fig. 10.15b). If the case includes bilateral total joint prostheses, the intermediate splint is inserted and maxillomandibular fixation applied. If it is a unilateral total joint prosthesis case, then go to Step 6.
-
6.
For unilateral total joint prosthesis, using separate instrumentation, a contralateral mandibular sagittal split osteotomy is performed and the mandible mobilized on that side. The intermediate splint and maxillomandibular fixation are applied. Rigid fixation is placed to secure the mandibular segments and incision closed.
-
7.
The surgeon changes gloves and gown, face is re-prepped if indicated, and the mouth and nose are sealed off once again with a Tegaderm film dressing.
-
8.
The total joint prostheses are inserted and fixed in position, placing the fossa component first and stabilizing with four, 6-mm-length and 2-mm-diameter screws. The mandibular component is inserted through the submandibular incision and secured with six bicortical 2-mm-diameter screws. A stab incision can be made about 1 cm below the earlobe and a trocar inserted to place screws in the holes at the top of the prosthesis that are difficult to access from the submandibular incision (Fig. 10.19a, b).
-
9.
The submandibular surgical areas are thoroughly irrigated with saline and then betadine solution. The masseter muscles are reattached to the mandible by placing three to four bicortical holes through the inferior aspect of the mandibular angle area where the muscle was originally attached. 2-0 PDS suture is used to tie the masseter muscle to the bone using the transosseous holes (Fig. 10.20a, b). The submandibular incisions are closed in layers.
-
10.
Fat grafts are harvested from the abdomen through incisions in the suprapubic region (Fig. 10.21a–c), previous scar line, umbilical area (Fig. 10.22a–d), or buttock with establishment of good hemostasis and closure of the incisions. A small drain and vacuum bulb can be inserted in the donor area if good hemostasis cannot be achieved.
-
11.
The articulating area of the prosthesis is thoroughly irrigated with saline and then betadine solution through the endaural or preauricular incisions. The fat grafts are packed around the articulating area of the prostheses (Fig. 10.23a–d) and the incisions closed in layers.
-
12.
The oral cavity is then entered, maxillomandibular fixation released, and intermediate splint removed.
-
13.
Maxillary osteotomies are performed and maxilla mobilized. If indicated, intranasal procedures such as turbinectomies and septoplasty are completed.
-
14.
The maxilla is segmented, palatal splint inserted, and maxillomandibular fixation applied. The maxilla is rigidly fixated with four bone plates (Fig. 10.24a, b). Bone grafts are positioned at the osteotomy sites if indicated.
-
15.
The alar base cinch suture is placed, and maxillary incision is closed in a V-Y design.
-
16.
Any other adjunctive procedures can be performed such as genioplasty, rhinoplasty, etc. Special care must be taken to prevent communication with the total joint prosthesis implantation site when performing a concomitant genioplasty procedure by ensuring a conservative posterior dissection along the symphysis/body region. Such a communication could increase the risk of infection.
-
17.
The muscles of mastication including the masseter, medial pterygoid, and temporalis muscles are usually detached. As a result, vertical support to the mandible and occlusion using elastics is required postsurgery. Bone screws or temporary anchoring devices (TADs) can be placed in the alveolar bone area to allow for inter-arch stability through the use of elastics. By shifting the constant inter-arch forces from tooth-borne options to these devices, the teeth are not extruded or displaced. The bone screws or TADs are usually necessary for 2–3 weeks postsurgery until the muscles of mastication can reattach and provide adequate vertical support.


(a) After preparation of the face, neck, ears, and oral cavity, a Tegaderm film dressing, 6 × 8 in., is applied to seal off the oral cavity and nasal airway from the surgical field. (b) Following mobilization of the mandible and preparation to enter the oral cavity to place the intermediate splint, sterile towels are draped around the mouth to prevent contamination of the extraoral surgical sites. The Tegaderm dressing is cut to provide access to the oral cavity for placement of the intermediate splint and maxillomandibular fixation. Following application of the splint and intermaxillary fixation, as well as removal of the towels, a new Tegaderm dressing is placed over the mouth and nose


Incisions for placing the total joint prostheses include an endaural (shown) or preauricular incision as well as a submandibular incision


The condylectomy is performed and joint debrided. (a) A coronoidectomy is indicated if the ramus is to be significantly lengthened vertically or advanced. (b, c) The coronoidectomy is performed through the endaural incision with a reciprocating saw and removed. The bone can be used to graft the maxillary osteotomy bony defects


(a) The mandibular mobilizer (b, c) is inserted through the submandibular incision and hooked over the sigmoid notch area and then pulled downward and forward to mobilize the mandible


(a) A trocar with drill guide and a retractor can be used to provide easy access for placement of screws in the holes at the top of the ramus component of the prostheses. (b) The trocar is inserted through a stab incision about 1 cm below the ear lobe. It is aligned to the hole in the prosthesis, hole drilled, and screw inserted through the trocar


The masseter muscle is reattached to the mandible. (a) Three to four holes are drilled at the bottom of the inferior border. (b) 2-0 PDS suture is used to secure the masseter muscle to the inferior border with continuous or interrupted sutures


(a, b) Fat harvested from the suprapubic area of the abdomen for placement around the articulating area of the prostheses. (c) Hemostasis obtained and incision closed


(a) Umbilical donor site with incision outlined. This donor site is more commonly used for teenage patients. (b) Dissection underway for harvesting of fat. (c) Fat graft being delivered. (d) The incision is closed


(a) Fat harvested from the abdomen for placement around the articulating area of the prostheses. (b) Patient-fitted prosthesis is observed via the endaural incision. (c) Packing the fat into the joint area. (d) Completion of fat packing and ready for incision closure


(a) Left side maxillary osteotomies completed with bone plate stabilization. Bone defects are obvious. (b) Bone grafting completed to provide bone continuity and to enhance healing
21 Special Considerations
A potential risk to patients receiving TMJ total joint prosthesis is infection. The occurrence rate is less than 5% with greater risk for immunodeficient patients and those on immunosuppressant medications such as rheumatoid patients or others with connective tissue/autoimmune diseases. Bacterial or viral contamination of the prosthesis can occur during surgery or develop at a later time from bacterial seeding through a hematological route or localized bacterial sources. As a result, strict adherence to sterile technique for the procedures performed can help prevent or reduce the chance of infection. A few techniques that the authors utilize to minimize infection risk include the placement of Xeroform or cotton ear plugs soaked in betadine in the external auditory canal to isolate contents in the ear from the surgical site, use of antibiotic in the irrigation, and resection of bilateral TMJs first followed by implantation and immediate closure to minimize the exposure time of the prosthesis. Appropriate IV antibiotics are used while in the hospital and then PO antibiotics for an additional 7–10 days after hospital discharge. This patient management scheme should minimize the risk of infection.
Postsurgically, light force vertical elastics are necessary to support the mandible since the muscles of mastication are detached during surgery and may take a few weeks to reattach and provide adequate support to the mandible. Otherwise, postsurgical patient management is the same as routine double-jaw orthognathic surgery [55, 57].
22 Utilization of Fat Grafts
Early on in the use of total joint prostheses, a common problem encountered in approximately 35% of the patients was postsurgical fibrosis and heterotopic bone formation around the prostheses causing jaw dysfunction, decreased incisal opening, and pain [58]. In 1992, Wolford developed a technique to place fat grafts (harvested from the abdomen or buttock) around the articulating area of the total joint prosthesis to eliminate the dead space. This prevents blood clot formation in the space around the prosthesis that could provide a matrix for fibrous ingrowth and pluripotent cells migration resulting in the development of heterotopic bone and dense fibrotic tissues. Also, in patients with previous failed alloplastic implants, the fat graft occupies areas around the implant preventing foreign-body giant-cell reaction (FBGCR) and formation of reactive bone. Wolford et al. [58,59,60] have demonstrated the improved outcomes for patients using fat grafts packed around the prostheses compared to patients that did not receive the fat grafts when evaluating function, pain, and elimination of additional surgical procedures such as joint debridement. Mercuri et al. [61] reported the efficacy of the fat grafts packed around the prostheses in TMJ ankylosis cases.
23 Case Examples Utilizing C-TJR-OS
Case 1: (Figs. 10.25, 10.26, 10.27, and 10.28)
This 48-year-old female sustained trauma to the TMJs at age 28 with subsequent development of bilateral TMJ reactive arthritis with resultant condylar resorption and development of an anterior open bite (Figs. 10.25a–c, 10.26a–c, 10.27a–d and 10.28a). She was in splint therapy for 16 years and underwent most of the nonsurgical management imaginable. She suffered daily headaches at a level of 8 (0 = no pain, 10 = worse pain imaginable), TMJ pain at 5, myofascial pain at 8, jaw function at 8 (0 = normal function, 10 = no jaw movement), diet at 8 (0 = normal diet, 10 = liquids only), and disability at 8 (0 = no disability, 10 = totally disabled). MRI showed severe TMJ arthritis, condylar resorption, and displaced non-salvageable discs (Fig. 10.27a–d). She was diagnosed with the following: (1) bilateral TMJ reactive arthritis with condylar resorption, (2) maxillary hypoplasia, (3) mandibular hypoplasia, (4) anterior open bite occluding only on the left posterior teeth, (5) sleep apnea related to decreased oropharyngeal airway, (6) bilateral turbinate hyperplasia causing nasal airway obstruction, and (7) TMJ pain, myofascial pain, and headaches requiring years of narcotic use. The maximal incisal opening with severe pain was 40 mm and without pain was 14 mm.


Case 1: (a–c) presurgery clinical pictures of 48-year-old female with reactive arthritis, maxillary and mandibular hypoplasia, anterior open bite, sleep apnea, and pain. (d–f) Clinical images at 2 years postsurgery with improved function and facial balance, resolution of sleep apnea, and elimination of pain


Case 1: (a–c) presurgery occlusion with a Class II open bite and occlusal contact only on the posterior teeth on the left side. (d–f) At 2 years postsurgery, the occlusion is stable with a Class I cuspid-molar relationship


Case 1: presurgery TMJ MRI sagittal images. (a) Right TMJ closed and (b) open views show severe arthritis of condyle (yellow arrow) and anteriorly displaced disc (white arrow) severely degenerated, nonreducing, and non-salvageable. (c) Left TMJ closed and (d) open views show severe destruction of the condyle (yellow arrow) with the articular disc (white arrow) severely degenerated, nonreducing, and non-salvageable


Case 1: (a) presurgical cephalometric tracing shows the retruded maxilla and mandible as well as the high occlusal plane angle (21°) and decreased oropharyngeal airway (3 mm). (b) The surgical treatment objective demonstrated the planned surgical changes with counterclockwise rotation advancement with the maxillary incisal edges advanced 8 mm, pogonion advanced 18 mm, and the occlusal plane angle decreased 13°
Her surgery was planned for C-TJR-OS using CASS technology and included the following (Fig. 10.28b): (1) bilateral TMJ reconstruction and counterclockwise rotation of the mandible with TMJ Concepts patient-fitted total joint prostheses; (2) bilateral coronoidectomies; (3) bilateral TMJ fat grafts packed around the articulating area of the prostheses, harvested from the abdomen; (4) multiple maxillary osteotomies for counterclockwise rotation and advancement; and (5) bilateral partial inferior turbinectomies.
At 2 years postsurgery, she reported no myofascial pain, TMJ pain, or headaches with elimination of pain medications. Her incisal opening improved to 46 mm pain-free. She rated her jaw function at 2, diet at 2, and disability at 2. A class I occlusion was obtained, improved facial balance was achieved, and sleep apnea was eliminated (Figs. 10.25d–f and 10.26d–f).
Case 2: (Figs. 10.29 and 10.30)
This 14-year-old female presented with juvenile idiopathic arthritis (JIA) of the TMJs with the onset at approximately 9 years old but first noted clinically at age 11, with progressively worsening facial deformity related to condylar resorption and difficulty breathing (Figs. 10.29a–c, 10.30a–c, 10.31a–d and 10.32a). She had no pain issues, and only other joints affected were the ankles. Her incisal opening was 47 mm and excursions 7 mm to the right and 8 mm to the left. Her diagnosis included the following: (1) bilateral TMJ JIA, (2) maxillary A-P and posterior vertical hypoplasia, (3) mandibular A-P and posterior vertical hypoplasia, (4) Class II occlusion, (5) microgenia, (6) decreased oropharyngeal airway with sleep apnea symptoms, and (7) hypertrophied turbinates creating nasal airway obstruction. The MRI scans (Fig. 10.31a–d) demonstrate the severe destruction of the condyles and resorption of the articular eminences.


Case 2: (a–c) a 14-year-old female with JIA and grossly resorbed mandibular condyles, retruded mandible and maxilla, posterior maxillary vertical hypoplasia, high occlusal plane angle facial morphology, decreased oropharyngeal dimension and sleep apnea symptoms, as well as hypertrophied turbinates and difficulty breathing through the nose. (d–f) The patient is seen at 2 years postsurgery demonstrating significantly improved facial balance and function with a stable occlusion


Case 2: (a–c) the patient has a Class II occlusion presurgery. (d–f) At 2 years postsurgery, she demonstrates a stable Class I occlusion


Case 2: MRI scans of the TMJs. (a) Left TMJ sagittal view. (b) Right TMJ sagittal view showing the destruction of the condyle and articular eminence, common in JIA cases. Notice the “mushrooming” of the remainder of the condylar neck process. (c) Left TMJ coronal view. (d) Right TMJ coronal view demonstrating the severe narrowing of the condylar neck stump


Case 2: (a) the cephalometric analysis shows the severe jaw deformity with retruded maxilla-mandible, high occlusal plane angulation, and decreased oropharyngeal airway. (b) The prediction tracing demonstrates the counterclockwise rotation of the maxillomandibular complex. The chin is augmented with a bony genioplasty. Maxillary incisors advanced 4 mm, pogonion advanced 28 mm, and the occlusal plane decreased 16°, creating improved function and facial balance
Her surgery was planned for C-TJR-OS using CASS technology. Figure 10.11 is a similar CASS workup. Surgery included the following (Fig. 10.32b, the prediction tracing): (1) bilateral TMJ reconstruction and counterclockwise rotation of the mandible with TMJ Concepts patient-fitted total joint prostheses; (2) bilateral coronoidectomies; (3) bilateral TMJ fat grafts packed around the articulating area of the prostheses, harvested from the abdomen; (4) multiple maxillary osteotomies for counterclockwise rotation and advancement; (5) anterior mandibular horizontal osteotomy to augment the chin; and (6) bilateral partial inferior turbinectomies.
At 2 years postsurgery, she remained pain-free, incisal opening at 40 mm but continuing to improve, excursive movements 3 mm to the right and 4 mm to the left, stable Class I occlusion, improved facial balance, good nasal airway, and elimination of sleep apnea symptoms (Figs. 10.29d–f and 10.30d–f).
Case 3: (Figs. 10.33, 10.34, and 10.35)
This 18-year-old male presented with unilateral right TMJ ankylosis and retruded, asymmetric maxilla and mandible (Figs. 10.33a–c, 10.34a–c and 10.35a). Pt reported a traumatic injury to the jaw a few years earlier resulting in a significantly limited incisal opening as well as the jaw deformity. The resultant right TMJ ankylosis stunted the mandibular growth on the right creating the significant facial asymmetry. He had moderate pain and headaches. CT scan and MRI showed right TMJ bony ankylosis but the left side TMJ anatomy was normal.


Case 3: (a–c) an 18-year-old male with unilateral right bony ankylosis. Maxilla and mandible are retruded and asymmetric. (d–f) The patient had the following procedures: (1) right TMJ reconstruction and mandibular advancement with TMJ Concepts total joint prosthesis, (2) right TMJ fat graft, (3) right coronoidectomy, (4) left mandibular ramus sagittal split osteotomy, (5) segmental maxillary osteotomies, and (6) bilateral partial turbinectomies. The patient is seen 1 year postsurgery pain-free, with incisal opening 48 mm, left excursion 3 mm and right excursion 5 mm, and improved facial balance


Case 3: (a–c) presurgery occlusion with a Class I occlusion but left side posterior open bite. (d–f) Postsurgery occlusion shows a nicely integrated bite relationship


Case 3: (a) presurgery lateral cephalogram shows the vertical asymmetry and retruded maxilla and mandible. (b) The surgical treatment plan included (1) right TMJ reconstruction and mandibular advancement with TMJ Concepts total joint prosthesis, (2) right TMJ fat graft, (3) right coronoidectomy, (4) left mandibular ramus sagittal split osteotomy, (5) segmental maxillary osteotomies, and (6) Bilateral partial turbinectomies
The patient was planned for C-TJR-OS using CASS technology. Surgery included the following steps with mandible-first approach (Fig. 10.35b): (1) unilateral right TMJ reconstruction and counterclockwise rotation advancement of the mandible with TMJ Concepts patient-fitted total joint prosthesis; (2) right TMJ fat grafts packed around the articulating area of the prosthesis, harvested from the abdomen; (3) right coronoidectomy; (4) left mandibular ramus sagittal split osteotomy for advancement; (5) maxillary osteotomies for counterclockwise rotation and advancement; and (6) bilateral partial nasal inferior turbinectomies.
At 1 year postsurgery, the patient was pain-free, with incisal opening at 45 mm, excursive movements 5 mm to the right and 3 mm to the left, and a stable Class I occlusion (Figs. 10.33d–f and 10.34d–f).
Case 4: (Figs. 10.36, 10.37, 10.38, 10.39, 10.40, and 10.41)
This 68-year-old male presented with bilateral degenerative joint disease and anterior disc displacement of the TMJs and moderate obstructive sleep apnea (Fig. 10.36a, b). Pt reported a 7-year history of severe pain, clicking, and popping in bilateral TMJs, worsened with PAP therapy. As a result, pt. had not been compliant with PAP therpay. Pt also stated significant daytime somnolence, fatigue, and restless sleep. Polysomnography showed a respiratory disturbance index (RDI) of 15.7 and lowest O2 of 89%. Drug-induced sleep endoscopy revealed retropalatal and retroglossal airway collapse. CT scan showed bilateral degenerative joint disease, and MRI demonstrated bilateral anterior disc displacement and degenerative changes of the condyle (Fig. 10.37).


Case 4: (a, b) a 68-year-old male with bilateral degenerative joint disease and anterior disc displacement of the TMJs and moderate obstructive sleep apnea. Mandible appears retrognathic


Case 4: MRI of the right TMJ shows anterior disc displacement and condylar remodeling


Case 4: (a) final positioning of the maxilla and mandible. (b) Fabrication of the right TMJ prosthesis in the final position. (c) Fabrication of the left TMJ prosthesis in the final position


Case 4: (a) preauricular approach showing exposure of the right condyle and fossa. (b) Image shows the right condyle, coronoid, and disc resected. Condyle and coronoid resected. (c) The right condylar and fossa components have been fixated to the ramus and zygomatic arch. (d) The maxilla is then advanced and rotated counterclockwise in the final position


Case 4: (a, b) pre- and postoperative lateral cephalometric image depicted the planned movements including counterclockwise rotation of the maxillomandibular complex, TMJ reconstruction, decrease in occlusal plane, and increase in airway space


Case 4: (a, b) pre- and postoperative profile views show significant advancement of the maxillomandibular structures
Given patient’s history of TMJ pathology and moderate OSA with significant pain and sleep apnea symptoms, he was planned for C-TJR-OS using CASS technology. Figure 10.38a–c depicts the CASS workup with final positioning of the maxilla and mandible and final positioning of the bilateral TMJs with TMC Concepts. Surgery included the following steps with mandible-first approach (Fig. 10.39a–d): (1) bilateral TMJ reconstruction including coronoidectomies and counterclockwise rotation of the mandible with TMJ Concepts patient-fitted total joint prostheses; (2) bilateral TMJ fat grafts packed around the articulating area of the prostheses, harvested from the abdomen; and (3) multiple maxillary osteotomies for counterclockwise rotation and advancement. Pre- and postoperative lateral cephalometric image depicted the planned movements including counterclockwise rotation of the maxillomandibular complex, TMJ reconstruction, and increase in airway space (Fig. 10.40a, b).
At 1 year postsurgery, he remained pain-free, with incisal opening at 45 mm, excursive movements 3 mm to the right and 3 mm to the left, stable Class I occlusion, and RDI less than five with elimination of sleep apnea symptoms (Fig. 10.41a, b).
24 Treatment Outcomes Utilizing These Treatment Protocols
Various publications over the years have demonstrated good stability and treatment outcomes utilizing the C-TJR-OS protocols. Various modifications to the TJR steps such as minimization of prosthesis exposure, fat graft placement, and use of ultrasonic BoneScalpel handpiece (Fig. 10.42) have reduced infection rates, fibrotic and heterotopic bone formation, and bleeding leading to improved outcomes. These modifications have been applied in the C-TJR-OS protocol leading to less complications and improved results in an already complex surgical procedure.


Case 4: a side-by-side comparison of the BoneScalpel to a conventional reciprocating saw. Note the comparable dimensions of the handpiece and cutting surfaces
Dela Coleta et al. [62] evaluated 47 female patients for surgical stability following bilateral TMJ reconstruction using TMJ Concepts patient-fitted TMJ total joint prostheses, TMJ fat grafts, and counterclockwise rotation of the maxillomandibular complex with menton advancing an average of 18.4 mm and the occlusal plane decreasing an average of 14.9°. Average follow-up was 40.6 months. Results demonstrated minor maxillary horizontal changes, while the mandibular measurements remained very stable. Pinto et al. [63] evaluated the same 47 female patients relative to pain and dysfunctional outcomes. Patients were divided into two groups based on the number of previous surgeries: Group 1 had zero to one previous surgeries, while Group 2 had two or more previous surgeries. Significant improvements (37–52%) were observed for TMJ pain, headaches, jaw function, diet, and disability. MIO increased 14%. Group 1 patients had better pain and jaw function results than Group 2 patients. For patients who did not receive fat grafts around the prostheses and had previous failure of alloplastic TMJ implants including Proplast-Teflon (PT) and silicone elastomers, more than half required secondary surgery including TMJ debridement for removal of FBGCR, fibrosis, and/or heterotopic bone formation. These two studies demonstrated that end-stage TMJ patients could be treated in one operation with TMJ Concepts patient-fitted TMJ total joint prostheses, fat grafts, and maxillomandibular counterclockwise rotation for correction of an associated dentofacial deformity with good stability and improvement in pain and TMJ function.
Although the life expectancy of this device is unknown, Wolford, Mercuri, et al. [64] recently published a 20-year follow-up study of 56 patients who had received the Techmedica total joint prostheses between 1989 and 1993. There were statistically significant improvements in all parameters including incisal opening, jaw function, TMJ pain and diet, and 85.7% of the patients reporting significant improvement in their quality of life. Furthermore, patients who underwent a greater number of previous TMJ surgeries reported a lower degree of subjective improvement but increased objective findings in regard to mandibular function and improved quality of life. There were no reports of device removal due to material wear or failure.
Wolford et al. [13,14,15,16,17, 62,63,64,65,66,67,68,69], Mercuri et al. [15,16,17, 70,71,72,73,74,75,76,77], and others [78,79,80,81] have published numerous studies in reference to outcome data using TMJ total joint prostheses. A summary of these publications have produced the following facts in reference to the TMJ Concepts total joint prostheses:
-
1.
TMJ Concepts prostheses are superior to autogenous tissues for end-stage TMJ reconstruction relative to subjective and objective outcomes [16, 65, 74, 75, 77].
-
2.
After two previous TMJ surgeries, autogenous tissues have a very high failure rate, whereas patient-fitted total joint prostheses have a high success rate [16, 64, 76, 77].
-
3.
No donor site morbidity.
-
4.
The increased number of previous TMJ surgeries produces a lower level of improvement related to pain and function outcomes compared to patients with zero to one previous TMJ surgery [14,15,16,17, 63, 64, 68,69,70,71,72,73,74,75,76,77].
-
5.
Failed TMJ alloplastic reconstruction (i.e., PT, Silastic, metal-on-metal articulation, etc.) can create a foreign-body giant-cell reaction and/or metallosis, best treated by joint debridement and reconstruction with patient-fitted total joint prostheses [14,15,16,17, 63,64,65,66, 69, 73].
-
6.
Fat grafts packed around the articulating area of the prostheses improves outcomes relative to decreased pain, improved jaw function, and decreased requirement for repeat surgery [58,59,60,61].
-
7.
Using Piezo technology such as ultrasonic BoneScalpel in TMJ reconstruction results in less blood loss when compared to surgeries employing the use of the conventional reciprocating saw [58].
-
8.
Osseointegration of the TMJ Concepts fossa and mandibular components occurs and is important for long-term stability [13,14,15,16,17, 49, 62,63,64,65, 67,68,69,70,71,72].
-
9.
Posterior stop on the fossa component is important to stabilize the joint, jaw position, and occlusion [13, 14, 16, 62, 63, 67, 68].
-
10.
Concomitant orthognathic surgery can be performed at the same time as the TMJs are reconstructed [13, 16, 49, 62, 63, 67, 68].
-
11.
Twenty-year follow-up study demonstrated improvements in pain, jaw function, diet, incisal opening, and quality of life [64].
25 Summary
Healthy and stable TMJs are necessary for quality treatment outcomes in orthognathic surgery. If the TMJs are found to have pathological changes, orthognathic surgery results may be unsatisfactory relative to function, esthetics, skeletal and occlusal stability, and pain. The oral and maxillofacial surgeon should be suspicious of possible TMJ problems in the following types of patients: (1) high occlusal plane angle facial morphologies with retruded maxilla and mandible; (2) developing anterior or lateral open bites; (3) progressively worsening occlusal and jaw relationship; (4) facial asymmetry, particularly with progressive worsening; and (5) patients reporting headaches, TMJ pain, myofascial pain, history of clicking and popping of the TMJs, and/or ear symptoms. The surgeon should not ignore these symptoms, and patients presenting with one or more of these symptoms should be evaluated for possible TMJ pathology. An MRI of the TMJs can aide in identification of the specific TMJ pathology. Failure to recognize and treat these conditions can result in significant relapse, increased pain, and a greater complexity of subsequent treatment.
During the past 30 years, major advancements have been made in TMJ diagnostics and the development of surgical procedures to treat and rehabilitate the pathological, dysfunctional, and painful TMJ. Research has clearly demonstrated that TMJ and orthognathic surgery can be safely and predictably performed at the same operation, but it does necessitate the correct diagnosis, formulation of a comprehensive treatment plan, and requirement of the surgeon to have expertise in both TMJ and orthognathic surgery. The surgical procedures can be separated into two or more surgical stages, but the TMJ surgery should be done first. Combined TMJ and orthognathic surgery requires a thorough analysis of facial soft tissue features, hard tissue shape and relative relationships, and TMJ pathological condition with physical examination and radiographic studies. Adherence to the general surgical principles as outlined above will maximize restoration of harmony among the osseous, dental, muscular, and cutaneous elements of the face and TMJ. As a result, coexisting TMJ pathology and dentofacial deformities treated concomitantly will provide patients with a youthful appearance, functional improvements, and overall satisfaction.
References
Wolford LM, Cassano DS, Goncalves JR. Common TMJ disorders: orthodontic and surgical management. In: JA MN, Kapila SD, editors. Temporomandibular disorders and orofacial pain: separating controversy from consensus. Craniofacial growth series, vol. 46. Ann Arbor: The University of Michigan; 2009. p. 159–98.
Wolford LM, Movahed R. Concomitant TMJ and orthognathic surgery: diagnosis and treatment planning. Oral Maxillofac Surg Knowledge Update. AAOMS online; 2014.
Wolford LM, Dhameja A. Planning for combined TMJ arthroplasty and orthognathic surgery. Atlas Oral Maxillofac Surg Clin North Am. 2011;19(2):243–70.
LM W. Mandibular asymmetry: temporomandibular joint degeneration. In: Bagheri SC, Bell RB, Khan HA, editors. Current therapy in oral and maxillofacial surgery. St. Louis: Elsevier; 2012.
Wolford LM, Reiche-Fischel O, Mehra P. Changes in temporomandibular joint dysfunction after orthognathic surgery. J Oral Maxillofac Surg. 2003;61(6):655–60; discussion 661.
Wolford LM. Idiopathic condylar resorption of the temporomandibular joint in teenage girls (cheerleaders syndrome). Proc (Bayl Univ Med Cent). 2001;14(3):246–52.
Granquist EJ. Treatment of the temporomandibular joint in a child with juvenile idiopathic arthritis. Oral Maxillofac Surg Clin North Am. 2018;30(1):97–107.
Henry CH, et al. Reactive arthritis and internal derangement of the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(1):e22–6.
Henry CH, Pitta MC, Wolford LM. Frequency of chlamydial antibodies in patients with internal derangement of the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91(3):287–92.
Henry CH, et al. Reactive arthritis: preliminary microbiologic analysis of the human temporomandibular joint. J Oral Maxillofac Surg. 2000;58(10):1137–42; discussion 1143–4.
Henry CH, et al. Identification of chlamydia trachomatis in the human temporomandibular joint. J Oral Maxillofac Surg. 1999;57(6):683–8; discussion 689.
Zeidler H, Hudson AP. New insights into chlamydia and arthritis. Promise of a cure? Ann Rheum Dis. 2014;73(4):637–44.
Mehra P, et al. Single-stage comprehensive surgical treatment of the rheumatoid arthritis temporomandibular joint patient. J Oral Maxillofac Surg. 2009;67(9):1859–72.
Wolford LM, et al. TMJ concepts/techmedica custom-made TMJ total joint prosthesis: 5-year follow-up study. Int J Oral Maxillofac Surg. 2003;32(3):268–74.
Mercuri LG, et al. Custom CAD/CAM total temporomandibular joint reconstruction system: preliminary multicenter report. J Oral Maxillofac Surg. 1995;53(2):106–15; discussion 115–6.
Wolford LM, Cottrell DA, Henry CH. Temporomandibular joint reconstruction of the complex patient with the techmedica custom-made total joint prosthesis. J Oral Maxillofac Surg. 1994;52(1):2–10; discussion 11.
Mercuri LG, et al. Long-term follow-up of the CAD/CAM patient fitted total temporomandibular joint reconstruction system. J Oral Maxillofac Surg. 2002;60(12):1440–8.
Wolford L, et al. Temporomandibular joint ankylosis can be successfully treated with TMJ concepts patient-fitted total joint prosthesis and autogenous fat grafts. J Oral Maxillofac Surg. 2016;74(6):1215–27.
Wolford LM. Chapter 9; Diagnosis and management of TMJ heterotopic bone and ankylosis. In: Bouloux G, editor. Complications of temporomandibular joint surgery. Cham: Springer; 2017.
Wolford LM, Rodrigues DB. Temporomandibular joint (TMJ) pathologies in growing patients: effects on facial growth and development. In: Preedy VR, editor. Handbook of growth and growth monitoring in health and disease. New York: Springer; 2012.
Schendel SA, Powell NB. Surgical orthognathic management of sleep apnea. J Craniofac Surg. 2007;18(4):902–11.
Jacobson RL, Schendel SA. Treating obstructive sleep apnea: the case for surgery; point/counterpoint. Am J Orthod Dentofacial Orthop. 2012;142:434–42.
Schendel S, Powell N, Jacobson R. Maxillary, mandibular, and chin advancement: treatment planning based on airway anatomy in obstructive sleep apnea. J Oral Maxillofac Surg. 2011;69(3):663–76.
Schendel SA, Broujerdi JA, Jacobson RL. Three-dimensional upper-airway changes with maxillomandibular advancement for obstructive sleep apnea treatment. Am J Orthod Dentofac Orthop. 2014;146(3):385–93.
Li KK, et al. Long-term results of maxillomandibular advancement aurgery. Sleep Breath. 2000;4(3):137–40.
Camacho M, et al. Large maxillomandibular advancements for obstructive sleep apnea: an operative technique evolved over 30 years. J Craniomaxillofac Surg. 2015;43(7):1113–8.
Gonçalves JR, et al. Airway space changes after maxillomandibular counterclockwise rotation and mandibular advancement with TMJ Concepts® total joint prostheses: three-dimensional assessment. Int J Oral Maxillofac Surg. 2013;42(8):1014–22.
Wolford LM, et al. Airway space changes after nasopharyngeal adenoidectomy in conjunction with Le Fort I osteotomy. J Oral Maxillofac Surg. 2012;70(3):665–71.
Coleta KE, et al. Maxillo-mandibular counter-clockwise rotation and mandibular advancement with TMJ Concepts total joint prostheses: part II–airway changes and stability. Int J Oral Maxillofac Surg. 2009;38(3):228–35.
Goncalves JR, et al. Postsurgical stability of oropharyngeal airway changes following counter-clockwise maxillo-mandibular advancement surgery. J Oral Maxillofac Surg. 2006;64(5):755–62.
Mehra P, et al. Pharyngeal airway space changes after counterclockwise rotation of the maxillomandibular complex. Am J Orthod Dentofac Orthop. 2001;120(2):154–9.
LM W. Chapter 74; Surgical planning in orthognathic surgery and outcome stability. In: Brennan S, Ghali C, editors. Maxillofacial surgery, vol. 2. St Louis: Churchill Livingstone; 2017.
Wolford LM. Overbite and vertical facial dimensions in terms of muscle balance. Angle Orthod. 1944;14(1):13–7.
Delaire J. L’Analyse architectural et structural craniofaciale (de profil): principles theoriques quelques examples d’emploi en chirurgie maxillofaciale. Rev Stomatol. 1978;79:1.
Delaire J, Schendel SA, Tulasne JF. An architectural and structural craniofacial analysis: a new lateral cephalometric analysis. Oral Surg Oral Med Oral Pathol. 1981;52(3):226–38.
Schendel SA, Carlotti AE. Variations of total vertical maxillary excess. J Oral Maxillofac Surg. 1985;43(8):590–6.
Schendel SA, Jacobson R, Khalessi S. Airway growth and development: a computerized 3-dimensional analysis. J Oral Maxillofac Surg. 2012;70(9):2174–83.
Movahed R, et al. Outcome assessment of 603 cases of concomitant inferior turbinectomy and Le Fort I osteotomy. Proc (Bayl Univ Med Cent). 2013;26(4):376–81.
Linder-Aronson S. Adenoids. Their effect on mode of breathing and nasal airflow and their relationship to characteristics of the facial skeleton and the denition. A biometric, rhino-manometric and cephalometro-radiographic study on children with and without adenoids. Acta Otolaryngol Suppl. 1970;265:1–132.
Harari D, et al. The effect of mouth breathing versus nasal breathing on dentofacial and craniofacial development in orthodontic patients. Laryngoscope. 2010;120(10):2089–93.
Hultcrantz E, et al. The influence of tonsillar obstruction and tonsillectomy on facial growth and dental arch morphology. Int J Pediatr Otorhinolaryngol. 1991;22(2):125–34.
Schendel SA, et al. The long face syndrome: vertical maxillary excess. Am J Orthod. 1976;70(4):398–408.
Riolo, et al. An atlas of craniofacial growth: cephalometric standards from the University School Growth Study, the University of Michigan. Ann Arbor: University of Michigan; 1974. p. 105–6.
Wolford LM, Karras SC, Mehra P. Considerations for orthognathic surgery during growth, part 1: mandibular deformities. Am J Orthod Dentofac Orthop. 2001;119(2):95–101.
Wolford LM, Rodrigues DB. Orthognathic considerations in the young patient and effects on facial growth. In: Preedy VR, editor. Handbook of growth and growth monitoring in health and disease. New York: Springer; 2012.
Wolford LM, Karras SC, Mehra P. Considerations for orthognathic surgery during growth, part 2: maxillary deformities. Am J Orthod Dentofac Orthop. 2001;119(2):102–5.
Chemello PD, Wolford LM, Buschang PH. Occlusal plane alteration in orthognathic surgery-part II: long-term stability of results. Am J Orthod Dentofac Orthop. 1994;106(4):434–40.
Wolford LM, Chemello PD, Hilliard F. Occlusal plane alteration in orthognathic surgery-part I: effects on function and esthetics. Am J Orthod Dentofac Orthop. 1994;106(3):304–16.
Wolford LM, Chemello PD, Hilliard FW. Occlusal plane alteration in orthognathic surgery. J Oral Maxillofac Surg. 1993;51(7):730–40; discussion 740–1.
Movahed R, Teschke M, Wolford LM. Protocol for concomitant temporomandibular joint custom-fitted total joint reconstruction and orthognathic surgery utilizing computer-assisted surgical simulation. J Oral Maxillofac Surg. 2013;71(12):2123–9.
Movahed R, Wolford LM. Protocol for concomitant temporomandibular joint custom-fitted total joint reconstruction and orthognathic surgery using computer-assisted surgical simulation. Oral Maxillofac Surg Clin North Am. 2015;27(1):37–45.
Xia J, et al. Computer-assisted three-dimensional surgical planning and simulation: 3D virtual osteotomy. Int J Oral Maxillofac Surg. 2000;29(1):11–7.
Gateno J, et al. Clinical feasibility of computer-aided surgical simulation (CASS) in the treatment of complex cranio-maxillofacial deformities. J Oral Maxillofac Surg. 2007;65(4):728–34.
Rotaru H, et al. Cranioplasty with custom-made implants: analyzing the cases of 10 patients. J Oral Maxillofac Surg. 2012;70(2):e169–76.
Wolford LM. Chapter 19; Postsurgical patient management. In: Fonseca, Marciani, Turvey, editors. Oral and maxillofacial surgery, vol. III. 2nd ed. St. Louis: Elsevier; 2008.
Silva R, et al. Benefits of using the ultrasonic BoneScalpel™ in temporomandibular joint reconstruction. J Craniomaxillofac Surg. 2017;45(3):401–7.
Wolford LM, Rodrigues DB, Limoeiro E. Orthognathic and TMJ surgery: postsurgical patient management. J Oral Maxillofac Surg. 2011;69(11):2893–903.
Wolford LM, Karras SC. Autologous fat transplantation around temporomandibular joint total joint prostheses: preliminary treatment outcomes. J Oral Maxillofac Surg. 1997;55(3):245–51; discussion 251–2.
Wolford LM, et al. Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formation. Proc (Bayl Univ Med Cent). 2008;21(3):248–54.
Wolford LM, Cassano DS. Autologous fat grafts around temporomandibular joint (TMJ) total joint prostheses to prevent heterotopic bone. In: Shiffman MA, editor. Autologous fat transfer. Berlin: Springer; 2010.
Mercuri LG, Ali FA, Woolson R. Outcomes of total alloplastic replacement with periarticular autogenous fat grafting for management of reankylosis of the temporomandibular joint. J Oral Maxillofac Surg. 2008;66(9):1794–803.
Dela Coleta KE, et al. Maxillo-mandibular counter-clockwise rotation and mandibular advancement with TMJ Concepts total joint prostheses: part I—skeletal and dental stability. Int J Oral Maxillofac Surg. 2009;38(2):126–38.
Pinto LP, et al. Maxillo-mandibular counter-clockwise rotation and mandibular advancement with TMJ Concepts total joint prostheses: part III—pain and dysfunction outcomes. Int J Oral Maxillofac Surg. 2009;38(4):326–31.
Wolford LM, et al. Twenty-year follow-up study on a patient-fitted temporomandibular joint prosthesis: the techmedica/TMJ concepts device. J Oral Maxillofac Surg. 2015;73(5):952–60.
Henry CH, Wolford LM. Treatment outcomes for temporomandibular joint reconstruction after proplast-teflon implant failure. J Oral Maxillofac Surg. 1993;51(4):352–8; discussion 359–60.
Franco PF, et al. Unilateral TMJ total joint reconstruction and the effects on the contralateral joint. AAOMS 79th Annual Meeting and Scientific Sessions. J Oral Maxillofac Surg. 55:113, 1997.
Wolford LM, et al. Successful reconstruction of nongrowing hemifacial microsomia patients with unilateral temporomandibular joint total joint prosthesis and orthognathic surgery. J Oral Maxillofac Surg. 2012;70(12):2835–53.
Wolford LM, et al. Outcomes of treatment with custom-made temporomandibular joint total joint prostheses and maxillomandibular counter-clockwise rotation. Proc (Bayl Univ Med Cent). 2008;21(1):18–24.
Wolford LM, et al. Comparison of 2 temporomandibular joint total joint prosthesis systems. J Oral Maxillofac Surg. 2003;61(6):685–90; discussion 690.
Mercuri LG, Edibam NR, Giobbie-Hurder A. Fourteen-year follow-up of a patient-fitted total temporomandibular joint reconstruction system. J Oral Maxillofac Surg. 2007;65(6):1140–8.
Wolford LM, Cardenas L. Idiopathic condylar resorption: diagnosis, treatment protocol, and outcomes. Am J Orthod Dentofac Orthop. 1999;116(6):667–77.
Mercuri LG, Giobbie-Hurder A. Long-term outcomes after total alloplastic temporomandibular joint reconstruction following exposure to failed materials. J Oral Maxillofac Surg. 2004;62(9):1088–96.
Mercuri LG. Subjective and objective outcomes in patients reconstructed with a custom-fitted alloplastic temporomandibular joint prosthesis. J Oral Maxillofac Surg. 1999;57(12):1427–30.
Mercuri LG. The TMJ concepts patient fitted total temporomandibular joint reconstruction prosthesis. Oral Maxillofac Surg Clin North Am. 2000;12(1):73–91.
Mercuri LG. The use of alloplastic prostheses for temporomandibular joint reconstruction. J Oral Maxillofac Surg. 2000;58(1):70–5.
Mercuri LG. Temporomandibular joint reconstruction. In: Fonseca R, editor. Oral and maxillofacial surgery. Philadelphia: Elsevier; 2008.
Mercuri LG. End-stage TMD and TMJ reconstruction. In: Miloro M, Ghali G, Larsen P, Waite P, editors. Peterson’s principles of oral & maxillofacial surgery. 3rd ed. Raleigh: PMPH, USA Ltd; 2012.
Giannakopoulos HE, Sinn DP, Quinn PD. Biomet microfixation temporomandibular joint replacement system: a 3-year follow-up study of patients treated during 1995 to 2005. J Oral Maxillofac Surg. 2012;70(4):787–94; discussion 795–6.
Machon V, et al. Total alloplastic temporomandibular joint replacement: the Czech-Slovak initial experience. Int J Oral Maxillofac Surg. 2012;41(4):514–7.
Sidebottom AJ, Gruber E. One-year prospective outcome analysis and complications following total replacement of the temporomandibular joint with the TMJ Concepts system. Br J Oral Maxillofac Surg. 2013;51(7):620–4.
Murdoch B, Buchanan J, Cliff J. Temporomandibular joint replacement: a New Zealand perspective. Int J Oral Maxillofac Surg. 2014;43(5):595–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter
Cite this chapter
Gupta, R.J., Schendel, S.A., Wolford, L. (2019). Concomitant Custom-Fitted Temporomandibular Joint Reconstruction and Orthognathic Surgery. In: Connelly, S.T., Tartaglia, G.M., Silva, R.G. (eds) Contemporary Management of Temporomandibular Disorders. Springer, Cham. https://doi.org/10.1007/978-3-319-99909-8_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-99909-8_10
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-99908-1
Online ISBN: 978-3-319-99909-8
eBook Packages: MedicineMedicine (R0)