
Abstract
Meckel’s diverticulum (MD) is the most common congenital anomaly found in the GI tract. It is a remnant of the omphalomesenteric duct that normally obliterates between weeks 5 and 7 of fetal development. It is usually found incidentally during surgical exploration for other pathologies, and it is symptomatic in less than 5 % of people. The most common presenting symptom is painless rectal bleeding, due to ectopic gastric mucosa causing ulceration of the adjacent ileum. This ectopic gastric mucosa is often diagnosed using a Meckel’s technetium scan. Other presenting symptoms are obstruction and diverticulitis. Meckel’s diverticulum is managed by complete resection of the diverticulum, removing all ectopic tissue. This chapter discusses the pathophysiology and clinical evaluation of MD but will predominantly focus on surgical management and laparoscopic technique. This chapter also discusses the controversy of regarding resection of incidentally found MD.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
- Meckel’s diverticulum
- Vitelline duct
- Omphalomesenteric duct
- Rectal bleeding
- Diverticulitis
- Littre’s hernia
- Intussusception
- Volvulus
- Meckel’s scan
- Enteroscopy
- Laparoscopy
Introduction
Epidemiology
Although Meckel’s diverticulum (MD) is an infrequent finding, it is the most common congenital anomaly in the GI tract. It is found in approximately 2 % of the general population [1]. It was first documented in the late sixteenth century, but it was not described in detail until 1809 by the German anatomist, Johann Meckel [2]. The majority of MD are found incidentally; less than 5 % are symptomatic, and the risk of developing symptoms decreases with age [3, 4]. The incidence of MD is equal between males and females; however, males have been found to be twice as likely to develop symptoms. Also, in a multicentered epidemiologic study, Alemayehu et al. reported a higher incidence of symptomatic MD in Caucasians (63.4 % compared to 4.7 % in Black Americans, 16.4 % in Hispanics) [5].
Embryology
Meckel’s diverticulum is caused by a failure of normal obliteration of the omphalomesenteric duct, also known as the vitelline duct. In early embryonic development, the omphalomesenteric duct provides the embryo nourishment from the yolk sac by serving as a channel between the yolk sac and the early midgut. With fetal growth, the yolk sac regresses as the placenta becomes the primary source of nourishment for the embryo; as a result, the omphalomesenteric duct also involutes and is obliterated by weeks 5–7.
The omphalomesenteric duct is associated with the right and left vitelline vessels. The omphalomesenteric duct and vitelline vessels, along with the urachus and the umbilical vessels, combine to form the umbilical cord. At this time, the umbilical vessels become the dominant blood supply to the fetus, and the vitelline vessels start to regress. The right vitelline artery remnant gives rise to the superior mesenteric artery (SMA), and the left obliterates [6, 7].
Incomplete obliteration of the omphalomesenteric duct can lead to a range of anomalies (Fig. 31.1). If the proximal segment next to the small bowel fails to obliterate, it forms a MD, which is the most common anomaly. The majority of MD are free of attachments to the abdominal wall (75 %) although some may remain attached to the umbilicus, the ileal mesentery, or another segment of the abdominal wall by a fibrous band [7, 8]. If the entire duct fails to obliterate, then it will develop into a fistula between the ileum and the umbilicus. If the distal portion persists and the proximal portion obliterates, then this will become a sinus tract at the umbilicus. If the central portion remains, then it creates an omphalomesenteric cyst. The duct can also incompletely obliterate and leave a fibrous band without a MD [9, 10]. Some of these anomalies may subsequently result in bowel obstruction either by causing internal hernias or proving a fixation point for volvulus.

(a) Meckel’s diverticulum, (b) omphalomesenteric fistula, (c) omphalomesenteric cyst, and (d) remnant vitelline artery/fibrous cord.
Pathophysiology
Meckel’s diverticulum is located on the antimesenteric border of the ileum and contains all of the layers of the intestinal wall making it a true diverticulum. It is located within 20–100 cm (average 50 cm) proximal to the ileocecal valve [2, 8, 11]. The blood supply to the MD is the remnant vitelline artery, which now arises from a terminal branch of the superior mesenteric artery (SMA) [10]. The rules of 2s are frequently used to describe MD [7, 12].
Rules of 2s
-
2 % of the population.
-
Twice as common in males.
-
2 % are symptomatic.
-
Usually 2 cm in diameter.
-
Usually 2 in. long.
-
Located within 2 ft of the ileocecal valve.
As the cells of the omphalomesenteric duct are pluripotent, the MD may contain ectopic mucosa. It has been estimated that 12–50 % of MD contain heterotopic mucosa, most commonly gastric mucosa followed by pancreatic tissue [4, 13–15]. Less commonly, the diverticulum may contain colonic tissue, Brunner’s glands, hepatobiliary tissue, and small bowel malignancies such as carcinoid, gastrointestinal stromal tumors, lymphoma, leiomyosarcoma, adenocarcinoma, and intraductal papillary mucinous neoplasm [5, 16].
Preoperative Evaluation
History
Most MD are asymptomatic and are usually found incidentally when undergoing surgical exploration for other intra-abdominal processes. The most common presentations for symptomatic MD are bleeding, intestinal obstruction, and inflammation.
Episodic painless hematochezia occurs when MD contains ectopic gastric mucosa that secretes hydrochloric acid. This can cause ulceration on the adjacent ileum, leading to bleeding and perforation. Meckel’s diverticulum is the most common etiology of intestinal bleeding in children. Bleeding can occur in MD containing malignancies, but this has been described predominantly in adults [17, 18].
Obstruction related to MD can be caused by intussusception, volvulus, or internal abdominal wall herniation. It is the second most common presentation of MD in children, but the most common presentation in adults. Intussusception can occur when the MD inverts into the lumen of the ileum, acting as a lead point. Volvulus most commonly occurs when a loop of small bowel twists around a fibrous band remnant or an incompletely obliterated omphalomesenteric duct connecting the small bowel to the umbilicus. Loops of bowel can also be obstructed through an internal herniation of bowel around a mesodiverticular band, which is the remnant vitelline artery from the diverticulum to the mesentery [13, 17]. Littre’s hernia is the presence of a Meckel’s diverticulum in a hernia sac, most commonly in an inguinal (50 % of cases), umbilical, or femoral hernia [7, 19].
Meckel’s diverticulitis most commonly occurs secondary to an enterolith in the lumen, similar to the pathophysiology of acute appendicitis, and most commonly occurs in adult patients. Inflammation of the MD can also occur from peptic ulceration of the ileal mucosa or from a foreign body in the diverticular orifice (i.e., gallstones or ingested foreign objects such as bones or toothpicks) [17, 20].
If the omphalomesenteric duct is completely patent or if the distal portion is patent, then umbilical drainage can also be a presenting symptom.
Exam
In most studies, the most common presenting symptom of MD in children under the age of 5 years is episodic painless hematochezia. This bleeding is acute and can be massive, often requiring blood transfusions. The stool is often dark red or “currant jelly.” These bleeding ulcers can also perforate and cause peritonitis. Obstruction is the second most common presentation and is more common in adults. These patients present with crampy abdominal pain, nausea, bilious emesis, and obstipation. Patients presenting with diverticulitis have signs and symptoms that are similar to those of acute appendicitis [4, 13].
Laboratory Testing
If the patient is presenting with rectal bleeding, a hemoglobin, hematocrit, and type and cross are required. A white blood cell count is also helpful to delineate an inflammatory process such as diverticulitis. If the patient is presenting with obstructive symptoms, a metabolic panel is indicated to evaluate for electrolyte abnormalities.
Imaging
Abdominal X-Ray
Conventional X-rays may occasionally show an enterolith, evidence of a bowel obstruction, or a gas-/fluid-filled diverticulum. If a patient has a perforation, then free air could optimally be seen on upright chest X-ray or at left lateral decubitus film. Barium studies may show a blind-ending pouch in the distal ileum, but it has low sensitivity secondary to poor filling of the diverticulum from stenosis of the neck, obstructing intestinal contents, contraction of the tunica muscularis, and/or overlapping of small bowel [21].
Ultrasound
High-resolution ultrasonography has been utilized in diagnosing MD. It classically would show a fluid-filled structure in the mid-lower abdomen with a connection to a peristaltic small bowel loop [22]. During episodes of diverticulitis, it would have an appearance similar to appendicitis.
Computed Tomography (CT)
CT is currently the most widely used imaging modality to evaluate for abdominal pain, obstructive symptoms, or potential inflammation. In a study by Kawamoto et al., MD was detected in up to 47.5 % of all patients and 57 % of symptomatic patients [23]. It is the best modality for Meckel’s diverticulitis and obstruction. An adjunctive imaging modality is CT enterography, where a large volume of oral contrast is ingested to achieve adequate small bowel distention to evaluate the small bowel [21].
Meckel’s Scan
This is the most accurate diagnostic study (sensitivity and specificity >90 %) for detecting MD containing gastric mucosa. It is performed using technetium-99 m, which is taken up by the mucin-secreting cells of the ectopic gastric mucosa. It is a commonly used diagnostic test for rectal bleeding since it is noninvasive with a low radiation burden [21, 24].
Angiography
This is another useful imaging modality if the patient presents with active large volume bleeding. Meckel’s diverticulum can be diagnosed by seeing a blush at the site of the persistent vitelline artery arising from the distal SMA. This has less sensitivity as it is only diagnostic if there is bleeding of at least >0.5 ml/min [21, 25]. This modality also allows the option of angiographic embolization that may control bleeding until operative resection.
Other Tests
Double Balloon Enteroscopy
This is a less commonly used modality for diagnosis. It is performed by transoral or transanal endoscopy. This diagnostic tool has also been described as an aid in surgical resection, where the endoscopic light is directed to the abdominal wall indicating the location of the diverticulum and allowing resection through a single small umbilical incision [9, 17, 26]. This modality has largely been replaced by laparoscopic evaluation.
Laparoscopy
Despite all of our imaging modalities, MD is still a difficult diagnosis to make, except in the setting of rectal bleeding with a positive Meckel’s scan. In cases when the diagnosis is uncertain, laparoscopy is recommended as the definitive diagnostic and therapeutic intervention [27, 28].
Surgical Indications
There is clear consensus that surgical resection is indicated for all symptomatic MD; however, there is controversy regarding resection of incidentally found MD. In a retrospective study of MD, Cullen et al. described a 6.4 % cumulative lifetime risk of developing complications and found surgical resection of incidental MD had less morbidity compared to surgical resection of complicated MD; therefore, they recommend surgical resection of all MD [29]. Alternatively, Soltero et al. recommended against prophylactic resection as they found a 9 % risk of morbidity after MD resection in these patients and calculated that 800 asymptomatic diverticula had to be removed to prevent one death [3]. Between these two extreme positions, other studies, such as Park et al., found that certain characteristics may be predictive for the development of complications and recommended diverticulectomy of incidental diverticula that meet any of the following four criteria: (1) male sex, (2) age less than 50 years, (3) diverticular length greater than 2 cm, and (4) abnormal features of the diverticula such as thickened tissue or a palpable mass [14]. Other studies have also recommended prophylactic resection if there is a narrow diverticular base [30]. At this time, most pediatric surgeons will perform a resection of an incidentally identified MD if it does not significantly increase the risk of the primary procedure.
Technique
Special Considerations
If a patient is presenting with obstruction, then either laparotomy or laparoscopy (performed by a surgeon experienced in laparoscopic small bowel resection and lysis of adhesions) is the procedure of choice. If a Littre’s hernia is present, then a MD resection should be performed first followed by herniorrhaphy [7, 31]. There are various new surgical techniques that are being published, such as hand-assisted laparoscopic resection and single-site surgery; however, these are beyond the scope of this chapter and will not be discussed further [32–34]. Instead, this chapter will focus on laparoscopic MD resection.
Anatomy
As described above, a MD is found on the antimesenteric border of the ileum within 2 ft of the ileocecal valve. It receives its own blood supply from the mesentery of the ileum, usually from the remnant vitelline artery.
Instruments
30° laparoscope, 10 or 12 mm trocar through the umbilicus for the laparoscope and subsequent endoscopic stapler, two additional 5 mm trocars as working ports, atraumatic bowel graspers, a laparoscopic electrocautery or other energy devices, or vascular clip can all prove useful for this procedure.
Steps
Standard general anesthesia and preoperative antibiotics are utilized. A preoperative time-out should be performed. For patients with hematochezia, blood products should be readily available. A Foley catheter should be placed for decompression of the bladder if the patient has not voided immediately before entering the OR suite. A chlorhexidine/alcohol skin preparation should be performed, and the patient should be draped to expose the entire abdomen.
-
The first step is entrance into the abdomen. We recommend entrance using the Veress needle technique or the Hassan technique using a 10–12 mm trocar through the umbilicus into the peritoneum under direct visualization and subsequent insufflation.
-
Insufflation is achieved using carbon dioxide pneumoperitoneum at 8–12 mmHg.
-
A 30° laparoscope should then be introduced through the umbilical port.
-
Two additional 5 mm trocars should then be inserted through the left lower quadrant and suprapubic region, similar to sites used for an appendectomy (Fig. 31.2).
Fig. 31.2. 
Trocar locations.
-
The cecum should first be identified, and this will be facilitated by moving the patient into a left lateral decubitus and Trendelenburg’s position.
-
A systematic exploration of the small intestine from the terminal ileum to the jejunum should then be performed in a retrograde fashion using blunt bowel graspers.
-
Once located, the diverticulum will need to be released from the mesentery by dividing the feeding vessel using an energy device or vascular clip.
-
The MD should then be grasped and delivered through the umbilical port site under direct visualization by placement of the laparoscope through one of the other working ports. The umbilical incision may need to be extended.
-
A segmental resection of the diverticulum and adjacent ileum should be performed if the patient is presenting with bleeding to ensure removal of all ectopic mucosa and the bleeding ileal ulcer (Fig. 31.3).
-
Re-approximation of the small bowel may be performed using a hand-sewn anastomosis or a side-to-side functional end-to-end stapled anastomosis.
Fig. 31.3. 
Segmental resection of MD and adjacent small bowel.
-
In the case of an incidentally found MD or if the patient is not presenting with bleeding or perforation, then a diverticulectomy may be performed by either a wedge resection (Fig. 31.4) with a hand-sewn anastomosis or a tangential diverticulectomy using a stapler (Fig. 31.5), taking care not to narrow the lumen.
Fig. 31.4. 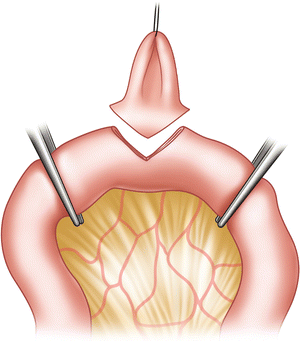
Wedge resection of MD.
Fig. 31.5. 
Tangential diverticulectomy with stapler.
-
Once the anastomosis is completed and hemostasis is achieved, the fascia and skin should be closed per the surgeon’s preference.




Pearls/Pitfalls
Although the majority of the ectopic mucosa is found at the tip of the diverticulum, there is the risk of potentially leaving remnant ectopic mucosa behind in the ileum when a tangential stapled resection is performed [35, 36]. This technique of MD resection is especially discouraged in patients presenting with bleeding or perforation and, therefore, a segmental resection of the MD and 2–3 cm of ileum to each side is frequently recommended [37, 38]. However, Palanivelu et al. report that a simple tangential diverticulectomy in complicated MD without evidence of base involvement is an acceptable alternative. He performed a tangential diverticulectomy in 10 patients with complicated MD and found that of the patients that were followed up (8 patients for 24 months), there was no evidence of disease recurrence [39].
Even in the cases of incidentally found MD, there is controversy as to the recommended surgical procedure. Sarli et al. recommend tangential resection if the MD is asymptomatic/uncomplicated and the diverticulum is not broad based or short, but suggest that all specimens should be inspected after removal to ensure there is no ectopic tissue at the resection margin [40]. A short diverticulum is defined as one that is less than twice the length of the base [37]. At this time, most surgeons will perform a tangential resection for uncomplicated MD.
Postoperative Care
Outcomes/Complications
The most common complication is bowel obstruction secondary to adhesions, occurring in up to 5–10 % of patients [29, 33, 41]. Other complications include bleeding, infection (wound infection and intra-abdominal abscess), wound dehiscence, anastomotic leak, and incisional hernia. Overall surgical morbidity and mortality in symptomatic MD are reported as 2–13 % and 0–2 %, respectively [8, 11, 14, 29, 42]. Park et al. reported a higher incidence of morbidity and mortality in incidental MD (20 % and 1 %) compared to symptomatic MD (13 % and 0 %); however, the complications could not be attributed to the actual diverticulectomy in the incidental patients [14]. A 1–2 % morbidity after an incidental diverticulectomy is more widely reported, although the majority of these studies do not describe the surgical techniques used in the patients [29]. In a 10-year retrospective review on outcomes after laparoscopic-assisted Meckel’s diverticulectomy, Chan et al. reported one complication of a wound infection in a total of 18 patients but required conversion of two cases to laparotomy for ischemic bowel and intussusception [43]. Shalaby et al. had no reported complications after laparoscopic resection of incidental and symptomatic MD at 1 year based on a study of 30 patients, and only one patient required conversion to a laparotomy for intestinal duplication [28]. Additional studies also describe low morbidity of 7–12 % for laparoscopic resection of MD, similar to laparotomy [30, 35, 44].
The consensus in the current literature is that laparoscopy is a safe and feasible method of managing MD without evidence of increased morbidity or mortality compared to laparotomy. However, it is clear that laparoscopy has several advantages compared to laparotomy. Ruscher et al. performed a retrospective study comparing the length of hospital stay and cost of laparoscopic versus open Meckel’s diverticulectomy [12]. Patients that underwent an open procedure had longer hospital lengths of stay and incurred higher hospital charges.
Summary
-
Although a rare anomaly, MD is the most commonly found congenital defect in the gastrointestinal tract, and the majority are asymptomatic.
-
The most common presenting symptoms are bleeding, obstruction, and inflammation.
-
There are multiple imaging modalities available to evaluate for a MD, but the only imaging modality with high specificity and sensitivity is a Meckel’s scan for bleeding secondary to ectopic gastric mucosa.
-
Surgical resection is indicated for all symptomatic MD, but there is controversy in regard to resection of incidentally found MD.
-
Most complication rates published are combined for open and laparoscopic diverticulectomy, but there is more recent data showing laparoscopic resection is a safe and cost-effective method for surgical management of a MD.
References
Haber JJ. Meckel’s diverticulum. Am J Surg. 1947;73:468–85.
Janjua RM, Shultka R, Goebbel L, Pait TG, Shields CB. The legacy of Johann Friedrich Meckel the Elder (1724-1774): a 4-generation dynasty of anatomists. Neurosurgery. 2010;66(4):758–71.
Soltero M, Alexander B. The natural history of Meckel’s diverticulum and its relation to incidental removal. A study of 202 cases of diseased Meckel’s diverticulum found in King County, Washington, over a fifteen year period. Am J Surg. 1976;132(2):168–73.
Chen JJ, Lee H, Yeng CY, Chan WT, Jiang CB, Sheu JC, Wang NL. Meckel’s diverticulum: factors associated with clinical manifestations. ISRN Gastroenterol. 2014;2014:390869.
Alemayehu H, Hall M, Desai AA, St Peter SD, Snyder CL. Demographic disparities of children presenting with symptomatic Meckel’s diverticulum in children’s hospitals. Pediatr Surg Int. 2014;30(6):649–53.
Carlson B. Human embryology and developmental biology. 5th ed. Philadelphia: Saunders; 2012.
Skandalakis PN, Zoras O, Skandalakis JE, Mirilas P. Littre hernia: surgical anatomy, embryology, and technique of repair. Am Surg. 2006;72(3):238–43.
St-Vil D, Brandt ML, Panic S, Bensoussan AL, Blanchard H. Meckel’s diverticulum in children: a 20-year review. J Pediatr Surg. 1991;26(11):1289–92.
Vane DW, West KW, Grosfeld JL. Vitelline duct anomalies. Experience with 217 childhood cases. Arch Surg. 1987;122(5):542–7.
Konvolinka CW. Patent omphalomesenteric duct. Surgery. 2012;131(6):689–90.
Matsagas M, Fatouras M, Koulouras B, Giannoukas AD. Incidence, complications and management of Meckel’s diverticulum. Arch Surg. 1995;130:143–6.
Ruscher KA, Fisher JN, Hughes CD, Neff S, Lerer TJ, Hight DW, Bourque MD, Campbell BT. National trends in the surgical management of Meckel’s diverticulum. J Pediatr Surg. 2011;46(5):893–6.
Turgeon DK, Barnett JJ. Meckel’s diverticulum. Am J Gastroenterol. 1990;85(7):777–81.
Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950–2002). Ann Surg. 2005;241(3):529–33.
Sancar S, Demirci H, Sayan A, Arikan A, Candar A. Meckel’s diverticulum: ten years’ experience. Ulus Cerrahi Derg. 2015;31(2):65–7.
Jadloweic C, Bayron J, Marshall WT. Is an incidental Meckel’s diverticulum truly benign? Case Rep Surg. 2015;10:679097.
Kharma R, Jain VK. Emergency surgery for Meckel’s diverticulum. World J Emerg Surg. 2008;3:27.
Caracappa D, Gullà N, Lombardo F, Burini G, Castellani E, Boseli C, Gemini A, Burattini MF, Covarelli P, Noya G. Incidental finding of carcinoid tumor on Meckel’s diverticulum: case literature review, should prophylactic resection be recommended? World J Surg Oncol. 2014;12:44.
Chan KW, Lee KH, Mou JW, Cheung ST, Tam YH. The use of laparoscopy in the management of Littre’s hernia in children. Pediatr Surg Int. 2008;24(7):855–8.
Chan KW. Perforation of Meckel’s diverticulum caused by a chicken bone: a case report. J Med Case Reports. 2009;3:48.
Elsayes KM, Menias CO, Harvin HJ, Francis IR. Imaging manifestations of Meckel’s diverticulum. AJR Am J Roentgenol. 2007;189(1):81–8.
Mostbec GH, Liskutin J, Dorffner R, Bittmann B, Resinger M. Ultrasonographic diagnosis of a bleeding Meckel’s diverticulum. Pediatr Radiol. 2000;30(6):382.
Kawamoto S, Raman SP, Blackford A, Hruban RH, Fishman EK. CT detection of symptomatic and asymptomatic Meckel diverticulum. AJR Am J Roentgenol. 2015;205(2):281–91.
Sinha CK, Pallewatte A, Easty M, Coppi P, Pierro A, Misra D, Biassoni L. Meckel’s scan in children: a review of 183 cases referred to two paediatric surgery specialist centres over 18 years. Pediatr Surg Int. 2013;29(5):511–7.
Mahajan MS. An unusual appearance of Meckel’s diverticulum as site of bleed on gastrointestinal bleeding scan. World J Nucl Med. 2013;12(3):111–5.
Fukushima M, Kawanami C, Inoue S, Okada A, Ima Y, Inokuma T. A case series of Meckel’s diverticulum: usefulness of double-balloon enteroscopy for diagnosis. BMC Gastroenterol. 2014;14:155.
Sagar J, Kumar V, Shah DK. Meckel’s diverticulum: a systematic review. J R Soc Med. 2006;99(10):501–5.
Shalaby RY, Soliman SM, Fawy M. Laparoscopic management of Meckel’s diverticulum in children. J Pediatr Surg. 2005;40(3):562–7.
Cullen J, Kelly KA, Moir CR, Hodge DO, Zinsmeister AR, Melton LJ. Surgical management of Meckel’s diverticulum. An epidemiologic, population-based study. Ann Surg. 1994;220(4):564–9.
Prasad S, Chui CH, Jacobsen AS. Laparoscopic-assisted resection of Meckel’s diverticulum in children. JSLS. 2006;10(3):310–6.
Qin D, Liu G, Wang Z. Littre’s hernia in a paediatric patient. Afr J Paediatr Surg. 2014;11(4):351–3.
Qi S, Huang H, Wei D, Lv C, Yang Y. Diagnosis and minimally invasive surgical treatment of bleeding Meckel’s diverticulum in children using double-balloon enteroscopy. J Pediatr Surg. 2015;50(9):1610–2.
Duan X, Ye G, Bian H, Yang J, Zheng K, Liang C, Sun X, Yan X, Yang H, Wang X, Ma J. Laparoscopic vs. laparoscopically assisted management of Meckel’s diverticulum in children. Int J Clin Exp Med. 2015;8(1):94–100.
Chan KW, Lee KH, Wong HY, Tsui SY, Wong YS, Pang KY, Mou JW, Tam YH. Laparoscopic excision of Meckel’s diverticulum in children: what is the current evidence? World J Gastroenterol. 2014;20(41):15158–62.
Alemayehu H, Stringel G, Lo IJ, Golden J, Pandya S, McBride W, Muensterer O. Laparoscopy and complicated Meckel diverticulum in children. JSLS 2014;18(3). doi:10.4293/JSLS.2014.00015.
Mukai M, Takamatsu H, Noguchi H, Fukushige T, Tahara H, Kaji T. Does the external appearance of a Meckel’s diverticulum assist in choice of laparoscopic procedure? Pediatr Surg Int. 2002;18:231–3.
Varcoe RL, Wong SW, Taylor CF, Newstead GL. Diverticulectomy is inadequate treatment for short Meckel’s diverticulum with heterotopic mucosa. ANZ J Surg. 2004;74:869–72.
Schmid SW, Schafer M, Krahenbuhl L, Buchler MW. The role of laparoscopy in symptomatic Meckel’s diverticulum. Surg Endosc. 1999;13:1047–9.
Palanivelu C, Rangarajan M, Senthilkumar R, Madankumar MV. Laparoscopic management of symptomatic Meckel’s diverticula: a simple tangential stapler excision. JSLS. 2008;12(1):66–70.
Sarli L, Costi R. Laparoscopic resection of Meckel’s diverticulum: report of two cases. Surg Today. 2001;31:823–5.
Lüdtke FE, Mende V, Köhler H, Lepsien G. Incidence and frequency or complications and management of Meckel’s diverticulum. Surg Gynecol Obstet. 1989;169(6):537–42.
Piñero A, Martínez-Barba E, Canterast M, Rodriquez JM, Castellanos G, Parrilla P. Surgical management and complications of Meckel’s diverticulum in 90 patients. Eur J Surg. 2002;168:8–12.
Chan KW, Lee KH, Mou JW, Cheung ST, Tam YH. Laparoscopic management of complicated Meckel’s diverticulum in children: a 10 year review. Surg Endosc. 2008;22(6):1509–12.
Prasad TR, Chui CH, Singaporewalla FR, Ong CPC, Low Y, Yap TL. Meckel’s diverticular complications in children: is laparoscopy the order of the day? Pediatr Surg Int. 2007;23:141–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Rodeberg, D., Abdulhai, S. (2017). Laparoscopic Meckel’s Diverticulectomy. In: Walsh, D., Ponsky, T., Bruns, N. (eds) The SAGES Manual of Pediatric Minimally Invasive Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-43642-5_31
Download citation
DOI: https://doi.org/10.1007/978-3-319-43642-5_31
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43640-1
Online ISBN: 978-3-319-43642-5
eBook Packages: MedicineMedicine (R0)