
Abstract
Expert surgical performance is characterized by high-level motor performance, the ability to concentrate for long periods of time, discriminating awareness of clinical situations, and several cognitive factors (e.g., mental preparedness, self-confidence, etc.). These abilities, developed through extensive experience, deliberate practice, and study, enable expert surgeons to manage challenging clinical situations effectively.
In addition to the well-researched benefit to technical skills proficiency, surgical simulation training may offer inexperienced surgeons, who are susceptible to experience performance degradations during difficult clinical situations, an opportunity to develop cognitive (e.g., mental imagery, relaxation strategies, attention management, etc.) and team-based skills (e.g., effective communication, leadership, etc.). These skills are often overlooked in traditional surgical training but are critical elements of expert surgical performance. Thus, simulation training may be an effective method to help trainees and non-expert surgeons reduce the learning curve to attain these trainable elements of surgical expertise and optimize their surgical performance.
The research on cognitive and team-based skills training in high-pressure domains like the military, aviation, and elite athletics indicates that this training can effectively enhance learners’ performance. While the research on nontechnical skills training in surgical education is still burgeoning, the results provide support that this type of training can enhance trainees’ and practicing surgeons’ performance. Accordingly, implementing cognitive and team-based skills during trainees’ simulation training should be a priority in the future of surgical education.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
High-level surgical performance is characterized by a mastery of extensive and ever-evolving knowledge, skills, and abilities to accurately diagnose illness and disorders in the body and offer direct treatment interventions [1]. Inherent components of successful surgical performance include executing intricate technical details flawlessly, maintaining concentration on relevant information amidst environmental distractions, communicating effectively with the surgical team, balancing attention, and sustaining sound clinical judgment. Surgeons must execute exceedingly difficult surgical procedures safely under challenging clinical situations that can impair cognitive and physical function in less proficient performers [2,3,4]. Thus, it is apparent that there can be significant differences in individual and intraprofessional surgical performance dependent upon proficiency at executing the aforementioned factors, experience, and management of the psychophysiological demands of surgery. In an effort to reduce the variability in surgeons’ performance, we will provide an operational definition of performance optimization, briefly discuss the process of skill mastery, outline programs designed to optimize performance in other high-stakes domains, identify how cognitive performance-enhancing strategies have been implemented in surgery, and consider the future of performance optimization in surgical education.
Performance Optimization
Individual Performance
Our definition of performance optimization is having the clarity and knowledge of what comprises expert performance and skill mastery in a specific domain and utilizing techniques and competencies to work toward consistently executing performance at that standard. Expert performance in any domain is context-specific, but it can generally be considered as consistently exceptional or extremely good performance that is in the uppermost range of a normalized performance distribution (see Fig. 1) [5].

Visualizing expertise through normalized performance distribution
Salthouse (1991) contends that aside from the obvious knowledge gaps between experts and novices, experts are free from information processing constraints, as they are able to use past experiences to manage expectations for performance, focus attention on relevant information, and develop a deeply structured understanding of how knowledge is interrelated, allowing for easy assimilation into performance [5]. Moreover, experts are able to consistently execute exceptional performance regardless of internal or external conditions. In order to masterfully execute skills in variable conditions, experts have likely developed techniques and competencies to reliably perform their best. Accordingly, the goal of interventions to facilitate individual performance optimization should focus on reducing the learning curve to attain the trainable elements of expertise and to consistently enable high-level performance irrespective of situational barriers.
Performance of the Team
Due to the inherent integration of most occupations, effective participation in groups and teams is a fundamental element of many performance contexts. Groups, defined by a common purpose, are comprised of individuals that influence each other and the ultimate performance of the group profoundly [6]. Group cohesion is the fundamental property of team performance that can ultimately impact interpersonal dynamics, communication, and individuals’ commitment to the group’s goals.
Cohesiveness is essentially the tendency of a group to remain unified in the quest for completion of its objectives, and it is impacted by situation factors (e.g., proximity), personal factors (e.g., individual satisfaction within the group), leadership factors (e.g., interrelationship of the leader with other members of the group), and team factors (e.g., clearly defined roles) [6]. Effective teams share a common mental model of knowledge about relevant environmental factors that represents their ability to share understanding about a situation and engage in intentional and coordinated efforts to accomplish their common goal [7]. In order to optimize the performance of the team, it is critical to enhance these factors, as they will ultimately impact the effective pursuit of the team’s goal.
Surgery-Specific Performance Optimization
In 1999, the Institute of Medicine released a report estimating between 44,000 and 98,000 deaths occur annually in hospitals in the United States directly resulting from medical errors [8]. Additionally, the Joint Commission reported in 2006, more than 60% of sentinel events in healthcare are caused by poor communication [9]. In a recent survey of 72 surgeons (i.e., residents and attendings) at an academic medical institution, 40% of respondents reported they had witnessed an intraoperative complication directly resulting from the primary surgeon’s stress level [10]. These numbers are alarming, as the errors are largely preventable. As previously outlined, surgery is an incredibly cognitively demanding profession, and those cognitive demands can exceed one’s ability to manage them which ultimately leads to stress [2,3,4]. In a study of the effects of stress on surgical performance, Wetzel et al. (2006) found that stress can impact surgeons’ manual dexterity, emotional control, decision-making ability, and communication with the surgical team [4]. However, in their review of the impact of stress on surgical performance, Arora et al. (2010) found that surgeons who utilized stress-coping skills were able to mitigate the negative effects of stress better than surgeons who did not utilize these skills [2]. Similarly, communication breakdowns throughout the continuum of surgical care have been identified as significant barriers to favorable patient outcomes and can directly lead to patient harm [11]. Still, communication breakdowns can also be averted through interventions such as medical team training [12]. Another barrier to surgical performance being more closely examined is surgeon burnout. Burnout, a psychological condition characterized by depersonalization, emotional exhaustion, and low perceived personal accomplishment, is strongly correlated with major medical errors committed by surgeons [13]. Similar to acute stress and communication breakdowns though, it is possible to facilitate skills to counteract burnout by enhancing physician resilience and psychological well-being [14].
It is clear that within healthcare, a domain with such high-stakes situations, performance lapses can directly reduce patient safety and ultimately lead to heightened mortality. It is also evident there are skills surgeons can develop at the individual and team level to prevent lapses in performance. Thus, it is incredibly important to identify methods of optimizing these skills, and subsequently, surgical performance at the individual and team level, as this can reduce the potential for errors and increase patient safety.
Skill Mastery
Defining Expert Surgical Performance
Abernethy et al. (2008) explain that expert surgical performance is defined by mastery of self-monitoring perceptual, motor, attentional, and cognitive attributes of performance [15]. The authors point out that through extensive experience, deliberate practice, and study, expert surgeons develop high-level sensitivity to cognitive and technical errors and formulate schemas to correct these errors quickly. Likewise, experts develop highly attuned pattern-recall and perceptual discrimination (i.e., between normal/safe and abnormal/unsafe situations) which contributes to their anticipation of imminent situations with limited information.
Expert surgeons also display the ability to make more efficient, economical motor movements (i.e., subtle, smooth movements, exerting force only when required) during surgery than less experienced surgeons, which allows them to resist operative fatigue more effectively [15]. Further, experts display an ability to automate actions, which allows them to balance attention between multiple relevant sources of information. Expert surgeons also have more comprehensive declarative and procedural knowledge to intervene and solve problems than non-experts. This is characterized by forward-thinking reasoning (i.e., highly structured progressive inferences to facilitate diagnostic solutions based on pattern-recognition and high-level clinical reasoning). In addition to these elements of surgical expertise, several cognitive factors have been cited as important characteristics for performance excellence in surgery [16].
McDonald et al. (1995) interviewed 33 highly proficient surgeons; and participants reported that mental readiness for surgery was a greater determinant of successful performance than technical or physical readiness [16]. Furthermore, participants explained that several mental factors are imperative for surgical success. These include self-belief and confidence, positive mental imagery, full focus, distraction control, commitment and motivation, and constructive self-evaluation.
The goal of surgical education is to help trainees develop high-level proficiency in all of the aforementioned nontechnical skills. However, due to the extensive amount of experience necessary to execute these knowledge, abilities, and skills expertly, there is an apparent need to identify techniques and competencies to optimize trainees’ performance in order to expedite the learning curve of mastering surgical proficiencies. Surgical simulation training, consisting of deliberate practice and effective feedback, could be a strategy to reduce the learning curve to attain surgical expertise and maintain expertise through continued training.
Deliberate Practice
Skill mastery exists on a continuum from cognitive, to associative, to autonomous phase. The cognitive phase is the initial phase of learning a skill, characterized by a high-level of instruction and conscious effort to think through procedural steps by learners. The associative phase is the intermediate level of learning, defined by skill refinement, and less cognitive effort during performance. The autonomous phase is the advanced phase of learning highly automatic skill execution, with very little conscious thought on procedure steps, and freedom to direct attention to other relevant information for performance (see Fig. 2) [17]. Expertise and skill mastery, the highest performance standard in any domain, cannot be simplified as the result of innate ability or experience alone [18]. While natural aptitude for a particular skill set or extensively acquired experience are certainly contributing factors to expertise, Ericsson et al. (1993) argue that the process of attaining the maximal possible level of performance in a given domain, even for highly experienced performers, can result from deliberate efforts to practice skills and improve.

Summary of Fitts and Posner’s (1967) three-stage theory of motor skill acquisition
The process of deliberate practice consists of motivation by learners to exert effort to improve skills, immediate and informative performance feedback from an external source, and awareness of their performance results [18]. Upon attaining basic competency at a skill, learners should be given the opportunity to learn individualized problem-solving and critical-thinking methods to correct performance deficits on their own through additional practice. This process has been shown to increase speed, accuracy, and performance of motor, cognitive, and perceptual tasks, which are all hallmarks of expert surgical performance [15]. Simulation-based medical education may offer learners at all levels of experience an opportunity for deliberate practice to learn and acquire surgical skills or optimize their proficiency of already-learned surgical skills.
Indeed, a meta-analytic review of the effectiveness of simulation-based medical education featuring deliberate practice found that simulation training with deliberate practice is superior to standard clinical training programs in the acquisition of a variety of skills, including laparoscopic surgery [19]. Even for expert surgeons, deliberate practice through simulation training may offer an opportunity to prevent arrested development or decline of skills and to continue to develop and improve as a function of continual refinement of advanced cognitive processes attaining greater control during performance [20]. However, individual practice alone may be insufficient to aid a performer in attaining expertise in a particular domain. Rather, this process can be enhanced further at any level of skill mastery through objective feedback and performance coaching.
Value of Objective Feedback and Coaching
Feedback is a critical method of performance optimization for performers at any level, as it offers insight into the deficient mechanics of a particular skill that require improvement or highlights positive areas of performance that should be replicated in future performances. There are two sources of feedback: intrinsically based, which involves self-assessment of skill relative to the intended goal of the task, and augmented feedback, which consists of information provided by an external source that supplements intrinsic feedback [21]. The information gained from feedback can serve to motivate a performer to maintain effort in practice, reinforce desirable behavior or punish undesirable behavior, and can identify errors, then methods to correct, performance.
Coaching, the act of empowering performers to achieve improved performance through personal growth and self-directed learning, involves a collaborative relationship between a learner and a mentor where the mentor provides augmented feedback to optimize the learner’s performance [22]. Effective augmented feedback consists of information that is relevant, immediate, factual, confidential, respectful, helpful, tailored, and encouraging [23]. In the scope of skill mastery and developing expertise, augmented feedback is most impactful to enhance learning of new skills during the cognitive phase of skill mastery, whereas expert performers in the autonomous phase of skill mastery learn to develop highly effective self-monitoring systems to gather intrinsic feedback to fine tune performance as needed [19], which is one of several important characteristics of expert surgical performance [15].
Nonetheless, attaining and maintaining expertise is an arduous process as outlined throughout this section. The literature suggests that less experienced surgeons may be susceptible to experience drastically deteriorated performance due to heightened stress and an inability to adaptively cope with the demands of those difficult situations due to their lack of expertise [2]. Also, even expert surgeons may experience performance declines due to complacency and lack of skill maintenance [18], which may be further exacerbated by challenging clinical situations. This potential deficiency in the performance of less experienced and expert surgeons alike highlights the additional need to offer methods to enhance surgical performance that can be practiced deliberately, during surgical simulation training. Cognitive skills, often implemented by elite performers in other domains, may offer surgeons at all levels of expertise reliable techniques to optimize their performance.
Performance Optimization Training
In order to perform a successful surgery, surgeons must utilize both technical and nontechnical skills. While technical skills represent the execution of physical actions required for surgical performance, nontechnical skills are considered to be the social skills (e.g., communication, leadership), personal resource factors (e.g., stress-coping skills), and cognitive skills (e.g., situational awareness, decision-making) which supplement technical skills to aid in efficient and successful surgical performance [24]. For our purposes, and for the sake of simplicity, the term “cognitive skill s” will refer to trainable psychological abilities that underpin successful learning and performance, which encompasses stress-coping strategies, techniques to develop and maintain awareness, and effective decision-making, among other proficiencies [25]. Importantly, cognitive skills consist of psychological strategies and competencies designed to help performers consistently achieve their ideal cognitive state for performance [26] and have been implemented extensively in high-stress domains outside of medicine to address the cognitive, behavioral, emotional, and psychophysiological barriers to excellent performance [27]. The effectiveness of these skills in other domains may offer important insights into methods of optimizing the performance of surgeons.
Military
It is widely known that tactical operators (e.g., Army Soldiers, Special Forces, etc.) within the military face some of the most arduous, stressful, and mentally demanding work environments relative to the norm. They are tasked to perform at an extremely high standard, as they must make split second decisions that can mean the difference between life and death. As is the case with expert surgeons, expert military professionals have acquired both technical and nontechnical abilities that lead to consistently high performance. Recognizing the need to provide operators with the cognitive skills to effectively cope with and manage the physical and psychological demands, many various military organizations deliberately train tactical operators in this capacity.
In 1993, the United States Military Academy (USMA) established the Center for Enhanced Performance (CEP) that focused on training mental skills to cadets in order to enhance their performance in the classroom, in athletics, and in their military training. As these graduates assumed leadership positions in the Army, they noticed that little was being done throughout the force to teach soldiers these cognitive skills. As the need grew and the value was recognized, the Army established the Army Center for Enhanced Performance (ACEP) in 2006. ACEP (now the Comprehensive Soldier and Family Fitness program, CSF2), through expert practitioners, teaches cognitive skills and competencies (e.g., goal setting, mental imagery, attention control, optimism, confidence, energy control, etc.) to soldiers in order to enhance their mental toughness and resiliency, thereby enhancing their performance on and off the battlefield [28, 29]. Various research studies have demonstrated positive effects in terms of performance as compared to control groups, knowledge of and use of mental skills, and resilience [28, 30, 31].
The Special Operations Command of the US Military also recognized the need for systematic training and development of cognitive skills to enhance performance, resilience, and overall well-being [32]. In 2014, the preservation of the CSF2 program was developed to help special operators and their families maintain and improve readiness, effectiveness in the battlefield, and long-term well-being. The program takes a holistic approach through training special operators in four domains of physical, spiritual, mental, and social well-being. The approach involves an interdisciplinary team comprised of strength and conditioning coaches, athletic trainers, physical therapists, dieticians, sport psychologists, and licensed clinical social workers.
In general, the military takes a developmental approach to training tactical operators. A common phrase outlining their approach is “crawl, walk, run,” which aligns nicely with the theory of deliberate practice. In the “crawl” stage, learners are given a description and purpose of the task or skill, description of performance standards, visual demonstration of the skill, and any necessary information required to execute the skill. In the “walk” stage, learners practice the skill in a slow, step-by-step pace, receive feedback throughout, and practice the skill until they can complete it entirely without feedback or coaching (i.e., akin to the cognitive and associative phases of deliberate practice). In the “run” stage, learners execute the skill at full speed under realistic battlefield conditions (akin to the autonomous stage of deliberate practice). In this stage, the military often relies on various forms of simulation to generate battlefield conditions without battlefield risk [33]. As the learner moves through the stages, the levels of challenge, stress, and pressure increase in order to test their ability under conditions they might face in the battlefield, which can be incredibly challenging and stressful [34]. Importantly, when learners reach the stage of learning where they participate in more advanced tactical simulations, they are less cognitively focused on the execution of the skill and able to apply those mental resources elsewhere (e.g., critical thinking and problem-solving).
Elite Athletics
Historically, performers’ use of cognitive skills has received the most attention in elite athletics . Dating back to Coleman Griffith’s (1928) work to study the psychology of sport and his application of psychological principles to enhance the performance of athletes [35], cognitive skills have been acknowledged as crucial elements of performance excellence in sport [26]. The US Olympic Committee first established a sport psychology program in 1983 [36], and since that time, cognitive skills training has been a prominent part of the training regimen for champion athletes.
Gould et al. (2002) interviewed ten Olympic champion athletes (representing nine disciplines) to determine what psychological factors had influenced their athletic performance [37]. The authors determined that cognitive skills such as mental imagery and rehearsal (i.e., mentally rehearsing a performance), arousal regulation (i.e., relaxation and activation skills to allow to optimize arousal levels), goal setting (i.e., setting effective goals for performance), attention management (i.e., maintaining focus and concentration), and well-developed action plans for competition (i.e., to directing thoughts and behaviors) are being used regularly by Olympic champions. Importantly, while these champion athletes reported they had learned some of these skills serendipitously through self-development, direct cognitive skills training from coaches and sport psychology consultants were important factors in their performance excellence. Cognitive skills training to optimize athletic performance has also been conducted effectively with professional athletes [38], collegiate athletes [39], and junior athletes [40], which highlights the applicability of this type of training across levels of experience.
Aviation
Similar to the expectations for surgeons and healthcare providers, pilots and cockpit crews are expected to consistently perform without errors, as the stakes for potential errors are extremely high [41]. The similarities of these fields extend to the benefit of deliberate practice through simulation training for skill mastery, as simulator-based decision-making training has been shown to enhance pilots’ skills at all levels (i.e., depending on the fidelity of the simulation) and decision-making [42, 43]. However, unlike the culture of healthcare where the acknowledgement of performance errors and the factors that contribute to it (e.g., stress, fatigue, interpersonal and team-related issues) has traditionally been discouraged, the aviation industry has created a culture where errors are acknowledged and dealt with effectively [41]. Furthermore, cognitive skills training programs to optimize performance, manage stress effectively, and maintain situational awareness (i.e., attention management), as well as team-based training to enhance teamwork and communication (i.e., based in human factors training), and manage crisis situations, effectively have been implemented with regularity.
Situational awareness has been identified as a significant component of effective decision-making in pilots, as it allows individuals to balance attention between the various relevant environmental elements, comprehend situational factors based on individual elements, and project the future status of a situation based on these factors [44]. Endsley and Robertson (2000) explain that one component of enhancing aviation teams’ situational awareness is to train individuals in cognitive and team-based skills in attention and thought management to reduce the impact of distractions, to develop action plans for contingencies, attention sharing and communication with others, and information seeking/filtering [45]. The authors developed a team-based situational awareness program that focused, in part, on implementing these skills to help individuals manage distractions, improve their situational awareness, and enhance teams’ communication and vigilance. The large majority of participants (89%) rated the skills as “very useful” or “extremely useful,” and at least 50% of participants reported a moderate behavioral change in their use of the skills taught through the program. There have also been attempts to implement cognitive skills to optimize the performance of military pilot trainees.
Military pilots are routinely confronted with challenging and stressful performance situations that require them to manage stress and thought processes effectively to optimize performance [46]. Fornette et al. (2012) implemented a cognitive-adaptation program with military pilot trainees in a randomized controlled study design, which implemented mindfulness and cognitive restructuring techniques. Mindfulness techniques are essentially strategies designed to increase awareness by maintaining open attention in the present moment and reserve judgment or visceral reactivity, whereas cognitive restructuring techniques aim to reprogram how we perceive or think about a particular situation which can lead to more positive and adaptive thoughts during stressful situations [46]. The authors found that trainees who had below-median performance prior to the intervention significantly improved their in-flight performance after cognitive-adaptation training, and 70% of all intervention-group trainees reported they were able to lower their in-flight stress more effectively after training. McCrory et al. (2013) introduced a cognitive skills training program consisting of goal setting, imagery, and attention management during cognitive skills coaching sessions with military pilot trainees to enhance their confidence to operate the aviation equipment and manage stress [47]. At the conclusion of the study, participants displayed significantly increased confidence, reduced anxiety, and increased self-regulatory behavior (flight planning, remembering flight brief information, contingency planning, etc.).
Lessons Learned for Surgical Education
There are several important factors related to effective cognitive and team-based skills training that can be extracted from high-pressure domains and applied to surgical education. For example, team-based skills training has consisted of teaching learners methods to communicate effectively and sharing mental models and information to enhance teams’ collective situational awareness [45]. Cognitive skills training has aimed to teach learners skills and competencies such as methods of developing effective goals and action plans for performance, mental imagery/rehearsal, attentional and thought control, situational awareness, optimism, methods to build confidence, energy management, mental toughness, and resilience [31, 37, 46, 47].
These skills are often implemented during simulation training where deliberate practice can be applied to facilitate the integration of these techniques as habits for performance as learners transition through the stages of learning. The development of these skills as performance habits frees up cognitive processing for problem-solving and decision-making in more advanced training scenarios [32, 47]. Furthermore, research with soldiers and Olympic athletes suggests that cognitive skills coaching from trained coaches and sport psychologists is an important source to help these performers learn how to use cognitive skills effectively [32, 37, 47]. These factors are important considerations when determining best practices of applying team-based and cognitive skills with surgeons. It is important, though, to identify how these skills have already been implemented in surgical education. This will help determine potential areas of improvement for nontechnical skills training.
Current State of Team-Based and Cognitive Skills Training in Surgery
Optimizing Team Performance
Effective teamwork is an incredibly important factor contributing to surgical success and ultimately patient outcomes [48,49,50]. There are several salient elements of effective surgical team performance, which have been discussed previously in this chapter but include leadership and understanding of roles, mutual performance monitoring, shared mental models and anticipation of needs, adaptability, common purpose (i.e., and placing that purpose above individual goals), and closed-loop communication [51]. Traditionally, surgical training has focused on enabling surgical trainees to improve their individual technical skills, but relatively little work has been done to enhance these interpersonal, team-based skills that are critical to the optimal performance of the entire surgical team [7]. One of the most significant advances in team training within healthcare has been the development of the Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS) [51].
TeamSTEPPS is a didactic-based curriculum that can assist healthcare systems to develop effective clinical teams and is available nationally through the Agency for Healthcare Research and Quality (AHRQ) [51]. The curriculum is delivered via five educational modules which help learners identify and understand the benefits of team training and teach them skills and competencies to enhance their leadership, communication, situational awareness and monitoring, and mutual support. In a randomized controlled study of this program’s effectiveness on multiple levels of healthcare provider performance (i.e., perception about ability to implement teamwork concepts in performance, learning of teamwork concepts, observed teamwork behaviors, and self-reported use of teamwork behaviors), the TeamSTEPPS-trained providers significantly enhanced their perceptions of their ability to perform teamwork behaviors, enhanced their performance on a written test of optimal teamwork behaviors (i.e., learning), increased their quality and quantity of preoperative case briefings and the quality of teamwork behaviors, and demonstrated positive changes in the culture of patient safety [52]. Gardner and Scott (2015) explain that simulation training may further optimize the effectiveness of team-based training, as surgical teams can be aided in the deliberate practice and mastery of these important interpersonal factors through contextually accurate environments and didactic reflection on best practices of team dynamics [7].
Leadership has also been recognized as an important factor in the performance of surgical teams [53]. Poor leadership from the primary surgeon, characterized by vague and ineffective communication, expression of frustration, poor situational awareness, and poor planning, is highly correlated with avoidable surgical errors [54]. Conversely, effective leadership consists of emphasizing the team’s collective goal, displaying motivation and enthusiasm, creating learning opportunities for teammates, forming bonds with teammates, engaging teammates to gather additional perspectives, and considering individual abilities and needs [53, 55]. Formal leadership training for experienced surgeons has been effective, as the majority of 21 surgeons who participated in a leadership training program felt that the program was effective and encouraged self-reflection to improve deficient intraoperative behaviors [56].
Surgical residents could greatly benefit from leadership training incorporated during simulation training, due to the limited opportunities for trainees to practice these skills in the clinical environment [57]. Bearman et al. (2012) implemented a 2-day nontechnical skills training course with 12 surgical residents which featured practice of intraoperative communication (e.g., identifying challenges and benefits, briefing, debriefing, task-focused communication, graded assertiveness) and role delegation (i.e., important elements of surgical leadership), during advanced cardiac life support simulation exercises. The authors found that all participants reported that all of the leadership skills taught and the simulation scenarios were valuable educational tools to enhance their nontechnical skills.
The findings of the few studies implementing teamwork and leadership skills during surgical simulation training have found promising results. However, based on the relatively limited research of the impact of these nontechnical skills on surgical performance, it is clear that much more work needs to be done to implement these skills in randomized controlled studies.
Optimizing Individual Performance
While teamwork and leadership skill development largely occur outside of the simulation lab, cognitive skills, like those psychological tools and strategies implemented in the military, in aviation, and in elite athletics, have begun to be implemented during surgical simulation training to optimize the individual performance of surgeons. While research on the effects of cognitive skills in surgical education is in its infancy, the literature is indicative that cognitive skills training may be an effective supplement to technical skills training [58,59,60,61,62,63,64,65,66,67,68].
In spite of the recognized importance of multiple psychological factors in successful surgical performance [16], surgical education researchers have primarily focused on implementing only one cognitive skill with learners, mental imagery (MI). Synonymous with mental rehearsal and mental practice, MI is the process of creating quasi-sensory imagined experiences, which exist in the mind in the absence of those physical stimulus conditions, which can produce genuine sensory and perceptual experiences [67, 68].
For surgical novices, Arora et al. (2011) demonstrated that a group who received MI training in addition to physical practice during simulated laparoscopic cholecystectomy (LC) training significantly outperformed controls that received physical practice alone and had a shorter learning curve of the procedure [58]. Arora et al. (2011) discovered participants reported significantly lower stress compared to a control group (measured subjectively with the State-Trait Anxiety Inventory (STAI) and objectively displayed lower stress (measured with heart rate and cortisol levels) [59]. In regard to optimizing the technical and nontechnical performance of surgical trainees, Komesu et al. (2009) found that obstetrics and gynecology residents who received MI training on the procedural steps of a cystoscopy significantly outperformed controls based on objective measures of surgical performance and considered MI to be a more useful pre-performance preparation strategy than reading a standard textbook [60]. MI may also be an effective tool to enhance trainee’s teamwork, as emergency, anesthesia, and surgery residents who received MI training significantly enhanced their teamwork during a simulated trauma resuscitation scenario compared to controls who only received technical training [61].
MI may also be an effective tool for continuing education of experienced surgeons. Immenroth et al. (2007) conducted a randomized controlled study with 98 experienced surgeons undergoing laparoscopic training and assigned participants to a MI group, an additional technical training group, and a control group [62]. Results indicated that LC performance on a physical simulator was significantly higher at posttest for the MI group, who reported that MI was a valuable tool in their education. Patel et al. (2012) found that vascular surgeons who received MI training had significantly less intraoperative errors during critical stages of arterial procedures [63].
Results from the research implementing MI with surgical novices, slightly more experienced trainees, and experienced surgeons have largely indicated that MI is an effective training tool [58,59,60,61,62,63]. In addition to the implementation of MI, there have been some, albeit significantly less, attempts to incorporate more comprehensive cognitive skills training in surgical education.
Maher et al. (2013) implemented a stress management program with first- and third-year surgical residents who were asked to perform a high-stress patient care simulation module [3]. The stress management group received training in energy and attention management techniques and MI. While differences in technical performance were not statistically significant, there was a trend toward enhanced performance (i.e., measured with OSATS) for the experimental group, and the stress management training program was rated as valuable by 91% of participants. In a randomized controlled study that implemented a stress management intervention with experienced surgeons, the experimental group displayed significantly increased observed teamwork (i.e., measured with the Observational Teamwork Assessment for Surgery), increased stress-coping skills (i.e., measured with the Surgical Coping Questionnaire), and reduced stress (i.e., measured with heart rate variability) compared to controls [4]. Experimental group participants also displayed improved technical skills, confidence, and decision-making after this training.
Recently, a novel and comprehensive mental skills curriculum (MSC) has been developed to reduce surgical trainees’ stress and enhance their performance [64,65,66]. A multidisciplinary team consisting of a surgeon educator with extensive experience in simulation-based research, a performance psychologist with extensive experience in mental skills training, and an education psychologist with expertise in instructional design collaborated to develop the curriculum based on David Kern’s (2009) model [64, 69]. Following a needs assessment, identification of goals and educational objectives, and development of instructional methods, the curriculum was formulated. Consisting of eight video-education modules, a workbook to allow for immediate practice of learned mental skills, and applied practice of skills during laparoscopic simulator training, this MSC teaches surgical trainees cognitive skills such as goal setting, energy management (i.e., relaxation and “psyching-up”), attention and thought management, mental imagery, refocusing strategies, and performance routines. Further information on this MSC is described in detail elsewhere [64].
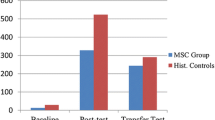
In a study of the efficacy of this novel MSC to enhance surgical novices’ laparoscopic intracorporeal suturing performance and use of performance-enhancing mental skills, results indicated that MSC-trained novices significantly enhanced their laparoscopic performance and increased their use of mental skills from baseline to posttest [64]. Additionally, the majority of participants expressed that the MSC was effective in optimizing their laparoscopic performance. In another study to determine the effectiveness of the curriculum to reduce novices’ stress during two validated stress tests (i.e., the Trier Social Stress Test and the O’Connor Tweezer Dexterity Test), the MSC was effective at reducing novices’ perceived stress and workload during both stress tests [65]. This finding indicates that this MSC may be effective at reducing novices’ stress in a variety of situations. In a subsequent randomized controlled trial of the effectiveness of the MSC to enhance surgical novices’ laparoscopic suturing performance compared to controls, MSC group participants displayed significantly enhanced mental skill use from baseline to posttest and significantly higher laparoscopic skill retention over a period without technical skills training compared to controls [66]. These findings indicate that a comprehensive MSC can offer several significant benefits to surgical novices, including significantly enhanced surgical skills [64], use of mental skills [64], reduced stress and workload during validated stress tests [65], and surgical skill retention [66]. It is evident, then, that a comprehensive MSC may offer incremental benefits to surgical performance beyond those of single-skill cognitive skill interventions.
Burnout, as described previously, is a detrimental psychological condition that can lead surgeons to commit significant medical errors [13]. Unlike acute disruptions to performance, like stress or loss of focus, burnout is a chronic syndrome that results from situational job demands (e.g., workload is too high, time pressures, lack of control, lack of feedback, etc.) that lead one to feel overloaded, which can contribute to diminished psychological well-being and ultimately, reduced quality of patient care [13, 70]. However, research has shown that psychological resilience and grit can enhance physicians’ psychological well-being and attenuate the negative effects of burnout on performance [14, 71, 72]. Resilience is considered to be one’s ability to respond and cope with stress in a positive and adaptive manner, “bounce back” when faced with challenges and grow stronger through this process [14]. Similarly, grit is a psychological trait characterized by passion and perseverance to pursue long-term goals [71]. Resilience and grit may moderate the relationship between burnout and performance, and interventions designed to enhance physicians’ resilience and grit could be effective at preventing or managing burnout and optimizing performance. Presently, there are no known attempts to implement resilience-enhancing interventions with surgeons. However, there have been attempts to implement such interventions with other healthcare providers, and these studies may provide insight into how skills to enhance resilience can be implemented effectively with surgeons. Sood et al. (2011) implemented a 90-min stress management and resilience training (SMART) intervention with department of medicine faculty that focused on teaching these physicians how to manage attention, nonjudgmentally, in the present moment and maintain a flexible psychological disposition to adapt to situations as opposed to maintaining fixed prejudices [73]. Also, participants were instructed on how to execute a paced breathing meditation for relaxation. In this randomized controlled study, the authors found that this resilience intervention led to significant improvements in resilience, perceived stress, and quality of life at 8 weeks post-intervention compared to controls. Essentially, this intervention focused on teaching similar principles to mindfulness, which has been described previously in this chapter and has been identified as a cognitive skill that can potentially reduce physicians’ burnout [46, 74, 75].
In a study of the effectiveness of a mindfulness-based intervention that taught physicians how to engage in mindful meditation exercises to develop self-awareness for cognitions and physiological states and awareness for how they communicate with others, Krasner et al. (2009) found that this intervention was effective at reducing participants’ burnout and total mood disturbances and increasing their empathy, conscientiousness, and emotional stability [74]. Similarly, a mindfulness-based stress reduction intervention that focused on teaching meditative exercises to increase relaxation was incorporated with healthcare providers in a randomized controlled study [75]. The authors found that this intervention was effective at reducing the providers’ perceived stress, burnout, and distress compared to controls. Based on this evidence with other healthcare providers, it is possible that cognitive skills interventions designed to increase psychological well-being and reduce burnout through mindfulness and psychological resilience techniques may be effective if applied with surgeons, but research must be performed in this area to determine the efficacy of these skills to reduce surgeons’ burnout and optimize performance.
Performance Coaching
The use of feedback to enhance clinical performance has long been incorporated in surgical education through the apprenticeship model [76]. Surgical faculty have traditionally provided knowledge to trainees on the execution of technical skills based on personal professional experience and advice [77]. Trainees are expected to absorb technical and nontechnical skills in the operating room directly through repetition or by observing modeled behavior paired with knowledge by surgical faculty. Surgical skills coaching takes this process a step further, as a coach can collaborate with trainees during deliberate practice of technical and nontechnical surgical skills during simulation training to achieve self-determined goals through objective assessment and feedback, structured debriefing, guided self-reflection, and behavior modeling [78, 79].
In a systematic review of the literature, Min et al. (2015) found that surgical skills coaching can be effectively incorporated in simulation training because this setting allows for a safe practice environment and by viewing videotapes of learners’ intraoperative performance, which allows for enhanced self-reflection of technical skills and delivery of individually tailored feedback [79]. Coaching interventions , which commonly consist of an informative lecture, augmented concurrent feedback, and debriefing, can significantly enhance technical performance. Importantly, coaching interventions were shown to reduce intraoperative error rates.
In regard to nontechnical skills coaching, these interventions focused primarily on enhancing learners’ team-based skills (e.g., communication) and leadership [78]. The majority of reviewed studies found that coaching significantly enhanced learners’ nontechnical skills. However, the results from these studies should be taken with some caution, as some of the studies did not use control groups, the majority of observers assessing intraoperative nontechnical skills were not blinded, and there were no longitudinal assessments of nontechnical skills.
The literature on the impact of surgical skills coaching to optimize surgeons’ technical and nontechnical skills performance is indicative that this is a highly effective training paradigm. For trainees, who are frequently performing surgical procedures in the operating room but lack accurate self-assessment and may not regularly reflect analytically on methods to optimize their performance, coaching during deliberate practice of skills may offer additional opportunities for experiential learning and growth [78]. It is unclear, though, how well-received coaching for continuing education would be for experienced surgeons. A recent study by Mutabdzic et al. (2015) indicated that some surgeons reported a lack of interest to participate in coaching to improve their technical skills because they did not feel that practicing technical skills further would enhance patient outcomes. There was concern that coaching would be perceived as being related to incompetence by peers and trainees, and there was concern that coaching would remove elements of control over self-directed learning [80]. However, Ericsson (1993, 2004) contends that even experienced surgeons may experience arrested skill development or surgical skill decay in the absence of continued deliberate practice of skills [18, 20]. Through deliberate practice that allows experienced performers to seek out training situations that challenge their current level of performance, these individuals are able to develop cognitive mechanisms to monitor and control performance in similar performance situations. A surgical skills coach could identify areas for experienced surgeons’ to improve their skills and appropriate tasks to challenge their current skill level, which could lead to further skill mastery and the attainment of expertise. Indeed, Stefanidis et al. (2016) recently conducted a study in which they reviewed intraoperative videos of practicing surgeons to identify areas for improvement, developed a coaching curriculum accordingly, and implemented the coaching curriculum with the participating surgeons in group and one-on-one sessions [81]. The authors found that blinded group sessions allowed practicing surgeons to participate in peer review of intraoperative technical skills, which afforded them the opportunity to learn from each others’ successful performances and areas for improvement. The authors also posit that the ideal surgical coach for technical skills is a well-respected peer, with contextually specific knowledge of the learner’s surgical subspecialty, whereas nontechnical skills coaching may be best served by a human factors specialist or similar domain-specific expert who can provide insightful performance feedback. These considerations emphasize the need to incorporate surgical skill coaching with trainees and experienced surgeons alike.
Future Directions for Performance Optimization in Surgery
The research strongly suggests that nontechnical techniques such as cognitive skills training, leadership and team-based skills training, and coaching are effective at optimizing surgical performance when implemented during surgical simulation training. However, the research on implementing nontechnical skills training in surgical education is still emerging, and researchers could benefit greatly from considering how these skills have been implemented in other high-stakes domains. For instance, mental imagery is the cognitive skill that has been used most frequently to enhance the surgical performance of surgical novices [58, 59], trainees [60, 61], and experienced surgeons [62, 63]. However, compared to the much more extensive cognitive skills training programs in the military [28,29,30, 32] and elite athletics [36,37,38,39,40] that have included multiple effective skills with performers, there is room to expand the application of cognitive skills training in surgical education to include several more strategies and competencies to optimize performance. Some skills, such as resilience and mindfulness, have been taught to healthcare providers outside of surgery, and the results of these studies indicate that these skills can reduce provider burnout and enhance empathy and quality of life [74, 75].
Indeed, there are few studies that have incorporated multiple cognitive and team-based skills into a comprehensive training curriculum that facilitates learners’ deliberate practice of these skills with the guidance of a coach during surgical simulation training. Research has clearly demonstrated that individual cognitive factors (e.g., confidence, positive MI, concentration, distraction control, commitment and motivation, and constructive self-evaluation) [16] and team dynamics (e.g., leadership and understanding of roles, mutual performance monitoring, shared mental models and anticipated needs, common purpose, adaptability, and closed-loop communication) [51] significantly impact surgical performance and are important elements of surgical expertise. The literature suggests that there is an extensive learning curve to become an expert surgeon [15], which illustrates the importance of developing strategies to supplement the experiential learning process and reduce the learning curve for surgical trainees and practicing surgeons to approach and achieve skill mastery.
Within medicine and other high-stress domains, deliberate practice through simulation training has offered learners a modality to practice skills in a safe environment [19]. This may be the ideal setting for learners to learn and train to use nontechnical skills to optimize their performance, as training during simulated exercises has proven to be an effective training paradigm to teach learners these skills [7]., In spite of a seemingly intuitive conclusion, that a comprehensive nontechnical skills curriculum which teaches multiple individual cognitive skills and team-based skills should be developed and implemented widely to offer surgical trainees the strategic flexibility to manage dynamic intraoperative challenges effectively, little work is being done to this end. TeamSTEPPS is one exception, as this national team-training curriculum is being implemented widely through the AHRQ to facilitate enhanced clinical team performance [51]. TeamSTEPPS has been largely accepted and implemented throughout several healthcare systems [52], and while it is effective at enhancing clinical team performance, it does not aim to enhance individual providers’ performance. Conversely, a recently developed comprehensive MSC has been successful at enhancing surgical novices’ laparoscopic suturing performance, use of mental skills [64], and surgical skill retention [66] and reducing their stress and workload during two validated stress tests [65].
If surgical educators are aiming to optimize surgical performance of trainees or practicing surgeons, they should develop a robust and comprehensive cognitive and team-based skills training curriculum, modeled after TeamSTEPPS and this novel MSC, which features skills training to enhance learners’ communication, leadership, stress-coping awareness and decision-making, attention management, and resilience (see Fig. 3). Furthermore, a comprehensive performance optimization curriculum should feature deliberate practice and objective feedback with performance coaching to offer learners an opportunity to master newly learned technical and nontechnical skills. Also, similar to the “crawl, walk, run” approach of the US military, educators should gradually increase the difficulty of training to coincide with the stages of learning, which will force trainees to develop increasingly complex cognitive processes to execute skills and optimize their performance under variable and challenging clinical situations. In conclusion, when training the next generation of surgeons, surgical educators should develop comprehensive curricula along these lines to teach and optimize technical and nontechnical skills concurrently.

The necessary components of a comprehensive performance optimization curriculum in surgery
Abbreviations
- ACEP:
-
Army Center for Enhanced Performance
- AHRQ:
-
Agency for Healthcare Research and Quality
- CEP:
-
Center for Enhanced Performance
- CSF2:
-
Comprehensive Soldier and Family Fitness program
- LC:
-
Laparoscopic cholecystectomy
- MI:
-
Mental imagery
- MSC:
-
Mental skills curriculum
- OSATS:
-
Objective structured assessment of technical skills
- SMART:
-
Stress-management and resilience training
- STAI:
-
State-Trait Anxiety Inventory
- TeamSTEPPS:
-
Team Strategies and Tools to Enhance Performance and Patient Safety
- USMA:
-
US Military Academy
- VR:
-
Virtual reality
References
Norman G, Eva K, Brooks L, Hamstra S. Expertise in medicine and surgery. The Cambridge handbook of expertise and expert performance. New York: Cambridge University Press; 2006. p. 339–53.
Arora S, Sevdalis N, Nestel D, Woloshynowych M, Darzi A, Kneebone R. The impact of stress on surgical performance: a systematic review of the literature. Surg. 2010;147(3):318–30.
Maher Z, Milner R, Cripe J, Gaughan J, Fish J, Goldberg AJ. Stress training for the surgical resident. Am J Surg. 2013;205(2):169–74.
Wetzel CM, Kneebone RL, Woloshynowych M, Nestel D, Moorthy K, Kidd J, et al. The effects of stress on surgical performance. Am J Surg. 2006;191(1):5–10.
Salthouse TA. Expertise as the circumvention of human processing limitations. In: Ericsson TA, Smith J, editors. Toward a general theory of expertise. New York: Cambridge University Press; 1991. p. 286–300.
Eys MA, Burke SM, Carron AV, Dennis PW. The sport team as an effective group. In: Williams JM, editor. Applied sport psychology: personal growth to peak performance. New York: McGraw-Hill; 2010. p. 132–48.
Gardner AK, Scott DJ. Concepts for developing expert surgical teams using simulation. Surg Clin North Am. 2015;95(4):717–28.
Institute of Medicine (IOM). In: Kohn LT, Corrigan JM, Donaldson MS, editors. To err is human: building a safer health system. Washington, D.C: National Academy Press; 2000.
The Joint Commission. The joint commission’s annual report on quality and safety. (https://www.jointcommission.org/assets/1/6/2007_Annual_Report.pdf) Accessed: 14 July 2016.
Anton NE, Montero PN, Howley LD, Brown C, Stefanidis D. What stress coping strategies are surgeons relying upon during surgery? Am J Surg. 2015;210(5):846–51.
Nagpal K, Vats A, Lamb B, Ashrafian H, Sevdalis N, Vincent C, Moorthy K. Information transfer and communication in surgery: a systematic review. Ann Surg. 2010;252(2):225–39.
Awad SS, Fagan SP, Bellows C, Albo D, Green-Rashad B, De La Garza M, Berger DH. Bridging the communication gap in the operating room with medical team training. Am J Surg. 2005;190(5):770–4.
Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, Collicott P, Novotny PJ, Sloan J, Freischlag J. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995–1000.
Epstein RM, Krasner MS. Physician resilience: what it means, why it matters, and how to promote it. Acad Med. 2013;88(3):301–3.
Abernethy B, Poolton JM, Masters RS, Patil NS. Implications of an expertise model for surgical skills training. ANZ J Surg. 2008;78(12):1092–5.
McDonald J, Orlick T, Letts M. Mental readiness in surgeons and its links to performance excellence in surgery. J Pediatr Orthop. 1995;15(5):691–7.
Fitts PM, Posner MI. Human performance. Oxford, England: Brooks/Cole; 1967.
Ericcson KA, Krampe RT, Teschromer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100(3):363–406.
McGaghie WC, Issenberg SB, Cohen ER, Barsuk JH, Wayne DB. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med. 2011;86(6):706–11.
Ericcson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10 Suppl):S70–81.
Coker CA, Fishman MG. Motor skill learning for effective coaching and performance. In: Williams JM, editor. Applied sport psychology: personal growth to peak performance. New York: McGraw-Hill; 2010. p. 21–41.
Bresser F, Wilson C. What is coaching? In: Passmore J, editor. Excellence in coaching: the industry guide. London: Kogan Page Limited; 2010. p. 9–27.
Ovando MN. Constructive feedback: a key to successful teaching and learning. Int J of Edu Mgmt. 1994;8:19–22.
Flin R, O’Connor P, Crichton M. Safety at the sharp end: a guide to non-technical skills. Aldershot: Ashgate; 2008.
Dictionary of Sport and Exercise Science and Medicine by Churchill Livingstone. S.v.psychological skills. (http://medicaldictionary.thefreedictionary.com/psychological+skills). Accessed: 15 July 2016.
Williams JM, Straub WF. Sport psychology: past, present, future. In: Williams JM, editor. Applied sport psychology: personal growth to peak performance. New York: McGraw-Hill; 2010. p. 1–17.
Defining the practice of sport and performance psychology. American Psychological Association: Division 47 (Exercise and Sport Psychology) Practice Committee of the American Psychological Association. (http://www.apadivisions.org/division-47/about/resources/defining.pdf). Accessed: 15 July 2016.
Hammermeister J, Pickering M, Lennox, A. Military applications of performance psychology methods and techniques: an overview of practice and research. J Perform Psychol. 2011;3–34.
Zinsser N, Perkins LD, Gervais PD, Burbelo GA. Military application of performance-enhancement psychology. Mil Rev. 2004;84(5):62–5.
Adler AB, Bliese PD, Pickering MA, Hammermeister J, Williams J, Harada C. Mental skills training with basic combat training soldiers: a group-randomized trial. J Appl Psychol. 2015;100(6):1752–66.
Bartone PT, Roland RR, Picano JJ, Williams TJ. Psychological hardiness predicts success in US Army special forces candidates. Int J of Sel and Assess. 2008;16(1):78–81.
Myatt CA, Auzenne JW. Resourcing interventions enhance psychology support capabilities in special operations forces. J Spec Oper Med. 2011;12(4):54–9.
Summers J. Simulation-based military training: an engineering approach to better addressing competing environmental, fiscal, and security concerns. J Wash Acad Sci. 2012;98(1):9–30.
Taylor MK, Sausen KP, Potterat EG, Mujica-Parodi LR, Reis JP, Markham AE, et al. Stressful military training: endocrine reactivity, performance, and psychological impact. Aviat, Sport, Environ Med. 2007;78(12):1143–9.
Griffith CR. Psychology of athletics. New York: Scribner; 1928.
U.S. Olympic Committee. U.S. Olympic committee establishes guidelines for sport psychology services. J Sport Psychol. 1983;5:4–7.
Gould D, Dieffenbach K, Moffett A. Psychological characteristics and their development in olympic champions. J Appl Sport Psychol. 2002;14(3):172–204.
Gardner FL. Applied sport psychology in professional sports: the team psychologist. Prof Psychol Res and Pract. 2001;32(1):34–9.
Daw J, Burton D. Evaluation of a comprehensive psychological skills training program for collegiate tennis players. Sport Psychol. 1994;8(1):37–57.
Mamassis G, Doganis G. The effects of a mental training program on juniors pre competitive anxiety, self-confidence, and tennis performance. J Appl Sport Psychol. 2004;16(2):118–37.
Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ. 2000;320(7237):745–9.
Hays RT, Singer MJ. Simulation fidelity in training system design: bridging the gap between reality and training. New York: Edwards; 1989.
Connolly TJ, Blackwell BB, Lester LF. A simulator-based approach to training in aeronautical decision making. Aviat Sp Environ Med. 1989;60:50–2.
Endsley MR. Toward a theory of situation awareness in dynamic systems. J Hum Factors Ergon Soc. 1995;37(1):32–64.
Endsley MR, Robertson MM. Training for situation awareness in individuals and teams. In: Endsley MR, Garland DJ, editors. Situation awareness analysis and measurement. Mahwah: Lawrence Erlbaum Associates; 2001. p. 349–62.
Fornette MP, Bardel MH, Lefrancois C, Fradin J, Massioui FE, Amalberti R. Cognitive-adaptation training for improving performance and stress management of air force pilots. Int J Aviat Psychol. 2012;22(3):203–23.
McCrory P, Cobley S, Marchant P. The effect of psychological skills training on self-regulation behavior, self-efficacy, and psychological skill use in military pilot trainees. Milit Psychol. 2013;25(2):136–47.
National Confidential Enquiry into Perioperative Deaths. Functioning as a Team: The 2002 Report of the National Confidential Enquiry into Perioperative Deaths; 2002. Available from: URL: http://www.ncepod.org.uk/pdf/2002/02full.pdf. Accessed: 22 July 2016.
Young GJ, Charns MP, Daley J, Forbes MG, Henderson W, Khuri SF. Best practices for managing surgical services: the role of coordination. Healthcare Manag Rev. 1996;22(4):72–81.
Sorbero ME, Farley DO, Mattke S, Lovejoy S. Outcome measures for effective teamwork in inpatient care (RAND technical report TR-462-AHRQ). Arlington: RAND Corporation; 2008.
King HB, Battles J, Baker DP, et al. TeamSTEPPS: team strategies and tools to enhance performance and patient safety. In: Henriksen K, Battles JB, Keyes MA, Rockville MD GML, editors. Advances in patient safety: new directions and alternative approaches, Performance and tools, vol. 3. Rockville: Agency for Healthcare Research and Quality (US); 2008.
Weaver SJ, Rosen MA, DiazGranados D, Lazzara EH, Lyons R, Salas E, et al. Does teamwork improve performance in the operating room? A multilevel evaluation. Jt Comm J Qual and Patient Saf. 2010;36(3):133–42.
Hu YY, Parker SH, Lipsitz SR, Arriaga AF, Peyre SE, Corso KA, et al. Surgeons’ leadership styles and team behavior in the operating room. J Am Coll Surg. 2016;222(1):41–51.
Siu J, Maran N, Paterson-Brown S. Observation of behavioral markers of non-technical skills in the operating room and their relationship to intra-operative incidents. Surgeon. 2016;14(3):119–28.
Patel VM, Warren O, Humphris P, Ahmed K, Ashrafian H, Rao C, et al. What does leadership in surgery entail? ANZ J Surg. 2010;80(12):876–83.
Flin R, Yule S, Paterson-Brown S, Youngson G. Teaching surgeons about non-technical skills. Surgeon. 2007;5(2):86–9.
Bearman M, O’Brien R, Anthony A, Civil I, Flanagan B, Jolly B, et al. Learning surgical communication, leadership, and teamwork during simulation. J Surg Educ. 2012;69(2):201–7.
Arora S, Aggarwal R, Sirimanna P, Moran A, Grantcharov T, Kneebone R. Mental practice enhances surgical technical skills: a randomized controlled study. Ann Surg. 2011;253(2):265–70.
Arora S, Aggarwal R, Moran A, Sirimanna P, Crochet P, Darzi A, Kneebone R, Sevdalis N. Mental practice: effective stress management training for novice surgeons. J Am Coll of Surg. 2011;212(2):225–33.
Komesu Y, Urwitz-Lane R, Ozel B, Lukban J, Kahn M, Muir T. Does mental imagery prior to cystoscopy make a difference? A randomized controlled trial. Am J Obstet and Gynecol. 2009;201(2):218–e1.
Lorello GR, Hicks CM, Ahmed SA, Unger Z, Chandra D, Hayter MA. Mental practice: a simple tool to enhance team-based trauma resuscitation. CJEM. 2016;18(02):136–42.
Immenroth M, Bürger T, Brenner J, Nagelschmidt M, Troidl H, Eberspächer H. Mental training in surgical education: a randomized controlled trial. Ann Surg. 2007;245(3):385–91.
Patel SR, Gohel MS, Hamady M, Albayati MA, Riga CV, Cheshire NJ. Reducing errors in combined open/endovascular arterial procedures: influence of a structured mental rehearsal before the endovascular phase. J Endovasc Ther. 2012;19(3):383–9.
Stefanidis D, Anton NE, McRary G, Howley LD, Pimentel M, Davis C, Yurco AM, Sevdalis N, Brown C. Implementation results of a novel comprehensive mental skills curriculum during simulator training. Am J Surg. 2017;213(2):353–61.
Anton NE, Howley LD, Pimentel M, Davis CK, Brown C, Stefanidis D. Effectiveness of a mental skills curriculum to reduce novices’ stress. J Surg Res. 2016;206(1):199–205.
Stefanidis D, Anton NE, Howley LD, Bean E, Yurco A, Pimentel ME, Davis CK. Effectiveness of a comprehensive mental skills curriculum in enhancing surgical performance: results of a randomized controlled trial. Am J Surg. 2017;213(2):318–24.
Richardson A. Mental imagery. London: Routledge & Kegan Paul; 1969.
Murphy SM. Imagery interventions in sport. Med Sci Sports Exerc. 1994;26:486–94.
Kern DE, Thomas PA, Hughes MT. Curriculum development for medical education: a six-step approach. 2nd ed. Baltimore: Johns Hopkins University Press; 2009.
Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52(1):397–422.
Salles A, Cohen GL, Mueller CM. The relationship between grit and resident Well-being. The Am J Surg. 2014;207(2):251–4.
Zwack J, Schweitzer J. If every fifth physician is affected by burnout, what about the other four? Resilience strategies of experienced physicians. Acad Med. 2013;88(3):382–9.
Sood A, Prasad K, Schroeder D, Varkey P. Stress management and resilience training among department of medicine faculty: a pilot randomized clinical trial. J Gen Internal Med. 2011;26(8):858–61.
Krasner MS, Epstein RM, Beckman H, Suchman AL, Chapman B, Mooney CJ, Quill TE. Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA. 2009;302(12):1284–93.
Shapiro SL, Astin JA, Bishop SR, Cordova M. Mindfulness-based stress reduction for health care professionals: results from a randomized trial. Int J Stress Managm. 2005;12(2):164.
Lenchus JD. The end of the “see one, do one, teach one” era: the next generation of invasive bedside procedural instruction. J Am Osteopath Assoc. 2010;110:340–6.
Alfa-Wali M. Surgical leadership through coaching. J Surg Educ. 2013;70(5):680–2.
Bonrath EM, Dedy NJ, Gordon LE, Grantcharov TP. Comprehensive surgical coaching enhances surgical skill in the operating room. Ann Surg. 2015;262(2):205–12.
Min H, Morales DR, Orgill D, Smink DS. Systematic review of coaching to enhance surgeons’ operative performance. Surgery. 2015;158(5):1168–91.
Mutabdzic D, Mylopoulos M, Murnaghan ML, Patel P, Zilbert N, Seemann N, et al. Coaching surgeons: is culture limiting our ability to improve? Ann Surg. 2015;262(2):213–6.
Stefanidis D, Anderson-Montoya B, Higgins RV, Pimentel ME, Rowland P, Scarborough MO, Higgins D. Developing a coaching mechanism for practicing surgeons. Surgery. 2016;160(3):536–45.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Anton, N.E., Bean, E. (2019). Performance Optimization. In: Stefanidis, D., Korndorffer Jr., J., Sweet, R. (eds) Comprehensive Healthcare Simulation: Surgery and Surgical Subspecialties. Comprehensive Healthcare Simulation. Springer, Cham. https://doi.org/10.1007/978-3-319-98276-2_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-98276-2_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-98275-5
Online ISBN: 978-3-319-98276-2
eBook Packages: MedicineMedicine (R0)