
Abstract
Although patch testing is regarded to be the most standardized and reliable method for diagnosis of delayed-type hypersensitivity to contact allergens, its substitution by in vitro techniques would be advantageous for several reasons.
The lymphocyte transformation test (LTT) measures the allergen-specific proliferation or activation of T cells in vitro and has been explored as potential alternative for patch testing for decades. Beside numerous attempts to increase its sensitivity and specificity, the major drawback of a cell culture-based method is the poor solubility of many contact sensitizers and the need for chemical modification of prohaptens.
The LTT is used with regularity only for diagnosis of hypersensitivity to beryllium and adverse reactions to drugs. Its usefulness in occupational dermatology is limited and restricted to special situations as a supplement for patch testing with large panels of well-established sensitizers.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Patch testing
- Lymphocyte transformation test
- Delayed-type hypersensitivity
- Beryllium
- Drug hypersensitivity
- In vitro testing
- MELISA
- Nickel
- Mercury
- T cells
- ELISpot
- Cytokines
- Cell proliferation
- Sensitivity
- Specificity
1 Core Messages
-
Patch testing is a standardized and reliable method for diagnosis of delayed-type hypersensitivity
-
In vitro testing is demanded as substitute for in vivo testing for several reasons.
-
The lymphocyte transformation test (LTT) is the most methodologically sound technique for in vitro testing.
-
Its specificity and sensitivity in comparison to patch testing as gold standard are dissatisfying.
-
The LTT is used with regularity only for diagnosis of hypersensitivity to beryllium and drugs.
-
Routine patch testing with a large panel of contact sensitizers cannot be substituted by in vitro techniques.
2 Introduction
Patch testing is regarded to be the most standardized and reliable method for diagnosis of delayed-type hypersensitivity to contact allergens. Although the method is indispensable for daily differential diagnosis of contact eczema, the development of in vitro tests for contact hypersensitivity is demanded as substitute or supplement for the in vivo exposure of patients to contact allergens. Concerns raised on patch testing can be summarized as follows:
-
1.
The clinical signs of eczema provoked by contact to an irritating or sensitizing compound are more or less nonspecific. A doubtless differentiation between allergic and irritant contact eczema using clinical, histological, and even molecular criteria is impossible. Additional indices obtained from in vitro tests should help to categorize a questionable compound as sensitizer or irritant in general and aid for proper diagnosis in single cases.
-
2.
The responsiveness of the skin during patch testing is augmented by inflammation and eczema even outside of the test area, critically. Therefore, patch testing is not recommended in chronic eczema or early after episodes of allergic contact dermatitis. In practice, this rule has to be broken in patients with persisting or frequently relapsing eczema. Patch test results obtained under such conditions need to be interpreted very cautiously, due to frequent false-positive reactions. In vitro testing might help to discriminate between a relevant sensitization and artifacts.
-
(a)
Beside factors related to the clinical situation of the patient, patch testing may be restricted by chemical or toxicological features of the allergen itself (cancerogenicity, teratogenicity, boosting of sensitization, iatrogenic sensitization). These hazards would be avoided by the use of an in vitro technique.
-
(a)
3 State of the Art of In Vitro Testing for Delayed-Type Hypersensitivity
Allergic contact eczema is the clinical manifestation of a delayed-type hypersensitivity reaction. The initial inflammatory signal depends on the specific activation of effector T cells, and an ideal in vitro test should spot this process with the same specificity and sensitivity as patch testing. T cell receptors recognize haptens covalently or noncovalently bound to peptides in the binding grove of MHC molecules. Every prerequisite and component necessary to build these target structures has to be provided in the in vitro situation; otherwise T cell activation fails. Any secondary process or signal specifically induced by this activation should be suitable as endpoint for an in vitro test. During an early stage of understanding the immunology of delayed-type hypersensitivity , methods like the migration inhibition test and procoagulant activity assay were explored. They have been replaced by techniques for the direct analysis of cell proliferation and cytokine production.
The detection of cell proliferation in cultures of mononuclear blood-derived cells is now the mostly accepted and well-referenced method of choice and named as lymphocyte transformation test (LTT), or the synonyms lymphocyte proliferation test (LPT) and lymphocyte activation test (LAT).
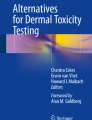
The LTT is poorly standardized, and several modifications have been suggested and explored to improve its sensitivity and specificity. Main technical aspects are summarized in Fig. 1.

Basic principle and modifications of the lymphocyte transformation test. PBMC peripheral blood mononuclear cells, BrdU bromodeoxyuridine, CFSE carboxyfluorescein diacetate succinimidyl ester
Peripheral blood mononuclear cells (PBMC) are prepared from heparinized blood by density gradient centrifugation. Although few groups use separation techniques for enrichment of antigen-presenting cells or T cells (Räsänen et al. 1991), most often, PBMC are stimulated with haptens, directly. One modification of the LTT is called MELISA (Stejskal et al. 1994). The technique avoids the use of heparin and utilizes a preculture of PBMC to minimize the amount of monocytes. Whether this technique is superior to the common LTT protocol is being controversially discussed (Cederbrant et al. 1997; Valentine-Thon et al. 2006).
To support the proliferation of activated T cells, cytokines like IL-4, IL-7, and IL-12 have been added. This results in a substantial improvement of sensitivity not even for nickel sulfate, which has become a model allergen in many studies, but also for other common allergens of the standard patch test series (Moed et al. 2005; Spiewak et al. 2007).
Most authors recommend the titration of haptens, some remove the antigen after short-term stimulation, but most ensure its presence during short-term culture for 3–7 days under sterile cell culture conditions. The most common method to quantify cell proliferation is the incorporation of [3H]thymidine or bromodeoxyuridine (BrdU ), alternatively. If the fluorescence marker carboxyfluorescein diacetate succinimidyl ester (CFSE) is added at the beginning of cell culture, its dilution by cell division can be quantified using flow cytometry. In addition, a selective analysis of surface markers of these dividing cells helps to identify subgroups of responding T cells (Milovanova et al. 2004). A similar analysis of T cell subgroups can be achieved by selective flow cytometric quantification of BrdU incorporation into the DNA of proliferating cells (Farris et al. 2000) or screening for the proliferation marker Ki-67 (Popple et al. 2016).
Beside cell proliferation, secretion of cytokines like IL-5 and interferon γ may be quantified by MELISA or following a modified protocol by the use of the ELISpot technique (Jakobson et al. 2002; Lindemann et al. 2003; Masjedi et al. 2003; Bordignon et al. 2008). Positive control mitogens or recall antigens like tetanus toxoid or candida antigens are used.
The results of the proliferation assays are presented as stimulation indexes calculated from the quotient of stimulated versus control cells. Cytokine levels are depicted as absolute values and ELISpot data as number of cytokine-secreting cells.
The LTT is validated by comparison to patch test results as gold standard. By this measure, sensitivity and specificity vary as a function of the hapten, method, and investigator. False-negative as well as false-positive results, especially those seen for metal salts, cannot be controlled without patch test results for comparison. Because in vitro testing has its indication when patch testing is impossible or produces doubtful reactions, its results should be rated as part of the complete diagnostic procedure but never as ultimate proof or exclusion of a clinically relevant sensitization.
4 The Limits of In Vitro Test Systems
The activation of effector T cells in a highly sensitive in vitro test system is a proof for the existence of these cells but not for clinically relevant contact hypersensitivity. Nowadays, a missing reaction to a contact allergen is rated not only as exclusion of a sensitization but also as possible reflection of a state of tolerance. The immune system might react to the hapten upon contact but does not allow the development of allergic contact dermatitis. An efficient in vitro test has to model this complex and as yet only incompletely understood process in detail; otherwise false-positive results are produced, inevitably. And indeed, for nickel sulfate and mercury, it has been demonstrated that many patients without nickel allergy (Lisby et al. 1999) or patch test reaction to mercury (Cederbrant et al. 1999) showed a positive response in the LTT.
The immunogenic hapten-peptide complex necessary for the restimulation of effector T cells is formed in the skin. Whether this process takes place in an aqueous cell culture system needs to be shown for every single allergen. Problems may arise for hydrophobic or completely water-insoluble compounds as well as for prohaptens (Chipinda et al. 2011). The latter are precursors of the actual allergen and formed by chemical modification in the skin but not necessarily in a cell culture system (Krasteva et al. 1993). An insufficient formation of the relevant hapten-peptide structure may be the main reason for false-negative results of the LTT.
5 Occupational Contact Sensitizers Studied with LTT Techniques
The LTT is not used routinely for diagnostics in occupational dermatology. But it is an important tool for early diagnosis of the granulomatous lung disorder chronic beryllium disease (CBD) (Mroz et al. 2009; Middleton and Kowalski 2010; Fireman et al. 2016). Due to the lack of standardized in vivo tests for drug hypersensitivity, the method is used in cases of an expected delayed-type mechanism (Pichler and Tilch 2004; Merk 2005; Kano et al. 2007; Doña et al. 2017) and has been explored for diagnosis of suspected occupational hypersensitivity to drugs in workers of pharmaceutical plants (Stejskal et al. 1986; Riviera et al. 1995; Ghatan et al. 2014). Most studies for evaluation of the LTT have been performed using a very common contact sensitizer like nickel (Ständer et al. 2017). In contrast, the number of studies describing a valuable contribution of in vitro testing for the diagnostic procedure in occupational dermatology is limited.
Table 1 lists occupational contact sensitizers which have been examined in the LTT as well as further studies covering allergens with relevance for occupational dermatology.
6 Conclusive Remarks on the Role of In Vitro Tests for Delayed-Type Sensitivity in Occupational Dermatology
Due to an inacceptable sensitivity and specificity, high costs, and the need for laboratory infrastructure, the LTT, including its modifications as well as any other in vitro technique, is not suitable as substitute or confirmation for routine patch testing with a large panel of contact sensitizers.
On the other side, if in vivo methods are inapplicable or generate doubtful results, the LTT may be useful for specialized centers as a supplement for diagnosis.
Irrespectively of the limited usefulness for clinical purpose, in vitro techniques offer fascinating opportunities for scientific studies and should help to further uncover basic molecular mechanism of delayed-type hypersensitivity.
Abbreviations
- BrdU:
-
Bromodeoxyuridine
- LTT:
-
Lymphocyte transformation test
- PBMC:
-
Peripheral blood mononuclear cells
References
Bordignon V, Palamara F, Cordiali-Fei P, Vento A, Aiello A, Picardo M, Ensoli F, Cristaudo A (2008) Nickel, palladium and rhodium induced IFN-gamma and IL-10 production as assessed by in vitro ELISpot-analysis in contact dermatitis patients. BMC Immunol 9:19. https://doi.org/10.1186/1471-2172-9-19
Bordignon V, Palamara F, Altomonte G, Sperduti I, Pietravalle M, Cavallotti C, Cordiali-Fei P, Fuggetta MP, Cristaudo A, Ensoli F (2015) A laboratory test based on determination of cytokine profiles: a promising assay to identify exposition to contact allergens and predict the clinical outcome in occupational allergic contact dermatitis. BMC Immunol 16:4. https://doi.org/10.1186/s12865-015-0066-3
Brand CU, Schmidli J, Ballmer-Weber B, Hunziker T (1995) Lymphocyte stimulation test, a possible alternative for verifying chloroacetophenone sensitization. Hautarzt 46:702–704
Byers VS, Castagnoli N Jr, Epstein WL (1979) In vitro studies of poison oak immunity. II. Effect of urushiol analogues on the human in vitro response. J Clin Invest 64:1449–1456
Cederbrant K, Hultman P, Marcusson JA, Tibbling L (1997) In vitro lymphocyte proliferation as compared to patch test using gold, palladium and nickel. Int Arch Allergy Immunol 112:212–217
Cederbrant K, Gunnarsson LG, Hultman P, Norda R, Tibbling-Grahn L (1999) In vitro lymphoproliferative assays with HgCl2 cannot identify patients with systemic symptoms attributed to dental amalgam. J Dent Res 78:1450–1458
Chipinda I, Hettick JM, Siegel PD (2011) Haptenation: chemical reactivity and protein binding. J Allergy (Cairo) 2011:839682. https://doi.org/10.1155/2011/839682
Doña I, Torres MJ, Montañez MI, Fernández TD (2017) In vitro diagnostic testing for antibiotic allergy. Allergy Asthma Immunol Res 9:288–298. https://doi.org/10.4168/aair.2017.9.4.288
Farris GM, Newman LS, Frome EL, Shou Y, Barker E, Habbersett RC, Maier L, Smith HN, Marrone BL (2000) Detection of beryllium sensitivity using a flow cytometric lymphocyte proliferation test: the Immuno-Be-LPT. Toxicology 143:125–140
Fireman E, Shai AB, Alcalay Y, Ophir N, Kivity S, Stejskal V (2016) Identification of metal sensitization in sarcoid-like metal-exposed patients by the MELISA® lymphocyte proliferation test – a pilot study. J Occup Med Toxicol 11:18. https://doi.org/10.1186/s12995-016-0101-1
Ghatan PH, Marcusson-Ståhl M, Matura M, Björkheden C, Lundborg P, Cederbrant K (2014) Sensitization to omeprazole in the occupational setting. Contact Dermatitis 71:371–375. https://doi.org/10.1111/cod.12305
Jakobson E, Masjedi K, Ahlborg N, Lundeberg L, Karlberg AT, Scheynius A (2002) Cytokine production in nickel-sensitized individuals analysed with enzyme-linked immunospot assay: possible implication for diagnosis. Br J Dermatol 147:442–449
Kano Y, Hirahara K, Mitsuyama Y, Takahashi R, Shiohara T (2007) Utility of the lymphocyte transformation test in the diagnosis of drug sensitivity: dependence on its timing and the type of drug eruption. Allergy 62:1439–1444
Kneilling M, Caroli U, Grimmel C, Fischer J, Eichner M, Wieder T, Maier FC, Röcken M, Biedermann T (2010) Para-phenylenediamine-specific lymphocyte activation test: a sensitive in vitro assay to detect para-phenylenediamine sensitization in patients with severe allergic reactions. Exp Dermatol 19:435–441
Krasteva M, Nicolas JF, Chabeau G, Garrigue JL, Bour H, Thivolet J, Schmitt D (1993) Dissociation of allergenic and immunogenic functions in contact sensitivity to para-phenylenediamine. Int Arch Allergy Immunol 102:200–204
Lindemann M, Böhmer J, Zabel M, Grosse-Wilde H (2003) ELISpot: a new tool for the detection of nickel sensitization. Clin Exp Allergy 33:992–998
Lisby S, Hansen LH, Menn T, Baadsgaard O (1999) Nickel-induced proliferation of both memory and naive T cells in patch test-negative individuals. Clin Exp Immunol 117:217–222
Martins LE, Duarte AJ, Aoki V, Nunes RS, Ogusuku S, Reis VM (2008) Lymphocyte proliferation testing in chromium allergic contact dermatitis. Clin Exp Dermatol 33:472–477
Masjedi K, Ahlborg N, Gruvberger B, Bruze M, Karlberg AT (2003) Methylisothiazolinones elicit increased production of both T helper (Th)1- and Th2-like cytokines by peripheral blood mononuclear cells from contact allergic individuals. Br J Dermatol 149:1172–1182
Merk HF (2005) Diagnosis of drug hypersensitivity: lymphocyte transformation test and cytokines. Toxicology 209:217–220
Middleton D, Kowalski P (2010) Advances in identifying beryllium sensitization and disease. Int J Environ Res Public Health 7:115–124
Milovanova TN, Popma SH, Cherian S, Moore JS, Rossman MD (2004) Flow cytometric test for beryllium sensitivity. Cytometry B Clin Cytom 60:23–30
Moed H, von Blomberg M, Bruynzeel DP, Scheper R, Gibbs S, Rustemeyer T (2005) Improved detection of allergen-specific T-cell responses in allergic contact dermatitis through the addition of ‘cytokine cocktails’. Exp Dermatol 14:634–640
Mroz MM, Maier LA, Strand M, Silviera L, Newman LS (2009) Beryllium lymphocyte proliferation test surveillance identifies clinically significant beryllium disease. Am J Ind Med 52:762–773
Pichler WJ, Tilch J (2004) The lymphocyte transformation test in the diagnosis of drug hypersensitivity. Allergy 59:809–820
Popple A, Williams J, Maxwell G, Gellatly N, Dearman RJ, Kimber I (2016) T lymphocyte dynamics in methylisothiazolinone-allergic patients. Contact Dermatitis 75:1–13. https://doi.org/10.1111/cod.12600
Räsänen L, Tuomi ML (1992) Diagnostic value of the lymphocyte proliferation test in nickel contact allergy and provocation in occupational coin dermatitis. Contact Dermatitis 27:250–254
Räsänen L, Sainio H, Lehto M, Reunala T (1991) Lymphocyte proliferation test as a diagnostic aid in chromium contact sensitivity. Contact Dermatitis 25:25–29
Riviera AP, Pezzini A, Zanoni G, Rocca M, Pagani M, Tridente G (1995) Immunological reactivity in ranitidine factory workers. Int Arch Occup Environ Health 66:407–411
Spiewak R, Moed H, von Blomberg BM, Bruynzeel DP, Scheper RJ, Gibbs S, Rustemeyer T (2007) Allergic contact dermatitis to nickel: modified in vitro test protocols for better detection of allergen-specific response. Contact Dermatitis 56:63–69
Ständer S, Oppel E, Thomas P, Summer B (2017) Evaluation of lymphocyte transformation tests as compared with patch tests in nickel allergy diagnosis. Contact Dermatitis 76:228–234. https://doi.org/10.1111/cod.12751
Stejskal VD, Olin RG, Forsbeck M (1986) The lymphocyte transformation test for diagnosis of drug-induced occupational allergy. J Allergy Clin Immunol 77:411–426
Stejskal VD, Forsbeck M, Nilsson R (1990) Lymphocyte transformation test for diagnosis of isothiazolinone allergy in man. J Invest Dermatol 94:798–802
Stejskal VD, Cederbrant K, Lindvall A, Forsbeck M (1994) MELISA-an in vitro tool for the study of metal allergy. Toxicol In Vitro 8:991–1000
Valentine-Thon E, Müller K, Guzzi G, Kreisel S, Ohnsorge P, Sandkamp M (2006) LTT-MELISA is clinically relevant for detecting and monitoring metal sensitivity. Neuro Endocrinol Lett 27(Suppl 1):17–24
Yawalkar N, Helbling A, Pichler CE, Zala L, Pichler WJ (1999) T cell involvement in persulfate triggered occupational contact dermatitis and asthma. Ann Allergy Asthma Immunol 82:401–404
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this entry

Cite this entry
Becker, D. (2020). In Vitro Delayed-Type Sensitivity Testing. In: John, S., Johansen, J., Rustemeyer, T., Elsner, P., Maibach, H. (eds) Kanerva’s Occupational Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-319-68617-2_85
Download citation
DOI: https://doi.org/10.1007/978-3-319-68617-2_85
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-68615-8
Online ISBN: 978-3-319-68617-2
eBook Packages: MedicineReference Module Medicine