
Abstract
Inflammatory heart diseases include rheumatic fever, Kawasaki disease, and myocarditis. These conditions all stem from an inflammatory process that may lead to significant cardiac morbidity and mortality. These patients often present initially to the emergency department, and prompt recognition and treatment of these conditions are essential. Rheumatic fever is caused by group A streptococcal (GAS) infections and is diagnosed using the Jones criteria. Rheumatic fever may lead to mitral and/or aortic valve dysfunction. Kawasaki disease is a systemic vasculitis that affects medium-sized arteries. Diagnostic criteria include fever, conjunctivitis, mucositis, extremity changes, rash, and lymphadenopathy. Patients may present with shock related to myocarditis and can develop aneurysms in the coronary arteries with the potential for ischemic heart disease. Treatment consists of immunomodulators and anticoagulation. Myocarditis has numerous causes but is most commonly secondary to a viral illness. Clinical presentation varies widely, but patients may present acutely in cardiogenic shock. Treatment consists of immunomodulators and heart failure medications.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Inflammatory heart disease
- Rheumatic fever
- Rheumatic carditis
- Kawasaki disease
- Coronary artery aneurysm
- Myocarditis
- Cardiomyopathy
Inflammatory illnesses, such as rheumatic fever, Kawasaki disease, and viral myocarditis, can cause substantial acute cardiovascular damage and lead to long-standing complications in children. The acute presentations of these conditions are variable and can range from mild, nonspecific symptoms to life-threatening cardiovascular collapse. The emergency department is often the first point of medical care for these patients, and early recognition and treatment of the underlying inflammation are essential to preventing cardiac damage.
Rheumatic Fever
Clinical Vignette
An 8-year-old-girl was admitted to the emergency department because of uncontrollable arm movements. Her parents reported that she had a 4-week history of worsening coordination and fidgeting. She has been tripping over objects and bumping into walls and is unable to sit still. Her teachers recently commented on a decline in her penmanship and said that she is more disruptive and moody in class. She has no remarkable medical history and no recent illnesses, except for a sore throat and fever several months ago that resolved spontaneously. Physical examination revealed a new 3/6 high-pitched systolic murmur at the apex that radiates to the left axillae.
The Pathophysiology of Rheumatic Fever
Acute rheumatic fever (ARF) is an acute inflammatory illness that follows group A streptococcal (GAS) pharyngitis caused by an abnormal immune response in a susceptible host. The immune response may cause inflammation of the heart, joints, brain, or connective tissue. Certain strains of GAS are more likely to cause ARF. These rheumatogenic strains express specific virulence factors, including the M protein, on the cell surface [1]. The pathogenesis of ARF is not completely understood, but current models suggest that after exposure to certain streptococcal antigens, a process known as “molecular mimicry” can begin an abnormal cellular and humoral immune response. Antibodies directed at GAS cross-react with host antigens, including cardiac antigens, initiating an inflammatory cascade. Endothelial cell damage leads to infiltration of additional inflammatory cells, and exposed cardiac proteins further activate the immune system in a process known as “epitope spreading.” Serial exposure to the GAS antigen may lead to recurrence of ARF and increase the likelihood of persistent and evolving cardiac changes manifesting as chronic rheumatic heart disease (RHD). The dominant abnormality in RHD is mitral valve dysfunction with variable combinations of insufficiency and stenosis. The aortic valve is less commonly affected. Although the incidence of ARF has declined sharply in developed countries, ARF leading to RHD remains the leading cause of heart failure in children and adolescents in the developing world [2].
The Acute Presentation of Rheumatic Fever
Acute rheumatic fever typically presents in children 5–15 years of age, although it occasionally affects younger children and older adolescents or young adults. The five major diagnostic criteria are carditis, arthritis, chorea, subcutaneous nodules, and erythema marginatum: the “Jones criteria.” Carditis and arthritis are the most common and are seen in 50–70% and 35–66% of cases, respectively. Chorea (10–30%) is less common, and subcutaneous nodules (0–10%) and erythema marginatum (<6%) are rare [3]. Most symptoms appear 10 days to 5 weeks after GAS pharyngitis, with chorea presenting up to 6 months after the initial illness. The GAS pharyngitis that precedes ARF may be mild or even subclinical. Patients most commonly seek medical care for joint pain and inflammation. Patients with cardiac involvement may present due to heart failure symptoms related to marked valve regurgitation or a new murmur detected on physical examination.
The Jones criteria have been used since 1944 and have been revised several times, most recently in 2015 (Table 19.1) [3]. The diagnosis of ARF is based on the presence of two major criteria or one major criterion and two minor criteria, in addition to evidence of a preceding GAS infection. Given the wide global variability in the incidence of ARF, the latest revision of the Jones criteria suggests that children should be categorized as low risk or moderate to high risk for ARF and that different diagnostic criteria should be used according to these categories (Table 19.1). Risk stratification is based on the population incidence of ARF and RHD. Low-risk patients reside in populations with an annual incidence of fewer than 2 cases of ARF per 100,000 school-aged children or an all-age prevalence of RHD of not more than 1 per 1000 population. Children clearly not from a low-risk population should be considered at moderate to high risk. The definition of major and minor criteria varies based on the child’s risk stratification (Table 19.1) [3]. Populations from most developed countries, including the USA, are considered to be low risk.
Carditis is the most common major feature of ARF. Carditis typically presents as a valvulitis with new-onset mitral insufficiency, with or without aortic valve insufficiency (Fig. 19.1). Mitral insufficiency is almost universal in ARF patients with carditis, presenting in up to 95% of carditis cases [2]. Aortic insufficiency is less common and usually presents in combination with mitral insufficiency. Mild valve insufficiency may not be recognized without an echocardiogram and is usually asymptomatic. Moderate and severe mitral insufficiency can lead to pulmonary congestion and edema, so affected patients may present with cough, dyspnea on exertion, shortness of breath, and orthopnea. Pericarditis and myocarditis may be present, but in the absence of valve insufficiency, they should not be considered a major manifestation of the Jones criteria. Pericarditis of ARF is rarely associated with large effusions or tamponade. Biopsies may reveal evidence of myocarditis, but unlike other forms of myocarditis, myocyte necrosis does not occur, and troponin concentrations are not elevated [2]. All patients with carditis should be referred to a cardiologist.

(a) Mitral insufficiency (asterisk) and (b) aortic insufficiency (arrow) in an 8-year-old boy with acute rheumatic fever at presentation. LA left atrium, LV left ventricle
Subclinical carditis has been described in rheumatic fever, and strict echocardiographic criteria have been established to diagnose features of carditis that may be inaudible. For this reason, all patients with confirmed or suspected ARF should undergo echocardiography. Clinical or subclinical carditis is a major criterion for the diagnosis of ARF in both risk groups.
Arthritis is a common feature of ARF and one that needs to be assessed carefully. The differential diagnosis for arthritis is broad and creates the potential for misdiagnosis. Additionally, salicylates and other nonsteroidal anti-inflammatory drugs relieve the pain, and ready access to these medications may alter the natural course of the arthritis. The classic presentation is a migratory polyarthritis of the large joints. The polyarthritis manifests as swollen and erythematous joints with pain that is often out of proportion to the physical findings. In addition to polyarthritis, aseptic monoarthritis has been described in high-risk populations. Polyarthralgia is a minor criterion in low-risk populations and a major criterion in high-risk populations. Post-streptococcal reactive arthritis should not be mistaken for the arthritis or polyarthralgia of ARF. As opposed to the arthritis of ARF, post-streptococcal reactive arthritis tends to involve small joints, is more persistent, and is less responsive to anti-inflammatory medications.
As exemplified in the clinical vignette above, chorea is the involuntary and purposeless movements of the trunk and extremities, as well as muscle weakness and emotional lability. It is a late finding in ARF, occurring 2–6 months after the initial GAS pharyngitis. Physical exam findings consistent with chorea include “milkmaid’s grip,” or irregular contractions of the fingers when squeezing an object; “pronator sign,” or the pronation of hands when extended above the head; and “spooning,” or the hyperextension of the fingers when the hands are extended forward while the eyes are closed. Parents may notice increased emotional lability or new difficulties with fine muscular coordination, such as degraded penmanship or the ability to button clothing. Chorea of ARF must be differentiated from other inherited and acquired neurologic disorders as described in the section below. Consulting with a neurologist is strongly encouraged.
The dermatologic findings in ARF include erythema marginatum and subcutaneous nodules. Erythema marginatum consists of a bright-pink, macular, nonpruritic, and often evanescent rash with serpiginous borders and a pale center. The rash is usually on the trunk and proximal extremities and rarely affects the face. The subcutaneous nodules are small, firm, painless nodules on the bony portions of the extensor surfaces of the joints and on the spinous processes of the back. They are not transient and may last for weeks. The cutaneous manifestations of ARF are usually associated with carditis and are rarely the only major criteria for diagnosis [3].
As with the major criteria, the minor criteria vary based on risk category (Table 19.1). As mentioned earlier, polyarthralgia is a minor criterion in low-risk patients. Fever is a consistent feature of ARF, and in high-risk populations, a lower fever is a minor criterion. Laboratory evidence of systemic inflammation is common and also varies based on the pretest probability of ARF. In the absence of an elevated C-reactive protein (CRP) concentration or erythrocyte sedimentation rate (ESR), the diagnosis of ARF is unlikely, except in cases presenting with chorea or indolent carditis. Finally, conduction abnormalities can be seen in ARF, with the most common being first-degree atrioventricular block, although a more advanced atrioventricular block can be seen as well.
Laboratory evidence of a preceding streptococcal infection from a positive throat culture, rapid strep test, or an elevated or rising anti-streptolysin O or anti-DNAse B titer is required for the diagnosis of ARF (Tables 19.1 and 19.2). However, evidence of a prior GAS infection may be absent in patients presenting with chorea or chronic valve insufficiency (chronic RHD), given the delayed presentation of these conditions.
The Differential Diagnosis of Rheumatic Fever
The differential diagnosis of ARF largely depends on the patient’s primary symptoms. The carditis of ARF should be distinguished from other causes of new valvar regurgitation, such as infective endocarditis or progressive valve insufficiency related to an underlying congenital abnormality. Innocent murmurs are common in school-aged children and should be differentiated from the regurgitant murmurs associated with ARF. Arthritis should be distinguished from a post-streptococcal reactive arthropathy, connective tissue diseases, and infectious causes, including viral arthropathies and septic arthritis. Isolated chorea should lead to a thorough investigation of inherited causes, such as Huntington disease, Wilson disease, Lesch-Nyhan syndrome, ataxia-telangiectasia, and Friedreich’s ataxia. Autoimmune disorders , such as lupus, endocrine and metabolic disorders, psychological disorders, and toxin or drug exposure should also be ruled out.
Managing Rheumatic Fever in the Emergency Department
The essential first step in managing inflammatory diseases with potential cardiac involvement such as ARF is to recognize the clinical features and diagnose the condition correctly. Initial treatment of ARF is aimed at eliminating the immune response, decreasing inflammation, and addressing valve insufficiency.
All patients with a diagnosis of ARF should be treated with antibiotics for GAS (Table 19.3). Patients with joint symptoms should be started on aspirin or other nonsteroidal anti-inflammatory medications. Treatment of chorea depends on the severity of symptoms; a neurology consultation should be strongly considered. Any patient in whom ARF is suspected should undergo echocardiography, and a cardiologist should be consulted if carditis is present. Patients with ARF and mild-to-moderate carditis should be treated with high-dose aspirin (80–100 mg/kg/day divided every 6 h in children or 4–8 g/day in adolescents and adults). In patients with moderate-to-severe carditis, many experts recommend a course of steroids (some recommend prednisone 2 mg/kg/day for 2 weeks followed by taper), although there is no evidence of clear benefit. Patients with subclinical and very mild carditis may be followed closely as outpatients, whereas those with moderate-to-severe carditis should be monitored as inpatients. Patients with signs of hemodynamic compromise related to marked valvular dysfunction should be admitted to an intensive care unit.
Ruptured mitral valve chordae can lead to severe valvular insufficiency and flail mitral leaflets. Patients presenting with severe valve insufficiency and hemodynamic compromise with severe heart failure should be evaluated for urgent surgical intervention. In this setting, medical management should not delay surgical repair. Until surgery, systemic vasodilators, such as nitroprusside or milrinone, may be considered to reduce afterload. These medications may promote antegrade flow and thereby decrease mitral insufficiency; however, the use of vasodilators in this setting is often limited by systemic hypotension.
Ongoing Management of Rheumatic Fever
All patients with ARF should be evaluated for cardiac involvement, and those with carditis should be referred to a cardiologist. For patients treated with salicylate or steroids, the optimal duration of therapy is unknown. Some experts recommend discontinuing treatment when concentrations of acute-phase reactants return to normal or after 4–6 weeks. Patients treated with prolonged high-dose salicylates should have salicylate concentrations between 20 and 30 mg/dL [2]. If steroids were prescribed initially, salicylates should be prescribed before discontinuing steroids to prevent rebound inflammation. Heart failure may need to be managed in patients with moderate-to-severe valve insufficiency; in which case, oral diuretics and afterload reduction may be necessary. Given the risk of progressive mitral insufficiency, some physicians recommend restricting patient activity during the acute phase of the illness.
All patients with ARF require long-term secondary prophylaxis against repeat GAS infections (Table 19.3). The duration of secondary prophylaxis is based on the degree of RHD. The importance of secondary prophylaxis should be emphasized at each encounter because the risk of RHD increases with each recurrence of ARF [2].
Complications of Acute Rheumatic Fever
The primary goal of early treatment and secondary prophylaxis in ARF is to prevent chronic RHD, which remains the leading cause of heart failure in children and adolescents worldwide. Like carditis of ARF, the primary manifestations of RHD in children include mitral and aortic insufficiency. In addition, mitral and aortic stenosis can develop over time and may present decades after the initial episode. These complications are more likely after severe initial carditis or frequent recurrences of ARF.
Rheumatic Fever Clinical Pearls
-
Acute rheumatic fever most commonly affects children between 5 and 15 years old
-
Cardiac involvement (carditis) may be clinical or subclinical and is related to regurgitation of the mitral or aortic valves
-
Echocardiograms should be obtained in all patients with confirmed or suspected ARF
-
Cardiac involvement may persist or evolve into chronic rheumatic heart disease
-
Joint symptoms have a broad differential diagnosis and may lead to misdiagnosis
-
Patients presenting with chorea or indolent carditis may have no evidence of GAS infection
Kawasaki Disease
Clinical Vignette
A 5-year-old boy presented to the emergency department after 9 days of persistent fever. On day 4 of his illness, his pediatrician noted fever and pain in the lower back and abdomen, diagnosed acute otitis media, and prescribed amoxicillin. On day 6 of his illness, the patient returned to his pediatrician with persistent fever, back pain, and a new peeling rash on his lower back. His antibiotic was changed to cefuroxime. By day 9 of his illness, still febrile, he was referred to the emergency department. A physical examination noted an irritable child with bilateral non-suppurative conjunctivitis, erythematous and cracked lips, and a macular rash on his lower back. His white blood cell count was 17,000, hematocrit was 38, and platelet count was 755,000. Urinalysis revealed 16 WBC per high-power field with no bacteria. Results of a comprehensive metabolic panel were normal. An echocardiogram showed a giant aneurysm of the left anterior descending coronary artery with thrombus formation.
The Pathophysiology of Kawasaki Disease
Kawasaki disease (KD) is a self-limited systemic vasculitis that occurs most often in infants and young children and affects the medium-sized muscular arteries. The vascular changes most often affect the coronary arteries, potentially resulting in aneurysm formation with the subsequent risk of thrombus formation or arterial narrowing [4]. Kawasaki disease was first described in 1967, yet the underlying cause remains unknown, although several hypotheses have proposed infectious, environmental, and autoimmune triggers of acute KD.
The acute inflammatory phase of KD involves both the adaptive and innate arms of the immune system. An initial influx of neutrophils and CD8+ T cells leads to a necrotizing arteritis. Aneurysms typically form in the acute phase and may be related to hemodynamic stresses because aneurysms are more commonly found in the proximal coronary arteries and at the branch points. Altered blood flow, particularly stasis, can cause thrombus formation and myocardial ischemia or infarction. Subacute vasculitis begins weeks after the initial episode but may last for months or years. Finally, luminal myofibroblastic proliferation narrows the vessel lumen and can also result in coronary stenosis and ischemic heart disease [4].
The Acute Presentation of Kawasaki Disease
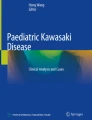
Kawasaki disease is a clinical diagnosis and typically presents in children less than 5 years old, although it can present in older children. The principal symptoms are the diagnostic criteria. The diagnosis of complete or “classic” KD can be made if there is fever lasting at least 5 consecutive days with at least four of five additional symptoms: bilateral , non-suppurative , conjunctival injections; oral mucosal changes; polymorphous rash; extremity changes, often as palmar and/or solar erythema and edema; and cervical lymphadenopathy (Fig. 19.2). These symptoms are often not concurrent, and a careful history is essential to elicit the diagnostic signs. Some experts suggest that the diagnosis can be made by day 4 of fever if four principal symptoms are clearly present. If less than 4 of the criteria for complete KD are present, the diagnosis of incomplete KD can be considered if at least two of the principal symptoms are present with additional laboratory or echocardiographic criteria (Fig. 19.3). Coronary artery dilation confirms the diagnosis of incomplete KD.

Classic clinical features of Kawasaki disease. (a) Rash characterized by maculopapular, diffuse erythroderma, or multiforme-like erythema. (b) Bilateral conjunctivitis and bulbar conjunctival injection without exudate. (c) Oral changes include cheilitis (erythema and cracking of the lips), strawberry tongue, and erythema of the oral and pharyngeal mucosa. (d) Palmar and (e) plantar erythema, which is usually accompanied by swelling and resolves with subsequent periungual desquamation in the subacute phase. (f) Cervical adenopathy, which is usually a unilateral node no more than 1.5 cm in diameter. (g) Coronary artery anuerysm in the right coronary artery with a nonocclusive thrombus and the left main coronary artery demonstrated on magnetic resonance imaging. Ao, aorta; AoV, aortic valve; LV, left ventricle; RV, right ventricle. (h) Peripheral artery anuerysms in the axillary, subclavian, iliac, and femoral arteries. Images reused with permission from American Heart Association

Evaluation of suspected incomplete Kawasaki disease. (1) In the absence of a “gold standard” for diagnosis, this algorithm cannot be evidence based but rather represents the informed opinion of the expert committee. Consultation with an expert should be sought any time assistance is needed. (2) Clinical findings of Kawasaki disease are listed in Table 19.3. Characteristics suggesting that another diagnosis should be considered include exudative conjunctivitis, exudative pharyngitis, ulcerative intraoral lesions, bullous or vesicular rash, generalized adenopathy, or splenomegaly. (3) Infants ≤6 months of age are the most likely to develop prolonged fever without other clinical criteria for Kawasaki disease; these infants are at particularly high risk of developing coronary artery abnormalities. (4) Echocardiography is considered positive for purposes of this algorithm if any of three conditions are met: Z score of left anterior descending coronary artery or right coronary artery ≥2.5; coronary artery aneurysm is observed; or ≥3 other suggestive features exist, including decreased left ventricular function, mitral regurgitation, pericardial effusion, or Z scores in left anterior descending coronary artery or right coronary artery of 2–2.5. (5) If the echocardiogram is positive, treatment should be given within 10 days of fever onset or after the 10th day of fever in the presence of clinical and laboratory signs (C-reactive protein [CRP], erythrocyte sedimentation rate [ESR]) of ongoing inflammation. (6) Typical peeling begins under the nail beds of fingers and toes. ALT indicates alanine transaminase, WBC white blood cells. Image reused with permission from the American Heart Association
Although most patients with KD do not have cardiac symptoms, a small subset present with acute KD shock syndrome. This syndrome is characterized by a more severe carditis, with decreased systolic and diastolic function. Kawasaki disease shock syndrome is not common, with one center describing shock symptoms in 7% of 187 KD patients over 4 years [5]. Some degree of left ventricular systolic dysfunction or mitral insufficiency may be present in up to 20% of acute KD patients. Patients with hemodynamic compromise related to KD are more likely to have laboratory findings supporting a greater degree of inflammation, higher rates of recrudescent fevers after treatment with intravenous immune globulin (IVIG), and a higher rate of coronary artery aneurysms [5, 6].
Patients with KD typically have remitting episodes of high fever. The fever is present for at least 5 consecutive days and, in the absence of treatment, lasts an average of 10 days but can persist for up to a month [4].
Conjunctival injection may be one of the earliest principal features and can occur shortly after the onset of fever. The injection is nonexudative and limbic-sparing. The limbus is a relatively avascular area around the iris and is thus spared from the inflammation. The conjunctivitis can resolve rapidly and may not be present at the time of clinical evaluation.
Mucosal changes consist of brightly erythematous lips, tongue, buccal mucosa, and pharynx. The lips are often dry and cracked, and the tongue has been described as “strawberry” because of the erythema and prominent papillae. Discrete ulcerative lesions and a pharyngeal exudate are not typical of KD.
The rash is nonspecific and is typically maculopapular. Several variations have been identified, but vesicular or bullous rashes are not among them [4]. The rash usually begins in the perineum and spreads to the chest and extremities. Desquamation can occur both on the extremities, typically periungual, and in the perineum.
Extremity changes manifest as erythema and induration of the palms and soles. The interphalangeal joints may also be swollen. Children will often avoid using their hands or weight-bearing because of the pain.
Cervical lymphadenopathy is typically unilateral. The affected lymph node should measure at least 1.5 cm and is typically not tender. Cervical lymphadenopathy is the least common of the principal features.
There is no pathognomonic test for KD, but blood and urine tests can aid in the diagnosis and are particularly helpful in the setting of incomplete KD, where they are part of the diagnostic algorithm (Fig. 19.3). During the acute presentation, laboratory evidence of systemic inflammation is nearly universal, with at least moderate elevations in CRP concentration and ESR. After treatment with IVIG, CRP concentrations are more representative of the patient’s inflammation because IVIG can actually increase ESR. Anemia and hypoalbuminemia are common. White blood cell counts can be increased and demonstrate a neutrophil predominance. Thrombocytosis typically appears during the second week of the illness. Liver function tests, including serum concentrations of transaminases and gamma-glutamyltranspeptidase, can also be elevated.
Noncardiac features of KD have also been described. Children may have prodromal symptoms of abdominal pain and diarrhea that precede fever. Hydrops of the gallbladder is well described and can present in up to 15% of patients. Children with fever and irritability often undergo a lumbar puncture to rule out meningitis which reveals aseptic meningitis. Urethritis and phimosis can occur during the acute phase and are often the impetus to obtain a urinalysis, which may show a sterile pyuria. Kawasaki disease has also been diagnosed in patients with simultaneous macrophage-activation syndrome.
The Differential Diagnosis of Kawasaki Disease
Diagnosing KD can be difficult, given the overlap of symptoms with infectious and rheumatologic conditions. Distinguishing among infectious diagnoses can be particularly challenging because these conditions may also present with fever, inflamed mucosa, nonspecific rashes, and changes in extremities. Common infections that may mimic these findings include staphylococcal and streptococcal skin infections as well as many viruses. Testing for viral infections, such as adenovirus, Epstein-Barr virus, and enterovirus, may be helpful. However, persistent fever, clinical features of a viral illness, and positive viral testing should not be dismissed as being inconsistent with KD if the clinical criteria for KD are met. Many patients with KD have a concomitant infectious or viral illness, and a positive viral study does not rule out KD [7]. Drug reactions, toxic shock syndrome, Stevens-Johnson syndrome, and staphylococcal scalded skin syndrome may present with similar cutaneous findings and desquamation. Rheumatologic conditions, such as juvenile rheumatoid arthritis, may present with elevated inflammatory markers and joint changes.
Children at both ends of the typical age spectrum for KD including those less than 6 months and greater than 5 years should be evaluated cautiously because they more commonly present with incomplete KD. Fever in an infant may prompt an infectious work-up, including analysis of cerebrospinal fluid and urine. A sterile pleocytosis or pyuria may be a sign of KD. Adolescents with fever and acalculous cholecystitis should also be evaluated for KD.
Managing Kawasaki Disease in the Emergency Department
As described above, KD patients can present with hemodynamic compromise and shock. In this setting, vasoactive infusions may be necessary along with careful volume resuscitation. These symptoms often prompt sepsis evaluations, and KD should be on the differential for patients with prolonged fever and aseptic meningitis or sterile pyuria. Any patient with hemodynamic compromise should be admitted to an intensive care unit for monitoring, treatment, and cardiology consultation. Patients in KD shock typically present with more severe inflammation and are more likely to be resistant to treatment with IVIG. They are also at higher risk for coronary artery aneurysms [5].
The challenge for the emergency physician confronting KD is not usually managing a critically ill child but rather recognizing the clinical features that may suggest KD, particularly in children outside of the typical age range for KD or who present with incomplete KD. A high index of suspicion is essential for timely diagnosis, hospital admission, and beginning therapy. The diagnosis of KD should be considered in any infant with a prolonged fever. A diagnosis of a viral syndrome does not rule out KD.
Ongoing Management of Kawasaki Disease
Intravenous immune globulin plus aspirin is the mainstay of therapy in treating KD and has greatly decreased the incidence of coronary artery aneurysms [8, 9]. Once diagnosed, the patient should be admitted and treatment begun. An echocardiogram is not necessary before starting therapies. Treatment should be started as soon as the diagnosis is made and ideally no later than 10 days after onset of the fever. If the diagnosis is not made until 10 days after the onset of fever, treatment should be reserved for patients with ongoing fever or evidence of systemic inflammation and those with evidence of coronary artery aneurysms. A 2 g/kg dose of IVIG should be infused over 10–12 h. Some centers recommend pretreatment with acetaminophen and diphenhydramine before beginning the infusion, given the risk of a hypersensitivity reaction including anaphylaxis. A slow infusion also prevents excessive volume load in a potentially poorly functioning left ventricle. A hemolytic reaction can occur after IVIG infusion and cause worsening anemia. After completing the initial infusion of IVIG, the patient should be monitored for recrudescence of fever for 36 h. If fever recurs, most experts recommend repeating a dose of IVIG and considering other therapies [4].
In addition to IVIG, aspirin should be given to all patients diagnosed with KD to decrease inflammation. A dosage of 80–100 mg/kg/day in four divided doses is commonly recommended, although lower doses of 30–50 mg/kg/day are used in other countries, with no evidence supporting one dose or the other. When the fever has been absent for 48–72 h, the patient is transitioned to low-dose aspirin (3–5 mg/kg/day) for its antiplatelet activity, although some experts suggest use of high-dose aspirin until the 14th day of illness. Low-dose antiplatelet aspirin is given at least until the patient is evaluated clinically and echocardiographically 6–8 weeks after the initial diagnosis. Systemic anticoagulation is reserved for patients with giant or complex coronary artery aneurysms because they have the highest risk of coronary artery thrombosis [4].
Complications of Kawasaki Disease
The most feared complication of KD is coronary artery aneurysms (Fig. 19.4). These coronary abnormalities typically present during the acute/subacute phase and may regress with treatment. Aneurysms are most likely to occur in children less than 6 months old or more than 8 years old and in boys. Aneurysms are classified based on the coronary artery Z score for body surface area and by their absolute dimensions. Aneurysms are classified as small (Z score ≥2.5 to <5), medium (Z score ≥5 to <10 and absolute diameter <8 mm), and large or giant (Z score ≥10 or absolute diameter ≥8 mm). Morbidity occurs primarily in patients with giant aneurysms and is related to the development of coronary stenoses and myocardial ischemic events. One study placed the cardiac event-free rate at 30 years at only 36% in those with giant aneurysms [10].

A giant coronary artery aneurysm in the left main coronary artery with thrombus formation (arrow) in a 6-year-old boy with Kawasaki disease
Patients with KD and current or regressed coronary artery aneurysms are at higher risk for early coronary artery disease and should have lifelong follow-up. These patients should be screened and treated for additional coronary artery disease risk factors. Individuals presenting with a history of KD and chest pain should be evaluated for acute coronary syndrome (Table 19.4).
Kawasaki Disease Clinical Pearls
-
Kawasaki disease should be on the differential for any infant or child with prolonged fever
-
Infants less than 6 months old typically present with incomplete Kawasaki disease
-
A subset of patients with Kawasaki disease may present with a shock-like clinical picture due to myocarditis and ventricular dysfunction
-
Exudative conjunctivitis and pharyngitis make the diagnosis of Kawasaki disease less likely
-
Confirmed diagnosis of a respiratory virus does not rule out Kawasaki disease because the conditions can coexist
-
Patients presenting with chest pain and a history of Kawasaki disease should be evaluated for acute coronary syndrome
Myocarditis
Clinical Vignette
A 10-year-old boy presents to the emergency department with a 5-day history of fever, cough, rhinorrhea, and abdominal pain. On day 4 of his illness, shortness of breath and exercise intolerance worsened. On day 5, he became lethargic and his mental status changed. On presentation, he was tachycardiac, tachypneic, and hypotensive with poor perfusion. An electrocardiogram revealed low-voltage QRS complexes with diffuse ST segment elevations. Troponin concentrations were elevated at 2.1 ng/mL. An echocardiogram revealed decreased left ventricular function with an ejection fraction of 18%.
The Pathophysiology of Myocarditis
Myocarditis is an inflammatory disease of the myocardium [11]. The inflammatory agent is most commonly viral, although other infectious agents, autoimmune conditions, and toxins can be responsible (Table 19.5). During the acute phase, local injury to myocytes activates the innate immune system. Toll-like receptors trigger the release of inflammatory cytokines. The subacute phase is marked by the arrival of additional inflammatory cells from both the innate and adaptive immune systems. These cells contribute to the inflammatory milieu and can directly damage myocytes. Like other inflammatory heart conditions, molecular mimicry may contribute to ongoing inflammation when exposed cardiac proteins, particularly myosin, lead to ongoing inflammation due to the autoimmune response.
The chronic phase of myocarditis may have several outcomes. Clearing the antigen with minimal damage to the myocytes will lead to complete recovery. Antigenic clearing with severe myocyte damage will lead to fibrotic changes and subsequent dilated cardiomyopathy. Pathologic cardiac remodeling is also likely if myocyte inflammation persists because of ongoing exposure to the antigen or autoimmune-mediated myocyte damage [12].
The Acute Presentation of Myocarditis
The clinical presentation of myocarditis is variable and can range from unrecognized asymptomatic cases to those with heart failure, life-threatening arrhythmias, or hemodynamic collapse. The age distribution is bimodal, with most children presenting in infancy or mid-teens. Four predominant clinical presentations are usually discussed in the literature: acute myocarditis, fulminant myocarditis, acute chest pain with features of acute coronary syndrome, and sudden death.
Acute myocarditis classically presents with progressive heart failure symptoms weeks to months after a viral infection. Exercise intolerance, dyspnea, and fatigue are all common features. Depending on the degree of heart failure, the physical examination may reveal normal to varying degrees of tachycardia, tachypnea, pallor, and poor perfusion. A gallop rhythm and a new mitral insufficiency murmur may be present. Echocardiograms commonly show LV dilation and dysfunction in acute myocarditis.
Fulminant myocarditis has a more severe presentation, in which patients present with rapidly progressive heart failure symptoms days to weeks after a respiratory or gastrointestinal viral illness. Ventricular dysfunction can be serious, and patients may present in cardiogenic shock with multi-organ failure. Ventricular arrhythmias are common and typically present as ventricular tachycardia. In contrast to the echocardiographic findings of acute myocarditis, fulminant myocarditis presents with a normal ventricular chamber size, severely decreased systolic function, and septal thickening secondary to myocardial edema. Children may be more likely than adults to present with fulminant myocarditis [13].
Patients in the acute phase of myocarditis can present with substantial chest pain and clinical findings suggesting an acute coronary syndrome. Chest pain is the predominant symptom, with ECG findings showing diffuse ST segment elevations or depressions (Fig. 19.5). Cardiac biomarker concentrations may be elevated, with troponin being more commonly elevated than creatine kinase [14]. Cardiac biomarker concentrations are not uniformly elevated in fulminant myocarditis. Echocardiography typically reveals normal or mildly decreased ventricular function. Cardiac catheterization is often performed in these patients but does not demonstrate coronary artery disease. However, coronary vasospasm has been found in patients with suspected myocarditis during intracoronary acetylcholine testing [12].

Low-voltage QRS complexes, ST segment changes, and Q waves characteristic of myocarditis in a 12-year-old girl with myocarditis
Sudden cardiac death from fatal arrhythmias can be the initial presentation of myocarditis. In adolescents and children, myocarditis is thought to be the primary cause of sudden death in 5–8% of cases. The incidence may be higher in infants because myocarditis has been implicated as a cause of sudden infant death syndrome. In one single-center autopsy study, 43% of 62 patients had a positive PCR viral assay [15].
Diagnosis can be challenging in patients with myocarditis because no single test is uniformly positive. In the emergency department, appropriate tests include ECG, blood tests, and echocardiography (Table 19.6).
An abnormal electrocardiogram in children with myocarditis may be the most common clinical finding. However, no single pathologic ECG finding has been consistently associated with myocarditis. The most common abnormalities are in the ST segment and T waves and can include ST elevation and T wave inversion. Q waves are variably present, as are low-voltage QRS waves. Varying degrees of heart block have been described, and premature ventricular contractions and more severe ventricular tachyarrhythmias can be present. Patients with sustained arrhythmias have a high risk of cardiac arrest and may need mechanical circulatory support [16]. A normal ECG cannot rule out myocarditis.
Laboratory results typically show evidence of cardiac injury, inflammation, infection, and electrolyte disturbances. Cardiac biomarker concentrations, including troponin T and I and creatine kinase (MB fraction), can be elevated. Some studies suggest that the degree of elevation is associated with outcomes. Troponin T concentration above 0.052 ng/mL has been suggested as an appropriate cutoff for the diagnosis of myocarditis [15]. However, myocarditis can occur in the absence of elevated troponin concentrations. B-type natriuretic peptide (BNP) or N-terminal pro-BNP concentrations may be elevated, particularly in the setting of severe ventricular dysfunction. Inflammatory markers, such as CRP and ESR, are often elevated, as are WBC counts and liver enzyme concentrations, but all are nonspecific for myocarditis. Electrolytes should be evaluated and corrected to minimize the risk of ventricular arrhythmias. The patient should be evaluated for infectious disease, and PCR-based viral testing is often performed. The meaning of a positive viral study in noncardiac tissue is unclear. Prospective studies of adults comparing serologic viral diagnoses to PCR analyses of endomyocardial biopsy samples have reported a correlate virus in only 4% of patients. Alternatively, in another study of 21 children with clinical myocarditis, viral PCR testing of serum samples for cardiotropic viruses was positive in 43%, whereas these viruses were present in only 3% of 75 children undergoing viral testing for a fever [15].
Cardiac imaging is important in diagnosing myocarditis. A chest radiograph will be abnormal in up to 90% of patients. The most common finding is cardiomegaly, but pleural effusions and pulmonary edema are also common. An echocardiogram typically reveals ventricular dilation and dysfunction. Global dysfunction is more common, but regional wall motion abnormalities may be present. As described above, echocardiography can help distinguish acute from fulminant myocarditis. Additional echocardiographic findings may include mitral insufficiency and pericardial effusions. Outside the emergency department, cardiac MRI evaluating myocyte inflammation and edema is used for diagnosing myocarditis and determining prognosis.
The Differential Diagnosis of Myocarditis
Given the nonspecific features of myocarditis, medical professionals should consider this diagnosis in any patient presenting with features of heart failure. Myocarditis was responsible for new-onset LV dysfunction in up to 20% of children in the UK [15]. Additional factors should also be considered for patients with new-onset ventricular dysfunction (Table 19.5). Genetic mutations in cardiac proteins, such as titin, lamin, or myosin, can cause dilated cardiomyopathy. Mitochondrial myopathies or X-linked conditions, such as Barth syndrome, can lead to similar cardiac phenotypes.
Additional diagnoses to consider include autoimmune disorders, such as polymyositis, Churg-Strauss syndrome, Wegener’s granulomatosis, systemic lupus erythematosus, and sarcoidosis. Inborn errors of metabolism, including glycogen storage diseases, are rare but can lead to cardiac dysfunction. Nutritional deficiencies in vitamins or minerals, such as thiamine and zinc, are rare and more related to alcoholism in adults. Antineoplastic drugs, particularly anthracyclines, commonly lead to LV dysfunction. Acute coronary syndromes are rare in children, but patients with chest pain, ECG abnormalities, and elevated troponin concentrations should be evaluated for coronary artery abnormalities and, in rare cases, for spontaneous coronary artery dissection.
Managing Myocarditis in the Emergency Department
Initial treatment of myocarditis is aimed at supporting cardiac output. Pediatric heart failure guidelines suggest milrinone or dobutamine as first-line agents for children with decompensated heart failure, with epinephrine reserved for patients with refractory hypotension and poor end-organ perfusion [17]. Dosages of epinephrine should be escalated cautiously because of its propensity to increase myocardial oxygen consumption. Respiratory support with noninvasive positive-pressure or mechanical ventilation is often necessary for patients with hemodynamic compromise during the acute phase. Mechanical circulatory support , including extracorporeal membrane oxygenation or ventricular assist devices, should be considered, particularly in patients with fulminant myocarditis, because 70–90% of these patients recover cardiac function and are transplant-free at long-term follow-up [15]. Antiarrhythmic medications may be necessary in the acute phase. Digoxin is not recommended in this phase because it has increased myocardial injury in animal studies [15]. Patients in this phase with less-severe symptoms at presentation but concerns for myocarditis should be admitted to the hospital given the possibility of ventricular arrhythmias. All patients with myocarditis should be seen by a cardiologist, especially in the event of ventricular dysfunction, arrhythmias, or hemodynamic compromise.
Ongoing Management of Myocarditis
Myocarditis is typically diagnosed definitively after the patient is stabilized in the emergency department. Historically, the gold standard for suspected myocarditis was an endomyocardial biopsy that met certain histologic criteria. However, biopsy-derived diagnoses can be challenging because of the nonuniform inflammation of the myocardium, as well as the risk associated with biopsy in very young patients and during the acute phase of illness. Cardiac MRI is increasingly used in cases of suspected myocarditis. New MRI diagnostic criteria, known as the Lake Louise criteria, can be used to diagnose myocarditis. These criteria are based on MRI evidence of myocardial inflammation on T2 signaling, global early gadolinium enhancement, or focal late gadolinium enhancement [18].
Ongoing evaluation of cardiac function is essential to determine appropriate therapies. Fluid status should be monitored carefully, and IV loop diuretics are first-line treatment for patients with fluid overload. Patients with persistent heart failure are commonly transitioned to treatments that often include angiotensin converting enzyme inhibitors and beta-blockers. In murine models, both of these drugs were associated with decreased inflammation, myocardial fibrosis, and autoantibody production [15]. Aldosterone antagonists may also be considered for patients with persistent heart failure symptoms based on improved survival in studies of adults. Escalation or weaning of clinical support is based on the clinical response to treatment.
Patients presenting with acute or fulminant myocarditis are commonly treated with IVIG and, less frequently, with steroids despite limited efficacy data. Among children enrolled in the National Heart, Lung, and Blood Institute-funded Pediatric Cardiomyopathy Registry, the use of IVIG did not improve LV function or survival [15]. The use of immunomodulator therapy and specific regimens vary by institution.
Complications of Myocarditis
The most important complications of myocarditis include persistent cardiac dysfunction, chronic heart failure, and persistent and/or progressive heart failure requiring consideration of heart transplantation. Cardiac transplant rates in patients with myocarditis range from 4 to 18%. Most children with myocarditis will recover normal cardiac function with about half regaining a normal ejection fraction after 3 years [15].
Myocarditis Clinical Pearls
-
The clinical presentation of myocarditis is variable and may include acute-onset chest pain, progressive heart failure, or sudden death
-
Troponin concentrations are more commonly elevated than are creatine kinase concentrations, but cardiac biomarkers may be negative
-
Electrocardiographic changes in myocarditis include ST segment changes, low-voltage QRS complexes, heart block, or abnormal Q waves
-
Patients in whom myocarditis is suspected should be admitted during the acute phase and monitored for cardiac arrhythmias
-
Cardiology consultation should be sought for patients with myocarditis
References
Marijon E, Mirabel M, Celermajer DS, Jouven X. Rheumatic heart disease. Lancet. 2012;379(9819):953–64.
Tani LY. Rheumatic fever and rheumatic heart disease. In: Allen HD, Shaddy RE, Penny DJ, Cetta F, Feltes TF, editors. Moss and Adams’ heart disease in infants, adolescents, and children, including the fetus and young adult. 9th ed. Philadelphia: Wolters Kluwer; 2016. p. 1373–404.
Gewitz MH, Baltimore RS, Tani LY, et al. Revision of the Jones criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography a scientific statement from the American Heart Association. Circulation. 2015;131:1806–18.
Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–71.
Kanegaye JT, Wilder MS, Molkara D, et al. Recognition of a Kawasaki disease shock syndrome. Pediatrics. 2009;123:e783–9.
Printz BF, Sleeper LA, Newburger JW, et al. Noncoronary cardiac abnormalities are associated with coronary artery dilation and with laboratory inflammatory markers in acute Kawasaki disease. J Am Coll Cardiol. 2010;57:86–92.
Turnier JL, Anderson MS, Heizer HR, Jone P-N, Glode MP, Dominguez SR. Concurrent respiratory viruses and Kawasaki disease. Pediatrics. 2015;136:e609–14.
Newburger J, Takahashi M, Burns JC, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med. 1986;315:341–7.
Cohen E, Sundel R. Kawasaki disease at 50 years. JAMA Pediatr. 2016;170(11):1093–9.
Newburger JW, Takahashi M, Burns JC. Kawasaki disease. J Am Coll Cardiol. 2016;67:1738–49.
Canter CE, Simpson KP. Diagnosis and treatment of myocarditis in children in the current era. Circulation. 2014;129:115–28.
Sagar S, Liu PP, Cooper LT. Myocarditis. Lancet. 2012;379:738–47.
Cooper LT. Myocarditis. N Engl J Med. 2009;360:1526–38.
Caforio ALP, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34:2636–48.
Simpson KE, Anwar S, Canter CE. Myocarditis. In: Allen HD, Shaddy RE, Penny DJ, Feltes TF, Cetta F, editors. Moss and Adams’ heart disease in infants, adolescents, and children, including the fetus and young adult. 9th ed. Philadelphia: Wolters Kluwer; 2016. p. 1313–30.
Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death—addenda. Eur Heart J. 2015;36:2793–867.
Kirk R, Dipchand AI, Rosenthal DN, et al. The International Society for Heart and Lung Transplantation guidelines for the management of pediatric heart failure: executive summary. J Hear Lung Transplant. 2014;33:888–909.
Friedrich MG, Sechtem U, Schulz-Menger J, et al. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol. 2009;53:1475–87.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this chapter

Cite this chapter
Ware, A.L., Truong, D.T., Tani, L.Y. (2018). Inflammatory Heart Diseases in Children. In: Sarnaik, A., Ross, R., Lipshultz, S., Walters III, H. (eds) Cardiac Emergencies in Children. Springer, Cham. https://doi.org/10.1007/978-3-319-73754-6_19
Download citation
DOI: https://doi.org/10.1007/978-3-319-73754-6_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-73753-9
Online ISBN: 978-3-319-73754-6
eBook Packages: MedicineMedicine (R0)