
Abstract
Toxic multinodular goiter (TMNG) and autonomously functioning thyroid nodules (AFTN) are common causes of hyperthyroidism. We discuss the nonsurgical management of TMNG and AFTN.
Radioactive iodine (RAI) is the most commonly used medical therapy for TMNG and AFTN with overall high cure rates. Antithyroid drugs (ATDs) are used often in preparation for RAI and should be considered in the elderly, in those with severe hyperthyroidism, or in individuals with cardiac comorbidities in which exacerbation of hyperthyroidism could have adverse outcomes.
Other medical therapies such as thermal ablation (for AFTN only) or long-term therapy with ATDs can be considered in special circumstances.
Radiofrequency ablation (RFA) and percutaneous laser ablation (PLA) have been used for more than 10 years, and they appear to be safe. RFA and PLA are effective in reducing the size of the nodule and control of hyperthyroidism in more than half of treated cases. While surgery and RAI are still the standard therapeutic options for TMNG and AFTN, both RFA and PLA are increasingly being used in patients with AFTN where both surgery and RAI are not feasible or acceptable options. Future studies are needed to improve the classification of these patient subgroups, while technology will improve the efficacy, and health economics will improve the availability of ablative procedures throughout the world.
Percutaneous ethanol injection (PEI) into the nodule was an ablative therapy used in the 1980s–1990s. Ethanol can dissipate beyond the target with the occurrence of significant complications. Therefore, PEI is no longer considered an option for AFTN.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Toxic multinodular goiter
- Autonomously functioning thyroid nodules
- Toxic adenoma
- Marine-Lenhart syndrome
- Hyperthyroidism
- Antithyroid drugs
- Graves’ disease
- Radioactive iodine
- Percutaneous ethanol injection
- Radiofrequency ablation
- Percutaneous laser ablation
Introduction
Hyperthyroidism occurs in 1.3 % of the population [1]. The most common cause of hyperthyroidism is Graves’ disease, followed by toxic multinodular goiter (TMNG) and autonomously functioning thyroid nodules (AFTN). The co-occurrence of autonomously functioning thyroid nodule(s) or TMNG with Graves’ disease is termed Marine-Lenhart syndrome or nodular Graves’. It is a rare presentation of hyperthyroidism that occurs in around 1–2.7 % of Graves’ disease cases [2, 3].
The standard therapy for TMNG and AFTN is either thyroid surgery or radioactive iodine (131I) therapy. However, in certain circumstances, such as patients with high surgical risk or patients not interested in surgery who also have a low radioactive iodine uptake, among others, alternative medical therapies can be considered. Herein we will discuss the nonsurgical management of toxic multinodular goiter, toxic thyroid nodules, and Marine-Lenhart syndrome.
Role of Radioactive Iodine (131I)
Since the discovery of artificial radioactivity in 1934, there has been growing interest of the potential applications of radioactive isotopes for the diagnosis and treatment of diseases. In regard to the thyroid gland, 128iodine(I) was the first isotope used to evaluate thyroid gland uptake in rabbits, but with a decay half-life of only 25 min, its use was not practical [4]. In the late 1930s, the radioactive isotopes 130I, 126I, and 131I were used for the study of thyroid iodine uptake and metabolism using a Geiger counter. In 1941,131I was used for the first time to treat hyperthyroidism in humans. 131I is now widely used for treatment of hyperthyroidism; it is a radionuclide taken up by thyroid tissue, and it has predominantly β-emissions, thus causing cell death. It has a decay half-life of about 8 days.
Efficacy
The ideal goal of therapy with radioactive iodine (RAI) is to achieve euthyroidism. However, in some cases hypothyroidism may develop after treatment with RAI. The cure rate defined as the development of hypothyroidism or euthyroidism after one dose of RAI varies among studies. It ranges between 60 and 93 % for TMNG [5–9] and between 71 and 97 % for AFTN [6, 8, 9]. Hyperthyroidism resolves at a mean time of 5.4 months [8]. RAI is also safe and efficacious in elderly individuals, with a reported cure rate of 80 % for TMNG and 86 % for AFTN at 12 months [9].
After RAI there is usually reduction in size of the goiter or of the toxic nodule. In TMNG the gland decreases in volume by 43 % at 24 months [7]. For AFTN, the nodule reduces in size by 35 % after 3 months and by 45 % at 24 months [10]. Ideally one dose of RAI should cure hyperthyroidism. However, if there is persistence of hyperthyroidism 6 months after RAI [11] or recurrence of hyperthyroidism, a second dose can be given. On occasions it can take up to 24 months for hyperthyroidism to completely resolve after RAI [9]; therefore, the use of antithyroid drugs (ATDs) can be considered with periodic monitoring of thyroid tests to evaluate for cure. In the case of severe refractory hyperthyroidism, surgery should be considered, specifically thyroid lobectomy for AFTN or near-total/total thyroidectomy for TMNG.
Treatment with RAI is also indicated for the rare patients with TMNG or AFTN that failed surgical therapy (<1 %) and are thus still hyperthyroid [12, 13].
Factors Associated with RAI Efficacy
Certain clinical and laboratory factors were thought to affect the response to RAI therapy such as size of the goiter, gender, age at diagnosis of thyrotoxicosis, TSH value, and pretreatment with antithyroid drugs. Of these factors, gender and age at time of diagnosis are not clearly associated with RAI therapy response in observational studies [5, 7]. However, larger goiters have been associated with lower cure rates [6]. Patients with low but detectable TSH values had a higher cure rate and hypothyroidism than those with undetectable TSH values before RAI [14]. The potential effect of pretreatment with antithyroid drugs and the response to RAI therapy will be discussed later.
Dose and Regimen
Even though RAI have been used for the treatment of hyperthyroidism since the 1940s [15], there is still debate on the appropriate dose or regimen used to cure hyperthyroidism while avoiding permanent hypothyroidism.
Dose and regimens used for RAI are often institution dependent, but in general, treatment with RAI can be given either as (1) a standard fixed activity or (2) as a calculated dose based on nodule size (for AFTN) or gland size (for TMNG) corrected for the RAI uptake. Fixed activities can be given as a standard fixed activity for everybody or by adapting the standard activity to the thyroid gland size. Usual fixed doses of 131I range between 10 and 30 mCi. For toxic adenoma and TMNG, higher fixed doses (20–30 mCi) are associated with higher cure rates and higher rates of hypothyroidism compared to lower doses (around 10 mCi). In a study comparing 2 doses of RAI, hypothyroidism occurred in 26 % of patients who received a higher dose of RAI compared to 11 % of those who received a lower dose [16].
Calculated doses of RAI are given with the goal of controlling hyperthyroidism and minimizing hypothyroidism. The premise is that a larger nodule (for AFTN) or larger goiter (for TMNG) requires higher RAI activity, and a higher RAI uptake, which means the tissue will more avidly take iodine, will require a lower RAI activity to achieve euthyroidism. Therefore, the dose of RAI administered can be calculated as follows:
Activity (μCi or MBq) = \( \frac{\mathrm{Gland}\ \mathrm{weight}\left(\mathrm{g}\right)\times \mathrm{desired}\ \mathrm{dose}\ \mathrm{per}\ \mathrm{gram}\ \mathrm{of}\ \mathrm{thyroid}\ \mathrm{tissue}}{\mathrm{Percentage}\ \mathrm{of}\ 24 - \mathrm{h}\ \mathrm{thyroid}\ \mathrm{uptake}} \) × 100
The gland weight in grams can be estimated by palpation, by ultrasound, or by nuclear imaging; in practice the first two methods are most commonly used. The desired dose to the thyroid tissue is expressed as the activity desired per gram of tissue (μCi/g or MBq/g), and it has ranged in studies between 90 and 200 μCi/g or 3.33–7.4 MBq/g. An activity of radioiodine between 150 and 200 μCi is usually recommended [11]. Several studies have reported outcomes of RAI given as fixed doses or calculated doses in hyperthyroidism [16, 17]; however, head-to-head trials comparing both methods are scarce. A study comparing different protocols of RAI therapy in toxic adenoma found a higher cure rate in the calculated high-dose protocol compared to a calculated low-dose, fixed high-dose, or fixed low-dose protocol [18]. At the same time, the rate of hypothyroidism was higher in the calculated and fixed high-dose groups compared to the lower-dose groups. A systematic review and meta-analysis of studies comparing fixed doses or estimated doses, based on thyroid size, to calculated doses in patients with hyperthyroidism showed no significant differences in cure of hyperthyroidism between the two methods. They included in the analysis patients with Graves’ disease, TMNG, and AFTN [19].
Pretreatment with Antithyroid Drugs
The antithyroid drugs (ATDs), methimazole, propylthiouracil, and carbimazole, inhibit the synthesis of new thyroid hormone from the thyroid gland, thus controlling the hyperthyroidism of TMNG, AFTN, or Graves’ disease. In the case of TMNG and toxic adenoma, they are frequently used before definite therapy with RAI.
In theory, RAI therapy can exacerbate signs and symptoms of thyrotoxicosis; therefore, the use of ATDs depletes thyroid hormone stores and can potentially ameliorate or prevent exacerbation of hyperthyroidism induced by RAI therapy. The benefit of this approach has not been thoroughly investigated in RCTs, and the use of ATDs in this setting is controversial with some advocating against the use of ATDs given the lack of evidence of benefit. Still some institutions use them routinely before administration of RAI. It is thought that RAI therapy exacerbates symptoms of thyrotoxicosis through induction of radiation thyroiditis. In a study of 34 patients with hyperthyroidism (11 with TMNG, 2 with AFTN, and 21 with Graves’ disease) who didn’t receive ATDs, all patients with TMNG had elevations of thyroid hormones after RAI compared to only 29 % of those with Graves’ disease. However, none had worsening symptoms of thyrotoxicosis [20]. Despite these findings there are reports in the literature of thyroid storm and severe hyperthyroidism after RAI [21, 22].
When considering pretreatment with ATDs, three main factors need to be addressed: (1) the severity of hyperthyroidism; (2) the patient’s comorbidities such as cardiovascular disease, cardiac arrhythmias, patient’s age, and overall health; and (3) the risk of decreasing the effectiveness of RAI in patients taking ATDs.
Patients with severe hyperthyroidism, elderly patients, or patients with cardiac disease are at higher risk of developing complications from exacerbation of the hyperthyroid state. Consequently these are the patients in which pretreatment with ATDs should be considered.
If ATDs are continued at the time of RAI, there is clear evidence that the cure rate in TMNG and AFTN is significantly lower compared to when no ATDs are given [23]. However, whether ATDs reduce the efficacy of 131I if they are stopped a few days before therapy is controversial. A systematic review and meta-analysis of 14 randomized controlled trials of the effect of ATDs on RAI found that the adjunctive use of ATDs was associated with higher RAI failure rates compared to no ATDs [24]. However, only 5/14 studies included patients with TMNG or AFTN, and 5 of the included studies gave ATDs concomitantly with RAI.
The most common practice is to discontinue ATDs before RAI, and the time interval between discontinuation of ATD and RAI therapy varies among studies between 2 and 7 days. If carbimazole is stopped 3 days before RAI, the cure rates were similar than if no ATDs were given [25].
If ATDs are given before RAI, it is preferred to use either methimazole or carbimazole instead of propylthiouracil (PTU) given the higher risk of liver dysfunction [26] and evidence from observational studies, suggesting radioresistance of the thyroid gland with PTU [27].
ATDs can be given for several weeks until hyperthyroidism is controlled; however, TSH should not be normalized to avoid the inadvertent therapy of the normal thyroid tissue, thus increasing the long-term risk of hypothyroidism. ATDs should be discontinued 3–7 days before RAI [11] and reinitiated 7 days later if there are concerns about risks associated with transient increase in thyroid hormone values. The dose of ATDs should be gradually decreased with the goal to discontinue them 1 month after RAI.
Should rhTSH Be Used to Augment RAI Uptake and Efficacy?
Recombinant human TSH (rhTSH) is commonly used with RAI ablative therapy after thyroidectomy for thyroid cancer. In the case of TMNG, the use of rhTSH has been considered in cases of low RAI uptake to increase the uptake and potentially increase the efficacy of RAI and the thyroid absorbed dose. Observational studies [28, 29] and one RCT [30] using rhTSH before RAI have included patients with nontoxic multinodular goiter and a subset of patients with TMNG with subclinical hyperthyroidism or mild hyperthyroidism. The RAI uptake increased two- to fourfold 24 h and 72 h after rhTSH, respectively. No clinical worsening of hyperthyroidism was reported after 0.1 or 0.3 mg of rhTSH. However, thyroid hormone levels increase after rhTSH, and exacerbation of hyperthyroidism can occur [31]. Consequently, more studies evaluating the safety and efficacy of rhTSH augmented RAI in TMNG compared to RAI alone are needed before recommending its use.
Risk of Hypothyroidism
The risk of hypothyroidism persists years after treatment with 131I. Rates of subclinical hypothyroidism or overt hypothyroidism as high as 72 % have been reported 8 years after RAI [32]. Higher doses of RAI are more likely to cause hypothyroidism [18, 32]. For TMNG the rate of hypothyroidism 5 years after treatment is between 7 % and 14 % for lower and higher doses of RAI, respectively [7, 33, 34]. The average rate of hypothyroidism is 2.7 %/year with 64 % of patients hypothyroid 24 years after RAI [35].
For autonomously functioning thyroid nodules, the rate of hypothyroidism is between 7 % and 55 % when lower and higher doses of RAI are given, respectively [17, 36], and the cumulative incidence of hypothyroidism is 7 % at 1 year, 28 % at 5 years, and up to 60 % at 20 years [37]. Besides the dose of RAI administered, other risk factors associated with higher rates of hypothyroidism include the presence of thyroid antibodies, a smaller or non-palpable thyroid gland, and the use of ATDs before 131I [6, 34, 38].
To prevent hypothyroidism, ATDs combined with thyroid hormone were used in 149 patients, with a reported rate of overt hypothyroidism of 3.3 %, 6.8 years after RAI [39]. The idea of this approach was to first control hyperthyroidism with ATDs and then give enough thyroid hormone to suppress TSH to avoid RAI uptake by normal thyroid tissue. This approach has not been validated and is therefore not recommended. Because the risk of hypothyroidism after RAI in TMNG and AFTN is significant, thyroid function tests should be periodically monitored even after clinical and biochemical evidence of euthyroidism.
Contraindications to RAI
Absolute contraindications to RAI therapy for hyperthyroidism from TMNG or toxic adenomas are pregnancy, concomitant diagnosis of thyroid cancer (for which surgery is the most appropriate therapy), women planning pregnancy within the next few months of therapy with RAI, or people unable to comply with radiation safety procedures [11].
Risks of RAI
Cancer Risk
The Cooperative Thyrotoxicosis Therapy Follow-Up Study has followed patients treated for hyperthyroidism in 26 medical centers in the United States and England. At 6 years of follow-up, the incidence of thyroid cancer mortality and leukemia was not increased in the patients treated with 131I compared to the patients treated with other modalities [40, 41]. At a mean follow-up of 21 years, there was no difference in overall cancer mortality in the 131I-treated patients compared to the general population. However, there was a small but significant increase in thyroid cancer deaths (SMR 3.94. CI: 2.52–5.86) in the 131I-treated patients [42]. Patients who died from thyroid cancer were more likely to have had toxic nodular goiter, suggesting that the increased risk in thyroid cancer might be related to nodular goiter itself and not to RAI.
Mortality and CVD Mortality Risk
Population-based studies have found an increased risk in CVD and all-cause mortality in patients with hyperthyroidism treated with 131I when compared to mortality estimates in the general population [43, 44]. A major limitation in these studies is the inability to differentiate the contribution of the RAI treatment itself to the increased mortality which could be solely explained by hyperthyroidism.
Induction of Thyroid Autoimmunity
Appearance of Graves-like disease after RAI for TMNG or AFTN has been repeatedly reported. Its occurrence is rare between 1 and 4 % [45, 46]. It usually manifests 3–6 months after RAI with elevation of thyroid hormone levels, appearance of thyrotropin receptor antibodies (TRAB), and a thyroid scan showing diffuse radioiodine uptake.
Thyroglobulin, a protein synthesized solely by follicular cells in the thyroid gland, is released to the systemic circulation after RAI. Therefore, it is thought that an increase in thyroid antigens following RAI may stimulate an immune response toward the TSH receptor.
In a study evaluating the risk to develop Graves’ disease after RAI, the phenotype occurred more commonly for TMNG than for toxic adenoma with rates of 2 % and 0.3 %, respectively, but none of those with toxic nodular goiter that didn’t receive 131I developed the disease [46]. This finding suggests that RAI therapy induces the thyroid autoimmune response. If a patient with TMNG or toxic adenoma develops recurrence of hyperthyroidism months after RAI therapy, it is much more likely to be from recurrence of autonomy than Graves’ disease. However, we recommend getting a thyroid 121I uptake and scan, and if there is diffuse uptake throughout the gland, Graves’ disease is more likely, and treatment with ATDs or retreatment with RAI should be considered.
Marine-Lenhart Syndrome
The diagnosis of this entity is usually made by the presence of hyperthyroidism, positive thyrotropin receptor antibodies, and thyroid nodules seen on ultrasound and thyroid uptake and scan. The treatment for Marine-Lenhart syndrome follows the same principles discussed. Radioactive iodine and surgery are the most commonly used therapies. The dose of RAI required for cure is usually similar to the dose required for TMNG or AFTN, which is higher than the dose required for Graves’.
Role of Antithyroid Drugs
Mechanism of Action
The thionamide compounds available in the United States are methimazole (MMI) and propylthiouracil (PTU). Carbimazole (CBZ) is another thionamide available and commonly used in some European and Asian countries. These compounds alleviate hyperthyroidism by inhibiting thyroid hormone synthesis. They inhibit the oxidation from iodide to iodine and iodine organification catalyzed by thyroperoxidase, a necessary step for the incorporation of iodine into thyroglobulin. Thionamides also inhibit coupling of iodotyrosines and alter the structure of thyroglobulin [47]. Carbimazole is metabolized to methimazole in serum. Propylthiouracil, but not methimazole or carbimazole, inhibits the conversion from T4 to T3 in extrathyroidal tissues.
Efficacy
ATDs control hyperthyroidism but don’t cause remission in toxic nodular goiter. After 12 months of therapy with ATDs, 95 % of patients with TMNG have recurrence of hyperthyroidism when ATDs are discontinued [48]. If ATDs are chosen as the main treatment, lifelong therapy will be required. Accordingly, surgery, radioactive iodine, or other ablative therapies are usually preferred over ATDs in the treatment of TMNG and AFTN (see Table 8.1). A study evaluating the effects of long-term therapy with methimazole in diffuse toxic goiter compared to RAI showed that methimazole therapy for 10 years is overall safe. Euthyroidism was achieved in 93 % of patients on MMI [49]. There were more thyroid test abnormalities at follow-up in the group that received RAI. However, there was a high number loss to follow up over all.
Nevertheless, long-term therapy with ATDs can be considered in elderly individuals with cardiac disease or other significant comorbidities when the risk for radioactive iodine or surgery is high. This is of particular importance for TMNG, because other therapeutic modalities to be discussed later, such as radiofrequency or thermal ablation, are effective in toxic adenomas but less so in TMNG.
Side Effects
Allergic reactions such as pruritus, rash, urticaria, and arthralgias occur in 5 % of people taking these medications and are the most common side effects. Agranulocytosis, polyarthritis, vasculitis, and hepatitis are rare but serious side effects. Agranulocytosis, which is an idiosyncratic reaction, occurs in 0.2–0.5 % with MMI, CBZ, or PTU [50]. Polyarthritis, vasculitis, and fulminant hepatitis are more commonly reported with PTU than MMI (frequency <1 %) [50]. Fulminant hepatitis occurs in 1:10,000 adults on PTU and is more common in children [26]. Liver dysfunction can also occur with MMI and is usually a cholestatic pattern [51]. Given the concern of significant hepatitis with PTU associated with deaths and liver transplantation, in most circumstances, MMI and CBZ are the first-line drug therapies for hyperthyroidism.
Role of Ablative Therapies
A large number of patients with nodular thyroid disease are advanced in age and have non-thyroidal comorbidities that increase the risk of a surgical intervention. It is also not uncommon for these patients to have large nodules without a very high uptake of radioactive iodine which leads to the need to use large doses of RAI (by comparison with Graves’ disease patients). On this background the developments of ultrasonography over the last couple decades has allowed the creation of procedures that target the thyroid nodules percutaneously with delivery of high energy or chemical agents in the nodular tissue under direct ultrasound visualization. The main area of use for these procedures has been the benign, nontoxic thyroid nodules. However, these procedures have also been employed in patients with toxic nodules that for cultural or other nonmedical issues have refused surgery or RAI. In almost all studies, the targeted nodules have been large nodules, many with documented compressive symptoms or at risk of producing such symptoms. The ultrasound-based procedures targeting thyroid nodules are radiofrequency ablation (RFA), percutaneous laser ablation (PLA), and percutaneous ethanol injection (PEI). Table 8.1 summarizes the clinical situations where the interventions described here could be considered.
Radiofrequency Ablation
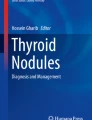
Radiofrequency ablation or radiofrequency thermal ablation (RFA) is the most utilized of the ablative therapies. Its use is based on the principle that ultrasound-based energy delivery into the thyroid tissue will raise the local temperature to about 101–105°C which will lead to local thrombosis followed by ischemia and fibrosis and subsequent shrinkage of the treated tissue volume (see Fig. 8.1). The needles employed are 14–18 G, some allowing further deployment of one to four expandable hooks that are then making contact with multiple portions of the targeted nodule. The procedure in all cases is performed under continuous ultrasound guidance. There are at least two techniques in practice: fixed-needle technique and “moving-shot” technique which are distinguished by the degree of manipulating the needle during the procedure. The energy delivered per nodule is a variable between reports, and it has been delivered for most patients in multiple sessions (mean is about two sessions/nodule from combining multiple studies data). The sessions were repeated based on thyroid function and/or nodule size response and performed 1–2 months apart. Local anesthesia with 2 % lidocaine has been employed for the superficial cervical tissue and the thyroid capsule. In most cases the cystic content, if present, is aspirated before the energy is delivered. No significant side effects or hospitalization was noted in these patients. A sensation of heat in the neck was reported by patients. That did not affect the course of the procedure. If pain developed the power was decreased or ablation stopped completely for few seconds. Some reports described repeat biopsies prior to procedure to ensure the benign character of the treated lesions.

Ultrasound images of thyroid nodule before and after radiofrequency ablation (RFA). Pre-RFA (a, b) and 3 months post-RFA (c, d) images of thyroid nodule in transverse (a, c) and longitudinal (b, d) views. Three months after RFA (c, d), the nodule volume decreased by 52 %
The efficacy of the procedure has been tested in a number of clinical studies. One of the early series [52] reported on 94 patients that included both toxic (28 patients) and nontoxic nodules (66 patients). They have utilized the 14G needles with four expandable hooks. Thyroid function normalized in all those with subclinical hyperthyroidism and in about 50 % of patients with overt hyperthyroidism. Added benefit was the decrease in the size of thyroid nodule in 50 % of patients. The discomfort was minimal and always local and there was no need for additional therapy for this side effect. There were no hospitalizations, local infections, nerve injuries, or any injuries to the neck vital structures. The authors followed with a more rigorous assessment of RFA [53] comparing ten patients with solid toxic nodules (<30 % cystic component) that they compared with a similar group of patients followed with observation only. Nontoxic nodules were evaluated the same way. Reassuringly 40 % of patients reached euthyroidism and another 40 % experienced a reduction in the dose of methimazole needed to control their hyperthyroidism. More importantly none developed worsening of their thyroid parameters. All the treated nodules shrank and the process was already noticeable at 1 month and continued for the 12 months of observation. The average decrease in volume was 86 % over that period. A simple symptom scoring system (no symptoms = 0, severe symptoms = 6) was employed reflecting compressive symptoms and esthetic complaints, and it was very encouraging to find the score improving in treated patients (from 3.4/6 to 0.6 at 12 months), while it worsened in the control group (3.0 to 4.1 at 12 months).
While one might wonder if these results are population specific, similar data emerged at about the same time from Korea. Those researchers [54] reported initially on 9 patients with toxic nodules that were treated with RFA. They have utilized 18G electrodes without additional prongs and used local anesthesia for pain control. A mean of 2.2 sessions were performed (range 1–4). The volume reduction was a mean of 36.4 % at 1 month and 70.7 % at 6 months. TSH level normalized in five out of nine patients, improved yet still suppressed in three, and remained elevated in one patient. Encouragingly no patient reported aggravation of hyperthyroid symptoms after therapy. Symptom and cosmetic scores improved in all but one patient. No adverse effects except for local heat and neck discomfort were reported, and no procedure had to be discontinued because of such symptoms. Most recently the same group reported on a multicenter study that evaluated the outcome of RFA for autonomously functioning thyroid nodules at five Korean institutions [55]. Following 44 patients they noticed again a rapid decline in the volume of the nodule (from 46 % at 1 month to 82 % at the last follow-up, mean of 20 months). The thyroid function normalized in 36/44 patients (82 %), but 18 % of patients still had a suppressed TSH despite repeat RFA. No case of hypothyroidism developed. The score for symptoms and cosmetic appearance improved significantly, while no patient reported deterioration of local symptoms or symptoms of hyperthyroidism.
RFA was repeated if TSH did not normalize, and thus a mean of 1.8 sessions/nodule was performed (maximum up to 6). Their results are thus consistent with the other studies on RFA.
It thus appears that the thyroid function is normalized in half to three quarters of these patients. It also appears that the moving-shot technique is slightly superior regarding volume reduction to the fixed-needle technique with expandable electrodes. It is also purported to be easier to perform given the difficulty with tracking and moving 2–4 separate electrodes. Clearly both techniques require a significant amount of expertise, and all the radiologists involved in these studies were trained specifically in this procedure. This is an essential component in order to replicate these results in other practices, both regarding efficacy and minimizing the side effects. Volume reduction was significantly correlated with the vascularity of the lesion at the initial ultrasound in one report but not described on the others.
Reassuringly no adverse effects were noted except for local pain which was fairly straightforward to control. It should be noted that none of these reports list any negative impact of RFA on subsequent thyroid surgery, but it is not clear that such sequence has been followed in any of the RFA-treated patients. Another practical issue to be considered is that of cost. We are not aware of any report of cost comparisons with surgery or radioactive iodine, but based on our experience, RFA will be of significantly lower cost compared with surgery but probably more expensive than RAI in the USA. Combining the efficacy and safety data with patients’ medical limitations and cultural preferences will be an ongoing process to understand the potential role for this procedure in clinical practice. As is, RFA evolves into an attractive approach for the therapy of AFTN.
Percutaneous Laser Ablation (PLA)
This procedure is very similar to the technique utilized for RFA. It has also similar side-effect profile with maybe slightly inferior efficacy. The protocol utilized in various trials has varied. The needles employed have been between 14 and 21G, and the number of fibers utilized to deliver the energy has been up to four, depending on the size and shape of the nodule. The treatments were delivered usually in 1–2 sessions spaced 1 month apart, preceded by local anesthesia with lidocaine. The total energy delivery per treatment was about 1800 J, but this also varied between reports. To prevent local pain and limit injection site edema, an injectable steroid can be used intramuscularly. Still local pain is reported but it appears to rarely require therapy, and when if it does so, it responds to NSAIDs. Occasionally repositioning of the needle away from the capsule is required in order to diminish pain. One of the early PLA series was completed in Italy [56] and treated both patients with isolated toxic nodules and patients with toxic MNG. After a median of three PLA sessions, they noted normalization of thyroid levels in all patients with toxic nodules and in 50 % of those with toxic MNG. Reassuringly there was only a mild and transient increase in T3/T4 values after the therapy session. The median decrease in nodule volume was 59 % at 1 year (range 24–72 %), and the nodules had a nonhomogeneous appearance on ultrasound. As RAI is a standard treatment modality for AFTN and toxic MNG, another Italian trial went further [57] and included 15 patients with large toxic nodules that received laser ablation followed by RAI 1 month later and compared them with RAI-alone therapy. Interestingly in 60 % of patients, TSH normalized at 1 month after PLA, and in 20 % of patients, RAI therapy was no longer employed. Nodule shrinkage was evident at 1 month post-therapy and at 2 years post-therapy reached 71 % reduction in the combination therapy compared with 47 % in the RAI-alone group.
Local compressive symptoms improved rapidly post-PLA, but at 2 years they were not different between the groups. From a nuclear medicine perspective, it is pertinent that the dose of RAI required for therapy was 21 % lower in the combination therapy group. This also led to outpatient therapy in all such patients as opposed to only 50 % of the RAI-only group (based on the RAI therapy regulations at the time in Italy). Similar data was obtained in other trials as well [58, 59], while only one early trial reported lack of significant benefit of PLA on AFTN [60].
The available data suggests that PLA is better suited for one or at most two autonomous nodules while being less effective for MNG. It is important to note the expected changes in the ultrasound appearance of nodules treated by PLA, to avoid raising unnecessary concerns. Thus, at 1 week post-procedure, ultrasound reveals a central area of cavitation (which is anechoic), surrounded by a rim of charred tissue (appearing hyperechoic on ultrasound), and at the periphery there is a hypoechoic area thought to represent coagulative necrosis [56].
PLA of TMNG has also been studied in some of the studies mentioned earlier. However, given the limited targeting of this procedure, it is to be expected that other toxic nodules can continue hypersecreting thyroid hormones and likely patients will remain hyperthyroid after one to two PLA sessions. The factors that influence the ultimate response in nodule size are not well defined, but it is presumed that the composition of the nodule (i.e., colloid vs. water content) and, like with RFA, the vascularity of the lesion are playing a significant role in the overall response [56]. Unfortunately no head-to-head trials between the RFA and PLA have been performed, and given the costs of the equipment involved and the training required to achieve sufficient expertise in each of these procedures, it is unlikely that such a trial will take place.
Alcohol Ablation
Alcohol ablation for solid nodules is to be distinguished from alcohol injection into a thyroid cyst. The ablation of solid nodules, also known as percutaneous ethanol injection (PEI), has been employed since 1990. The procedure was being done under anesthesia or sedation at some centers or without any such support at others. It employed 95 % alcohol that is injected using a 20–22G needle directly in the nodule in question. The volume injected varied with some centers using 1/3 of the volume of the nodule and other using a variable dose between 1 and 5 ml administered slowly over 2–5 min [61–63]. There are usually multiple injections that allow targeting different areas in the nodule. The side-effect profile, as reported initially, was largely represented by a burning sensation noted in ~ 30 % of sessions that was reported to last 30–60 min and radiate to the jaw or sides of the neck.
Early studies [61, 64] reported the effectiveness of PEI alone or followed by RAI as similar to RAI alone. It controlled hyperthyroidism in almost 100 % of patients but offered additionally a significant reduction in nodule size combined with the ability to use a lower dose of RAI.
These encouraging initial efficacy results were followed by slightly different reports more recently [65] in which 45 % of individuals either did not reach euthyroidism or had recurrence of it within 3 years. When the procedure was employed in TMNG, all patients had persistent hyperthyroidism.
After the procedure started to be employed by a larger number of medical centers, a number of reports started to surface that redefined the adverse event rate and profile of PEI. It thus was found that the local discomfort rate and intensity was higher than reported initially. Also it appeared that the alcohol could infiltrate the surrounding extranodular and occasionally extrathyroidal tissue [66, 67]. This pro-fibrotic effect could clearly be a complicating factor for subsequent surgery needed in case of PEI failure. Also reports of subcutaneous hematoma and temporary hoarseness surfaced [68], while a more detailed profile of the adverse effects associated with PEI was depicted by Bennedbaek and Hegedus [69] as they described additional problems that followed the procedure: transient thyrotoxicosis, permanent ipsilateral facial dysesthesia, increased tear flow, and para-nodular fibrosis impeding subsequent surgery in few patients but various degrees of pain and tenderness in majority of PEI-treated patients. A severe case of toxic laryngitis and dermatitis [70] showed the possibility for the alcohol to flow back from the nodule into the surrounding tissues with significant consequences. These reports led to a departure from the view of PEI as a routine procedure and started to limit its subsequent use. As some of these cases have occurred even with experienced operators, the use of the procedure has declined rapidly over the last few years, and it is now mainly used for sclerosing cystic thyroid lesions and for therapy of small thyroidal or lymphatic foci of papillary thyroid carcinoma [71].
Of note, all these procedures are known to distort the histology of the nodule and thus limit the usefulness of subsequent fine-needle aspiration. While toxic nodules are not usually subjected to cytological evaluation before therapy, it is possible that an FNA would be pursued at a later time, and the clinicians should be aware of the possible atypical results brought on by the procedure-induced tissue damage.
Based on the available evidence regarding ablative procedures, as a practical approach, in a select subgroup of patients, such as individuals who refuse surgery, or are at high surgical risk and have access to centers with excellent expertise in these procedures, RFA (or PLA) could be offered first, followed by RAI in patients that are persistently hyperthyroid.
Abbreviations
- AFTN:
-
Autonomously functioning thyroid nodule
- ATDs:
-
Antithyroid drugs
- CVD:
-
Cardiovascular disease
- PEI:
-
Percutaneous ethanol injection
- PLA:
-
Percutaneous laser ablation
- RAI:
-
Radioactive iodine
- RFA:
-
Radiofrequency ablation
- TMNG:
-
Toxic multinodular goiter
References
Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. 2002;87(2):489–99.
Charkes ND. Graves’ disease with functioning nodules (Marine-Lenhart syndrome). J Nucl Med. 1972;13(12):885–92.
Carnell NE, Valente WA. Thyroid nodules in Graves’ disease: classification, characterization, and response to treatment. Thyroid. 1998;8(8):647–52.
Becker DV, Sawin CT. Radioiodine and thyroid disease: the beginning. Semin Nucl Med. [Historical Article Research Support, Non-U.S. Gov’t]. 1996;26(3):155–64.
Goncalves E, Castro JA, Gross JL. Standard dose 131I therapy for toxic multinodular goiter in an endemic goiter region. Braz J Med Biol Res. 1986;19(6):723–9.
Erem C, Kandemir N, Hacihasanoglu A, Ersoz HO, Ukinc K, Kocak M. Radioiodine treatment of hyperthyroidism: prognostic factors affecting outcome. Endocrine. 2004;25(1):55–60.
Nygaard B, Hegedus L, Ulriksen P, Nielsen KG, Hansen JM. Radioiodine therapy for multinodular toxic goiter. Arch Intern Med. [Research Support, Non-U.S. Gov’t]. 1999;159(12):1364–8.
Kang AS, Grant CS, Thompson GB, van Heerden JA. Current treatment of nodular goiter with hyperthyroidism (Plummer’s disease): surgery versus radioiodine. Surgery. [Comparative Study]. 2002;132(6):916–23; discussion 23.
Erkan ME, Demirin H, Asik M, Celbek G, Yildirim M, Aydin Y, et al. Efficiency of radioactive I-131 therapy in geriatric patients with toxic nodular goiter. Aging Clin Exp Res. 2012;24(6):714–7.
Nygaard B, Hegedus L, Nielsen KG, Ulriksen P, Hansen JM. Long-term effect of radioactive iodine on thyroid function and size in patients with solitary autonomously functioning toxic thyroid nodules. Clin Endocrinol (Oxf). [Research Support, Non-U.S. Gov’t]. 1999;50(2):197–202.
Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract. [Practice Guideline]. 2011;17(3):456–520.
Erickson D, Gharib H, Li H, van Heerden JA. Treatment of patients with toxic multinodular goiter. Thyroid. [Clinical Trial Comparative Study]. 1998;8(4):277–82.
Vidal-Trecan GM, Stahl JE, Eckman MH. Radioiodine or surgery for toxic thyroid adenoma: dissecting an important decision. A cost-effectiveness analysis. Thyroid. 2004;14(11):933–45.
Pedersen-Bjergaard U, Kirkegaard C. Serum TSH and the response to radioiodine treatment of toxic multinodular goitre. Eur J Endocrinol. 1997;137(4):365–9.
Kaplan MM, Meier DA, Dworkin HJ. Treatment of hyperthyroidism with radioactive iodine. Endocrinol Metab Clin North Am. [Comparative Study Review]. 1998;27(1):205–23.
Sonmez B, Erem C, Dogan I, Ersoz HO, Sonmez M. Efficacy of low and high fixed dose radioactive iodine therapy in patients with toxic nodular goiter. Minerva Endocrinol. 2011;36(2):117–21.
Ross DS, Ridgway EC, Daniels GH. Successful treatment of solitary toxic thyroid nodules with relatively low-dose iodine-131, with low prevalence of hypothyroidism. Ann Intern Med. [Research Support, U.S. Gov’t, P.H.S.]. 1984;101(4):488–90.
Zakavi SR, Mousavi Z, Davachi B. Comparison of four different protocols of I-131 therapy for treating single toxic thyroid nodule. Nucl Med Commun. [Comparative Study Controlled Clinical Trial Randomized Controlled Trial Research Support, Non-U.S. Gov’t]. 2009;30(2):169–75.
de Rooij A, Vandenbroucke JP, Smit JW, Stokkel MP, Dekkers OM. Clinical outcomes after estimated versus calculated activity of radioiodine for the treatment of hyperthyroidism: systematic review and meta-analysis. Eur J Endocrinol. [Comparative Study Meta-Analysis Review]. 2009;161(5):771–7.
Koornstra JJ, Kerstens MN, Hoving J, Visscher KJ, Schade JH, Gort HB, et al. Clinical and biochemical changes following 131I therapy for hyperthyroidism in patients not pretreated with antithyroid drugs. Neth J Med. 1999;55(5):215–21.
Thyroid storm shortly after 131 I therapy of a toxic multinodular goiter? Am J Med. [Case Reports]. 1972;52(6):786–96.
McDermott MT, Kidd GS, Dodson LE, Jr., Hofeldt FD. Radioiodine-induced thyroid storm. Case report and literature review. Am J Med. [Case Reports Review]. 1983;75(2):353–9.
Clerc J, Izembart M, Dagousset F, Jais JP, Heshmati HM, Chevalier A, et al. Influence of dose selection on absorbed dose profiles in radioiodine treatment of diffuse toxic goiters in patients receiving or not receiving carbimazole. J Nucl Med. 1993;34(3):387–93.
Walter MA, Briel M, Christ-Crain M, Bonnema SJ, Connell J, Cooper DS, et al. Effects of antithyroid drugs on radioiodine treatment: systematic review and meta-analysis of randomised controlled trials. Bmj. [Meta-Analysis Research Support, Non-U.S. Gov’t Technical Report]. 2007;334(7592):514.
Walter MA, Christ-Crain M, Schindler C, Muller-Brand J, Muller B. Outcome of radioiodine therapy without, on or 3 days off carbimazole: a prospective interventional three-group comparison. Eur J Nucl Med Mol Imaging. [Controlled Clinical Trial]. 2006;33(6):730–7.
Cooper DS, Rivkees SA. Putting propylthiouracil in perspective. J Clin Endocrinol Metab. [Evaluation Studies]. 2009;94(6):1881–2.
Imseis RE, Vanmiddlesworth L, Massie JD, Bush AJ, Vanmiddlesworth NR. Pretreatment with propylthiouracil but not methimazole reduces the therapeutic efficacy of iodine-131 in hyperthyroidism. J Clin Endocrinol Metab. 1998;83(2):685–7.
Duick DS, Baskin HJ. Utility of recombinant human thyrotropin for augmentation of radioiodine uptake and treatment of nontoxic and toxic multinodular goiters. Endocr Pract. 2003;9(3):204–9.
Duick DS, Baskin HJ. Significance of radioiodine uptake at 72 hours versus 24 hours after pretreatment with recombinant human thyrotropin for enhancement of radioiodine therapy in patients with symptomatic nontoxic or toxic multinodular goiter. Endocr Pract. [Clinical Trial Multicenter Study]. 2004;10(3):253–60.
Nielsen VE, Bonnema SJ, Boel-Jorgensen H, Veje A, Hegedus L. Recombinant human thyrotropin markedly changes the 131I kinetics during 131I therapy of patients with nodular goiter: an evaluation by a randomized double-blinded trial. J Clin Endocrinol Metab. [Clinical Trial Randomized Controlled Trial Research Support, Non-U.S. Gov’t]. 2005;90(1):79–83.
Magner J. Problems associated with the use of thyrogen in patients with a thyroid gland. N Engl J Med. [Comment Letter]. 2008;359(16):1738–9; author reply 9.
Kahraman D, Keller C, Schneider C, Eschner W, Sudbrock F, Schmidt M, et al. Development of hypothyroidism during long-term follow-up of patients with toxic nodular goitre after radioiodine therapy. Clin Endocrinol (Oxf). [Research Support, Non-U.S. Gov’t]. 2012;76(2):297–303.
Huysmans DA, Hermus AR, Corstens FH, Kloppenborg PW. Long-term results of two schedules of radioiodine treatment for toxic multinodular goitre. Eur J Nucl Med. 1993;20(11):1056–62.
Khanna CM, Magdum M, Ravishankar L, Dham DN, Chugh P. Evaluation of long-term results of two schedules of treatment for toxic multinodular goitre with radioiodine therapy (I 131). J Assoc Physicians India. [Clinical Trial Comparative Study]. 1996;44(2):102–5.
Holm LE, Lundell G, Israelsson A, Dahlqvist I. Incidence of hypothyroidism occurring long after iodine-131 therapy for hyperthyroidism. J Nucl Med. [Comparative Study Research Support, Non-U.S. Gov’t]. 1982;23(2):103–7.
Tzavara I, Tzanela M, Vlassopoulou B, Kouyioumoutzakis G, Kyriazopoulou V, Alevizaki C, et al. Long term thyroid function after (131)I treatment for toxic adenoma. Hormones (Athens). 2002;1(2):99–103.
Ceccarelli C, Bencivelli W, Vitti P, Grasso L, Pinchera A. Outcome of radioiodine-131 therapy in hyperfunctioning thyroid nodules: a 20 years’ retrospective study. Clin Endocrinol (Oxf). 2005;62(3):331–5.
Ahmad AM, Ahmad M, Young ET. Objective estimates of the probability of developing hypothyroidism following radioactive iodine treatment of thyrotoxicosis. Eur J Endocrinol. 2002;146(6):767–75.
Paghera B, Panarotto MB, Maira G, Magri GC, Bertagna F, Bosio G, et al. (1)(3)(1)I treatment of toxic nodular goiter under combined thyrostatic-thyromimetic medication is at low risk of late hypothyroidism. Q J Nucl Med Mol Imaging. 2010;54(3):341–7.
Dobyns BM, Sheline GE, Workman JB, Tompkins EA, McConahey WM, Becker DV. Malignant and benign neoplasms of the thyroid in patients treated for hyperthyroidism: a report of the cooperative thyrotoxicosis therapy follow-up study. J Clin Endocrinol Metab. 1974;38(6):976–98.
Saenger EL, Thoma GE, Tompkins EA. Incidence of leukemia following treatment of hyperthyroidism. Preliminary report of the Cooperative Thyrotoxicosis Therapy Follow-Up Study. JAMA. 1968;205(12):855–62.
Ron E, Doody MM, Becker DV, Brill AB, Curtis RE, Goldman MB, et al. Cancer mortality following treatment for adult hyperthyroidism. Cooperative Thyrotoxicosis Therapy Follow-up Study Group. Jama. [Research Support, Non-U.S. Gov’t Research Support, U.S. Gov’t, P.H.S.]. 1998;280(4):347–55.
Franklyn JA, Maisonneuve P, Sheppard MC, Betteridge J, Boyle P. Mortality after the treatment of hyperthyroidism with radioactive iodine. N Engl J Med. [Comparative Study Research Support, Non-U.S. Gov’t]. 1998;338(11):712–8.
Metso S, Jaatinen P, Huhtala H, Auvinen A, Oksala H, Salmi J. Increased cardiovascular and cancer mortality after radioiodine treatment for hyperthyroidism. J Clin Endocrinol Metab. [Research Support, Non-U.S. Gov’t]. 2007;92(6):2190–6.
Nygaard B, Faber J, Veje A, Hegedus L, Hansen JM. Transition of nodular toxic goiter to autoimmune hyperthyroidism triggered by 131I therapy. Thyroid. [Research Support, Non-U.S. Gov’t]. 1999;9(5):477–81.
Meller J, Siefker U, Hamann A, Hufner M. Incidence of radioiodine induced Graves’ disease in patients with multinodular toxic goiter. Exp Clin Endocrinol Diabetes. [Comparative Study]. 2006;114(5):235–9.
Werner SC, Ingbar SH, Braverman LE, Utiger RD. Werner & Ingbar’s the thyroid: a fundamental and clinical text. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2005.
van Soestbergen MJ, van der Vijver JC, Graafland AD. Recurrence of hyperthyroidism in multinodular goiter after long-term drug therapy: a comparison with Graves’ disease. J Endocrinol Invest. [Comparative Study]. 1992;15(11):797–800.
Azizi F, Ataie L, Hedayati M, Mehrabi Y, Sheikholeslami F. Effect of long-term continuous methimazole treatment of hyperthyroidism: comparison with radioiodine. Eur J Endocrinol. [Clinical Trial Comparative Study Randomized Controlled Trial]. 2005;152(5):695–701.
Watanabe N, Narimatsu H, Noh JY, Yamaguchi T, Kobayashi K, Kami M, et al. Antithyroid drug-induced hematopoietic damage: a retrospective cohort study of agranulocytosis and pancytopenia involving 50,385 patients with Graves’ disease. J Clin Endocrinol Metab. [Evaluation Studies]. 2012;97(1):E49–53.
Arab DM, Malatjalian DA, Rittmaster RS. Severe cholestatic jaundice in uncomplicated hyperthyroidism treated with methimazole. J Clin Endocrinol Metab. [Case Reports]. 1995;80(4):1083–5.
Spiezia S, Garberoglio R, Milone F, Ramundo V, Caiazzo C, Assanti AP, et al. Thyroid nodules and related symptoms are stably controlled two years after radiofrequency thermal ablation. Thyroid. [Clinical Trial]. 2009;19(3):219–25.
Faggiano A, Ramundo V, Assanti AP, Fonderico F, Macchia PE, Misso C, et al. Thyroid nodules treated with percutaneous radiofrequency thermal ablation: a comparative study. J Clin Endocrinol Metab. [Comparative Study Controlled Clinical Trial Research Support, Non–U.S. Gov’t]. 2012;97(12):4439–45.
Baek JH, Moon WJ, Kim YS, Lee JH, Lee D. Radiofrequency ablation for the treatment of autonomously functioning thyroid nodules. World J Surg. 2009;33(9):1971–7.
Sung JY, Baek JH, Jung SL, Kim JH, Kim KS, Lee D, et al. Radiofrequency ablation for autonomously functioning thyroid nodules: a multicenter study. Thyroid. [Multicenter Study]. 2015;25(1):112–7.
Barbaro D, Orsini P, Lapi P, Pasquini C, Tuco A, Righini A, et al. Percutaneous laser ablation in the treatment of toxic and pretoxic nodular goiter. Endocr Pract. [Clinical Trial]. 2007;13(1):30–6.
Chianelli M, Bizzarri G, Todino V, Misischi I, Bianchini A, Graziano F, et al. Laser ablation and 131-iodine: a 24-month pilot study of combined treatment for large toxic nodular goiter. J Clin Endocrinol Metab. [Clinical Trial]. 2014;99(7):E1283–6.
Dossing H, Bennedbaek FN, Bonnema SJ, Grupe P, Hegedus L. Randomized prospective study comparing a single radioiodine dose and a single laser therapy session in autonomously functioning thyroid nodules. Eur J Endocrinol. [Comparative Study Randomized Controlled Trial Research Support, Non-U.S. Gov’t]. 2007;157(1):95–100.
Spiezia S, Vitale G, Di Somma C, Pio Assanti A, Ciccarelli A, Lombardi G, et al. Ultrasound-guided laser thermal ablation in the treatment of autonomous hyperfunctioning thyroid nodules and compressive nontoxic nodular goiter. Thyroid. 2003;13(10):941–7.
Pacella CM, Bizzarri G, Spiezia S, Bianchini A, Guglielmi R, Crescenzi A, et al. Thyroid tissue: US-guided percutaneous laser thermal ablation. Radiology. [Clinical Trial]. 2004;232(1):272–80.
Del Prete S, Russo D, Caraglia M, Giuberti G, Marra M, Vitale G, et al. Percutaneous ethanol injection of autonomous thyroid nodules with a volume larger than 40 ml: three years of follow-up. Clin Radiol. 2001;56(11):895–901.
Monzani F, Caraccio N, Goletti O, Lippolis PV, Casolaro A, Del Guerra P, et al. Five-year follow-up of percutaneous ethanol injection for the treatment of hyperfunctioning thyroid nodules: a study of 117 patients. Clin Endocrinol (Oxf). 1997;46(1):9–15.
Guglielmi R, Pacella CM, Bianchini A, Bizzarri G, Rinaldi R, Graziano FM, et al. Percutaneous ethanol injection treatment in benign thyroid lesions: role and efficacy. Thyroid. 2004;14(2):125–31.
Zingrillo M, Modoni S, Conte M, Frusciante V, Trischitta V. Percutaneous ethanol injection plus radioiodine versus radioiodine alone in the treatment of large toxic thyroid nodules. J Nucl Med. [Clinical Trial Comparative Study Randomized Controlled Trial]. 2003;44(2):207–10.
Yano Y, Sugino K, Akaishi J, Uruno T, Okuwa K, Shibuya H, et al. Treatment of autonomously functioning thyroid nodules at a single institution: radioiodine therapy, surgery, and ethanol injection therapy. Ann Nucl Med. 2011;25(10):749–54.
Gharib H, Papini E. Thyroid nodules: clinical importance, assessment, and treatment. Endocrinol Metab Clin North Am. [Review]. 2007;36(3):707–35, vi.
Hegedus L. Clinical practice. The thyroid nodule. N Engl J Med. [Review]. 200421;351(17):1764–71.
Brkljacic B, Sucic M, Bozikov V, Hauser M, Hebrang A. Treatment of autonomous and toxic thyroid adenomas by percutaneous ultrasound-guided ethanol injection. Acta Radiol. 2001;42(5):477–81.
Bennedbaek FN, Hegedus L. Percutaneous ethanol injection therapy in benign solitary solid cold thyroid nodules: a randomized trial comparing one injection with three injections. Thyroid. [Clinical Trial Comparative Study Randomized Controlled Trial Research Support, Non-U.S. Gov’t]. 1999;9(3):225–33.
Mauz PS, Maassen MM, Braun B, Brosch S. How safe is percutaneous ethanol injection for treatment of thyroid nodule? Report of a case of severe toxic necrosis of the larynx and adjacent skin. Acta Otolaryngol. [Case Reports]. 2004;124(10):1226–30.
Hay ID, Lee RA, Davidge-Pitts C, Reading CC, Charboneau JW. Long-term outcome of ultrasound-guided percutaneous ethanol ablation of selected “recurrent” neck nodal metastases in 25 patients with TNM stages III or IVA papillary thyroid carcinoma previously treated by surgery and 131I therapy. Surgery. 2013;154(6):1448–54; discussion 54–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
De Ycaza, A.E.E., Stan, M.N. (2017). The Role of Medical Management for Nodular Hyperthyroidism. In: Roman, S., Sosa, J., Solórzano, C. (eds) Management of Thyroid Nodules and Differentiated Thyroid Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-43618-0_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-43618-0_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43616-6
Online ISBN: 978-3-319-43618-0
eBook Packages: MedicineMedicine (R0)