
Abstract
Imaging has a limited role in diagnosis [1]. Most head and neck (H&N) tumours are referred for imaging after the diagnosis has been confirmed or strongly suspected clinically. That said, with some less common malignancies, magnetic resonance imaging (MRI) has a more significant diagnostic role. Also, in people with squamous cell cancer (SqCC) neck nodes, and no obvious primary site on clinical examination, MRI/CT will demonstrate the primary in approximately one third of cases.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Imaging has a limited role in diagnosis [1]. Most head and neck (H&N) tumours are referred for imaging after the diagnosis has been confirmed or strongly suspected clinically.Footnote 1 That said, with some less common malignancies, magnetic resonance imaging (MRI) has a more significant diagnostic role.Footnote 2 Also, in people with squamous cell cancer (SqCC) neck nodes, and no obvious primary site on clinical examination, MRI/CT will demonstrate the primary in approximately one third of cases.
TNM staging system is a clinico-pathological system but it is good practice when reporting scans to apply the principles of the system and offer a radiological stage. The advantage is analysis and description of the scan in a logical manner with appropriate emphasis on features of particular importance for planning treatment.
4.1 Primary Diagnosis/Staging
Primary tumour (T)
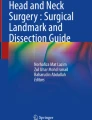
MRI, the single most important imaging modality for staging the primary tumourFootnote 3 (Fig. 4.1).

Coronal fat saturated T2W MRI scan showing a very large malignancy originating in the left side of the tongue (arrows) and extending into the sublingual space and across the midline
Nodes (N)
MR and CT, performed routinely to stage the neck (Fig. 4.2, 4.3, and 4.4). The overall false positive and false negative rates are 15–20% [2]. Ultrasound (USS) with fine needle aspiration is currently the most reliable and widely available technique for assessing cervical lymphadenopathy ; most often used when there are equivocal nodes on CT/MR.Footnote 4

Transverse image from contrast CT scan demonstrating an enhancing tumour of the right tongue base (white arrows) extending posterolaterally to abut right level II lymphadenopathy

Transverse image from contrast CT scan demonstrating centrally necrotic squamous cell carcinoma of the right tongue base (small arrows) and necrotic enlarged right level II lymph node (large arrow head) typical of regional nodal metastasis

Coronal STIR sequence from MRI scan on patient with tongue base carcinoma demonstrating necrotic right level II (arrow) and retropharyngeal (arrowheads) lymphadenopathy
Metastases (M)
For all but the smallest tumours , chest computed tomography (CT) is performed, on grounds that the most common site of distant metastases is the lungs.Footnote 5 It seems logical to extend the CT to include the extracranial H&N at the same time since this potentially offers additional information about local tumour extension, especially if MRI is equivocal or of poor quality, e.g., if the patient has moved.
Synchronous tumours outside the H&N are demonstrated in around 1%, two thirds carcinoma of bronchus, the remainder mostly oesophageal carcinoma [5,6,7].
4.2 Post Treatment Assessment
4.2.1 Sequelae of Surgery
Excision of the primary tumor is usually accompanied by repair of the defect with a reconstructive flap and neck dissection.Footnote 6 The individual tissue components of the reconstructive surgery , especially bone/fat, are easy to identify on both CT/MRI. Acute changes post-surgery , e.g., loss of tissue planes, oedema, normal structure distortion/swelling, lymphatic engorgement, seromas and enhancement of damaged tissue following contrast can be identified on CT/MRI; most resolve by 6 weeks.
4.2.2 Sequelae of Radiotherapy
With the exception of structural changes, radiotherapy provokes similar acute appearances, often over a larger area, persisting longer (up to 12 weeks) and with more pronounced and persistent subcutaneous and deep fat oedema (soft tissue stranding) and widespread mucosal swelling, especially in the larynx; usually symmetrical but sometimes surprisingly asymmetrical.
There is usually at least some degree of salivary gland inflammation (associated with high signal on MR and diffuse post-contrast enhancement on MRI/ CT) with subsequent atrophy. Although these features lessen with time there will be some persistence of all of them.
Between 6 weeks and 6 months while granulation tissue evolves into mature stable scar tissue the appearance is quite active on CT and, especially, MRI with post-contrast enhancement . From 6 to 12 months the stereotypical appearance of inert unenhancing scar tissue appears [8]. Although in some cases areas of enhancement persist.
Tumour recurrence, most often locoregional, is characterised by areas of enhancement, increasing bulk or new foci of soft tissue, often irregular and infiltrating, further loss of tissue planes and damage to normal structures, including bone erosion [9]. It is sometimes associated with nodal relapse and/or distant metastases, usually pulmonary. Isolated nodal or distant metastatic disease is less common [10].
A baseline scan around 3–6 months after intervention to demonstrate tumour response and record baseline post intervention changes, followed by surveillance scans for 3–5 years, often yearly, or more frequently, is a commonly used surveillance regime. The accuracy of early tumour detection with this sort of regime remains unclear.Footnote 7
4.3 Radiotherapy Planning
Imaging plays a key role here. Accurate radiological assessment is crucial to radiotherapy planning in the H&N as the distance between tissue containing tumour and critical, radiation sensitive organs is often very small. Most H&N radiotherapy is now planned using a dedicated CT scan with the person immobilised in the treatment position in a thermoplastic shell. CT allows tissue density information which is used to predict radiotherapy dose distribution.
In addition, imaging is increasingly used during radiotherapy to further improve targeting of radiotherapy, image guided radiotherapy. IMRT provides one such example.Footnote 8 For people treated radically, to improve accuracy, the original planning CT position is compared with cone beam CT acquired on the treatment day and adjustments of patient position is made if this comparison falls outside predetermined thresholds.Footnote 9
For tumours not easily visualised with CT, incorporation of MRI may reduce the chance of accidentally omitting tissue containing tumour from the high dose area [15]. Diffusion weighted MRI may provide superior information to conventional MRI for radiotherapy planning [16]. The evolving role of PET/CT is considered in the PET/CT chapter.
4.4 Normal Variants and Artefacts
Metal, most commonly dental amalgam , may cause large areas of image distortion or loss (attenuation artefacts).Footnote 10
Prominent normal nodes are often impossible to differentiate from metastatic nodes on CT/MRI, especially in younger adults when normal nodes (especially level II) are relatively large (frequently 10–15 mm, maximum transverse diameter).
4.5 Advantages of MR, CT and USS
4.5.1 MRI
The single greatest advantage is high quality demonstration of soft tissue with good contrast between normal structures, benign and malignant pathology. It is generally the best investigation for delineation of the tumour mass, demonstration of local extension and, in the case of more advanced lesions, into more distant but clinically critical sites, particularly the neural foramina of the skull base and spread into the cranial cavity itself (Fig. 4.5) [17,18,19].

Large right oropharyngeal squamous cell carcinoma invading posterolaterally into the masticator space (large arrow) and posterosuperiorly into the preverterbal space and skull base, via the foramen ovale, and into Meckel’s cave (small arrow)
4.5.2 CT
Offers complementary information to MRI about the local tumour stage (Fig. 4.6), particularly bone invasion which CT detects with an accuracy in excess of 90%, being marginally less sensitive than MRI but more specific [22,23,24,25,26]. It is currently the only imaging modality able to demonstrate small pulmonary metastases.

Aggressive malignancy of the right hard palate extending into the maxillary antrum and out through the lateral wall into the cheek (arrow). Posterior extension takes the tumour into the pterygopalatine fossa (black arrowhead), a critical site of extension since this allows easy access to the cranial cavity and orbit (via the foramen rotundum and inferior oblique fissure). High volume level II (large white arrowheads) and right retropharyngeal (small white arrowhead) lymphadenopathy is present
4.5.3 Ultrasound
Often combined with Doppler and potentially emerging techniques, e.g., elastography offers excellent characterisation of superficial soft tissue structures, e.g., neck nodes. It can demonstrate the presence, number, size, shape and internal architecture of nodes (all features that may be altered by the presence of metastatic tumour). It is extremely useful for sequential examinations (to monitor equivocal lesions) and to guide biopsies (fine needle and cutting needle).
4.6 Limitations of MR, CT, USS
4.6.1 MRI
People unable to lie flat and/or still for the time involved in scanning and/or tolerate the surface coil, e.g., due to claustrophobia, shortness of breath, pain, marked cervicothoracic scoliosis are unsuitable for MRI.
A minority of metallic foreign bodies constitute a hazard for MRI scanning either because of tissue damage due to heating (spinal nerve stimulaters), movement of metal fragments in the magnetic field (old-style intracranial aneurysm clips, intra-orbital foreign bodies) or malfunction (cochlea implants, pacemakers) [27, 28].
4.6.2 CT
A relatively common problem with CT is artefact arising from high-density material in the area of interest [29]. This is a particular problem in the oral cavity, where high-density fillings may degrade large areas of the image. Postoperatively, metal surgical clips may also produce significant streak artifacts.
Renal dysfunction and contrast hypersensitivity constitute respectively relative and absolute contraindications to the administration of intravenous contrast.
Both CT and MRI have particular anatomical sites where accurate tumour staging is difficult, notoriously with respect to invasion of the prevertebral space, still probably best assessed clinically, unless there is marked invasion with obvious muscle/bone changes.
4.6.3 USS
Virtually all ultrasound is reflected at interfaces between soft tissue and air or bone. Consequently, some lesions cannot be visualized, e.g., deep to the mandible or directly through air-filled structures, e.g., behind the trachea. Retropharyngeal nodes therefore cannot be assessed with ultrasound. Also, attenuation of ultrasound rapidly increases with thickness of tissue and therefore there is limited information available about deep lying structures, a problem worsened when there is thick superficial scarring in the neck.
4.7 Pitfalls
-
1.
Misdiagnosing a cystic neck mass, most frequently at the mandibular angle, a classical pitfall. The differential usually lies between a SqCC node metastasis and a branchial cleft cyst. Less commonly presentation of metastatic disease from papillary carcinoma of thyroid or cervical nodal tuberculosis. As a general rule, SqCC should be the considered diagnosis; branchial cleft cyst only very cautiously, and especially in people over 40.
-
2.
Overlooking disease outside the primary area of concern, e.g., skip lesions of adenoid cystic carcinoma at the skull base, extracranial disease in people with neurological presentations, upper aerogestive tract, thorax, upper abdomen synchronous tumours.
-
3.
In initial staging/assessment of potential recurrent tumour MRI tends to overstage due to associated peritumoral (or post-intervention) oedema and reactive inflammatory changes. Similarly, periodontal infection and recent dental extraction may be misdiagnosed as tumourFootnote 11 [22].
-
4.
The distinction of an aggressive-appearing lesion after treatment is between metachronous tumours [6], radiation-induced sarcomas (usually many years post-treatment, average around 9 years, range 3–37 years [30]) and osteroradionecrosis (ORN) , where there is bone destruction.
ORN most commonly affects the mandible and demonstrates the typical appearance of osteomyelitis (permeative areas of bone destruction, cortical interruptions, sequestra and pathological fractures) with a surrounding soft tissue inflammatory mass which is often contiguous with swollen and enhancing masticatory muscles. It may appear similar to recurrence but differentiating features include the clinical picture (inflammatory features including the presence of pus and draining sinuses), areas of sclerosis, as the bone attempts healing, and diffuse swelling rather than destruction of adjacent soft tissue structures (particularly the muscles). Most of these features are best seen with CT rather than MRI [31, 32].
Key Points
-
Imaging has a limited role in diagnosis
-
Most head and neck (H&N) tumours are referred for imaging after the diagnosis has been confirmed or strongly suspected clinically
-
MRI, the single most important imaging modality for staging the primary tumour
-
MR and CT, performed routinely to stage the neck. The overall false positive and false negative rates are 15–20%
-
Ultrasound (USS) with fine needle aspiration is currently the most reliable and widely available technique for assessing cervical lymphadenopathy; most often used when there are equivocal nodes on CT/MR
-
Most H&N radiotherapy is now planned using a dedicated CT scan with the person immobilised in the treatment position in a thermoplastic shell.
-
CT allows tissue density information which is used to predict radiotherapy dose distribution.
-
Diffusion weighted MRI may provide superior information to conventional MRI for radiotherapy planning
-
The single greatest advantage of MRI is high quality demonstration of soft tissue with good contrast between normal structures, benign and malignant pathology.
-
CT offers complementary information to MRI about the local tumour stage particularly bone invasion
-
Ultrasound (often combined with Doppler and potentially emerging techniques, e.g., elastography) offers excellent characterisation of superficial soft tissue structures, e.g., neck nodes.
-
Renal dysfunction and contrast hypersensitivity constitute respectively relative and absolute contraindications to the administration of intravenous contrast.
-
Both CT and MRI have particular anatomical sites where accurate tumour staging is difficult, notoriously with respect to invasion of the prevertebral space.
Notes
- 1.
Especially with the commonest sites of malignancy (oral cavity, oropharynx, larynx).
- 2.
Notably paranasal sinuses, skull base and deep lobe parotid lesions may present non-specifically for example with features of sinusitis, nasal obstruction or cranial nerve symptoms (trigeminal neuropathy, facial or with cavernous sinus involvement, oculomotor palsy).
- 3.
For MR technique, please see Appendix (8).
- 4.
For MRI/CT/USS criteria for the diagnosis of nodal involvement, please see Appendix (9).
- 5.
- 6.
For different types of neck dissection see Appendix (7). For types of surgical reconstruction see Appendix (6).
- 7.
In the first year following intervention MRI in particular is prone to false positives, up to 58% between 3 and 6 months following treatment [10]. Subsequently, a wide range of accuracy is reported, with perhaps surprisingly, sensitivity of at least 86% and specificity of 80% for CT compared to 50% and 83% respectively for MRI (admittedly on different study groups) [11, 12]. It remains uncertain how much this improves with diffusion weighted imaging or other specialised MRI techniques [13]. Looking specifically at persistent lymph node disease CT and MRI have similar relatively poor sensitivities and specificities of around 53% and 74% respectively compared to 88% and 66% for ultrasound (rising to a specificity of 96% for ultrasound guided fine needle aspiration cytology) [14].
- 8.
IMRT is rapidly becoming the standard for radical H&N treatment because it results in more conformal radiotherapy plans which ensure that radiation beams are delivered to follow the shape of the tumour very closely, ensuring all of the tumour is encompassed inside the radiotherapy field and healthy tissue is avoided as far as possible. This allows better sparing of adjacent organs such as salivary glands and facilitates dose escalation with the promise of improved cures rates [20, 21].
- 9.
Cone beam CT is currently state-of-the-art IGRT. A flat panel detector and a kV radiation source are integrated into a linear accelerator. Multiple projection radiographs are acquired immediately before an RT fraction with short acquisition times, via rotation of the linac gantry. The image obtained [cone beam image] is registered onto the planning CT for calculation of the target position in relation to the planned position.
- 10.
Iatrogenically positioned material (fixating plates across osteotomy sites) and traumatically acquired foreign bodies cause similar artefacts.
- 11.
As a general (but not invariable) rule, if there is signal change only on the STIR sequence but not the T1W images, the process is benign; if changes occur on both, it more likely represents tumour invasion.
References
Arya S, Rane P, Deshmukh A. Oral cavity squamous cell carcinoma: role of pretreatment imaging and its influence on management. Clin Radiol. 2014;69(9):916–30.
Bondt RBJ, Nelemans PJ, Hofman PAM, et al. Detection of lymph node metastases in head and neck cancer: a meta-analysis comparing US, USgFNAC, CT and MR imaging. Eur J Radiol. 2007;64:266–72.
Fukuhara T. Usefulness of chest CT scan for head and neck cancer. Auris Nasus Larynx. 2015;42(1):49–52.: S0385-8146(14)00131-X. https://doi.org/10.1016/j.anl.2014.08.013.
Loh KS, Brown DH, Baker JT, et al. A rational approach to pulmonary screening in newly diagnosed head and neck cancer. Head Neck. 2005;27(11):990–4.
Rennemo E, Zätterström U, Boysen M. Synchronous second primary tumors in 2,016 head and neck cancer patients: role of symptom-directed panendoscopy. Laryngoscope. 2011;121(2):304–9.
Priante AV, Castilho EC, Kowalski LP. Second primary tumors in patients with head and neck cancer. Curr Oncol Rep. 2011;13(2):132–7.
Jain KS, Sikora AG, Baxi SS, et al. Synchronous cancers in patients with head and neck cancer: risks in the era of human papillomavirus-associated oropharyngeal cancer. Cancer. 2013;119(10):1832–7. https://doi.org/10.1002/cncr.27988. Epub 2013 Feb 19
Offiah C, Hall E. Post-treatment imaging appearances in head and neck cancer patients. Clin Radiol. 2011;66:13–24.
Lell M, Baum U, Greess H, et al. Head and neck tumours: imaging recurrent tumour and post-therapeutic changes with CT and MRI. Eur J Radiol. 2000;33:239–47.
Collan J, Lundberg M, Vaalavirta L. Patterns of relapse following surgery and postoperative intensity modulated radiotherapy for oral and oropharyngeal cancer. Acta Oncol. 2011;50(7):1119–25.
Som PM, Urken ML, Biller H, et al. Imaging the postoperative neck. Radiology. 1993;187:593–603.
Kangelaris GT, Yom SS, Huang K et al. Limited utility of routine surveillance MRI following chemoradiation for advanced-stage oropharynx carcinoma. Int J Otolaryngol. 2010;2010. pii: 904297. https://doi.org/10.1155/2010/904297. Epub 2010 Aug 31.
de Bree R, van der Putten L, Brouwer J, et al. Detection of locoregional recurrent head and neck cancer after (chemo)radiotherapy using modern imaging. J Neuropathol Exp Neurol. 2013;72(7):600–13.
Nishimura G, Matsuda H, Taguchi T. Treatment evaluation of metastatic lymph nodes after concurrent chemoradiotherapy in patients with head and neck squamous cell carcinoma. Anticancer Res. 2012;32(2):595–600.
Newbold K, Powell C. PET/CT in radiotherapy planning for head and neck cancer. Front Oncol. 2012;2(189):2234–943.
Tsien C, Cao Y, Chenevert T. Clinical applications for diffusion magnetic resonance imaging in radiotherapy. Semin Radiat Oncol. 2014;24(3):218–26.
Alberico RA, Husain SH, Sirotkin I. Imaging in head and neck oncology. Surg Oncol Clin N Am. 2004;13(1):13–35.
Rumboldt Z, Gordon L, Bonsall R, et al. Imaging in head and neck cancer. Curr Treat Options Oncol. 2006;7(1):23–34.
Evangelista L, Cervino AR, Chondrogiannis S, et al. Comparison between anatomical cross-sectional imaging and 18F-FDG PET/CT in the staging, restaging, treatment response, and long-term surveillance of squamous cell head and neck cancer: a systematic literature overview. Nucl Med Commun. 2014;35(2):123–34.
Nutting C. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011;12(2):127–36.
Miah A. Dose-escalated intensity-modulated radiotherapy is feasible and may improve locoregional control and laryngeal preservation in laryngo-hypopharyngeal cancers. Int J Radiat Oncol Biol Phys. 2012;82(2):539–47.
Imaizumi A, Yoshino N, Yamada I, et al. A potential pitfall of MR imaging for assessing mandibular invasion of squamous cell carcinoma in the mandible. AJNR Am J Neuroradiol. 2006;27:114–22.
Vidiri A, Guerrisi A, Pellini R, et al. Multi-detector row computed tomography (MDCT) and magnetic resonance imaging (MRI) in the evaluation of the mandbiular invasion by squamous cell carcinomas (SCC) of the oral cavity. Correlation with pathological data. J Exp Clin Cancer Res. 2010;29:73–9.
Handschel J, Naujoks C, Depprich RA, et al. CT-scan is a valuable tool to detect mandibular involvement in oral cancer patients. Oral Oncol. 2012;48:361–6.
Li C, Men Y, Yang W, et al. Computed tomography for the diagnosis of mandibular invasion caused by head and neck cancer: a systematic review comparing contrast-enhanced and plain computed tomography. J Oral Maxillofac Surg. 2014;72:1601–15.
Goerres GW, Schmid DT, Schuknecht B, et al. Bone invasion in patients with oral cavity cancer: comparison of conventional CT with PET/CT and SPECT/CT. Radiology. 2005;237:281–7.
http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/PublichHealthNotifications/ucm242613
http://www.nhs.uk/Conditions/MRI-scan/Pages/Who-can-use-it.aspx
Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics. 2004;24:1679–91.
Cai P, Yao-pan W, Li L, et al. CT and MRI of radiation-induced sarcomas of the head and neck following radiotherapy for nasopharyngeal carcinoma. Clin Radiol. 2013;68:683–9.
Chong J, Hinkley LK, Ginsberg LE. Masticator space abnormalities associated with mandibular osteoradionecrosis. AJNR Am J Neuroradiol. 2000;21:175–8.
Hermans R. Imaging of mandibular osteoradionecrosis. Neuroimaging Clin N Am. 2003;13:597–604.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Kabala, J., Beasley, M. (2018). Radiological Imaging in Head and Neck Tumours. In: Wong, W. (eds) PET/CT in Head and Neck Cancer. Clinicians’ Guides to Radionuclide Hybrid Imaging(). Springer, Cham. https://doi.org/10.1007/978-3-319-61440-3_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-61440-3_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-61439-7
Online ISBN: 978-3-319-61440-3
eBook Packages: MedicineMedicine (R0)