
Abstract
This chapter is an overview of the issues for older people in relation to transport and technology. I demonstrate that mobility and technology are intertwined in complex ways, and that non-transport technologies may impact older people’s experience and achievement of mobility. Understanding the nexus between mobility, information and communication technologies and older people can help us design accessible and acceptable technologies to support well-being and health in older age. This matters because new ICT is increasingly relied on to support service delivery in both the public and private sectors. Older people are heterogeneous, with different attitudes, levels of income and education affecting technology uptake. Age-related cognitive and physical impairments can also impact on technology adoption. The chapter concludes with how age-friendly design principles can support active ageing.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Active ageing
- Transport
- Self-driving vehicles
- Assistive technologies
- E-Health
- Technology adoption/take-up
Introduction
This chapter is an overview of the issues for older people in relation to the nexus between transport and technology , that is intended to set a context to complement the other contributions to this volume particularly Chapters 5 and 9. A key aim of this chapter is to demonstrate that mobility and technology are intertwined in complex ways, and that even non-transport technologies may impact older people’s experience and achievement of mobility . Understanding the nexus between mobility , information and communication technologies (ICT) and older people can help us design accessible and acceptable technologies to support well-being and health in older age. This matters because new ICT is increasingly being relied upon to support service delivery in both the public and private sectors. For example, ICT is increasingly harnessed to support centralisation of aspects of service provision, or even to virtualise it entirely. In many cases, this removes, or modifies, the need to travel to access certain services. For example, personal banking can be carried out online, from transferring money between accounts to paying bills. This removes the need to travel to a branch, and as a result of increasing uptake, banks have rationalised and reduced their branch networks. As a society, this should make us ask the question ‘How does this impact on people, and what are their perceptions of this shift?’ If we find that particular groups within society, such as older people, are significantly negatively impacted, we should consider if there are good societal reasons to mitigate these effects in some way. Indeed, in the UK some banks are making some efforts to engage different groups with new technology , for example Barclays Bank has a ‘Digital Eagles’ scheme, for which older adults are a key audience.Footnote 1 In relation to the development of new technologies in general, it is recognised that older people may be more likely to experience a reluctance or difficulty in adopting the technologies. However, being over 65 is not in itself a predictor of low technology adoption . The older age groups are heterogeneous, with different levels of income and education affecting adoption rates. The greater prevalence of cognitive and physical impairments can also impact on technology adoption . Attitudes are also relevant, as some older people may not see a need to adopt technologies that they have managed many decades without (Smith 2014).
Conversely, there are opportunities to utilise ICT to improve the experience of service access specifically for older people. Healthcare is one domain where ICT is increasingly used to support older people, for example through assistive technologies , the majority of which are not intended to support out-of-home mobility , but to support ageing-in-place and reduce the need for travel to health centres. Where travel to health centres and hospitals is still necessary, centralisation of service provision in the health sector, and loss of public transport in the transport sector have had the twin effects of creating a great burden for people of any age experiencing ill-health , but it is particularly problematic for older adults who cannot access a car. ICT could be used to dovetail appointment times with available transport, but this type of change needs to be led and delivered by the healthcare provider, ideally in collaboration with transport providers.
ICT and other technologies are converging rapidly in the transport sector, enabling almost real-time access to demand responsive services, which have existed for some decades with pre-booking first by telephone, but with online options introduced later. This transport-ICT convergence is resulting in the emergence of many new services based on the affordances of smartphone technology . However, older people are not usually regarded as the target market for these products—Alba (2016) deduces from smartphone sales trends that the market is more or less saturated such that everyone who wants one has one, and by further inference from the demographics of smartphone ownership, older people own them at lower rates than younger people (e.g. Pew Research Center 2017). There are a number of reasons why smartphone adoption is lower amongst older people—new technology adoption in general slows with age (as mentioned above), and it is clear to see that most advertising of new technology products portray images of youth, unless it is a technology designed mainly for older people (such as stair lifts or mobility scooters). Another key reason is likely to be design or usability, particularly in relation to the touch screen-based user interface, which poses particular issues for people with visual or upper limb impairments (Mi et al. 2014). Conversely, older people are often described as a key beneficiary of a game-changing technology which is on the brink of an innovation breakthrough. For example, autonomous , or self-driving vehicles (SDV), are described by some authors as a key assistive technology for maintaining out-of-home mobility .
The remainder of this chapter is structured by a brief reprise of the importance of out-of-home mobility for healthy ageing in the context of an ageing global population, touching on the heterogeneity of needs and wants amongst older people. The next section will examine aspects of the nexus between mobility , ICT and older people in order to show how well-being and health can be supported using technologies that are accessible and accepted by older people, with subsections on mobility technologies and possible future developments. The final section before the conclusions and policy recommendations considers the potential role of age-friendly design in transport policy and cities. The perspective is primarily one from the Global North.
The Importance of Out-of-Home Mobility for Healthy Ageing
The ability to move about—and by extension to travel—is required to navigate from point A to point B, to seek out places of subjective interest or that are essential to meeting daily material needs , to participate in cultural and recreational activities, and to maintain social relations, familiar habits, and life styles—in short, to live an autonomous life for as long as one’s mental and physical capacities permit one to participate actively in society (Schaie, 2003). At the same time, age-related changes such as physical, cognitive, and/or sensory impairments and social losses may limit older adults’ possibilities of ambulating and venturing out. (Mollenkopf et al. 2017, p. 267)
As is evident from the quotation from Mollenkopf et al. (2017) above, mobility is a crucial issue for healthy ageing, and we are we are reaching greater ages at unprecedented rates. It is forecast that the proportion of the global population of 80 years or older will be 20% by 2050 (UN 2015). Setting that into the context of a global population that is growing at 1% per annum, the growth rate in the 80+ age group is 4% (HelpAge International 2012 cited by Sixsmith 2013). Geographically, more than 60% of the older population are in less developed regions, with the 2050 forecast being 80%. This poses a considerable challenge for service providers in supporting older people to extend good health and quality of life for as long as possible. The concept of ‘active ageing ’ is increasingly dominating the policy discourse, defined by the World Health Organization as:
Active ageing is the process of optimizing opportunities for health , participation and security in order to enhance quality of life as people age … It allows people to realize their potential for physical, social, and mental well being throughout the life course and to participate in society according to their needs , desires and capacities, while providing them with adequate protection, security and care when they require assistance. (WHO 2002, p. 12)
Active ageing spans many policy areas, including health , education, and housing, though mobility underpins all of them (Johnson et al. 2017), as the key individual and policy goal is perceived as being maintaining autonomy and independence for as long as possible. Somewhat confusingly however, the Active Ageing Framework also talks of interdependence and intergenerational giving (WHO 2002).
Bodily mobility is more likely to be compromised in older adults, making the achievement of out-of-home mobility more challenging. However, there is a sizeable body of research that demonstrates that out-of-home mobility is an important determinant of quality of life for older adults (Metz 2000; Spinney et al. 2009; Gilhooly et al. 2002), where quality of life includes aspects such as being autonomous and having a social life (Ziegler and Schwanen 2011), being able to obtain daily necessities and healthcare, and be part of a community (Kaiser 2009), which collectively are associated physical and mental benefits that we might term ‘well-being’ (Reardon and Abdallah 2013; Simonsick et al. 2005). In summary therefore, mobility , and especially out-of-home/outdoor mobility , has clearly been identified to be a key factor in successful ageing for older adults (Mollenkopf 2005; Kaspar et al. 2015), due to the powerful effect of a sense of fulfilment that is conferred by independence (Mokhtarian et al. 2015; Musselwhite 2011).
What factors influence the levels of out-of-home mobility that older adults are able to achieve? Numerous research studies have quantified the out-of-home mobility of older people such as those cited by Mollenkopf et al. (2017) who note that whilst there are differences explainable through national ‘peculiarities’, there are general tendencies.
Firstly, the amount of travel undertaken by older adults has been increasing over the last twenty years. However, within the ‘older adult’ category, the amount of travel is significantly reduced with increasing age. This is not surprising, as it is mainly due to a decline in health and an increase in sensory impairment. Secondly, in relation to a key transport concern of mode choice, those with a driving licence and access to a car will tend to travel more than those who do not have such access. There is thus a gender effect, as the current cohort of older women has a lower level of education, a lower income and is less likely to have a driving licence than men of the same age. Thirdly, therefore, older women use public transport more than older men, who use the car more often, travelling more often and further (see, e.g., Banister and Bowling 2004; Marottoli et al. 1997; Mollenkopf et al. 2004; Rosenbloom 2004).
As possession of driving licence and access to a car is a significant predictor of higher overall mobility , the effect of ill-health and sensory impairment resulting in driving cessation can be significant (Zeitler and Buys 2015; Souders and Charness 2014). Maratolli et al. (2000) found a strong association between driving cessation and decreased out-of-home activity, even after correcting for sociodemographic and health -related factors. In a highly car-dependent society, a lack of alternatives to driving leads to transport disadvantage amongst older adults (Engels and Liu 2011). This is juxtaposed against a normative expectation of increased mobility amongst older adults (Alsnih and Hensher 2003). Consequently, a great deal of effort is expended on extending safe driving for longer, through various, technological means, in order to prolong independent living (Nordbakke and Schwanen 2015).
In contrast to these efforts to maintain driving as a component of independent living , there are parallel developments, largely from the health sector, which focus on ICT as a technological support for independent living that bypasses a need for ‘out-of-home’ mobility .
Mobility, ICT and Healthy Old Age
ICT has emerged as a major strand in research and development for older people, as it is perceived as being able to provide better ‘care’ at potentially lower cost. Health -related ICT, or e-health , is largely intended to deliver remote health monitoring of older people living in the community (‘care at a distance’, O’Hanlon et al. 2012) rather than in residential care, but it overlaps quite heavily with ‘efficiency’ measures in healthcare provision, through reducing the need for human-delivered care. Remote health monitoring is now quite highly advanced, and can involve contactless sensors capable of detecting falls , or providing continuous monitoring of important indicators such as blood pressure (Malasinghe et al. 2017). Whilst the motive is one of benefit for the patient in being able to remain in personal environments, there is also a cost advantage to avoiding hospital stays:
With the new remote health monitoring applications, elderly patients can engage in daily activities without support from a caretaker. So, these applications support activities like sitting, standing, using the bathroom, watching television, reading and sleeping, with least inconvenience to the user. Even if there are wearable sensors, these pose minimum effect to the activities. One such example is smart wrist-watch based sensors. (Malasinghe et al. 2017, p. 1)
However, this is not necessarily a perfect solution, for as with the inexorable shift online of banking services, e-health also potentially reduces the amount of social contact and out-of-home mobility that older people experience.
However, Sixsmith (2013) points out that the majority of assistive technology and e-health research is focused on assisting those who are already impaired in some way, when it is actually the case that the majority of older adults are currently healthy and active. He recommends that technology Research and Development should focus on providing this group with products and services that maintain their proactive and independent status for as long as possible. Thus, wearable technologies that encourage physical activity such as Fitbit, IQ-FIT, Moov Now or Garmin could perhaps be promoted more specifically to the older adult market. Research suggests that they could be useful for older adults by providing them with data for self-monitoring and to encourage greater levels of activity to support health (O’Brien et al. 2015; Lyons et al. 2017).
The social and political tendency to stereotype older people as passive and dependent overlooks the fact that most older people are proactive agents living healthy and independent lives, and the goal should be to support this status, rather than expecting that they will become passive receivers of care (notwithstanding the increased proportion of self-reported ill-health after 75 years). It is increasingly recognised that old age is not a homogenous category (Haustein 2012). In terms of health , this variety means that ‘chronological age is not a relevant marker for understanding, measuring, or experiencing healthy aging’ (Lowsky et al. 2014, p. 640).
Technology Take-up Amongst Older People
Attitudes to technology are similarly heterogeneous. Interface design studies from the turn of the twenty-first century demonstrated that older technology users are much more diverse than younger and middle-aged users (Gregor et al. 2002). In a survey of ICT use amongst the over-60s in England and Wales, Selwyn et al. (2003) found that part of the reason for the low usage of ICT in this age group, despite the growing numbers of ‘silver surfers’, is to do with ‘relevance’. In essence, ICT was used if it had relevant function or content for the user. Other literature also suggested that many older people are not technophobe per se but see little relevance in the use of digital technologies in their daily lives, despite the ‘information society’ rhetoric and advances in individualisation (Pangbourne et al. 2010).
The MOBILATE study conducted a survey across 5 European countries of senior people’s mobility , and included some data on technology use and acceptance. At that time, 2005, the share of use of the technologies studied was low amongst the over 55s, but these older people’s experiences of common technologies like cash machines were quite positive, though public transport ticket dispensers were less well received, and commonly regarded as excessively complicated. It was noted that a high educational level, high income and good health were all factors that contributed to older adults being able to overcome barriers to use (Tacken et al. 2005).
As described in the introduction, older people are under considerable pressure to adopt new technologies across their lives: services as diverse as government, banking, insurance, transport ticketing, healthcare services and shopping are increasingly shifting to web-based and mobile interfaces, with physical branches and telephone call centres increasingly less available or frustrating to access. However, at the time of the MOBILATE study most people over the age of 55 were not habitual users of PCs in the workplace, and have thus had much less opportunity to become familiar with the conventions of human-computer interfaces. The spread of smartphones has introduced new conventions and affordances for those who adopt them.
New generations continuously enter the senior age brackets, and increasingly have familiarity with at least some ICTs. Nevertheless, adoption and acceptance cannot be taken for granted—many older people are suspicious of contactless and mobile payment methods for example, and are also more guarded (yet less skilled) when it comes to issues of personal data privacy and location tracking services. It is not clear whether this is a cohort effect or a reflection of some of the cognitive effects of ageing. However, if the technology adoption rate of mobile services matches that of the take-up of smartphones, internet and broadband amongst older people, then it is most likely a cohort effect that is fading—see, for example, recent statistics from the United States, where older adults up to 69 have similar rates of internet and broadband use as the general population, though smartphone adoption is more strongly linked to income (Anderson and Perrin 2017).
The newer interfaces, often with new business models or concepts such as multi-layer menu systems, are harder to adopt for older people than for younger people, whilst due at least in part to a general ‘slowing down’ of cognitive ability, lack of uptake is more likely to relate to an attitudinal reluctance to keep learning new things, or a view that there is really no need for novelty, unless the ICT supports hobbies or other interests that increase individual motivation to overcome the learning hurdles that everyone experiences. There are also practical difficulties for older people—eyesight increasingly becomes a factor in using smartphones and items with screens and keyboards. MOBILATE found that increasing age and being female were associated with lower levels of technology adoption , notwithstanding some interesting reversals, as women used ticket dispensing machines more than men. This is assumed to be because, as more frequent users of public transport , they have more knowledge of how to use public transport , including how to buy tickets. Nevertheless, MOBILATE’s data show that gender and age are important predictors for the use of new technology (Tacken et al. 2005, p. 131).
Older People and Technologies for Mobility
It is important to remember that with the exception of unaided walking ,Footnote 2 all our out-of-home mobility is facilitated by technologies of varying degrees of sophistication. To date, the technological innovation in transport with the largest impact has to be the emergence and rapid dominance of the internal combustion engine, particularly in how it has provided personal mobility to millions through the car. The unique features of automobiles have totally transformed the organisation of society wherever car ownership has taken hold. Because of ‘automobility’s exceptional power to remake time-space, especially because of its peculiar combination of flexibility and coercion’ (Urry 2004, p. 27), our societal preconceptions of mobility in older age are inevitably underpinned by the general expectation that the car is the main provider of personal mobility for most of our lives. The car also underpins the generally increased expectation of mobility as highlighted above. In other words the invention of the car totally reconfigured social practices , urban layout and the distribution of land uses, which helps to explain the great focus in the mobility and ageing literature on the impact of driving cessation as a significant event for older people, carrying with it a number of negative connotations and impacts in contexts where vital services are dislocated in time and space from homes (as touched on above).
Nevertheless, it is intuitive to expect that other transport technologies that support out-of-home mobility Footnote 3 will become a bigger issue in relation to an ageing population. At the same time, ICT innovation is having as rapid and profound an impact on the shape of transport provision as it is in healthcare. Yet as discussed above, these innovations tend to achieve a slower rate of uptake amongst older people than younger. What does this imply for utilising ICT in providing future mobility services for older people?
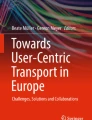
In a focus group study, Pangbourne et al. (2010) (Fig. 3.1) demonstrated that the concerns of older people in relation to interactions between transport, healthcare and ICT are personal (the need for services to address feelings of vulnerability, a perception of a loss of social contact where ICT is used, but recognition that ICT can support individualisation), that there are informational requirements (older people want to be consulted about changes to services, they want healthcare information online, and they want communication about bookings and transport to healthcare appointments). Associated with these perceptions is an awareness that accessibility (to real-time travel information, transport and appointment times not matching up, having online appointment booking facilities) is not assured, and that usability of interfaces need attention. These issues emerged through discussion that initially appeared to be about reliability of transport services, parking at hospitals, locations of healthcare facilities, and ICT (hardware and software) that they use.

Focus group findings regarding intersections between transport, health care and ICT raised by older people (Pangbourne et al. 2010, p. 322)
Against this background, discussion of the role of ICT technologies for supporting mobility amongst older people tends to be that which somehow compensates them for their ‘diminished’ life experience in relation to getting out and about. ICT aimed at older people is seen often seen as mitigation and adaptation rather than a positive development. However, there are now developments to support those with cognitive impairments to continue enjoying outdoor mobility by using GPS trackers (Kaspar et al. 2015), as it has been shown that outdoor mobility is a critical factor in healthy ageing. Careful use of ICT is only one factor: social practices , and design of the built environment (e.g. buildings with heavy external doors can ‘trap’ mobility -impaired people inside, rendering them dependent on another person to be able to get outside), also need age-friendly evolution (Rantanen 2013).
ICT, Transport and Future Developments in Mobility
Within the transport environment itself, ICT is developing quite rapidly in diverse ways. Within the public transport environment ICT is pervasive, characterised as delivering better management, greater safety and increased flexibility. It is also substituting for employees: information provision is increasingly via the internet through online automated systems and at boarding points with real-time passenger information systems. Ticket purchase is via ticket machines at stations both manned and unmanned. On metro systems, ticket gates and validation machines provide the ticket enforcement. Some transport services now don’t even need drivers (e.g. the London Docklands Railway, the Personal Rapid Transit systems that have been trialled in Masdar and at London Heathrow airport).
The loss of ‘eyes on the street’ in the transportation system, and the general perceptions of personal security on public transport , particularly for older people, is an issue which has attracted some attention in research. For example, Sochor (2013) has investigated whether Swedish older adults find a range of public transport ICTs reassuring (video surveillance in public transportation, real-time travel information, and a personal, pedestrian navigation system with public transportation information). Perceptions were neutral regarding privacy and positive in support a sense of assurance, especially for women, who are known to feel more vulnerable in certain mobility settings, though men were more interested in the ‘technology ’. Surprisingly, personal control over the ICT (in the case of a navigation system with information) did not enhance the sense of assurance. In a further development of this work, Sochor and Nikitas (2016) added evidence from Britain to a Swedish study of the technology perceptions of visually impaired people. They conclude that whilst the attitudes of older people are generally accepting, they are prosocial in considering the benefits rather than personal, as sometimes the technologies are perceived as ‘complicated’. They conclude that these technologies are only one element in a complex sociotechnical system that is challenging for meeting the needs of older people.
There are a number of vehicle developments that are sometimes portrayed as likely to be beneficial for older adults. The key innovation, which is not yet market ready, is the emergence of self-driving vehicles (SDV), also known as autonomous vehicles. Therefore, it is difficult to evaluate the likely outcomes for older people. On the face of it, SDV could be regarded as an assistive technology , and inevitably one that would have quite a radical restructuring impact on social practices and other transport modes (Shergold et al. 2015). Shergold (2016) also review what is currently known about the impacts of SDVs and driver assistance technologies, and conclude that the benefits of this group of technologies is likely to have particular benefits for older people at risk of losing independence as a result of driving cessation.
However, in order to ensure that any technology , including the built environment itself, is able to support the mobility and independence of older people, attention needs to be paid to design issues (e.g. I referred above to the particular difficulties posed by smartphone touch screens). In the next section, consideration is given to age-friendly design and policy .
Age-Friendly Design and Transport Policy
Rantanen (2013) described evocatively how the design choice of a heavy front door can impede an older person’s outdoor mobility (see above). At the larger scale, transport and the built environment is dictated by a complex web of urban and transport policies. Johnson et al. (2017) have reviewed national approaches to older adult’s transport needs in Europe. Drawing on their own literature review, and on the TRACY Project (2012) they identify 11 qualities of an age-friendly transport system (Affordability, Availability, Barrier-free, Comfortable, Comprehensible, Efficient, Friendly, Reliable, Safe, Secure and Transparent). Aguiar and Macário (2017) also highlight the need for mobility policy to be more focused on the needs of an older population, highlighting important infrastructure measures that may seem trivial, such as pavement improvements, that have very positive benefits for older people. In a similar vein, the GLIDE project in Singapore trialled technologies to provide longer crossing times for older or physically challenged pedestrians (Debnath et al. 2011). These age-friendly, active ageing initiatives and criteria are entirely compatible with the World Health Organization’s ‘age-friendly cities’ objective, which highlights that by means of inclusive design , all age groups benefit (WHO 2007). However, in Johnson et al’s (ibid) study, their findings suggest that the most consistent qualities that are addressed by government are safety, barrier freedom and affordability. They conclude that the emphasis placed on these qualities is due to their tangibility and relative ease of implementation rather than any objective assessment of likely benefit. The neglect of the softer intangibles has attracted some research attention (e.g. Hounsell et al. 2016; Grotenhuis et al. 2007 or O’Neill 2016), but has yet to gain much traction in implementation.
Conclusions
Whilst the technologies that are being advanced in both e-health and transport are exciting and could be of significant benefit to society, the predominant government and industry discourse carries a clear ‘technology optimism bias’ which colours thinking about the capabilities/benefits of all technological innovations, including ICTs. Of course for the industry, this comes from the fact that they are marketing their products. Governments, presumably, are marketing themselves as re-electable and wish to be perceived as forward thinking or facilitative of commerce. A lot of the ICT initiatives at the nexus of Smart Mobility and Smart Cities can only be implemented in cities that have high quality infrastructure already in place, and there are many areas (urban, peri-urban and rural in the both the Global North and Global South) where the telecommunications infrastructure is simply behind the curve, and where the most useful ICTs cannot yet be deployed, even quite basic real-time passenger information. This is a serious shortcoming that affects everyone, not only older people. In rural areas, where populations are predominantly older, there is clearly a significant issue that needs to be addressed, as many transport innovations will be unavailable or unaffordable in ‘unconnected’ areas.
As we have seen, Johnson et al.’s (2017) analysis suggests that both research and policy have thus far focused on objective and measurable qualities (safety, barrier freedom and affordability in particular), neglecting the softer, more subjective qualities of the lived experience of older people. Increasingly, research is showing that the subjective and context-related factors are very significant in suppressing the mobility of older people, whilst at the same time, getting out and about independently is increasingly understood as a crucial issue in supporting health and well-being.
Thus qualities such as security (in the sense that transport provision is perceived as secure, and addresses confidence issues that older people may have), friendliness and comfort should be more directly addressed. Significantly, Johnson et al. (2017) also talk of the single-mode specificity of most of the policy documents they evaluated. This neglects the need to join up transport policies to improve age-friendliness. For example, having policies which limit driving licences for older people are essential for safety reasons, but without providing alternatives with the right age-friendly qualities, those affected are doomed to profound and damaging immobility.
Policy and Research Recommendations
Society needs to ask critical questions—are mobility technology changes such as a wholesale transition to self-driving vehicles worth striving for or is remote service provision, including healthcare a better option? More probably there should be a blend of approaches, given the role that out-of-home mobility plays in maintaining healthy physical and mental outlooks at any age, though particularly in older age. The introduction of new technologies, whether transport or health -related, will shape future societies and the lived experience of older people through subtle impacts on social practices . However, it is good to remember the words of the World Health Organization, in its age-friendly cities guidance document:
Because active ageing is a lifelong process, an age-friendly city is not just “elderly friendly”. Barrier-free buildings and streets enhance the mobility and independence of people with disabilities, young as well as old. Secure neighbourhoods allow children, younger women and older people to venture outside in confidence to participate in physically active leisure and in social activities. Families experience less stress when their older members have the community support and health services they need. The whole community benefits from the participation of older people in volunteer or paid work. Finally, the local economy profits from the patronage of older adult consumers. The operative word in age-friendly social and physical urban settings is enablement. (WHO 2007, p. 6)
Notes
- 1.
- 2.
Some would contend that shoes are also technology and certainly orthotics can be added to footwear as assistive technologies .
- 3.
It should be noted that most of the gerontology and health literature conceptualise ‘mobility ’ as an embodied capacity, i.e. the ability to walk, and perform independent actions, within the home, rather than as an act of travel, and mobility assistive technologies are wheelchairs, walkers, scooters, etc.
References
Aguiar, B., and R. Macário. (2017). The Need for an Elderly Centred Mobility Policy. Transportation Research Procedia 25: 4355–4369.
Alba, D. 2016. It’s Official: The Smartphone Market Has Gone Flat. Wired. https://www.wired.com/2016/04/official-smartphone-market-gone-flat/. Accessed 31 October 2017.
Alsnih, R., and D.A. Hensher. 2003. The Mobility and Accessibility Expectations of Seniors in an Aging Population. Transportation Research Part A: Policy and Practice 37 (10): 903–916.
Anderson, M., and A. Perrin. 2017. Technology Use Among Seniors. Pew Research Center. http://www.pewinternet.org/2017/05/17/technology-use-among-seniors/. Accessed 6 September 2017.
Banister, D., and A. Bowling. 2004. Quality of Life for the Elderly: The Transport Dimension. Transport Policy 11: 105–115.
Boschmann, E.E., and S.A. Brady. 2013. Travel Behaviors, Sustainable Mobility, and Transit-Oriented Developments: A Travel Counts Analysis of Older Adults in the Denver, Colorado Metropolitan Area. Journal of Transport Geography 33: 1–11.
Broome, K., K. McKenna, J. Fleming, and L. Worrall. 2009. Bus Use and Older People: A Literature Review Applying the Person–Environment–Occupation Model in Macro Practice. Scandinavian Journal of Occupational Therapy 16 (1): 3–12.
Broome, K., E. Nalder, L. Worrall, and D. Boldy. 2010. Age-Friendly Buses? A Comparison of Reported Barriers and Facilitators to Bus Use for Younger and Older Adults. Australasian Journal on Ageing 29 (1): 33–38.
Debnath, A.K., M. Haque, and H. Chin. 2011. Sustainable Urban Transport: Smar Technology Initiatives in Singapore. Transportation Research Record 2243: 38–45.
Engels, B., and G.J. Liu. 2011. Social Exclusion, Location and Transport Disadvantage Amongst Non-Driving Seniors in a Melbourne Municipality, Australia. Journal of Transport Geography 19 (4): 984–996.
Gilhooly, M., K. Hamilton, M. O’Neill, J. Gow, N. Webster, F. Pike, and D. Bainbridge. 2002. Transport and Ageing: Extending Quality of Life for Older People via Public and Private Transport.
Gregor, P., A.F. Newell, and M. Zajicek. 2002. Designing for Dynamic Diversity: Interfaces for Older People. ASSETS ’02 Proceedings of the Fifth International ACM Conference on Assistive Technologies, 151–156.
Grotenhuis, J.-W., B.W. Wigmans, and P. Rietveld. 2007. The Desired Quality of Integrated Multimodal Travel Information in Public Transport: Customer Needs for Time and Effort Savings. Transport Policy 14: 27–38.
Haustein, S. 2012. Mobility Behavior of the Elderly: An Attitude-Based Segmentation Approach for a Heterogeneous Target Group. Transportation 39 (6): 1079–1103.
Hounsell, N.B., B.P. Shrestha, M. McDonald, and A. Wong. 2016. Open Data and the Needs of Older People for Public Transport Information. Transport Research Procedia 14: 4334–4343.
Johnson, R., J. Shaw, J. Berding, M. Gather, and M. Rebstock. 2017. European National Government Approaches to Older People’s Transport System Needs. Transport Policy 59: 17–27.
Kaiser, H.J. 2009. Mobility in Old Age: Beyond the Transportation Perspective. Journal of Applied Gerontology 28: 411–418.
Kaspar, R., F. Oswald, H.W. Wahl, E. Voss, and M. Wettstein. 2015. Daily Mood and Out-of-Home Mobility in Older Adults: Does Cognitive Impairment Matter? Journal of Applied Gerontology 34: 26–47.
Lowsky, D.J., S.J. Olshansky, J. Bhattacharya, and D.P. Goldman. 2014. Heterogeneity in Healthy Aging. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 69 (6): 640–649.
Lyons, E.J., M.C. Swartz, Z.H. Lewis, E. Martinez, and K. Jennings. 2017. Feasibility and Acceptability of a Wearable Technology Physical Activity Intervention with Telephone Counseling for Mid-Aged and Older Adults: A Randomized Controlled Pilot Trial. JMIR mHealth and uHealth 5 (3): Online only.
Malasinghe, L.P., N. Ramzan, and K.J. Dahal. 2017. Remote Patient Monitoring: A Comprehensive Study. Journal of Ambient Intelligence and Humanized Computing, 1–20. https://doi.org/10.1007/s12652-017-0598-x.
Marottoli, R.A., C.F.M. de Leon, T.A. Glass, C.S. Williams, L.M. Cooney Jr., L.F. Berkman, and M.E. Tinetti. 1997. Driving Cessation and Increased Depressive Symptoms: Prospective Evidence from the New Haven EPESE. Established Populations for Epidemiological Studies of the Elderly. Journal of the American Geriatrics Society 45: 202–206.
Marottoli, R.A., C.F.M. de Leon, T.A. Glass, C.S. Williams, L.M. Cooney Jr., and L.F. Berkman. 2000. Consequences of Driving Cessation Decreased Out-of-Home Activity Levels. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 55 (6): S334–S340.
Metz, D.H. 2000. Mobility of Older People and Their Quality of Life. Transport Policy 7 (2): 149–152.
Mi, N., L.A. Cavuoto, K. Benson, T. Smith-Jackson, and M.A. Nussbaum. 2014. A Heuristic Checklist for an Accessible Smartphone Interface Design. Universal Access in the Information Society 13: 351–365.
Mokhtarian, P., I. Salamon, and M. Singer. 2015. What Moves Us? An Interdisciplinary Exploration of the Reasons for Traveling. Transport Reviews 35: 250–274.
Mollenkopf, H. 2005. Enhancing Mobility in Later Life: Personal Coping, Environmental Resources and Technical Support; The Out-of-Home Mobility of Older Adults in Urban and Rural Regions of Five European Countries, vol. 17. Amsterdam, The Netherlands: IOS Press.
Mollenkopf, H., A. Heiber, and H.W. Wahl. 2017. Continuity and Change in Older Adults’ Out-of-Home Mobility Over Ten Years: A Qualitative-Quantitative Approach. In Knowledge and Action, Knowledge and Space, ed. P. Meusburger et al., Chapter 15, 267–289.
Mollenkopf, H., F. Marcellini, I. Ruoppila, Z. Széman, M. Tacken, and H.W. Wahl. 2004. Social and Behavioural Science Perspectives on Out-of-Home Mobility in Later Life: Findings from the European Project MOBILATE. European Journal of Ageing 1 (1): 45–53.
Musselwhite, C.B.A. 2011. Successfully Giving Up Driving for Older People.
Nordbakke, S., and T. Schwanen. 2015. Transport, Unmet Activity Needs and Wellbeing in Later Life: Exploring the Links. Transportation 42: 1129–1151.
O’Brien, T., M. Troutman-Jordan, D. Hathaway, S. Armstrong, and M. Moore. 2015. Acceptability of Wristband Activity Trackers Among Community Dwelling Older Adults. Geriatr Nurs. 36 (2 Suppl.): S21–S25.
O’Hanlon, S., A. Bourke, and V. Power. 2012. E-Health for Older Adults. Engaging Older Adults with Modern Technology: Internet Use and Information Access Needs: Internet Use and Information Access Needs, 229.
O’Neill, D. 2016. Towards an Understanding of the Full Spectrum of Travel-Related Injuries Among Older People. Journal of Transport and Health 3: 21–25.
Pangbourne, K., P.T. Aditjandra, and J.D. Nelson. 2010. New Technology and Quality of Life for Older People: Exploring Health and Transport Dimensions in the UK context. IET Intelligent Transport Systems 4 (4): 318–327.
Pew Research Center. 2017. Mobile Fact Sheet. http://www.pewinternet.org/fact-sheet/mobile/. Accessed 31 October 2017.
Rantanen, T. 2013. Promoting Mobility in Older People. Journal of Preventive Medicine and Public Health 46 (Suppl. 1): S50–S54.
Reardon, L., and S. Abdallah. 2013. Well-Being and Transport: Taking Stock and Looking Forward. Transport Reviews 33 (6): 634–657.
Rosenbloom, S. 2004. Mobility of the Elderly: Good News and Bad News. In Transportation in an Aging Society: A Decade of Experience, Technical Papers and Reports from a Conference, November 7–9, 1999. Bethesda, Maryland: Transportation Research Board.
Selwyn, N., S. Gorard, J. Furlong, and L. Madden. 2003. Older Adults’ Use of Information and Communications Technology in Everyday Life. Ageing & Society 23 (05): 561–582.
Shergold, I., G. Lyons, and C. Hubers. 2015. Future Mobility in an Ageing Society: Where are We Heading? Journal of Transport and Health 2: 86–94.
Shergold, I., M. Wilson, and G. Parkhurst. 2016. The Mobility of Older People, and the Future Role of Connected Autonomous Vehicles. Project Report. Centre for Transport and Society, University of the West of England, Bristol, Bristol. http://eprints.uwe.ac.uk/31998. Accessed 31 October 2017.
Simonsick, E.M., J.M. Guralnik, S. Volpato, J. Balfour, and L.P. Fried. 2005. Just Get Out the Door! Importance of Walking Outside the Home for Maintaining Mobility: Findings from the Women’s Health and Aging Study. Journal of the American Geriatrics Society 53 (2): 198–203.
Sixsmith, A. 2013. Technology and the Challenge of Aging. In Technologies for Active Aging, vol. 9, ed. A. Sixsmith and G. Gutman, 7–26. New York: Springer Science and Business Media.
Smith, A. 2014. Older Adults and Technology Use, Pew Research Center, Report 202.419.4500. http://www.pewinternet.org/2014/04/03/older-adults-and-technology-use/. Accessed 30 October 2017.
Sochor, J. 2013. The Reassuring Affects of ICT in Public Transportation: The Perspectives of Older Adults. Gerontechnology.
Sochor, J., and A. Nikitas. 2016. Vulnerable Users’ Perceptions of Transport Technologies. In Proceedings of the Institution of Civil Engineers, Urban Design and Planning.
Souders, D.J., and N. Charness. 2014. Travel Safety and Technology Adoption by Elderly Populations.
Spinney, J.E., D.M. Scott, and K.B. Newbold. 2009. Transport Mobility Benefits and Quality of Life: A Time-Use Perspective of Elderly Canadians. Transport Policy 16 (1): 1–11.
Tacken, M., F. Marcellini, H. Mollenkopf, I. Ruoppila, and Z. Szeman. 2005. Use and Acceptance of New Technology by Older People. Findings of the International MOBILATE Survey: ‘Enhancing Mobility in Later Life’. Gerontechnology 3 (3): 126–137.
TRACY Project. 2012. Work Package 2: Determining the State of the Art. Transportation Research Group (2006) ‘Virtual mobility’. Available at http://www.trg.soton.ac.uk/vm/m-r.htm. Accessed 12 October 2006.
United Nations. 2015. World Population Ageing. http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf. Accessed 31 October 2017.
Urry, J. 2004. The ‘System’ of Automobility. Theory, Culture and Society 21: 25–39.
World Health Organisation. 2002. Active Ageing: A Policy Framework. Geneva: Switzerland.
World Health Organisation. 2007. Global Age-Friendly Cities: A Guide. Geneva: Switzerland.
Zeitler, E., and L. Buys. 2015. Mobility and Out-of-Home Activities of Older People Living in Suburban Environments: ‘Because I’m A Driver, I Don’t Have A Problem’. Ageing & Society 35 (4): 785–808.
Ziegler, F., and T. Schwanen. 2011. ‘I Like to Go Out to Be Energized by Different People’: An Exploratory Analysis of Mobility and Wellbeing in Later Life. Ageing & Society 31 (5): 758.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 The Author(s)
About this chapter

Cite this chapter
Pangbourne, K. (2018). Mobility and Ageing: A Review of Interactions Between Transport and Technology from the Perspective of Older People. In: Curl, A., Musselwhite, C. (eds) Geographies of Transport and Ageing. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-319-76360-6_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-76360-6_3
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-319-76359-0
Online ISBN: 978-3-319-76360-6
eBook Packages: Social SciencesSocial Sciences (R0)