
Abstract
As cardiovascular diseases (CVD) are the main cause of death in women worldwide, they are also frequently present in breast cancer (BC) patients and in late survivors. Radiation therapy, chemotherapy, immunotherapy and angiogenic therapy may induce cardiotoxicity and vascular damage. In the rapidly evolving field of cardio-oncology it is recommended that pre-existing CVD risk factors should be assessed in all BC patients and aggressively managed, starting at the time of treatment (or even before) and continuing throughout survivorship. The use of advanced cardiac imaging techniques improves earlier detection of cardiac damage and heart failure, enabling a more timely treatment.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Anthracyclines
- Blood pressure
- BRCA 1/2 mutation carriers
- Breast cancer
- Cardiotoxicity
- Cardio-oncology
- Chemotherapy
- Ejection fraction
- Immunotherapy
- Systolic heart failure
- Radiation therapy
- Risk factors
- Trastuzumab
Introduction
In Western populations one out of eight women will develop breast cancer (BC). Due to improved screening modalities and the development of novel cancer treatments, including targeted and immunologic therapies, 5 year BC survival rates are more than 90%. Ten-year survival rates for invasive BC is now approximately 83% (www.seer.cancer.gov). Despite these impressive advancements in survival, cardiovascular toxicity is increasingly observed as a serious complication of treatment. This has led to the rapid evolving field of cardio-oncology with a bread focus not only on myocardial toxicity, but also on vascular disease, accelerated onset of hypertension and arrhythmias. New strategies are currently being developed to better preserve and restore cardiovascular health in patients with cancer and cancers survivors, for which an optimal interdisciplinary collaboration and understanding is needed [1, 2].
Cardiovascular Risk in Breast Cancer Patients
As cardiovascular diseases (CVD) are the main cause of death in women worldwide, they are also frequently present in BC patients and in late survivors (Fig. 7.1). In a population of 415 postmenopausal women with hormone receptor (HR) positive early BC the 10-year predicted CVD risk was equivalent to or higher than BC recurrence risk [3]. Risk factors like obesity, diabetes and hypertension are important in the occurrence of both CVD and BC [4,5,6,7]. Women with unhealthy lifestyle behavior, CVD risk factors and genetic factors are more susceptible for cardiotoxicity during BC therapy [8, 9]. This concept is also known as the ‘multiple-hit’ hypothesis. Preliminary data also suggest that cancer itself may induce subclinical myocardial damage before any treatment has been started [10]. Despite the individual differences in CVD risk profile, the various classifications/stages of BC and the variety of BC treatment regimens that are needed, a tailored patient approach with early and late cardio-surveillance is not yet standard routine care (Fig. 7.2) [11]. This may result in (too) late referral for cardiac treatment, as illustrated in the patient case. In 2016 the ESC has released a first position paper on cancer treatments and cardiovascular toxicity [12].

CVD and breast cancer deaths in women. Source: US Centers for Disease Control and Prevention [1999–2013]


Patient surveillance in treatment for breast cancer
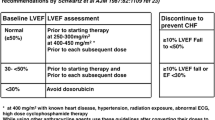
In this paper it is recommended that pre-existing CVD risk factors should be assessed and aggressively managed, starting at the time of treatment (or even before) and continuing throughout survivorship. Baseline risk factors for cardiotoxicity are depicted in Table 7.1.
Cardiovascular Risk in BRCA Mutation Carriers
Over the past decades an increasing number of women have been identified with hereditary BC, related to mutations in one of the two BRCA genes. The cumulative risk in BRCA1 mutation carriers by age 70 is 57–65% for breast and 39% for ovarian cancer and in BRCA2 carriers 45–49% and 10–18% respectively [13]. It has been suggested that BRCA1/2 mutation carriers are at increased risk of CVD compared to the general population [14, 15]. The exact mechanisms have not been elucidated yet, however the intrinsic risk of carrying a BRCA1/2 mutation, exposure to preventive risk reducing salpingo-oophorectomy (RRSO) before 40–45 years of age, chemotherapy and radiation therapy may add to a higher CVD risk [16]. In BRCA1/2-knockout mice, a higher susceptibility towards doxorubicin-induced cardiotoxicity has been reported [17]. However, a prospective study in 39 BRCA1/2 mutation carriers compared to 42 sporadic BC patients did not show an increased risk of anthracycline-induced cardiotoxicity in BRCA1/2 mutation carriers [18].
Risk of Radiation Therapy for Breast Cancer
Radiation therapy has been reported to increase the longterm risk of death due to CVD, even after 20 years of follow-up [19]. This risk is especially present for left-sided BC patients as with older radiation techniques part of the heart might be included in the irradiated volumes. In an older Swedish cohort of BC patients it was found that women treated with radiation therapy for left-sided BC had more ischemic heart disease (IHD) than women treated for right-sided BC, especially in the mid-left anterior descending artery and diagonal branches [20]. In a population based case-control study absolute radiation risks for ischemic heart disease (IHD) were greater in women with preexisting CVD risk factors than in those without [21]. The increased risk for coronary events started within the first 5 years after radiotherapy and continued for three decades thereafter. It is unknown yet to which extent radiation therapy induces coronary microvascular dysfunction (CMD). Current smoking increases the sensitivity of myocardial cells to the ionizing effects of radiation therapy, enhancing the risk for fibrosis and IHD [7]. The use of breath-hold techniques for left-sided BC patients is currently more often applied to reduce the individual heart dose of radiation [22, 23]. This technique may also be protective in right-sided BC patients who need loco-regional treatment (including the internal mammary lymph nodes) [24].
Cardiotoxicity of Chemotherapy for Breast Cancer
The cardiotoxic effects of anti-neoplastic agents can be divided into irreversible cardiomyocyte loss (type I) and reversible (type II) myocardial damage [25]. Type I is caused by anthracyclines, such as doxorubicin and epirubicin, and leads to cardiomyocyte apoptosis and necrosis. The harmful effects are cumulative and dose-dependent, with an interindividual range in toxic threshold depending on age (>65 years), renal failure, specific genetic polymorphisms, presence of hypertension, previous radiotherapy and combined use of type II agents [12, 26]. Subclinical LV deterioration occurs in 10–50% of treated patients, with a mean decline of 10% in LV function when compared to pre-treatment values, especially in the first year after treatment [27, 28]. This early asymptomatic loss of LV function can progress over time (years) to symptomatic heart failure (HF), which is most frequently seen in elderly women above 65 years of age. Of note is that subclinical HF may remain undiagnosed (for years), whereas symptoms of tiredness and dyspnea at effort are attributed to previous BC and ageing.
Immuno- and Targeted Therapies
Trastuzumab is a monoclonal antibody indicated in >20% of BC patients who are positive for the human epidermal growth factor receptor 2 (HER2) and in women with metastatic BC. The use of trastuzumab has increased over the past 15 years and is associated with an absolute 14% higher incidence rate for HF with reduced ejection fraction (HFrEF) or cardiomyopathy over 3 years of follow-up [29]. Although still debated, its cardiotoxic effects on LV function are assumed to be reversible (type II) and not related to cumulative dose but to the number of treatment sessions (see patient case) [30, 31]. Determinants of cardiotoxicity with trastuzumab are concomitant or prior treatment with anthracyclines, higher age, and the presence of hypertension. Trastuzumab cardiotoxicity usually manifests early during treatment [31]. In BC-trials, the incidence of symptomatic HF in trastuzumab-treated patients was 2–4% and the incidence of cardiac dysfunction was 3–19% [32,33,34]. In most BC registries treatment with trastuzumab is (temporarily) interrupted when ejection fraction (EF) falls below 45% [34]. Although not proven yet, early administration of HF drugs, such as ACE and ARBs, is likely to limit LV deterioration [28]. Currently, novel anti-HER2 targeted therapies are on the market (pertuzumab, lapatinib), which are potentially safer for the myocardium but less well investigated [35].
Cardiovascular Risk with Anti-angiogenic and Endocrine Therapies
The use of vascular endothelial growth factors (VEGF) inhibitors, such as bevacizumab for metastatic BC has increased over the past years. Nearly all patients who are treated with VEGF signaling inhibitors have an increase in blood pressure, often within 1 week of treatment [36]. The overall incidence of hypertension is reported to be 20–25% [37]. In a low percentage of patients (1–2%) signs if LV dysfunction and HF are described [38]. Given the high prevalence of hypertension in the ageing female population, adequate monitoring and management of blood pressure is needed when anti-VEGF agents are administered.
Endocrine therapy with the selective estrogen receptor modulator (SERM) tamoxifen (TAM) has been used for over decades and has a very low CVD risk [39, 40]. It is approved as adjuvant therapy and palliative therapy for hormone receptor positive primary and metastatic BC. In patients at increased thrombotic and CVD risk, tamoxifen may increase the occurrence of VTE and stroke [41]. In a meta-analysis it was recently found that aromatase inhibitors (AI) (exemestane, anastrozole, letrozole) are superior to TAM as adjuvant hormonal therapy for postmenopausal ER-positive BC [42]. However, AI’s are associated with increased risk of developing CVD especially with longer treatment durations [43, 44]. Conflicting data have been reported on adverse effects of AI’s on lipid profiles, which may add to a higher CVD risk [45].
Optimal Cardiac Surveillance and Treatment During/After BC Therapy
The first step to identify patients at increased risk for cardiotoxicity during BC therapy is to assess their baseline CVD risk (see Table 7.1) [12]. It remains to be determined however, which determinants are most important to predict future cardiotoxicity. Whereas BC treatment has evolved into highly patient-tailored treatment strategies, the concurrent use of cardiac evaluation tools that can accurately assess both cardiac function and structure is presently lacking in the cardiac monitoring of BC patients with the use of routine echocardiography or radionuclide angiography. It may be more appropriate to use new ultrasound techniques with 3D possibilities, strain imaging and cardiac magnetic resonance (MRI), which are safe for the patients and reveal more earlier signs of LV damage [46,47,48]. Cardiac MRI is complementary to echocardiography and allows for unique and non-invasive insights into myocardial structure such as the tissue relaxation properties and the presence of diffuse fibrosis [49]. In Table 7.2 the currently available diagnostic tools are described.
Thus far it is still debated whether preventive use of ACE inhibitors, ARBs and b-blockers is indicated before anthracycline treatment has started, when baseline EF is normal [12]. Cardiotoxic effects of trastuzumab can be reduced by a drug-free interval after initial chemotherapy [32, 50]. It is advised to temporarily interrupt trastuzumab therapy when EF falls below 45% or when there is a drop of >10% in LVEF from baseline. Several studies have confirmed the beneficial effects of HF medication such as ACE inhibitors, ARBs and (additional) b-blockers when subclinical or overt HF occurs during BC treatment and more preventive studies are on the way [28, 51, 52]. Arrhythmias, especially atrial fibrillation (AF) can occur at all stages of BC treatment and need to be treated with antiarrhythmic drugs/b-blockers and antithrombotic medication, with considerations on quality of life, life expectancy and potential (bleeding) risks. There is no evidence as yet that the use of a defibrillator (ICD) prolongs life when sever HF due to cardiotoxicity occurs (see patient case).
Key Issues Cardio-surveillance During/After BC Treatment
-
Assess individual baseline CVD risk before BC treatment
-
Initiate HF medication when LVEF decreases >10% (ACE or ARB, and B-blocker) or LVEF <45%.
-
Consider temporarily interruption of trastuzumab if EF <45% or >10% decrease in baseline LVEF
-
Continue HF medication when EF reduction persists after treatment
-
Monitor/treat blood pressure with use VEGF -inhibitors
-
Long-term follow-up LV function advised after signs of cadiotoxicity during treatment
-
Maintain a healthy lifestyle, as far as possible, during and after BC treatment
References
Barac A, et al. Cardiovascular health of patients with cancer and cancer survivors: a roadmap to the next level. J Am Coll Cardiol. 2015;65(25):2739–46.
Moslehi JJ. Cardiovascular toxic effects of targeted cancer therapies. N Engl J Med. 2016;375(15):1457–67.
Bardia A, et al. Comparison of breast cancer recurrence risk and cardiovascular disease incidence risk among postmenopausal women with breast cancer. Breast Cancer Res Treat. 2012;131(3):907–14.
Calle EE, et al. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348(17):1625–38.
Larsson SC, Mantzoros CS, Wolk A. Diabetes mellitus and risk of breast cancer: a meta-analysis. Int J Cancer. 2007;121(4):856–62.
Xue F, Michels KB. Diabetes, metabolic syndrome, and breast cancer: a review of the current evidence. Am J Clin Nutr. 2007;86(3):s823–35.
Hooning MJ, et al. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst. 2007;99(5):365–75.
Jones LW, et al. Early breast cancer therapy and cardiovascular injury. J Am Coll Cardiol. 2007;50(15):1435–41.
Lal H, Kolaja KL, Force T. Cancer genetics and the cardiotoxicity of the therapeutics. J Am Coll Cardiol. 2013;61(3):267–74.
Pavo N, et al. Cardiovascular biomarkers in patients with cancer and their association with all-cause mortality. Heart. 2015;101(23):1874–80.
Maas AH, et al. Cardiovascular surveillance in breast cancer treatment: a more individualized approach is needed. Maturitas. 2016;89:58–62.
Zamorano JL, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for practice guidelines: the Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(36):2768–801.
Antoniou A, et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72(5):1117–30.
Arts-de Jong M, et al. BRCA1/2 mutation carriers are potentially at higher cardiovascular risk. Crit Rev Oncol Hematol. 2014;91(2):159–71.
Mai PL, et al. Potential excess mortality in BRCA1/2 mutation carriers beyond breast, ovarian, prostate, and pancreatic cancers, and melanoma. PLoS One. 2009;4(3):e4812.
van Westerop LL, et al. Cardiovascular risk of BRCA1/2 mutation carriers: a review. Maturitas. 2016;91:135–9.
Singh KK, et al. BRCA2 protein deficiency exaggerates doxorubicin-induced cardiomyocyte apoptosis and cardiac failure. J Biol Chem. 2012;287(9):6604–14.
Barac A, et al. Cardiac function in BRCA1/2 mutation carriers with history of breast cancer treated with anthracyclines. Breast Cancer Res Treat. 2016;155(2):285–93.
Bouillon K, et al. Long-term cardiovascular mortality after radiotherapy for breast cancer. J Am Coll Cardiol. 2011;57(4):445–52.
Nilsson G, et al. Distribution of coronary artery stenosis after radiation for breast cancer. J Clin Oncol. 2012;30(4):380–6.
Darby SC, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987–98.
Swanson T, et al. Six-year experience routinely using moderate deep inspiration breath-hold for the reduction of cardiac dose in left-sided breast irradiation for patients with early-stage or locally advanced breast cancer. Am J Clin Oncol. 2013;36(1):24–30.
Mast ME, et al. Left-sided breast cancer radiotherapy with and without breath-hold: does IMRT reduce the cardiac dose even further? Radiother Oncol. 2013;108(2):248–53.
Essers M, et al. Should breathing adapted radiotherapy also be applied for right-sided breast irradiation? Acta Oncol. 2016;55(4):460–5.
Suter TM, Ewer MS. Cancer drugs and the heart: importance and management. Eur Heart J. 2013;34(15):1102–11.
Lenneman CG, Sawyer DB. Cardio-oncology: an update on cardiotoxicity of cancer-related treatment. Circ Res. 2016;118(6):1008–20.
Takemura G, Fujiwara H. Doxorubicin-induced cardiomyopathy from the cardiotoxic mechanisms to management. Prog Cardiovasc Dis. 2007;49(5):330–52.
Cardinale D, et al. Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation. 2015;131(22):1981–8.
Chen J, et al. Incidence of heart failure or cardiomyopathy after adjuvant trastuzumab therapy for breast cancer. J Am Coll Cardiol. 2012;60(24):2504–12.
Procter M, et al. Longer-term assessment of trastuzumab-related cardiac adverse events in the Herceptin Adjuvant (HERA) trial. J Clin Oncol. 2010;28(21):3422–8.
Farolfi A, et al. Trastuzumab-induced cardiotoxicity in early breast cancer patients: a retrospective study of possible risk and protective factors. Heart. 2013;99(9):634–9.
Slamon D, et al. Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med. 2011;365(14):1273–83.
Romond EH, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353(16):1673–84.
Suter TM, et al. Trastuzumab-associated cardiac adverse effects in the Herceptin Adjuvant trial. J Clin Oncol. 2007;25(25):3859–65.
Swain SM, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724–34.
Chen HX, Cleck JN. Adverse effects of anticancer agents that target the VEGF pathway. Nat Rev Clin Oncol. 2009;6(8):465–77.
Li W, et al. Vascular and metabolic implications of novel targeted cancer therapies: focus on kinase inhibitors. J Am Coll Cardiol. 2015;66(10):1160–78.
Cameron D, et al. Adjuvant bevacizumab-containing therapy in triple-negative breast cancer (BEATRICE): primary results of a randomised, phase 3 trial. Lancet Oncol. 2013;14(10):933–42.
Bonanni B, et al. Effect of tamoxifen at low doses on ultrasensitive C-reactive protein in healthy women. J Thromb Haemost. 2003;1(10):2149–52.
Pinkerton JV, Thomas S. Use of SERMs for treatment in postmenopausal women. J Steroid Biochem Mol Biol. 2014;142:142–54.
Davies C, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381(9869):805–16.
Ryden L, et al. Aromatase inhibitors alone or sequentially combined with tamoxifen in postmenopausal early breast cancer compared with tamoxifen or placebo – meta-analyses on efficacy and adverse events based on randomized clinical trials. Breast. 2016;26:106–14.
Amir E, et al. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: a systematic review and meta-analysis. J Natl Cancer Inst. 2011;103(17):1299–309.
Chlebowski RT, et al. Benefit/risk for adjuvant breast cancer therapy with tamoxifen or aromatase inhibitor use by age, and race/ethnicity. Breast Cancer Res Treat. 2015;154(3):609–16.
Lintermans A, Neven P. Safety of aromatase inhibitor therapy in breast cancer. Expert Opin Drug Saf. 2015;14(8):1201–11.
Kerkhove D, et al. How to monitor cardiac toxicity of chemotherapy: time is muscle! Heart. 2014;100(15):1208–17.
Thavendiranathan P, et al. Reproducibility of echocardiographic techniques for sequential assessment of left ventricular ejection fraction and volumes: application to patients undergoing cancer chemotherapy. J Am Coll Cardiol. 2013;61(1):77–84.
Walker J, et al. Role of three-dimensional echocardiography in breast cancer: comparison with two-dimensional echocardiography, multiple-gated acquisition scans, and cardiac magnetic resonance imaging. J Clin Oncol. 2010;28(21):3429–36.
Plana JC, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2014;15(10):1063–93.
Curigliano G, et al. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO clinical practice guidelines. Ann Oncol. 2012;23(Suppl 7):vii155–66.
Gulati G, et al. Prevention of cardiac dysfunction during adjuvant breast cancer therapy (PRADA): a 2 × 2 factorial, randomized, placebo-controlled, double-blind clinical trial of candesartan and metoprolol. Eur Heart J. 2016;37(21):1671–80.
Seicean S, et al. Cardioprotective effect of beta-adrenoceptor blockade in patients with breast cancer undergoing chemotherapy: follow-up study of heart failure. Circ Heart Fail. 2013;6(3):420–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Maas, A.H.E.M. (2017). Cardiotoxicity During and After Breast Cancer Treatment. In: Maas, A., Bairey Merz, C. (eds) Manual of Gynecardiology. Springer, Cham. https://doi.org/10.1007/978-3-319-54960-6_7
Download citation
DOI: https://doi.org/10.1007/978-3-319-54960-6_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-54959-0
Online ISBN: 978-3-319-54960-6
eBook Packages: MedicineMedicine (R0)