
Abstract
Cerebral vasospasm is caused by subarachnoid hemorrhage (SAH) most often secondary to aneurysm rupture. Other less common causes of SAH include hemorrhage from an arteriovenous malformation, vasculitis, reversible cerebral vasoconstriction syndrome as well as cerebral trauma.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Vasospasm
- Avoidance
- Treatment
- Cerebral vasospasm
- Subarachnoid hemorrhage
- Aneurysm rupture
- Arteriovenous malformation
- Vasculitis
- Reversible cerebral vasoconstriction syndrome
- Cerebral trauma
Introduction
Cerebral vasospasm is caused by subarachnoid hemorrhage (SAH) most often secondary to aneurysm rupture. Other less common causes of SAH include hemorrhage from an arteriovenous malformation, vasculitis, reversible cerebral vasoconstriction syndrome (RCVS) as well as cerebral trauma.
Clinical Features
Delayed cerebral ischemia (DCI) from cerebral vasospasm is most common cause of secondary morbidity and mortality following aneurysmal subarachnoid hemorrhage (SAH).
Pathophysiology
-
Blood products in subarachnoid space trigger contraction of smooth muscle cells leading to ischemia and eventual infarction.
-
The precise signaling cascades responsible for this phenomenon remain to be fully elucidated.
Risk of Vasospasm
-
Studies have shown higher risk of vasospasm with increasing Hunt and Hess grade and CT characteristics including the initial presence, volume, density, and duration of hemorrhage.
-
70 % SAH patients will demonstrate angiographic vasospasm.
-
20–30 % of these patients develop symptomatic vasospasm.
-
Up to half of these patients suffer neurologic deficits or death.
-
Early diagnosis and treatment is essential to preserve neurologic function in this group.
Time Course
Most commonly occurs 3–14 days following hemorrhage, peaking around day 7.
Diagnostic Evaluation
Clinical Assessment
-
No definitive prediction algorithm exists so vigilant clinical monitoring is essential, particularly for patients in the high-risk time window.
-
Any of the following signs and symptoms should raise concern:
-
New focal motor deficits
-
Sudden changes in mental status
-
Nonfocal neurologic changes: confusion, increasing somnolence, and combativeness
-
-
Consider and rule out other potential causes of symptoms:
-
Hydrocephalus
-
Seizures
-
Delirium
-
Patients who are neurologically impaired or comatose from initial SAH may not have a meaningful clinical exam and be more dependent on radiographic monitoring.
Laboratory
There are no laboratory studies to diagnose cerebral vasospasm. Vigilant clinical assessment with radiographic imaging is required.
Imaging
The goals of imaging patients during the high-risk vasospasm window:
-
Rule out other pathologies.
-
Detect vasospasm.
-
Assess severity of vasospasm.
Transcranial Doppler (TCD) Ultrasonography
-
First-line modality for monitoring for vasospasm and excellent triaging tool
Advantages: Noninvasive, inexpensive, easily performed at bedside, and high specificity for proximal vessel spasm.
Disadvantages: Sensitivity decreases in more distal vascular territories and can vary with adequacy of vessel insonation and operator experience.
Non-contrast Head Computed Tomography (NCCT)
-
Initial evaluation in patients with altered clinical exam and/or TCD findings
-
Provides rapid survey for established infarctions and rules out other etiologies of neurological deterioration before subsequent interventions are considered
Computed Tomography Angiography (CTA)
-
Highly sensitive for severe vasospasm (>50 % luminal reduction) and excellent negative predictive value
Computed Tomography Perfusion (CTP)
-
Provides rapid perfusion evaluation to compliment demonstration of vasospasm by CTA and TCD
-
Measured parameters include mean transit time (MTT), cerebral blood volume (CBV), and cerebral blood flow (CBF).
-
The following patterns of abnormal perfusion are observed in the setting of vasospasm:
-
Benign oligemia: Increased MTT, normal CBF, and normal or increased CBV
-
Penumbra: Increased MTT, decreased CBF, and normal or increased CBV
-
Irreversible ischemia: Increased MTT, decreased CBF, and decreased CBV
-
The balance between the amount of salvageable penumbra and established infarct in a territory determines whether aggressive intervention should be pursued.
Magnetic Resonance Angiography (MRA) and Perfusion-Weighted
Magnetic Resonance (MR) Imaging
-
Generally not as widely adopted as CT-based modalities given the logistical challenges of MR imaging in acutely ill patients
Digital Subtraction Angiography (DSA)
-
DSA remains the gold standard for evaluating cerebral vasospasm and is the foundation for endovascular treatments.
-
Highly sensitive and specific for vasospasm, provides real-time hemodynamic assessment.
-
Minimal risk of iatrogenic complications.
-
Its cost and resource requirements, however, make it impractical as a screening tool; patients should usually only be triaged to catheter angiography based on suggestive noninvasive imaging findings.
Indications for Intervention
Once you have identified a patient with symptomatic vasospasm whose imaging findings suggest the presence of a salvageable territory, they should be promptly triaged toward medical or endovascular therapy.
Medical Therapy
-
First-line therapy for the majority of patients with symptomatic vasospasm.
-
HHH (hypervolemia, hypertension, and hemodilution) therapy has been shown to be effective for improving perfusion and clinical outcomes.
-
It will not prevent vasospasm in all cases, and up to 19 % of patients may still develop major neurologic deficits or death due to vasospasm despite medical treatment.
Endovascular Therapy
Modalities:
-
Intra-arterial (IA) vasodilator infusion
-
Transluminal balloon angioplasty
-
Combination of both
Candidates for endovascular therapy include:
-
Patients who are unable to tolerate prolonged courses of hemodynamic therapy due to underlying medical comorbidities (e.g., cardiac or renal insufficiency)
-
Patients who have a poor response to medical therapy
Contraindications
The presence of a sizeable infarct core in the vasospasm territory precludes any aggressive therapies as the risk of reperfusion hemorrhage outweighs the potential benefits of recovering the penumbra region.
Relative contraindication to angioplasty of recently clipped or coiled vessels as fatal rupture can occur.
Anatomy
-
Prior to performing any interventions, the patient’s baseline anatomy on DSA should be reviewed carefully, with attention to the vessel morphology and diameter.
Note: the presence of normal variants; hypoplastic segments should not be confused for vasospasm (common locations: A1 segment, intradural vertebral artery, P1 segment, posterior communicating artery).
Note: the location of coils and clips as angioplasty in these regions is associated with a higher risk of iatrogenic rupture:
-
Location and degree of vasospasm have important implications for treatment planning.
-
Proximal vasospasm can be addressed with balloon angioplasty, which is generally thought to provide a more durable effect.
-
Distal vasospasm can be treated with IA vasodilator infusion.
Equipment
Intra-arterial Vasodilators
Calcium channel blockers (CCBs) are the most commonly used agents due to excellent safety profiles and efficacy. They act primarily by inhibition of voltage-gated calcium channels on smooth muscle cells, but there is also evidence of indirect neuroprotective effects. The use of these agents currently remains off-label.
Commonly used CCBs:
-
Nicardipine – T½ ~ 16 h
-
Verapamil – T½ ~ 7 h
-
Nimodipine – T½ 8–9 h
Catheters/Balloons
The use of balloon angioplasty for treatment of vasospasm has been studied for over half a decade. Mechanical flattening of smooth muscle and endothelial cells produces a durable patency of the spastic vessel segment. Coronary balloons were used historically, but more compliant, trackable, dedicated intracranial systems have since been developed.
Intracranial balloon catheter systems:
-
Hyperglide (ev3 Neurovascular, Irvine, California)
-
Hyperform (ev3 Neurovascular, Irvine, California)
Balloon inflation syringe:
-
1-ml Cadence syringe (ev3 Neurovascular, Irvine, California)
Procedure
Perform baseline cerebral angiography of anterior and posterior circulation to assess for vasospasm. Compare with prior angiogram if available and determine if treatment will involve proximal vessels (Distal ICA, M1, and A1) or distal vessel (M2, A2, etc.).
Treatment Plan and Technique
-
Proximal vessel treatment – angioplasty and/or vasodilator infusion (Fig. 1)
Fig. 1 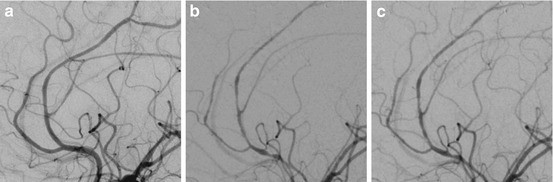
Fifty-three-year-old female who presented with “thunderclap” headache and a negative CT scan. Lumbar puncture demonstrated RBCs that did not clear, and patient was transferred for presumed SAH. (a) Baseline angiography demonstrated a few scattered areas of stenosis. The differential diagnosis included vasculitis and RCVS. The patient subsequently developed an intracerebral hemorrhage, and her neurological exam deteriorated while being treated for vasculitis. Brain biopsy was negative for vasculitis. (b) Repeat angiography demonstrated progressive segmental narrowing in the pericallosal and callosomarginal arteries. (c) Angiography post-infusion of 2 mg of nicardipine demonstrated improvement in the appearance of the blood vessels helping to confirming the diagnosis of RCVS. Despite a slow nicardipine infusion, the patient required pressor support during and after the infusion
-
Distal vessel treatment – vasodilator infusion (Fig. 2)
Fig. 2 
Forty-three-year-old female with history of SAH secondary to ruptured ACOM aneurysm. Eight days post-aneurysm clipping the patient began to have deterioration in her neurological status. Cerebral angiogram demonstrated bilateral MCA and ACA vasospasm. Both MCAs were treated with angioplasty and infusion of nicardipine (2 mg). ACAs were not treated with angioplasty due to small size and recent aneurysm clipping. (a) Baseline left ICA diagnostic angiogram prior to clipping. (b) Angiogram from left common carotid demonstrating severe vasospasm of left A1 and M1 segments. (c) Control angiogram status post-angioplasty of left M1 segment with underinflated 4 mm × 7 mm HyperForm balloon


Vasodilator Infusion
Infusion Site
-
Proximal infusion site from the internal carotid artery or vertebral artery is used for mild to moderate vasospasm in the anterior or posterior circulations, respectively.
-
Superselective injections have been performed for severe vasospasm, but there is no evidence in the literature to support the efficacy of this strategy versus proximal infusion.
-
Consider systemic heparinization when performing prolonged infusion (ACT > 250).
Infusion Rate
Nicardipine
-
Dilute to concentration of 0.1 mg/ml
-
0.5–1 mg nicardipine per minute
-
Total dose 0.5–6.0 mg per arterial tree
Verapamil
-
Dilute to concentration of 0.1 mg/ml
-
0.5–1 mg verapamil per minute
-
Total dose 1–3 mg per arterial tree
Nimodipine
-
Dilute to concentration of 0.1 mg/ml
-
1–4 mg nimodipine per hour
-
Total dose 0.5–3 mg per arterial tree
Arterial pressures should be titrated carefully:
-
Infusion should be stopped when a drop in the mean arterial pressure (MAP) of >15 mmHg or systolic blood pressure of >25 mmHg occurs.
-
Infusion can be resumed after pressures return to baseline.
After infusion, control angiography should be performed to evaluate response to treatment (Fig. 1).
Potential Side Effects
-
It is important to monitor patient vitals carefully during the infusion to avoid complications from hypotension or elevated intracranial pressure.
-
Vasopressor support may occasionally be needed if there is a severe reduction in mean arterial pressure.
Balloon Angioplasty
Balloon diameter should be purposefully undersized from the projected normal caliber of the target vessel segment to reduce the risk of acute vessel rupture.
Administer heparin to achieve ACT > 250 s prior to advancing guidewire and balloon.
The balloon should be advanced to the distal portion of the segment to be treated and angioplasty performed from distal to proximal. Though it may require more dilations, a shorter balloon may be easier to advance through a tight carotid siphon.
Balloons should be inflated with a 50/50 mixture of 300 mg/ml iodinated contrast and saline. A calibrated syringe can be used to inflate the balloon catheter. When using balloon catheter systems in which the guidewire occludes the distal catheter opening, one must be careful not to retract the guidewire into the catheter once the system is in place. Backflow of blood into the balloon lumen dilutes the contrast thereby reducing balloon opacification, which can lead to unintentional overinflation.
Perform control angiography to assess response to treatment and evaluate for complications (Fig. 2).
A vasodilator may be administered prior to angioplasty to help prevent catheter-induced vasospasm prior to angioplasty.
Results
The rate of clinical improvement following balloon angioplasty has been reported in case series at a mean of 62 %, with a range of 11–93 %. There remains no efficacy data from randomized controlled trials to further clarify these results.
Studies have suggested that the rate of clinical improvement when angioplasty is performed within two hours of vasospasm may be higher than outside that window, but further evidence is necessary to fully clarify the ideal window to initiate therapy.
The efficacy of IA vasodilator infusions has also only been described in clinical series, which have reported rates of clinical improvement of up to 76 %. Infusion doses and rates have varied between studies, and a definitive protocol remains to be established.
Complications
Acute vessel rupture occurs in approximately 1 % of cases. This risk has been reduced from the past with the adoption of more compliant, dedicated neurovascular balloon systems and increased technical experience. Severe vessel spasm can still present a challenge due to limited distal visualization – particular care should be taken in these cases to avoid iatrogenic perforation.
Reperfusion injury is a relatively uncommon complication and should be avoided with appropriate analysis of noninvasive studies and avoidance of large infarcts.
Follow-Up
The effect of IA vasodilators is generally not as durable as angioplasty so the critical care team should be aware of the potential for recurrent vasospasm.
Alternative Therapies
Medical therapy should be instituted first in patients with symptomatic vasospasm.
Key Points
-
Do not pursue aggressive treatment in patients with significant infarct cores.
-
Review baseline angiographic appearance with attention to normal variants during treatment planning.
-
Balloon diameter should be undersized with respect to normal vessel caliber.
-
Patients may require retreatment, especially if treated only with vasodilators.
Suggested Reading
Avitsian R, Fiorella D, Soliman MM, et al. Anesthetic considerations of selective intra-arterial nicardipine injection for intracranial vasospasm: a case series. J Neurosurg Anesthesiol. 2007;19:125–9.
Feng L, Fitzsimmons BF, Young WL, et al. Intraarterially administered verapamil as adjunct therapy for cerebral vasospasm: safety and 2-year experience. AJNR Am J Neuroradiol. 2002;23:1284–90.
Janardhan V, Biondi A, Riina HA, et al. Vasospasm in aneurysmal subarachnoid hemorrhage: diagnosis, prevention, and management. Neuroimaging Clin N Am. 2006;16:483–96.
Jestaedt L, Pham M, Bartsch AJ, et al. The impact of balloon angioplasty on the evolution of vasospasm-related infarction after aneurysmal subarachnoid hemorrhage. Neurosurgery. 2008;62:610–7, discussion 610–7.
Lysakowski C, Walder B, Costanza MC, et al. Transcranial Doppler versus angiography in patients with vasospasm due to a ruptured cerebral aneurysm: a systematic review. Stroke. 2001;32:2292–8.
Tejada JG, Taylor RA, Ugurel MS, et al. Safety and feasibility of intra-arterial nicardipine for the treatment of subarachnoid hemorrhage-associated vasospasm: initial clinical experience with high-dose infusions. AJNR Am J Neuroradiol. 2007;28:844–8.
Wintermark M, Ko NU, Smith WS, et al. Vasospasm after subarachnoid hemorrhage: utility of perfusion CT and CT angiography on diagnosis and management. AJNR Am J Neuroradiol. 2006;27:26–34.
Wolf S, Martin H, Landscheidt JF, et al. Continuous selective intraarterial infusion of nimodipine for therapy of refractory cerebral vasospasm. Neurocrit Care. 2010;12:346–51.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Radvany, M.G., Chen, J. (2014). Avoidance and Treatment of Vasospasm. In: Murphy, K., Robertson, F. (eds) Interventional Neuroradiology. Techniques in Interventional Radiology. Springer, London. https://doi.org/10.1007/978-1-4471-4582-0_9
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4582-0_9
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4581-3
Online ISBN: 978-1-4471-4582-0
eBook Packages: MedicineMedicine (R0)