
Abstract
This chapter aims at describing dyscalculia, based on definitions from the WHO and DSM, and how behavioral experts can examine whether a low-performing student in math has dyscalculia or not. Based on a protocol for dyscalculia, three criteria, which must be met in order to diagnose dyscalculia, will be described. Five steps of conducting process research will be described in terms of the learnability of students. Because prevention is more promising than remediation, early education will be highlighted as an important moment to start helping young children in mastering math prerequisites, so they can start grade 1 without any big delay.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
Roughly a quarter of the population worldwide experience difficulties with mathematics (Dowker, 2017). This can have major consequences for their further educational career and for their ability to live independently in society. Math problems that are very serious and persistent in nature may indicate developmental dyscalculia. Although there is inconsistent use of terminology in the literature, researchers agree that dyscalculia refers to the existence of a severe disability in learning mathematics. Ruijssenaars, Van Luit, and Van Lieshout (2016, p. 28) defined dyscalculia as a disorder characterized by persistent problems with learning and fluency and/or accurate recall and/or application of mathematical knowledge (facts and understanding). The prevalence of dyscalculia is estimated to be between 2% and 3% in students in the Netherlands (Ruijssenaars et al., 2016). Percentages are higher in international research (3–8%), depending on how researchers define a mathematical disorder or dyscalculia (Desoete, Roeyers, & De Clercq, 2004; Dowker, 2005; Shalev, Manor, & Gross-Tsur, 2005). The disability can be highly selective, affecting learners with normal intelligence (e.g., Landerl, Bevan, & Butterworth, 2004), although it also co-occurs with other developmental disorders, including reading disorders (Ackerman & Dykman, 1995; Gross-Tsur, Manor, & Shalev, 1996) and attention-deficit hyperactivity disorder (ADHD; Monuteaux, Faraone, Herzig, Navsaria, & Biederman, 2005).
The World Health Organization (WHO) initiated the “International Classification of Diseases” (ICD). ICD is the foundation for the identification of health trends and statistics globally and the international standard for reporting diseases and health conditions. It is the diagnostic classification standard for all clinical and research purposes. In the ICD-10 (version 2016), dyscalculia is mentioned as “specific disorder of arithmetical skills” (code: F 81.2). This classification involves a specific impairment in arithmetical skills that is not solely explicable on the basis of general mental retardation or of inadequate schooling. The deficit concerns mastery of basic computational skills of addition, subtraction, multiplication, and division rather than of the more abstract mathematical skills involved in algebra, trigonometry, geometry, or calculus.
Another very common used classification system worldwide is the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2000). The now-obsolete diagnostic criteria for mathematics disorder (code: 315.1) were:
-
A.
Mathematical ability, as measured by individually administered standardized tests, is substantially below than expected given the person’s chronological age, measured intelligence, and age-appropriate education.
-
B.
The disturbance in Criterion A significantly interferes with academic achievement or activities of daily living that require mathematical ability.
-
C.
If a sensory deficit is present, the difficulties in mathematical ability are in excess of those usually associated with it.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) takes a different approach to learning disorders than previous editions by broadening the category, in order to increase diagnostic accuracy and effectively target care. Specific learning disorder is now a single, overall diagnosis, incorporating deficits that impact academic achievement. The criteria describe shortcomings in general academic skills and provide detailed specifiers for the areas of reading, mathematics, and written expression. Diagnosis requires persistent difficulties in reading, writing, arithmetic, or mathematical reasoning skills during the formal years of schooling. Symptoms may include inaccurate or slow and effortful reading, poor written expression that lacks clarity, difficulties remembering number facts, or inaccurate mathematical reasoning. Current academic skills must be well below the average range of scores in culturally and linguistically appropriate tests of reading, writing, or mathematics. The individual’s difficulties must not be better explained by developmental, neurological, sensory (vision or hearing), or motor disorders and must significantly interfere with academic achievement, occupational performance, or activities of daily living.
Despite the changes from DSM-IV-TR to DSM-5, it remains necessary to perform extensive diagnostic testing to establish whether dyscalculia is present. Since recent research has increasingly recognized the heterogeneity of dyscalculia by differentiating between underlying cognitive deficits (Kaufmann et al. 2013; Rubinsten & Henik, 2009; Skagerlund & Träff, 2016), identification of dyscalculia does not on its own provide enough information about the educational needs of an individual student with math problems. The Dutch protocol “Dyscalculia: Diagnostics for Behavioural Professionals” (DDBP protocol; Van Luit, Bloemert, Ganzinga, & Mönch, 2014) describes how behavioral experts can examine whether a student has dyscalculia or a severe difficulty in math.
The DDBP protocol deals with three criteria that must be met in order to diagnose dyscalculia (Van Luit, 2012; Van Luit et al., 2014):
-
Criterion 1: To determine the presence and severity of the math problem
-
Criterion 2: To determine the math problem related to the personal abilities
-
Criterion 3: To determine obstinacy of the mathematical problem
In the protocol is also mentioned that in many research a fourth criterion is included: the difficulties already exist before the age of 7 years. For most children this is true, but (high) gifted children are mostly recognized for dyscalculia at a later age.
Differential Diagnosis of Dyscalculia
Kucian and Von Aster (2015) mention that dyscalculia is assumed to be a very heterogeneous disorder putting special challenges to define homogeneous diagnostic criteria. Dyscalculia is a disorder that can be characterized through perseverant problems in the process of learning and easy and/or accurate applying of math knowledge (facts/agreements). The DDBP protocol (Van Luit et al., 2014) contains guidelines and suggestions about the variables that can be investigated, and the methods used, during a diagnostic examination of dyscalculia. Due to its structured and comprehensive nature, the DDBP protocol has now been systematically implemented in most social care settings in education in the Netherlands and Flanders (Belgium). The DDBP protocol deals with three criteria that must be met in order to diagnose dyscalculia (Van Luit et al., 2014).
Criterion 1: To Determine the Presence and Severity of the Math Problem
The criterion of severity is determined by deficiencies in both automated and substantive math skills of the diverse domains.
Criterion of severity:
-
1a.
There is a significant delay in automated math skills as compared to peers and/or fellow children.
-
2a.
There is a significant delay in mastering the substantive math skills of the domains.
To meet criteria 1a and 1b, there has to be at the end of primary school (sixth grade) a delay of at least 2 years on a standard (national) math test. For such a test, this would mean that a student at the end of sixth grade should perform not higher than moderate at a test that is adequate for children at the end of fourth grade. Dyscalculia is rarely diagnosed before the end of third grade. The delay has to be at least 1 year at that moment to meet this criterion. For the diagnosis it is important that math education was given at an adequate level.
Dyscalculia can also be diagnosed in children in secondary school, when there is a delay of at least 2 years in their level of math skills compared to children at the end of primary school. In secondary school, students with dyscalculia also perform weak in, for example, economics, geography, and physics.
To determine criterion 1a, an automation/memorization test is necessary. To determine criterion 1b and clarify the extent of the math delay, the therapist has to conduct a process research on the math level of the student. Process research produces more detailed information than standard tests. The therapist can see what the child can and cannot do, furthermore determining the extent of the delay. The therapist can determine the quality, stability, flexibility, and agility of the knowledge and skills.
Process research can be conducted with problems adopted from a regular math test that is adequate for the skill level of the student. To conduct process research, it is important to start at an appropriate level, not too difficult nor too easy. To determine on which specific level can be started, the therapist needs information from the teacher about the exact math level of the student.
Process research has a twofold goal: examining the way in which a student creates an answer and determining in detail the achievement level on the different subdomains. In process research, often prototypical tasks are used to test hypotheses regarding the nature of the problem of the student. In process research the focus is determining the math delay (or deviance of the norm) in terms of math goals/end terms and the underlying shortcomings in procedures and strategies (including declarative knowledge). The four steps the therapist follows to adjudicate the severity of the math problem are (see for a concrete example of step d the Appendix):
-
(a)
Observing open actions (use of blocks), hidden actions (secretly counting on fingers or with the use of looking to a big corral necklace in the classroom), and task approach during math exams (orientating or immediately starting)
-
(b)
Questioning the strategy chosen by the student to resolve the math task (thinking out loud regarding the problem solution, questioning the strategy chosen)
-
(c)
Variation in different math tasks which are in terms of questioning and level near the most difficult correctly and the easiest wrongly dissolved tasks
-
(d)
Providing help examining the degree in which the student needs which type of help, by means of continuing “the five phases of math help” (see for an example the Appendix). The help is provided at the most difficult tasks (step 3) that students just couldn’t solve themselves in each domain. The five phases of help are:
-
1.
Offering more structure
-
2.
Decrease of complexity
-
3.
Giving verbal help
-
4.
Giving material help
-
5.
Modelling of step d (demonstrate, associate, mimic)
-
1.
During process research different levels of tasks will be varied, and no tests will be fully completed. As a consequence, it is not always possible to make precise pronunciations on the exact extent of the student’s math delay. This means that the degree of severity is an estimation. For example, a student who cannot count with steps of 25 (matching the math skill level of third or fourth grade), but can count with steps of 5 (matching the math skill level of second grade), therefore a pronunciation of the level of the student regarding this math aspect is possible. The inconsistency in what the student can and cannot do produces important information regarding the ultimate support and treatment needed. It is advisable that the focus of help provided after the diagnostic research is on the specific subjects the student does not master sufficiently. The information provided by school produces supporting information regarding the student’s level. Examining the way the student failed or succeeded to solve tasks is possible using the provided test sheets, including scratch paper.
Criterion 2: To Determine the Math Problem Related to the Personal Abilities
This means: There is a significant delay with respect to what can be expected from a child, based on his/her individual development. The cognitive level is mostly determined by an intelligence test. Children with dyscalculia can have an under- or above-average intelligence level. It is not possible to determine dyscalculia when the student has an intelligence score of 70 or below, because in that case, the mathematical skills are expected related to the personal abilities. In case the total IQ score is between 71 and 85, diagnosing dyscalculia has to be done with caution. Mathematics requires a complex skillset, which relies on higher cognitive functions. Therefore it is not realistic to expect from children with an IQ score between 71 and 85 to develop and achieve the same math level as their peers with an average IQ score. This means that, to determine dyscalculia in these children, the math problems should not only be explicable by a lower intelligence score. There should, for example, also be a lag of speed in problem-solving and a deficiency in insight. Note that there is no scientific evidence for ascripting a declaration of dyscalculia to a person with an IQ score between 71 and 85. In that case the lag in mathematical skills needs to be larger (at the end of grade six at least 3 years) than the lag of mathematical skills of a person with an average intelligence score (at the end of grade six at least 2 years).
From an analysis of the student’s file, there should appear a specific failure in mathematics. In case the performance in other learning areas is also low, this indicates a general learning problem or a broad learning disorder. Low performances on tests in reading and spelling can also indicate dyslexia as a comorbid disorder. In the latter case, a protocol of diagnostics of dyslexia must be followed to determine whether the student (also) has dyslexia. Dyscalculia can also be diagnosed in children with dyslexia when their mathematical performances are not significantly lower than their (limited) performances on tests for reading and spelling. In that case dyscalculia is diagnosed when there is a discrepancy between the mathematical performances and the intelligence, and it is clear that the mathematical problems are not a consequence of reading problems. Whether the mathematical problems are a consequence of reading problems can be investigated during process research.
Mathematical problems of gifted children often get noticed later than usual. In the beginning of their school career, these children often profit from their good memory which enables them to conceal their lags of mathematical skills by applying fast solving strategies. In the course of primary school, this strategy is not enough anymore and their lag in mathematical skills reveals itself. It is important not to withhold these children a declaration of dyscalculia, because of their sufficient performances in the first math tests at the start of secondary school.
In case a student has a comorbid disorder (e.g., ADHD), his or her math performances have to be considerably lower than usually expected of children with the disorder (see Kuhn, 2015). For other comorbid disorders like dyslexia, autism, and DCD, such lower scores are not necessary.
Criterion 3: To Determine Obstinacy of the Mathematical Problem
This means: There is an obstinate mathematical problem, which is resistant to specialized help. To determine the obstinacy, the third and latter criteria for determining dyscalculia, the structural and specialized help a student received in mathematics is investigated. Leading are the reports of offered help. According to the model of “response-to-instruction,” didactic resistance can only be determined with great certainty, when the conditions on all three levels have been complied (Fuchs & Vaughn, 2012). Dyscalculia cannot be diagnosed if criterion 3 has not been complied. This also applies for children in secondary school. To determine if the criterion of didactic resistance has been met, the available school records (student file) need to be evaluated. In addition a process research is necessary to determine whether a student is able to learn new strategies and reproduce them independently.
As mentioned earlier, adequate instruction and practice can be described on three different levels, according to the model of “response-to-instruction.” In the description is disclosed whether the instruction and practice given by the teacher were adequate. In the description is also disclosed what was concluded based on the evaluation of the individual education program, and in which way during 6 months, at least 1 h per week (individual or in a little group), help of good quality with mathematics has been given by a qualified therapist. The help with mathematics needs to be based on a start measurement, specific and measurable goals have to be set for the mathematical behavior, and the content needs to match the most basic failure. The effectiveness of specialized extra help with mathematics is evaluated, examining the progress during the period of help. The help has been effective when the student’s performance after 6 months on the same test as the start measurement reveals a progress comparable to 4 months of education (see Fig. 38.1). The help in mathematics has not been effective when the progress after 6 months is less than 4 months. This is about determining whether a student barely benefited from help of good quality. In that case didactic resistance (third criterion) is determined. The above raised questions like “How do we determine the start measurement? What content do we choose, and especially how broad should the offer of content be? Will the student receive mathematics instruction together with his class? After half a year, do we administer the same test (which test)?” Logically it is not possible to determine one direction for every individual case. Per student an individual strategy has to be determined.

Performance graph for progress in math (example) (Van Luit et al., 2014). * A score in this area or above: the progress is sufficient; ** A score in this area: the progress is not sufficient; ***E = end, M = middle
For example, a student at the start of third grade starts with half a year specialized help in mathematics. The regular content is too complex for the student. The therapist establishes a baseline at the level of halfway second grade. This means that the student does not get the same content as the rest of the class, but preferably takes math lessons in second grade. The student also could practice mathematics with materials given by the therapist, in its own classroom. What test does the therapist choose to evaluate the effect of the help? Of course the same test suitable for halfway second grade could be administered. This is helpful when determining possible development. If the result is better than expected, then it is also possible to administer a test suitable for children at the end of second grade. However, it is often impossible to tackle every component of mathematics in half a year. In that case the effectiveness of the help can also be determined administering a selective, qualitative test with the components that have been practiced during the period of help.
In case the student has an IQ score between 71 and 85, the didactic resistance is determined when the progress after help of good quality after 6 months is no more than 3 months (which is more or less half of the progress that is expected in children without mathematical problems). Note that to determine didactic resistance, the learning efficiency with regular mathematics instruction is less than 67% (Fig. 38.1). This is also the criterion with adequate math help.
Literature is missing clinically oriented research involving an adequate number of students diagnosed with persistent mathematical learning disabilities (i.e., dyscalculia). The limited amount of research into dyscalculia is largely due to issues of feasibility and generalisability. The difference between mathematics disorder and dyscalculia seems to be the gravity. About the lowest 25% of the children with a mathematics disorder (this is the case for 1 out of 10 children) does have dyscalculia. The other 75% has also severe difficulties, but doesn’t meet all three criteria for dyscalculia fully. What is called as dyscalculia in one study may be conceptualized as a form of mathematical disorder in another study (Kaufmann et al., 2013).
Process Research
In process research help is enhanced gradually to determine whether a student is learnable concerning mathematics. In case of systematic errors (classification), using a number of selected tasks in process research is investigated what the reasons for those errors are and what the starting points are to offer help (indication analysis).
In process research the “five steps of help in mathematics” have been mentioned earlier. Some children find it difficult to deduce the relevant information from the task context. For those children offering more structure can be helpful. In case children have difficulty when it comes to big numbers, the complexity can be reduced to see if that enables a student to solve the task. There are also children who benefit from verbal support while solving the task. This can be helpful to more or less guiding the student from one step to another. Other children benefit from material support, using, for example, cubes or beads (corral necklace), but this is also called visualizing the task. In particular when a student has a weak working memory, in this manner he always has the necessary information at his disposal. When a student has no idea how to solve a task, modelling the strategy could be helpful. In that way a student can learn the most efficient strategy for a specific type of task (Van Luit et al., 2014). In the Appendix several tasks are elaborated (per (sub)component) and the different levels of help are demonstrated. This way insight is given in how the diagnosticians can variate in levels of offering help. The target is, on one hand, to determine how much the student benefits from the offered help and, on the other hand, to determine explanations for the difficulties the student has with mathematics and what his or her strengths are. It is important to get an insight in what level of help is adequate for the student. By variating the levels of help, it is possible to investigate what is and what is not helpful for the student (Van Luit et al., 2014).
Learnability
The process research is ideal to investigate the learnability of a student. Preferably a process research takes place two times in a diagnostic investigation with 1 or 2 weeks in between. To clarify the learnability, it’s advisable to look for the zone of proximal development. This concept concerns investigating the level of mathematics at which an individual student can solve tasks independently and how much and of what intensity a student needs help when the complexity of tasks is slightly enhanced. By offering help (using the five phases of help) a few proceedings can be practiced with the student. At the second research moment could be checked in which quantity the student has remembered the taught proceeding and is able to reproduce it. The ease with which the student can reproduce the strategies after 1 or 2 weeks with similar tasks is an indication for learnability. We realize that it is hard to enforce during practice, but we strongly advice to proceed. For some children the taught strategies appear to be unfamiliar, even when the strategies have been practiced intensively. In that case their learnability appears to be small. Other children are capable of reproducing the taught and practiced strategies with similar tasks, which indicates at least some learnability.
Math Problems in Early Education
Children learn many mathematical skills already before formal mathematics instruction starts at primary school. These early numeracy skills, especially counting skills, have been found good predictors for later mathematics performance at first, second, and third grades but are even predictors for math knowledge in secondary school (Siegler, 2009). Therefore in this chapter, there will be also attention for this part of (difficulties in) math education. In addition, in younger children, the tendency to spontaneously focus on numerosities was found a good predictor for counting skills in preschool age. The main goal to highlight early math here is because prevention is more promising than remediation.
As a result far out, most 6-year-old children (at this age most children in Western Europe are going from kindergarten into grade 1 in primary school) have quite well developed early numeracy (primary understanding of amounts and acoustic, asynchronic, synchronic, resultative, and shortened counting; see Aunio, Heiskari, Van Luit, & Vuorio, 2015), including the ability to make relational statements about numerical and nonnumerical quantity situations and to operate with number word sequence for whole numbers. In the first grade of primary school, children are expected to learn the basic skills of addition and subtraction. The first graders usually operate with numbers between 0 and 100, although the emphasis in addition and subtraction is with numbers 0–20.
In talks with parents and teachers from children who have mathematical difficulties or even dyscalculia diagnosed on a later age (from 9 years on), they indicate that the child with a math difficulty had already problems, especially with resultative and shortened counting during kindergarten (Dowker, 2017). Mostly when children are 9 or 10 years old, they still have difficulties with these stages of counting and they often still count on their fingers. For example, when they have to solve 5 + 3, they count their fingers starting with a dump: 1 and then 2, 3, 4, 5, and further on with the other hand 6, 7, 8. Mostly, they are not able to see five as a whole to count further on. Finger counting and not using 5 and 10 as wholes is characteristically for children who will meet difficulties in math during their school career. Using a lot of time through counting is a sign for difficulties in math (Tobia, Rinaldi, & Marzocchi, 2018). It is not possible to prevent dyscalculia; nevertheless it is possible to observe weak math performance in an early stage of the school career of a child. It is very important to help these low-performing children from an early start point (Toll & Van Luit, 2014a).
Most kindergartners develop early numeracy almost automatically, while for a minority of the children (around 20%), this development is less naturally. Research shows the importance of mastering such skills before children move toward formal math in first grade of primary school (Jordan, Glutting, & Ramineni, 2010). Especially for children who find these skills difficult, it is of great importance to support them adequately. Therefore, specific instruction and exercise in preparatory math skills are necessary in young age.
Dowker (2005) points out that more and more indications are being found that, apart from the possibility of early signaling (Van Luit & Van de Rijt, 2009), treating early mathematical learning problems improves further mathematical education (Gersten, Jordan, & Flojo, 2005; Van Luit & Schopman, 2000). Dowker (2005) states that the prevention of these problems during kindergarten forms a main challenge in research for the following decades. Morgan, Farkas, and Wu (2009) highlight that it is very important to trace problems in early numeracy as early as possible to be able to provide the best possible support at that stage, also when they later turn out to have dyscalculia.
Our own research shows that kindergartners greatly benefit from early detection. It’s not just about determining a score, but more importantly identifying specific deficits. Hereby it is possible to help children specifically at areas where they experience problems (Van Luit, 2011). For this purpose effective programs have been developed (Aunio, Hautamäki, & Van Luit, 2005; Toll & Van Luit, 2014b; Van Luit & Schopman, 2000).
Dyscalculia can’t be prevented with it, but potentially weak math children can learn a lot from it, and the necessary help for children with dyscalculia should be started at a young age for the highest chance on school success.
From Problems at a Young Age to Dyscalculia
Incorrect number sense at the preparatory level and problems with elementary arithmetic in first grade increasingly lead to more limitations in the abilities of children to adequately solve mathematical tasks. Therefore, these difficulties manifest in children with dyscalculia at a young age in gaining early numeracy during the first half of primary school. These basic difficulties become observable when kindergartners, for example, have problems with fluently naming small quantities (using structure), counting, and automatizing number symbols (Van Luit, 2011).
One of the most striking characteristics Dowker (2005) identifies for dyscalculia is a weakness in recollecting numeric knowledge from memory (e.g., in a young age – 6 to 8 years – they do not know that five is between four and six or that adding four to three equals seven). This problem can persist through older age. Furthermore, they keep using (sometimes into adulthood) number lines to solve simple math problems (12 + 6 = 12, 13, 14, 15, 16, 17, 18, while they keep track of additional units using their fingers under the table). These two characteristics, although on a more basic level, are also observable in kindergartners. It is not yet possible to diagnose dyscalculia in kindergartners. However, children who turn out to have dyscalculia from third grade and upward were also among the weakest kindergartners concerning early numeracy.
Literature provides multiple explanations for the cause of dyscalculia (Van Luit, 2015): poor planning skills, a strongly limited capability for using and learning to use correct strategies, having no control over their math actions, lacking good short-term memory, an inadequate knowledge of automatized numeracy, limited knowledge in math, little or no self-confidence, having no confidence in self-improvement, lacking faith in personal growth, and not being open to help from others. On top of that, it appears that memorization or even automatization problems (not being able to remember that 7×8 equals 56 quickly), discrimination problems (not being able to understand that the number 3 in 13 is worth less than the number 1), and thinking problems (not using association to quickly solve 19 minus 7 via 9 minus 7) play an important role in having no or strongly challenged math learning abilities (Tobia et al., 2016).
Therefore, dyscalculia is especially concerned with the failure of declarative knowledge: numeric facts and naming numbers, such as a deficiency in fluently naming numeric information like numbers and quantities (Busch, Schmidt, & Grube, 2015; Fuchs et al., 2005; Landerl et al., 2004; Willburger, Fussenegger, Moll, Wood, & Landerl, 2008). This implies that automatization problems are always present with dyscalculia (see Criterion 1). However, some children practice so intensively that they in the end of primary school are able to remember, for example, multiplication tables or all summations up to 10. Unfortunately, this knowledge is not adaptable and remains fragmented. For example, when multiplying they will know that “4×8 = 32”, but they don’t know how to solve “14×8” (not seeing by themselves that “14×8” consist of “10×8” and “4×8”). For children with dyscalculia, this will be true already at a young age. They would not see, for instance, that when four toy cars and one toy car are added up, they can continue counting from five toy cars when they add another one. These children will invariably start counting from the first toy car. A deficiency in declarative knowledge almost never stands alone. It will in turn complicate the establishment of procedural knowledge: understanding solution procedures. For example, using the solution procedure for solving “9×6” by subtracting “1×6” from “10×6” assumes that the facts “10×6 = 60” and “60–6 = 54” are known. It also assumes that the student has insight into the act of multiplication, is able to visualize it, has insight into the connection between different multiplication problems, multiplying and adding, and as in this example, even between multiplying and subtracting. When this insight is present, a child will understand how mathematical facts are related and would not need as much automatized knowledge. Factual and procedural knowledge are therefore strongly related.
To sum up the most important characteristics of children with dyscalculia (see also Dowker, 2005):
-
(a)
Regarding declarative knowledge: automation/memorization deficits, namely, problems remembering the basic combinations and easy and/or accurate recalling of math facts from memory.
-
(b)
Regarding procedural knowledge: problems implementing procedures, namely, progressive schemes, applying terms and concepts needed for applying these plans, and the sequence of these steps in complex algorithms.
-
(c)
Regarding visual-spatial processing: problems with notion and conception of space. Problems placing numbers on a number line, mixing numbers in big digits, and problems with geometry and reading time.
-
(d)
Regarding number knowledge: lack of notion of the number system and insufficient knowledge regarding the position value of numbers (not knowing the value of a unit, a dozen, or the value of numbers in fractions above and under the line).
Conclusion
There is need for accurate diagnostics of dyscalculia (Rubinsten & Henik, 2009). To diagnose dyscalculia, three criteria have to be determined: severity, delay, and didactic resistance. To be able to judge whether these criteria are met, different test instruments, process research, and an evaluation of the school records should be used. In addition the clinical therapist is expected to be able to observe during the research moments. It might appear that a student does not benefit from instruction and practice of new strategies on the first research moment and is not able to independently reproduce the strategies. This is an indication for obstinacy. Furthermore it is important to start in kindergarten when children lag behind in match prerequisites. Prevention and early help show better results over time than remediation on a later moment in their school career. Adequate early math education will not prevent dyscalculia, but might help for a better basis.
References
Ackerman, P. T., & Dykman, R. A. (1995). Reading-disabled students with and without comorbid arithmetic disability. Developmental Neuropsychology, 11, 351–371.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed. text rev ed.). Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Aunio, P., Hautamäki, J., & Van Luit, J. E. H. (2005). Mathematical thinking intervention programmes for preschool children with normal and low number sense. European Journal of Special Needs Education, 20, 131–146.
Aunio, P., Heiskari, P., Van Luit, J. E. H., & Vuorio, J. M. (2015). The development of early numeracy skills in kindergarten in low-, average- and high-performance groups. Journal of Early Childhood Research, 13, 3–16.
Busch, J., Schmidt, C., & Grube, D. (2015). Arithmetic fact retrieval. Are there differences between children with developmental dyscalculia and those with mathematical difficulties? Zeitschrift fűr Psychologie, 223, 110–119.
Desoete, A., Roeyers, H., & De Clercq, A. (2004). Children with mathematics learning disabilities in Belgium. Journal of Learning Disabilities, 37, 50–61.
Dowker, A. (2005). Early identification and intervention for children with mathematics difficulties. Journal of Learning Disabilities, 38, 324–332.
Dowker, A. (2017). Interventions for primary school children with difficulties in mathematics. Advances in Child Development and Behavior. Retrieved from https://doi.org/10.1016/bs.acdb.2017.04.004
Fuchs, L. S., Compton, D. L., Fuchs, D., Paulsen, K., Bryant, J. D., & Hamlett, C. L. (2005). The prevention, identification, and cognitive determinants of math difficulty. Journal of Educational Psychology, 97, 493–513.
Fuchs, L. S., & Vaughn, S. (2012). Responsiveness-to-intervention; a decade later. Journal of Learning Disabilities, 45, 195–203.
Gersten, R., Jordan, N. C., & Flojo, J. R. (2005). Early identification and interventions for children with mathematics difficulties. Journal of Learning Disabilities, 38, 293–304.
Gross-Tsur, V., Manor, O., & Shalev, R. S. (1996). Developmental dyscalculia: Prevalence and demographic features. Developmental Medicine & Child Neurology, 38, 25–33.
ICD-10 (2016). Dyscalculia. Retrieved from: apps.who.int/classifications/icd/en
Jordan, N. C., Glutting, J., & Ramineni, C. (2010). The importance of number sense to mathematics achievement in first and third grades. Learning and Individual Differences, 20, 82–88.
Kaufmann, L., Mazzocco, M. M., Dowker, A., von Aster, M., Göbel, S. M., Grabner, R. H., et al. (2013). Dyscalculia from a developmental and differential perspective. Frontiers in Psychology, 4(516), 1–5.
Kucian, K., & Von Aster, M. (2015). Developmental dyscalculia. European Journal of Pediatrics, 174, 1–13.
Kuhn, J.-T. (2015). Developmental dyscalculia. Neurobiological, cognitive, and developmental perspectives. Zeitschrift fűr Psychologie, 223, 69–82.
Landerl, K., Bevan, A., & Butterworth, B. (2004). Developmental dyscalculia and basic numerical capacities: A study of 8-9-year-old children. Cognition, 93, 99–125.
Monuteaux, M. C., Faraone, S. V., Herzig, K., Navsaria, N., & Biederman, J. (2005). ADHD and dyscalculia: Evidence for independent familial transmission. Journal of Learning Disabilities, 38, 86–93.
Morgan, P. L., Farkas, G., & Wu, Q. (2009). Five-year growth trajectories of kindergarten children with learning difficulties in mathematics. Journal of Learning Disabilities, 42, 306–321.
Rubinsten, O., & Henik, A. (2009). Developmental dyscalculia: Heterogeneity might not mean different mechanisms. Trends in Cognitive Sciences, 13, 92–99.
Ruijssenaars, A. J. J. M., Van Luit, J. E. H., & Van Lieshout, E. C. D. M. (2016). Rekenproblemen en dyscalculie [Arithmetic difficulties and dyscalculia]. Rotterdam, The Netherlands: Lemniscaat.
Shalev, R. S., Manor, O., & Gross-Tsur, V. (2005). Developmental dyscalculia: A prospective six-year follow-up. Developmental Medicine and Child Neurology, 47, 121–125.
Siegler, R. S. (2009). Improving the numerical understanding of children from low-income families. Child Development Perspectives, 3, 118–124.
Skagerlund, K., & Träff, U. (2016). Number processing and heterogeneity of developmental dyscalculia: Subtypes with different cognitive profiles and deficits. Journal of Learning Disabilities, 49, 36–50.
Tobia, V., Rinaldi, L., & Marzocchi, G. M. (2018). Time processing impairments in preschoolers at risk of developing difficulties in mathematics. Developmental Science. Advance online publication. https://doi.org/10.1111/desc.12526
Toll, S. W. M., & Van Luit, J. E. H. (2014a). Effects of remedial numeracy instruction throughout kindergarten starting at different ages: Evidence from an large-scale longitudinal study. Learning and Instruction, 33, 39–49.
Toll, S. W. M., & Van Luit, J. E. H. (2014b). Explaining numeracy development in weak performing kindergartners. Journal of Experimental Child Psychology, 124, 97–111.
Van Luit, J. E. H. (2011). Difficulties with preparatory skills in kindergartners. International Journal of Disability, Development and Education, 58, 89–95.
Van Luit, J. E. H. (2012). Protocol dyscalculie als leidraad voor diagnostiek [Protocol dyscalculia as a guide for diagnostics]. Reken-wiskundeonderwijs: Onderzoek, Ontwikkeling, Praktijk, 31(3), 16–21.
Van Luit, J. E. H. (2015). Good math education in kindergarten cannot prevent dyscalculia. Revista de Psicología y Educación/Journal of Psychology and Education, 10(2), 43–60.
Van Luit, J. E. H., Bloemert, J., Ganzinga, E. G., & Mönch, M. E. (2014). Protocol dyscalculie: Diagnostiek voor gedragsdeskundigen (2nd herziene druk) [Protocol dyscalculia: Diagnostics for clinical therapists (2th ed., text rev.)]. Doetinchem, The Netherlands: Graviant.
Van Luit, J. E. H., & Schopman, E. A. M. (2000). Improving early numeracy of young children with special educational needs. Remedial and Special Education, 21, 27–40.
Van Luit, J. E. H., & Van de Rijt, B. A. M. (2009). Utrechtse getalbegrip toets – Revised [Early numeracy test – Revised]. Doetinchem, The Netherlands: Graviant.
Willburger, E., Fussenegger, B., Moll, K., Wood, G., & Landerl, K. (2008). Naming speed in dyslexia and dyscalculia. Learning and Individual Differences, 18, 224–236.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Appendix
Appendix
The Five Steps of Math Help
Example
Tim saves for a new drum set. He has already saved € 623.
The drum set will cost € 1017. How much money does he need to” have to save more?
-
1.
Offering more structure
Reorganization of the written task
-
Tim has to pay € 1017 for a new drum set.
-
Tim already has € 623.
-
How much does he need?
-
-
2.
Decrease of complexity.
Using less complex numbers
-
Tim has to pay € 500 for a new drum set.
-
Tim already has € 350.
-
How much does he needs?
-
-
3.
Giving verbal help.
Asking questions about the content of the task
-
How much money does Tim have?
-
What is the price for the drum set?
-
Does he have enough money to buy the drum set?
-
How much more money does he need?
-
-
4.
Giving material help.Presenting the task with help of a picture (see Fig. 38.2).
-
As you can see, Tim has € 350.
-
The price of the drum set is € 500.
-
What is the difference between 500 and 350?
-
Which sum is connected with this problem?
-
How much more money does Tim need?
-
What is the answer for this sum?
Fig. 38.2 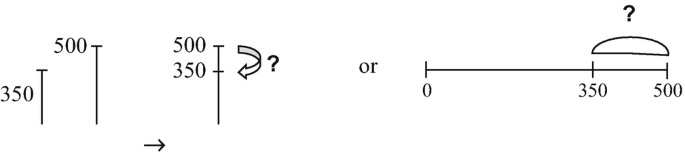
Presenting the task with the help of a picture
-
-
5.
Modelling of step 4.
Demonstration, doing together, and imitation
-
Tim has already € 350, but the drum set is € 500.
-
The drum set is more expensive and therefore Tim needs more money.
-
The question is how much money does he need.
-
This is about the difference between 500 and 350.
-
I make, for example, a picture of the number line. I write down 350 and 500.
-
The problem is solvable by counting from 350 to 500. First I am doing plus 100 that makes 450 and after that another 50 makes 500.
-
The answer is 500 minus 350 makes € 150.
-
Tim needs € 150 more.
-

Take care
If a more easy math task has been done with a good result (in one of the phases of help), more comparable and a little bit more complex tasks can be given after that. For example:
-
The drum set costs € 800. Tim has already € 363 saved. How much does Tim needs more?
or
-
The drum set costs € 1000. Tim has already € 360 saved. How much does Tim needs more?
When this was going well, then you can return to the original task.
Take care
If a more easy math task has been done without a good result (in one of the phases of help), more comparable and a little bit less complex tasks can be given.
For example only using hundreds:
-
The drum set costs € 300 and Tim has already € 200 saved. How much does Tim needs more?
With this more easy task, the same levels of help will be followed.
Rights and permissions
Copyright information
© 2019 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
van Luit, J.E.H. (2019). Diagnostics of Dyscalculia. In: Fritz, A., Haase, V.G., Räsänen, P. (eds) International Handbook of Mathematical Learning Difficulties. Springer, Cham. https://doi.org/10.1007/978-3-319-97148-3_38
Download citation
DOI: https://doi.org/10.1007/978-3-319-97148-3_38
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-97147-6
Online ISBN: 978-3-319-97148-3
eBook Packages: EducationEducation (R0)