
Abstract
The insula was for a long time considered as one of the most challenging areas of the brain. This is mainly related to its location, deep and medial to the frontoparietal, temporal, and fronto-orbital opercula. Another difficulty is the content of the lateral fossa, located between the insula and the opercula, which contains the trunks, stem, arteries, and cortical branches of the insular (M2) and opercular (M3) segments of the middle cerebral artery (MCA). Finally, the insula is surrounded by several white matter tracts and cortical structures having important functional roles, especially for language in the dominant hemisphere; the insula is indeed located between a dorsal phonological stream, centered by the arcuate fasciculus and lateral to the posterior insula, and a ventral semantic system, medial to the ventral aspect of the insula and centered by the inferior fronto-occipital fasciculus (IFOF). This chapter reviews some of these surgically relevant anatomical relationships.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Insula
- Anatomy
- Opercula
- Inferior fronto-occipital fasciculus
- Uncinate fasciculus
- Arcuate fasciculus
- Middle cerebral artery
2 Sulco-Gyral Relationships [1,2,3]
The opercula (Latin, meaning “little lid”) are made of the inferior border of the frontal and parietal lobes and the superior border of the temporal lobe. They cover and hide the insula, deeply located in the lateral fissure.
The lateral fissure is subdivided into three segments (Fig. 3.1): the middle one parallels the main axis of the temporal lobe and separates the opercular part of the inferior frontal and subcentral gyri (frontoparietal operculum) from the superior temporal gyrus (temporal operculum); the anterior segment of the lateral fissure anteriorly splits into a vertical and a horizontal ramus; finally the posterior segment of the lateral fissure ascends posterodorsally within the anterior part of the inferior parietal lobule (supramarginal gyrus).

Two steps of dissection of a left human hemisphere, lateral views. (a) Cerebral cortex after removal of the arachnoid, superficial vessels, and pia mater. The insula is hidden by the opercula. The lateral compartment of the lateral fissure is subdivided into three segments: middle (Lat Fissure Mid seg) slightly ascending posteriorly, between the temporal and frontal opercula; posterior (Lat Fissure Post seg), ascending and surrounded by the supramarginal gyrus (P2SM G); and anterior (Lat Fissure Ant seg), which divides into a horizontal and a vertical ramus limiting the pars triangularis (F3tr) from the pars opercularis (F3op) and orbitalis (F3or) of the inferior frontal gyrus. The frontoparietal operculum is made of F3tr, F3op, subcentral gyrus (SubC G), and part of P2SM G located dorsal and anterior to the Lat Fissure Post seg. The temporal operculum includes the remaining part of P2SM G ventral and posterior to the Lat Fissure Post Seg, continued by the superior temporal gyrus (T1). The fronto-orbital operculum is smaller and reunites F3or and the posterior part of the lateral orbital gyrus (Lat Orb G). The circular and central sulci of the insula (see (b) for legends) are projected in yellow onto the cortical surface, showing that F3tr points toward the anterior insula. The junction point of Lat Fissure Mid seg and Lat Fissure Post seg projects at the level of the posterosuperior corner of the insula. Finally, the central sulcus of the insula has about the same orientation as the central sulcus (Cent S) but may begin a few millimeters anterior or posterior to its ventral tip. (b) Dissection showing the insula after the opercula were removed. The insula has a triangular limit, the circular sulcus of the insula, made of anterior (Ant Circul S insula), superior (Sup Circul S insula), and inferior (Inf Circul S insula) segments. The limen insulae is located at the junction of Ant Circul S insula and Inf Circul S insula. The central sulcus of the insula (Central S Insula) subdivides the insula in long insular gyri (Long Insul G) posteriorly, and short insular gyri (Short Insul G) anteriorly. The lateral fissure, inferior precentral-inferior frontal sulci, the superior temporal sulcus, and central sulcus are projected in orange onto the insula to show that the two ventral thirds of the insula are hidden by the temporal operculum. Ant SubC S anterior subcentral sulcus, F1 superior frontal gyrus, F2 middle frontal gyrus, Inf Front S inferior frontal sulcus, Inf Precent S inferior precentral sulcus, Insul apex insular apex, Intrapariet S intraparietal sulcus, P1 superior parietal lobule, P2 Ang G sngular gyrus (posterior part of the inferior parietal lobule), Post SubC S posterior subcentral sulcus, Postcent G postcentral gyrus, Postcent S postcentral sulcus, Precent G precentral gyrus, Sup Front S superior frontal sulcus, Sup Precent S superior precentral sulcus, Sup Temp S superior temporal sulcus, T2 middle temporal gyrus, and T3 inferior temporal gyrus
The frontoparietal operculum is bordered anteriorly by the horizontal ramus of the lateral fissure and posteriorly by its posterior ascending segment. It includes (Fig. 3.1), from anterior to posterior [1, 4,5,6], the triangular and opercular parts of the inferior frontal gyrus and the subcentral gyrus.
-
The inferior frontal gyrus (or F3) is limited ventrally by the lateral fissure, posteriorly by the inferior precentral and anterior subcentral sulci, and dorsally by the inferior frontal sulcus. The inferior precentral sulcus—sometimes fused with its superior homologue—runs parallel and anterior to the central sulcus. It more or less reaches the lateral fissure and is perpendicularly connected to the inferior frontal sulcus. This one runs anteriorly, parallel to the middle segment of the lateral fissure, and finally curves anteroventrally to become the lateral orbital sulcus. The inferior frontal gyrus is subdivided by both rami of the anterior segments of the lateral fissure: its triangular part is located between them, whereas the opercular part is posterior to the vertical ramus and the orbital part is anteroventral to the horizontal ramus.
-
The subcentral gyrus is the inferior frontoparietal pli de passage connecting the pre- and postcentral gyri. It curves around the ventral tip of the central sulcus and usually separates its inferior tip from the lateral fissure. The subcentral gyrus is thus located just posterior to the inferior frontal gyrus, from which it is limited by the anterior subcentral sulcus, a small notch originating from the lateral fissure. Similarly the subcentral gyrus is posteriorly limited from the supramarginal gyrus by the posterior subcentral sulcus. The supramarginal gyrus is the anterior part of the inferior parietal lobule (P2), its posterior part being the angular gyrus; the supramarginal gyrus curves around the posterior segment of the lateral fissure and is thus continuous with the subcentral gyrus dorsally and the superior temporal gyrus ventrally.
The fronto-orbital operculum covers the anterior part of the insula and is sometimes included in the frontoparietal operculum. It is made of the orbital part of the inferior frontal gyrus (ventral to the horizontal ramus of the anterior segment of the lateral fissure) and the posterior part of the lateral orbital gyrus.
The superior temporal gyrus (T1) forms the temporal operculum. It is bordered by the lateral fissure dorsally and by the superior temporal sulcus ventrally. The latter is a deep, continuous sulcus, which slightly ascends posteriorly and often splits into two posterior rami, one continuing its initial course and the second having a more ascending trajectory. These posterior rami of the superior temporal sulcus are surrounded by the angular gyrus, which is the posterior part of the inferior parietal lobule (P2).
The superior aspect of the superior temporal gyrus (T1) is subdivided into three distinct areas by the transverse temporal sulcus. The latter is posteromedially oriented and joins the lateral fissure, at the superficial aspect of the brain, to the circular sulcus of the insula, close to the junction point of its superior and inferior segments (see below). The planum temporale, located posterior to the transverse temporal sulcus, is the most posterior part of the superior aspect of the superior temporal gyrus. It is a flat area, posteriorly continuous with the anterior part of the supramarginal gyrus. The temporal transverse gyrus, containing the primary auditory area, is a strip of cortex having sometimes a double pattern; it follows the same posteromedial course as the temporal transverse sulcus, which is its posterior limit. Finally, the superior aspect of the superior temporal gyrus ends anteriorly as a second flat area, the planum polare, reaching the temporal pole.
Each of the opercula has three aspects (Fig. 3.2): lateral, visible from a surface inspection of the brain, dorsal (for the temporal operculum) or ventral (for the frontoparietal operculum), and medial, facing the insula. The junction point between the insula and the medial aspect of the opercula is the circular sulcus of the insula (Fig. 3.1). It is a triangle made of three segments that border the insula: superior, limiting the insula from the frontoparietal operculum; inferior, between the insula and the temporal operculum; and anterior, between the insula and the fronto-orbital operculum. In other words, the lateral fissure, limiting the frontoparietal operculum from the temporal one, appears as a straight cleft on a coronal slice (Fig. 3.2), with a latero-medial direction (opercular cleft); it medially splits into two branches, the insular clefts [7], oriented dorsomedially and ventromedially, limiting the medial aspect of the opercula from the insula. Taken together, the opercular and insular clefts have the shape of a “Y” or a “T” lying on its side on a coronal section. They limit a space, the lateral fossa, located between the medial aspects of the opercula laterally and the insula medially. The lateral fossa opens laterally through the lateral fissure. In the dorso-ventral direction, the fossa is wider at its anterior part, since the height of the insula decreases posteriorly.

Schematic coronal slice at the level of the hippocampal uncus. The lateral fossa (Lat fossa) is the space bordered by the insula medially and the opercula laterally, which contains branches of the middle cerebral artery. It is continued by the lateral segment of the lateral fissure (Lat fissure), which opens at the superficial aspect of the brain. The space located between the opercula is also known as the opercular cleft, whereas the ones located between the opercula and insula are known as the insular clefts. On this slice, the frontal and temporal opercula are made of the opercular part of the inferior frontal gyrus (F3op), and the superior temporal gyrus (T1), respectively. They are limited from the insula by the superior (SupCircul S Insula) and inferior circular sulci of the insula (Inf Circul S Insula). Several structures are found deep to the insula, from lateral to medial: the extreme capsule (Extr caps), the claustrum, the external capsule (Exter caps), the putamen (Pu), the lateral (Gpl) and medial (Gpm) parts of the globus pallidus and the internal capsule (Int caps). The Extr caps and Exter caps fuse at the inferior limit of the claustrum to become the temporal stem (T stem), located between the inferior circular sulcus of the insula (Inf Circul S Insula) and the temporal horn of the lateral ventricle (th). The three capsules and callosal fibers fuse at the superior aspect of the putamen and claustrum to form the corona radiata, making the Int caps more vulnerable at the superior aspect of the insula. Amyg Amygdala, Cn Caudate nucleus (body), F1 Superior frontal gyrus, F: Middle frontal gyrus, Hip unc Hippocampal uncus, Inf Front S Inferior frontal sulcus, Sup Temp S Superior temporal sulcus, T2 Middle temporal gyrus, T3 Inferior temporal gyrus, T4 Fusiform gyrus, T5 Parahippocampal gyrus, Thal Thalamus
3 White Matter Relationships
Several white matter tracts surround the insula (Fig. 3.3): one is dorsolateral and two are ventromedial (inferior fronto-occipital (IFOF) and uncinate (UF) fasciculi.

Step-by-step Klingler’s dissection of the peri-insular white matter tracts. The red arrows point the approximate level of dissection on a coronal schematic slice. (a) Lateral segments of the arcuate fasciculus. After removing the cortex and short association “U” fibers, the two most superficial segments of the arcuate fasciculus appear: the vertical posterior segment (SLF vert) is posterior to the insula and joins the supramarginal gyrus to the posterior part of the superior and middle temporal gyri; the horizontal anterior segment (SLF hor), dorsal to the insula, joins the supramarginal gyrus and posterior part of the superior temporal gyrus, to the subcentral gyrus. Due to the partial removal of the frontoparietal (Fr-Par operc), temporal (Temp operc) and fronto-orbital (Fr-Orb operc) opercula, the insula appears. (b) Deep long segment of the SLF, or arcuate fasciculus (SLF arc). After the superficial segments of the SLF were removed, its deep or arcuate segment appears. It curves around the posterior tip of the insula and joins the superior, middle and inferior temporal gyri to the ventral precentral area, pars opercularis of the inferior frontal gyrus and posterior part of the middle frontal gyrus. The insula clearly appears, limited from the opercula by its circular sulcus (Circul S insula), and subdivided by the central sulcus of the insula (Central S insula) into long (Long insul G) and short insular (Short insul G) gyri. (c) Extreme capsule. The extreme capsule appears after the insular cortex is removed and contains the superficial insulo-insular “U” fibers. Its dorsal part (Extr caps dorsal) also includes insulo-opercular projection fibers, having a radiating pattern, whereas its ventral part (Extr caps ventral) is made of the trunks of the uncinate (UF) and Inferior Fronto-occipital fasciculi (IFOF). (d) Claustrum and external capsule. The claustrum is subdivided into a denser dorsal part (Claustrum dorsal), medial to the dorsal Extr caps, and a ventral part (Claustrum ventral) made of small islands of gray matter intermingled with the trunks of the IFOF and UF. The ventral part of the external capsule (Exter caps ventral) is continuous with Extr caps ventral and is made of the trunks of the IFOF and UF. Its dorsal part (Exter caps dorsal) is made of radiate claustro-cortical fibers. The putamen (Pu) appears just medial to Exter caps dorsal after a few fibers are removed. (d) Putamen (Pu). The Pu appears after removing the Exter caps. (e) The uncinate fasciculus (UF). The UF runs ventral within the extreme and external capsules and connects the anterior portion of the three temporal gyri, anterior to the amygdala, to the gyrus rectus, orbital cortex and subcallosal area. The trunk of the IFOF is dorsal to the UF; it connects the frontal to the parieto-occipital lobes. Dorsal to the putamen, the extreme, external and internal capsule fuse to form the corona radiata. (f) Internal capsule (Int caps). The Pu and globus pallidus are removed and the Int caps appears medial to them. It is continued dorsally by the corona radiata and posteriorly by the stratum sagittale (SS). The SS may be regarded as the equivalent of the corona radiata for the temporal and occipital area and contains fibers of the sublentiform portion of the internal capsule (including optic and auditory radiations), fibers of the anterior commissure, and fibers of the IFOF.
The SLF turns around the posterior part of the insula to connect the frontoparietal and temporal opercula [8,9,10]. It includes two superficial components (anterior or horizontal and posterior or vertical) and a deep one (arcuate fasciculus). The anterior horizontal segment is dorsal and lateral to the insula, just medial to the short association U-fibers of the frontoparietal operculum. It connects the supramarginal gyrus and posterior part of the superior temporal gyrus to the subcentral gyrus. The posterior vertical segment has weaker relationships to the insula: it is located posterior to the insula and is also superficial, just medial to the short U-fibers. It connects the supramarginal gyrus and posterior part of the middle and superior temporal gyri. Finally, the deep or arcuate segment is medial to the two previous ones and connects the posterior part of the superior, but also middle and inferior temporal gyri to the ventral precentral area, to the pars opercularis of the inferior frontal gyrus, and to the posterior part of the middle frontal gyrus. It is thus C-shaped and curves around the posterior angle of the insula, limited by the intersection of the superior and inferior segments of the circular sulcus of the insula.
The white matter located medial to the insula is organized in three capsules (extreme, external, and internal) separated by gray matter (claustrum and lenticular nucleus).
-
The extreme capsule is located just medial to the insular cortex. It may be subdivided into dorsal and ventral components. The dorsal extreme capsule contains short insulo-insular and long insulo-opercular association fibers that will be described in the chapter dedicated to insular projections. The ventral extreme capsule contains the trunk of the UF and IFOF [5, 11], a densely packed group of fibers having a global anteroposterior direction.
-
The claustrum is a thin layer of gray matter lying between the extreme (laterally) and external (medially) capsules. Its dorsal part is compact, whereas its ventral part is made of small islands of gray matter intermingled with the fibers of the trunk of the IFOF and UF.
-
The external capsule, which is medial to the claustrum, is also subdivided into dorsal and ventral parts: the dorsal external capsule contains radiate claustro-cortical fibers, whereas the trunk of the UF and IFOF forms the ventral external capsule.
-
The lenticular nucleus is located medial to the external capsule and is triangular on a coronal slice: its lateral base is formed by the putamen, medially continued by the lateral and medial parts of the pallidum.
-
Finally, the internal capsule lies medial to the lenticular nucleus and follows a ventromedial direction to reach the mesencephalon. It is subdivided into anterior and posterior limbs joined by a genu [12]. The anterior limb, located between the caudate and lenticular nuclei (lenticulo-caudate portion), is anterolaterally oriented on a horizontal slice. The fibers of the posterior limb of the internal capsule are fanning between the thalamus and caudate nucleus. Due to the rotation of the caudate nucleus around the thalamus, these fibers have a radiate orientation: some are mainly running dorsally and appear above the putamen (lenticulo-thalamic portion), some are posteriorly oriented (retrolentiform portion), and some are running ventrally, between the lenticular nucleus and the tail of the caudate nucleus (sublentiform portions). Fibers of the corticospinal tract run in the posterior limb of the internal capsule and project medial to the long insular gyri, whereas the corticonuclear tract, located in the genu, runs medial to the posterior short insular gyrus [13].
The internal, external, and extreme capsules and callosal fibers fuse dorsal to the superior limit of the claustrum and putamen to form the corona radiata. Similarly, the stratum sagittale, which may be regarded as the equivalent of the corona radiata for the temporal and occipital area, contains fibers of the sublentiform portion of the internal capsule (including optic and auditory radiations), fibers of the anterior commissure, and fibers of the IFOF. The distinction of these different contingents of fibers during dissection is a matter of debate in the anatomical literature; some authors are describing each of these fasciculi separately [9, 14, 15], while others are claiming that their fibers are so intermingled that any individual dissection is impossible, the stratum sagittale being only described as a whole [12].
The anteroventral part of the insula is in close relationships with the trunks of the UF and IFOF [5, 11], which occupy the ventral part of the extreme and external capsules. IFOF and UF are both made of two fans connected by a trunk.
-
The IFOF joins the frontal to the parieto-occipital lobes and was described as made of two layers [15, 16]; its superficial dorsal one joins the inferior frontal gyrus (pars opercular, triangular, and orbicular) to the superior parietal lobule and superior and middle occipital gyri. Its deep ventral layer runs from the orbital gyri, the middle frontal gyrus, and the frontal pole to the inferior occipital gyrus and ventral aspect of the middle occipital gyrus and temporobasal cortex.
-
The UF trunk is located ventrolateral to the IFOF trunk. The temporal portion of the UF fans in the anterior portion of the three temporal gyri, anterior to the amygdala; its frontal part reaches the gyrus rectus, orbital cortex, and subcallosal area [17].
Trunks of both the UF and IFOF extend from the external and extreme capsules to the temporal stem (Fig. 3.4). The latter is the white matter connecting the temporal lobe to the rest of the brain, between the inferior circular sulcus of the insula and the temporal horn of the lateral ventricle [17, 18]. It extends anteroposteriorly from the coronal plane of the amygdala to that one of the lateral geniculate body [18] and is continuous on a coronal section with the ventral part of the external and extreme capsule. It contains the UF and IFOF trunk anteriorly and the anterior commissure and optic radiations posteriorly [17,18,19]. The anterior commissure has a ventrolateral course from the midline and crosses the inferior limit of the insula to enter the temporal lobe via the temporal stem [19].

Peri-insular white matter tracts. White matter tracts obtained from the dissection using Klingler’s method were scanned at each step of dissection using a 3D scanner laser, 3D-reconstructed and ported into the reference space of the dissected specimen postmortem MRI (see [33] for details). The figure represents ex vivo MRI coronal slices of a left hemisphere, from the anterior insula (A) to a slice just retroinsular (D). Main peri-insular tracts are superimposed in color onto these MRI images: the horizontal segment of the superior longitudinal fasciculus (SLF-Hor, green) is located dorsal and lateral to the insula; the vertical segment of the same fasciculus (SLF-Vert, yellow) is posterior to the insula; the deep segment of the SFL, or arcuate fasciculus (SLF-AF, red) turns around the posterior insula to extend into the posterior temporal and ventral frontal lobes; the uncinate (UF, purple) and inferior fronto-occipital fasciculi (IFOF, light blue) trunks are located in the ventral external and extreme capsules. ILF Inferior longitudinal fasciculus (dark blue)
4 Vascular Relationships
The lateral fossa is the space located between the insula medially and the medial aspect of the opercula laterally. It is continued by the lateral part (or operculo-insular, [5]) and basal part (or stem [5]) of the lateral fissure: the lateral part of the lateral fissure was previously described and corresponds to the opening of the lateral fossa at the surface of the brain; the basal aspect of the lateral fissure is the cleft located between the ventral aspects of the frontal and temporal lobes; it runs from the limen insulae, where it laterally communicates with the lateral fossa, to the anterior perforated space, located medially.
Ventral to the anterior perforated space and lateral to the optic chiasm (Fig. 3.5), the internal carotid artery bifurcates into the anterior (ACA) and middle cerebral arteries (MCA), the latter being about 4 mm in diameter, roughly twice that of the ACA [20].
-
The M1 or sphenoidal segment of the MCA runs laterally, parallel, and posterior to the sphenoidal ridge. It is located in the basal part of the lateral fissure and reaches the limen insulae. It divides into two (78% of hemispheres), three (12%), or multiple (10%) trunks. It is therefore described as made of pre- and post-bifurcation segments [20], which continue their course parallel to each other. The respective size of these trunks is variable, and, in case of bifurcation, equivalent trunks are observed in about 2 out of 8 hemispheres, whereas superior dominant (3 out of 8) or inferior dominant (3 out of 8) patterns are more common [20]. The M1 segment perforators, the anterolateral central (or anterolateral lenticulostriate) arteries, mainly originate from the pre-bifurcation segment of M1 and ascend to reach the anterior perforated space. Depending on their origin, they are subdivided into lateral, medial, and sometimes intermediate groups. The lateral and intermediate groups run through the putamen to vascularize the head and body of the caudate and superior part of the internal capsule. The medial group vascularizes part of the globus pallidus, anterior limb of the internal capsule, and head of the caudate [20].
-
At the level of the limen insulae, the MCA turns posterodorsally, with an angle of approximately 90°, to enter the lateral fossa (Fig. 3.6). This sharp angle, or genu, clearly visible on a frontal angiogram, is the limit between the M1-sphenoidal and M2-insular segments of the MCA. The trunks of the MCA divide here in a mean of eight stem arteries [5,6,7,8,9,10,11] fanning at the surface of the insula [7]. These stem arteries divide into two or more cortical arteries that reach the circular sulcus of the insula, considered as the distal limit of the M2 insular segment of the MCA. This division of the stem arteries in cortical arteries usually occurs before or at the level of the circular sulcus of the insula [7, 20]. Due to the shape of the insula, the M2 segment has a global triangular distribution, visible on lateral angiograms. Most of the arteries vascularizing the insula originate from the M2 segment [13]; the antero-dorsal part of the insula (short insular, accessory and transverse gyri, anterior circular sulcus, apex) is mainly vascularized by the superior trunk of the MCA and its branches; the posteroventral insula (posterior long insular gyrus, limen) is supplied by the inferior trunk and branches of the MCA; the central part of the insula (central sulcus of the insula and anterior long insular gyrus) gets a double vascularization from both trunks. Finally early branches, originating from M1 before its bifurcation, can supply every part of the insula except its central sulcus. A detailed description of the arterial supply of each insular gyrus is given in [7], other descriptions with a more extensive territory for the superior trunk being proposed by other authors [6, 13]. Most insular arteries are short [6, 21] and only supply the insular cortex and underlying extreme capsule; 10% are medium sized and vascularize also the claustrum and external capsule; finally 3–5% of insular arteries are long and reach deeper structures, as the corona radiata [13]. Three to eleven such long insular perforators are found per hemisphere; in about 80%, they originate from branches of the superior trunk at the level of M2 segment (51.6%), M2–M3 junction (37.4%), or proximal M3 (11%) [13]. These long perforators enter the dorsal part of the insula, close to the superior circular sulcus: at the level of the central insula in 36%, of the long insular gyri in 29%, and the anterior part of the insula in 35% [13, 21]. These perforators have an ascending direction, orthogonal to the insula, toward the body of the lateral ventricle. They then reach deep targets: arcuate fasciculus for all of them, corticonuclear tract for those penetrating the dorsal part of the short insular gyri, corticospinal tract for those penetrating the dorsal part of the long insular gyri [21].
-
At the level of the circular sulcus of the insula, the MCA branches follow a hairpin curve to reach the medial aspect of the opercula. This 180° curve, which is more obvious for the M2 branches having an ascending course, is visible on angiograms and marks the limit between the M2-insular and M3-opercular segments. Once arrived at the junction of the medial and horizontal part of the opercula (superior for the temporal one, and inferior for the frontoparietal one), M3 changes again its direction to run laterally with a new turn of about 90° before reaching the lateral limit of the lateral fissure, which marks the limit between the M3-opercular and M4-cortical segments.
-
From this point, the branches of the M4 segment exit the lateral fissure and spread over the surface of the cortex to reach their terminal destination. The territory of the MCA is subdivided into 12 different areas served by cortical arteries with a variable branching pattern from the stem arteries: orbitofrontal, prefrontal, precentral, central, anterior parietal, posterior parietal, angular, temporo-occipital, posterior temporal, middle temporal, anterior temporal, and temporopolar arteries [7, 20].

M1 and M2 segments of the Middle cerebral artery. (a) Ventral view of a left hemisphere after part of the temporal lobe (TempLobe) was opened to show the temporal horn (TempHorn) of the lateral ventricle and choroid plexus (ChoPlex). From proximal to distal, the internal carotid artery (ICA) gives the posterior communicating artery (Pcom), the anterior choroidal artery (AntCho). It finally divides lateral to the optic chiasm (Chiasm) in precommunicating (A1) segment of the anterior cerebral artery and sphenoidal segment (M1) of the middle cerebral artery. The later runs in the basal compartment of the lateral fissure where it divides in trunks (M1Trunks). The prebifurcation part of M1 gives perforators, the anterolateral central (or lenticulate, LSA) arteries. After passing the limen insulae (Limen), M1 is continued by the insular segment (M2) of the middle cerebral artery. (b) Detailed view of the distal branches of the ICA and LSA. (c) Lateral view of the left hemisphere after the temporal operculum (TempOperc) was partially removed and the frontoparietal operculum (FrOperc) was retracted to show the limen, the long insular gyri (LongIns G), the central insular sulcus (Cent S Ins), and the most posterior short insular gyrus (ShortIns G). At the level of the limen insulae, the trunks of the middle cerebral artery follows a 90° angle that marks the M1–M2 limit. Arteries belonging to the M2 segment fan and divide at the surface of the insula, up to the circular sulcus of the insula (CircSIns). A2 Post communicating segment of the anterior cerebral artery, Acom Anterior communicating artery, Fr-OrbCort Fronto-orbital cortex, III Oculomotor nerve, MamBod Mammillary body, Op tract Optic tract, P1 Precommunicating segment of the posterior cerebral artery, P2 Postcommunicating segment of the posterior cerebral artery, SCA Superior cerebral artery

Insular (M2) segment of the middle cerebral artery. Lateral view of a left hemisphere, after the opercula were removed to expose the short (Short G) and long (Long G) gyri of the insula. The sphenoidal (M1) segment of the MCA divides in a superior (M1s) and an inferior (M1i) trunks, which pass the limen insulae to enter the lateral segment of the lateral fossa. An early branch originates proximal to this bifurcation to reach the anterior part of the insula and the fronto-orbital operculum. The insular segment of the MCA (M2) is the one running at the surface of the insula, from the limen to the circular sulcus of the insula (Circul S, dash line). It is made of the main trunks (M2 Trunk), which divides in stem arteries (Stem a). The latter then divide again, close to the Circul S in cortical arteries. Distal to the Circul S, the MCA branches are known as the opercular segment (M3) which follow the medial and then horizontal aspects of the opercula to reach the lateral aspect of the brain
5 Venous Relationships
The venous pattern of the insula is variable, but four insular veins are commonly described:
-
The anterior insular vein runs close to the anterior circular sulcus with a ventro-posterior direction, toward the limen insulae. It drains the anterior circular sulcus and the anterior short insular gyrus.
-
The precentral insular vein drains the middle short insular gyrus and apex and follows the insular precentral sulcus with a ventro-posterior direction.
-
The central insular vein courses along the central sulcus of the insula to drain the posterior short and anterior long gyri, central insular sulcus, and limen insulae.
-
The postcentral vein follows the postcentral insular sulcus and gets blood from the posterior long gyrus, posterior circular sulcus, and limen insulae [7].
Classically, these insular veins join together near the limen insulae to form the deep middle cerebral veins (DMCV), which courses in the basal segment of the lateral fissure. At the level of the anterior perforated space, it anastomoses with the anterior cerebral vein to form the anterior part of the basal vein. The drainage of the insular veins was shown [7] to be more complex, some of them having a partial or total drainage toward the superficial middle cerebral vein (SMCV or superficial Sylvian vein). The SMCV parallels the lateral segment of the lateral fissure, usually coursing a few millimeter ventral to it. At the anterior tip of the lateral part of the lateral fissure, it turns medially to reach its basal part before ending in the sphenoparietal or more rarely in the cavernous or sphenopetrosal sinuses. On the way it drains superficial cortical veins, divided into frontosylvian, parietosylvian, and temporosylvian groups but also some of the insular veins, especially the anterior and precentral ones.
6 Surgical Consequences
Due to its deep location, surgical approaches of the insula have to deal with the opercula and the vessels contained in the lateral fossa. The transsylvian and subpial approaches will be detailed chapter XXX, but a few surgically relevant details are pointed here.
6.1 Transsylvian Approach
Identifying the lateral fissure is usually trivial, but in case of large expansive processes or malformation (for instance, megalencephaly), the usual anatomical landmarks can be left. The lateral fissure can then be identified as the sulcus where numerous arteries (M4 segment) exit with ascending and descending courses over its ventral and dorsal lips, to reach their terminal cortical territories.
The opening of the lateral fossa can be tailored depending of the area of the insula to be reached; the area of the limen insulae and basal compartment of the lateral fissure can be reached to access the ICA, MCA bifurcation, arterial circle, and sphenoidal ridge. A reliable landmark to open the lateral fissure in this area is the inferior tip of the triangular part of the inferior frontal gyrus, the approach being conducted ventrally from this point. More posterior approaches can benefit from the projection of the superficial sulci onto the insula (Fig. 3.1). Briefly:
-
The dorsal end of the vertical ramus of the anterior segment of the lateral fissure projects onto the anterior insula, close to the superior circular sulcus [7].
-
The central sulcus of the insula has about the same orientation as the central sulcus. Its dorsal tip can face the ventral tip of the central sulcus in 60% [13] or be located a few millimeters anterior or posterior to it.
-
The middle horizontal segment of the lateral fissure corresponds to the juxtaposition of the frontoparietal and temporal opercula, whereas its posterior segment is surrounded by the supramarginal gyrus. In other words, the middle segment is the only one facing the lateral fossa and insula, and the junction of the middle horizontal and posterior ascending segments of the lateral fissure is a good landmark for the posterodorsal limit of the insula (junction of the superior and inferior circular sulci.
Whatever the considered part of the lateral fissure, retraction of the opercula has to be as limited as possible, especially in the subcentral area to avoid postoperative contralateral facial palsy but also in the superior temporal and inferior frontal and inferior precentral gyri in the dominant hemisphere to preserve language areas.
Once the lateral fossa is opened, if the trunks, stem, and cortical arteries of the MCA need to be dissected, two main areas have to be especially considered because of perforators:
-
The area located medial to the limen insulae (basal compartment of the lateral fissure) contains perforators (anterolateral central arteries) issued from the M1 segment of the MCA. The resection of a tumor in this area has to remain lateral to the most lateral of these arteries to avoid postoperative ischemia of the internal capsule and basal ganglia. The level of this most lateral M1 perforator can be considered as the lateral limit of the anterior perforated space. The area located between the anterior perforated space and the limen insulae, or limen recess, is free of perforators and is usually about 15 mm width [7].
-
The second area with important relationships to perforators is the superior part of the insula, close to the superior circular sulcus. As shown by [13, 21] long perforators of the M2/M3 segments of the MCA penetrate the insula in this area and may reach deep structures: arcuate fasciculus for all of them, corticonuclear tract for those penetrating the dorsal part of the short insular gyri, and corticospinal tract for those penetrating the dorsal part of the long insular gyri. These perforators have of course to be respected during the dissection of the MCA branches in the lateral fossa.
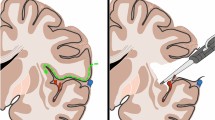
The transsylvian approach was proposed to reach the temporal horn of the lateral ventricle (Fig. 3.7) to perform selective amygdalohippocampectomy [22]. In this approach, an incision of about 2 cm is performed along the anterior part of the inferior circular sulcus of the insula to reach the temporal horn of the ventricle at a depth of about 0.5 mm [7]. Such an approach has the advantage to avoid neocortical resection but implies the manipulation of MCA branches and, above all, the disconnection of the anterior part of the temporal stem, with possible lesions to the uncinate fasciculus, anterior commissure, and anterior part of the temporal loop of the optic radiations [19, 23].

Surgical consequences of amygdalohippocampectomy. The transsylvian approach (a) preserves most of the neocortex as compared to trans-superior temporal sulcus (b) or trans T2 (c) approaches. It nevertheless implies to cut the anterior part of the temporal stem (T stem). H Hippocampus, T1 Superior temporal gyrus, T2 Middle temporal gyrus, T3 Inferior temporal gyrus, T4 Fusiform gyrus, T5 Parahippocampal gyrus
6.2 Transopercular Approach
This approach begins by the partial resection of the temporal or/and frontoparietal opercula after the superficial pia mater was cut parallel to the inferior or superior lip of the lateral fissure, respectively. The extension of this resection depends on the part of the insula to be reached, a temporal approach being for instance privileged in the case of a temporo-insular glioma. The projection of the sulci of the lateral aspect of the hemisphere onto the insula shows that about 2/3 of the insula is located medial to the temporal operculum, the remaining dorsal third being hidden by the frontal operculum. This explains why a temporal resection is usually preferred when a subpial approach is proposed for a glioma limited to the insula [24].
The resection is performed subpially, the pia mater being followed from the lateral, to the inferior or superior, and then medial aspects of the operculum to reach the inferior or superior circular sulcus, giving access to the insula. In this approach the vascular dissection is minimal, branches of the MCA remaining embedded by the pia mater covering the walls of the lateral fossa. It nevertheless implies the resection of possibly highly functional areas involved in language (inferior frontal and inferior precentral gyrus, superior temporal gyrus in the dominant hemisphere) or motor function (subcentral area). For this reason, a cortical and subcortical mapping using direct electrical stimulation (DES) and awake surgery has to be performed prior and during the opercular resection [24]. For instance [25], dysarthria is induced by stimulation of the ventral sensorimotor cortex (vSMC) on both hemispheres (ventral part of the pre- and postcentral gyri and subcentral gyrus [26]) or by stimulation of the anterior horizontal segment of the SLF; it connects to the supramarginal gyrus (articulatory loop). A total motor arrest can be induced by DES of the vSMC or pars opercularis of the inferior frontal gyrus. Phonological disorders can be elicited by DES of the dorsal phonological stream: arcuate fasciculus around the posterodorsal part of the insula and areas it connects in the frontal (opercular part of the inferior frontal gyrus, posterior third of the middle frontal gyrus) and temporal lobes (posterior third of the middle and inferior temporal gyri). Semantic disturbances (or at maximum, anomia) are induced by stimulation of cortical components of the ventral semantic stream in the dominant hemisphere: pars opercularis of the inferior frontal gyrus, posterior part of the superior and middle frontal gyri, and superior temporal sulcus [27].
6.3 Resection of the Insula
During tumor resection, several areas of the insula need to be approached with caution.
First, as previously mentioned, the entry area of the long perforators is located at the superior aspect of the insula. These vessels have to be respected in that they vascularize deep white matter.
The ventral aspect of the extreme and external capsules, located just medial to the ventral insula, also has to be respected because it contains the trunks of the IFOF and UF. The role of the UF remains unclear in the literature, but its preservation seems not to be crucial for language [27, 28]. In the dominant hemisphere, the situation is completely different for the IFOF, which completes the semantic network mentioned above, at the cortical level. DES of the IFOF consistently induces transient verbal (semantic paraphasia, anomia) [29, 30] and nonverbal semantic disturbances (impossibility to associate images belonging to the same semantic field during for instance the pyramid and palm tree test) [31]. It also produces a certain degree of unawareness of the induced deficits [31] and perseveration [32]. Its lesion induces non-compensable permanent deficit, pleading for a systematic use of DES during resection of insular lesions.
The internal capsule, including fibers of the corticonuclear and corticospinal tracts, is separated from the insula by the extreme capsule, claustrum, external capsule, and lenticular nucleus. The internal capsule is thus relatively preserved from a direct injury during insular resection, except at the superior border of the putamen, where the extreme, external, and internal capsules fuse to become the corona radiata. As a consequence the white matter located medial to the superior part of the insula needs to be frequently tested using DES to control extension of the resection in this direction.
Conclusion
Surgical approach of the insula remains quite challenging due to its deep location, medial to the opercula, and also a rich environment made of vessels and white matter tracts. It is nevertheless possible, bearing in mind a few anatomical information, important to avoid postoperative deficits.
References
Duvernoy HM. The human Brain. Surface, blood supply, and three-dimensional sectional anatomy. 2nd ed. Wien, New York: Springer; 1999. 491 p.
Destrieux C, Terrier LM, Andersson F, Love SA, Cottier J-P, Duvernoy H, et al. A practical guide for the identification of major sulcogyral structures of the human cortex. Brain Struct Funct. 2017;222(4):2001–15.
Destrieux C, Fischl B, Dale A, Halgren E. Automatic parcellation of human cortical gyri and sulci using standard anatomical nomenclature. Neuroimage. 2010;53:1–15.
Guenot M, Isnard J, Sindou M, et al. Surgical anatomy of the insula. Adv Tech Stand Neurosurg. 2004;29:265–88.
Türe U, Yaşargil DC, Al-Mefty O, Yaşargil MG. Topographic anatomy of the insular region. J Neurosurg. 1999;90(4):720–33.
Varnavas GG, Grand W. The insular cortex: morphological and vascular anatomic characteristics. Neurosurgery. 1999;44(1):127–36; discussion 136–8.
Tanriover N, Rhoton AL Jr, Kawashima M, Ulm AJ, Yasuda A. Microsurgical anatomy of the insula and the sylvian fissure. J Neurosurg. 2004;100(5):891–922.
Martino J, De Witt Hamer PC, Berger MS, Lawton MT, Arnold CM, de Lucas EM, et al. Analysis of the subcomponents and cortical terminations of the perisylvian superior longitudinal fasciculus: a fiber dissection and DTI tractography study. Brain Struct Funct. 2013;218(1):105–21.
Fernandez-Miranda JC, Rhoton AL, Alvarez-Linera J, Kakizawa Y, Choi C, de Oliveira EP. Three-dimensional microsurgical and tractographic anatomy of the white matter of the human brain. Neurosurgery. 2008;62(6 Suppl 3):989–1026. discussion 1026-8.
Catani M, Jones DK, ffytche DH. Perisylvian language networks of the human brain. Ann Neurol. 2005;57(1):8–16.
Fernandez-Miranda JC, Rhoton AL, Kakizawa Y, Choi C, Alvarez-Linera J. The claustrum and its projection system in the human brain: a microsurgical and tractographic anatomical study. J Neurosurg. 2008;108(4):764–74.
Goga C, Türe U. The anatomy of Meyer’s loop revisited: changing the anatomical paradigm of the temporal loop based on evidence from fiber microdissection. J Neurosurg. 2015;122(6):1253–62.
Delion M, Mercier P, Brassier G. Arteries and veins of the Sylvian fissure and insula: microsurgical anatomy. In: Schramm J, editor. Advances and technical standards in neurosurgery [Internet]. Cham: Springer International Publishing; 2016. p. 185–216. [cited 2017 Aug 13]. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/978-3-319-21359-0_7.
Sarubbo S, De Benedictis A, Milani P, Paradiso B, Barbareschi M, Rozzanigo U, et al. The course and the anatomo-functional relationships of the optic radiation: a combined study with ‘post mortem’ dissections and ‘in vivo’ direct electrical mapping. J Anat. 2015;226(1):47–59.
Martino J, Brogna C, Robles SG, Vergani F, Duffau H. Anatomic dissection of the inferior fronto-occipital fasciculus revisited in the lights of brain stimulation data. Cortex. 2009;46:691–9.
Sarubbo S, De Benedictis A, Maldonado IL, Basso G, Duffau H. Frontal terminations for the inferior fronto-occipital fascicle: anatomical dissection, DTI study and functional considerations on a multi-component bundle. Brain Struct Funct. 2013;218(1):21–37.
Ebeling U, von Cramon D. Topography of the uncinate fascicle and adjacent temporal fiber tracts. Acta Neurochir. 1992;115(3–4):143–8.
Kier EL, Staib LH, Davis LM, Bronen RA. MR imaging of the temporal stem: anatomic dissection tractography of the uncinate fasciculus, inferior occipitofrontal fasciculus, and Meyer’s loop of the optic radiation. AJNR Am J Neuroradiol. 2004;25(5):677–91.
Peuskens D, van Loon J, Van Calenbergh F, van den Bergh R, Goffin J, Plets C. Anatomy of the anterior temporal lobe and the frontotemporal region demonstrated by fiber dissection. Neurosurgery. 2004;55(5):1174–84.
Rhoton AL. The supratentorial arteries. Neurosurgery. 2002;51(4 Suppl):S53–120.
Delion M, Mercier P. Microanatomical study of the insular perforating arteries. Acta Neurochir. 2014;156(10):1991–8.
Yasargil MG. Microneurosurgery: in 4 volumes. Vol. 1. New York Stuttgart: Thieme Stratton ; Georg Thieme Verlag; 1984. 4 v. in 6.
Destrieux C, Bourry D, Velut S. Surgical anatomy of the hippocampus. Neurochirurgie. 2013;59(4–5):149–58.
Duffau H, Capelle L, Lopes M, Faillot T, Sichez JP, Fohanno D. The insular lobe: physiopathological and surgical considerations. Neurosurgery. 2000;47(4):801–10. discussion 810–1.
Mandonnet E, Sarubbo S, Duffau H. Proposal of an optimized strategy for intraoperative testing of speech and language during awake mapping. Neurosurg Rev [Internet]. 2016 19 [cited 2016 Jul 3]; Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/s10143-016-0723-x
Bouchard KE, Mesgarani N, Johnson K, Chang EF. Functional organization of human sensorimotor cortex for speech articulation. Nature. 2013;495(7441):327–32.
Duffau H. The anatomo-functional connectivity of language revisited New insights provided by electrostimulation and tractography. Neuropsychologia. 2008;46(4):927–34.
Duffau H, Gatignol P, Moritz-Gasser S, Mandonnet E. Is the left uncinate fasciculus essential for language? A cerebral stimulation study. J Neurol. 2009;256(3):382–9.
Almairac F, Herbet G, Moritz-Gasser S, de Champfleur NM, Duffau H. The left inferior fronto-occipital fasciculus subserves language semantics: a multilevel lesion study. Brain Struct Funct. 2015;220(4):1983–95.
Duffau H, Herbet G, Moritz-Gasser S. Toward a pluri-component, multimodal, and dynamic organization of the ventral semantic stream in humans: lessons from stimulation mapping in awake patients. Front Syst Neurosci [Internet]. 2013 Aug 26 [cited 2015 Aug 28];7. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752437/
Moritz-Gasser S, Herbet G, Duffau H. Mapping the connectivity underlying multimodal (verbal and non-verbal) semantic processing: a brain electrostimulation study. Neuropsychologia. 2013;51(10):1814–22.
Khan OH, Herbet G, Moritz-Gasser S, Duffau H. The role of left inferior fronto-occipital fascicle in verbal perseveration: a brain electrostimulation mapping study. Brain Topogr. 2014;27(3):403–11.
Zemmoura I, Serres B, Andersson F, Barantin L, Tauber C, Filipiak I, et al. FIBRASCAN: a novel method for 3D white matter tract reconstruction in MR space from cadaveric dissection. Neuroimage. 2014;103:106–18.
Acknowledgments
We thank Daniel Bourry, photographer at the University of Tours, for his help in picture acquisition and post processing.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Destrieux, C., Lima Maldonado, I., Terrier, LM., Zemmoura, I. (2018). Surgical Anatomy of the Insula. In: Turgut, M., Yurttaş , C., Tubbs, R. (eds) Island of Reil (Insula) in the Human Brain. Springer, Cham. https://doi.org/10.1007/978-3-319-75468-0_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-75468-0_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-75467-3
Online ISBN: 978-3-319-75468-0
eBook Packages: MedicineMedicine (R0)