
Abstract
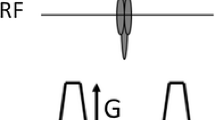
Imaging techniques applied to medical practice depend on two major characteristics: the ability to consistently define anatomically coherent findings and adequate contrast between tissues. MR diffusion-weighted imaging (DWI) uses the signal loss associated with the random thermal motion of water molecules in the presence of magnetic field gradients to derive a quantitative parameter (the so-called apparent diffusion coefficient—ADC) that directly reflects the translational mobility of the water molecules in the tissues [1]. It is fundamentally different from the conventional morphological and hemodynamically based imaging techniques [2]. Early abdominal applications of DWI were limited due to susceptibility effects, suboptimal fat suppression and artifacts related to random and periodic motion [3, 4]. Many of these issues have not been completely solved but are today minimized considering current hardware and software improvements. As such, DWI has become an indispensable day-to-day tool for liver imaging, proving its value on various clinical scenarios, from focal liver lesion detection to characterization and/or diffuse liver disease assessment. Specific advantages consist on its short examination time, independence of exogenous sources of contrast, and the ability to provide qualitative and quantitative information [5, 6]. The following chapter addresses the most common current clinical applications of DWI in the setting of liver malignancies, considering basic methodologies on how to assess diffusion-weighted images in qualitative and quantitative manner and reviewing clinical results for oncologic applications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
3.1 Introduction
Imaging techniques applied to medical practice depend on two major characteristics: the ability to consistently define anatomically coherent findings and adequate contrast between tissues. MR diffusion-weighted imaging (DWI) uses the signal loss associated with the random thermal motion of water molecules in the presence of magnetic field gradients to derive a quantitative parameter (the so-called apparent diffusion coefficient—ADC) that directly reflects the translational mobility of the water molecules in the tissues [1]. It is fundamentally different from the conventional morphological and hemodynamically based imaging techniques [2]. Early abdominal applications of DWI were limited due to susceptibility effects, suboptimal fat suppression and artifacts related to random and periodic motion [3, 4]. Many of these issues have not been completely solved but are today minimized considering current hardware and software improvements. As such, DWI has become an indispensable day-to-day tool for liver imaging, proving its value on various clinical scenarios, from focal liver lesion detection to characterization and/or diffuse liver disease assessment. Specific advantages consist on its short examination time, independence of exogenous sources of contrast, and the ability to provide qualitative and quantitative information [5, 6]. The following chapter addresses the most common current clinical applications of DWI in the setting of liver malignancies, considering basic methodologies on how to assess diffusion-weighted images in qualitative and quantitative manner and reviewing clinical results for oncologic applications.
3.2 Reading DWI: Qualitative Reading
In clinical practice, the information conveyed by DWI is rapidly prone to a qualitative evaluation and, together with the ADC map display is generally sufficient to be used as the reading working strategy. DWI should not be a standalone sequence for interpretation purposes but be integrated and read in conjunction with all the available information arising from the remainder morphological sequences. Tissues with high cellularity such as tumors or abscesses, will display restricted diffusion consisting on hyperintensity on high b values (>400–500 s/mm2) images and low ADC values (less than the normal parenchyma). Conversely, cystic or necrotic tissues will show a signal intensity loss on high b value images and return high ADC values. DWI signal intensity, however, depends not only on water diffusivity, but also on the magnetic properties of the tissue itself. Tissues possessing long T2-relaxation times–such as hemangiomas may remain with high signal on high b values, and high values on ADC mapping (the so-called T2 shine-through effect). Contrarily, lesions with low-signal intensity on T2-w images may not show hyperintensity on DWI even if they have increased cellularity (the so-called T2-black out effect) [5]. Restricted diffusion is a property commonly seen in malignancy but is by no means specific as described before. As it is well known, several malignant liver tumors will tend to show restricted diffusion such as hepatocellular carcinoma, intrahepatic cholangiocarcinoma, or hepatic metastases [5, 7]. Also, ADC values of solid benign lesion can overlap with ADC values of malignant lesion [7, 8].
A schematic overview of possible signal intensity combinations on T2-w, DWI and ADC is provided in the table below.

For malignant lesions, DWI is useful in distinguishing the different components of tumors (cystic and/or necrotic vs solid components). False positives for malignancy may occur from T2 shine-through effect, partial volume averaging or misregistration artifacts (Fig. 3.1). False negatives may also result from metastases of mucin-producing tumors (cystic-like behavior), from well-differentiated tumors (no restriction) and from necrotic tumors (either primarily necrotic or secondary to treatment), and finally when image artifacts conceal focal liver lesions [5].

Hemangioma and shine-through effect. (a) T2-w fat-suppressed image showing the typical light bulb sign. (b) DWI obtained with a b value of 800 s/mm2 reveals pseudo-restriction. (c) ADC map confirms a high ADC value compatible with hemangioma
3.3 Reading DWI: Quantitative Reading of ADC
The ADC of the liver calculated from diffusion acquisition can be appraised by either visual assessment of the ADC map or by drawing regions of interest (ROI) on the ADC maps to record the mean or median ADC values in the tissue of interest. Several problems still exist with the latter approach. A wide variation of values dependent of technical issues renders ADC measurements variable and therefore of limited use in the daily clinical practice. It has been shown that values may vary not only among different equipment vendors but also within the same vendor and even within the same patient [9]. Consequently, these problems should be addressed and overcome in order to derive meaningful comparative results in order to use DWI as a routine biomarker especially for evaluation of tumor response. Also, ADC measurements will vary with other confounder factors such as liver iron deposition, fat, fibrosis and/or changes in microcirculation. Most workstations and many clinical studies provide ADC values based on monoexponential models, with considerable variation of the protocols and proposed b values [5,6,7,8]. These factors also influence the final ADC measurement. As previously stated, diffusion in tissues is more accurately reflected by a bi-exponential model, and thus deriving ADC measurements from monoexponential fitting curves will add to the lack of precision [10,11,12,13,14]. To note that average ADC values does not reflect tumor heterogeneity. Other approaches, such as histogram analysis of a single ROI may prove to be a better depicter of tumor heterogeneity, and it has been investigated as a possible parameter for tumor assessment [15, 16]. Kurtosis, a measurement of the amount of this deviation from the Gaussian behavior in a dimensionless metric called “excess kurtosis,” may assist in the goal of assessing intralesional heterogeneity and has been investigated for tumor follow-up [17].
3.3.1 Lesion Characterization with DWI—A Shift from Classical Qualitative Assessment?
As already stated, DWI interpretation bases itself on the detection of restricted diffusion. This represents an area of high signal on high b values. For instants, ADC of hemangiomas or cysts will tend to be significantly higher than ADC of malignant liver lesions, but ADC values did not allow a confident diagnosis among different types of liver malignancies. Published data attempted to test sensitivity and specificity of parameters derived from IVIM (using bi-exponential models) to characterize focal liver lesion [10]. However, use of the perfusion component of DWI (Dfast) using the IVIM approach [13] showed a sensitivity of 90.1% and specificity of 85.2% for the distinction of HCC from intrahepatic cholangiocarcinoma, thus reflecting the different tumor vascularization. To which extent these results are reproducible or additive to clinical decision process remains unknown. Using the same IVIM approach other authors have tried to derive conclusions regarding HCC differentiation and reported a higher accuracy [10] however conflicting data has also been published on this regard [14]. Despite microperfusion information provided by the IVIM approach of derived data with contrast-enhanced studies seem to lack a good correlation [14] or may be lower, meaning that IVIM perfusion assessment needs to be better understood.
3.4 Application of DWI to Hepatocellular Carcinoma
Detection of HCC is improved by DWI [18], with low b value DWI showing higher sensitivity due to the vascular signal suppression that increases the conspicuity of nearby lesions. The expected impact of DWI for HCC detection has been proved to be lower than the one reported for liver metastases [19]. As recommended by the LI-RADS classification system from the American College of Radiology, the term “restricted diffusion” should be applied to lesions that are hyperintense relative to the surrounding liver when acquired with at least moderate diffusion weighting (e.g., b ≥ 400 s/mm2) and from which the generated ADC map, shows low apparent diffusion coefficient (ADC)—i.e., lower than that of liver by visual estimation. LI-RADS also recommend that if unsure about this feature, it should not be used to perform lesion characterization [20]. In fact, HCC may be difficult to discriminate from the surrounding cirrhotic changes or even dysplastic nodules, as these can have similar behavior and ADC values [6]. Also, it has low sensitivity (range between 62–91%) [21], due to false negatives especially arising from well-differentiated HCC that will tend to show no restriction on DWI in the context of a fibrotic, heterogeneous background liver parenchyma. DWI seems to provide an additional clue regarding the assessment of tumor aggressiveness. Some studies pinpoint a lower ADC in cases of poorly differentiated HCC [22,23,24], thus allowing the distinction of low- from high-grade HCC lesions (Fig. 3.2). Association between low ADC value, aggressiveness, and poor response to treatment (such as chemoembolization, thermal ablation, surgical resection, or anti-angiogenic therapy) including a higher recurrence rate after treatment and consequently poor prognosis, has been described [25,26,27,28]. DWI can be useful in the diagnosis of macrovascular invasion especially in the infiltrative forms of HCC, with the intravascular tumor casts revealing restricted diffusion and hyperintensity on the high b value DWI (Fig. 3.3).

DWI and HCC differentiation. Although sensitivity of DWI to depict HCC remains low, signal intensity on high b value DWI tends to be directly proportional to the degree of tumor differentiation. (a) Moderately differentiated HCC showing DWI restriction (b = 800). (b) Late arterial phase depicting typical wash-in. (c) Well-differentiated HCC showing absence of DWI restriction. (d) Late arterial phase depicting typical wash-in

Hepatocellular carcinoma with extensive portal venous invasion. Tumor thrombosis is clearly depicted on DWI images due to its intrinsic high contrast resolution and black blood effect on normal vessels. (a) T2-w image with portal vein enlargement and high-signal intensity. (b) Tumor casts extending to intrahepatic branches. (c, d) Corresponding DWI images obtained with high b value (b = 800)
DWI in the context of HCC can be beneficial once a DWI positive nodule is recognized but lacks the typical wash-in/washout pattern. Until now, and together with other imaging signs, apart from the vascular behavior, high b value DWI positivity in a nodule otherwise deemed hypovascular in the dynamic study, is one of the ancillary findings that may trigger a closer follow-up of these patients. Hyperintensity on DWI (using high b values) of hypovascular nodules in patients with cirrhosis has been shown to predict progression to hypervascularity, although at a very low rate [23]. LI-RADS is currently the only western classification system that incorporates DWI in the non-invasive diagnosis of liver nodules in cirrhosis, but only as an ancillary feature. It can be used as a “tie-break” rule pointing toward probable malignancy (as well moderate T2 hyperintensity; microscopic fat-containing nodule, T1 hypointensity on the hepatospecific phase, etc.), allowing the upgrade of a suspicious nodule up to but not beyond LR-4.
3.4.1 Assessment of Tumor Response to Treatment (HCC)
Locoregional treatment of HCC results in dynamic changes and lesion remodeling occurring at the site of treatment. DWI can contribute to the diagnosis of residual tumor and should be interpreted in conjunction with the mRECIST criteria (Fig. 3.4). Residual or recurrent tumor will manifest as area/s of low ADC contrarily to nonviable areas that will display high ADC values. In patients with contra-indications to contrast media injection DWI can be offered as an alternative solution for tumor response evaluation. DWI has also the potential to act as a prognostic indicator in patients with HCC. Low pretreatment ADC has been shown to be a risk factor for early HCC recurrence after surgical resection, and to predict a worse response to transarterial chemoembolization (TACE) [25]. Additionally, ADC changes of tumors following TACE were shown to be an independent predictor of overall survival [11]. An increase in ADC 1 month after TACE or radioembolization (TARE) is indicative of a good prognosis [25, 28]. Deriving the perfusion fraction with IVIM although appealing is still a matter of research as an early predictor of response after chemoembolization [28].

Follow-up MR after thermal ablation of HCC. Despite the high signal intensity of the nodule on the T2-w image, both the dynamic study after contrast administration and DWI (b 800 and ADC map) are contributive to affirm complete tumor necrosis. (a) T2-w fat-sat FSE. (b) 3D T1-w GRE at the late arterial phase of liver enhancement. (c) DWI at b 800 s/mm2. (d) Corresponding ADC map visually displaying high ADC of the nodule
Mean ADC measurements may not be an adequate way to assess tumor heterogeneity after treatment. In this sense, kurtosis calculation may be representing more accurately this feature [17]. Kurtosis after HCC treatment performed better than ADC alone, with better sensitivity (85.7% vs 79.6%) and specificity (98% vs 58.3%), for predicting HCC recurrence.
At the time of this writing there is no clear-cut evidence that ADC quantification for tumor response evaluation is superior or just additive to the mRECIST criteria. In fact, it has been shown that contrast-enhanced MRI with subtraction technique shows a more significant correlation with the histopathologic findings concerning the degree of necrosis estimation after TACE, compared with DWI. Adding for this last topic, advanced quantification of the lesion perfusion with analysis of the Ktrans parameter can also be performed but again its clinical relevance remains to be seen.
3.5 Application of DWI to Intrahepatic Cholangiocarcinoma
Intrahepatic cholangiocarcinoma (IHCCK) is the second most common primary hepatic malignant tumor arising from the epithelium of the bile ducts [29]. Sensitivity is expected to be very high, with series reporting all cholangiocarcinomas to be detectable on DW-MR images with restricted diffusion [30]. In the cirrhotic patient it is fundamental for patient management to recognize and differentiate IHCCK from HCC since the former contraindicates liver transplantation due to its very bad prognosis and early tumor relapse. As a rule of thumb, the majority of IHCCK will show restriction to diffusion and low ADC values. A typical sign that has been associated with this tumor type is the presence of a peripheral rim with high b value DWI. In fact, DWI may show a more hyperintense peripheral rim and a larger central hypointense central zone (Fig. 3.5). Pathological correlation reveals that the peripheral rim corresponds to the higher cellularity areas and the inner core to the predominantly fibrotic component of the tumor. This aspect on DWI together with all the remainder imaging descriptors (lobulated contours, rim enhancement in the arterial phase, target appearance on the hepatobiliary phase, capsular retraction, and upstream dilatation of intrahepatic ducts) are consistent with IHCCK. It has been however reported on multivariate logistic regression analysis that only the target appearance on the DWI was a significant and independent variable predictive of ICCK, making it the most reliable imaging feature for distinction of small mass forming IHCC from small HCC [31, 32]. Other ancillary findings (such as capsule or enhancing septa) would favor HCC [32].

Intrahepatic cholangiocarcinoma typical pattern on contrast-enhanced MR and DWI. The last sequence allows to differentiate the peripheral cellular area showing restriction and the central zone where the less cellular fibrous tumor stroma is predominantly located. (a) DWI with b = 800 s/mm2. (b) 3D GRE T1-w at the arterial phase of liver enhancement
3.6 Application of DWI in Liver Metastasis
Hepatic metastases usually demonstrate low ADC except if totally necrotic, calcified (before or after treatment), or derived from mucin-producing tumors (Fig. 3.6) [5, 7, 33].

Pseudo-shine-through effect in patient with colorectal cancer liver metastasis. The primary tumor was a mucin-producing adenocarcinoma. (a) T2-w fat-sat image showing the right lobe liver metastasis with similar signal intensity to the spleen. (b) DWI with b800 s/mm2. (c) Corresponding ADC map revealing a high ADC value of the liver metastasis in line with the mucinous content
Radiologists should be aware that focal liver abscesses, due to its cellular debris and exudates, will return low ADC values and, in the absence of clinical or laboratory findings, can be confused with metastatic liver disease (Fig. 3.7). There is now abundant evidence of the role of DWI in detection and locoregional staging of metastatic liver disease.

Liver abscess displaying marked restriction on DWI. (a) DWI with b = 800 s/mm2. (b) Low-signal intensity on the ADC map. (c) GRE T1-w dynamic image showing the typical peripheral enhancement and perilesional perfusion abnormalities
As stated from a recent consensus report from the seventh International Forum for Liver Magnetic Resonance Imaging, the combination of hepatobiliary phase images with DW-MR images yields a higher detection rate, particularly in the setting of sub-centimeter liver metastasis [34]. In a meta-analysis dealing with DWI in liver metastases, there was no difference between DWI and Gd-enhanced studies concerning detection rate [19]. In this study however, Gd-enhanced studies were pooled between extracellular and liver-specific contrast agents. Another meta-analysis, based on 39 articles including a large population (nearly 2000 patients with nearly 4, 000 liver metastases) shows that the sensitivity of combined MR (DWI + Gd-EOB-DTPA) is significantly higher than either of the two techniques interpreted separately [33]. However, and despite its excellent results, DWI alone is less sensitive than gadoxetic acid-enhanced MR imaging for detecting liver metastases in the sub-centimeter range. Some arguments may be expanded concerning the different DW protocols and b values among institutions, that may have impacted results as a potential source of false negative results when compared with the more homogeneous and widespread contrast-enhanced 3D-GRE technique. In fact, highest b values ranged from 400 to 1000 s/mm2, with less than half the studies including low b values.
Mean sensibility and specificity for metastasis detection.
Sensitivity | Specificity | |
|---|---|---|
Mean DW-MR | 82.2% [(95% CI, 69.4–90.4%)] | 90.4% [(95% CI, 82.8–94.8%)] |
Gd-EOB-DTPA | 91.2% [(95% CI, 83.7–95.4%)] | 90.4% [(95% CI, 82.8–94.8%)] |
Combined | 95.0% [(95% CI, 89.9–97.6%)] | 82.4% [(95% CI, 70.5–90.2%)] |
When dealing with detection of liver metastases the use of low and high b values in DWI (in our institution 50–100 and 800 s/mm2) is mandatory as low b value DWI provide higher SNR, are less prone to motion-induced signal loss and suffer less from eddy current-induced distortions, justifying its greater sensitivity. The “black blood” appearance of vessels on DWI, especially on the more anatomical low b value images is an essential component and often, in this setting, DWI is the first sequence to map focal liver lesions. In daily practice a common setting is to use DWI for lesion identification and interpret together low and high b values image sets for detection and characterization.
Since 30% of patients with colorectal liver metastases are surgical candidates, three main goals should be considered in order to offer advanced imaging studies such as hepatobiliary-enhanced MRI:
-
1.
to precisely define the tumor burden
-
2.
to provide accurate lesion mapping
-
3.
to verify resection margins around major vessels
DWI deals well with the first two questions while HBCA-MR, due to its superior SNR and 3D spatial resolution capabilities, provides the answer for the last question. To note that in general, the third question addresses the immediate presurgical information while the first two are related to a prior step of patient management (to map and measure lesions before neoadjuvant therapy). Thus, in the initial evaluation of tumor burden and/or tumor response evaluation DWI is a fundamental step and, at this stage, hepatobiliary CA can be skipped.
Special care should be taken not to overlook the so-called “vanishing metastases” corresponding to a dramatic change of metastasis size or signal intensity after chemotherapy. A study addressing patients with this “disappearing” or “tiny residual metastasis” of colorectal cancer after chemotherapy on DWI or Gd-EOB-DTPA, showed an in situ recurrence rate of 15.7% and 33.2%, respectively, at 2 years [35]. So even if not apparent on DWI, the location of prior liver metastases should be carefully inspected and ultimately resected (Fig. 3.8). An ADC transient reduction 24–48 h after initiation of chemotherapy has been described, thought to result from acute cell swelling and/or reduction of interstitial volume. Further ADC decrease along time may correspond to tumor regrowth, fibrosis or tissue remodeling, together with decreased perfusion [36, 37] Thus, in patients submitted to chemotherapy, ADC changes may differentiate between responders and nonresponders, increasing (as expected) in the responders, a finding that may be detected even after the first cycle [38].

Liver metastasis post-chemotherapy with pathologically proven residual active tumor. The typical imaging findings are lacking, and thus detection and/or characterization may be difficult. Prior comparison is mandatory. (a) The T2-w FS sequence is negative. (b) DWI with b = 800 s/mm2. The lesion is barely perceptible and only a discrete hyperintense rim is disclosed. (c) The metastasis is clearly depicted although tumor viability may be difficult to ascertain
For patients with unresectable CRC liver metastases, tumor burden and lower pretreatment ADC values correlate with worst response to radioembolization with 90Yttrium-microspheres. Lower ADC values (<0.935 × 10−3 mm2/s) were seen in nonresponders before treatment and early ADC changes (within the first 2 months after treatment) meaning increased survival rate [39, 40]. Another interesting observation relates to the histogram analysis of the apparently tumor-free parenchyma. A trend toward larger standard deviation of the parenchyma, and lower ADC values (in the fifth percentile) may be an early predictor of micrometastatic disease [41, 42].
In conclusion, for metastatic liver disease, DWI is highly sensitive for lesion detection, and thus should be routinely and incorporated in every MR liver protocol [43]. DWI increases the accuracy for lesion characterization with the combined reading of two or more b values along with the contrast-enhanced MR study. DWI appears as a potential biomarker for tumor response evaluation albeit unsolved issues such as reproducibility, artifact control and suboptimal SNR.
3.7 Future Directions
Most DW-MR imaging studies have been conducted by using 1.5-T MR systems. 3.0-T are increasingly available, have potential for improved image quality, due to increased SNR provided by 3.0-T fields, which is used to improve spatial resolution, to lower the acquisition time (or both), and enables the use of higher b values, which are more sensitive to diffusion and less sensitive to T2 relaxation time.
In DWI, there can be an up to two-fold increase in SNR but with greater magnetic susceptibility artifacts, image distortion and signal loss, greater conspicuity of metal or gas, particularly, with EPI sequences used in DWI, and incomplete fat saturation [44]. There are also reported significant differences between ADC measurements performed at 1.5 and 3 T. Some of these problems can be reduced with a higher receiver bandwidth and parallel imaging techniques.
3.8 Conclusions
DWI can add potentially useful qualitative and quantitative information to conventional imaging sequences. It is quick, can be easily incorporated to existing protocols, is a nonenhanced technique (performed without the use of gadolinium-based contrast media), thus easy to repeat, is useful in patients with severe renal dysfunction at risk for nephrogenic systemic fibrosis.
Variable field strength, number of b values used for diffusion-weighted imaging in each study, the “IVIM” effect, contribute for lack of homogeneity of results and lack of external validity. This is mostly true for quantitative approaches do DWI. However, regarding qualitative reading, which is the most thoroughly used in clinical practice, there doesn’t seem to be as much variation on the interpretation of findings, on the expected sensibility of detections of malignant lesions (especially metastases). This made it possible for very quick and smooth incorporation of DWI in standard abdominal scanning.
We expect that further standardization will be necessary to ensure reproducibility and implementation of quantitative studies. Furthermore, we believe that more data, other than just ADC values and qualitative parameters will be available. Such data may derive from exploring tumor heterogeneity (“the main reason why we are failing treating cancers after all these years”) as was proposed with implementation of kurtosis. There is also the exploit of IVIM and it’s still to accurately determine molecular findings, a phenomenon which was initially not taken in account for, but presents with a promising field for ability to discriminate focal liver lesions, to predict its behavior or clinical significance in a follow-up, provided reproducibility is ensured.
References
Luypaert R, Boujraf S, Sourbron S, Osteaux M. Diffusion and perfusion MRI: basic physics. Eur J Radiol. 2001;38:19–27.
Muhi A, et al. High-b-value diffusion-weighted MR imaging of hepatocellular lesions: estimation of grade of malignancy of hepatocellular carcinoma. J Magn Reson Imaging. 2009;30:1005–11.
Chandarana H, Taouli B. Diffusion and perfusion imaging of the liver. Eur J Radiol. 2010;76:348–58.
Namimoto T, Yamashita Y, Sumi S, Tang Y, Takahashi M. Focal liver masses: characterization with diffusion-weighted echo-planar MR imaging. Radiology. 1997;204:739–44.
Taouli B, Koh D-M. Diffusion-weighted MR imaging of the liver. Radiology. 2010;254:47–66.
Papanikolaou N, Gourtsoyianni S, Yarmenitis S, Maris T, Gourtsoyiannis N. Comparison between two-point and four-point methods for quantification of apparent diffusion coefficient of normal liver parenchyma and focal lesions. Value of normalization with spleen. Eur J Radiol. 2010;73(2):305–9.
Gourtsoyianni S, Papanikolaou N, Yarmenitis S, Maris T, Karantanas A, Gourtsoyiannis N. Respiratory gated diffusion-weighted imaging of the liver: value of apparent diffusion coefficient measurements in the differentiation between most commonly encountered benign and malignant focal liver lesions. Eur Radiol. 2008;18(3):486–92.
Goshima S, et al. Diffusion-weighted imaging of the liver: optimizing b value for the detection and characterization of benign and malignant hepatic lesions. J Magn Reson Imaging. 2008;28:691–7.
Zhu J, et al. Apparent diffusion coefficient normalization of normal liver: will it improve the reproducibility of diffusion-weighted imaging at different MR scanners as a new biomarker? Medicine (Baltimore). 2017;96:e5910.
Woo S, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of hepatocellular carcinoma: correlation with enhancement degree and histologic grade. Radiology. 2014;270:758–67.
Wu L, et al. ADC total ratio and D ratio derived from intravoxel incoherent motion early after TACE are independent predictors for survival in hepatocellular carcinoma. J Magn Reson Imaging. 2017;46:820. https://doi.org/10.1002/jmri.25617.
Guiu B, Cercueil J-P. Liver diffusion-weighted MR imaging: the tower of Babel? Eur Radiol. 2011;21:463–7.
Choi IY, et al. Intravoxel incoherent motion diffusion-weighted imaging for characterizing focal hepatic lesions: correlation with lesion enhancement. J Magn Reson Imaging. 2016;45:1589–98.
Hectors SJ, et al. Intravoxel incoherent motion diffusion-weighted imaging of hepatocellular carcinoma: is there a correlation with flow and perfusion metrics obtained with dynamic contrast-enhanced MRI? J Magn Reson Imaging. 2016;44:856–64.
Drevelegas K, Nikiforaki K, Constantinides M, Papanikolaou N, Papalavrentios L, Stoikou I, Zarogoulidis P, Pitsiou G, Pataka A, Organtzis J, Papadaki E, Porpodis K, Kougioumtzi I, Kioumis I, Kouskouras C, Akriviadis E, Drevelegas A. Apparent diffusion coefficient quantification in determining the histological diagnosis of malignant liver lesions. J Cancer. 2016;7(6):730–5.
Liang H-Y, et al. Potential of MR histogram analyses for prediction of response to chemotherapy in patients with colorectal hepatic metastases. Eur Radiol. 2016;26:2009–18.
Goshima S, et al. Diffusion kurtosis imaging to assess response to treatment in hypervascular hepatocellular carcinoma. AJR Am J Roentgenol. 2015;204:W543–9.
Gluskin JS, Chegai F, Monti S, Squillaci E, Mannelli L. Hepatocellular carcinoma and diffusion-weighted MRI: detection and evaluation of treatment response. J Cancer. 2016;7:1565–70.
Wu L-M, Hu J, Gu H-Y, Hua J, Xu J-R. Can diffusion-weighted magnetic resonance imaging (DW-MRI) alone be used as a reliable sequence for the preoperative detection and characterization of hepatic metastases? A meta-analysis. Eur J Cancer. 2013;49:572–84.
CT/MRI LI-RADS v2017. Available from: https://www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/LIRADS/2017/LIRADS_2017_Core.pdf?la=en. Accessed 29 June 2017.
Kim YK, Kim CS, Han YM, Lee YH. Detection of liver malignancy with gadoxetic acid-enhanced MRI: is addition of diffusion-weighted MRI beneficial? Clin Radiol. 2011;66:489–96.
Sandrasegaran K, et al. The usefulness of diffusion-weighted imaging in the characterization of liver lesions in patients with cirrhosis. Clin Radiol. 2013;68:708–15.
Kim YK, et al. Hypovascular hypointense nodules on hepatobiliary phase gadoxetic acid-enhanced MR images in patients with cirrhosis: potential of DW imaging in predicting progression to hypervascular HCC. Radiology. 2012;265:104–14.
Chang W-C, et al. Histological grade of hepatocellular carcinoma correlates with arterial enhancement on gadoxetic acid-enhanced and diffusion-weighted MR images. Abdom. Imaging. 2014;39:1202–12.
Mannelli L, Kim S, Hajdu CH, Babb JS, Taouli B. Serial diffusion-weighted MRI in patients with hepatocellular carcinoma: prediction and assessment of response to transarterial chemoembolization. Preliminary experience. Eur J Radiol. 2013;82:577–82.
Corona-Villalobos CP, et al. Functional magnetic resonance imaging response of targeted tumor burden and its impact on survival in patients with hepatocellular carcinoma. Investig Radiol. 2015;50:283–9.
Rhee TK, et al. Tumor response after yttrium-90 radioembolization for hepatocellular carcinoma: comparison of diffusion-weighted functional MR imaging with anatomic MR imaging. J Vasc Interv Radiol. 2008;19:1180–6.
Mannelli L, et al. Assessment of tumor necrosis of hepatocellular carcinoma after chemoembolization: diffusion-weighted and contrast-enhanced MRI with histopathologic correlation of the explanted liver. AJR Am J Roentgenol. 2009;193:1044–52.
Lee J, et al. Mass-forming intrahepatic cholangiocarcinoma: diffusion-weighted imaging as a preoperative prognostic marker. Radiology. 2016;281:119–28.
Fattach H, et al. Intrahepatic and hilar mass-forming cholangiocarcinoma: qualitative and quantitative evaluation with diffusion-weighted MR imaging. Eur J Radiol. 2015;84:1444–51.
Park HJ, Kim YK, Park MJ, Lee WJ. Small intrahepatic mass-forming cholangiocarcinoma: target sign on diffusion-weighted imaging for differentiation from hepatocellular carcinoma. Abdom Imaging. 2013;38:793–801.
Min JH, et al. Differentiation between cholangiocarcinoma and hepatocellular carcinoma with target sign on diffusion-weighted imaging and hepatobiliary phase gadoxetic acid-enhanced MR imaging: classification tree analysis applying capsule and septum. Eur J Radiol. 2017;92:1–10.
Vilgrain V, et al. A meta-analysis of diffusion-weighted and gadoxetic acid-enhanced MR imaging for the detection of liver metastases. Eur Radiol. 2016;26:4595–615.
Merkle EM, Zech CJ, Bartolozzi C, et al. Consensus report from the 7th international forum for liver magnetic resonance imaging. Eur Radiol. 2016;26:674–82. https://doi.org/10.1007/s00330-015-3873-2.
Kim SS, et al. Disappearing or residual tiny (</=5 mm) colorectal liver metastases after chemotherapy on gadoxetic acid-enhanced liver MRI and diffusion-weighted imaging: is local treatment required? Eur Radiol. 2016;27:3088. https://doi.org/10.1007/s00330-016-4644-4.
Nishiofuku H, et al. Increased tumour ADC value during chemotherapy predicts improved survival in unresectable pancreatic cancer. Eur Radiol. 2016;26:1835–42.
Wagner M, et al. Assessment of the residual tumour of colorectal liver metastases after chemotherapy: diffusion-weighted MR magnetic resonance imaging in the peripheral and entire tumour. Eur Radiol. 2016;26:206–15.
Kim JH, et al. Diffusion-related MRI parameters for assessing early treatment response of liver metastases to cytotoxic therapy in colorectal cancer. AJR Am J Roentgenol. 2016;207:W26–32.
Schmeel FC, et al. Prognostic value of pretreatment diffusion-weighted magnetic resonance imaging for outcome prediction of colorectal cancer liver metastases undergoing 90Y-microsphere radioembolization. J Cancer Res Clin Oncol. 2017;143:1531. https://doi.org/10.1007/s00432-017-2395-5.
Schmeel FC, et al. Diffusion-weighted magnetic resonance imaging predicts survival in patients with liver-predominant metastatic colorectal cancer shortly after selective internal radiation therapy. Eur Radiol. 2017;27:966–75.
Deckers F, et al. Apparent diffusion coefficient measurements as very early predictive markers of response to chemotherapy in hepatic metastasis: a preliminary investigation of reproducibility and diagnostic value. J Magn Reson Imaging. 2014;40:448–56.
Lambregts DMJ, et al. Whole-liver diffusion-weighted MRI histogram analysis: effect of the presence of colorectal hepatic metastases on the remaining liver parenchyma. Eur J Gastroenterol Hepatol. 2015;27:399–404.
Donato H, França M, Candelária I, Caseiro-Alves F. Liver MRI: from basic protocol to advanced techniques. Eur J Radiol. 2017;93:30–9.
Chilla GS, Tan CH, Xu C, Poh CL. Diffusion weighted magnetic resonance imaging and its recent trend-a survey. Quant Imaging Med Surg. 2015;5:407–22.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Alves, F.C., Silva, F.P. (2021). Malignant Liver Lesions. In: Matos, C., Papanikolaou, N. (eds) Diffusion Weighted Imaging of the Hepatobiliary System. Springer, Cham. https://doi.org/10.1007/978-3-319-62977-3_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-62977-3_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-62976-6
Online ISBN: 978-3-319-62977-3
eBook Packages: MedicineMedicine (R0)