
Abstract
Giant cell arteritis (GCA) is a complex condition in which many loci across the genome may be involved in its susceptibility and phenotypic expression. However, recent large-scale genetic data has shown that the HLA system exerts most of the genetic influence to disease risk, particularly class II genes. This is in contrast with that observed in Takayasu arteritis, the other large vessel vasculitis, in which the HLA association is mainly driven by class I haplotypes. The use of novel imputation methods has made possible an analysis of the HLA system at the amino acid level in GCA. In this context, three polymorphic amino acid positions (positions 13 and 56 of the class II molecules HLA-DRβ1 and HLA-DQα-1, respectively, and position 45 of the class I molecule HLA-B) have been proposed as the causative variants for the HLA association with this type of vasculitis. Although functional experiments may be carried out to confirm these findings, the current data clearly reinforces the idea of GCA as an antigen-driven disease with a major role of T cells.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Human Leukocyte Antigen
- Giant Cell Arteritis
- Human Leukocyte Antigen Class
- Takayasu Arteritis
- Human Leukocyte Antigen Allele
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Giant cell arteritis (GCA) is an immune-mediated vasculitis characterised by inflammatory lesions in medium and large vessels. It shows a complex etiology, in which different factors (including genetic, epigenetic and environmental factors) may interact for its development and clinical manifestations [1]. Cumulated knowledge, based on the study of gene expression profiles and genetic markers of disease susceptibility, indicates that GCA is an antigen-driven condition [2]. In this regard, it has been described that different T cell populations are directly involved in the immunopathological mechanisms leading to GCA, including IFNγ-producing Th1 cells, Th17 cells, Treg cells and Th9 cells [3–6]. Consistent with the above, the main genetic associations with GCA are harbored within the human leukocyte antigen (HLA) region [7], as it occurs in most autoinflammatory and autoimmune diseases, emphasizing the central role of immunity in the pathogenesis of GCA.
The use of high-throughput genotyping platforms has allowed us to have a better perspective of the genetic background underlying GCA predisposition. Thanks to the recent large-scale genetic analysis performed in a well-powered GCA cohort from different populations of European origin [8], we currently know that HLA genes represent a considerably high proportion of the heritability of this type of vasculitis. Therefore, understanding how the HLA system influence GCA development may definitively help us in the challenging endeavour of designing more effective therapeutic strategies for this condition.
In this chapter, we will give an overview of the structure and function of the HLA system and we will summarise the recent findings on its contribution to GCA risk.
2 Structure and Function of HLA Class I and II Molecules
The acronym ‘HLA’ was first established more than six decades ago to list a group of serologically defined antigens, which varied from individual to individual and were associated with organ transplant rejection. Nowadays, we know that the HLA system is a complex genetic region involved in an important mechanism of the immune system aimed to differentiate self-components from potentially harmful non-self agents. Specifically, the HLA genes encode for surface glycoproteins that recognise and present antigens to the immune cells, thus having a major role in the control of the immune response. As this system operates not only in humans but also in most vertebrate species, the term ‘Major Histocompatibility Complex’ (MHC) was proposed to name the system in general. Therefore, the HLA genes are the human versions of the MHC [9].
The HLA region is located at the short arm of chromosome 6 and includes, amongst others, two major sets of genes: the HLA class I genes (HLA-A, -B, and -C) and the HLA class II genes (HLA-DR, -DQ, and -DP). Both classes of HLA genes have different biological functions.
The HLA class I proteins are expressed on the membrane of all nucleated cells in the body, and their main function is to display intracellular peptides to CD8+ T cells. They are composed of three α domains (encoded by the HLA class I genes ) and are linked non-covalently to the β2-microglobulin, which is not polymorphic. In physiological conditions, CD8+ T cells are tuned during thymocyte maturation to the specific set of HLA class I and self proteins produced by the corresponding individual, and will not be activated in response to them in a process known as immune tolerance . However, if a foreign or strange peptide is presented by a HLA class I protein (because of a viral infection, for instance), an immediate immune response will be triggered against the infected cell [10].
On the other hand, HLA class II proteins consist of two homogenous peptides (designated as α and β chains), both of which are encoded by HLA class II genes. Their expression is generally restricted to some cell types known as antigen presenting cells (including dendritic cells, macrophages, and B cells), which do not present cytosolic antigens but those derived from extracellular components to CD4+ helper T cells. This is the mechanism that commonly operates in bacterial infections. In this case, extracellular pathogens are endocytosed, digested in lysosomes, loaded onto the antigen-binding groove of the HLA molecule, and recognised as non-self by CD4+ helper T cells, which, as a consequence, initiate an appropriate immune response consisting of monoclonal expansion, localised inflammation, release of chemoattractant cytokines to recruit phagocytes, and production of specific antibodies against the pathogen [11].
3 The Complexity of the HLA Genomic Region
The HLA region spans around 4-megabase pairs (Mbp) within the chromosome position 6p21.3 and it is characterised by three main features: (1) it contains a high gene density (more than 400 genes and pseudogenes have been annotated, many of them with related immune functions), (2) it shows an extreme sequence variation (more than 8000 alleles have been described for the classical HLA genes), and (3) there is an extensive linkage disequilibrium (LD) in the region [12]. These characteristics are a consequence of a unique evolutionary history that has shaped the genetic structure of this genomic region not only by recombination and gene conversion, but also by natural selection, which makes it difficult to tease apart effects of individual loci in disease association studies [13]. To facilitate this, a systematic nomenclature system based on the early serological studies was developed by the ‘WHO Nomenclature Committee for Factors of the HLA System’ (http://hla.alleles.org/nomenclature/committee.html), which first met in 1968 and laid down the criteria for successive meetings [14]. At first, to define the different serotyped haplotypes (i.e. combinations of specific sets of amino acids of the HLA proteins responsible for transplant rejection), this nomenclature included names composed of the HLA gene that encoded the corresponding protein, followed by two-digit numbers (e.g. HLA-DRB1*01 ). Consequently, these two-digit alleles correlated with the variation of the protein epitopes to which the antibodies were bound. Later on, the use of the polymerase chain reaction (PCR) and DNA sequencing techniques allowed a better estimation of the sequence variation of the HLA genes, and names containing four-digits were established to define haplotypes including non-synonymous changes within exons (e.g. HLA- DRB1*01:01). Although successive digits have been added to improve the accuracy of the defined haplotypes (to consider synonymous changes, for example), it was accepted by consensus that the analysis of 4-digit types, known as classical HLA alleles, is an appropriate approach to obtain a good estimation of the HLA contribution to the studied phenotypes (Fig. 9.1).

Comparison of the amino acid sequence between different HLA-DRB1 classical alleles at two- and four-digit types. The reference sequence corresponds to that of the HLA-DRB1*01 allele. For the HLA-DRB1*01 sequences shown, a hyphen indicates identity to the reference sequence, whereas non-identity to the reference sequence is shown by displaying the appropriate residue at that position. The DNA codons for the two amino acids present in position 13 are also shown, with red bases indicating presence of different alleles of single-nucleotide polymorphisms
However, it is important to note that the classical HLA alleles do not consider all genetic variants and polymorphic amino acid positions within the HLA region, but only specific haplotypes covering each of the HLA genes. As a consequence of the broad LD across many genes, the interpretation of the HLA associations with clinical phenotypes remains difficult. An optimal approach to identify causal variants for those associations would be to analyse the complete sequence data across the HLA region, but this represents a major challenge due to its complex genetic structure. Considering the above, researchers from the Broad Institute (Cambridge, Massachusetts, USA) proposed an alternative methodology consisting of testing single-nucleotide polymorphisms (SNP) and polymorphic amino acid positions individually, instead of the traditional approach of testing the established haplotypes [15]. To do that in a cost-effective manner, and taking advantage of the high-throughput genomics, they developed an imputation method that infers the variation within the HLA region of SNPs, classical HLA alleles, and amino acid polymorphisms at class I and II loci, using a reference panel of 5225 individuals of European origin with genotyping data of 8961 SNPs and indel polymorphisms across the HLA region, as well as four-digit genotyping data of the HLA class I and II molecules [16]. As discussed below, the imputation and association testing at the amino acid level have remarkably facilitated the fine-mapping of primary HLA association signals for many immune-mediated conditions, including GCA.
4 HLA and Human Disease
The HLA region has been associated with a wide spectrum of clinical conditions in humans, more than any other region of the genome, including autoimmune and autoinflammatory diseases, infectious diseases, cancer, graft-versus-host disease, and severe side-effects of drugs [17, 18].
With regards to autoimmunity, typical diseases associated with classical HLA class I alleles include ankylosing spondylitis (HLA-B*27), Behçet’s disease (BD) (HLA-B*51) and Takayasu disease (TAK) (HLA-B*51); whereas some examples of HLA class II diseases are type 1 diabetes (HLA-DRB1*04 and HLA-DRB1*03), rheumatoid arthritis (RA) (HLA-DRB1*04 and HLA-DQA1*03), celiac disease (CeD) (HLA-DQA1*05 and HLA-DQB1*02), multiple sclerosis (HLA-DRB1*15), systemic sclerosis (SSc) (HLA-DRB1*11 and HLA-DRB1*07 ), systemic lupus erythematosus (SLE) (HLA-DRB1*03), ulcerative colitis (HLA-DRB1*11), and GCA (HLA-DRB1*04 ), amongst others [18]. However, the extensive LD of this genomic region, together with the fact that disease predisposition concerns subtle effects of common alleles, has made it difficult to pinpoint causal coding or regulatory variants of those primary associations with conflicting results.
In any case, the novel imputation and fine-mapping approach described in the previous section have shed light into the pathological mechanisms underlying the HLA associations with autoimmune diseases. The first published study using this method was performed in RA in 2012 [19]. The authors proposed a model of three amino acid positions in HLA-DRβ1 (11, 71 and 74), one in HLA-DPβ1 (9), and one in HLA-B (9), that explained almost completely the HLA association with this rheumatic disease. All associated amino acids were located in peptide-binding pockets, implying a functional impact on antigenic peptide presentation to T cells.
Subsequent studies have also analysed the HLA region at the amino acid level in other autoimmune diseases such as SSc, SLE , BD, and GCA [8, 20–22], making a valuable contribution to the current knowledge about the complex HLA associations that account for most of their phenotypic variance.
In the following section we will summarise the recent advances achieved in the study of the HLA contribution to GCA susceptibility.
5 HLA Contribution to GCA Susceptibility
5.1 Early Studies
Despite being limited by a low statistical power, many studies from the early 1990s clearly pointed out the HLA class II as the most relevant genomic region for GCA pathogenesis. Specifically, HLA-DRB1*04 alleles (generally DRB1*0401 but also DRB1*0404) were directly involved in disease predisposition in almost all the independent candidate gene studies conducted in this type of vasculitis, which included populations of European ancestry from USA, Spain, Italy, France, and Denmark [23–30] (Table 9.1). Some studies also reported a correlation between these alleles and both resistance to corticosteroid treatment and the development of visual complications in GCA patients [25, 31, 32].
Regarding HLA class I, some classical alleles were also suggested as GCA risk factors, including HLA-A*31, HLA-B*8, HLA-Cw3 and HLA-Cw6, described in the early 1980s, and the more recent associations with HLA-B*15 and with the MHC class I polypeptide-related sequence A (MICA) gene [33–36]. Nevertheless, the results of those studies were inconsistent in most cases and were not replicated in independent populations [37].
5.2 Novel Associations Using High-Throughput Data
The recently published large-scale genetic screening on GCA has represented a turning point in the elucidation of the HLA contribution to disease pathogenesis [8]. The study was possible thanks to the establishment of an exciting international collaborative effort, in which many research groups and hospitals worldwide, including the ‘European Vasculitis Genetics Consortium’, the ‘Spanish GCA Consortium’, the ‘UKGCA Consortium’ and the ‘Vasculitis Clinical Research Consortium’, contributed with more than 1,600 GCA samples (with a diagnosis confirmed either by temporal artery biopsy or imaging techniques) from seven countries (Spain, Italy, UK, USA, Canada, Germany and Norway). For the analysis, more than 15,000 matched controls were also included, thus representing the largest case–control cohort investigated in a genetic study on GCA so far.
Besides the high statistical power, what made this study of high relevance for the investigation of the HLA system in GCA, was the use of the ‘Human Immuno DNA Analysis BeadChip Kit’ (known as the Immunochip ). This genotyping platform was designed by a consortium of leading groups covering all of the major autoimmune and seronegative diseases to identify immune-related risk variants [38]. The Immunochip includes probes to type almost 200,000 SNPs, rare variants, and insertion/deletion polymorphisms located within 186 known susceptibility loci for autoimmune and inflammatory disorders. The use of the Immunochip has been considerably helpful for the identification of novel specific and common genetic risk factors in multiple immune-mediated diseases, including TAK, CeD, RA and SSc amongst others [21, 39–42]. Remarkably, the chip has a dense coverage of polymorphisms within the HLA region, which can be used to impute classical alleles and amino acid variations with the method described in the third section of this chapter.
The study confirmed class II genes ( HLA-DRB1 and HLA-DQA1) as the main contributors to disease risk. Indeed, the considerably higher statistical significance observed within this region in comparison with the rest of immune genes analysed, suggested that most of the genetic component of GCA relies on HLA class II. This is consistent with the pathogen infection hypothesis proposed to explain the initial activation and expansion of local dendritic cells within the vessel wall of GCA patients [43]. Contrary to that observed in GCA, the strongest susceptibility markers for TAK, the other large vessel vasculitis, are harboured in the HLA class I region (specifically HLA-B*52). The different pattern of HLA associations observed between these two similar conditions is striking, and could reflect disease-specific mechanisms during the early development of both type of vasculitides [44].
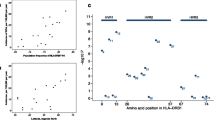
However, the most relevant insight of the Immunochip study on GCA was the analysis of the HLA system at the amino acid level. The authors proposed a model of three amino acid positions that explained most of the differences in the HLA region between cases and controls. This model included the positions 13 and 56 of the HLA class II molecules HLA-DRβ1 and HLA-DQα1, respectively (representing the major contribution), and the position 45 of the HLA class I molecule HLA-B (which conferred a weaker but still significant disease risk) (Fig. 9.2). Remarkably, all three amino acid positions were located in the binding groove of their corresponding molecule, and they have been described to have a direct interaction with the bound antigen, which gives a functional implication to the model.

Amino acid model that best explains the HLA association with giant cell arteritis susceptibility. The location of the associated amino acid positions is represented with a yellow sphere in the ribbon representation of each HLA molecule. P-values, odds ratios (OR) and effect conferred by the different residues at each position are also indicated (Data from Carmona et al. [8])
The amino acid with higher effect size amongst the six possible residues in the position 13 of HLA-DRβ1 was histidine (which was also the top signal in the whole Immunochip study). This is one of the polymorphic amino acids that defines the HLA alleles associated classically with GCA, HLA-DRB1*04:01 and HLA-DRB1*04:04 (Fig. 9.1). Hence, it is likely that the presence of this histidine in the binding pocket of the HLA-DR molecule can predispose antigen-presenting cells to recognise self-antigens within the vascular walls.
It is interesting to note that the histidine in position 13 of HLA-DRβ1 (and, consequently, the HLA-DRB1*04 alleles that contain this residue) is one of the most associated variants with RA susceptibility [19]. In this context, old studies described an association between GCA and HLA-DRB1*04 alleles carrying the ‘shared epitope’ (a common region of the β chain of HLA-DR, comprising positions 67–74, that is commonly present in RA patients and could be involved in presenting auto-immunological peptides) [26, 27]. In addition, PTPN22 (a central regulator of both B and T cell receptor signalling) also represent the strongest non-HLA marker for both diseases [45, 46], and a genetic score predictive for RA was shown to yield significantly higher values in GCA patients compared to controls [8]. Altogether, these evidences may suggest common pathological mechanisms between GCA and RA. However, these two diseases seldom co-occur and they clearly show a different phenotypic expression. It could be speculated that the risk HLA-DRB1 haplotypes (i.e. those including a histidine in position 13) act as major contributors to the loss of tolerance influencing the first stages of both conditions, with other genes acting as secondary ‘modifiers’ of the final phenotype leading to GCA or RA.
6 Future Perspectives
The establishment of an International GCA consortium, involving many groups and hospitals from Europe and North America, has allowed the fulfilment of the first large-scale genetic analysis on GCA, which has produced very exciting insights on the role of the HLA system in this type of vasculitis. However, the main conclusions are based on the assumption that all the effects are conferred on a log-additive scale, that is, the first and second copies of an allele from an associated variant multiplicatively increase risk by the same amount (so homozygosis for an associated allele would double the disease risk of heterozygosis). However, recent lines of evidence suggest that non-additive genetic effects of dominance and epistasis, as a consequence of differences in autoantigen-binding repertoires between a heterozygote’s two expressed HLA variants, may modulate the risk of autoimmune diseases [47]. To continue shedding light into the influence of the HLA system in GCA, this approach should be considered, as it could explain moderate fractions of the phenotypic variance.
On the other hand, the ongoing collaboration of the GCA consortium will increase the current case–control cohort, and additional subphenotype analyses of the HLA system accordingly with the main clinical complications of the disease could be performed. These studies may have relevant therapeutic implications, as it could be possible that different HLA haplotypes are related with higher risk to develop severe complications like visual loss or with relapses after corticosteroid tapering [43].
7 Conclusion
Thanks to the advent of the new technologies for high-throughput genotyping, we have now a clearer overview of the genetic basis predisposing to complex traits such as the autoimmune diseases. Platforms like the GWAS or the Immunochip have helped us to make an accurate estimation of the contribution of the HLA system to the development of autoimmunity. We now know that the HLA region explains more disease risk than any other locus in the genome in most immune-mediated disorders. Elucidation of the functional implications of the autoimmune disease-associated HLA alleles is essential for a better understanding of the pathophysiology of these conditions, and may ultimately lead to more effective treatments. Regarding GCA, a comprehensive analysis of the HLA system has been possible taking advantage of the dense SNP coverage of the Immunochip for this genomic region and the use of novel imputation methods. The data indicated that certain amino acids located in the binding groove of the HLA-DR and HLA-DQ molecules confer the strongest risk for GCA development, with a weaker contribution of class I residues. These data support the hypothesis that GCA is an antigen-driven disease likely triggered by a pathogen infection.
References
Ly KH, Regent A, Tamby MC, Mouthon L (2010) Pathogenesis of giant cell arteritis: more than just an inflammatory condition? Autoimmun Rev 9:635–645
Weyand CM, Goronzy JJ (2013) Immune mechanisms in medium and large-vessel vasculitis. Nat Rev Rheumatol 9:731–740
Terrier B, Geri G, Chaara W, Allenbach Y, Rosenzwajg M, Costedoat-Chalumeau N et al (2012) Interleukin-21 modulates Th1 and Th17 responses in giant cell arteritis. Arthritis Rheum 64:2001–2011
Espigol-Frigole G, Corbera-Bellalta M, Planas-Rigol E, Lozano E, Segarra M, Garcia-Martinez A et al (2013) Increased IL-17A expression in temporal artery lesions is a predictor of sustained response to glucocorticoid treatment in patients with giant-cell arteritis. Ann Rheum Dis 72:1481–1487
Samson M, Audia S, Fraszczak J, Trad M, Ornetti P, Lakomy D et al (2012) Th1 and Th17 lymphocytes expressing CD161 are implicated in giant cell arteritis and polymyalgia rheumatica pathogenesis. Arthritis Rheum 64:3788–3798
Ciccia F, Rizzo A, Guggino G, Cavazza A, Alessandro R, Maugeri R et al (2015) Difference in the expression of IL-9 and IL-17 correlates with different histological pattern of vascular wall injury in giant cell arteritis. Rheumatology (Oxford) 54:1596–1604
Carmona FD, Gonzalez-Gay MA, Martin J (2014) Genetic component of giant cell arteritis. Rheumatology (Oxford) 53:6–18
Carmona FD, Mackie SL, Martin JE, Taylor JC, Vaglio A, Eyre S et al (2015) A large-scale genetic analysis reveals a strong contribution of the HLA class II region to giant cell arteritis susceptibility. Am J Hum Genet 96:565–580
Bodmer WF (1987) The HLA, system: structure and function. J Clin Pathol 40:948–958
Hewitt EW (2003) The MHC, class I antigen presentation pathway: strategies for viral immune evasion. Immunology 110:163–169
Cresswell P (1994) Assembly, transport, and function of MHC class II molecules. Annu Rev Immunol 12:259–293
Horton R, Wilming L, Rand V, Lovering RC, Bruford EA, Khodiyar VK et al (2004) Gene map of the extended human MHC. Nat Rev Genet 12:889–899
Traherne JA (2008) Human MHC, architecture and evolution: implications for disease association studies. Int J Immunogenet 35:179–192
Marsh SG, Albert ED, Bodmer WF, Bontrop RE, Dupont B, Erlich HA et al (2010) Nomenclature for factors of the HLA system, 2010. Tissue Antigens 75:291–455
de Bakker PI, Raychaudhuri S (2012) Interrogating the major histocompatibility complex with high-throughput genomics. Hum Mol Genet 21:R29–R36
Jia X, Han B, Onengut-Gumuscu S, Chen WM, Concannon PJ, Rich SS et al (2013) Imputing amino acid polymorphisms in human leukocyte antigens. PLoS One 8, e64683
Petersdorf EW (2013) The major histocompatibility complex: a model for understanding graft-versus-host disease. Blood 122:1863–1872
Trowsdale J, Knight JC (2013) Major histocompatibility complex genomics and human disease. Annu Rev Genomics Hum Genet 14:301–323
Raychaudhuri S, Sandor C, Stahl EA, Freudenberg J, Lee HS, Jia X et al (2012) Five amino acids in three HLA proteins explain most of the association between MHC and seropositive rheumatoid arthritis. Nat Genet 44:291–296
Kim K, Bang SY, Lee HS, Okada Y, Han B, Saw WY et al (2014) The HLA-DRbeta1 amino acid positions 11-13-26 explain the majority of SLE-MHC associations. Nat Commun 5:5902
Mayes MD, Bossini-Castillo L, Gorlova O, Martin JE, Zhou X, Chen WV et al (2014) Immunochip analysis identifies multiple susceptibility loci for systemic sclerosis. Am J Hum Genet 94:47–61
Ombrello MJ, Kirino Y, de Bakker PI, Gul A, Kastner DL, Remmers EF (2014) Behcet disease-associated MHC class I residues implicate antigen binding and regulation of cell-mediated cytotoxicity. Proc Natl Acad Sci U S A 111:8867–8872
Gonzalez-Gay MA, Amoli MM, Garcia-Porrua C, Ollier WE (2003) Genetic markers of disease susceptibility and severity in giant cell arteritis and polymyalgia rheumatica. Semin Arthritis Rheum 33:38–48
Rauzy O, Fort M, Nourhashemi F, Alric L, Juchet H, Ecoiffier M et al (1998) Relation between HLA DRB1 alleles and corticosteroid resistance in giant cell arteritis. Ann Rheum Dis 57:380–382
Gonzalez-Gay MA, Garcia-Porrua C, Llorca J, Hajeer AH, Branas F, Dababneh A et al (2000) Visual manifestations of giant cell arteritis. Trends and clinical spectrum in 161 patients. Medicine 79:283–292
Weyand CM, Hunder NN, Hicok KC, Hunder GG, Goronzy JJ (1994) HLA-DRB1 alleles in polymyalgia rheumatica, giant cell arteritis, and rheumatoid arthritis. Arthritis Rheum 37:514–520
Dababneh A, Gonzalez-Gay MA, Garcia-Porrua C, Hajeer A, Thomson W, Ollier W (1998) Giant cell arteritis and polymyalgia rheumatica can be differentiated by distinct patterns of HLA class II association. J Rheumatol 25:2140–2145
Cid MC, Ercilla G, Vilaseca J, Sanmarti R, Villalta J, Ingelmo M et al (1988) Polymyalgia rheumatica: a syndrome associated with HLA-DR4 antigen. Arthritis Rheum 31:678–682
Weyand CM, Hicok KC, Hunder GG, Goronzy JJ (1992) The HLA-DRB1 locus as a genetic component in giant cell arteritis. Mapping of a disease-linked sequence motif to the antigen binding site of the HLA-DR molecule. J Clin Invest 90:2355–2361
Combe B, Sany J, Le Quellec A, Clot J, Eliaou JF (1998) Distribution of HLA-DRB1 alleles of patients with polymyalgia rheumatica and giant cell arteritis in a Mediterranean population. J Rheumatol 25:94–98
Martinez-Taboda VM, Bartolome MJ, Lopez-Hoyos M, Blanco R, Mata C, Calvo J et al (2004) HLA-DRB1 allele distribution in polymyalgia rheumatica and giant cell arteritis: influence on clinical subgroups and prognosis. Semin Arthritis Rheum 34:454–464
Salvarani C, Boiardi L, Mantovani V, Ranzi A, Cantini F, Olivieri I et al (1999) HLA-DRB1, DQA1, and DQB1 alleles associated with giant cell arteritis in northern Italy. J Rheumatol 26:2395–2399
Armstrong RD, Behn A, Myles A, Panayi GS, Welsh KI (1983) Histocompatibility antigens in polymyalgia rheumatica and giant cell arteritis. J Rheumatol 10:659–661
Hansen JA, Healey LA, Wilske KR (1985) Association between giant cell (temporal) arteritis and HLA-Cw3. Hum Immunol 13:193–198
Kemp A, Marner K, Nissen SH, Heyn J, Kissmeyer-Nielsen F (1980) HLA antigens in cases of giant cell arteritis. Acta Ophthalmol 58:1000–1004
Gonzalez-Gay MA, Rueda B, Vilchez JR, Lopez-Nevot MA, Robledo G, Ruiz MP et al (2007) Contribution of MHC class I region to genetic susceptibility for giant cell arteritis. Rheumatology (Oxford) 46:431–434
Richardson JE, Gladman DD, Fam A, Keystone EC (1987) HLA-DR4 in giant cell arteritis: association with polymyalgia rheumatica syndrome. Arthritis Rheum 30:1293–1297
Cortes A, Brown MA (2011) Promise and pitfalls of the Immunochip. Arthritis Res Ther 13:101
Saruhan-Direskeneli G, Hughes T, Aksu K, Keser G, Coit P, Aydin SZ et al (2013) Identification of multiple genetic susceptibility loci in Takayasu arteritis. Am J Hum Genet 93:298–305
Trynka G, Hunt KA, Bockett NA, Romanos J, Mistry V, Szperl A et al (2011) Dense genotyping identifies and localizes multiple common and rare variant association signals in celiac disease. Nat Genet 43:1193–1201
Eyre S, Bowes J, Diogo D, Lee A, Barton A, Martin P et al (2012) High-density genetic mapping identifies new susceptibility loci for rheumatoid arthritis. Nat Genet 44:1336–1340
Parkes M, Cortes A, van Heel DA, Brown MA (2013) Genetic insights into common pathways and complex relationships among immune-mediated diseases. Nat Rev Genet 14:661–673
Carmona FD, Martin J, Gonzalez-Gay MA (2015) New insights into the pathogenesis of giant cell arteritis and hopes for the clinic. Expert Rev Clin Immunol 12:57–66
Carmona FD, Gonzalez-Gay MA, Martin J (2015) Genetic analysis of large vessel vasculitis. Nephron 129:3–5
Begovich AB, Carlton VE, Honigberg LA, Schrodi SJ, Chokkalingam AP, Alexander HC et al (2004) A missense single-nucleotide polymorphism in a gene encoding a protein tyrosine phosphatase (PTPN22) is associated with rheumatoid arthritis. Am J Hum Genet 75:330–337
Serrano A, Marquez A, Mackie SL, Carmona FD, Solans R, Miranda-Filloy JA et al (2013) Identification of the PTPN22 functional variant R620W as susceptibility genetic factor for giant cell arteritis. Ann Rheum Dis 72:1882–1886
Lenz TL, Deutsch AJ, Han B, Hu X, Okada Y, Eyre S et al (2015) Widespread non-additive and interaction effects within HLA loci modulate the risk of autoimmune diseases. Nat Genet 47:1085–1090
Jacobsen S, Baslund B, Madsen HO, Tvede N, Svejgaard A, Garred P (2002) Mannose-binding lectin variant alleles and HLA-DR4 alleles are associated with giant cell arteritis. J Rheumatol 29:2148–2153
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Carmona, F.D., Martín, J. (2016). HLA System and Giant Cell Arteritis. In: Dammacco, F., Ribatti, D., Vacca, A. (eds) Systemic Vasculitides: Current Status and Perspectives. Springer, Cham. https://doi.org/10.1007/978-3-319-40136-2_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-40136-2_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-40134-8
Online ISBN: 978-3-319-40136-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)