
Abstract
The prevalence rate of ADHD varies from age to age. To better understand the development of ADHD from childhood to adolescence, different age groups of ADHD from large dataset are needed to explore the development pattern of brain activities. In this study, amplitude of low frequency fluctuation (ALFF), fractional amplitude of low frequency fluctuation (fALFF) and regional homogeneity (ReHo) were extracted from resting-state functional magnetic resonance imaging (rs-fMRI) of both ADHD subjects and typical developing (TD) subjects from 7 to 16 years old. The result showed that the different areas mainly appear at the bilateral superior frontal cortex, anterior cingulate cortex (ACC), precentral gyrus, right superior occipital lobe, cerebellum and parts of basal ganglia between all ADHD subjects and all TD subjects. Besides, compared with TD, there were different brain activity patterns at different ages in ADHD, which appear at the left ACC and left occipital lobe. The result can inspire more studies on comparisons between functional connectivity methods.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Attention deficit hyperactivity disorder (ADHD) is generally considered to be a neurodevelopmental disorder with high incidence in childhood [1, 2]. It is mainly characterized by lack of attention, excessive activity (restless in adult), or difficulty controlling behavior which is not appropriate for a person’s age [3]. It was estimated that the prevalence of ADHD in pre-school children (3–6 years old) in Europe is 1.8–1.9% [4]. Although there is no global consensus, meta-regression analyses have estimated the worldwide ADHD prevalence at between 5.29% and 7.1% in children and adolescents, and at 3.4% in adults [5,6,7]. In addition, about 30–50% of people diagnosed with ADHD in childhood continue to have symptoms into adulthood and about 2–5% of adults also have the symptoms [8]. Since the incidence of ADHD varies between ages, in order to understand the development of ADHD from childhood to adolescence, it is necessary to explore the difference patterns of regional brain activities between ADHD subjects and typical developing (TD) subjects from different age groups.
Functional magnetic resonance imaging (fMRI) has been widely used to measure brain activities in-vivo. Compared to the task-related fMRI, resting-state fMRI (rs-fMRI) does not require subject to perform any task, which greatly simplifies the fMRI procedure for patients with difficulty to accomplish certain tasks. Brain activity could be characterized by different measurements, such as amplitude of low frequency fluctuation (ALFF), fractional amplitude of low frequency fluctuation (fALFF) and regional homogeneity (ReHo). Since Zang et al. [9] applied ALFF to probe the abnormal spontaneous neuronal activities of ADHD patients, ALFF has been widely used in the studies of various mental diseases, such as schizophrenia [10, 11], autism spectrum disorder [12], attention deficit hyperactivity disorder [13]. However, some researchers found that ALFF of ADHD patients increased abnormally in some brain areas but the energy consumption of these regions did not increase correspondingly, which was likely to be caused by noise. Therefore, Zou et al. [14] proposed fALFF to reduce the abnormal value in ALFF. At the same time, Zang et al. [15, 16] firstly proposed the regional homogeneity approach and explored the functional abnormalities of Parkinson’s patients using ReHo. Subsequently, many studies have validated the feasibility of ReHo in the analysis of fMRI data from multiple aspects [17, 18].
The different brain activities between ADHD and TD have been identified in previous studies. For example, comparing the value of ALFF between 17 ADHD boys (7.51 ± 1.96 years old) and 17 matched controls (9.73 ± 1.57 years old), Yang et al. [13] found that ADHD showed higher ALFF in the left superior frontal gyrus and sensorimotor cortex (SMC) as well as lower ALFF in the bilateral anterior, middle cingulate and the right middle frontal gyrus (MFG). Using ALFF and ReHo on a smaller sample, in contrast to 12 controls (12.5 ± 14.1 years old), the 12 ADHD (11 ± 14.8 years old) patients exhibited significant resting-state brain activities in the bilateral VI/VII (BA 17/18/19), left SI (BA 3), left AII (BA 22), bilateral thalamus, left dorsal brainstem and midbrain [19]. For 29 boys with ADHD (11.00 ± 16.50 years old) and 27 matched controls (11.25 ± 14.92 years old), Cao et al. [20] indicated that ReHo of ADHD patients decreased in the frontal–striatal–cerebellar circuits, but increased in the occipital cortex. However, study of ADHD with small sample size is difficult to cover the brain activity patterns of ADHD which vary with age.
In this study, a large rs-fMRI dataset with 266 ADHD subjects and 719 TD subjects from 7 to 16 years old were adopted. ALFF, fALFF and ReHo of each subject were calculated and compared to study the abnormal brain activity of ADHD.
2 Method
2.1 Dataset
Data were acquired from the database–1000 Functional Connectomes Project (1000-FCP) [21]. It is a neuroimaging database that collects resting-state fMRI data from multiple sites. For the TD participants in our study, inclusion criteria included: age from 7 to 16 years old, with no mental disease, image at least cover 95% of brain. Especially, the ADHD data are acquired from the ADHD-200 dataset, which is a sub set of 1000-FCP. It contains resting-state fMRI and anatomical MRI images aggregated across 8 independent imaging sites, which are obtained from children and adolescents with ADHD (ages: 7–21 years old). Finally we got 266 ADHD subjects and 719 TD subjects with age from 7 to 16 years. To further explore the developmental changes of regional brain activities in ADHD, We divided the TD participants and the ADHD participants into two groups respectively, one for childhood from 7 to 11 years old (TD: 407; ADHD: 169) and the other for adolescence from 12 to 16 years of old (TD: 312; ADHD: 97).
2.2 Image Processing
Resting state fMRI data were preprocessed with DPARSF [22]. The first ten time point was removed to avoid magnetization instability. All images were corrected for slice timing to minimize the difference during image acquisition and realigned to the middle volume to avoid excessive head motion. Then, these images were spatially normalized to a standard template (Montreal Neurological Institute) and resampled to 3 mm × 3 mm × 3 mm voxel resolution. Spatial smoothing was performed with a Gaussian kernel of 4 mm full-width at half-maximum (FWHM) to improve the SNR (signal-to-noise ratio). Besides, the mean signal of white matter and cerebrospinal fluid were removed as covariates. After that, linear trend removal as well as band-pass filtering (0.01–0.1 Hz) were also performed. The brain is divided into 90 ROIs by AAL (automated anatomical labeling) atlas [23] in order to further localize the local variation. Finally, ALFF, fALFF and ReHo of each voxel across participants were be calculated with REST [24].
3 Statistics Analysis
All statistics analysis were performed with SPM12 [25].The brain activity measurements (ALFF, fALFF and ReHo) between ADHD and TD are compared by two-sample t-test on each voxel, taking a significant threshold of P < 0.01, with age as covariate, and corrected for multiple comparisons with false discovery rates (FDR). Voxels with P < 0.01 and cluster size > 270 mm3 were regarded to show a significant group difference. We also performed two-sample t-test on ALFF, fALFF and ReHo for childhood and adolescence groups with the method above.
4 Result
4.1 The Comparison of ALFF, fALFF and ReHo Between Two Groups
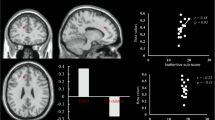
Compared with TD, ADHD showed significant divergence of ALFF, fALFF and ReHo in extensive regions. The main group differences between ADHD and TD on three measures are shown on Table 1 and Fig. 1.

The bright areas mean that the major differences between all ADHD subjects and all TD subjects. (ADHD: Attention deficit hyperactivity disorder group, TD: Typically developing group)
4.2 The Comparison of ALFF, fALFF and ReHo of Two Age Groups
As we can see, there were some subtle but important differences of the three measurements between two groups in childhood and adolescence. The main age groups differences between ADHD and TD on three measures are shown on Table 2 and Fig. 2.

The bright areas mean that the major differences between ADHD and TD in different age groups. (ADHD: Attention deficit hyperactivity disorder group, TD: Typically developing group)
5 Discussion
In this study, three measurements were used to describe the voxel-based local changes in brain activities from different aspects. Firstly, ALFF reflects the level of spontaneous activity of single voxel according to the level of oxygen content, which can directly observe the changes of regional brain activities [9]. Similar to ALFF, fALFF is the ALFF of a given frequency band expressed as a fraction of the sum of amplitudes across the entire frequency range in a given signal, which represents the relative contribution of specific low frequency oscillations to the whole detectable frequency range [26]. Finally, ReHo depicts the coherence of neural activity of a specific brain region with its neighboring or adjacent brain regions [27]. Using the three measurements, we found, after removing the confounding factor age, all ADHD subjects showed abnormal regional activities in the movement pathway and cognitive control circuits, which was in line with previous studies [28, 29]. For all of three measurements, on the one hands, ADHD showed stronger activation than TD in the parts of basal ganglia (caudate nucleus, putamen and pallidum), supplementary motor area, precentral gyrus, cerebellum and thalamus which was related to dysfunction of movement control and execution functions [30, 31]. On the other hands, ADHD exhibited the lower activation than TD in superior occipital lobe in three measurements, which may be associated with attention lapse [32]. Besides, there were its unique activation areas for each index which was mainly concentrated in brain areas involved in advanced cognitive control. For example, the decreased ALFF, fALFF and ReHo appeared in the left superior temporal gyrus, right anterior cingulate cortex and superior frontal cortex respectively.
From the developmental point of view, compared to TD group, the ALFF of left anterior cingulate cortex (ACC) in ADHD group was significantly increased in childhood, which may be connected to compensation mechanism of inattention in ADHD [10]. But in adolescence, there was no significant difference. The result may demonstrate that the degree of ADHD symptoms has improved with age, which could be associated with drug treatment and other factors [33]. As for fALFF, the difference between the two age groups was not very obvious, which was caused by the insensitivity of fALFF to age. Finally, in childhood, the ReHo value of ACC in ADHD was higher than TD, but the differences of ReHo between ADHD and TD disappeared in adolescence. This result suggests that the complex cognitive ability of patients with ADHD has improved with age, specially, in the aspects of regulating stimulus selection and response selection in the attention process [13]. In contrast, the decreased ReHo of ADHD appeared at left inferior occipital lobe in childhood and disappears in adolescence, which could be related to pay attention to multiple irrelevant visual stimuli from the environment simultaneously. Thus, the abnormal activities of ACC and left inferior occipital lobe may jointly result in inattention problems with ADHD [9, 34].
In conclusion, our study shows the abnormal brain activities of ADHD in rs-fMRI which are different from TD using three measurements (ALFF, fALFF and ReHo) from the perspective of development. Moreover, it facilitates our understanding for the mechanism of ADHD and examines the effectiveness of these three measurements. However, there are some limitations in this study. First, the gender factor is not considered, which may affect the result. Second, the division standard of age groups is arbitrary to a certain extent and we still need to explore more suitable criterion. Finally, the source of data is acquired from different institutes, which causes some bias of parameter setting that may influence the further analysis.
References
Sroubek, A., Kelly, M., Li, X.: Inattentiveness in attention-deficit/hyperactivity disorder. Neurosci. Bull. 29(1), 103–110 (2013). doi:10.1007/s12264-012-1295-6
Clauss-Ehlers, C.S. (ed.): Encyclopedia of Cross-Cultural School Psychology. Springer, Boston (2010). doi:10.1007/978-0-387-71799-9
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edn, pp. 59–65. American Psychiatric Publishing, Arlington (2013)
Wichstrøm, L., Berg-Nielsen, T.S., Angold, A., Egger, H.L., Solheim, E., Sveen, T.H.: Prevalence of psychiatric disorders in preschoolers. J. Child Psychol. Psychiatry 53(6), 695–705 (2012). doi:10.1111/j.1469-7610.2011.02514.x
Polanczyk, G., de Lima, M.S., Horta, B.L., Biederman, J., Rohde, L.A.: The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am. J. Psychiatry 164(6), 942 (2007). doi:10.1176/ajp.2007.164.6.942
Fayyad, J., De, G.R., Kessler, R., Alonso, J., Angermeyer, M., Demyttenaere, K., et al.: Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br. J. Psychiatry 190(5), 402–409 (2007). doi:10.1192/bjp.bp.106.034389
Willcutt, E.G.: The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurother. J. Am. Soc. Exp. Neurother. 9(3), 490–499 (2012). doi:10.1007/s13311-012-0135-8
Ginsberg, Y., Quintero, J., Anand, E., Casillas, M., Upadhyaya, H.P.: Underdiagnosis of attention-deficit/hyperactivity disorder in adult patients: a review of the literature. Primary Care Companion J. Clin. Psychiatry 16(3), 470–472 (2014). doi:10.1007/s13311-012-0135-8
Zang, Y.F., He, Y., Zhu, C.Z., Cao, Q.J., Sui, M.Q., Liang, M., et al.: Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev. 29(2), 83–91 (2007). doi:10.1016/j.braindev.2006.07.002
Welsh, R.C., Chen, A.C., Taylor, S.F.: Low-frequency BOLD fluctuations demonstrate altered thalamocortical connectivity in schizophrenia. Schizophr. Bull. 36(4), 713 (2010). doi:10.1093/schbul/sbn145
Yu, R., Chien, Y.L., Wang, H.L., Liu, C.M., Liu, C.C., Hwang, T.J., et al.: Frequency-specific alternations in the amplitude of low-frequency fluctuations in schizophrenia. Hum. Brain Mapp. 35(2), 627–637 (2014). doi:10.1002/hbm.22203
Itahashi, T., Yamada, T., Watanabe, H., Nakamura, M., Ohta, H., Kanai, C., et al.: Alterations of local spontaneous brain activity and connectivity in adults with high-functioning autism spectrum disorder. Mol. Autism 6(1), 30 (2015). doi:10.1186/s13229-015-0026-z
Yang, H., Wu, Q.Z., Guo, L.T., Li, Q.Q., Long, X.Y., Huang, X.Q., et al.: Abnormal spontaneous brain activity in medication-naive ADHD children: a resting state fMRI study. Neurosci. Lett. 502(2), 89–93 (2011). doi:10.1016/j.neulet.2011.07.028
Zou, Q.H., Zhu, C.Z., Yang, Y., Zuo, X.N., Long, X.Y., Cao, Q.J., et al.: An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J. Neurosci. Methods 172(1), 137–141 (2008). doi:10.1016/j.jneumeth.2008.04.012
Zang, Y., Jiang, T., Lu, Y., He, Y., Tian, L.: Regional homogeneity approach to fMRI data analysis. Neuroimage 22(1), 394–400 (2004). doi:10.1016/j.neuroimage.2003.12.030
Wu, T., Long, X., Zang, Y., Wang, L., Hallett, M., Li, K., et al.: Regional homogeneity changes in patients with Parkinson’s disease. Hum. Brain Mapp. 30(5), 1502 (2009). doi:10.1002/hbm.20622
Jiang, L., Xu, T., He, Y., Hou, X.H., Wang, J., Cao, X.Y., et al.: Toward neurobiological characterization of functional homogeneity in the human cortex: regional variation, morphological association and functional covariance network organization. Brain Struct. Funct. 220(5), 2485–2507 (2015). doi:10.1007/s00429-014-0795-8
Liu, Y., Wang, K., Yu, C., He, Y., Zhou, Y., Liang, M., et al.: Regional homogeneity, functional connectivity and imaging markers of Alzheimer’s disease: a review of resting-state fMRI studies. Neuropsychologia 46(6), 1648–1656 (2008). doi:10.1016/j.neuropsychologia.2008.01.027
Tian, L., Jiang, T., Liang, M., Zang, Y., He, Y., Sui, M., et al.: Enhanced resting-state brain activities in ADHD patients: a fMRI study. Brain Develop. 30(5), 342–348 (2008). doi:10.1016/j.braindev.2007.10.005
Cao, Q., Zang, Y., Sun, L., Sui, M., Long, X., Zou, Q., et al.: Abnormal neural activity in children with attention deficit hyperactivity disorder: a resting-state functional magnetic resonance imaging study. NeuroReport 17(17), 1033–1036 (2006). doi:10.1097/01.wnr.0000224769.92454.5d
1000 Functional Connectomes Project. http://fcon_1000.projects.nitrc.org/
Data Processing Assistant for Resting-State fMRI. http://www.restfmri.net/forum/DPARSF
Tzouriomazoyer, N., Landeau, B., Papathanassiou, D., Crivello, F., Etard, O., Delcroix, N., et al.: Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 15(1), 273 (2002). doi:10.1006/nimg.2001.0978
Resting-State fMRI Data Analysis Toolkit. http://www.restfmri.net/forum/REST
Statistical Parametric Mapping. http://www.fil.ion.ucl.ac.uk/spm/
Wei, C., Ji, X., Jie, Z., Feng, J.: Individual classification of ADHD patients by integrating multiscale neuroimaging markers and advanced pattern recognition techniques. Front. Syst. Neurosci. 6, 58 (2012). doi:10.3389/fnsys.2012.00058
An, L., Cao, Q.J., Sui, M.Q., Sun, L., Zou, Q.H., Zang, Y.F., et al.: Local synchronization and amplitude of the fluctuation of spontaneous brain activity in attention-deficit/hyperactivity disorder: a resting-state fMRI study. Neurosci. Bull. 29(5), 603–613 (2013). doi:10.1007/s12264-013-1353-8
Posner, J., Park, C., Wang, Z.: Connecting the dots: a review of resting connectivity MRI studies in attention-deficit/hyperactivity disorder. Neuropsychol. Rev. 24(1), 3–15 (2014). doi:10.1007/s11065-014-9251-z
Tibbetts, P.E.: Cognitive neuroscience: the biology of the mind. Q. Rev. Biol. (2009). doi:10.1086/603482
Conn, P.J., Battaglia, G., Marino, M.J., Nicoletti, F.: Metabotropic glutamate receptors in the basal ganglia motor circuit. Nat. Rev. Neurosci. 6(10), 787–798 (2005). doi:10.1038/nrn1763
Devinsky, O., Morrell, M.J., Vogt, B.A.: Contributions of anterior cingulate cortex to behaviour. Brain 118(1), 279 (1995). doi:10.1093/brain/118.1.279
Posner, M.I., Petersen, S.E.: The attention system of the human brain. Annu. Rev. Neurosci. 13(1), 25 (1990). doi:10.1146/annurev.ne.13.030190.000325
Shang, C.Y., Yan, C.G., Lin, H.Y., Tseng, W.Y., Castellanos, F.X., Gau, S.S.: Differential effects of methylphenidate and atomoxetine on intrinsic brain activity in children with attention deficit hyperactivity disorder. Psychol. Med. 46(15), 3173 (2016). doi:10.1017/S0033291716001938
Cubillo, A., Halari, R., Ecker, C., Giampietro, V., Taylor, E., Rubia, K.: Reduced activation and inter-regional functional connectivity of fronto-striatal networks in adults with childhood attention-deficit hyperactivity disorder (ADHD) and persisting symptoms during tasks of motor inhibition and cognitive switching. J. Psychiatr. Res. 44(10), 629–639 (2010). doi:10.1016/j.jpsychires.2009.11.016
Acknowledgements
This paper was supported by NFSC (National Natural Science Foundation of China) (Grant No. 61403148).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper

Cite this paper
Tang, C., Wei, Y., Zhao, J., Zhang, X., Nie, J. (2017). Abnormal Brain Activity in ADHD: A Study of Resting-State fMRI. In: Zeng, Y., et al. Brain Informatics. BI 2017. Lecture Notes in Computer Science(), vol 10654. Springer, Cham. https://doi.org/10.1007/978-3-319-70772-3_17
Download citation
DOI: https://doi.org/10.1007/978-3-319-70772-3_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-70771-6
Online ISBN: 978-3-319-70772-3
eBook Packages: Computer ScienceComputer Science (R0)