
Abstract
The major role of the vestibulo-ocular reflex (VOR) is to stabilize the eyes for clear vision during movement in daily life. Periodic head movements during normal life activities move the head at fundamental frequencies of 2–4 Hz, with harmonics extending above these frequencies. The other ocular control systems are relatively insensitive above 2 Hz and therefore the VOR functions as the primary control system for visual stabilization during locomotion. Traditional testing using caloric stimulation of the lateral semicircular canal is limited to a very low-frequency response, and only one canal of the labyrinth is tested. Traditional rotational chair systems test only the lateral semicircular canal and at relatively low-frequency levels. At a constant rotational velocity, the semicircular canals are not stimulated, only with acceleration or deceleration. This chapter is to cover active and passive head movements to test the VOR from 2 to 6 Hz, using the autorotational test and the video head impulse test (vHIT) that simulates more authentic daily VOR challenges.
Eye movements resulting from low-frequency rotational testing are composed of slow and fast phases of nystagmus. The slow phase is directed by VOR, and the fast phase is a result of compensation by the paramedian pontine reticular formation which causes the saccadic eye movements. Linear analysis of the VOR cumulative eye position results in relatively accurate gain and phase because of the apparent linearity of the system. Phase and gain change abnormalities are the basis of the testing paradigm.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
The vestibulo-ocular reflex (VOR) is a vestigial reflex that serves to maintain visual focus on a target during head movement. The reflex arc includes the end organs of balance – the three paired semicircular canals and two paired otolith organs – the vestibular and oculomotor nuclei, and extraocular muscles; it is also under modulatory control by the cerebellum [1, 2]. VOR can be suppressed when desired, such as when reading in a moving vehicle, and it is most active with high-frequency head movements greater than 2 Hz. In fact, at slower frequencies, eye movements are under the control of a variety of reflexes, including optokinetics, smooth pursuit, and the cervico-ocular reflex. Therefore, high-frequency head movements specifically test VOR and, by proxy, the peripheral vestibular system [3].
Head movement stimulates the semicircular canal (or canals) ipsilateral and in the plane of the head movement; simultaneously, the contralateral semicircular canals are inhibited. First, this afferent signal travels to the ipsilateral vestibular nucleus. The signal then decussates, traveling to and stimulating the contralateral abducens nucleus. Internuclear neurons travel via the medial longitudinal fasciculus to the ipsilateral oculomotor nucleus. The sum of these signals is a slow eye movement opposite the head movement. For example, head movement to the left would result in an excitatory impulse to the right abducens nucleus and left oculomotor nucleus, creating contraction of the right lateral rectus and left medial rectus with resultant movement of both eyes to the right. The eyes remain focused on their target, and the visual scene is not disturbed by head motion [3]. The particular set of semicircular canals and otolithic end organs stimulated by a head motion is determined by the location of the head relative to gravity, the rotation in x, y, and z axes, and the amount of pitch (rotation around an axis through the external auditory canals), yaw (rotation around a cranial caudal axis), and roll (rotation around an anterior to posterior axis) [2, 4]. Results of VOR testing are often expressed in terms of gain – a numeric value derived from the ratio of the area under of the curve of eye velocity and the area under the curve of head velocity [3]. Gain of 1 suggests perfect compensation of eye movements with head movement. When VOR fails, corrective saccades re-center the point of interest on the gaze; they are typically contralateral to the direction of stimulation. The movement of the target in the visual scene, known as retinal slip, targets visual re-fixation on the target [5]. Overt saccades are easily visible by an observer testing the vestibular system and are the basis of bedside head impulse testing (see below) [6]. In contrast, covert saccades are not readily detectable by a clinician and require objective, precise measurement of eye movement and head movement [7].
Described by Barany in his work on the vestibular system that ultimately won the Nobel Prize in 1914, caloric testing was long the gold standard test of peripheral vestibular function [8]. However, caloric testing is generally a specific testing of the horizontal semicircular canals and, by extension, the superior vestibular nerve. Therefore, interest grew in provocative tests that evaluate the VOR and, by extension, the function of any of the three paired semicircular canals and otolith end organs. In general, these provocative tests can be divided into whole body or head-only impulse testing. Whole body impulse testing in the form of rotary chair gained popularity in the 1980s as a way to evaluate the VOR. However, rotary chair testing is limited by the frequency a rotary chair can produce and the velocity patients can tolerate. Frequencies more than 1 Hz are technically infeasible, which confounds results given the non-vestibular reflexes that dominate eye movements at these frequencies [9]. In contrast, the head alone can be rotated rapidly to reach VOR-specific frequencies of greater than 2 Hz; this is referred to as head-only impulse testing. Head-only impulse testing can be classified into active and passive testing. In active testing, patients are in control of head motion; in passive testing, the examiner controls the patient’s head movements.
Halmagyi and Curthoys first described passive head impulse testing in 1988. In this testing paradigm, the head is rapidly turned by the examiner 15–20° from neutral in one direction, while the patient is instructed to fix their gaze on a central midpoint. The patient is observed for overt catch-up saccades, suggestive of vestibular dysfunction ipsilateral to the direction of the head turn [6]. If the vestibular end organs in the plane of the head thrust on the ipsilateral side are hypofunctioning, the VOR will fail and eyes will drift with head movement; therefore, a corrective saccade to the contralateral side will be necessary to re-center the visual scene. Scleral search coils have been used with this paradigm to provide objective data about eye movements; however, comfort and expense make this technique of limited clinical utility [3]. While bedside head thrust testing is appealing for its simplicity, its sensitivity is too low to function independently as a test of peripheral vestibular function; it is, however, highly specific [10]. The position of the head during head thrust can be altered to more specifically test particular semicircular canals or otolithic end organs. Clinical evaluation of catch-up saccades has provided quick, simple bedside testing of peripheral vestibular function and can provide valuable evaluation about the semicircular canals and otolithic end organs [11].
In active head thrust or autorotational testing, subjects rotate their heads while fixing their gaze on a central target. They are directed to rapidly rotate their heads in response to auditory stimulation in the form of clicks or beeps; these sound cues result in headshake in the range of 2–6 Hz. Electrooculography with electrodes at the lateral canthi bilaterally is used to obtain objective measurements of eye movement [12]. The gain measures in autorotational testing have proven valuable in a number of clinical scenarios. The use of this testing has revealed significant decrease in gain with cisplatin (vestibulotoxic chemotherapy) [13], increased gain in Meniere’s disease [14], and decreased gain in acoustic neuroma that positively correlates in many cases to the size of the tumor [15]. Similarly, autorotational testing has been shown to pick up peripheral vestibular pathology that caloric testing may miss when compared head to head [16]. However, volitional head movements can still be confounded by secondary reflexes, such as the cervico-ocular reflex, even at high frequencies [2]. Therefore, autorotational testing has fallen out of favor.
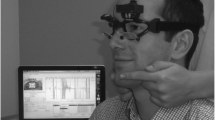
Passive head-only impulse testing has taken a modern form in video head impulse testing (vHIT). vHIT testing involves high-impulse head movements combined with video software that measures pupil velocity. For patients, it is a relatively simple and noninvasive test; instead of electrooculography or scleral coils, a set of goggles that precisely track pupil movements are worn (Fig. 5.1). Data suggests that this tracking technology is equivalent to the precision seen with scleral search coils while being more comfortable and cost-effective [17]. Two sets of data can be collected with vHIT technology. In head impulse testing or HIMP testing, the patient fixes their gaze on a set target, while an examiner performs head thrust maneuvers. Eye and head velocity, along with overt and covert catch-up saccades, are recorded. Secondary data can be obtained with suppression head impulse or SHIMP testing. In this paradigm, the stimulus of rapid, passive, unpredictable head turns is unchanged; however, the visual target moves with the patient’s head. In contrast to HIMP testing, patients with normal vestibular function make the catch-up saccade as they overcome VOR to fix on the visual target [18]. In contrast, patients with vestibular dysfunction are able to track the moving target freely with rapid head thrust. SHIMP testing eliminates the need to monitor for overt saccades in patients with peripheral vestibular pathology, with easy interpretation of results [3, 19]. As with bedside head thrust testing, the position of the head during the examination can be manipulated to provide information more specific to certain portion of the peripheral vestibular system. These data sets are complementary and can provide significant information for the examiner about the function of the peripheral vestibular system.

The testing set up for video head impulse test. At left, neutral head position with video goggles in place. Right: after thrust 15–20° lateral, patient continues to fix their eyes on a midline target
Some authors have suggested vHIT may replace caloric testing as the gold standard screen for peripheral vestibular system function, and it has shown significant promise (Figs. 5.2 and 5.3). vHIT has shown value in a number of clinical scenarios. In acoustic neuroma, vHIT shows ipsilesional decreased gain and presence of catch-up saccades. Similarly, decreases in gain have been shown to positively correlate with tumor size [20]. In acute vestibular neuritis, vHIT both can show unilateral weakness in terms of ipsilesional reduced gain and presence of catch-up saccades and improvement in ipsilesional gain that correlates with clinical recovery [21] (Fig. 5.4). In Meniere’s disease, outside of active vertigo, vHIT testing can be variable and may be normal or gain may be decreased [22]. In Meniere’s disease, significant decrease in vHIT gain after ablative intratympanic gentamicin injection has been shown to correlate with symptom control [23]. Additionally, vHIT provides two complementary forms of data in calculations of gain and presence of saccades, and the presence of catch-up saccades in the presence of normal calculated gain may still be of significant clinical importance in some scenarios [24, 25]. However, McCaslin et al. found that mild unilateral peripheral weakness (<40% UW) detectable on caloric testing may be missed with measurement of vHIT gain [26]. Others have found that caloric testing is more sensitive than vHIT in detecting unilateral weakness associated with acoustic neuroma [27]. vHIT continues to grow in clinical use and is a valuable complementary test in the peripheral vestibular test battery, but further research is needed to determine its utility in various clinical scenarios.

Normal vHIT tracing. Blue represents head thrust to the left (in this case, in the plane of the lateral semicircular canal); orange represents head thrust to the right. The green tracing is calculated vestibulo-ocular reflex activity during head thrust. In normal patients, there is excellent compensation for head thrust by the VOR

vHIT in bilateral vestibular loss. Blue represents head thrust to the left; orange represents head thrust to the right. The green tracing is calculated vestibulo-ocular reflex activity during head thrust. Red represents compensatory saccades. Head thrust in either direction in the planes of all semicircular canals shows decreased VOR activity compared to head thrust with catch-up saccades noted. Note that for testing of the anterior and posterior canals, the contralateral thrust is to the appropriate LARP or RALP pairing. Top panel, lateral canal testing; middle panel, LARP testing; bottom panel, RALP testing

vHIT in acute left superior vestibular neuritis. Blue represents head thrust to the left; orange represents head thrust to the right. The green tracing is calculated vestibulo-ocular reflex activity during head thrust. Red represents compensatory saccades. On head thrust to the ipsilesional side for the lateral and anterior semicircular canals, VOR activity is decreased compared to head thrust and catch-up saccades are noted (top and middle panels). vHIT tracings, in contrast, for the ipsilesional posterior semicircular canal are expectedly normal (bottom panel). Note that for testing of the anterior and posterior canals, the contralateral thrust is to the appropriate LARP or RALP pairing
References
Beh SC, Frohman TC, Frohman EM. Cerebellar control of eye movements. J Neuroophthalmol. 2017;37(1):87–98. https://doi.org/10.1097/WNO.0000000000000456.
Furman JM. Rotational testing. Handb Clin Neurol. 2016;137:177–86. https://doi.org/10.1016/B978-0-444-63437-5.00012-1.
Halmagyi GM, Chen L, MacDougall HG, Weber KP, McGarvie LA, Curthoys IS. The video head impulse test. Front Neurol. 2017;8:258. https://doi.org/10.3389/fneur.2017.00258.
Kheradmand A, Zee DS. The bedside examination of the vestibulo-ocular reflex (VOR): an update. Rev Neurol (Paris). 2012;168(10):710–9. https://doi.org/10.1016/j.neurol.2012.07.011.
Schubert MC, Hall CD, Das V, Tusa RJ, Herdman SJ. Oculomotor strategies and their effect on reducing gaze position error. Otol Neurotol. 2010;31(2):228–31. https://doi.org/10.1097/MAO.0b013e3181c2dbae.
Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol. 1988;45(7):737–9.
Weber KP, Aw ST, Todd MJ, McGarvie LA, Curthoys IS, Halmagyi GM. Head impulse test in unilateral vestibular loss: vestibulo-ocular reflex and catch-up saccades. Neurology. 2008;70(6):454–63. https://doi.org/10.1212/01.wnl.0000299117.48935.2e.
Barany R. (1876–1936) – investigator of labyrinthine function. JAMA. 1965;191:132–3.
Jenkins HA, Honrubia V, Baloh RH. Evaluation of multiple-frequency rotatory testing in patients with peripheral labyrinthine weakness. Am J Otolaryngol. 1982;3(3):182–8.
Harvey SA, Wood DJ, Feroah TR. Relationship of the head impulse test and head-shake nystagmus in reference to caloric testing. Am J Otol. 1997;18(2):207–13.
Kessler P, Tomlinson D, Blakeman A, Rutka J, Ranalli P, Wong A. The high-frequency/acceleration head heave test in detecting otolith diseases. Otol Neurotol. 2007;28(7):896–904.
Fineberg R, O’Leary DP, Davis LL. Use of active head movements for computerized vestibular testing. Arch Otolaryngol Head Neck Surg. 1987;113(10):1063–5.
Kitsigianis GA, O’Leary DP, Davis LL. Active head-movement analysis of cisplatin-induced vestibulotoxicity. Otolaryngol Head Neck Surg. 1988;98(1):82–7. https://doi.org/10.1177/019459988809800114.
O’Leary DP, Davis LL. Vestibular autorotation testing of Menière’s disease. Otolaryngol Head Neck Surg. 1990;103(1):66–71. https://doi.org/10.1177/019459989010300110.
O’Leary DP, Davis LL, Maceri DR. Vestibular autorotation test asymmetry analysis of acoustic neuromas. Otolaryngol Head Neck Surg. 1991;104(1):103–9. https://doi.org/10.1177/019459989110400119.
Saadat D, O’Leary DP, Pulec JL, Kitano H. Comparison of vestibular autorotation and caloric testing. Otolaryngol Head Neck Surg. 1995;113(3):215–22. https://doi.org/10.1016/S0194-5998(95)70109-5.
Macdougall HG, McGarvie LA, Halmagyi GM, Curthoys IS, Weber KP. The video Head Impulse Test (vHIT) detects vertical semicircular canal dysfunction. PLoS One. 2013;8(4):e61488. https://doi.org/10.1371/journal.pone.0061488.
Crane BT, Demer JL. Latency of voluntary cancellation of the human vestibulo-ocular reflex during transient yaw rotation. Exp Brain Res. 1999;127(1):67–74.
Shen Q, Magnani C, Sterkers O, et al. Saccadic velocity in the new suppression head impulse test: a new indicator of horizontal vestibular canal paresis and of vestibular compensation. Front Neurol. 2016;7:160. https://doi.org/10.3389/fneur.2016.00160.
Tranter-Entwistle I, Dawes P, Darlington CL, Smith PF, Cutfield N. Video head impulse in comparison to caloric testing in unilateral vestibular schwannoma. Acta Otolaryngol (Stockh). 2016;136(11):1110–4. https://doi.org/10.1080/00016489.2016.1185540.
Palla A, Straumann D. Recovery of the high-acceleration vestibulo-ocular reflex after vestibular neuritis. J Assoc Res Otolaryngol. 2004;5(4):427–35.
Cordero-Yanza JA, Arrieta Vázquez EV, Hernaiz Leonardo JC, Mancera Sánchez J, Hernández Palestina MS, Pérez-Fernández N. Comparative study between the caloric vestibular and the video-head impulse tests in unilateral Menière’s disease. Acta Otolaryngol (Stockh). 2017;137(11):1178–82. https://doi.org/10.1080/00016489.2017.1354395.
Nguyen KD, Minor LB, Della Santina CC, Carey JP. Vestibular function and vertigo control after intratympanic gentamicin for Ménière’s disease. Audiol Neurootol. 2009;14(6):361–72. https://doi.org/10.1159/000241893.
Perez-Fernandez N, Eza-Nuñez P. Normal gain of VOR with refixation saccades in patients with unilateral vestibulopathy. J Int Adv Otol. 2015;11(2):133–7. https://doi.org/10.5152/iao.2015.1087.
Pérez-Fernández N, Gallegos-Constantino V, Barona-Lleo L, Manrique-Huarte R. Clinical and video-assisted examination of the vestibulo-ocular reflex: a comparative study. Acta Otorrinolaringol Esp. 2012;63(6):429–35. https://doi.org/10.1016/j.otorri.2012.04.010.
McCaslin DL, Jacobson GP, Bennett ML, Gruenwald JM, Green AP. Predictive properties of the video head impulse test: measures of caloric symmetry and self-report dizziness handicap. Ear Hear. 2014;35(5):e185–91. https://doi.org/10.1097/AUD.0000000000000047.
Blödow A, Blödow J, Bloching MB, Helbig R, Walther LE. Horizontal VOR function shows frequency dynamics in vestibular schwannoma. Eur Arch Otorhinolaryngol. 2015;272(9):2143–8. https://doi.org/10.1007/s00405-014-3042-2.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Walsh, E.M., Bojrab, D.I. (2019). The Vestibulo-ocular Reflex and Head Impulse Testing. In: Babu, S., Schutt, C., Bojrab, D. (eds) Diagnosis and Treatment of Vestibular Disorders. Springer, Cham. https://doi.org/10.1007/978-3-319-97858-1_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-97858-1_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-97857-4
Online ISBN: 978-3-319-97858-1
eBook Packages: MedicineMedicine (R0)