
Abstract
Objective: Although secondary insults such as raised intracranial pressure (ICP) or cardiovascular compromise strongly contribute to morbidity, a growing interest can be noticed in how the pre-hospital management can affect outcomes after traumatic brain injury (TBI). The objective of this study was to determine whether pre-hospital co-morbidity has influence on patterns of continuously measured waveforms of intracranial physiology after paediatric TBI.
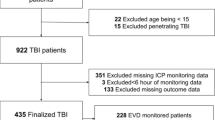
Materials and methods: Thirty-nine patients (mean age, 10 years; range, 0.5–15) admitted between 2002 and 2015 were used for the current analysis. Pre-hospital motor score, pupil reactivity, pre-hospital hypoxia (SpO2 < 90%) and hypotension (mean arterial pressure < 70 mmHg) were documented. ICP and arterial blood pressure (ABP) were monitored continuously with an intraparenchymal microtransducer and an indwelling arterial line. Pressure monitors were connected to bedside computers running ICM+ software. Pressure reactivity was determined as the moving correlation between 30 10-s averages of ABP and ICP (PRx). The mean ICP and PRx were calculated for the whole monitoring period for each patient.
Results: Those with pre-hospital hypotension were susceptible to higher ICP [20 (IQR 8) vs 13 (IQR 6) mmHg; p = 0.01] and more frequent ICP plateau waves [median = 0 (IQR 1), median = 4 (IQR 9); p = 0.001], despite having similar MAP, CPP and PRx during monitoring. Those with unreactive pupils tended to have higher ICP than those with reactive pupils (18 vs 14 mmHg, p = 0.08). Pre-hospital hypoxia, motor score and pupillary reactivity were not related to subsequent monitored intracranial or systemic physiology.
Conclusion: In paediatric TBI, pre-hospital hypotension is associated with increased ICP in the intensive care unit.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others

Keywords
Introduction
Traumatic brain injury is a major cause of morbidity, particularly in children. After the initial injury, secondary injuries, such as raised intracranial pressure (ICP), decreased cerebral perfusion pressure (CPP), impaired cerebral blood flow regulation or hyperthermia, contribute to further intracranial and systemic insult and, importantly, represent a potential avenue for therapy [1]. Thus, in adults and children, prevention of secondary injury forms an integral part of the intensive care management.
Monitoring of ICP affords the opportunity to detect evolving intracranial pathology and monitor the efficacy of ICP-lowering therapies. However, deciding which patients may benefit from ICP monitoring is uncertain, particularly in children. Current guidelines from adults indicate that ICP monitoring should be considered in those with a Glasgow Coma Score of 8 or less, or with an abnormal computed tomography (CT) scan [2].
At the scene of the brain trauma, several features are available that can indicate impaired oxygen delivery to the brain, such as systemic hypoxia and systemic hypotension, or provide an early indication of secondary cerebral dysfunction such as impaired pupillary reactivity or impaired motor response to painful stimuli. How these early clinical features relate to the intracranial variables subsequently monitored on the intensive care unit, such as ICP, cerebral pressure reactivity (PRx), CPP and mean arterial pressure (MAP), is unknown.
Methods
Patients
Thirty-nine patients were recruited from the paediatric intensive care unit at Addenbrooke’s Hospital, Cambridge, UK, between the years of 2002 and 2015. The data are routinely collected for clinical purposes and guides the management of patients. The analysis of data within this study for the purposes of service evaluation was approved by the Cambridge University Hospital NHS Trust, Audit and Service Evaluation Department (Ref. 2143) and did not require ethical approval or patient consent. Patients were included in this cohort if they had a clinical need for ICP monitoring. Patients were treated according to current paediatric traumatic brain injury guidelines [3], which aim to keep the ICP below 20 mmHg through a stepwise regime, including: positioning, sedation, paralysis, osmotic agents, ventriculostomy and induced hypothermia. Pre-hospital clinical features—hypotension (age adjusted [4]), hypoxia (SpO2 < 90%), pupil reactivity and motor score—were extracted from the pre-hospital phase of management (first recorded measure).
Data Acquisition and Analysis
Arterial blood pressure (ABP) was measured at the radial or femoral artery, zeroed at the level of the heart (Baxter Healthcare, Westlake Village, CA, USA; Sidcup, UK). ICP was measured with an intraparenchymal microsensor in the frontal cortex (Codman ICP Micro-Sensor; Codman & Shurtleff, Raynham, MA, USA). ICP and ABP data were collected at 100 Hz with an analogue to digital converter (DT9801, Data Translation, Marlboro, MA, USA) coupled with a laptop computer running ICM+ software (University of Cambridge, Cambridge Enterprise, Cambridge, UK, http://www.neurosurg.cam.ac.uk/icmplus). Pressure reactivity index (PRx) was calculated as the moving correlation between 10-s averages of ICP and ABP. Patients ICP, PRx, mean arterial pressure (MAP) and CPP were then averaged over the first 72 h of their intensive care unit stay.
Statistical Analysis
Mean ICP, PRx, CPP and MAP over the first 3 days of monitoring were calculated. The influence of the presence or absence of prehospital factors (hypotension, hypoxia, more than one unreactive pupil, motor score 3 or less) on subsequent ICP and PRx were tested using a non-parametric Wilcoxon test. All data manipulations and analysis were performed using R language and software environment for statistical computation (version 2.12.1) [5].
Results
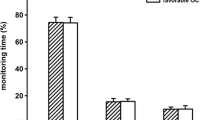
The median age was 12 years (range, 0.5–15). Of the 39 patients, 14 were female, 15 had pre-hospital hypoxia, 9 had pre-hospital hypotension, 7 had at least one unreactive pupil and 12 had a motor score of 3 or less. Those with pre-hospital hypotension had a higher mean ICP over the first 3 days of monitoring (median 13.7, IQR 6.33 vs 20.6, IQR 8.33 mmHg p = 0.01; Fig. 1). Those with unreactive pupils tended to have higher ICP than those with reactive pupils (18.02 vs 13.68 mmHg, p = 0.08). Those with pre-hospital hypotension had more plateau waves, and tended to have a lower power of slow waves of ICP. Pre-hospital clinical factors did not influence subsequently monitored PRx (Table 1), MAP or CPP (data not shown).

Relationship between pre-hospital hypotension and mean ICP after TBI (n = 33). Paediatric TBI patients with pre-hospital hypotension (MAP less than 70 mmHg) had higher mean ICP during subsequent multimodality monitoring
Discussion
In this study, we investigated the relationship between pre-hospital clinical factors and subsequent intracranial physiology after severe traumatic brain injury in children. Children with pre-hospital hypotension went on to develop higher ICP. Pre-hospital hypotension should alert the clinician to the potential for subsequent problems with ICP control.
Pre-hospital hypotension in the setting of traumatic brain injury can have many causes, including blood loss, obstructive shock or a systemic inflammatory response, and its presence has been shown to be an indicator of poor prognosis in both adults and children [6]. After brain trauma, any systemic hypotension reduces cerebral perfusion pressure and thus potentially causes cerebral hypoperfusion and ischaemia.
Against this context, our finding of increased ICP following hypotension could have a variety of causes. It is possible that an early cerebral ischaemia triggers a cascade of events that result in cerebral swelling and raised ICP. In support of this, Marmarou et al. [7] examined the combined effects of hypoxia and hypotension on subsequent brain swelling and found an increased ICP with the combination of early insults.
The tendency of unreactive pupils to be related to ICP is consistent with the thesis that raised intracranial pressure can disrupt the function of the oculomotor nerve. Pre-hospital hypoxia and impaired motor response to pain did not seem to influence subsequent ICP. No pre-hospital factors were related to subsequently monitored PRx, MAP or CPP, perhaps indicating that these factors are more closely related to insults occurring in the intensive care unit rather than before admission to the hospital.
Implications
Early prediction of raised ICP has the potential to facilitate the management of traumatic brain injury patients by alerting the clinicians to patients who require more intensive monitoring or perhaps a lower threshold for ICP treatment. However, prediction remains difficult and is usually confined to analysis of high-frequency ICP waveforms [8]. Thus, the current preliminary findings, if confirmed, could enhance existing ICP prediction tools. In addition, the current data potentially indicate that enhanced pre-hospital care may aid in avoiding secondary insults occurring up to 72 h after admission to hospital. Furthermore, the finding of a relationship between pre-hospital hypotension and subsequent ICP highlights the need to include pre-hospital factors in the analyses between physiological variables and patient outcome.
Limitations
As this current analysis is from quite a small dataset, we cannot exclude that more subtle relationships between pre-hospital factors and ICP or PRx may emerge with a larger dataset [9].
Conclusion
After severe paediatric traumatic brain injury, those patients with pre-hospital hypotension go on to develop higher ICP.
References
Kolias A, Guilfoyle M, Helmy A, et al. Traumatic brain injury in adults. Pract Neurol. 2013;13:228–35.
Brain Trauma Foundation. Guidelines for the management of severe traumatic brain injury, 3rd edition. J Neurotrauma. 2007;24(Suppl 1):S37–44.
Kochanek PM, Carney NA, Adelson PD, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents—second edition. Pediatr Crit Care Med. 2012;13(Suppl):S1–82.
Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S876–908. doi:https://doi.org/10.1161/CIRCULATIONAHA.110.971101
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2015. http://www.r-project.org/.
Pigula FA, Wald SL, Shackford SR, Vane DW. The effect of hypotension and hypoxia on children with severe head injuries. J Pediatr Surg. 1993;28:310–6.
Kita H, Marmarou A. The cause of acute brain swelling after the closed head injury in rats. Acta Neurochir Suppl (Wien). 1994;60:452–5.
Hu X, Xu P, Asgari S, Vespa P, Bergsneider M. Forecasting ICP elevation based on prescient changes of intracranial pressure waveform morphology. IEEE Trans Biomed Eng. 2010;57:1070–8.
Cabella B, Donnelly J, Cardim D, Liu X, Cabeleira M, Smielewski P, Haubrich C, Hutchinson P, Kim DJ, Czosnyka M. An association between ICP-derived data and outcome in TBI patients: the role of sample size. Neurocrit Care. 2017;27(1):103–7.
Conflicts of interest statement
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this paper

Cite this paper
Young, A.M.H. et al. (2018). Pre-hospital Predictors of Impaired ICP Trends in Continuous Monitoring of Paediatric Traumatic Brain Injury Patients. In: Heldt, T. (eds) Intracranial Pressure & Neuromonitoring XVI. Acta Neurochirurgica Supplement, vol 126. Springer, Cham. https://doi.org/10.1007/978-3-319-65798-1_2
Download citation
DOI: https://doi.org/10.1007/978-3-319-65798-1_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-65797-4
Online ISBN: 978-3-319-65798-1
eBook Packages: MedicineMedicine (R0)