
Abstract
Subarachnoid hemorrhage frequently leads to vasospasm. The treatment includes hyperdynamic therapy and if that is ineffective, then endovascular intervention. Chemical spasmolysis and angioplasty may provide durable resolution of vasospasm. Indications, techniques, and perioperative management are discussed.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Indications for Treatment and Case Selection
-
Symptomatic vasospasm secondary to SAH from ruptured aneurysm that is not responsive to a 2–4 h trial of maximal pharmacological therapy (Fig. 13.1).
Fig. 13.1 
Left vertebral angiogram demonstrating vasospasm of basilar artery. Flow restriction because of the vasospasm is demonstrated by the significant contrast reflux into the right vertebral artery (VA). The spasm of the basilar artery has resulted in the caliber of this vessel appearing smaller than that of the VAs. In addition to caliber, vasospasm is also diagnosed by observing the caliber of the affected vessel at termination, i.e., where it branches. A vessel in vasospasm will appear bulbous or of a larger caliber at termination. By contrast, a congenitally hypoplastic or stenosed vessel does not demonstrate this bulbosity
-
Vasospasm secondary to mechanical manipulation.

Preoperative Management
-
The aneurysm should be secured by clipping or coiling prior to pharmacological or endovascular management of vasospasm.
-
Ensure the MAP is ≥70 mmHg.
-
Preoperative intubation, if there are any concerns about the patient’s ability to protect airway.
-
Verify laboratory values including platelet count, BUN, CR, APTT, PT/INR, and ß-HCG for females of reproductive age group.
-
In case of renal insufficiency, diabetes, CHF, etc., ensure usage of diluted non-ionic contrast agent and carefully pre-plan to maintain contrast load to minimum.
-
NPO (for ≈6 h) when procedure is to be performed under general anesthesia.
-
Obtain informed consent for angiography and angioplasty.
-
Ensure two IV lines inserted.
-
Insert Foley. Patient will be more comfortable and cooperative with an empty bladder in case the procedure becomes prolonged.
-
Position patient on neuroangiography table.
-
Attach patient to pulse oximetry and ECG leads for monitoring O2 saturation, HR, cardiac rhythm respiratory rate, and BP.
Technique
-
After the groin region is appropriately prepped and draped, palpate the femoral artery.
-
Immobilize a segment of the artery between the index and middle fingers.
-
Infiltrate the skin overlying the immobilized segment with local anesthesia using 1% lidocaine with epinephrine.
-
Make a small, superficial stab incision in the anesthetized skin.
-
Using modified Seldinger technique, perform an arteriotomy (see Chap. 2 for technique for arteriotomy and sheath placement) and make an exchange over wires to place a sheath in the femoral artery.
-
The sheath should be ≥6 Fr, just in case a procedure such as angioplasty needs to be performed.
-
The sheath is connected to a continuously running flush of heparinized saline.
-
Connect a diagnostic catheter (e.g., 5 Fr Glidecath) to a continuously running flush of heparinized saline.
-
Introduce a 0.035 glidewire into the catheter.
-
Ensure that sheath and catheter systems are free of air, or any other foreign bodies.
-
Once the catheter is in the sheath, advance it over the wire using fluoroscopy.
-
If the patient’s vasculature is anticipated to be non-tortuous, consider using a Guide catheter, e.g., 6 Fr Envoy instead of the diagnostic catheter. It will save the time required for exchanging the diagnostic catheter for a guide catheter, in case intervention is decided upon.
-
During diagnostic angiography esp. when using a guide catheter, when a vasospastic segment is identified, it is best to treat it at least chemically before proceeding to the next vessel. It may save some time by eliminating the need to catheterize the same artery more than twice.
-
Study the vasculature most at risk of vasospasm first based on history (i.e., if location of an aneurysm is known), symptomatology and studies such as TCD’s. We usually also perform a CT perfusion study to assess whether or not angiography or intervention is warranted.
Selective Intra-arterial Pharmacological Intervention
-
The guide catheter is securely positioned in the pertinent artery of the neck (Carotid or vertebral depending upon the intracranial vessel being treated).
-
A microcatheter (e.g., Excelsior SL 10 with transcend 0.010 or 0.014 guidewire) is prepared.
-
The microcatheter is connected to a continuously running flush of heparinized saline.
-
It is ensured that the entire system is free of air or any other foreign matter.
-
Advance the microcatheter with contained microwire into the RHV of the guide catheter.
-
Advance the microcatheter over the microwire until both reach the distal tip of the guide catheter.
-
Perform a roadmap.
-
With the help of roadmap guidance, advance the microcatheter over the microwire to position the catheter tip just distal to the segment in spasm.
-
Remove the microwire.
Verapamil
-
Indicated for mild non-flow limiting vasospasm that does not warrant angioplasty or moderate vasospasm that cannot be safely treated with angioplasty.
-
It may also be indicated in those who have vasospasm consequent to manipulation during endovascular intervention.
-
We also use it prior to performing angioplasty, so that the dilatation is performed on the relaxed dilated artery rather than a relatively rigid vasoconstricted artery.
-
Verapamil is our agent of first choice. We have found it to be safe and effective to the extent that, we use it almost exclusively.
Dose: 5–10 mg is injected gradually (over 2–10 min) as the microcatheter is withdrawn through the spasmodic segment. Up to 20 mg may be given into each arterial tree. Inject gradually to ensure there is no significant drop in BP or bradycardia.
Alternatively, verapamil injection is frequently performed through the diagnostic or guide catheter positioned further proximally in internal carotid artery (ICA), or VA. This approach has the significant advantage of being quicker and bypasses the complexities of using a microcatheter. However, the amount of verapamil reaching the spastic segment may be less.
Contraindications
-
Acute MI, severe CHF, cardiogenic shock, severe hypotension, second or third degree AV block, sick sinus syndrome, marked bradycardia, hypersensitivity to the drug, Wolff–Parkinson–White syndrome, Lown–Ganong–Levine syndrome.
Nicardipine
-
Nicardipine is diluted with normal saline to a concentration of 0.1 mg/ml and administered in 1-ml aliquots to a maximum dose of 5 mg per vessel.
-
Similar to verapamil administration above, administer gradually as the catheter is withdrawn through the spastic segment of the vessel. Gradual administration will also attenuate the likelihood of untoward side effects, e.g., transient tachycardia, hypotension or, increased intracranial pressure (ICP).
Contraindications
-
Hypersensitivity to the drug.
-
Aortic stenosis.
Papavarine
-
It is a short acting, with a half life of less than 1 h.
-
It may be used for cerebral vasospasm. However, due to the short duration of action other agents, e.g., verapamil are preferable.
-
Papavarine may be used for angioplasty pre-treatment to enable placement of balloon catheter by causing vasodilatation.
Dose: Available in 3% concentration (30 mg/ml) at pH 3.3. 300 mg of Papaverine is diluted in 100 ml of normal saline to obtain a 0.3% concentration.
-
Papavarine is administered intra-arterially through the microcatheter, which is positioned just proximal to the segment in vasospasm.
-
The 300-mg dose is administered at a rate of 3 ml/minute.
-
Do not mix Papaverine with contrast agents or heparin. That may result in precipitation of crystals.
-
Side effects include, rapid increase in ICP, thrombocytopenia, hypotension, seizures, etc. (see ‘Papavarine’ in Chap. 18 ‘Pharmacological Agents’ for details).
Contraindications
-
Increased ICP; glaucoma; hypersensitivity to Papaverine; atrioventricular block; acute myocardial infarction; recent stroke and, liver function disorders.
Nitroglycerine
-
It is used more in case of vessel spasm during catheterization rather than SAH-induced vasospasm.
Dose: 100–300 µg through the catheter.
-
Side effects include headache, orthostatic hypotension and tachycardia, paradoxical bradycardia and anaphylactoid reactions.
Contraindications
-
Hypersensitivity to drug, severe anemia, increased ICP and methemoglobinemia.
Angioplasty
-
Is indicated in refractory vasospasm that does not respond to pharmacological and hemodynamic interventions.
Devices
-
An Envoy guide catheter is deployed as indicated above, which should be at least 6 Fr.
-
However, if the patient has a tortuous vasculature, then use a 6 Fr shuttle sheath (80 cm; a longer sheath may be used if the patient is tall), which may be advanced initially over dilator into the descending aorta and then into the cervical carotid, or subclavian artery over 6 Fr H1 slip catheter. A shuttle sheath is preferable in tortuous vasculature because it will provide greater support and significantly decrease the likelihood of the apparatus collapsing into the aortic arch at critical time points, e.g., during stent deployment.
-
6 Fr H1 slip catheter.
-
Rotating hemostatic valves (2). Ensure the RHV attached to the guide catheter is ≥0.096″ or 2.44 mm.
-
Pediatric transducers (30 ml/hr; 2).
-
Diagnostic catheter: Terumo® front angled glidecath 5 Fr (for diagnostics).
-
Front angled glidewire (0.035; Terumo).
-
Balloon dilatation catheter (non-compliant or semi-compliant).
-
For treatment of vasospasm, we recommend usage of a non-compliant/semi-compliant balloon catheter. We have found that compliant catheters expand much more in the non-stenosed segment before they affect the stenosed segment (the stenosed segment will appear as a ‘waist’). It may result in arterial rupture at the overinflated non-stenosed segment, while attempting to dilate the stenosed segment to the desired diameter. This is not a problem with non-compliant/semi-compliant catheters.
-
The size and type of balloon dilatation catheter will depend upon the location of spasm in the arterial tree. Table 13.1 below contains examples of balloon dilatation catheters for various locations.
Table 13.1 Examples of semi-compliant balloon dilatation catheters that may be used for overcoming vasospasm -
The size of the balloon dilatation catheter is based on the vessel size, as explained later in the ‘procedure’ section. For safety reasons, the balloon diameter should be equal to or less than the caliber of the normal vessel.
-
Inflation device with manometer.
-
Syringes 20 cc, 10 cc (at least 3), 20 cc (at least 4), 3 cc (for ACT).
-
Three-way stopcock: 3.
-
Torque device.
-
Telfa strip.
-
Mandrel for shaping microwire tip.
-
Angioseal™ closure device (6 Fr). Use larger size if a larger sheath is inserted.
-
Angioplasty using a Gateway™ balloon dilatation catheter is described below. The technique remains the same with other dilatation catheters.
-
Remove the contents of the Gateway™ dilatation catheter from its package and transfer them onto the table, maintaining sterile precautions.
-
Remove the catheter from the protective hoop.
-
Ensure the catheter is not kinked, bent, or otherwise damaged.
-
Hold the catheter proximal to its balloon segment and with the other hand, gently remove the stylet from the distal tip of the catheter.
-
Slide the protective sheath off the balloon.
-
Note that the balloon has radiopaque markers to aid in its positioning in the stenosed segment.
-
We prep the catheter in vivo. However, below is the ex vivo technique as described by the manufacturer.
-
Fill a luer-lock syringe with 3 ml of contrast medium.
-
Connect a three-way stopcock to the provided port on the balloon catheter. Flush through the stopcock using heparinized saline.
-
Connect the syringe with contrast to the stopcock.
-
Hold the syringe with nozzle pointing downward and aspirate for 5 sec. Then, release the plunger.
-
Remove the syringe and evacuate all air from the barrel.
-
Reconnect the syringe and aspirate until bubbles no longer appear during aspiration. If air bubbles persist, do not use the device.
-
Disconnect the syringe.
-
Wet the hydrophilic outer shaft of the balloon catheter.
-
Fill a 20-cc syringe with 15 cc contrast and 5 cc heparinized NS (2/3:1/3 concentration).
-
Attach a three-way stopcock to the inflation device and connect the 20-cc syringe containing contrast medium to the sideport of the stopcock.
-
Aspirate the contrast into the inflation device, leaving only 1–2 cc within the syringe.
-
Purge any air out of the barrel and tubing of the inflation device, all the way to the distal portal of the stopcock.
-
Leave inflation device on table, until needed.
Deployment
-
Attach the balloon catheter to a continuously running flush of heparinized saline via the provided portal using a three-way stopcock. Carefully advance the guidewire through the hub of the balloon catheter.
-
Advance the over-the-wire (OTW) balloon catheter using fluoroscopy and road mapping.
-
In case a microcatheter is already in the desired location, an exchange length microwire may be advanced through it and the microcatheter retracted and removed. The OTW balloon catheter can then be advanced over the wire.
-
Loosen the RHV of the guide catheter and advance the balloon catheter, over the wire, into it.
-
In case of RX balloon catheter, ensure that the guidewire exits the notch 25 cm proximal to the RX balloon catheter tip.
-
Then tighten the RHV just enough to prevent excessive blood loss, while not causing a hindrance in advancing the balloon catheter.
-
Advance the balloon catheter over the wire into the guide catheter.
-
Take care that the position of the guidewire is maintained during this maneuvering. Occasionally, confirm the same by fluoroscopy.
-
Continue to advance the dilatation catheter over the guidewire until the proximal marker on the balloon catheter aligns with the hemostatic valve. This indicates that the balloon catheter tip has reached the tip of guide catheter. Doing so also spares the patient unnecessary irradiation.
-
Perform roadmapping for further navigation and appropriate deployment of the balloon catheter system.
-
Using fluoroscopy and roadmapping, continue to advance the balloon catheter over the guidewire until it is appropriately positioned in the stenosed segment (Fig. 13.2a).
Fig. 13.2 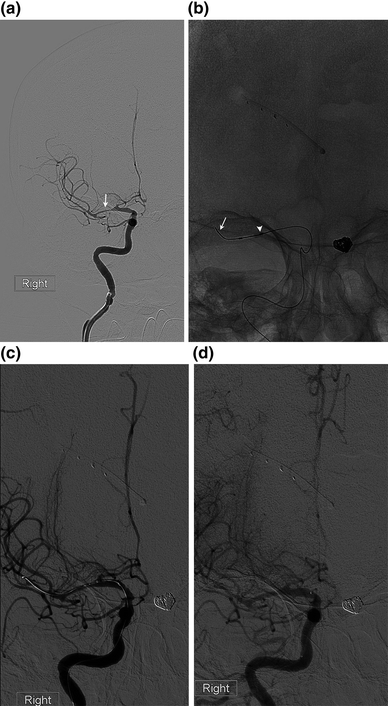
a Severe vasospasm of RMCA (arrow) in a patient with a coiled left PComm aneurysm. She was administered 20 mg of verapamil infiltrated into the middle cerebral artery (MCA) as the microcatheter was retracted. This resulted in attenuation of the spasm on angiography performed 20 min later. At this point, a Gateway™ 2 × 9 mm balloon catheter was advanced over microwire into the affected MCA segment. Angioplasty was performed for sustained results. b is a fluoroscopy image during angioplasty, demonstrating the tip of the microwire beyond the MCA bifurcation (arrow). The dilated proximal aspect of the balloon can be appreciated (arrowhead). Repeat angiography with balloon catheter still in MCA (c) and following retraction of catheter (d), demonstrates significant attenuation of the vasospasm esp. if compared to pre-treatment angiogram (a). Note that the ACA, which was not treated, continues to manifest vasospasm through all the images

Angioplasty
-
Recover the inflation device from the table.
-
Use the distal free port of the stopcock attached to the inflation device (which is in line with the inflation device) to make a wet (meniscus to meniscus) connection with the balloon port of the catheter.
-
Ensure that this connection is secure so that it will not disconnect during angioplasty.
-
Close the stopcock to the inflation device.
-
To perform in vivo balloon preparation, aspirate the syringe (with nozzle pointing down) attached to the sideport of the stopcock to purge air out of the balloon catheter system.
-
Slowly release the plunger of the syringe, so that the air in the catheter is replaced with contrast left in syringe for purpose. Repeat this step once or twice.
-
Close the stopcock to syringe and open it to the inflation device.
-
Place the compliance card in front of you in the operating field, where you can easily look at it while performing angioplasty.
-
Initially, inflate the balloon to a very low pressure (1 atm) and again confirm that it is appropriately positioned across the stenosed segment. Also look at the radiopaque markers for confirmation of balloon position. These markers are more easily visualized on the native image. While viewing the compliance card periodically, begin inflating the angioplasty balloon using the balloon inflation device.
-
Inflate slowly by turning the screw provided on the inflation device at a rate ≤1 atm/15 s (to ‘stretch’ not ‘crack’ the vessel).
-
Keep track of and document the inflation time (during which the blood flow will be interrupted by the balloon).
-
Step on fluoroscopy pedal frequently to visualize progression of angioplasty (Fig. 13.2b).
-
During inflation, the balloon may acquire a ‘waist’ due to the stenosis. It resolves with the progression of angioplasty.
-
Once the goal pressure is reached, deflate the device.
-
Confirm complete balloon deflation fluoroscopically.
-
In order to achieve complete deflation, one may need to open the stopcock to the syringe and vigorously aspirate. Close the stopcock to syringe while the aspiration is fully applied.
-
Confirm complete balloon deflation fluoroscopically.
-
Perform follow-up (f/u) angiography to evaluate results of angioplasty (Fig. 13.2c). If needed, repeat the angioplasty.
-
Do not exceed the recommended balloon pressures indicated on the compliance card.
-
Once angioplasty is completed and balloon completely deflated, withdraw the balloon catheter over guidewire partially. Use fluoroscopy to ensure the guidewire does not move down as well and continues to cross the lesion.
-
Perform angiography to assess results angioplasty (Fig. 13.2d).
-
Following completion of procedure, perform post-interventional angiography in standard half Townes (Townes in case of VA) and lateral views to rule out any complication such as vessel cut off due to embolism, prior to giving up access.
-
At this point, if no further intervention is planned both catheter and wire may be retracted.
-
Once the balloon catheter exits from the hemostatic valve of the guide catheter, wipe it clean with Moist Telfa and store it by keeping it submerged in a basin with heparinized saline.
-
If the guide catheter has a RHV, ensure it is tightened adequately following balloon catheter withdrawal.
Postoperative Management and Follow Up
-
Admit patient to NSICU for at least overnight observation. Further ICU stay will depend upon the patient’s clinical condition.
-
Generally, 0.9% NS + 20 meq KCl @ 150 cc/hr × 2 h, then decrease to 100 cc/hr while patient is NPO.
-
Keep right/left leg (whichever side was used for arteriotomy) straight × 2 h (in case of angioseal closure) or 6–8 h (in case manual compression was applied), with HOB elevated 15°.
-
Check groins, DP’s, vitals and neuro checks q 15 min × 4, q 30 min × 2, then q hr.
-
After arteriotomy closure, initiate IV heparin for 12 h, if there are no contraindications. We usually administer 900 IU/hr for 12 h in patients <70 kg and 1300 IU/hr for those >70 kg. Some oozing from arteriotomy side may occur while patient is receiving heparin and usually is of no concern.
-
Advance diet as tolerated.
-
Review/Resume preprocedure medications (except oral hypoglycemics, which are initiated 48 h post-intervention and if good PO intake is established).
Suggested Reading
Ringer AJ, Nichols C, Khan SH, Abruzzo TA, Angioplasty and stenting for management of intracranial arterial stenosis. in Hemorrhagic and Ischemic Stroke (Eds. Bendok RB, Naidech AM, Walker MT, Batjer HH) 402–412 (Thieme, New York, 2011).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Khan, SN.H., Ringer, A.J. (2017). Vasospasm. In: Handbook of Neuroendovascular Techniques. Springer, Cham. https://doi.org/10.1007/978-3-319-52936-3_13
Download citation
DOI: https://doi.org/10.1007/978-3-319-52936-3_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-52934-9
Online ISBN: 978-3-319-52936-3
eBook Packages: MedicineMedicine (R0)