
Abstract
Parkinson’s disease is a progressive disorder caused by degeneration of the dopaminergic neurons of the substantia nigra. Years before the substantia nigra compacta (SNc) and cortex are involved, there is pathological evidence of PD in the medulla oblongata, pontine tegmentum and olfactory bulb. The motor problems can be preceded by several years by subtle clinical symptoms such as rapid eye movement sleep behaviour and hyposmia during the prodromal period of PD. The striatonigral pathway plays a regulatory role in the system of positive and negative pathways that serve to modulate feedback from the thalamus to the motor cortex. This chapter reviews PD with emphasis on the age of onset. Parkinson’s disease usually begins in middle to late life (LOPD). In about 5–10%, PD begins before the age of 50 (EOPD). There are some distinguishing features between both.
Access provided by CONRICYT-eBooks. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Parkinson’s disease
- Glucocerebrosidase (GBA) gene mutations
- Late-onset Pompe disease (LOPD)
- Early-onset Pompe disease (EOPD)
- Lewy bodies
- Striatonigral pathway
- Secondary parkinsonism
Introduction
Parkinson’s disease is considered a movement disorder [1, 2]. In idiopathic Parkinson’s disease , there is accumulation of alpha-synuclein in neuronal perikarya (Lewy bodies) and neuronal processes (Lewy neuritis) [3]. The majority of PD cases are sporadic, and about 10% are the rare familial forms, gene-linked encoding alpha-synuclein, parkin, dJ-1, PINK-1 and LRRK2 [4]. Glucocerebrosidase (GBA) gene mutations are now recognised as numerically the most important risk factor for PD [5]. Early-onset PD with slower progression than the idiopathic disorder is produced by mutations in parkinsonism and results in loss of midbrain dopamine neurones [6].
In PD alpha-synuclein misfolds and forms intracellular inclusions called Lewy bodies which are the pathological hallmark of PD [7]. Several genes may be involved [8], and misfolding of proteins and dysfunction of the ubiquitin-proteasome pathway play an important role in PD pathogenesis [9]. Accumulation of alpha-synuclein may be related to synaptic dysfunction in PD [10] and is brought about by either environmental or genetic factors [11] triggered by a chain of events resulting in dopaminergic neuronal death and dopamine depletion in the striatum which is the hallmark of PD [12]. Parkinsonian symptoms are believed to be due to abnormal synchronous oscillating activity within the basal ganglia [12] and play a vital role in the generation of the disease [13]. Loss of dopaminergic neurones in the midbrain [14] is commonly associated with dysfunction of the basal ganglia. Loss of dopaminergic inputs to the basal ganglia, that is, subthalamic nuclei and globus pallidus, results in increased oscillatory firing and synchronisation [15].
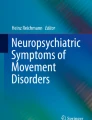
Increased knowledge and better understanding of the organisation of the basal ganglia in both health and disease have led to the hypothesis of direct and indirect pathways of the flow through the basal ganglia of cortical information [16] (Fig. 1). The internal basal ganglia circuits are controlled by several pre- and postsynaptic mechanism [1].

Schematic diagram of direct and indirect pathways of the basal ganglia motor circuits. Direct pathway (blue) (D1). Projections from the caudate/putamen, GPi, thalamus to premotor cortex. Excitatory inputs from the substantia nigra and cortex to the putamen/caudate are also shown. Indirect pathway (red) (D2). Projections from the caudate/putamen, GPe, subthalamic nucleus, GPi, thalamus to motor cortex. GPe also receives excitatory input from the cortex and inhibitory from the substantia nigra. There is an excitatory input from the subthalamic nucleus to the GPi
Clinical Manifestations
According to Braak et al. [8] long before the substantia nigra compacta (SNc) and cortex are involved even over years, there is pathological evidence of PD as defined by the presence of Lewy bodies in the medulla oblongata, pontine tegmentum and olfactory bulb. The onset motor problems can be preceded by several years by subtle clinical symptoms such as rapid eye movement sleep behaviour and hyposmia during the prodromal period of PD [17]. Parkinson’s disease usually begins in middle to late life (LOPD). In about 5–10%, PD begins before the age of 50 (EOPD). There are some distinguishing features between both (Table 1). LOPD exhibited more often tremor at the beginning [18], and tremor is only present in half the number of patients with early onset. Rigidity and akinesia are more prominent with EOPD with rapid establishment of full-blown clinical picture and deterioration of the therapeutic efficacy of L-dopa [19]. The response to levodopa was greater and duration shorter in EOPD patients, and posture and gait symptomatology were less responsive in older patients [20]. Although the response to levodopa is significant, side effects are seen early [19], and this group has a greater proclivity to levodopa-induced dyskinesias and fluctuations as early as 6 months. LOPD patients are more susceptible to psychiatric complications [21]. The progression of the disease is slower with EOPD patients, but it is related more to the age of the patient rather than to the age of disease onset [22].
The early stages of PD may often be characterised by non-specific symptoms such as depression and fatigue, aching and tightness in the leg and arm, clumsiness of the hand, subtle decrease in mobility with less arm swing and flexed posture with difficulty in swallowing. The tremor may be intermittent. There is little difficulty in recognising idiopathic Parkinson’s disease when it is well established. The combination of tremor, rigidity, bradykinesia and gait disorder is the classic syndrome of the idiopathic Parkinson’s disease. This syndrome is not seen in any other neurological disorder. The difficulty may arise in some cases in differentiating it in the early stages of the disease, or when it presents with rigidity and bradykinesia, from other movement disorders. The tremor is present at rest, decreases with movement and disappears during sleep. It may involve the hand, jaw and feet. The rhythmic pronation and supination of the arm characteristically cause the ‘pill-rolling’ of the opposed thumb and fingers. The rigidity affects all muscles most markedly the trunk and neck. A cogwheel effect is often noted on passive movement of the extremities due to the combination of tremor and rigidity. There is slowness (bradykinesia) in the carrying out of voluntary movements. Flexion of the neck and trunk and the arms produces the distinctive posture with postural instability and falls. Posture and gait disorders are the least distinguishing of the presenting features. The ‘mask-like’ face is very obvious to the trained observer. The speech is dysarthric (monotonous, slow and low volume). The hand writing is micrographic, and there is drooling of saliva.
Differential Diagnosis
There are few conditions that may be confused with Parkinson’s disease. Benign essential tremor is commonly mistaken for PD. Although the tremor is postural, this may be the initial and only sign of early PD causing difficulties in diagnosis. The patient with essential tremor would have had it for several years, and there is often a family history. The tremor worsens with skilled acts and there is often a head tremor and there is no rest tremor, rigidity or bradykinesia.
The clinical presentation of drug-induced parkinsonism is exactly the same as classic PD and clinically indistinguishable. The common drugs which are culpable are the older antipsychotics, for example, haloperidol and antiemetics such as prochlorperazine and metachlorpropamide. A careful history must be taken in patients who present with Parkinson’s. A few neurodegenerative disorders like progressive supranuclear palsy, nigrostriatal degeneration, MSA-P syndrome and other conditions like normal pressure hydrocephalus and multiple cerebral infarctions may mimic PD. Box 1 shows the clinical features differentiating them from PD.
Box 1 Clinical Features of Parkinson-Plus Syndromes
Absence of typical tremor
Early onset and predominance of unsteady gait and postural defect and falls
Atypical rigidity and dystonic features
Early onset of dementia
Abnormal deep tendon reflexes and plantar responses
Early onset of bladder dysfunction
Impaired extraocular movements
Very poor response to anti-parkinsonian treatment
Rapid progression of disability
Early occurrence of postural hypotension even prior to treatment
Progressive supranuclear palsy is a progressive disease with stiffness, unsteady gait, falls and visual complaints. Vertical downward gaze is lost and axial more than appendicular rigidity, dysarthria and slow mentation (subcortical dementia) with poor response to levodopa. In nigrostriatal degeneration, there are bradykinesia, unsteady gait, dysarthria, orthostatic hypotension and rigidity. Mentation is intact and response to treatment is poor. Dyspraxic gait, incontinence and dementia are the classical triad of normal pressure hydrocephalus. The gait is short and shuffling or ‘magnetic’ (like walking in mud). With multiple cerebral infarctions, there are increased muscle tone, some degree of bradykinesia and gait disorder, and the diagnosis is based on the presence of focal cerebral dysfunction. The clinical features of Parkinson-plus syndromes differ from that of idiopathic Parkinson’s disease as in Table 2.
Management of Parkinson’s Disease
Most people with early PD are treated by the primary care physician, and it is important that the primary care physician should have an understanding of what happens in Parkinson’s disease. However, initially to confirm the diagnosis and later with increasing severity and complications, referral to a neurologist and co-management is necessary.
The decision to initiate treatment depends on several factors, for instance, age of the patient at the onset of the disease, degree of disability, patients’ expectations and social and occupational demands, and hence treatment must be individualised. Evaluation of the patient can be quantitative or qualitative. The former is often time-consuming, but the latter is relatively simple and rapid. There are a number of clinical rating scales available, but the one widely used is the Unified Parkinson’s Disease Rating Scale (UPDRS) which assesses 42 items on a four-point score system to determine the patient’s mental status, activities of daily living, motor function and complications of therapy [28].
Levodopa is still considered the most effective drug for the treatment of Parkinson’s disease even though long-term therapy is associated with motor complications that can be as disabling as the disease itself. Patients encounter symptoms of severe involuntary movements and the ‘switching-off’ phenomenon possibly due to abnormal pulsatile delivery of the dopamine. Levodopa-induced dyskinesia may be reduced with non-selective N-methyl-D-aspartate antagonist amantadine and fipamezole (noradrenergic alpha2A antagonism) can potentially reduce dyskinesia.
To improve motor outcomes, dopamine agonists (pramipexole, ropinirole, rotigotine), monoamine oxidase B inhibitors (rasagiline) and catechol-O-methyltransferase inhibitors (entacapone) can provide continuous oral delivery of dopaminergic stimulation [29]. The dopamine agonists are longer acting, may be neuroprotective and slow the progression of the disease [30, 31]. Dopamine agonists are less likely to produce long-term motor complications but are not as effective as L-dopa. They can be used before going on to L-dopa, except in those aged over 70 years with significant disability. Neither bromocriptine nor pergolide is used anymore because they are ergot alkaloids and have significant side effects. The most important of these are mediastinal and cardiac (valvular) fibrosis. Cabergoline, another ergot dopamine agonist, also causes fibrotic reaction in the cardiac valves. It is used as a monotherapy in PD in the early phase. It could be used in combination with L-dopa and decarboxylase such as carbidopa in progressive phase of PD. Patients on cabergoline should be screened regularly with X-ray of chest, electrocardiogram and renal function tests.
Another class of medications helpful in treating PD are the non-ergot dopamine agonists, oral ropinirole, Requip, pramipexole, Mirapex, and the rotigotine transdermal patch. They act like levodopa and are useful in the early stages of the disease and an option for an initial treatment for younger patients with mild to moderate symptoms [32, 33]. These can be used in combination with levodopa and may reduce the amount of ‘off time’ when patients have difficulty with motor activity. Both however have been linked with new onset of compulsive behaviours such as gambling and hypersexuality. Rotigotine, a non-ergot dopamine agonist, delivers a more regular dopamine stimulation through a transdermal patch, releasing approximately 2 mg per 24 h. It is indicated as monotherapy or in combination with existing levodopa therapy in patients with early to advanced disease.
Rasagiline is the newer drug and is preferred by many to selegiline. It has been extensively used in Europe. There are reports that rasagiline slows progression of the disease and improves control of motor fluctuations in advanced disease and in the treatment of motor symptoms. It may be useful in early PD and is a potent selective irreversible MAO-type B inhibitor. It impairs thinking and reactions and can produce unexpected drowsiness, and motor vehicle accidents have occurred as a result. Certain foods and beverages that are high in tyramine should be avoided.
The anticholinergics are most effective in those with significant tremor, but their side effects limit their use especially in the elderly. Muscarine M4 cholinergic antagonists are useful in the treatment of PD tremor, but tolerability is often poor [34]. Other options include clozapine, antidepressant mirtazapine and 5-HT2A [34]. The COMT inhibitors decrease the degradation of levodopa thereby reducing the end-of-dose wearing-off effect. However, it has been associated with fatal hepatotoxicity and requires close monitoring with liver function tests. Entacapone (COMT-I) in combination with L-dopa preparations (Stalevo) smooths the delivery of dopamine to the brain thus reducing the amount of time spent ‘switched off’. Potential side effects include nausea, dizziness, diarrhoea and involuntary movements. Some patients especially those with early onset show earlier and more often severe motor fluctuations and dyskinesias. In these patients, surgery or alternate routes of administration of dopaminergic medications have been shown to reduce the motor fluctuations. Apomorphine is an injectable form of dopamine agonist and has been shown to reduce daily off time of about 50% and maintained for long-term benefit [35]. In advanced Parkinson’s disease, more stable plasma levels can be achieved by DUODOPA which is a combination of levodopa and carbidopa in the form of a gel and is administered by a portable pump directly into the duodenum through a tube inserted in a percutaneous endoscopic gastrostomy (PEG). The commonly used drugs are shown in Table 3.
Co-enzyme Q-10 is being used “off-label” as a neuroprotective agent to slow progression. It is an antioxidant sold as a dietary supplement and is also involved in mitochondrial processes. Over recent years, there has been a renewed interest in surgery, and this has largely been due to the limitations of medication. Chronic levodopa-associated motor fluctuations and dyskinesias, the variable response to tremors and advances in stereotactic surgery are some of the reasons for this shift.
In moderate to severe PD patients, where drug treatment was ineffective, and in those with certain drug reactions, Wu et al. [40] have listed the following options, namely, (1) striatum stereotactic pallidotomy, (2) stereotactic technique of deep brain stimulation, (3) stem cell implantation via brain stereotactic surgery, (4) subarachnoid stem cell implantation via lumbar puncture and (5) gene-targeted stem cell implantation in subarachnoid via lumber puncture. Surgery in PD is carried out on structures that are responsible for the modification of movements, e.g. globus pallidus, thalamus and subthalamic nucleus. Currently the more important surgical techniques are lesioning (pallidotomy, thalamotomy) and chronic deep brain stimulation (DBS) especially of the subthalamic nucleus [29]. There is considerable reduction in the symptoms, and the patients are able to reduce their medications.
Pallidotomy has been replaced largely by thalamotomy. Thalamotomy is believed to relieve tremor more consistently than pallidotomy with lower rate of symptom recurrence and found to be effective in relieving rigidity and drug-induced dyskinesias. It is usually performed in patients under 65 years with normal memory and intellectual functions. Thalamotomy is rarely done today and largely replaced by deep brain stimulation. Deep brain stimulation (DBS) is considered the surgical treatment of choice for PD and is effective in the right situation. There is less destruction of brain tissues than other surgical methods which is effective and safe. Stimulation of the ventral pallidum relieves rigidity, and the ventrolateral nucleus of the thalamus abolishes tremor. Stimulation of the STN and GP may reduce tremor, on-off motor fluctuations and abnormal movements (dyskinesias) induced by long-term use of levodopa. The Algorithm 1 addresses the problem of management of idiopathic Parkinson’s disease.

Addresses the Problem of Management of Idiopathic Parkinson’s Disease. *Unpredictable abrupt fluctuation in motor state between undertreated and overtreated states, **Shorter duration of benefit after L-dopa, ##After several years of levodopa therapy, ***Beginning of dose deterioration, !DBS = deep brain stimulation, #Drug and disease related, ###Globus pallidus internal-segment pallidotomy, deep brain stimulation and nigral transplantation hold promise for the future
The motor symptoms of PD are well recognised, but the non-motor symptoms have been neglected for years. There is now an increase in awareness that they are equally important in the effectual management of the patient with PD. These symptoms may sometimes be present before the diagnosis of PD but inevitably emerge as the disease progresses [41]. They are quite disabling and contribute to reduced quality of life, increase in caregiver burden and institutionalisation and shorten life expectancy [41].
Depression is the most commonly occurring non-motor symptom in PD and manifests somewhat differently from the depression in otherwise healthy people. According to Braak et al. [42], several areas outside of substantia are involved. The PD group has been reported to have less pleasure, less sadness, less guilt and less energy [43]. Other non-motor symptoms include cognitive disturbances, disorders of sleep, psychiatric symptoms, such as hallucinations, and autonomic disturbances. Even in early stages of the disease, several neuropsychological deficits such as defective use of memory stores, impaired behavioural regulation and planning tasks have been recognised [44]. Dementia is a late development in PD. Some of the non-motor symptoms such as sleep problems, genitourinary symptoms, pain, constipation and diarrhoea can be improved with available treatment [41] (Boxes 2, 3 and 4).
Box 2: Nonmotor Symptoms of PD
Psychiatric
Mood disorders-depression
Anxiety/panic attacks
Hallucinations, paranoia
Impulse control disorders
Apathy
Cognitive disturbances
Slowing of voluntary and involuntary response
Dementia
Sleep disorders
REM sleep disorder
Daytime somnolence
Sensory impairment
Autonomic disturbances
Erectile dysfunction
Constipation
Gastric dysmobility
Information sources: Chadhuri et al. [41]; Postuma et al. [45]; Simuni T, Sethi [46]; Truong et al. [47].
Box 3 Key Points: Clinical Expression of Parkinson’s Disease
PD usually begins in middle to late life (late onset), and in 5–10%, it begins before the age of 50 years.
The early stages of PD is characterised by non-specific symptoms.
In about 5–10%, PD begins before the age of 50 (EOPD). There are some distinguishing features between both.
The combination of tremor, rigidity, bradykinesia and gait disorder is the classic syndrome of idiopathic PD.
The difficulty in diagnosis may arise in some cases in the early stages or when it presents with rigidity and bradykinesia from other movement disorders.
The non-motor symptoms in PD are equally important.
The decision to treat depends on several factors, for instance, age of the patient at time of onset, degree of disability, patients expectations and social and occupational demands.
Box 4 Key Points: Treatment of Parkinson’s Disease
L-Dopa is the most effective drug, but patients may encounter severe involuntary movements and the ‘switching off’. Dopamine agonists less likely to give rise to side effects but are less effective. Neither bromocriptine nor pergolide is used now because they are ergot alkaloids.
Another class of non-ergot dopamine agonists is ropinirole and pramipexole. Both have a new set of side effects: compulsive behaviours, gambling and hypersexuality.
In recent years, there is a renewed interest in surgery-surgical techniques – lesioning (thalamotomy and pallidotomy) and deep brain stimulation (DBS). Stimulation of the ventral pallidum relieves rigidity, and the ventrolateral nucleus of the thalamus abolishes tremor.
Impact
As the disease progresses, patients with PD experience worsening of their physical manifestations such as developing swallowing difficulties, walking difficulties and difficulty in communication, becoming cognitively impaired and developing behavioural problems and autonomic problems such as sexual dysfunction and lightheadedness, amongst others [48]. PD continues to be an unrelenting progressive disorder resulting in severe disability despite progress in newer pharmacological treatments [29]. PD can affect many aspects of the person’s daily life and negatively affect their social interactions. They develop psychosocial issues which affect their QoL. It adversely affects motor functioning resulting in disability and impact on QoL [49]. In a study of 95 patients with PD with regard to the impact of the disease on functional condition, the researchers found that impairment occurred in three categories, ‘walk’, ‘social interaction’ and clarity of mind’, and the highest percent was in ‘motor control’ and least in ‘emotional stability’ [49]. PD can affect severely the health-related quality of life (HR-QoL) [50] in both patients and carers [49] as the disease progresses. Patients with early-onset and late-onset PD have different clinical profile and hence have different impact on their lives. There is a higher prevalence of mood disorder and anxiety in individuals with Parkinson’s disease which play an important role to worsen quality of life in both groups [27]. Patients with PD have a high likelihood of increasing dependency, premature ageing and reduced occupational performance [27]. PD markedly reduces HR-QoL of patients and caregivers and places a tremendous economic burden on society. The economic costs include direct health-care costs and indirect costs (lost worker productivity) [51], and the economic costs of PD are high particularly for patients in the advanced stages and with motor complications [52].
Multiple Choice Questions
-
1.
The following in Parkinson’s disease are true, except:
-
A.
Degeneration of the dopaminergic cells in the substantia nigra results in the dysfunction of the striatonigral-thalamic outflow.
-
B.
Dopamine is not bound to the postsynaptic receptors and inactivated by binding to the autoreceptors and is also inactivated by enzymes monoamine oxidase type B (MAO-B) and catechol-O-methyltransferase (COMT).
-
C.
The intraneuronal enzymes required for dopamine synthesis are diminished.
-
D.
It is a pyramidal disorder.
-
A.
-
2.
The following in Parkinson’s disease (PD) are true except:
-
A.
In PD there are scattered neurons containing eosinophilic inclusions known as Lewy bodies which are the hallmark of the disease.
-
B.
Age of onset is between 60 and 70 years.
-
C.
The non-motor symptoms of PD are not important.
-
D.
The decision to treat does depend on factors such as age of the patient at onset, degree of disability and patient’s expectations, amongst others.
-
A.
-
3.
The following management options in PD are true except:
-
A.
L-Dopa is most effective.
-
B.
Dopamine agonists, bromocriptine and pergolide, are not used anymore because they are ergot alkaloids.
-
C.
Non-ergot dopamine agonists such as ropinirole and pramipexole cannot be used in combination with L-dopa.
-
D.
Side effects of ropinirole and pramipexole are a new set of compulsive behaviours such as gambling and hypersexuality.
-
A.
-
4.
The following statements relating to PD are true, except:
-
A.
Presently the more important surgical interventions are lesioning (thalamotomy) and deep brain stimulation.
-
B.
Stimulation of the ventral pallidus abolishes tremor.
-
C.
Stimulation of the ventrolateral nucleus of the thalamus relieves rigidity.
-
D.
Deep brain stimulation is ineffective and unsafe.
-
A.
MCQ Answers
1 = D; 2 = C; 3 = B; 4 = D
Extended Matching Questions (EMQ)
-
1.
Gastrointestinal effects are common to all dopaminergic medications, but there are side effects which are characteristic of certain drug types. Given below are the side effects. Chose the appropriate drug type to match the side effects.
-
A.
Ergoline dopamine agonist (bromocriptine, cabergoline, pergolide)
-
B.
Levodopa
-
C.
Non-ergoline dopamine agonist (pramipexole, ropinirole, rotigotine, apomorphine)
-
D.
Entacapone (COMT)
-
E.
MAO-B inhibitor (selegiline, rasagiline)
-
F.
Anticholinergic
Side effects
-
1.
Discoloration of urine
-
2.
Somnolence, oedema, compulsive behaviours(gambling, hypersexuality)
-
3.
Pleuropulmonary fibrosis, effusions, retroperitoneal fibrosis
-
4.
Cognitive, psychiatric and insomnia
-
5.
Hypotension, ‘wearing off’, dyskinesias
-
6.
Cognitive Effects
-
A.
EMQ Answers
1 = D; 2 = C; 3 =A; 4 = E; 5 = B; 6 = F
References
Obeso JA, Rodriguez-Oroz MC, Benitez-Temino B, Blesa FJ, Guridi J, Marin C, et al. Functional organisation of the basal ganglia: therapeutic implications for Parkinson’s disease. Mov Disord. 2008;23 Suppl 3:S548–59.
Weinberge M, Hutchison WD, Lozano AM, Hodale M,Dostrovsky JO. Increased gamma oscillatory activity in the subthalamic nucleus during tremor in Parkinson’s disease patients. J Neurophysiol. 2009;101(2);789–02.
Dickson DW. Parkinson’s disease and Parkinsonism: Neuropathology. Cold Spring Harbor Perspectives in Medicine. 2012.Cold Spring Laboratory Press. .
Thomas B, Beal MF. Parkinson’s disease Hum Mol Geriatr. 2007;16(Spec No2):R183–R194.
Schapira AHV. Recent advances in neurology 2013–2014; Eur J Neurol 2014;21:1425–1434.
Nakamura K, Edwards RH. Physiology versus pathology in Parkinson’s disease. Proc Nat Acad. Sci. http://www.pnas.org/content/104/29/11867.extract.
Chua CE, Tang BL. Alpha-synuclein and Parkinson’s disease: the first road block. J Cell Mol Med. 2006;10(4):837–s.
Glasson BI, Lee VM-Y. Parkin and molecular pathways of Parkinson’s disease. Neuron. 2001;31(6):885–888.
Dauer W, Przedborski S. Parkinson’s Disease. Neuron. 2003;39(6):889–909.
Outeiro TF, Lopes LV. Synaptic dysfunction in Parkinson’s disease: From protein misfolding to functional alterations. Folding for the synapse. Andreas Wyttenbach, Vincent O’Connor. Springer US. 2011;257–267.
Schapira AHV. Etiology of Parkinson’s disease. Neurology. 2006;66(10): suppl 4 S10–S23.
Bergman H, Deuschl G, Pathophysiology of Parkinson’s disease: from clinical neurology to basic neuroscience and back. Mov Disord. 2002;17 Suppl 3:S28–40.
Rivlin-Etzion M, Marmor O, Heimer G, Raz A, Nini A, Bergman H. Basal ganglia oscillations and pathophysiology of movement. Curr Opin Neurobiol. 2006;16(6):629–37.
Hornykiewicz O. Dopamine (3 hydroxytyramine) and function. Pharmacol Rev. 1966;1892:825–64.
Bergman H, Wichmann T, Karmon R, De Long MR. The primate subthalamic nucleus. II. Neuronal activity in the MPTP model of parkinsonism. J Neurophysiol. 1994;72:507–20.
Smith Y, Bevan MD, Shink E, Bolam JP. Microcircuitry of direct and indirect pathways of the basal ganglia. Neuroscience. 1998;86 (2):353–397.
Braak H, Del Tredici K, Rub U, de os RN, Steur E, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24:197–211.
Bostantjopulou S, Logothetis J, Katsarou Z, Mentenopoulos G. Clinical observations in early and late onset Parkinson’s disease. Funct Neurol. 1994;6(2):145–9.
Giovannini P, Piccolo I, Genitrini S, Soliveri P, Girotti F, Geminiani G, et al. Early-onset Parkinson’s disease. Mov Disord. 1991;6(1):36–42.
Arevalo GG, Jorge R, Garcia O, Scipioni G, Gershaniko O. Clinical and pharmacological differences in early versus late-onset Parkinson’s disease. Mov Disord. 1997; 12:277–284.
Friedman A. Old-onset Parkinson’s disease comparted with young-onset disease: clinical differences and similarities. Acta Neurol Scand. 1994; 89(4): 258–61.
Hindle JV. Ageing neurodegeneration and Parkinson’s disease. Age and Ageing. 2010;39(2):156–161
Tang H, Huang J, Nie K, Gan R,Wang L, Zhao J, et al. Cognitive profile of Parkinson’s disease patients: a comparative study between early onset and late onset Parkinson’s disease. Int J Neurosci. https://doi.org/10.3109/00207454.2015.1010646.
Bertucci Fiho D, Teive HA, Werneck LC. Early-onset Parkinson’s disease and depression. Arg Neuropsiquiatr. 2007;65(1):5–10.
Parkinson’s Disease Foundation. Parkinson’s Disease symptoms vary with age of disease onset. http://www.pdf.org/en/science_news/release/pr_1300644766. Accessed 27 October 2015.
Mehanna R, Moore S, Hou JG, Sarwar A, Lai EC. Comparing clinical features of young-onset, middle-onset and late-onset Parkinson’s Disease. Baylor College of Medicine.
Fereshtehnejad S-M, Hadizadeh H, Farhadi F, Shahidi GA, Delbari A, Lokk J. Comparison of the psychological symptoms and disease-specific quality of life between early and typical onset Parkinson’s disease patients. Parkinson’s Disease Vol 2014 (2014) Article ID 819260 7 pages. https://doi.org/10.1155/2014/819260.
Ramaker C, Marinus J, Stiggelbout AM, van Hilten BJ. Systematic evaluation of rating scales for impairment and disability in Parkinson’s Disease. Mov Disord. 2002;17(5):867–976.
Rascol O, Lozano A, Stern M, Poewe W. Milestones in Parkinson’s disease therapeutics. Mov Disord. 2011;26(6):102–82.
Lang AE, Lozano AM. Parkinson’s disease: first of two parts. N Engl J Med. 1998; 339(15):1044–53.
Lang AE, Lozano AM. Parkinson’s disease: second of two parts. N Engl J Med. 1998; 339 (16)1130–43.
Giladi N, Boroojerdi B, Korczyn AD, Burn DJ,Clarke CE,Schapira AH, SP513 Investigators. Rotigotine transdermal patch in early Parkinson’s disease: a randomized double-blind controlled study versus placebo and ropinirole. Mov Disord. 2007;22:2398–2404.
Hauser RA, Schapira AH, Rascol O, Barone P, Mozuno Y, Salin L. et al. Randomized double-blind multicentre evaluation of pramipexole extended-release once daily in early Parkinson’s disease. Mov Disord. 2010;25:2542–2549.
Fox SH. Non-dopamaminergic treatment for motor control in Parkinson’s disease. Drugs. 203;73(13):405–15.
Hughes A, Bishop DS, Kleedorfer B, Turjanski N, Fernandez W, Lees AJ, et al. Subcutaneous apomorphine in Parkinson’s disease: response to chronic administration for up to five years. Mov Disord. 1993;8:165–170.
DeMaagd G, Philip A. Part 2. Introduction to the pharmacotherapy of Parkinson’s disease, with focus on the use of dopaminergic agents. PT 2015;40(9):590–600.
Chen JJ, Swope DM. Parkinson’s disease. In DiPiro JT, Talbert RL, Yee GC, et al., editors. Pharmacotherapy: A Pathophysiologic Approach. 9th ed. New York, New York: McGraw-Hill; 2014.
Perez-Lloret S, Rascol O. Dopamine receptor agonists for the treatment of early or advanced Parkinson’s disease. CNS Drugs. 2010;24:941–968.
Jenner P. Dopamine agonists, receptor selectivity and dyskinesia induction in Parkinson’s disease. Curr Opin Neurol. 2003;16(suppl 1):S3-S7.
Wu L, Wang X, Cheng B. Parkinson’s disease. http://www.wustemvcells.com/en/clinicalcenter/parkinson_245142636.htm?gclid+CNO... accessed 6 November 2015.
Chaudhuri RK, Healy DG, Schapira HV. Non-motor symptoms of Parkinson’s disease: diagnosis and management. The Lancet Neurol. 2006;5:235–245.
Braak H, Braak E, Yilmazer D, Schultz C, De Vos RA, Jansen EN, et al. Nigral and extranigral pathology in Parkinson’s disease. J Neural Transmission Suppl 1995;46:15–3.
Ehrt U. Depressive symptom profile in Parkinson’s disease: a comparison with depression in elderly patients without Parkinson’s disease. Int J Geriatr Psychiatry. 2006; 21(3): 252–258.
Dubois B, Pillon B. Cognitive deficits in Parkinson’s disease. J Neurol. 1996; 44 (1):2–8.
Postuma RB, Gagnon JF, Vendite M, Charland K,Montplaisir J. Manifestations of Parkinson’s disease differ in associated with REM sleep disorder. Mov Disord. 2008; 25:1665–72.
Simuni T, Sethi K. Nonmotor symptoms of Parkinson’s disease. Ann Neurol. 2000; 64: 565–80.
Truong DD, Bhidayasiri R, Wolters E. Management of non motor symptoms in advanced Parkinson’s disease. J Neurol Sci. 2008;266: 216–28.
Long term effects. http://hmm.edu/programs/parkinsons-disease-related-movement-disorders-center/health/long-effects disorders-center/health/long-effects. Accessed on 28 October 2015.
Myalovitska O, Lobanova I. Generalized assessment of the impact of Parkinson’s disease on functional condition[version1:referees:2not approved]F1000Research 2013:2121 (https://doi.org/10.12688/11000research2-121v1).
Gallagher DA, Schrg A. Impact of newer pharmacological treatments on quality of life in patients with Parkinson’s disease. CNS Drugs. 2008;22(7):563–86.
Scheife RT, Schumock GT, Burstein A, Gottwald MD, Luer MS. Impact of Parkinson’s disease and its pharmacologic treatment on quality of life and economic outcomes. Am J Health Syst.Pharm. http://www.medscape.com/viewarticle/406885 accessed 28 October 2015.
Dowding CH, Shenton CL, Salek SS. A review of the health-related quality of life and economic impact of Parkinson’s disease. Drugs Aging. 2006;23(9):693–721.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this entry

Cite this entry
Nagaratnam, N., Nagaratnam, K., Cheuk, G. (2018). Parkinson’s Disease. In: Geriatric Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-33434-9_42
Download citation
DOI: https://doi.org/10.1007/978-3-319-33434-9_42
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33433-2
Online ISBN: 978-3-319-33434-9
eBook Packages: MedicineReference Module Medicine