
Abstract
Advanced practice nursing was officially recognized in France in 2018. This legislative development marks the culmination of a process that originated in the late 1980s in a project led by the nursing profession to promote the development of clinical nursing expertise. However, this recognition was only possible after lengthy negotiations whose main objective was to adopt a strategy to guarantee the population access to care in a context of increased demand and medical shortages. Now that this legislative step has been taken, the goal is to introduce the first advanced practice nurses in practice environments, to sustain this type of practice and to allow it to develop in order to effectively meet the needs of the population while maintaining this new function in the nursing realm.
This chapter has been written before the 2020 APN ICN guidelines were published and reflects the views of the authors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
France is often better known abroad for the universal health coverage offered to its population than for the nature of the specific contribution nurses make to the health system (World Health Organization 2000).
The profile of the modern nurse, introduced in France in 1878, has been described by Poisson as the “French republican model” (Poisson 1998). Its characteristics were shaped by the political, demographic, social and medical context of the France of the Third Republic, which was marked in particular by a fundamentally anticlerical government (Poisson 1998).
This model breaks with the organization of French healthcare institutions which, until that period, was entrusted to religious congregations such as the Daughters of Charity of Saint Vincent de Paul or the Augustinian Sisters of the Hôtel Dieu in Paris (Leroux-Hugon 1992).
Initially very dependent on the medical profession which had been at the origin of its creation, the nursing group followed a slow process of professionalization. This process began at the end of the First World War under the impetus of an emblematic figure in the French nursing pantheon: Léonie Chaptal (Debout and Magnon 2014).
The apogee of this movement of emancipation and affirmation of the nursing profession in the field of health will be observed especially during the last quarter of the twentieth century.
It will manifest itself in different fields: organization of nursing care, nursing leadership in hospital management, reform of education but also development of clinical nursing. The development of the clinical nursing practice observed in France since the beginning of the 1990s can be considered as one of the factors for asserting the specificity of the nursing perspective and positioning this function in the multi-professional team (Debout 2014). This initiative will be one of the major factors that will foster the emergence of the concept of advanced nursing practice in France. Nurses involved in the development of clinical nursing will strive to ensure that advanced practice is not only understood as a palliative to the medical shortage in a substitution logic but also as an innovative nursing role constituting a new link in the patient care chain.
It will take more than 16 years of discussions, consultations and experimentations before the legislator finally decides to introduce advanced nursing practice in France at a time when the supply of care, particularly in the medical field, has continued to deteriorate. The profile of advanced practice nurses introduced in France in 2018 focuses on a specific area of intervention, currently there are four, but this number will probably change in the years to come in order to adapt to the needs of the population and the inadequacies of the healthcare supply. Compared with the international reference frameworks defined by the International Council of Nurses (ICN) Advanced Practice Nurse Network (Schober 2016), the advanced practice nurse as defined in France is very similar to the profile of clinical nurse specialist. In France, the advanced practice nurse certainly has autonomy and the authority to prescribe, or more precisely to renew or adapt a prescription, but his/her autonomy is still very much supervised by the physician who refers the patient to her and is not positioned as a first-line healthcare provider (Debout 2018).
After clarifying a few elements relating to the context of health in France and the characteristics of the nursing profession in this country, the factors that will lead to the introduction into French legislation of advanced practice for nurses during the summer of 2018 will be specified, in particular the development of clinical nursing. The many challenges that remain to be met in the introduction phase of advanced practice nurses will finally be identified, in particular the evaluation of the service provided.
2 Health in France
Before outlining the contribution made by the nursing profession to the supply of care in France and identifying the characteristics of advanced practice nursing, it is appropriate to present the main characteristics of the French health context, focusing on identifying the needs and expectations of the population in this field, but also the organization of the supply of care and the structure of the health professions.
The state of health of the population living in France is generally good. Life expectancy in 2015 was 85 years for women and 78.9 years for men. These figures are constantly rising. Cancers and cardiovascular diseases are the most frequent causes of death (27.6 and 25.1%) in France (Directorate of Research 2017).
However, high-risk health behaviours can be observed in the population, particularly in terms of nutrition and tobacco consumption. Similarly, heavy alcohol consumption among young people is a cause for concern (Research Directorate 2017).
France’s economic situation influences the health status of its population. Significant differences are noted between the well-off social classes and those in a more precarious financial situation; the latter have a combination of risk factors (Direction de la recherche 2017).
In addition, disparities are observed in health between French regions, which impact on the life span of individuals.
2.1 Organization of the Health System and Healthcare Provision in France
The French health system and social security have provided the population with universal health coverage since the end of the Second World War (Tabuteau 2013). The approach adopted for many years favoured curative rather than preventive care (OECD 2017). Highly hospital-centred, the health system has long given primacy to university hospitals. Its governance is now guided by the principles of New Public Management applied to the health sector (Simonet 2014). The provision of care in the community is largely based on the private practice of physicians, nurses and other health professionals. The notion of the healthcare team in the community is therefore fragmented.
Changes in the demographic and epidemiological characteristics of the French population have necessitated a profound reorientation of the healthcare system in recent years. An ambulatory shift has been initiated in order to better meet the health needs of an aging population increasingly affected by non-communicable diseases but also to reduce health expenditures (Debout 2016).
This reform has profoundly transformed healthcare institutions; a hyper-concentration of supply is underway in hospital superstructures (Vigneron 2018). The search for productivity gains is very significant in these hospitals, making environments less and less favourable to the practice of professionals (Brami et al. 2012). The result is high turnover in teams and an increase in the incidence of burnout phenomena (Desailly-Chanson et al. 2016).
2.2 Structure of the Health Professions
The model that structures the health professions in France can be described as old-fashioned. It gives primacy to the physician, who is always placed as first-line provider in the health system.
The other health professions are subject to medical authority and are referred to as “medical auxiliaries” in the Public Health Code. Although some professions, such as nurses or physiotherapists, have an autonomous role since 1978, they are still considered auxiliary professions.
The contribution made by nurses to the system is significant: there are more than 600,000 nurses in France working in a wide variety of environments (DREES 2018). However, there are only three nursing specialties recognized in the Public Health Code (childcare nurse, nurse anaesthetist and operating room nurse). This very small number of nursing specialties is surprising given that hospital care environments are increasingly specialized (Mossé 2018); the notion of versatility is favoured for nurses in order to facilitate human resource management. A large majority of nurses are employed in the public sector (DREES 2018). Most home care nursing care is provided by nurses who practise independently (Bourgueil et al. 2005). The nursing profession obtained a self-regulating body in 2006, the National Nursing Order.
On the other hand, the academization of nursing education started very late. It was not until 2009 that a bachelor’s degree was required to enter the nursing profession. This delay impeded the development of nursing research capacity.
France does not currently have a nursing shortage. However, a prospective study points out that the system will have to increase its nursing workforce by more than 50% by 2040 in order to cope with increasing healthcare needs (DREES 2018).
The current and future challenges that the healthcare system will have to face in order to meet the growing needs of the population will be a major challenge.
3 The Development of Clinical Nursing: The Roots of Advanced Nursing Practice
To fully use the autonomy given to nurse by legislation, it was necessary to offer them additional education enabling them to reflect on their practice and to use theoretical frameworks developed by the nursing discipline. It was the prerequisite to redefine their professional contribution within the multi-professional team and to use their autonomous therapeutic role for the benefit of patients and their relatives. It was also necessary to promote the development of clinical nursing expertise in practice environments.
3.1 The Origins of a Project
The development of the clinical nursing began in the 1980s in response to the changing needs and expectations of the population in terms of health and nursing care but also to the aspirations of nurses.
This project was launched jointly between French-speaking Switzerland and France under the impetus of Rosette Poletti, a Swiss nurse (Debout 2014).
3.2 Shaping a Profile
The targeted profile was influenced by the clinical nurse specialist function that has been established for many years in North America. It directs the activity of this type of nurse, certainly towards patients and their families but also towards healthcare professionals and organizations. The aim is for these nurses to be change agent and to make a significant contribution to continuous quality improvement and risk management. This clinical curriculum represents a new type of career pathway for nurses outside of management or education.
When it was created, the clinical career pathway was conceived as gradual including three levels spread over several years:
-
Level 1: Certified Clinical Nurse
-
Level 2: Clinical nurse specialist (in French the term was translated as “infirmière spécialiste clinique” in France which means “nurse specialist in clinical nursing”) the transformative power of this function is emphasized within nursing teams in order to change the organization of care and the practice of nurses.
-
Level 3: Nurse consultant
A rather generalist approach was preferred even if some more specialised training courses have also been proposed, notably in the field of cancerology.
3.3 Characteristics of the Curriculum
The modular curriculum, spread over several years, is implemented on a part-time basis; allowing the nursing to reain on her job, which favours the integration of the contents.
The programme is mainly offered by private school working outside the academic environment. Numerous attempts to establish partnerships with French and foreign universities have not yielded positive results.
Nurses who benefit from this programme develop the skills enabling them to fully invest the autonomy granted to their profession with the aim of improving the care provided to patients and achieving positive care results in a global approach to their health. One of the major objectives of this type of programme is to increase the level of expertise of clinical reasoning and to promote the use of nursing taxonomies, particularly nursing diagnoses, in order to clarify nurses’ clinical judgements. The autonomous therapeutic role of the nurse is strongly developed in the programme.
This programme is characterized by a strong porosity to the knowledge produced by the nursing discipline that provides nurses with theoretical frameworks for their clinical practice. The contribution of physicians in this programme is almost non-existent.
In addition to these purely clinical contents, the programme also encourages nurses to acquire a systemic understanding of organizations. It develops in the trainees the skills required to support the professional development of healthcare teams and to exercise effective clinical leadership that facilitates the introduction of innovation and support for change in healthcare sectors.
The final certification is organized before a jury of peers, which was initially international in nature.
3.4 A Formal Recognition of the Role That Was Narrowly Missed
In 1995, as part of the reform of the education programme of nurse managers, consideration was given to giving statutory and financial recognition to nurses who became certified in clinical nursing. Unfortunately, this project could not become a reality. A French society of clinical nurses having registered the title of clinical nurse, the reaction of schools wishing to continue offering these programmes was not long in coming, opening up legal proceedings for many years before a decision was handed down in their favour.
In this context of internal tension within the profession, the Ministry of Health decided to refrain from recognizing this role. 1995 therefore remains the year of missed opportunity for clinical nurse specialists.
3.5 Difficult Census of Certified Clinical Nurse Specialists
It is difficult to identify certified professionals at the various levels of the clinical career pathway; it should be remembered that the law establishing a National Order of Nurses dates only from 2006 (Hamel 2008). However, it can be estimated that many nurses have been certified at level 1, much fewer at level 2 and a very small number at level 3 (ANFIIDE 2016).
The majority of these nurses have reinvested the knowledge and skills gained from this programme in their clinical practice, whether they are employed or working in private practice.
3.6 Reinvestment of Clinical Competencies in Healthcare Environments
This type of programme has been attractive to nurses. While nurses initially enrol in these courses on an individual basis, the positive results obtained by certified nurses led hospitals to set up in-service training programmes in order to certify many nurses in the hospital.
There was no shortage of opportunities for reinvestment, as many changes were introduced in the healthcare sector during this period requiring clinical nursing expertise.
Examples include public health plans focusing on pain management, AIDS, the development of palliative care or cancer care. The increase in the prevalence and incidence of patients living with a chronic disease has also created new needs that clinical nurse specialists could meet, particularly in the area of therapeutic education.
In addition, the introduction of hospital accreditation in the late 1990s made it necessary to rely on this type of nurse prepared to implement the continuous quality improvement process.
Despite the added value generated by clinical nurse specialists, they did not obtain legislation change and financial recognition commensurate with their investment. The great majority of them did not agree to remain on the status quo of 1995.
A specific common interest group was created at the beginning of 2000 within the national nursing association (ANFIIDE); it quickly took the name of Advanced Practice Nursing Network (RéPASI). The work of this group is mainly based on the publications of the Advanced Practice Nurse Network of the International Council of Nurses.
4 From Clinical Nursing to Advanced Practice in Nursing
In a context marked by a search for a better match between the supply and demand for care, two dynamics have converged since the early 2000s to lead to the introduction of advanced practice in French legislation and regulations, which was achieved in July 2018. These two trends take a different view of the concept of advanced practice.
The first initiative emanates from nursing professionals who aspire to develop their clinical expertise. This desire results from the evolution of patients’ needs (complex situations, end-of-life support, support for people living with a chronic disease, etc.) and the process of professionalization of the nursing group. This movement has its origins in the development of the clinical career pathway and in the positions taken by the professional organizations of clinical nurse and clinical nurse specialists, in particular the RéPASI. Advanced practice is approached by the nursing profession as a strategy that could bring a nursing contribution to the problem of access to care while encouraging the development of nursing expertise for the benefit of patients. Frames of reference developed by ICN nurse practitioner/advanced practice nursing network and lessons learned from foreign experiences in this field were integrated into this vision of advanced practice carried by the nursing profession.
The second initiative, which emerged in the early 2000s, approaches advanced practice as an effective strategy to address the problem of medical shortages. This shortage is the consequence of the application of a very strict numerus clausus at the end of the first year of medical studies coupled with the complete freedom left to young physicians to choose where they wish to practise in France, even though their university training is largely subsidized by the state within public universities. The main aim of this strategy is to save medical time by transferring to other professionals activities that were previously the exclusive medical prerogative of the state. This vision of advanced practice is influenced by the concept of task shifting introduced by the WHO (World Health Organization 2007). These recommendations were formulated in a report written in 2003 by Professor Berland, Dean of the Faculty of Medicine of Marseille (Berland 2003).
The bibliographical search carried out in the context of the preparation of this report highlighted the benefits of advanced nursing practice in the countries that have implemented it. However, the proponents of this trend retain only certain characteristics of the concept. The approach remains strongly centred on the patient’s health problem addressed primarily from the biophysical perspective and often omits the added value of the holistic nursing approach centred on the patient’s experience that characterizes advanced practice.
It can therefore be observed that a plural vision of advanced practice animates the stakeholders involved in the reflection aimed at evaluating the relevance of its introduction in the French context. However, political decision-makers seem much more influenced by the second current in their understanding of the concept.
5 Experimentations and Lengthy Negotiations
Changing the structure of the health professions and transferring to “medical auxiliaries” activities previously exclusively implemented by physicians is always a sensitive subject in France. For some physicians and for many medical professional organizations, in particular the private practice physicians’ unions, it gives rise to a feeling of loss of monopoly in the field of health and, for some, potential financial loss as well. Didier Tabuteau points out that this fear might be linked to the history of the medical profession, which lost its monopoly during the French Revolution with the creation of health officers (Tabuteau 2012); it took a century to the medical profession to recover it at the end of the nineteenth century, and now they want to keep it.
This highly political subject has, in fact, undergone many changes in line with the orientations of successive governments during the 15 years of discussions surrounding this project.
Reports and experiments have multiplied, generating a significant latency in decision-making. In 2011 in particular, the Hénart-Berland-Cadet report nevertheless stressed the urgency of reaching decisions in this field in view of the constant increase in the population’s health needs and the growing difficulties of access to care (Hénart et al. 2011). This latency has had harmful consequences in clinical environments, forcing professionals to find solutions to the difficulties encountered, even if it means going beyond their scope of practice, as highlighted by the public survey conducted by the HAS in 2007 (Haute Autorité de Santé 2007).
In 2009, as part of the adoption of a broader public health law, an article introduced the concept of cooperation between health professionals based on protocols (Ministry of Health 2009). These protocols, drafted by the professionals concerned at local level (hospital, health centre, etc.), must be validated by the Regional Health Agency (ARS) and the High Authority for Health (HAS). The aim of this article was to legalize the transfer of activities by describing them in an explicit protocol. This mechanism is directly inspired by the concept of task shifting introduced in 2007 by the WHO (World Health Organization 2007). However, the methodology imposed to draft a protocol is very cumbersome to implement by teams wishing to engage in a project of this nature. Moreover, the nominative nature of these protocols sometimes creates difficulties for professionals and institutions in terms of continuity of care provision. Indeed, if the delegator (the physician) or the delegate (e.g. the nurse) is absent, the activity can no longer be implemented. Similarly, a nurse forced to move to another hospital for personal reasons does not retain the benefit of the skills developed in the position he/she just left. There was no economic model attached to this type of practice until 2019: a nurse who develops these complementary skills and implements these derogatory activities does not receive additional remuneration. Finally, the additional education required to develop the skills needed to implement the activity delegated by the physician is very focused on the intervention and does not necessarily include the development of nursing expertise, which would be essential for the effective implementation of a protocol of this nature in a patient-centred approach. These shortcomings were identified in the evaluations of the methodology carried out by the HAS (Haute Autorité de Santé 2015). However, and despite these shortcomings, this system will be maintained; the methodology will simply be simplified (Ministry of Solidarity and Health 2018a). These cooperation protocols have been criticized by many professional organizations, including the National Nursing Order. Implemented in conjunction with the discussions on the introduction of advanced nursing practice, this project has created a lot of confusion, creating the false impression that any nurse included in a cooperation protocol could be considered an advanced practice nurse.
As the publication of legislation introducing advanced practice in nursing was repeatedly announced as imminent by successive ministers of health but was repeatedly postponed until later, some universities wanted to take the lead in anticipating the education of future advanced practice nurses. Two master’s programmes dedicated to advanced practice have thus been proposed by two French universities. In the absence of legislation defining the function of advanced practice nurse in France and in order to avoid encouraging nurses for the illegal practice of medicine, the expected profile of these programmes was that of clinical nurse specialist, but the commonly used name was advanced practice nurse. From 2012, the political changes that have taken place lead the ministers of health and higher education to veto the development of other programmes of this type in the absence of legislation governing advanced practice in France.
In 2016, a study performed by ANFIIDE identified approximately 103 nurses graduated from these programmes (ANFIIDE 2016). The introduction of these professionals in often unprepared practice environments has made it difficult for them to reinvest the gains they have made from their master’s and has led many of them to feel frustrated. In addition, some of these advanced practice nurses have integrated a cooperation protocol in order to benefit from a legal framework for their practice.
These phenomena have increased the confusion between advanced practice and cooperation protocol in the French context.
Finally, the Ile-de-France Regional Health Agency (ARS) launched an initiative in 2014, the PREFICS project, with the aim of encouraging hospitals and health centres in this region to create advanced practice nursing positions. Some master’s degree programmes were identified within the framework of this project in order to prepare the future nurses included in this initiative, but great heterogeneity can be observed in these programmes (Agence Régionale de Santé-Ile-de-France 2016).
It should be noted that all of these professionals coming from different educational pathways considered themselves to be in advanced practice.
6 A Lengthy Process of Developing Legislation and Regulations for Advanced Nursing Practice
Article 119 of the law on the modernization of the health system voted in 2016 (Safon 2016) was obtained after long negotiations; in the future it will allow all professions qualified as “medical auxiliaries” to get access to advanced practice. Many professional organizations have worked to achieve this outcome, targeting not only decision-makers but also the nursing profession in all its diversity.
After this law was passed, the aim was to maintain lobbying activities on the subject in order to obtain text to implement this article of the law.
It took almost a year for the Ministry of Health to begin the process of drafting these texts.
A first step towards this goal has been taken from December 2016 to April 2017. The Ministry of Health has set up a large group of experts in a process that was announced as “participatory”. Hearings of professionals and managers from clinical environments have been organized in order to better identify needs but also to identify innovations in this field. Many graduates from the two clinical master’s programmes were thus able to present their approach to care to this group of experts. The experiences gathered were diverse, hospital, ambulatory and occupational health sectors, and addressed somatic as well as psychiatric health problems. However, the Ministry of Health did not wish to involve the three existing nursing specialties in the reflection on the introduction of advanced practice creating a profound resentment.
Following these hearings, a final meeting was held in April 2017 during which a draft text was presented by the representatives of the Ministry of Health to the experts of the working group. The latter considered that the proposals made did not reflect the work of the group stressing that the Ministry of Health opted for a very restrictive vision of advanced practice imposing a strong dependency of advanced practice nurses to the medical authority. This proposal was rejected by the nursing representatives.
French political events then interrupted this work for several months. After the election of a new President and a new National Assembly as well as the appointment of a new government in the first half of 2017, the debate only resumed in the autumn of 2017 part of a national plan to improve access to healthcare (Ministry of Solidarity and Health 2017).
However, the methodology adopted by the new ministers in charge of the project was different from the previous one. Three very tight groups were set up and a very tight schedule was imposed on them. The number of nurses around the negotiating table was small.
The first group, led by the Ministry of Health, was tasked with drafting the texts governing the practice of advanced practice nurses. Areas of tension were quickly identified during the negotiation process within this group, particularly about the lack of positioning first-line healthcare provider, the autonomy granted to advanced practice nurses, etc. The areas of certification selected were also the subject of controversy. The initial project planned to propose four areas of certification: chronic disease, oncology/hemato-oncology, chronic kidney disease/dialysis/renal transplantation and psychiatry/mental health. However, despite the major needs identified in the area of psychiatry and mental healthcare provision in France, representatives of psychiatrists refused to introduce advanced practice nurses in this field. In order not to delay the publication of the texts, the Ministry of Health decided to create three areas in 2018 and to continue negotiations for an additional year for the psychiatry and mental health area.
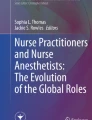
The second group was led by the Ministry of Higher Education and Research. The aim was to define the curriculum in order to be alabl to admit first students in autumn 2018. A list of activities and a competency framework (Fig. 10.1) were developed as well as a national curriculum which sets out the broad outlines of the educational pathway advanced practice nursing students must follow. The criteria for university accreditation have also been defined.

French advanced practice nurse competency framework
Finally, the third group’s mission was to propose an economic model that would enable this type of exercise to be paid.
It should be noted that all of these texts were prepared quickly in order to meet the ambitious timetable set by the government. The first two groups began their work at the same time, while the third group was postponed.
Moreover, in the context of the final validation of these draft texts, the High Council of Paramedical Professions (HCPP), which brings together representatives of the professions qualified as “medical auxiliaries”, did not give its approval, considering them insufficiently ambitious.
Despite this lack of validation by this consultative body, the implementing texts were published in July 2018. They were then amended in August 2019 in order to introduce the field of psychiatry-mental health certification finally accepted by psychiatrists after an additional year of negotiations.
7 Summary of the Texts Published in July 2018 and August 2019 Defining the Advanced Practice Nursing Practice
The implementation texts, published in July 2018 and amended in August 2019, are based on the elements already set by Article 119 of the law on the modernization of our health system voted in 2016 (Ministère des Affaires Sociales et de la Santé 2016).
The advanced practice nurse in France is therefore governed by one law (Ministère des Affaires Sociales et de la Santé 2016), two decrees (Ministère de l’enseignement supérieur, de la recherche et de l’innovation 2018; Ministère des solidarités et de la santé 2018b) and three acts (Ministère des solidarités et de la santé 2018c, d; Ministère des solidarités et de la santé-Ministère de l’enseignement supérieur, de la recherche et de l’innovation 2018). They establish a specific protected title for this role.
An analysis of these texts reveals the salient aspects of the advanced practice nurse profile in France.
-
The advanced practice nurse must necessarily be part of a team, and his/her activity is therefore interdependent with that of the other members of the team he/she works with in a hospital or in the community.
-
Advanced practice nurse can be employed in the public (civilian sector as well as in the military health service) or private sector; he/she can as well work in private practice.
-
The advanced practice nurse’s scope of practice is broader than that of other nurses; they have prescribing authority. However, the autonomy granted to this category of nurses is supervised by the physician who decides to refer patients with stabilized chronic disease to an advanced practice nurse. Patients may refuse this proposition. The physician identifies beforehand patient’s diagnosis and prescribes the treatment. The advanced practice nurse organizes the patient’s care pathway.
An organization protocol written and signed by the physician and the advanced practice nurse determines their methods of intervention and collaboration. Within this collaborative practice with the physician, the advanced practice nurse is responsible for its decisions and actions.
An advanced practice nurse is certified in one of the four areas of intervention currently defined by the texts:
-
Stabilized chronic disease, prevention and common polypathologies in primary care
-
Oncology and hemato-oncology
-
Chronic kidney disease, dialysis, kidney transplantation
-
Psychiatry-mental health
Any patient with a pathology included in one of these fields can benefit from the intervention of an advanced practice nurse regardless of age if his/her condition is deemed stable by his physician.
More specifically, advanced practice nurse’s activities fall into two categories: clinical and focused on team/organisation.
7.1 Clinical Activities
Advanced practice nurse’s area of certification determines the nature of the clinical activities that the nurse can implement in the follow-up of patients living with a chronic disease considered to be stabilized who are referred to it by a physician. The nurse mobilizes his/her skills with the aim of working with the patient to maintain this state of stability by implementing a wide range of activities:
-
Preventive activities, in particular therapeutic education of the patient
-
Renewal or adaptation of the treatment plan initially prescribed by the physician
-
Prescription of diagnostic tests (lab test, X-ray, etc.) in order to support the nurse’s clinical reasoning or that of the physician (the list of tests that an advanced practice nurse is authorized to prescribe is set by an act)
-
Performance of specific technical procedures
-
Prescription of nursing care provided by home care nurses
-
Referral of patients to the appropriate health professional to meet their needs
In addition, advanced practice nurse implements activities relating to the clinic within the framework of the missions assigned to it.
7.2 Activities Focused on Team/Organisation
They are essentially team-centred and aim to improve the quality and safety of care as well as individual/team performance.
The range of activities that the advanced practice nurse can implement to achieve this objective is varied: knowledge transfer to staff, promotion of evidence-based nursing, implementation of continuous quality improvement and risk management process, introduction of clinical innovations, continuous professional development of nurse, contribution to research, etc.
In hospitals, these activities are implemented in the context of a collaborative practice established with nurse managers.
8 Curriculum
Section 119 of the law passed in 2016 insisted on the need to validate qualifying programme to obtain the title of advanced practice nurse. This programme must be provided in a university setting. Universities (schools of medicine) wishing to offer this type of programme must be accredited by the Ministry of Higher Education, Research and Innovation (MESRI).
A decree and an act set the outline of the national curriculum. The curriculum is based on a competency-based approach.
The curriculum published in 2018 includes innovative elements in the nursing education scheme. In order to respect the autonomy of universities, flexibility has thus been left to the faculties in the implementation of the national curriculum, and the pedagogical choices are validated by the university internal authorities. The final certification is issued by the university.
Flexibility can be introduced in particular in:
-
The design of the pedagogical project based on the curriculum
-
The modalities of implementation of the programme (face-to-face, distance learning or mixed model)
-
The student selection process
-
The summative evaluation framework
For the first time in France, a curriculum dedicated for nurses will be fully implemented by the university (faculties of medicine), while preregistration nursing education (baccalaureate level) and graduate programme for nurse anaesthetists are implemented within the framework of a partnership between the school of nursing and the university. Physicians and nurses will contribute their respective skills to the programme in both its theoretical and clinical components.
At the end of the programme, the student receives a state diploma that allows him/her to practise in advanced practice (protected title), and the level of study that he/she has attained is recognized at the master’s degree level, but the national master’s degree is not awarded.
The implementation of this programme is evaluated by the High Council for the Evaluation of Research and Higher Education (HCERES) as part of the periodic evaluation of all the missions and activities of the university concerned.
8.1 Selection of Students
The methods of selection of students differ from those previously used in nursing education. No annual admission quota is set at either national or regional level. Each university determines its students intake capacity according to the educational resources it is able to mobilize.
The selection process is determined by each university in accordance with the criteria and procedures determined by the university itself. Only one condition is imposed at national level: the candidate must have a nursing diploma or an equivalent title giving him/her authorization to practise in France.
Another particularity of the selection process is the possibility to enter in the programme directly after the preregistration course. However, in this situation, the newly graduated will only be able to practise as an advanced practice nurse after obtaining a diploma if he/she attests to a minimum of 3 years of experience as a nurse.
A validation of prior learning is possible allowing direct entry into semester 3. Nurses with a master’s degree in clinical nursing can, if they wish, apply to take advantage of this pathway. However, no specific collective measures (grandfathering) have been planned for this candidate profile, so they must undertake an individual approach, the results of which are linked to their career path but also to their ability to make the most of it in the resumé they write.
8.2 Programme Structure
The programme is Y-shaped and is spread over four semesters. Clinically oriented teaching units are predominant in this programme, given the centrality of this type of activity to the work of advanced practice nurse.
It is implemented by a teaching team made up of physician/nurse pairs.
Semesters 1 and 2 constitute the common core of the programme. A 2 months of clinical internship is scheduled during the second semester.
At the end of the second semester, the student selects the domain in which he/she wishes to be certified at the end of the programme.
Semesters 3 and 4 are specific to each domain.
During semester 3, clinical teaching remains central. Students can deepen their knowledge and apply their skills in their chosen field of practice, thus reinforcing fundamental knowledge and developing mastery of clinical reasoning as well as skills to efficiently coordinate a pathway of patients.
Semester 4 has a different format; students need to perform a 4-month internship and must write a master’s thesis allowing students to implement the research process while benefiting from supervision.
8.3 Clinical Internships
The two internships allow students to benefit from the integration of theory and practice. The student also benefits from tutoring during the internship period implemented by a pair of physician and nurse.
The first clinical placement, of a minimum duration of 2 months, must be validated during semester 2. It allows the student to understand the activities and the scope of the role he or she aspires to exercise. This internship also allows him/her to develop skills in clinical reasoning, in particular the performance of clinical examinations.
The second internship, carried out during semester 4, lasts a minimum of 4 months. This internship should enable the student to reinvest the clinical knowledge acquired during the previous semesters in a specific clinical domain. In addition, it enables the student to implement all the missions assigned to advanced practice nurse, particularly activities dedicated for healthcare teams, by exercising effective clinical leadership.
8.4 The Master’s Thesis
An important part of semester 4 is devoted to activities related to the thesis to be completed by the student under the supervision of a nurse or an advanced practice nurse.
The curriculum offers four modalities for the realization of this master’s thesis:
-
A literature review
-
An analysis of professional practices
-
A critical analysis, based on clinical experience, inspired by a specific theoretical framework
-
A research study
At the end of their programme, students are awarded a state diploma as well as a master’s degree attesting to the academic level reached by the university where they studied. In this system, the structure that prepares the student is the same as that which certifies the advanced practice nurse.
Equipped with this professional title, the newly graduated advanced practice nurse can then register his or her new qualification with the Nursing Order and practise his or her role.
9 Stakeholder Reactions After the Publication of the Texts
The publication of the texts governing the practice and education of advanced practice nurse has generated a great deal of reactions.
Curiously, patient associations have expressed little opinion on this subject.
On the other hand, there was no lack of reactions from medical professional organizations. The unions of private practice physician in particular expressed their positions more strongly, stating that physicians did not need advanced practice nurses but rather administrative assistants who would allow them to have more clinical time. The fear of a loss of remuneration in the private practice sector was also perceptible. Some medical professional organizations adopted a protective discourse towards patients and population, insisting on the supervision that physicians will perform on the clinical activity of advanced practice nurses, thus creating a potentially negative image of the competency and skills developed by this new category of nurses.
Nursing organizations did not fail to react to the profile of advanced practice nurse created by the legislation, especially since the draft texts had been disapproved by the HCPP. While ANFIIDE welcomed the introduction of this role in the health system, the lack of ambition in the texts was deplored. Many professional nursing organizations regretted the medical suzerainty imposed on this new role, which reduced advanced practice nurse’s autonomy; the level of competency and skills attained by students at the end of their education seems to be underestimated. They are also surprised by the low porosity of French texts with international evidence, despite the large amount of international data available on the subject. The lack of positioning of advanced practice nurse as first-line health provider is also deplored in view of the insufficient supply of primary care in many French regions. Finally, they underline the semantic choices made in the texts that reserve certain terms such as diagnosis, consultation, etc. for the physician.
These positions taken by professional organizations have been relayed by the media and social networks.
Graduates from Master of Clinical Nursing also expressed bitterness and dissatisfaction in the summer of 2018. The legislator did not wish to introduce a grandfathering process or a bridge dedicated to this group of nurses. The files of those who wish to benefit from a validation are therefore examined individually by the programme managers of the universities in which they are applying, which may lead to variable validations.
10 Perspectives
The introduction of advanced practice nurses in the French health system suggests that, in the long term, benefits similar to those evaluated in other national environments will be observable:
-
Improved access to healthcare for the population, particularly for people living with chronic diseases
-
Highlighting the added value for patients benefiting from advanced practice nurses’ interventions
-
Creation of practice environments more favourable to nursing practice in synergy with nursing management
-
Production of evidence showing the benefits for patients of a comprehensive nursing approach
-
Evolution of social representations of nurses
However, many challenges remain to be met in order to introduce this new nursing function into the health system and to ensure its sustainability.
10.1 Effective Implementation of the National Curriculum
While educational programmes are most often implemented by medical faculties, it is essential for this programme to be anchored in the nursing discipline and that nursing leadership can be exercised throughout it. Although the national curriculum provides for the establishment of nurse/physician pairs to ensure the coordination of units, the academic status of the nurse is not specified, unlike that of the physician; this observation may seem paradoxical when at the same time a body of nursing faculty was created in France in 2019.
In view of the innovative nature of this role, it is necessary to adequately prepare tutors. The first students will indeed be tutored by expert nurses and physicians, and then, as advanced practice nurses’ staff grows, this tutoring can be carried out by their peers.
The pioneering spirit often motivates the first students who take up this new role. This pioneering position also prevents them from benefiting from the modelling process that is nevertheless essential to the development of professional identity or more precisely to its adaptation to the specificities of advanced practice nursing.
During the first years, students will have to work hard to make known this new role for which they are destined, all the more so as many misconceptions still surround advanced practice in France.
It will also be necessary to observe the career paths of students who have undertaken this programme immediately after registration. There is a significant risk of loss of skills and competency if the newly graduated advanced practice nurse cannot carry out its role during this 3-year period.
Finally, the autonomy left to the universities in the implementation of the programme combined with the role of certifier that has been assigned to them exposes them to the risk of heterogeneity of advanced practice nurse profiles.
10.2 Successful Deployment of Advanced Practice Nurses in Clinical Environments
The phases of introduction of the advanced practice nurse and deployment of the first qualified professionals are always singular moments within a health system. It is therefore necessary to anticipate their deployment in clinical environments and to provide them with a favourable practice environment in order to create attractiveness for this type of position.
Indeed, it is not enough to succumb to the fashion effect by simply creating one or more advanced practice nurse positions in the hope that they will find their place in the multi-professional team. Initiating a project of this nature implies rethinking the organization of care within a team in order to integrate this new player (Schober 2017). Models of care organization should be developed both in hospitals and in the community, taking into account the available evidence in this field.
The advanced practice nurse will have to establish a collaborative practice with physicians.
They will also have to gain the legitimacy and credibility necessary to exercise effective clinical leadership within the nursing team. It is essential that the first advanced practice nurses continue to identify themselves with the nursing profession.
It will also be important for those who will be working in a hospital to create synergy with the nursing management in order to avoid any impression of competition between the two roles.
10.3 Assessing the Added Value of Advanced Practice Nurse
French Members of Parliament have asked the Ministry of Health to carry out an initial assessment of the impact of the introduction of advanced practice nurses in the health system by the end of 2021. The results of this evaluation will be decisive for the future of this role. However, the Ministry of Health has not yet communicated on the method that will be used. It is crucial that the choice of indicators as well as the methods of evaluation be adapted; it is absolutely necessary to avoid an evaluation of the activity that is too focused on the medical time saved and does not take into account the added value of the global approach adopted by the advanced practice nurse.
10.4 Propose an Economic Model That Is Commensurate with the Contribution Made
The economic model designed to remunerate the activity of the advanced practice nurses working in the public or private sector as well as in independent practice is not yet fully known. The first decisions made in this area concern the advanced practice nurse who will be working in private practice, and they fall far short of the expectations of advanced practice nurse students. Moreover, the first projections concerning remuneration in the public sector have also led to disappointment for future advanced practice nurses.
The economic model chosen will reflect the social recognition attributed to this role and will also be a factor of attractiveness towards this clinical career.
10.5 Changing Profile and Creating New Areas of Intervention
Healthcare is being restructured in France. In this dynamic context, it will be necessary in the future to influence the ministerial positions regarding advanced practice nurse as first-line health provider. It would improve access to primary healthcare and relieve congestion in the emergency services.
New areas of intervention could be created to better meet the health needs of the population. For example, a consultation was launched in November 2019 to examine the potential contribution of advanced practice nurse in emergency departments. Other sectors have also expressed a desire to benefit from advanced practice nurse, such as the army health service as well as occupational health teams.
However, it will be necessary to avoid too great a fragmentation of the areas of certification, which would expose to the risk of overlapping fields of intervention of advanced practice nurses.
11 Conclusion
At the end of this description of the French situation, it appears that the profile of advanced practice nurse that has been introduced into the health system is certainly an evolution for the healthcare supply and for the nursing profession, but not a real revolution. Following the example of foreign experiences in this field, it is likely that this first legislative decision opens the way for further developments, particularly in terms of the autonomy granted to advanced practice nurse.
The process of introducing advanced nursing practice in France began with initiatives in the field of education combined with changes in the practice of nurses who had benefited from these skill developments before obtaining an appropriate legislative framework. A significant latency has been deplored coupled with highly fluctuating political orientations on this topic. Three profiles of advanced practice nurses have thus followed one another, resulting from three educational systems: nonacademic, master’s degree, and university education recognized at master’s level. This sequence can be frustrating for professionals who, due to the lack of a legislative framework and a suitable practice environment, have had difficulty putting into practice the skills developed during their course of study.
The long negotiation process that preceded the publication of the legislative texts and the content of these texts are also indicative of the sociology of the health professions in France and the way nursing professional leadership is exercised in France. The current context of healthcare in France is marked by an erosion of leadership exercised by nurses and nurse managers to the benefit of the medical profession, which, at clinical level, in management and in education, seems to wish to occupy a predominant position. The choices made related to the scope of practice of advanced practice nurse fail to take into account certain population needs, ignoring the recommendations published in this field (Bryant-Lukosius and DiCenso 2004) with the aim of maintaining the initial structure of the health professions between the medical profession on the one hand and “medical auxiliaries” on the other. The semantic analysis of the terms used in the legislation and regulations is indicative of the frame of reference used by those who wrote them, as are the terms that seem to have been deliberately avoided because they are considered to be exclusively reserved for physicians. However, it is interesting to highlight the essential role of the national nursing association in this project but also to note that even before the first advanced practice nurse graduated, a dedicated trade union was created to defend their interests and their future working conditions as well as their remuneration. This is a rather singular phenomenon in the nursing profession.
A new phase in the history of nurses in France is therefore underway. In the future, advanced practice nurses will undoubtedly contribute to preserving universal health coverage and, consequently, the health of the population living in France.
This topic will also offer many objects to explore through research.
References
Agence Régionale de Santé-Ile-de-France (2016) Projet “Préfiguration d’Infirmiers Cliniciens Spécialisés”. Rapport final—Synthèse
ANFIIDE (2016) L’infirmière de pratique avancée, bilan d’étape, état des lieux en France
Berland Y (2003) Mission “Coopération des professions de sante: le transfert de tâches et de compétences”. Rapport d’étape
Bourgueil Y, Marek A, Mousquès J (2005) La participation des infirmières aux soins primaires dans six pays européens et au Canada
Brami L, Damart S, Kletz F (2012) Réformes de l’hôpital, crise à l’hôpital: une étude des liens entre réformes hospitalières et absentéisme des personnels soignants. Politiques et management public 29:541–561
Bryant-Lukosius D, DiCenso A (2004) A framework for the introduction and evaluation of advanced practice nursing roles. J Adv Nurs 48:530–540
Debout C (2014) [The clinical nursing practice some elements of clarification in the French context]. Soins; la revue de reference infirmiere 26–31
Debout C (2016) Vieillissement, chronicité et virage ambulatoire: impact sur les soins à domicile. Journal de droit de la santé et de l’assurance maladie 25–29
Debout C (2018) Infirmière de pratique avancée en France: première esquisse. Soins 63:59–65
Debout C, Magnon R (2014) Léonie Chaptal, un leader visionnaire. Les Tribunes de la santé 73–83
Desailly-Chanson MA, Siahmed H, Elshoud S (2016) Etablissements de santé Risques psychosociaux des personnels médicaux: recommandations pour une meilleure prise en charge Mise en responsabilité médicale: recommandations pour une amélioration des pratiques. Rapport Inspection Générale des Affaires Sociales [Report of the Inspector General of Social Affairs]
Direction de la recherche, des études, de l’évaluation et des statistiques (2017) L’état de santé de la population en France: rapport 2017
DREES (2018) 53% d’infirmiers en plus entre 2014 et 2040, une forte hausse qui répond à la demande de soins. Etudes et rapports
Hamel F (2008) Mouvements infirmiers, représentation professionnelle et conflits sociaux. Rech Soins Infirm 44–48
Haute Autorité de Santé (2007) Les pratiques actuelles de coopération: analyse des témoignages des professionnels de santé
Haute Autorité de Santé (2015) Les protocoles de coopération art 51
Hénart L, Berland Y, Cadet D (2011) Rapport relatif aux métiers en santé de niveau intermédiaire
Leroux-Hugon V (1992) Des saintes laïques. Les infirmières à l’aube de la IIIe République, Paris. Sciences en situation
Ministère de l’enseignement supérieur, de la recherche et de l’innovation (2018) Décret no 2018-633 du 18 juillet 2018 relatif au diplôme d’Etat d’infirmier en pratique avancée
Ministère de la Santé (2009) Loi Hôpital, patients, santé et territoires (HPST)
Ministère des Affaires Sociales et de la Santé (2016) LOI n° 2016-41 du 26 janvier 2016 de modernisation de notre système de santé
Ministère des solidarités et de la santé (2017) Renforcer l’accès territorial aux soins
Ministère des solidarités et de la santé (2018a) Ma santé 2022: un engagement collectif
Ministère des solidarités et de la santé (2018b) Décret no 2018-629 du 18 juillet 2018 relatif à l’exercice infirmier en pratique avancée
Ministère des solidarités et de la santé (2018c) Arrêté du 18 juillet 2018 fixant la liste des pathologies chroniques stabilisées prévue à l’article R. 4301-2 du code de santé publique
Ministère des solidarités et de la santé (2018d) Arrêté du 18 juillet 2018 fixant les listes permettant l’exercice infirmier en pratique avancée en application de l’article R. 4301-3 du code de santé publique
Ministère des solidarités et de la santé-Ministère de l’enseignement supérieur, de la recherche et de l’innovation (2018) Arrêté du 18 juillet 2018 relatif au régime des études en vue du diplôme d’Etat d’infirmier en pratique avancée. JORF
Mossé P (2018) Une économie politique de l’hôpital-contre Procuste
OECD (2017) How much do OECD countries spend on prevention? (OECD health working papers no. 101). https://doi.org/10.1787/f19e803c-en
Poisson M (1998) Origines républicaines d’un modèle infirmier, (1870-1900): histoire de la profession infirmière en France. Editions hospitalières, Vincennes
Safon M-O (2016) Loi de modernisation de notre système de santé. IRDES, Paris
Schober M (2016) Introduction to advanced nursing practice: an international focus. Springer
Schober M (2017) Strategic planning for advanced nursing practice. In: Strategic planning for advanced nursing practice. Springer, pp 9–33
Simonet D (2014) Assessment of new public management in health care: the French case. Health Res Policy Syst 12:57
Tabuteau D (2012) Santé et politique en France. Rech Soins Infirm 6–15
Tabuteau D (2013) Les pouvoirs de la santé: la complexité d’un système en quête de régulation. Les tribunes de la santé
Vigneron E (2018) Histoire et Préhistoire de la coopération hospitalière et des groupements hospitaliers de territoire (GHT). Bull Acad Natl Med 202:1967–1979
World Health Organization (2000) The world health report 2000: health systems: improving performance. World Health Organization
World Health Organization (2007) Task shifting: rational redistribution of tasks among health workforce teams: global recommendations and guidelines
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Debout, C. (2021). From the Nurse Specialist in Clinical Nursing to the Advanced Practice Nurse with Prescribing Rights: The French Case. In: Fulton, J.S., Holly, V.W. (eds) Clinical Nurse Specialist Role and Practice. Advanced Practice in Nursing. Springer, Cham. https://doi.org/10.1007/978-3-319-97103-2_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-97103-2_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-97102-5
Online ISBN: 978-3-319-97103-2
eBook Packages: MedicineMedicine (R0)