
Abstract
Oocyte cryopreservation has become a great alternative for many women who need to preserve their fertility, especially for those suffering from cancer malignancy, in whom, independently of age, there is a great need to safeguard their reproductive capacity before undergoing the potentially sterilizing treatment. In addition, oocyte cryopreservation is the most valuable option for women who wish to delay their motherhood due to nonmedical-related issues. This situation is increasingly frequent, especially in developed countries, raising the proportion of women at advanced ages that desire to get pregnant.
In addition, oocyte cryo-storage results very useful in many other situations. Therefore, the most common drawbacks involved with ovum donation conducted with fresh oocytes, such as synchronization between donors and recipients, long waiting lists subject to the availability of a suitable donor, and the absence of a quarantine period, can be overcome by the use of vitrified oocytes from donors’ egg-banks. Oocyte cryo-storage brings additional advantages to ART programs being helpful to solve different clinical situations as in low-responder patients, unpredictable unavailability of semen sample collection from the male partner, risk of suffering ovarian hyperstimulation syndrome (OHSS), or some other cases in which the embryo transfer is not advisable.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Learning Objectives-
To understand the basic principles of vitrification and how we can achieve it in our clinical settings
-
To analyze the contribution of oocyte vitrification to clinical practice
-
To describe the methodology, logistics, and technical aspects related to oocyte vitrification
1 Introduction
The essential role of cryopreservation in ART has become obvious since the establishment of the infertility treatment, bringing flexibility and efficiency to the practice. Semen and embryo cryopreservation has been a successful strategy, and its routine application is a reality since the onset of the IVF practice. However, in spite of numerous studies conducted over two decades, the reliability of oocyte cryopreservation is relatively recent. All of the efforts made are clearly justified, mostly because an efficient oocyte cryopreservation program is actually quite welcome and widely applied in ART, since there are many indications for this strategy, including egg-banking for ovum donation. Beneficiaries of this approach include cancer patients who need an option for fertility preservation before undergoing their oncological treatment [1], or women who wish to delay their motherhood due to a variety of reasons [2], government restrictions on IVF [3, 4], ethical reasons against embryo cryopreservation and practical reasons such us unavailability of the male gamete the day of pickup [5, 6].
Despite all of this wide diversity of potential applications, egg-banking has not been a routine procedure until relatively recent. This fact can be explained because the methodology to cryopreserve human oocytes was disappointing, with results that have not always been reproducible, especially during the 1980s and 1990s. During the early 2000s, vitrification brought efficient and reproducible outcomes to the clinical practice. Some fundamental principles of cryobiology would be helpful to understand how difficult it has been to reach the goal of safe cryopreservation of human oocytes.
2 Cryobiology Background
There are some reasons that could explain the low rate of successes initially observed with the first protocols available for oocytes cryopreservation. At first, the size and shape of the oocytes are intrinsic cell features that strongly challenge the outcome. These gametes are the largest cells of the human body, fact that could explain, at least in part, the great differences in cryotolerance between them and, for example, the spermatozoa. In addition, the spherical shape of the oocyte could disturb the uniform distribution of cryoprotectants (CPAs) along the cytoplasm. In addition, considering the oocytes as a unique cell, there is 50% choice of survival and 50% choice of cell death. This situation is completely different from the one observed in tissues composed of millions or thousands of cells, i.e., semen samples, in which the damage could be compensated in different proportions.
Other major factors responsible for the high oocyte sensitivity to cryopreservation include chilling injury and intracellular ice crystal formation. These factors are related to the cryopreservation method. There are two main strategies in cryobiology : slow freezing and vitrification. During the former, the cells are gradually dehydrated in the presence of CPAs, and the temperature is lowered at a very slow cooling rate (−0.3 °C) [7]. In this way, the cells are exposed to low temperatures during an extended period of time, which can lead to what is known as chilling injury [8]. At the final stage, water solidifies into ice crystals. Chilling injury can be defined as the irreversible damage following exposure of cells to low temperatures, before the nucleation of ice [9]. This detrimental event affects mainly the cytoskeleton [10] and cell membranes [11]. The ice crystal formation within the cytoplasm must be avoided at all cost in order to guarantee the survival and integrity of the cells when they are later thawed. Chilling injury can be minimized during vitrification by the use of high cooling rates [12].
Vitrification, in particular by means of methodologies that use a minimum volume, yields extremely successful outcomes, that have not been achieved with other approaches [6]. The physical phenomenon of vitrification takes place when the solidification of the solution occurs not by ice crystallization but by extreme elevation in viscosity, which is achieved by using extremely high cooling rates from −15,000 to −30,000 °C per minute, allowing to avoid the risk of chilling injury [12]. This ice-free cryopreservation method has been modified in order to optimize results. One such modification has been to reduce the volume of the vitrification solution containing the oocytes, which allows the CPA concentration and, consequently, the cytotoxicity to be decreased [13, 14]. As mentioned, this procedure circumvents the two major limiting factors for achieving optimal cryopreservation: chilling injury [14] and ice formation [15]. Chilling injury can be minimized during vitrification by the use of high cooling rates in order to avoid the range of temperature at which chilling takes place (+15 °C to −5 °C) [12]. Additionally, the velocity of the process is dependent on the volume of the vitrification solution. Thus, the smaller the volume of the sample, the higher the cooling rate. On the other hand, direct contact with liquid nitrogen also contributes to increase the cooling rate. Ice formation can be also avoided during vitrification by the use of high CPA concentrations [12], despite the fact that such high concentrations are considered toxic to cells [16]. Nonetheless, an appropriate, phased composition of CPA could mitigate the toxic and osmotic consequences of highly concentrated CPA mixtures [6]. In this way, a combination of two or three of these agents can decrease the individual specific toxicity of these agents. The most common mixture employed for this purpose consists of ethylene glycol, dimethyl sulfoxide, and sucrose or trehalose [6]. To optimize the results, in addition to an appropriate selection of CPAs, it is also helpful to use these agents at as low a concentration as possible, while maintaining the necessary composition able to achieve vitrification. By dramatically increasing the cooling rate, the CPA concentration could be reduced. As a result, a high cooling rate avoids chilling injury, and allows the reduction of the concentration of CPA, thereby preserving the cells at nontoxic concentrations of cryoprotectant. Several approaches fit these conditions. The “minimum drop vitrification” method , proposed by Arav, uses a very small volume of vitrification solution by placing the samples on a specific device that must be cooled very quickly [17]. Extremely high cooling rates are achieved when samples loaded in minimum volume are directly immersed in LN. These methods are also known as open systems. Hermetically closed vials achieve lower cooling rates as compared with open devices. Nevertheless, it is worth mentioning that the direct contact of samples with LN has raised some concerns due to the theoretical risk of cross-contamination mainly because the LN itself is considered as a potential source of pathogen agents, even though no case of cross-contamination has ever been reported in ART in many years of practice, highlighting that such eventuality could be extremely unlikely.
A wide variety of open approaches have been reported in the literature [18,19,20,21,22,23] as well as closed ones [24, 25].
3 Contribution of Oocyte Vitrification to Clinical Practice
3.1 Ovum Donation Programs
Oocyte cryo-storage results are very useful to overcome the most common drawbacks involved with ovum donation as currently applied, such as synchronization between donors and recipients, long waiting lists subject to the availability of a suitable donor, and most importantly the absence of a quarantine period.
3.1.1 Management of Egg-Banking in our Clinical Setting
3.1.1.1 Egg Donor Selection
Spanish Assisted Reproduction Law is based on legislation that was passed in November 1988 (Law 35/1988) (► https://www.boe.es/buscar/doc.php?id=BOE-A-1988-27108). Although some countries already had regulations on, Spain was the first country to create a specific law to cover this area of medicine. Royal Decree 412/1996 and Ministerial Order of 25 March 1996 establish donor requirements , as well as mandatory standard screening procedures, to rule out the transmission of genetic, hereditary, or infectious diseases (► https://www.boe.es/buscar/doc.php?id=BOE-A-1996-9723). In 2006, the newly approved Spanish Law on Assisted Reproduction (Law 14/2006) (► https://www.boe.es/buscar/act.php?id=BOE-A-2006-9292) regulates the requirements for gamete and embryo use and rules on financial compensation aspects.
These are the most important topics included in Spanish Law on Egg Donation:
-
Donation of human gametes is a formal confidential contract between the donor and the reproductive medicine center. Identity of donors must remain anonymous.
-
The donation cannot be revoked.
-
The maximum number of children generated from a single donor’s gametes should not exceed six.
To be accepted as an egg donor, women must be aged between 18 and 35 years old and be healthy. The following steps are necessary for the admission as an egg donor in our clinics:
-
Medical History: During the first consultation, the applicant is interviewed in order to complete the familiar and personal history.
-
Psychological Screening: Psychological evaluation and counseling by a qualified mental health professional. The potential donor is evaluated by a psychologist, to ensure that she fully understands the benefits and risks of egg donation, and is properly motivated to become a donor.
-
Gynecological examination: Menstrual cycles, ovaries examination by ultrasound and antral follicles count are performed. At the same time, body mass index is calculated.
-
Medical Screening: This involves testing for blood type, antibody screening, complete blood count, hemostasis, biochemistry and infectious disease screening, such as HIV, CHV, CHV, and syphilis among others.
-
Genetic Screening: Blood tests for karyotype and for carrier screening tests for severe recessive and X-linked childhood diseases based on NGS (549 genes implicated in 623 disease phenotypes).
3.1.1.2 Ovarian Stimulation
To initiate, an oral contraceptive pill is administered for a maximum of 21 days, which starts on day 1 or 2 of the menses of the previous cycle [26]. After a 5-day washout period after taking the last pill, donors start their stimulation protocol with 150–225 IU of recombinant FSH, 225 IU of HP-hMG, or 150–225 IU of recombinant FSH plus 75 IU HP-hMG. Regular vaginal ultrasound monitoring of donors is performed during FSH injections to measure follicle growth. Daily doses of 0.25 mg GnRH antagonist (Ganirelix or Cetrorelix) start on day 5 of stimulation. Once the leading follicle reaches 18 mm in diameter, a single dose of GnRH agonist is administered to trigger the final oocyte maturation. Transvaginal oocyte retrieval takes place 36 h later after GnRH agonist administration. Donors receive light sedation for the egg retrieval procedure to ensure their comfort, and they rest for 2 h at the clinical setting until they are discharged. In some cases, a vaginal ultrasonography scan is scheduled 2–3 days following egg retrieval [27].
3.1.2 Oocyte Recipients
Oocyte recipients enter our egg donation program for one of the following main diagnoses: premature ovarian failure/menopause, failure to achieve pregnancy after at least three cycles of assisted reproduction techniques, genetic or chromosomal disorders, low response to controlled ovarian hyperstimulation, and recurrent miscarriages.
The vast majority of oocyte recipients undergoes hormone replacement therapy (HRT) . In patients with ovarian function, depot GnRH-a is administered in the midluteal phase of their cycle, or GnRH-ant, administered daily with menstruation for 5 days. HRT is initiated on days 1–3 of the following cycle with oral estradiol valerate or an estradiol transdermal patch [28,29,30]. Recipients without ovarian function are submitted to the same endometrial preparation protocol but are not administered depot GnRH-a. On day 15 or 16 day of HRT, a transvaginal ultrasound is performed to measure endometrial thickness, and serum E2 and progesterone levels are tested. Most recipients are ready to receive embryos within 2–3 weeks after starting HRT , although administration of estradiol valerate can be maintained for a maximum of 50 days until a suitable donation becomes available. Micronized progesterone (800 mg/d, vaginally) is initiated on the day after oocyte donation, and embryos are transferred in the blastocyst stage.
The recipient continues taking estrogen and progesterone with a positive pregnancy test, and these hormonal supplements are then continued through 12 weeks of pregnancy.
Before treatment begins, the recipient undergoes preliminary testing. This assessment phase includes infectious disease screening, e.g., HIV, CHV, CHV, syphilis, and blood type, and Rh factor for both parents. In women older than 45 years old, a recent mammogram, full blood count, coagulation tests, and blood biochemistry may also be required.
3.1.3 Donor-Recipient Matching Process
In our center, we have developed a consistent software tool that accounts for different characteristics of the woman and her partner, as phenotypic features, blood type, etc. The tool provides a list of available donors and number of oocytes available, thus simplifying greatly the process of donor-recipient matching.
Matching is known as the time when we select a donor for a recipient after taking into account several features. We consider many different factors during donor selection: race, reproductive history, the physical characteristics that match those of the female partner, blood type, and genetic carrier screening.
The time for donors-recipients matching has changed in the last 6 years thanks to the improvement in the oocytes vitrification technique and the establishment of the egg donor bank. However, it is important to note that in our current practice, we conduct donations both with fresh and vitrified oocytes, as long as fresh donations are still allowed in our country. The decision about conducting one strategy or the other depends on different circumstances related to the availability of oocytes and the needs of the recipient.
If there is the case that the recipient requires particular rare characteristics, i.e., blood type (0 negative, AB negative), specific race, screening for specific genetic diseases, or partners who would like to have another baby with the same donor as they had before, the procedure would be as follows:
-
First, we use our donor selection database and select one donor or two with the required characteristics. If there are no suitable donors undergoing ovarian stimulation by the moment of the matching, we search for another appropriate donor within the list provided by the tool after the matching process and ask them for their availability to return to initiate the ovarian stimulation for this specific donation.
-
Second, all the oocytes obtained during pickup are vitrified and reserved for the recipient.
-
Finally, the recipient chooses the best time to schedule embryo transfer, and we provide them with instructions to begin HRT depending on the day of the embryo transfer.
-
Recipients who do not need specific characteristics:
-
The date for embryo transfer is already set.
-
First, we reserve oocytes from our egg donor bank.
-
Second, the recipient begins HRT depending on embryo transfer.
-
Finally, we have two options:
-
-
We use fresh oocytes when we have a donor pickup scheduled on the same date as the donation (with the same characteristics as the partner). The prior reservation of oocytes is canceled in these cases.
-
The date for embryo transfer is not set yet.
-
The recipient starts HRT and remains on the waiting list
-
If on these dates an egg donor with the same characteristics as the recipient undergoes pickup, we use fresh oocytes for the egg donation.
-
If the recipient stays on the waiting list longer than 20–25 days, we use oocytes from the egg donor bank.
-
-
3.1.4 Clinical Outcome
The first live birth after vitrification was achieved from a donated oocyte using an open system device (OPS) in 1999 (Kuleshova et al. [33]). Since then, numerous publications using different types of devices corroborate the effectiveness of the technique. ◘ Table 55.1 shows a list of the survival and pregnancy rates by different groups using donated vitrified oocytes.
In 2008, our group published a study aimed to assess the impact of vitrification using donated oocytes, in terms of survival and development potential when compared to fresh oocytes (Cobo et al. [1, 5]). A cohort of oocytes from a single donor was randomly divided into two groups: in the first one, the oocytes were vitrified, while in the second one, the remaining oocytes were kept in the incubator (control fresh oocytes). Oocytes were warmed up 1 h after vitrification. After two hours, we proceeded to simultaneous insemination of the fresh and vitrified oocytes. The Cryotop method employed for oocyte vitrification was that previously described by Kuwayama (22). The study included 30 donors and 30 recipients (509 oocytes; 231 vitrified oocytes and 219 fresh oocytes). After a survival rate of 96.9%, we found no differences in the rate of division in day 3 (77.6% vs. 84.6% in vitrified in fresh) or the morphological quality of embryos (80.8 vs. 80.5% of good quality embryos vitrified vs. fresh). Likewise, both the blastocyst rate (48.7% vs. 47.5%) and quality of embryos (81.1% vs. 70%) was similar comparing fresh and vitrified.
Another randomized, prospective, triple-blind , controlled-clinical trial, which included the largest sample size published to date, aimed to validate ovum donation via egg-banking [31]. The study included 600 donor/recipients (300 per each branch) and 3039 vitrified versus 3185 fresh oocytes. In this study we demonstrated the non-inferiority of vitrified oocytes regarding ongoing pregnancy rate by intention to treat (Odds ratio = 0.921, 95% CI 0.667 to 1.274). The overall survival rate in this study was 92.5% and ongoing pregnancy rate by intention to treat was 43.7% in the case of patients who received vitrified oocytes compared to 41.7% obtained with fresh oocytes. This study definitively confirmed our previous observations about the non-alteration of vitrified oocytes potential to develop into embryos capable of generating competent ongoing pregnancies in a similar proportion to fresh oocytes.
The availability of surplus embryos to cryopreserve after the embryo transfer in ovum donation cycles conducted with vitrified oocytes is quite common due to the high developmental potential of these oocytes. In these cases, two rounds of vitrification are involved, at MII stage and at day 3 or blastocyst stage. A study published in 2013 showed that the double vitrification has no effect on the delivery rate or live birth rates (Cobo et al. 2013). This study included 796 vitrified embryos generated from vitrified oocytes (N = 471 cycles) and 4394 vitrified embryos generated from fresh oocytes (N = 2629 cycles). The overall embryo survival rate was 97.2% (95% CI 95.9 to 98.6) versus 95.7% (95% CI 94.9 to 96.4) for double versus once vitrified embryos, respectively (NS). The live birth rate per warming cycle was 33.8% versus 30.6% (NS). As showed, the odds ratio of the delivery rate and the double vitrification had no effect on embryos regardless of whether they were in early stage development (day 3) or blastocyst stage (OR = 0.867; 95% CI 0.657 to 1.203).
A couple of years ago, we published an observational study in which our experience of 6 years with the egg-banking program (Cobo et al. [34]) was described. The analysis included 3610 cycles of oocyte donation where 42,152 MII were warmed. Survival rate was 92.6%. The impact of storage time on the survival rate and clinical outcome was calculated by establishing different time intervals from less than 6 months to over 5 years. The storage time did not impair survival or clinical outcomes in any case. We believe that this is a very reassuring information, especially for those women considering fertility preservation. The clinical, ongoing pregnancy, and delivery rates were 55.0%, 45.3%, and 37.6%, respectively, thus confirming the consistency of the results as compared to our previous findings (Cobo et al. [1, 5, 31]). The likelihood of having surplus embryos available for additional cryotransfers was very high in this series due to the mean number of oocytes donated. The possibility of further cryotransfers increased cumulative outcomes, and thus maximized the yield of a single donation cycle, which is precisely what we show herein. The cumulative delivery rate per donation cycle increased to over 70% after three cryotransfers and rose to nearly 80% after five cryotransfers. These results render the donation cycle as highly efficient.
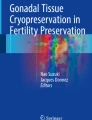
Kaplan-Meier analysis observed in ◘ Fig. 55.1 provides interesting information about the number of vitrified oocytes consumed by a recipient (either in one or more cycles of ovum donation) necessary for a newborn. The analysis showed that the live birth rate increases exponentially and the patient can achieve a baby with a probability of nearly 100% when about three to four cycles of egg donation (around 35–40 oocytes) are completed. This result confirms our previous findings while showing the excellent efficiency of egg-banking.

The Kaplan-Meier curve for the cumulative live birth rates (CLBR) of at least one baby, depending on the total number of oocytes consumed
3.2 Fertility Preservation
Vitrification of oocytes is currently being offered as an option for women who wish to preserve their gametes to allow them to have a chance to conceive in the future and to have their own genetic offspring (Cobo et al. [34]). The main beneficiaries of this strategy are cancer patients who must undergo chemotherapy or radiotherapy and patients with other diseases who require potentially gonadotoxic treatments.
The first reported case in Europe of a pregnancy after FP using vitrification of oocytes was from our group in a patient whose ovarian cortex was cryopreserved first, and after grafting, four stimulation cycles were performed to accumulate and vitrify mature oocytes; a later IVF cycle successfully ended in a twin pregnancy. Since then, various studies have reported clinical outcomes with cryopreserved oocytes for FP in cancer patients (◘ Table 55.2).
Although FP may initially concern cancer patients, there are many other medical conditions that may compromise fertility, such as endometriosis or high risk for early ovarian failure, where an intervention as safeguarding gametes for future use is required to uphold fertility potential. In addition, age-related decline of fertility is a very common condition in assisted reproductive technology (ART) . Elective oocyte vitrification for nonmedical conditions is increasingly accepted as an option to postpone motherhood (Cobo et al. [36]).
We have recently reported, in the largest series to date, our experience in FP in a population of women who electively decided to vitrify their gametes for future use (Cobo et al. [36]).
A clear, and expected, effect of female age was observed in our data. Higher outcomes were achieved in women aged ≤35 years. In this group a larger number of oocytes were retrieved and finally vitrified, and the survival and clinical outcomes were equivalent to those achieved in our egg-banking program for ovum donation, with the highest success rates in the youngest group of women (≤29 years). Otherwise, predictably fewer oocytes and worse outcomes were achieved as the age increased, resembling the results of the infertile population of similar age. There is a clear different probability of having a baby according to the number of oocytes consumed when the ≤35-year-old and >36-year-old groups are compared (P < 0.05) (◘ Fig. 55.2). Obviously, the more oocytes, the higher the probability, but the relationship is not linear, as shown by the curves, and is strongly related to a powerful confounder, i.e., the age of the patient. When we looked at our data, we observed a huge difference in CLBR when using only five oocytes (15.4%) compared with using eight (40.8%), which means an 8.4% increase in CLBR per additional oocyte if women were ≤35 years old. If they were >36 years old using the same number of oocytes, the increase in CLBR was considerably more modest (from CLBR of 5.1% with the use of five oocytes to 19.9% when eight oocytes were consumed, meaning an increase in CLBR of 4.9% per additional oocyte). With 15 oocytes, the CLBR continued to increase in the ≤35-year-old group, whereas with the same number of oocytes the plateau was already reached in the group of women aged >36 years, meaning that at this point the success is independent from the number of oocytes used up. In light of this, we suggest that at least eight to ten MII oocytes should be vitrified to obtain a reasonable success rate.

Kaplan-Meier plotting of the CLBR of at least one baby, depending on the total number of consumed oocytes and categorized by age
3.3 Low-Responder Patients
A potential alternative to the management of low-responder (LR) is to create a large stock of oocytes by accumulating vitrified MII oocytes over several stimulation cycles and inseminating them simultaneously. Theoretically, this could help to increase the chances of success by “converting” poor responders into a “normoresponder-like” status.
We reported, in 2012, a study aimed to assess the efficiency of this new strategy for managing LR that takes advantage of vitrification as a way of creating larger cohorts of oocytes (Cobo et al. [37]). This study included 242 LR patients (594 cycles) whose mature oocytes were accumulated by vitrification and inseminated simultaneously (LR-Accu-Vit) and 482 patients (588 cycles) undergoing IVF/embryo transfer with fresh oocytes in each stimulation cycle (LR-fresh). The embryo-transfer cancellation per patient was significantly lower in the LR-Accu-Vit group (9.1%) than the LR-fresh group (34.0%). This result showed that this strategy is useful to avoid patients abandoning treatment due to negative results that impair their ability to cope with the situation. Live birth rate (LBR)/patient was higher in the LR-Accu-Vit group (30.2%) than the LR-fresh group (22.4%), which confirmed the efficiency of this method for managing LR patients . The positive effects of this strategy are even more evident when cumulative outcome is considered, which endorses the treatment as a successful alternative for LR patients.
Other authors also reported the evaluation of this form of vitrification in the context of standard infertile patients. Rienzi et al. [38] conducted a prospective randomized sibling-oocyte study that included 120 fresh and 124 vitrified sibling oocytes from 40 infertile patients (mean age 35.5 ± 4.8 years). The survival rate was 97%, with a fertilization rate after ICSI of 77% (95/124) per warmed oocyte and 79% (95/120) per warmed/inseminated oocyte. Moreover, the proportions of excellent-quality embryos were the same in each group.
In another study, the cumulative outcome after the transfer of embryos derived from fresh and vitrified oocytes from a single ovarian stimulation cycle was calculated. The study included 182 ICSI cycles in which oocyte vitrification was also performed. The cumulative CPR was calculated when after failing a fresh embryo transfer, the patient underwent a second embryo transfer using embryos derived from the vitrified oocytes. Implantation rates in fresh and vitrification cycles were not significantly different for women ≤34 years (Ubaldi et al. [39]).
All these evidences suggest that vitrified oocytes are functionally similar to fresh oocytes in terms of fertilization, development, and implantation potential.
4 Practical Aspects of Oocyte Vitrification
4.1 Laboratory Procedure
The procedure described below is that developed for Cryotop. However, different methods exist on the market, and it is advisable to follow the manufacturer’s recommendations.
Required Equipment
-
Cryotop (Kitazato Biopharma, Tokyo, Japan)
-
Repro Plate (Kitazato Biopharma, Tokyo, Japan)
-
Cooling rack (styrene box for liquid nitrogen)
-
Liquid nitrogen
-
Storage tank
-
Stereomicroscope, stopwatch or timer, tweezers, Pasteur pipette, micropipettes, and tips
Solutions:
-
1.
Basic solution (BS) is made of Hepes-buffered TCM-199 supplemented with hydroxypropyl cellulose (HPC), only for oocyte vitrification.
-
2.
Equilibration solution (ES) consists of 7.5% ethylene glycol (EG) and 7.5% dimethylsulphoxide (DMSO) dissolved in BS.
-
3.
Vitrification solution (VS) consists of 15% EG, 15% DMSO, and 0.5 M trehalose dissolved in BS.
-
4.
Thawing solution (TS) consists of 1.0 M trehalose dissolved in WS.
-
5.
Dilution solution (DS) consists of 0.5 M trehalose dissolved in WS.
-
6.
Washing solution (WS) is made of Hepes-buffered TCM-199 supplemented with HPC.
4.1.1 Vitrification Procedure
Preparation on the Day
-
1.
Bring BS, ES, and VS to room temperature (24–26 °C) 1 h before application.
-
2.
Fill the cooling rack completely with liquid nitrogen.
-
3.
Write necessary information about the patient on the handle of the vitrification device.
Equilibration Step
-
1.
Aspirate the oocytes from the culture dish and keep them at the tip of the capillar or Pasteur pipette, and transfer them within minimum drop volume to 20 μl of BS into a reproplate well (Kitazato, biomedical supply, Tokyo, Japan).
-
2.
Add 20 μl of ES surrounding the previous drop containing the oocytes (Kitazato, biomedical supply, Tokyo, Japan). Wait for 3 min at room temperature.
-
3.
Add another drop of 20 μl of ES in the same way as in the previous step and wait for 3 min more.
-
4.
Add 240 μl of ES slowly circling the previous drops and wait between 6 and 9 min. At the end of this step, the oocytes should be re-expanded and should recover their original appearance.
Vitrification Step
-
1.
Dispense 300 μl of VS solution into two wells of the reproplate.
-
2.
After equilibrium, aspirate the oocytes at the tip of the pipette. Afterward, place them on the surface of the VS. Try to carry a minimum volume of ES solution. Note that the oocytes will float due to the high density of the VS media.
-
3.
Remove the ES medium just placed together with the oocytes (it will be noted clearly due to the difference in density) and wash the pipette outside the VS well. Keep removing continuously and keep on discarding the medium outside the plate. Repeat this operation as many times as possible within 30 s.
-
4.
Aspirate the oocytes and bring them to the bottom of the plate (the floating will stop as soon as they start to equilibrate with the medium).
-
5.
Repeat the same procedure in the next VS well. Place the oocytes in the bottom of the plate and move them many times around the well, repeating the washing process during 30 more seconds.
-
6.
Aspirate the oocytes and maintain them at the tip of the pipette within minimum volume of VS.
-
7.
Place the Cryotop under the microscope.
-
8.
Proceed to load the oocytes onto the Cryotop within minimum volume.
-
9.
Aspirate excess medium to make sure they are contained within minimum volume.
-
10.
Immerse the Cryotop directly into the liquid nitrogen container.
-
11.
Place the plastic protector Cryotop.
-
12.
Transfer the oocytes to the storage tank.
4.1.2 Warming Procedure
Preparation on the day
-
1.
Warm TS vial and a petri dish up to 37 °C at least 1 h.
-
2.
Bring DS and WS to room temperature (24–26 °C) 1 h before application.
-
3.
Fill the cooling rack completely with liquid nitrogen and retrieve the Cryotop from the storage tank. Keep it submerged in liquid nitrogen.
-
4.
Drop 300 μl DS into first well and 300 μl WS each into second and third well of the repro plate.
Dilution and Warming Step
-
1.
Remove the protective straw maintaining the Cryotops immersed in liquid nitrogen.
-
2.
Remove the Cryotop from the liquid nitrogen container, and submerge it instantly (straight and quick movement) into 4 ml of a solution containing 1.0 M trealose (TS) (Kitazato, medical supply, Tokyo, Japan).
-
3.
Visualize the oocytes and immediately start the countdown to 60 s.
-
4.
Do not manipulate the oocytes within the first 40 s.
-
5.
Retrieve the oocytes from the Cryotop with very gentle manipulations within a minute in TS solution.
-
6.
Transfer the oocytes to the DS well in the reproplate. Aspirate the oocytes very gently, and continue to aspirate TS until the column reaches approximately 2 mm in length.
-
7.
Take the pipette to the DS well and immerse it to the bottom. Dispense the 2 mm column at first. The column of TS within DS will be clear due to the difference in density of both. Leave the oocytes on the “top” of this column. Wait for 3 min.
-
8.
Transfer the oocytes to well WS exactly as in the previous step. Wait for 5 min.
-
9.
Transfer the oocytes to the next well of WS well. Leave the oocytes on the surface of this media; they will drop down immediately due to the absence of differential density between media. Wait for 1 min.
-
10.
Transfer the oocytes to the regular culture dish and place them in the incubator at 37 °C. wait for 2 h before ICSI.
5 Equipment and Facilities
All our samples are cryopreserved by vitrification. This procedure, as currently performed, is entirely manual-operated, making not necessary the use of any equipment to carry out the vitrification process itself. The ease and efficiency of vitrification have been a turning point in the field of cryopreservation, making the whole process no longer than 20 min (vitrification and warming) involving very simple tools. However, the fact that the samples are vitrified mostly contained in very low volumes represents a challenge for further handling, storage, and maintenance of the vitrified samples.
The storage vessel can be the traditional liquid nitrogen tanks or vapor tanks. In our oocyte-bank facilities, we use vapor phase storage tanks (CBS V1500; Custom Biogenic Systems, Michigan, USA), which consist of an outer jacket with liquid N2. This area is responsible for cooling the storage area where the oocytes are maintained in a N2 gas atmosphere. The cold spreads from the vacuum-insulated jacket by convection and through vents in the storage compartment that expel the nitrogen vapor downward to the bottom of the freezer, thus creating a flow of extremely cold air through the entire storage area. The exceptional uniformity of temperature allows the whole storage tank to be used, achieving temperatures below −180 °C at the upper level and −195 °C at the bottom. Samples can be manipulated in safe temperature ranges (−180 °C) thanks to the working area located on top of the storage area, thus avoiding any risk of accidental warming. An additional advantage of this storage system is that the supply of liquid nitrogen can be programmable, although it also can be performed manually. We have demonstrated the effectiveness of this storage vessel as a strategy for preventing the risk of cross-contamination due to direct contact with the liquid nitrogen (LN), showing comparable results between oocytes vapor-stored versus those stored in conventional LN tanks [31].
A temperature monitoring system is strongly advised as a part of the routine quality control (QC) of the cryolab. In our facilities, we use a system that allows continuous monitoring of the temperature of every storage tank in our unit (DataCare, ControlTemp, Barcelona). The system is able to provide numeric and graphic records and to display alarms in real time with updates every second. A record of incidents occurring during the alarm can be also easily assessed differentiating between active alarms or alarms that were active but are no longer in that state. In case of alarm, the system sends alerts and warnings messages to the authorized personnel.
On the other hand, in order to ensure efficiency, only highly skilled professionals who have to overcome a long learning curve should perform vitrification. Therefore, an adequate learning curve is also one of the most important requirements when performing vitrification that requires close attention. Our training program has produced satisfactory results since the introduction of vitrification in our clinical setting. It consists of different phases that gradually increase in difficulty. To pass to the next level, trainees must acquire the necessary skills as well as achieve a preset survival rate.
References
Cobo A, Domingo J, Pérez S, Crespo J, Remohi J, Pellicer A. Vitrification, an effective new approach to oocyte banking in healthy women, could be applied in cancer patients to preserve their fertility. Clin Transl Oncol. 2008;10:268–73.
Homburg R, van der Veen F, Silber SJ. Oocyte vitrification-Women’s emancipation set in stone. Fertil Steril. 2009;91:1319–20.
Boggio A. Italy enacts new law on medically assisted reproduction. Hum Reprod. 2005;20:1153–7.
Borini A, Lagalla C, Bonu MA, Bianchi V, Flamigni C, Coticchio G. Cumulative pregnancy rates resulting from the use of fresh and frozen oocytes: 7 years’ experience. Reprod Biomed Online. 2006;12:481–6.
Cobo A, Bellver J, Domingo J, Pérez S, Crespo J, Pellicer A, Remohi J. New options in ART: the Cryotop method of oocyte vitrification. Case reports Introduction RBM on line. 2008; In press.
Vajta G, Nagy ZP. Are programmable freezers still needed in the embryo laboratory? Review on vitrification. Reprod Biomed Online. 2006;12:779–96.
Woods EJ, Benson JD, Agca Y, Critser JK. Fundamental cryobiology of reproductive cells and tissues. Cryobiology. 2004;48:146–56.
Mazur P. Principles of cryobiology. In: Fuller B, Lane M, Benson E, editors. Life in the frozen state. New York: CRC Press; 2004. p. 4–55.
Watson PF, Morris GJ. Cold shock injury in animal cells. Symp Soc Exp Biol. 1987;41:311–40.
Pickering SJ, Braude PR, Johnson MH, Cant A, Currie J. Transient cooling to room temperature can cause irreversible disruption of the meiotic spindle in the human oocyte. Fertil Steril. 1990;54:102–8.
Ghetler Y, Yavin S, Shalgi R, Arav A. The effect of chilling on membrane lipid phase transition in human oocytes and zygotes. Hum Reprod. 2005;20:3385–9.
Liebermann J, Dietl J, Vanderzwalmen P, Tucker MJ. Recent developments in human oocyte, embryo and blastocyst vitrification: where are we now? Reprod Biomed Online. 2003;7:623–33.
Kuwayama M, Vajta G, Cobo A. Vitrification of oocytes – general considerations and the use of the Cryotop method. Oxon: Informa Healthcare; 2007.
Vajta G, Kuwayama M. Improving cryopreservation systems. Theriogenology. 2006;65:236–44.
Mazur P. Freezing of living cells: mechanisms and implications. Am J Phys. 1984;247:C125–42.
Fuller B, Paynter S. Fundamentals of cryobiology in reproductive medicine. Reprod Biomed Online. 2004;9:680–91.
Arav A. Vitrification of oocyte and embryos. In: Lauria AGF, editor. New trends in embrvo transfer. Cambridge, UK: Portland Press; 1992. p. 255–64.
Lane M, Gardner DK. Vitrification of mouse oocytes using a nylon loop. Mol Reprod Dev. 2001;58:342–7.
Liebermann J, Nawroth F, Isachenko V, Isachenko E, Rahimi G, Tucker MJ. Potential importance of vitrification in reproductive medicine. Biol Reprod. 2002;67:1671–80.
Martino A, Songsasen N, Leibo SP. Development into blastocysts of bovine oocytes cryopreserved by ultra-rapid cooling. Biol Reprod. 1996;54:1059–69.
Matsumoto H, Jiang JY, Tanaka T, Sasada H, Sato E. Vitrification of large quantities of immature bovine oocytes using nylon mesh. Cryobiology. 2001;42:139–44.
Papis K, Shimizu M, Izaike Y. Factors affecting the survivability of bovine oocytes vitrified in droplets. Theriogenology. 2000;54:651–8.
Vajta G, Holm P, Kuwayama M, Booth PJ, Jacobsen H, Greve T, Callesen H. Open pulled straw (OPS) vitrification: a new way to reduce cryoinjuries of bovine ova and embryos. Mol Reprod Dev. 1998;51:53–8.
Kuwayama M, Ieda S, Zhang J, Kato O. The CryoTip method: aseptic vitrification of oocytes and embryos. Fertil Steril. 2005;84(Suppl.1):S187.
Vanderzwalmen P, Zech N, Prapas Y, Panagiotidis Y, Papatheodorou A, Lejeune B, Jareno D, Vanderzwalmen S, Ectors F. Closed carrier device: a reality to vitrify oocytes and embryos in aseptic conditions. Gynecol Obstet Fertil. 2010;38:541–6.
Remohi J, Vidal A, Pellicer A. Oocyte donation in low responders to conventional ovarian stimulation for in vitro fertilization. Fertil Steril. 1993;59:1208–15.
Remohi J, Gartner B, Gallardo E, Yalil S, Simon C, Pellicer A. Pregnancy and birth rates after oocyte donation. Fertil Steril. 1997;67:717–23.
Freour T, Dessolle L, Lammers J, Lattes S, Barriere P. Comparison of embryo morphokinetics after in vitro fertilization-intracytoplasmic sperm injection in smoking and nonsmoking women. Fertil Steril. 2013;99:1944–50.
Remohi J, Gutierrez A, Cano F, Ruiz A, Simon C, Pellicer A. Long oestradiol replacement in an oocyte donation programme. Hum Reprod. 1995;10:1387–91.
Soares SR, Troncoso C, Bosch E, Serra V, Simon C, Remohi J, Pellicer A. Age and uterine receptiveness: predicting the outcome of oocyte donation cycles. J Clin Endocrinol Metab. 2005;90:4399–404.
Cobo A, Romero JL, Perez S, de los Santos MJ, Meseguer M, Remohi J. Storage of human oocytes in the vapor phase of nitrogen. Fertil Steril. 2010;94:1903–7.
Alvarez M, Solé M, Devesa M, Fábregas R, Boada M, Tur R, Coroleu B, Veiga A, Barri PN. Live birth using vitrified--warmed oocytes in invasive ovarian cancer: case report and literature review. Reprod Biomed Online. 2014;28(6):663–8. https://doi.org/10.1016/j.rbmo.2014.02.010. Epub 2014 Mar 4. Review.
Kuleshova L, Gianaroli L, Magli C, Ferraretti A, Trounson A. Birth following vitrification of a small number of human oocytes: case report. Hum Reprod. 1999;14:3077–9.
Cobo A, Castello D, Vallejo B, Albert C, de los Santos JM, Remohi J. Outcome of cryotransfer of embryos developed from vitrified oocytes: double vitrification has no impact on delivery rates. Fertil Steril. 2013;99:1623–30.
Cobo A, Garrido N, Pellicer A, Remohi J. Six years’ experience in ovum donation using vitrified oocytes: report of cumulative outcomes, impact of storage time, and development of a predictive model for oocyte survival rate. Fertil Steril. 2015;104:1426–34.e8.
Cobo A, Garcia-Velasco JA, Coello A, Domingo J, Pellicer A, Remohi J. Oocyte vitrification as an efficient option for elective fertility preservation. Fertil Steril. 2016;105:755–64.e8.
Cobo A, de los Santos MJ, Castellò D, Gámiz P, Campos P, Remohí J. cleavage-stage and blastocyst-stage embryos in a cryopreservation program: evaluation of 3,150 warming cycles. Fertil Steril. 2012;98:1138–46.e1.
Rienzi L, Romano S, Albricci L, Maggiulli R, Capalbo A, Baroni E, et al. Embryo development of fresh ‘versus’ vitrified metaphase II oocytes after ICSI: a prospective randomized sibling-oocyte study. Hum Reprod. 2010;25:66–73.
Ubaldi F, Anniballo R, Romano S, Baroni E, Albricci L, Colamaria S, et al. Cumulative ongoing pregnancy rate achieved with oocyte vitrification and cleavage stage transfer without embryo selection in a standard infertility program. Hum Reprod. 2010;25:1199–205.
Yang D, Brown SE, Nguyen K, Reddy V, Brubaker C, Winslow KL. Live birth after the transfer of human embryos developed from cryopreserved oocytes harvested before cancer treatment. Fertil Steril. 2007;87:1469.e1–4.
Porcu E, Bazzocchi A, Notarangelo L, Paradisi R, Landolfo C, Venturoli S. cryopreservation in infertility and oncology. Curr Opin Endocrinol Diabetes Obes. 2008;15:529–35.
Sanchez-Serrano M, Crespo J, Mirabet V, Cobo AC, Escriba MJ, Simon C, et al. Twins born after transplantation of ovarian cortical tissue and oocyte vitrification. Fertil Steril. 2010;93:268.e11–3.
Kim MK, Lee DR, Han JE, Kim YS, Lee WS, Won HJ, et al. Live birth with vitrified-warmed oocytes of a chronic myeloid leukemia patient nine years after allogenic bone marrow transplantation. J Assist Reprod Genet. 2011;28:1167–70.
García-Velasco JA, Domingo J, Cobo A, Martinez M, Carmona L, Pellicer A. Five years’ experience using oocyte vitrification to preserve fertility for medical and nonmedical indications. Fertil Steril. 2013;99:1994–9.
da Motta EL, Bonavita M, Alegretti JR, Chehin M, Serafini P. Live birth after 6 years of oocyte vitrification in a survivor with breast cancer. J Assist Reprod Genet. 2014;31:1397–400.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Review Questions
Review Questions
-
1.
What are the reasons responsible for the ability of vitrification to rule out chilling injury and the crystallization of the cytoplasm?
-
2.
What role does the cooling and warming rate play in vitrification protocols?
-
3.
Which population can benefit from oocyte vitrification?
-
4.
How can the toxicity of cryoprotectants be reduced in vitrification protocols?
-
5.
What are the main benefits of egg-banking for ovum donation programs?
-
6.
What factors are mainly responsible for success in the elective fertility preservation?
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Cobo, A. (2019). Oocyte Vitrification and Current Clinical Applications. In: Nagy, Z., Varghese, A., Agarwal, A. (eds) In Vitro Fertilization. Springer, Cham. https://doi.org/10.1007/978-3-319-43011-9_55
Download citation
DOI: https://doi.org/10.1007/978-3-319-43011-9_55
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-43010-2
Online ISBN: 978-3-319-43011-9
eBook Packages: MedicineMedicine (R0)