
Abstract
The mitochondrial diseases are a heterogeneous group of rare disorders which can affect virtually all organ systems, like the heart, the brain and the skeletal muscles. Most of the mitochondrial diseases are caused by mutations in the nuclear DNA, but approximately 15% are caused by mutations in the mitochondrial DNA, making genetic counseling difficult. The combination of cardiomyopathy, deafness, diabetes, encephalopathy and myopathy suggests mitochondrial disease.
Cardiomyopathy, however, may be the first and only symptom. MELAS syndrome with hypertrophic cardiomyopathy and Kearns-Sayre syndrome with progressive conduction disorders are two examples of mitochondrial disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Hypertrophic Cardiomyopathy
- Cardiac Involvement
- Mitochondrial Disease
- Mitochondrial Myopathy
- Right Bundle Branch Block
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Mitochondria are the major sites of energy production in the cell as they harbor the process of oxidative phosphorylation (OXPHOS). The OXPHOS system consists of five enzyme complexes, of which complexes I–IV give rise to the mitochondrial respiratory chain, located at the inner mitochondrial membrane. Energy produced by this respiratory chain drives the production of adenosine-tri-phosphate (ATP) from adenosine-di-phosphate (ADP) by complex V.
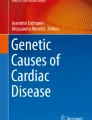
As the heart is an energy-dependent tissue, mitochondria constitute 20–40 % of the cellular volume of cardiomyocytes (Fig. 9.1). The mitochondrial energy production is under the genetic control of both nuclear (99 %) and mitochondrial genes (mtDNA) (1 %) [1]. Mutations within these genes may cause defects in oxidative phosphorylation and have severe consequences for those organs that are heavily dependent on energy production like the heart, the brain, and skeletal muscle. Because myopathy is often one of the main presenting symptoms, patients with mitochondrial diseases tend to be seen primarily by neurologists and pediatricians. However, the importance of mitochondrial disease in cardiology is being more and more recognized, as cardiomyopathy may be the first and only manifestation of mitochondrial disease.

A cardiomyocyte demonstrating the high numbers of mitochondria in between the contractile filaments
Mitochondrial DNA (mtDNA) is a circular double-stranded genome of 16.5 kilobases, encoding 13 polypeptides of the respiratory chain subunits, 28 ribosomal RNAs, and 22 transfer RNAs (tRNAs). All these mitochondrial gene products are involved in mitochondrial energy production, but as stated before, many other components of the respiratory chain and regulatory mitochondrial proteins are coded by nuclear genes. Mitochondrial diseases may thus be caused by mutations in mtDNA, but most are caused, however, by mutations in nuclear DNA.
Therefore, different modes of inheritance may be observed in mitochondrial disease, as mtDNA is exclusively maternally inherited, while nuclear DNA follows Mendelian inheritance. The maternal inheritance of mtDNA is due to the fact that the mammalian egg contains about 100,000 mitochondria and mtDNA, whereas the sperm contains only in the order of 100 mtDNA [2].
Mammalian mtDNA has a very high mutation rate in comparison to nuclear DNA. Each cell contains hundreds to thousands of mitochondria and each mitochondrion contains many copies of mtDNA. Mutations in mtDNA therefore result in heteroplasmy: the presence of two or more different genomes (with and without a mutation) in one cell, the proportion of which may change over time as the mitochondria multiply and are randomly distributed over daughter cells during cell division. Due to this process, the proportion of mutant mtDNA varies considerably between organ systems and even within a specific tissue, resulting in different phenotypes and marked variability in severity and symptom patterns. The heart, central nervous system (CNS), and the skeletal muscles are particularly vulnerable to defects in energy metabolism, and therefore are often involved in mitochondrial disease.
Phenotype–genotype correlation in mitochondrial disease is complex: patients with the same clinical syndrome do not always show the same mutation in the mtDNA and, conversely, a single mutation can be associated with different clinical syndromes [3].
Many mutations in mtDNA may lead to cardiomyopathy, mostly hypertrophic, but dilating cardiomyopathy and left ventricular noncompaction are also possible [4]. A list of known mutations reported in patients with cardiomyopathy is reviewed elsewhere and some are shown in Table 9.1 [5].
Besides mutations in the mtDNA, many mutations in nuclear genes encoding mitochondrial proteins may also cause cardiomyopathy. Some examples include mutations in the mitochondrial transport protein frataxin leading to Friedreich’s ataxia, an autosomal recessive neurodegenerative disorder characterized by progressive ataxia, dysarthria, and hypertrophic cardiomyopathy, and mutations in the gene encoding the protein tafazzin, resulting in Barth syndrome, an X-linked neonatal disorder characterized by dilating cardiomyopathy, skeletal myopathy, cyclic neutropenia, and growth retardation. A comprehensive list of mitochondrial diseases associated with cardiomyopathy is reviewed elsewhere [1].
The most frequently reported cardiac manifestations in mitochondrial disease are mentioned in the Table 9.2.
Many mitochondrial disorders become apparent in the first years of life. The frequency of cardiomyopathy in mitochondrial disease has been reported to be from 17 % to 40 % and the incidence of mitochondrial cardiomyopathy in children and young adults is estimated to be at least 1/50,000 [4, 6]. Children with mitochondrial cardiomyopathy generally have an earlier onset, more severe morbidity, and increased mortality compared with children who have mitochondrial disorders without cardiac involvement [7]. One study showed that of the patients with cardiomyopathy 71 % died or underwent heart transplantation, in contrast to 26 % in patients with mitochondrial disease without cardiomyopathy [6]. Risk factors for major adverse cardiac events in patients with mitochondrial disease were intraventricular conduction block left bundle branch block (LBBB), right bundle branch block (RBBB), left anterior fascicular block (LAFB), left posterior fascicular block (LPFB), diabetes, premature ventricular complexes (>15 PVC/Hr) and left ventricular hypertrophy [8].
As mentioned before, cardiac involvement in mitochondrial disease is usually part of multisystem manifestations of the disorders in oxidative phosphorylation. It is important to realize, however, that seemingly isolated cardiac pathology may be the presenting symptom in mitochondrial disease. In one study this was the case in approximately 10% of patients [9]. Furthermore, a novel mutation in mtDNA (m.8528 T > C) was described in four young patients presenting with an isolated hypertrophic cardiomyopathy, further underlining OXPHOS defects as a potential cause of isolated cardiomyopathy [7].
In this Chapter, two syndromes will be described in more detail: mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS) and Kearns–Sayre syndrome.
MELAS Syndrome
This is a multisystem clinical syndrome manifested by mitochondrial myopathy, encephalopathy, lactic acidosis, and recurrent stroke-like episodes [10]. The most commonly described gene mutation causing MELAS syndrome is a mitochondrial adenine-to-guanine transition at nucleotide pair 3243 (m.3243A > G) encoding the mitochondrial tRNA(Leu) [11]. At least 29 other specific point mutations have been associated with the MELAS syndrome [12]. These mutations lead to impaired oxidative phosphorylation, resulting in the inability of the mitochondria to produce sufficient ATP to meet the energy needs of the cell. This causes a shift to lactate production, which can be systemically noticed as lactate acidosis.
Due to the variability in severity and symptoms and the problems confirming the diagnosis, the incidence of MELAS syndrome is difficult to assess. It is estimated to be as common as neuromuscular diseases like Duchenne muscular dystrophy (frequency 18 per 100,000) [12].
The clinical features of MELAS syndrome vary widely, but almost all patients are diagnosed with stroke-like episodes before 40 years of age, encephalopathy characterized by seizures, dementia, or both, and lactic acidosis. Although age at onset may be high in some patients, most patients, however, present with initial symptoms between 2 and 20 years of age [10]. Other symptoms related to MELAS syndrome are hearing loss, migraine headaches, peripheral neuropathy, depression, learning disabilities, growth failure, diabetes mellitus, gastrointestinal symptoms, renal involvement, and myopathy.
Cardiac involvement in MELAS syndrome is reported to be as high as 18–100 % [13–15]. The most common pathology is nonobstructive concentric hypertrophy, although dilatation is also reported and might be seen as progression of the initial hypertrophic cardiomyopathy. Left ventricular hypertrophy (LVH) appears to correlate positively with LV dilatation and negatively with systolic function [16]. In children, cardiomyopathy may actually be the first manifestation of MELAS syndrome. Wolff–Parkinson–White (WPW) syndrome has also been reported in MELAS syndrome in up to 17 % of patients [13, 17].
The clinical suspicion for mitochondrial disease is based on the combination of symptoms related to different organ systems. On the other hand, especially in young children, the presence of a cardiomyopathy may be the only manifestation of a mitochondrial disorder.
Laboratory examination will show lactic acidosis in almost all patients. Magnetic resonance imaging (MRI) of the brain in MELAS syndrome will typically show asymmetric lesions of the occipital and parietal lobes, mimicking ischemia, although not restricted to one specific vascular region.
ECGs may demonstrate specific abnormalities suggestive of cardiomyopathy, like LVH, negative T-waves in the precordial leads, a left-oriented electrical axis, and prolonged QTc [6]. Echocardiographic examination is mandatory in demonstrating cardiac involvement in mitochondrial disease. In addition to LVH, diastolic and systolic dysfunction may be present.
Muscular biopsy in most patients will show ragged red fibers: deposits of mitochondrial material beneath the sarcolemma, visualized by Gomori trichrome staining or succinate dehydrogenase [12, 14].
Ultrastructural analysis of the heart demonstrates abnormal and markedly enlarged mitochondria.
Molecular diagnosis of mtDNA mutations is complicated by the variability in heteroplasmy depending on the specific tissue sampled. A detectable mutation in muscle cells is not necessarily detectable in leucocytes, cells regularly used for DNA analysis. Urine sediment cells and cheek mucosa appear to be a better alternative for DNA analysis [18].
No specific treatment is available for mitochondrial cardiomyopathies, although there are some suggestions that the use of l-arginine and coenzyme Q10 in addition to vitamin supplementation might be advantageous [12]. As in other cardiomyopathies, regular heart failure therapy is indicated, consisting of diuretics, angiotensin-converting enzyme (ACE) inhibitors, and β-blockers. In cases of refractory heart failure, despite optimal medical therapy, heart transplantation can be considered in selected patients [19]. This requires extensive evaluation of extracardiac involvement, especially with regard to potential contraindications such as recurrent strokes, dementia, and muscle wasting.
Furthermore, heart transplantation and other operations are generally accompanied by a significantly increased perioperative risk, in particular due to stroke, coma, seizures, respiratory failure, and cardiac arrhythmias [20]. Perioperative management includes generous hydration, loading with intravenous glucose, and careful control of body temperature and pH. Ringer’s solution should be avoided because of the lactate load. Anesthetic agents in these patients may increase the susceptibility to reactive oxygen species (ROS) and apoptosis, resulting in neurotoxicity. In general, an increased sensitivity to anesthetics is reported, requiring adjustment of dosing and careful management during surgery, including optimal oxygenation [20].
In summary, given the high incidence of cardiac involvement, all patients with MELAS syndrome should undergo regular cardiac examination because of the therapeutic and prognostic consequences of cardiac involvement. On the other hand, patients with hypertrophic cardiomyopathy at a younger age should be considered having mitochondrial disease, especially when they also suffer from short stature, seizures, hemiparesis, hemianopsia, or cortical blindness. MELAS syndrome is maternally inherited, but genotype–phenotype correlation is complex, which hampers the role of genetic counseling in this syndrome.
Kearns–Sayre Syndrome (KSS)
Clinically, this mitochondrial disease is characterized by progressive external ophthalmoplegia resulting in ptosis, and pigmentary retinopathy. Other manifestations of KSS are short stature, cerebellar signs, hearing loss, mental retardation, vestibular system dysfunction, delayed puberty, and high cerebrospinal fluid protein content. Typical onset is before the age of 20. Progression of the disease can be accompanied by proximal myopathy [21].
Cardiac pathology consists of conduction defects caused by infra-His block, resulting in total AV-block, right bundle branch block, or left anterior hemiblock [22, 23]. These conduction defects may be rapidly progressive and result in acute cardiac death. Transition of a normal electrocardiogram into total AV-block has been reported within the course of 10 months [24]. Complete heart block may also be the presenting symptom of KSS in some patients [25]. It seems plausible that early pacemaker implantation improves survival, but criteria for prophylactic implantation have not been clearly defined. Third-degree and advanced second-degree AV block associated with neuromuscular disease like KSS, with or without symptoms constitute a class I indication for permanent pacemaker implantation [26]. Given the rapid progression to complete AV block, the presence of a fascicular block in KSS has been suggested to warrant prophylactic implantation of a pacemaker [27]. In patients with a normal ECG, regular ECG follow-up, at least every year, is advisable.
Although conduction defects constitute the main cardiac problems in KSS, cardiomyopathy has been reported in a minority of cases [28]. The incidence of cardiomyopathy in KSS, may increase in the future due to the prolonged longevity in patients treated by early pacemaker implantation [27].
In contrast to the MELAS syndrome, which is caused by a point mutation in the mtDNA and is maternally inherited, genetic analysis in KSS typically shows a large deletion of mtDNA and most cases are sporadic [23, 29]. Early mortality in this syndrome is often related to sudden cardiac death due to AV-block, which may be prevented by timely pacemaker implantation.
Conclusion
The mitochondrial diseases are a heterogeneous group of disorders that can affect virtually all organ systems, not only in infancy, but also during the early-to-mid adult years. Most of the mitochondrial diseases are caused by mutations in the nuclear DNA, of which several have been identified thus far. Approximately 15 % are caused by mutations in the mitochondrial DNA. Some examples are reviewed elsewhere and a list of genes is regularly updated at MitoMap (www.mitomap.org/MITOMAP) [1].
Mitochondrial diseases should be included in the differential diagnosis whenever a patient presents with progressive multisystem involvement that does not clearly fit with an established pattern of disease. The combination of cardiomyopathy, deafness, diabetes, together with encephalopathy and myopathy are highly susceptible of mitochondrial disease [21]. Diagnostic algorithms for mitochondrial disease have been recently suggested [1, 30].
Cardiomyopathy may be the presenting and predominant clinical expression of MELAS syndrome and is one of the causes of death in this disease, underlining the importance of this condition to the cardiologist. The same holds for the progressive conduction disorders in Kearns–Sayre syndrome, which may require pacemaker implantation to prevent sudden death.
Apart from these rather well-delineated disorders, many others exist and the phenotypes frequently overlap, complicating things even further.
Given these facts, genetic counseling in mitochondrial disease is difficult. There is only a very small chance that males with mtDNA mutations will transmit the disease. The risk in females is depending on the level of heteroplasmy, but it remains difficult to give advice in the clinical routine.
Diagnosis of mitochondrial diseases is notoriously difficult and relies on a high level of suspicion, but is important, given the potential management implications, not only with respect to cardiac disease, but also more in general like decreased anesthetic requirement during surgical procedures.
Take Home Message
-
Mitochondrial diseases are rare and can be caused by mutations in nuclear DNA as well as mitochondrial DNA, making genetic counseling difficult.
-
The combination of cardiomyopathy, deafness, diabetes, encephalopathy, and myopathy suggests mitochondrial disease.
-
Cardiomyopathy may be the first and only symptom.
-
MELAS syndrome with hypertrophic cardiomyopathy and Kearns–Sayre syndrome with progressive conduction disorders are two examples of mitochondrial disease.
References
Brunel-Guitton C, Levtova A, Sasarman F. Mitochondrial diseases and cardiomyopathies. Can J Cardiol. 2015;31:1360–76.
Wallace DC. Mitochondrial defects in cardiomyopathy and neuromuscular disease. Am Heart J. 2000;139:S70–85.
Ashizawa T. What is Kearns-Sayre syndrome after all? Arch Neurol. 2001;58:1053–4.
Scaglia F, Towbin JA, Craigen WJ, et al. Clinical spectrum, morbidity, and mortality in 113 pediatric patients with mitochondrial disease. Pediatrics. 2004;114:925–31.
Garcia J-M, Goldenthal MJ. Understanding the impact of mitochondrial defects in cardiovascular disease: a review. J Card Fail. 2002;8:347–61.
Holmgren D, Wahlander H, Eriksson BO, Oldfors A, Holme E, Tulinius M. Cardiomyopathy in children with mitochondrial disease. Eur Heart J. 2003;24:280–8.
Ware SM, El-Hassan N, Kahler SG, et al. Infantile cardiomyopathy caused by a mutation in the overlapping region of mitochondrial ATPase 6 and 8 genes. J Med Genet. 2009;46:308–14.
Wahbi K, Bougouin W, Béhin A, et al. Long-term cardiac prognosis and risk stratification in 260 adults presenting with mitochondrial diseases. Eur Heart J. 2015;36:2886–93.
Yaplito-Lee J, Weintraub R, Jamsen K, et al. Cardiac manifestations in oxidative phosphorylation disorders of childhood. J Pediatr. 2007;150:407–11.
Pavlakis SG, Phillips PC, DiMauro S, De Vivo DC, Rowland LP. Mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes: a distinctive clinical syndrome. Ann Neurol. 1984;16:481–8.
Goto Y, Nonaka I, Horai S. A mutation in the tRNA (Leu) (UUR) gene associated with the MELAS subgroup of mitochondrial encephalomyopathies. Nature. 1990;348:651–3.
Sproule D, Kaufman P. Mitochondrial encephalopathy, lactic acidosis and strokelike episodes. Basic concepts, clinical phenotype, and therapeutic management of MELAS syndrome. Ann N Y Acad Sci. 2008;1142:133–58.
Hirano M, Pavlakis SG. Mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes (MELAS) current concepts. J Child Neurol. 1994;9:4–13.
Vydt TCG, de Coo RFM, Soliman OII, ten Cate FJ, van Geuns RJM, et al. Cardiac involvement in adults with m.3242A>G MELAS gene mutation. Am J Cardiol. 2007;99:264–9.
Wortmann SB, Rodenburg RJ, Backx AP, Schmitt E, Smeitink JAM, Morava E. Early cardiac involvement in children carrying the A3243G mtDNA mutation. Acta Paediatr. 2007;96:450–1.
Okajima Y, Tanabe Y, Takayanagi M, Aotsuka H. A follow up study of myocardial involvement in patients with mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes (MELAS). Heart. 1998;80:292–5.
Sproule DM, Kaufmann P, Engelstad K, et al. Wolff-Parkinson-White syndrome in patients with MELAS. Arch Neurol. 2007;64:1625–7.
Shanske S, Pancrudo J, Kaufmann P, et al. Varying loads of mitochondrial DNA A3243G mutation in different tissues: implications for diagnosis. Am J Med Genet. 2004;130A:134–7.
Bhati RS, Sheridan BC, Mill MR, Selzman CH. Heart transplantation for progressive cardiomyopathy as a manifestation of MELAS syndrome. J Heart Lung Transplant. 2005;24:2286–9.
Muravchick S. Clinical implications of mitochondrial disease. Adv Drug Deliv Rev. 2008;60:1553–60.
Finsterer J. Mitochondriopathies. Eur J Neurol. 2004;11:163–86.
Roberts NK, Perloff JK, Kark RAP. Cardiac conduction in the Kearns-Sayre Syndrome (a neuromuscular disorder associated with progressive external ophthalmoplegia and pigmentary retinopathy). Am J Cardiol. 1979;44:1396–400.
Anan R, Nakagawa M, Miyata M, Higuchi I, Nakao S, et al. Cardiac involvement in mitochondrial diseases. A study on 17 patients with documented mitochondrial DNA defects. Circulation. 1995;91:955–61.
Welzing L, von Kleist-Retzow JC, Kribs A, et al. Rapid development of life-threatening complete atrioventricular block in Kearns-Sayre syndrome. Eur J Pediatr. 2009;168:757–9.
Chawla S, Coku J, Forbes T, Kannan S. Kearns-Sayre syndrome presenting as complete heart block. Pediatr Cardiol. 2008;29:659–62.
Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 guidelines for device based therapy of cardiac rhythm abnormalities. J Am Coll Cardiol. 2008;51:e1–e62.
Charles R, Holt S, Kay JM, et al. Myocardial ultrastucture and the development of atrioventricular block in Kearns-Sayre syndrome. Circulation. 1981;63:214–9.
Channer KS, Channer JL, Campbell MJ, Russel RJ. Cardiomyopaty in the Kearns-Sayre syndrome. Br Heart J. 1988;59:486–90.
Limongelli G, Tome-Esteban M, Dejthevaporn C, et al. Prevalence and natural history of heart disease in adults with primary mitochondrial respiratory chain disease. Eur J Heart Fail. 2010;12:114–21.
Bates MGD, Bourke JP, Giordano C, et al. Cardiac involvement in mitochondrial DNA disease: clinical spectrum, diagnosis and management. Eur Heart J. 2012;33:3023–33.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
de Jonge, N., Kirkels, J.H. (2016). Mitochondrial Cardiomyopathy. In: Baars, H., Doevendans, P., Houweling, A., van Tintelen, J. (eds) Clinical Cardiogenetics. Springer, Cham. https://doi.org/10.1007/978-3-319-44203-7_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-44203-7_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-44202-0
Online ISBN: 978-3-319-44203-7
eBook Packages: MedicineMedicine (R0)